Back to Journals » International Medical Case Reports Journal » Volume 16
Acute Liver Failure Caused by Secondary Hemophagocytic Lymphohistiocytosis After COVID-19 Vaccination – Case Report and Literature Review
Authors Premec H ![]() , Živko M
, Živko M ![]() , Mijić M, Jelić-Puškarić B, Lalovac M, Filipec Kanižaj T, Sobočan N
, Mijić M, Jelić-Puškarić B, Lalovac M, Filipec Kanižaj T, Sobočan N
Received 26 May 2023
Accepted for publication 22 July 2023
Published 7 August 2023 Volume 2023:16 Pages 449—455
DOI https://doi.org/10.2147/IMCRJ.S417347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Hrvoje Premec,1 Matea Živko,2 Maja Mijić,1 Biljana Jelić-Puškarić,3,4 Miloš Lalovac,1,5 Tajana Filipec Kanižaj,1,2 Nikola Sobočan1,2
1Department of Gastroenterology, University Hospital Merkur, Zagreb, Croatia; 2School of Medicine, University of Zagreb, Zagreb, Croatia; 3Department of Pathology and Cytology, University Hospital Merkur, Zagreb, Croatia; 4School of Medicine, Catholic University of Croatia, Zagreb, Croatia; 5University of Dubrovnik, Dubrovnik, Croatia
Correspondence: Nikola Sobočan, Email [email protected]
Abstract: Hemophagocytic lymphohistiocytosis (HLH) is a congenital or acquired hyperinflammatory syndrome, in some cases accompanied by acute liver failure. We present a case report of acute liver failure associated with HLH after COVID-19 vaccination and bring a literature review of the connection between HLH and COVID-19 vaccination. HLH has significant mortality rate, and liver transplantation is not a therapeutic option. Therefore, early recognition and timely conservative treatment are corner stones in reducing HLH-related morbidity and mortality.
Keywords: hemophagocytic lymphohistiocytosis, acute liver failure, COVID-19 vaccine, multisystem inflammatory syndrome
Introduction
Acute liver failure (ALF) is a condition of severe liver damage accompanied by jaundice, coagulopathy, elevated liver enzymes and encephalopathy, without any signs of previous liver disease.1 Drug-induced liver failure (DILI) is the most common cause of ALF in developed countries, viral hepatitis being the most common cause globally, while the cause is unknown in a third of cases.2,3 The coronavirus disease 2019 (COVID 19) pandemic has led to a rapid development of vaccines with different mechanisms of action. The most commonly used vaccines in Europe are those based on messenger RNA BNT162b2 (Pfizer-BioNTech) and mRNA-1237 (Moderna Therapeutics) or DNA vaccines utilising adenoviral vectors ChAdOx1 nCov-19 (AstraZeneca-Oxford) and Ad26.COV2.S (Janssen-Johnson and Johnson).4–6 Although vaccines decreased COVID-19 associated mortality, various side effects have been reported after vaccination, mostly mild (myalgia, headache, fever, fatigue, injection site pain).4,5 However, more serious haematological complications were reported in the form of thrombotic immune thrombocytopenia after ChAdOx1 nCov-19 and multisystem inflammatory syndrome (MIS-V) after BNT162b2 vaccination.7,8
Hemophagocytic lymphohistiocytosis is a congenital or acquired hyperinflammatory syndrome caused by excessive activation of macrophages and cytotoxic T lymphocytes. Liver damage of various stages occurs in most patients, but HLH rarely results in acute liver failure when it comes to adult patients.3,9 We bring a case report of a patient with acute liver failure caused by secondary HLH that occurred due to the use of a DNA vector vaccine against COVID-19.
