Back to Journals » Journal of Inflammation Research » Volume 15
Acute Ischemic Stroke in Tubercular Meningitis Patients Without Conventional Vascular Risk Factors: A Retrospective Case Control Study
Authors Tang S ![]() , Liu L, Xie Z, He Y, Zhang Y, Xie Y, Chen S
, Liu L, Xie Z, He Y, Zhang Y, Xie Y, Chen S ![]() , Liu Y
, Liu Y ![]() , Wei Y, Liang Z
, Wei Y, Liang Z ![]()
Received 11 October 2022
Accepted for publication 18 November 2022
Published 7 December 2022 Volume 2022:15 Pages 6617—6627
DOI https://doi.org/10.2147/JIR.S392040
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Shiting Tang,1,* Liuyu Liu,1,* Zhouhua Xie,2 Yaoqin He,2 Yunli Zhang,3 Yiju Xie,4 Shijian Chen,1 Yayuan Liu,1 Yunfei Wei,1,5 Zhijian Liang1
1Department of Neurology, The First Affiliated Hospital of Guangxi Medical University, Guangxi Key Laboratory of Precision Medicine in Cardio-Cerebrovascular Diseases Control and Prevention & Guangxi Clinical Research Center for Cardio-Cerebrovascular Diseases, Nanning, People’s Republic of China; 2Department of Tuberculosis, The Fourth People’s Hospital of Nanning City, Nanning, People’s Republic of China; 3Department of Neurology, People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, People’s Republic of China; 4Department of Neurology, Wuming Hospital of Guangxi Medical University, Nanning, People’s Republic of China; 5Department of Neurology, The Second Affiliated Hospital of Guangxi Medical University, Nanning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhijian Liang, Department of Neurology, The First Affiliated Hospital of Guangxi Medical University, Guangxi Key Laboratory of Precision Medicine in Cardio-cerebrovascular Diseases Control and Prevention & Guangxi Clinical Research Center for Cardio-cerebrovascular Diseases, Nanning, People’s Republic of China, Email [email protected] Yunfei Wei, Department of Neurology, The Second Affiliated Hospital of Guangxi Medical University, Nanning, People’s Republic of China, Email [email protected]
Objective: Ischemic stroke is a common complication in patients with tubercular meningitis (TBM). However, the risk factors for Ischemic stroke in TBM patients are not fully understood, especially in those patients without conventional vascular risk factors. The aim of the present study was to explore the clinical features and independent risk factors for tubercular meningitis-related Ischemic stroke (TBMRIS).
Methods: Tubercular meningitis patients with acute Ischemic stroke without conventional vascular risk factors were recruited between July 2010 and July 2020 as the TBMRIS group. Patients who solely had tubercular meningitis were recruited as the control group (TMB group). Demographic characteristics, clinical presentations, and cerebrospinal fluid (CSF) examinations were collected, and multiple logistic regression analysis was applied to analyse the independent risk factors for TBMRIS.
Results: A total of 70 TBMRIS patients and 70 TMB patients were enrolled. Most (82.86%) of the TBMRIS patients experienced Ischemic stroke events within 3 months after the diagnosis of tubercular meningitis. The multiple logistic regression analysis revealed that variation in red blood cell distribution width (RDW-CV), mean platelet volume (MVP), C-reactive protein (CRP), CSF glucose and Modified Research Council Grade II (MRC Grade II) were independent risk factors for TBRIS. The AUC of the identification model was 0.808, with a sensitivity of 68.60% and a specificity of 84.30%.
Conclusion: This study revealed that RDW-CV, MVP, CRP, CSF glucose and MRC Grade II are potential independent risk factors for TBMRIS. The identification model established in this study may help monitor TBM patients who are at high risk of developing TBMRIS.
Keywords: tubercular meningitis, Ischemic stroke, tubercular meningitis-related Ischemic stroke, independent risk factor
Introduction
Tubercular meningitis (TBM) remains a challenging illness with significant morbidity and mortality in developing countries. The main complications of TBM include stroke, hydrocephalus and tuberculoma formation.1 It has been reported that the incidence of stroke in TBM patients is approximately 13–57%, and that stroke occurs more likely during the third stage of TBM,2,3 Modified Research Council grade III referring to Modified Medical Research Council criteria. Stroke is also a major predictor of permanent disability.4 Consequently, prevention of Ischemic stroke is of great importance to TBM patients. However, the risk factors for Ischemic stroke in TBM patients are not fully understood, especially in those patients without conventional vascular risk factors.
