Back to Journals » Clinical and Experimental Gastroenterology » Volume 17
Acute Necrotizing Pancreatitis Complicated with Paroxysmal Nocturnal Haemoglobinuria: A Case Report
Authors Xiao M ![]() , Di Y, An Y, Cui Y
, Di Y, An Y, Cui Y
Received 28 November 2023
Accepted for publication 16 April 2024
Published 29 April 2024 Volume 2024:17 Pages 141—145
DOI https://doi.org/10.2147/CEG.S449594
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Andreas M. Kaiser
Mengbo Xiao,1 Ying Di,1 Yu An,1 Yunfeng Cui2
1Tianjin Medical University, Tianjin, People’s Republic of China; 2Department of Hepatobiliary and Pancreatic Surgery, Department of Surgery, Tianjin Nankai Hospital, Nankai Clinical School of Medicine, Tianjin Medical University, Tianjin, People’s Republic of China
Correspondence: Yunfeng Cui, Department of Hepatobiliary and Pancreatic Surgery, Department of Surgery, Tianjin Nankai Hospital, Nankai Clinical School of Medicine, Tianjin Medical University, 6 Changjiang Road, Nankai District, Tianjin, 300100, People’s Republic of China, Tel +86-150-2263-3356, Email [email protected]
Abstract: This report presents a unique case of acute necrotizing pancreatitis(ANP) concomitant with paroxysmal nocturnal hemoglobinuria(PNH), a combination that has not been documented in existing literature. The impact of PNH on ANP and its treatment remains uncertain due to the lack of consensus. The case described herein involves a patient who exhibited both ANP and PNH, subsequently experiencing splanchnic vein thrombosis (SVT), resulting in substantial intra-abdominal and gastrointestinal hemorrhaging. We attempted to analyze the role of PNH in the formation of SVT in ANP and propose some new insights and hypotheses for the treatment of such patients.
Keywords: acute necrotizing pancreatitis, paroxysmal nocturnal hemoglobinuria, splanchnic vein thrombosis
Introduction
Acute pancreatitis is a disease characterized by the activation of pancreatic enzymes due to various causes, resulting in local or systemic inflammatory reactions in the pancreas, with or without associated organ dysfunction.1 Acute necrotizing pancreatitis(ANP) is a more severe form, defined as pancreatic parenchymal necrosis with or without involvement of surrounding tissues, and is associated with a high morbidity and mortality rate.2,3
Paroxysmal nocturnal hemoglobinuria(PNH) is an acquired hematopoietic disorder associated with a somatic mutation in the phosphatidylinositol glycan class A (PIG-A) gene on the X chromosome.4 PNH is characterized by intravascular hemolysis, manifested by paroxysmal episodes of hemoglobinuria and life-threatening venous thrombosis formation.4
We report a case of ANP complicated with PNH in a patient who rapidly developed splanchnic vein thrombosis (SVT) and later experienced severe complications such as intra-abdominal hemorrhaging and gastrointestinal hemorrhaging.