Case Presentation
The 61-year-old patient is Caucasian, with a past history of arterial hypertension and Warthin’s right parotid gland tumour. Fever occurred ten days after receiving viral vector vaccine against COVID-19 (Ad26.COV2.S). The patient was examined in the outpatient clinic and given amoxicillin orally. Due to a persistent fever up to 40°C, algic syndrome and diarrhoea, the patient was admitted to a local hospital. Upon admission, the laboratory findings showed leukocytosis (13.2 x109/L), mildly elevated liver enzymes (AST 52 U/L; ALT 90 U/L), along with a normal INR range and renal function. Viral hepatitis (A, B, C) and HIV were excluded. Immunological analysis revealed a decreased level of the complement component 4, ANA was negative and immunoelectrophoresis test was in the normal range. Abdominal MSCT scan showed hepatosplenomegaly. Blood and urine cultures remained sterile. The patient was treated empirically and given multiple intravenous antibiotics (cefuroxime, ciprofloxacin, metronidazole, piperacillin/tazobactam). Consequently, Clostridium difficile toxin antigen was isolated from the stool and vancomycin was administered orally. After vancomycin treatment, diarrhoea stopped and repeated C. difficile test was negative. Despite empiric and targeted antibiotic therapy, fever was still present. Although bone marrow aspirate revealed no signs of hemophagocytosis, HLH was suspected and Dexamethasone (20 mg IV) was introduced on the twelfth day of hospitalisation, after which the patient was afebrile. An increase in liver enzymes was noted starting on day 7 of hospitalisation (AST 224 U/L; ALT 194 U/L), reaching its peak value on day 14 (AST 3658 U/L; ALT 4494 U/L), joined by the development of jaundice (total bilirubin 139 µmol/L), coagulation disorder (INR 2.71) and portal systemic encephalopathy (WH 3). The dynamic of serum transaminases is shown in Figure 1 and the dynamic of serum bilirubin and INR in Figure 2.
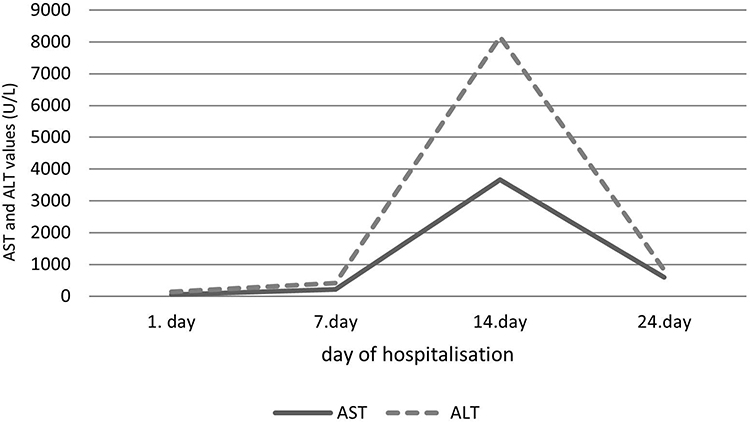 |
Figure 1 Dynamic of serum AST, ALT values in a patient with secondary HLH during hospitalisation. |
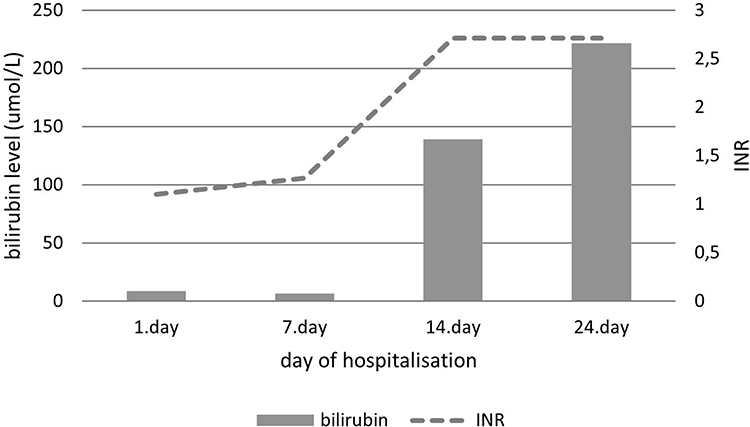 |
Figure 2 Dynamic of INR and serum bilirubin values in a patient with secondary HLH during hospitalisation. |
The patient was transferred to our tertiary referral centre on day 20 of hospitalisation, and transplantation treatment of acute liver failure was considered. The laboratory workup was repeated and leukocytosis (12.5x109/L), anemia (82 g/L), thrombocytopenia (82x109/L), hypofibrinogenemia (1.3 g/L), coagulation disorder (INR 2.0), elevated values of D-dimers (18.3 mg/L), hyperbilirubinemia (344 µmol/L) and increased serum creatinine level (201 µmol/L) were confirmed. The serum ferritin value was 12,954 µg/L. The patient had encephalopathy and jaundice, with palpable hepatomegaly. A mild pretibial oedema was found.