In 1989, Teoh R. reported 2 patients with tubercular meningitis who suffered from rapid internuclear ocular palsy during anti-tuberculosis treatment and died within 14 days. The autopsy results of one of the patients revealed multiple intracranial infarction lesions with diffuse inflammatory infiltration of the basement artery accompanied by thrombosis, suggesting that tubercular meningitis might directly cause Ischemic stroke, namely, tubercular meningitis-related Ischemic stroke (TBMRIS).5 Since then, acute Ischemic stroke has been continuously reported in patients with TBM. However, most of these studies were radiological studies6–8 and showed that the stage of TBM, basal meningeal enhancement, hydrocephalus, exudate and hypertension were related to stroke in TBM patients.2 Only a few studies focusing on the clinical correlation of Ischemic stroke in TBM patients have been reported.9,10 However, none of the risk factors were identified as independent risk factors in the retrospective analysis. The negative result of these studies may be related to their included subjects, some of whom had cerebral vascular risk factors, such as diabetes mellitus, hypertension and hyperlipidemia. It is well known that the exact mechanisms of stroke may differ between patients with or without conventional vascular risk factors. Therefore, we conducted this study to evaluate the clinical features and the independent risk factors for TBMRIS. Patients with conventional vascular risk factors were excluded from our study to decrease the impact of atherosclerosis.
Materials and Methods
Patients (>18 years of age) with a clinical or confirmed diagnosis of TBM attending the inpatient facilities of The First Affiliated Hospital of Guangxi Medical University, The Second Affiliated Hospital of Guangxi Medical University, Guangxi Zhuang Autonomous Region People’s Hospital, Wuming Hospital affiliated with Guangxi Medical University and The Fourth People’s Hospital of Nanning City were enrolled between July 2010 and July 2020. The study was approved by the Review Boards of the First Affiliated Hospital of Guangxi Medical University and local hospitals.Approval Number: 2022-E314-01. The written informed consent was waived because of the retrospective nature of our study. During the data collection, personally identifiable information such as names, addresses and phone numbers of the study participants were never recorded. The collected data were kept confidentially and used only for the purpose of the study.
Definition of TBMRIS
Referring to the conception of cancer-associated Ischemic stroke,11,12 the definition of TBMRIS in the present study was defined as patients with tubercular meningitis (TBM) and acute Ischemic stroke without conventional vascular risk factors. According to American Heart Association diagnostic criteria for stroke,13 acute Ischemic stroke was diagnosed as follows: patients who newly suffered from focal neurological deficits, such as fatigue or aphasia, who had weakness or numbness in one or both limbs, and who had brain MRI and/or CT that identified Ischemic lesions that were consistent with the neurological symptoms. Stroke severity was assessed by the National Institute of Health Stroke Scale (NIHSS).14
The conventional stroke risk factors were defined as follows: (i) hypertension (taking antihypertensive drugs, diastolic blood pressure ≥ 90 mmHg, or systolic blood pressure ≥ 140 mm Hg); (ii) diabetes (taking anti-diabetic drugs or random blood glucose level ≥ 11.1 mmol/L);15 (iii) hyperlipidaemia (taking lipid-lowering drugs, low-density lipoprotein > 3.64 mmol/L, serum total cholesterol > 5.72 mmol/L or triglycerides > 1.70 mmol/L);16 and (iv) smoking and drinking, coronary artery disease, rheumatic heart valve disease, and atrial fibrillation (history of disease, or assessed by a cardiologist according to electrocardiogram and transthoracic echocardiography at admission).
The exclusion criteria for the TBMRIS group were (i) patients with malignant tumor, HIV or Treponema pallidum infection, or autoimmune disease; (ii) patients with heart, kidney or liver failure; (iii) patients with bacterial, fungal pneumonia or sepsis; (iv) patients who took glucocorticoids and immunosuppressants in the last 3 months; (v) dead patients; and (vi) patients with incomplete clinical or imaging data.