Case Report
A 39-year-old male patient was admitted to the emergency department of our hospital with acute abdominal pain. On admission, his amylase level was 1809 U/L. A computed tomography (CT) of the abdomen revealed diffuse edema of the pancreas, peripancreatic effusion, and gallbladder stones (Figure 1). In the last four weeks, the patient still had symptoms such as fever and chills, suggesting that the infection in and around the pancreas was not effectively controlled. The 2019 WJES (World Journal of Emergency Surgery) guidelines for acute pancreatitis state that CE-CT scanning is recommended when the clinical status worsens or shows no sustained improvement, or when invasive interventions are considered.5 Contrast-enhanced CT was performed to identify the patient’s abdominal and retroperitoneal infection, to determine whether pancreatic necrosis was present, and to determine whether more aggressive invasive intervention was needed. The abdominal enhanced CT scan conducted on the patient twenty-seven days post-admission exhibited the existence of patchy regions lacking contrast enhancement in the neck of the pancreas, implying the occurrence of pancreatic necrosis. Moreover, the presence of venous thrombosis in the splenic vein, portal vein, and superior mesenteric vein was indicated by the findings (Figure 2). Additionally, cuneiform low-density shadows were observed in a patchy distribution within the spleen, aligning with the characteristics of splenic infarction. It is puzzling that despite the patient having a severe abdominal infection for a long period of time and frequently experiencing fever symptoms, the patient’s white blood cell does not match the symptoms (WBC 2.61 × 109/L). The patient’s red blood cell and neutrophil counts are even slightly lower than normal, and the reticulocyte counts is higher than normal (RBC 1.28× 1012/L, NEUT 1.21×109/L, RET 0.12×1012/L). Additionally, we also noted that the patient’s previous urine occult blood tests had shown positive results multiple times. It raised our suspicion of a hematologic disorder in the patient. Upon further detailed inquiry into the patient’s medical history, we learned that the patient had previously experienced haemoglobinuria and lower back pain before the current illness. We highly suspect that the patient has PNH. To confirm this diagnosis, we performed peripheral blood flow cytometry according to guidelines. The test result confirmed that the patient indeed had PNH (Figure 3). During the second week of the patient’s illness, an ultrasonography-guided abdominal puncture was performed in the area around the head and neck of the pancreas, which drained a reden-brown peripancreatic fluid collection rather than necrotic pancreatic tissue and pus. However, later in the patient’s illness, there was purulent fluid outflow from this duct, which also confirmed the diagnosis of pancreatic neck necrosis on enhanced CT on day 27. On the basis of the contrast-enhanced CT obtained on day 27, CT-guided retroperitoneal puncture was performed at week 4, and minimally invasive pancreatic necrosectomy was performed at week 7. On the morning of the third day after surgery, bright red blood with a volume of about 300mL appeared around the abdominal incision and drainage tube, and coffee-colored fluid flowed from the gastrointestinal decompression tube of the patient. On the second day after bleeding, the patient’s stool was black, and the fecal occult blood test was positive. Subsequently, the patient underwent digital subtraction angiography (DSA) to identify the source of bleeding, but no identifiable arterial bleeding was observed. The hemorrhage ceased following interventions including gauze compression, administration of hemocoagulase and norepinephrine saline through the drainage tube, infusion of omeprazole, and blood transfusion. We considered bleeding from a rupture of a certain splanchnic vein, but unfortunately we did not have definitive evidence. Following CT-guided abdominal puncture drainage, minimally invasive pancreatic necrosectomy, and other surgical interventions, along with conventional anti-infective measures and nutritional support, the patient’s condition improved and was discharged. Subsequent CT examination conducted six months later revealed a significant amelioration in peripancreatic exudation and complete resolution of necrotic tissue in the pancreatic neck (Figure 4).
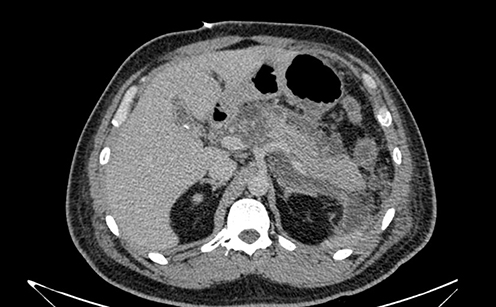 |
Figure 1 The CT showed diffuse edema of the pancreas, accompanied by peripancreatic fluid collection and gallstones. |
 |
Figure 2 The abdominal enhanced CT results indicate the presence of venous thrombosis in the splenic vein, portal vein, and superior mesenteric vein. |
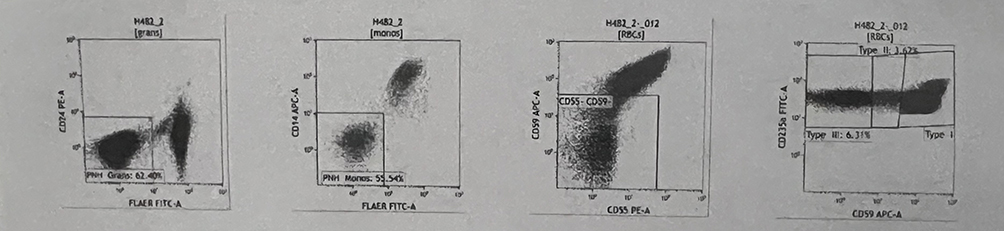 |
Figure 3 The patient has been diagnosed with PNH (paroxysmal nocturnal hemoglobinuria) through flow cytometry. |
 |
Figure 4 The CT scan shows a significant improvement in peripancreatic effusion, and the area of necrosis in the neck of the pancreas has noticeably decreased compared to before. |
To address the patient’s PNH, SVT, and the associated risk of secondary thrombosis and severe vascular complications, a comprehensive treatment approach was employed. This included the administration of anticoagulant medications to prevent thrombosis, infusion of granulocyte colony-stimulating factor (G-CSF) and oral leucogen to enhance white blood cell and platelet counts, and infusion of red blood cells, iron, and folic acid to ameliorate anemia. Additionally, hormone pulse therapy was utilized to mitigate the progression of PNH.