In order to rule out infiltrative liver disease, a transjugular liver biopsy was performed, and submassive liver necrosis was found in the pathohistological sample. Bone marrow aspiration was repeated, and a high number of phagocytes was found in aspirate smears, along with individual cytophages (Figure 3). A haematologist was involved in the treatment. H-score value was 186 (75% probability of HLH diagnosis) with 6 out of 8 criteria of HLH-2004 (fever, splenomegaly, bicytopenia, low fibrinogen level, hemophagocytosis in bone marrow aspirate and high ferritin level), resulting in the diagnosis of HLH. (4) Dexamethasone treatment was continued (40 mg i.v. per day) with the addition of intravenous immunoglobulins (2g/kg). Despite such treatment, the patient’s clinical condition rapidly deteriorated, and on the fourth day of transfer, the patient fell into refractory vasodilatory shock, followed by the development of acute respiratory insufficiency and cardiorespiratory arrest. Despite intensive treatment measures, the patient died 46 days after vaccination.
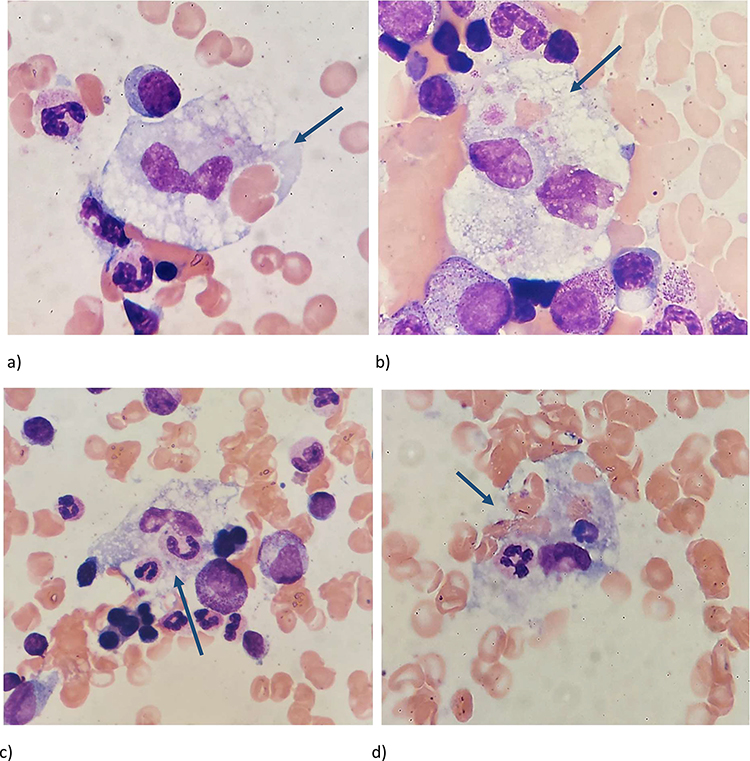 |
Figure 3 Figures description in order of appearance (a–d): Repeated bone marrow aspirate smears: The arrow points macrophages ingesting erythrocytes (a,b and d) and neutrophils (c and d), May Grunwald-Giemsa staining, ×1000. |
Discussion
There is a growing recognition of hemophagocytic lymphohistiocytosis among adult patients of all age groups.10 HLH is divided into two forms - primary/familial and secondary/acquired (sHLH). Mutations in the genes controlling the cytolytic function and survival of lymphocytes cause the primary form of the disease, while the secondary form of the disease is most often provoked by chronic inflammation, immunosuppression, infections, malignancies, drugs and vaccines. Primary HLH mostly occurs among children, although it may also occur among adolescents and young adults, while sHLH is most common among adults. Hemophagocytic lymphohistiocytosis is characterised by blood cytopenias, hepatocellular injuries, coagulopathy, and in severe cases, signs of multiorgan system failure.9 High fever, arthralgia and lymphadenopathy persisting without a clear infectious focus and despite adequate antimicrobial therapy should arouse suspicion of HLH. There are no clinical or laboratory parameters that can unambiguously establish the diagnosis of HLH.10 Currently, the diagnosis of secondary forms of HLH is based on the HLH-2004 criteria, although they are initially intended to include children with the primary form of the disease in clinical trials.