Diagnostic Criteria of Tubercular Meningitis
TBM was diagnosed according to a standard case definition published in 2010.17 Patients were defined as having “definite” TBM if acid-fast bacilli were seen in the cerebrospinal fluid (CSF), Mycobacterium tuberculosis was cultured from the CSF, or a CSF positive commercial nucleic acid amplification test was obtained. Patients were defined as having “probable” TBM if their diagnostic score was ≥ 12 (at least 2 points either from the CSF or cerebral imaging criteria) plus exclusion of alternative diagnoses. Patients were defined as “possible” TBM if their diagnostic score was 6 to 11 and if there was exclusion of alternative diagnoses.
The severity of meningitis was graded according to the modified British Medical Research Council criteria as follows: Stage I: prodromal phase with no definite neurological symptoms and a Glasgow coma scale score ≥15; Stage II: signs of meningeal irritation with slight or no clouding of the sensorium and minor (cranial nerve palsies), or no neurological deficit and a Glasgow coma scale score between 11 and 14; and Stage III: severe clouding of the sensorium, convulsions, focal neurologic deficits and involuntary movements and a Glasgow coma scale score ≤10.18
Age-, sex- and living condition-matched acute TBM patients without radiological evidence of an infarct were recruited as the control group, which was also named the TBM group.
Collection of Clinical Data
Data regarding the baseline demography, comorbidities (hypertension, diabetes mellitus, and HIV), clinical symptoms, signs, laboratory parameters, inflammatory markers, imaging examination (such as cranial CT, CT angiography, digital subtraction angiography, MRI, magnetic resonance angiography, diffusion-weighted MRI, chest CT or X-ray), details and duration of treatment (all patients received routine anti-tuberculosis treatment according to the recommendations of the World Health Organization (Fourth edition)) were obtained. CSF was examined for opening pressure, protein, cells, glucose, and bacteria. CSF was also tested by polymerase chain reaction (PCR) to detect mycobacterial deoxyribonucleic acid. India ink preparation of CSF was performed to exclude cryptococcal meningitis.
For the TBMRIS patients, the laboratory data were collected according to the following conditions: (i) data from the patients who were admitted for acute Ischemic stroke while they were diagnosed with TBM during the treatment of Ischemic stroke were collected within 48 hours after admission. (II) Data from the patients who were diagnosed with acute Ischemic stroke during the treatment of TBM were collected within 72 hours of the acute Ischemic stroke attack. All data were independently verified by three authors. This study was performed in accordance with the principles outlined in the Declaration of Helsinki and approved by the ethical committee and the institutional review board.
Statistical Analysis
Statistical analyses were performed using SPSS 26.0. p<0.05 was considered statistically significant. Continuous variables are presented as the mean ± standard deviation or median with interquartile range (IQR). Significance testing was carried out using Student’s t-test for normally distributed data and the Mann‒Whitney U-test for nonnormal data. The chi-square test or Fisher’s exact test was used for categorical variables. All variables were initially tested by univariate analysis, and those with a P < 0.05 were entered stepwise into a multivariate analysis by using the forward conditional method. To explore a reliable model to identify TBMRIS, we combined the independent risk factors for TBMRIS named the identification model. Moreover, ROC analysis was used to compare the area under the ROC curve (AUC) of the identification model with every independent risk factor using MedCalc version 15.8 software packages. The largest AUC variable and index (calculated by sensitivity and specificity) were called the reliable method to determine TBMRIS in this study.
Results
In this study, a total of 967 patients had a diagnosis of TBM. Among these, 371 patients had a diagnosis of Ischemic stroke, and 301 patients were excluded, including 110 patients with traditional stroke risk factors, 23 patients with hematological system diseases, 39 patients with HIV and/or syphilis infection, 72 patients with fungal meningitis or bacterial meningitis, 30 patients with heart, kidney, liver or lung failure, and 27 patients with incomplete clinical data. Finally, 70 patients aged 21–88 years (median 59.50 [IQR 18], 46 males, 24 females) who met the TBMRIS criteria were enrolled. In the TBM group, 70 patients were included who were aged 46–75 years (median 54.00 [IQR 13], 42 males, 28 females) (Figure 1). A comparison of the presenting clinical features in TBMRIS and TBM is presented in Table 1. Significant differences were not found in age, sex, diagnostic category, extracranial tuberculosis or living conditions between the two groups (p > 0.05) (Table 1). The two groups of patients shared similar tubercular meningitis manifestations: headache, fever, meningeal irritation, vomiting, and altered mentation.