Discussion
We believe that PNH plays an important role in the formation of splenic vein, portal vein, and superior mesenteric vein thrombosis in this patient, which together with ANP leads to the formation of venous thrombosis.
SVT is a commonly observed complication of acute pancreatitis, with an incidence ranging from 1.8% to 22.6%. The main pathophysiological mechanisms of pancreatitis-associated SVT may include: (a) The pancreas exhibits swelling and necrosis, and the infiltration of inflammation in the vicinity can directly affect the visceral veins, resulting in damage to the vascular endothelium. The local spread of severe acute pancreatitis’s inflammatory process can affect neighboring blood vessels, leading to the weakening of vessel walls and the obstruction of blood flow due to the presence of proteolytic enzymes. (b) The enlargement of the pancreas and/or the formation of pseudocysts exert pressure on sclerotic veins, leading to the stagnation of blood flow and subsequently promoting the occurrence of venous thrombosis. (c) Increased concentrations of inflammatory mediators have the potential to trigger the activation of the coagulation system, leading to the accumulation of platelets and thrombin-rich fibrin, thereby instigating the occurrence of venous thrombosis. (d) The release of tissue factor directly into the bloodstream from the impaired pancreas serves as the catalyst for a series of coagulation reactions.
PNH is characterized by acute or chronic intravascular hemolysis, particularly occurring during nighttime, bone marrow failure, and thrombotic events.6 The most severe complication associated with PNH is thrombosis. In 85% of cases, thrombosis originates from venous sources, while arterial sources account for 15% of cases, and 20.5% of cases involve multiple sites simultaneously. Previous instances of SVT resulting from PNH have also been documented.7,8 Platelet activation, complement-mediated hemolysis, impaired nitric oxide (NO) bioavailability, impairment of the fibrinolytic system, and inflammatory mediators have been postulated as potential mechanisms underlying the heightened thrombotic risk observed in patients with PNH.9
PNH is a relatively rare disease in the hematological system. The occurrence of PNH in patients with ANP increases the possibility of SVT, leading to poor prognosis. Based on this case, we believe that we should be alert to the results of blood tests that are not consistent with the patient’s infectious symptoms, and ask the patient’s medical history in detail to rule out the possibility of the patient’s blood system. We do not recommend bone marrow aspiration, flow cytometry, and other tests to confirm the diagnosis of blood diseases without relevant evidence. When SVT is found in imaging examination, we should not only consider that SVT is a complication of ANP, but also consider whether SVT is caused by other diseases that can cause splanchnic venous thrombosis. Once the cause is identified, timely treatment should be performed.
The presence of PNH in cases of ANP may elevate the likelihood of SVT, thereby amplifying the potential for severe outcomes such as gastrointestinal bleeding and abdominal bleeding resulting from SVT, ultimately increasing the risk of mortality. To prevent or delay the further progression of PNH in an infection state, a variety of targeted measures should be taken. In addition, anticoagulant drugs should be taken at an early stage of the disease in order to improve coagulation and prevent thrombosis formation. Necrotizing pancreatitis infected with bacteria is currently treated with a minimally invasive step-up approach that starts with catheter drainage. International guidelines advocate for deferring catheter drainage and antibiotic administration until the infected pancreas and peripancreatic necrosis have become encapsulated, a process known as walled-off necrosis that typically requires approximately four weeks to occur.10 Further research and discussion are necessary to determine the necessity of implementing more proactive intervention measures for the prevention of SVT and severe vascular complications in patients diagnosed with ANP complicated with PNH.