The diagnosis of HLH must include 5 of the following 8 elements of the HLH-2004 criteria: fever, splenomegaly, cytopenia affecting at least two blood cell lines, hypertriglyceridemia and/or hypofibrinogenemia, hemophagocytosis, hyperferritinemia, high levels of sIL-2R, and low NK cell activity levels.9,11 A diagnosis of non-familial forms of the disease can be made using the online available H-score (http://saintantoine.aphp.fr/score/).12 Multisystem inflammatory syndrome in children (MIS-C), which is caused by a dysregulated immune response to SARS-CoV-2 infection, is closely related to HLH.13 MIS-C develops in children, 4–6 weeks after probable SARS-CoV-2 infection, with signs of cardiac shock and involvement of the respiratory, gastrointestinal system alongside mucocutaneous changes. More recently, a similar clinical picture occurring up to 12 weeks after confirmed COVID-19 in patients older than 21 years without respiratory symptoms was recognized as a separate entity – multisystem inflammatory syndrome in adults (MIS-A).14 Lately, the development of a syndrome similar to MIS-A/C, after mRNA and inactivated vaccine exposure, called MIS-V, has been described in the literature. The pathophysiology of MIS-V probably reflects those of MIS-C/A.7,15 The aberrant immune response to vaccination, in addition to being linked to the development of MIS-V, is also associated with the development of antibodies resembling those recognising PF4-heparin complex. The described antibodies can cause atypical thrombosis and pronounced thrombocytopenia 1–2 weeks after vaccination with ChAdOx1 nCov-19, an entity called vaccine-induced thrombotic thrombocytopenia (VITT).8
Liver injury is a common complication of HLH and is reported in about 85% of patients with a secondary form of the disease in earlier studies, the injury usually following the course of the disease.3,9,16,17 In most patients, only a slight increase in AST and ALT is present, although progression to acute liver failure is possible as a result of multiple-organ failure and lymphocytic infiltration of the periportal liver spaces with hepatic parenchyma necrosis.18–20
Liver transplantation is not an accepted method of treating ALF caused by HLH.3 Wright et al presented a case of a patient who underwent an ALF transplant based on unrecognised secondary HLH, and the said patient died three weeks after transplant.21 The key point in the treatment of secondary forms of HLH is early identification of the causative agent. By performing extensive diagnostic treatments on our patient, no autoimmune or malignant provoking factors were found. Clostridium difficile infection rarely triggers secondary HLH. To our best knowledge, three cases were described, exclusively in immunosuppressed patients (long-term corticosteroid therapy due to earlier HLH, NKT lymphoma, and ulcerative colitis therapy with 6-mercaptopurine).22 Our patient was immunocompetent, which alongside a clinical and microbiological resolution of the C. difficile infection after vancomycin therapy, makes it unlikely C. difficile infection being provoking factor. A possible limitation of our case report is the absence of Epstein–Barr viremia confirmation in the context of urgent need for pretransplantation work-up. Epstein–Barr virus is a commonly present provoking factor in setting of sHLH in adults. However, sHLH in most occasions is induced by EBV reactivation in immunocompromised patients.9,23 Prior to vaccination, our patient had no clinical signs of acute viral illness nor immune deficiency, and therefore we believe that although EBV infection or reactivation is possible, it is unlikely the provoking factor. Considering all mentioned, it was suspected that the recent vaccination with a DNA vector vaccine against COVID-19 triggered HLH. Seventeen cases of secondary HLH caused by COVID-19 vaccine were found in the available literature. All patients were vaccinated with mRNA, DNA vector or inactivated vaccines, nine of which male and eight of which female patients aged 20 to 85 years. All patients satisfied H-score. The symptoms occurred after vaccination, from the day of vaccination until the 21st day after vaccination.24–33