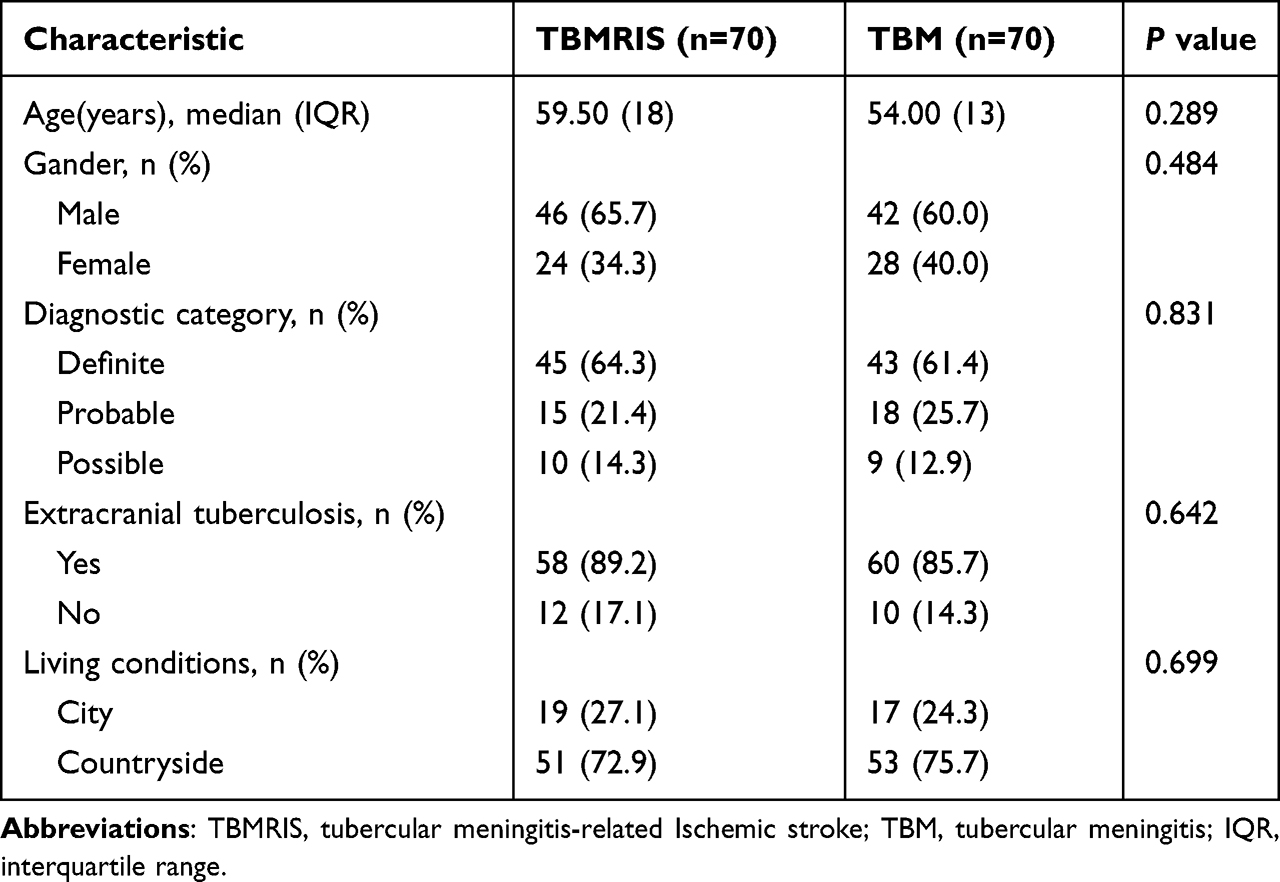 |
Table 1 General Data |
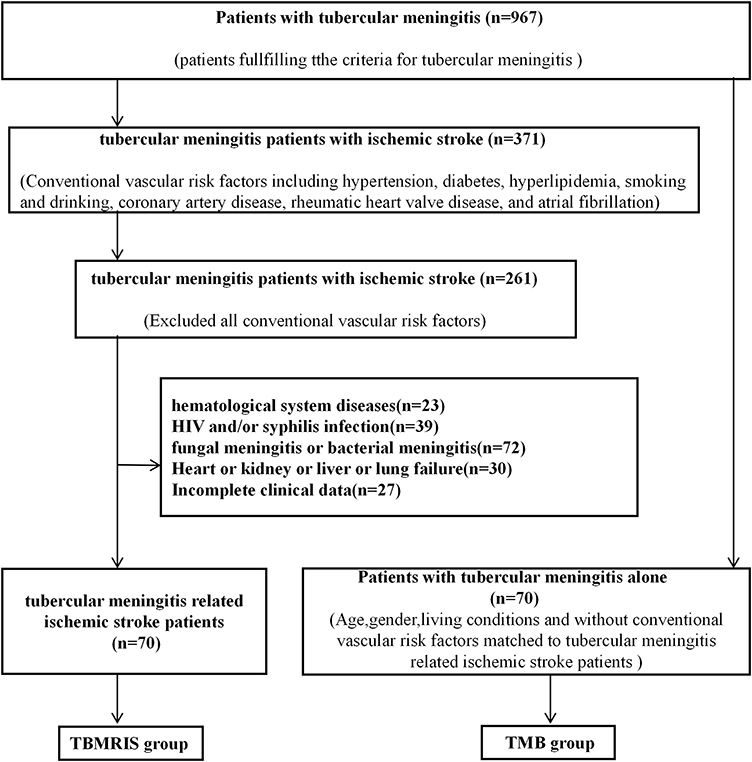 |
Figure 1 Flowchart of the screening of patients with tubercular meningitis-related Ischemic stroke. Abbreviations: TBMRIS, tubercular meningitis-related Ischemic stroke; TBM, tubercular meningitis. |
In the TBMRIS group, 10 (14.29%) patients were first hospitalized for Ischemic stroke, were diagnosed with tubercular meningitis during hospitalization and initiated anti-tuberculosis treatment. Sixty (85.71%) patients presented with tubercular meningitis as the initial manifestation and were diagnosed with Ischemic stroke during anti-tuberculosis treatment. Among the TBMRIS group, 58 (82.86%), 8 (11.43%) and 4 (5.71%) patients experienced Ischemic stroke in the first 3 months, 4–6 months and more than 6 months, respectively.
The infarctions of the TBMRIS’ patients were scattered and unevenly distributed. The anatomical locations that were most often involved were the basal ganglia area, followed by the frontal lobe, parietal lobe, radiative crown area and side ventricle horn. Subsequently, locations such as the occipital lobe, temporal lobe, cerebellum, and brainstem were less involved (Table 2 and Figure 2).
 |
Table 2 The Distribution of Cerebral Infarction Lesions in TBMRIS Patients |
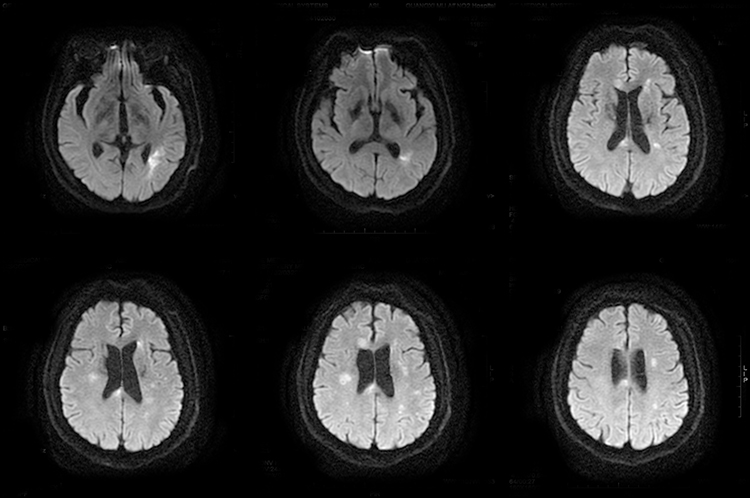 |