Ethics and Consent Statement
The authors declare that the case details in this case report do not require any institutional approval for publication. Written informed consent about the case report and accompanying images was obtained from the patient for publication of this report.
Funding
This case report was supported by: 1. China Medical and Health Development Foundation, Young and Middle-aged Doctors Excellent Talent, Pei Ying Program, Clinical study on prevention and treatment of exocrine pancreatic insufficiency associated with severe acute pancreatitis. 2. Tianjin Nankai Hospital integrated Traditional Chinese and Western medicine prevention and treatment key technology and program optimization 2022 key project, A multi-omics study of the microenvironment of abdominal inflammation in acute pancreatitis based on minimally invasive individualized integrated traditional Chinese and Western Medicine surgical treatment system, NKYY-IIT-2022-009-2. 3. Tianjin key areas of traditional Chinese medicine science and technology project, Clinical study of combined treatment of TCM and Western medicine with pancreato-intestinal therapy based on peritoneal microecology in the treatment of acute pancreatitis 2022005. 4. Tianjin Natural Science Foundation key project, Establishment of individualized surgical treatment system for severe acute pancreatitis and intelligent evaluation of multimodal imaging. 5. Tianjin Administration of Traditional Chinese Medicine fund of traditional Chinese and Western medicine integrated research project, Study on the change of peritoneal microecology in acute pancreatitis and the effect of Qingyi Decoction 2021006. 6. Tianjin 131 innovative talent team, innovation team for Diagnosis and treatment of acute abdomen related to biliary and pancreatic diseases 201938.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Harris S, Nadkarni NA, Naina HV, Vege SS. Splanchnic vein thrombosis in acute pancreatitis: a single-center experience. Pancreas. 2013;42(8):1251–1254. doi:10.1097/MPA.0b013e3182968ff5
2. Lankisch PG, Apte M, Banks PA. Acute pancreatitis. Lancet. 2015;386(9988):85–96. doi:10.1016/S0140-6736(14)60649-8
3. Shah AP, Mourad MM, Bramhall SR. Acute pancreatitis: current perspectives on diagnosis and management. J Inflamm Res. 2018;11:77–85. doi:10.2147/JIR.S135751
4. Hillmen P, Lewis SM, Bessler M, Luzzatto L, Dacie JV. Natural history of paroxysmal nocturnal hemoglobinuria. N Engl J Med. 1995;333(19):1253–1258. doi:10.1056/NEJM199511093331904
5. Leppäniemi A, Tolonen M, Tarasconi A, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019;14(1):27. doi:10.1186/s13017-019-0247-0
6. Peacock-Young B, Macrae FL, Newton DJ, Hill A, Ariëns RAS. The prothrombotic state in paroxysmal nocturnal hemoglobinuria: a multifaceted source. Haematologica. 2018;103(1):9–17. doi:10.3324/haematol.2017.177618
7. Gupta A, Al Fulaij R, Gupta RK, Gupta G, Marouf R. Development of paroxysmal nocturnal haemoglobinuria in systemic lupus erythematosus: an unusual cause of portal vein thrombosis. Lupus. 2009;18(8):743–746. doi:10.1177/0961203308100558
8. Tedde R, Sechi LA, Marigliano A, Loriga V. [Paroxysmal nocturnal hemoglobinuria with multiple venous thrombosis and acute renal insufficiency. Description of a case]. Minerva Med. 1989;80(6):615–618. Italian.
9. Hill A, Kelly RJ, Hillmen P. Thrombosis in paroxysmal nocturnal hemoglobinuria. Blood. 2013;121(25):4985–4996. doi:10.1182/blood-2012-09-311381
10. Boxhoorn L, van Dijk SM, van Grinsven J, et al. Immediate versus postponed intervention for infected necrotizing pancreatitis. N Engl J Med. 2021;385(15):1372–1381. doi:10.1056/NEJMoa2100826
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.