Acute liver failure was the predominant presentation in a 24-year-old female patient without significant comorbidities after BNT162b2 vaccination. Sixteen days after vaccination, the patient developed a clinical picture of HLH (H-score 259, >99% HLH probability), and she was treated with intravenous immunoglobulins from the 24th day of the disease with the addition of intravenous dexamethasone from the 29th day. Despite the therapy, she developed acute liver failure on day 30.33
Most of other patients were treated with pulse steroid therapy, with the addition of intravenous immunoglobulins.24–33 The effectiveness of the IL-1 blocker, ie, anakinra, in refractory cases is particularly noteworthy.24,33
The above-mentioned patient received anakinra from the 29th to the 41th day with a good clinical and biochemical response.33 We found an additional case of a 33-year-old patient without significant comorbidities, who was hospitalised 58 days after the second dose of BNT162b2 due to intermittent fever, pancytopenia and elevated liver enzymes. Initially, a diagnosis of adult-onset Still disease (AOSD) was suspected, so a corticosteroid therapy was initiated with a clinical improvement. The patient was followed up outpatient. After tapering the dose of corticosteroids, the patient developed fever, arthralgia, rash and jaundice, which resulted in hospitalisation one month after the initial one. The therapy which included corticosteroids, anakinra and intravenous immunoglobulins was initiated without clinical response. H-score was 274 (>99% HLH probability). Therefore, treatment is initiated on HLH 2004 protocol (etoposide and dexamethasone). However, acute liver failure developed and etoposide was discontinued with an unfavourable outcome.34
Mortality among adult patients with HLH ranges from 42% to 88%, while mortality among reported patients with secondary HLH induced by COVID-19 vaccine was 22% (4/18 patients).24–34
The pathophysiological mechanism beneath sHLH development after vaccination is not fully understood. HLH is caused by a positive feedback loop between macrophages, activated CD8+ T cells and antigen-presenting cells. They stimulate each other, leading to a “cytokine storm”. The inability to neutralize viruses and other intracellular pathogens causes persistent antigenic stimulation of T cells.9 Adenovirus, utilised as a vector in DNA vaccines, enters the host cells, where part of virus DNA and spike protein SARS-CoV-2 are translated into respective proteins, inducing host cellular and humoral responses.35 It is proposed that up-regulated secretion of interleukin 1 beta (IL-1-beta) from macrophages in response to the spike protein encoded by the mRNA vaccine is responsible for hyperinflammatory syndrome development after SARS-CoV-2 mRNA vaccination.33 In the case of DNA adenoviral vector vaccines, we assume that hyperinflammatory syndrome arises as a result of a similar mechanism or due to hyperimmune host response to the adenoviral components of the vaccine.
Conclusion
HLH in adults is difficult to diagnose and the mortality rate is high. Early recognition, as well as an early start of treatment, are key to a good and favourable outcome. The disease can progress to ALF, and in that case, a transplant treatment is not an option. It can be concluded that one of the possible etiological factors in adults might be the currently available COVID-19 vaccines.
Abbreviations
ALF, acute liver failure; ALT, alanine aminotransferase; AST, aspartate aminotransferase; ANA, antinuclear antibody; HLH, hemophagocytic lymphohistiocytosis; IL-1, interleukin 1; INR, international normalized ratio; MIS-C/A, multisystem inflammatory syndrome in children/adults; MIS-V, multisystem inflammatory response after vaccination; MSCT, multi-slice computed tomography; NK, natural killer cells; PF4, platelet factor 4; SARS-CoV-2, severe acute respiratory syndrome corona virus 2; sIL-2R, soluble interleukin 2 receptor; VITT, vaccine induced thrombotic thrombocytopenia; WH, West Haven.
Ethics
The patient signed informed consent, on the day of admission to hospital, regarding the use of their medical information for scientific purposes. Despite our best efforts to contact the patient’s next of kin for consent to publish, they are lost to follow-up. The Editor-in-Chief has approved the publication of this case based on COPE guidelines. Given information presented in this case report, institutional approval was not required to publish the case details.
Disclosure
The authors have no conflict of interest to declare for this work.