Figure 2 Typical neuroimaging of a patient with acute Ischemic stroke and active tuberculosis meningitis. Images are from a male in his 50s who had acute Ischemic stroke without conventional stroke risk factors and who was initially diagnosed with active tuberculosis meningitis during the treatment of Ischemic stroke. Six MRI diffusion-weighted images show multiple high-signal lesions in multiple arterial regions of the brain. |
Compared to the TBM group, the TBMRIS group had lower levels of red blood cell (RBC) count, mean platelet volume (MPV), and cerebrospinal fluid (CSF) glucose (p < 0.05) (Table 3). The variations in red blood cell distribution width (RDW-CV), D-dimer, and C-reactive protein (CRP) in TBMRIS were significantly higher than those in the TBM group (p < 0.05) (Table 2). Significant differences were also found in the Modified Research Council (MRC) Grade between the two groups (p < 0.05) (Table 3). Furthermore, multiple logistic regression analysis revealed that variation of RDW-CV (odds ratio [OR]:1.261, 95%confidence interval [CI]:1.056–1.506, p<0.05), MPV (OR:0.657, 95% CI:0.464–0.930, p<0.05), CRP (OR:1.012, 95% CI:1.001–1.023, p<0.05), Glucose (OR:0.500, 95% CI:0.309–0.809, p<0.05), and MRC Grade II (OR:3.578, 95% CI:1.441–8.886, p<0.05) were independent risk factors for TBMRIS (Table 4).