References
1. Kumar R, Anand U, Priyadarshi RN. Liver transplantation in acute liver failure: dilemmas and challenges. World J Transplant. 2021;11(6):187–202. doi:10.5500/wjt.v11.i6.187
2. Bernal W, Wendon J. Acute liver failure. N Engl J Med. 2013;369:2525–2534. doi:10.1056/NEJMra1208937
3. Lin S, Li Y, Long J, Liu Q, Yang F, He Y. Acute liver failure caused by hemophagocytic lymphohistiocytosis in adults: a case report and review of the literature. Medicine. 2016;95(47):e5431. doi:10.1097/MD.0000000000005431
4. Gee J, Marquez P, Su J, et al. First Month of COVID-19 vaccine safety monitoring - United States, December 14, 2020-January 13, 2021. MMWR Morb Mortal Wkly Rep. 2021;70(8):283–288. doi:10.15585/mmwr.mm7008e3
5. Bae S, Lee YW, Lim SY, et al. Adverse Reactions Following the First Dose of ChAdOx1 nCoV-19 Vaccine and BNT162b2 Vaccine for Healthcare Workers in South Korea. J Korean Med Sci. 2021;36(17):e115. doi:10.3346/jkms.2021.36.e115
6. COVID-19 vaccine tracker. European center for disease prevention and control; 2023. Available from: https://vaccinetracker.ecdc.europa.eu/public/extensions/COVID-19/vaccine-tracker.html#distribution-tab.
7. Nune A, Iyengar KP, Goddard C, Ahmed AE. Multisystem inflammatory syndrome in an adult following the SARS-CoV-2 vaccine (MIS-V). BMJ Case Rep. 2021;14(7):e243888. doi:10.1136/bcr-2021-243888
8. Greinacher A, Thiele T, Warkentin TE, Weisser K, Kyrle PA, Eichinger S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N Engl J Med. 2021;384(22):2092–2101. doi:10.1056/NEJMoa2104840
9. Griffin G, Shenoi S, Hughes GC. Hemophagocytic lymphohistiocytosis: an update on pathogenesis, diagnosis, and therapy. Best Pract Res Clin Rheumatol. 2020;34(4):101515. doi:10.1016/j.berh.2020.101515
10. La Rosée P, Horne A, Hines M, et al. Recommendations for the management of hemophagocytic lymphohistiocytosis in adults. Blood. 2019;133(23):2465–2477. doi:10.1182/blood.2018894618
11. Henter JI, Horne A, Aricó M, et al. HLH-2004: diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007;48(2):124–131.
12. Fardet L, Galicier L, Lambotte O, et al. Development and validation of the HScore, a score for the diagnosis of reactive hemophagocytic syndrome. Arthritis Rheumatol. 2014;66(9):2613–2620. doi:10.1002/art.38690
13. Kumar D, Rostad CA, Jaggi P, et al. Distinguishing immune activation and inflammatory signatures of multisystem inflammatory syndrome in children (MIS-C) versus hemophagocytic lymphohistiocytosis (HLH). J Allergy Clin Immunol. 2022;149(5):1592–606.e16. doi:10.1016/j.jaci.2022.02.028
14. Vogel TP, Top KA, Karatzios C, et al. Multisystem inflammatory syndrome in children and adults (MIS-C/ A): case definition & guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine. 2021;39(22):3037–3049. doi:10.1016/j.vaccine.2021.01.054
15. Brown M, Garbajs NZ, Zec S, et al. A case of adult multisystem inflammatory syndrome following COVID-19 vaccine. J Community Hosp Intern Med Perspect. 2022;12(4):7–13. doi:10.55729/2000-9666.1087
16. Li J, Wang Q, Zheng W, et al. Hemophagocytic lymphohistiocytosis: clinical analysis of 103 adult patients. Medicine. 2014;93:100–105. doi:10.1097/MD.0000000000000022
17. Otrock ZK, Eby CS. Clinical characteristics, prognostic factors, and outcomes of adult patients with hemophagocytic lymphohistiocytosis. Am J Hematol. 2015;90:220–224. doi:10.1002/ajh.23911
18. Mayordomo-Colunga J, Rey C, Gonzalez S, et al. Multiorgan failure due to hemophagocytic syndrome: a case report. Cases J. 2008;1:209. doi:10.1186/1757-1626-1-209
19. Li F, Yang Y, Jin F, et al. Clinical characteristics and prognostic factors of adult hemophagocytic syndrome patients: a retrospective study of increasing awareness of a disease from a single-center in China. Orphanet J Rare Dis. 2015;10:20. doi:10.1186/s13023-015-0224-y
20. Ost A, Nilsson-Ardnor S, Henter JI. Autopsy findings in 27 children with haemophagocytic lymphohistiocytosis. Histopathology. 1998;32(4):310–316. doi:10.1046/j.1365-2559.1998.00377.x
21. Wright G, Wilmore S, Makanyanga J, et al. Liver transplant for adult hemophagocytic lymphohistiocytosis: case report and literature review. Exp Clin Transplant. 2012;10(5):508–512. doi:10.6002/ect.2011.0204
22. Boldig K, Kiamos A, Agrawal A, Reddy P. Hemophagocytic lymphohistiocytosis and clostridium difficile infection: a diagnostic dilemma. Cureus. 2023;15(1):e33865. doi:10.7759/cureus.33865
23. Ramos-Casals M, Brito-Zerón P, López-Guillermo A, Khamashta MA, Bosch X. Adult haemophagocytic syndrome. Lancet. 2014;383(9927):1503–1516. doi:10.1016/S0140-6736(13)61048-X
24. Park HW, Min GJ, Kim TY, Cho SG. A case of hemophagocytic lymphohistiocytosis following second dose of COVID-19 Vaccination. Acta Haematol. 2023;146(1):65–71. doi:10.1159/000526980
25. Ai S, Awford A, Roncolato F. Hemophagocytic lymphohistiocytosis following ChAdOx1 nCov- 19 vaccination. J Med Virol. 2022;94(1):14–16. doi:10.1002/jmv.27279
26. Tang LV, Hu Y. Hemophagocytic lymphohistiocytosis after COVID-19 vaccination. J Hematol Oncol. 2021;14(1):87. doi:10.1186/s13045-021-01100-7
27. Cory P, Lawrence H, Abdulrahim H, Mahmood-Rao H, Hussein A, Gane J. Lessons of the month 3: haemophagocytic lymphohistiocytosis following COVID-19 vaccination (ChAdOx1 nCoV-19). Clin Med. 2021;21(6):e677–9. doi:10.7861/clinmed.2021-0564
28. Baek DW, Hwang S, Kim J, et al. Patients presenting high fever with lymphadenopathy after COVID-19 vaccination were diagnosed with hemophagocytic lymphohistiocytosis. Infect Dis. 2022;54(4):303–307. doi:10.1080/23744235.2021.2010801
29. Attwell L, Zaw T, McCormick J, Marks J, Mc-Carthy H. Haemophagocytic lymphohistiocytosis after ChAdOx1 nCoV-19 vaccination. J Clin Pathol. 2022;75(4):282–284. doi:10.1136/jclinpath-2021-207760
30. Sassi M, Khefacha L, Merzigui R, Rakez R, Boukhriss S, Laatiri MA. Haemophagocytosis and atypical vacuolated lymphocytes in bone marrow and blood films after SARS-CoV-2 vaccination. Br J Haematol. 2021;195(5):649. doi:10.1111/bjh.17660
31. Rocco JM, Mallarino-Haeger C, Randolph AH, et al. Hyperinflammatory syndromes after severe acute respiratory syndrome coronavirus 2 (SARSCoV-2) messenger RNA vaccination in individuals with underlying immune dysregulation. Clin Infect Dis. 2022;75(1):e912–5. doi:10.1093/cid/ciab1024
32. Caocci G, Fanni D, Porru M, et al. Kikuchi–Fujimoto disease associated with hemophagocytic lymphohistiocytosis following the BNT162b2 mRNA COVID-19 vaccination. Haematologica. 2022;107(5):1222–1225. doi:10.3324/haematol.2021.280239
33. Hieber ML, Sprute R, Eichenauer DA, Hallek M, Jachimowicz RD. Hemophagocytic lymphohistiocytosis after SARS-CoV-2 vaccination. Infection. 2022;50:1399–1404. doi:10.1007/s15010-022-01786-y
34. Awan RU, Rashid S, Nabeel A, Samant H. COVID-19 vaccination-related hemophagocytic lymphohistiocytosis presenting as acute liver failure. Proc Bayl Univ Med Cent. 2022;36(1):78–80. doi:10.1080/08998280.2022.2123665
35. Vanaparthy R, Mohan G, Vasireddy D, Atluri P. Review of COVID-19 viral vector-based vaccines and COVID-19 variants. Infez Med. 2021;29(3):328–338.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.