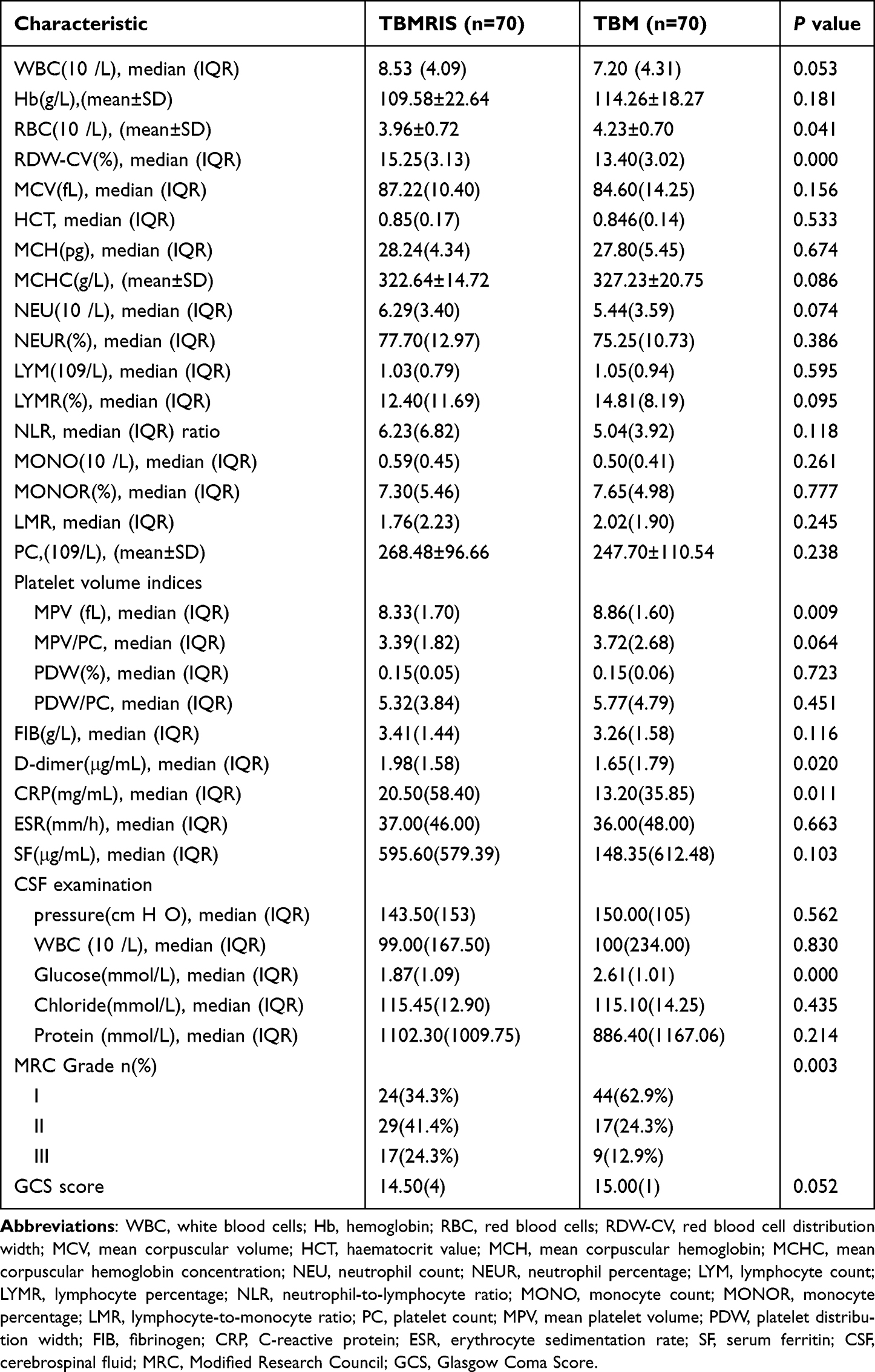 |
Table 3 Comparison of the Laboratory Data Between the TBMRIS Group and the TBM Group |
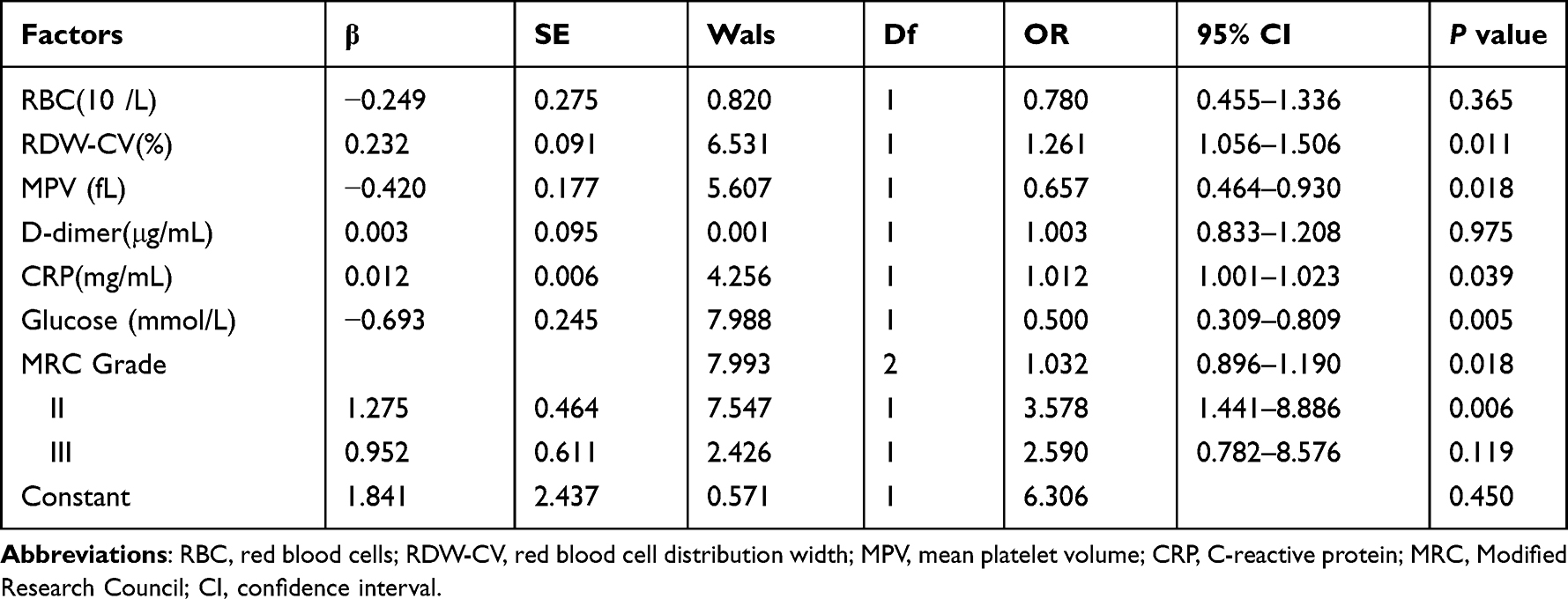 |
Table 4 Multivariate Logistic Regression Analysis |
Compared to the AUC of RDW-CV, MPV, CRP, glucose, and MRC grade II, the AUC of the identification model was the largest (AUC=0.808, sensitivity 68.60%, specificity 84.30%, Index 0.529), which means that the combined model had the greatest predicting ability for TBMRIS (Table 5 and Figure 3).
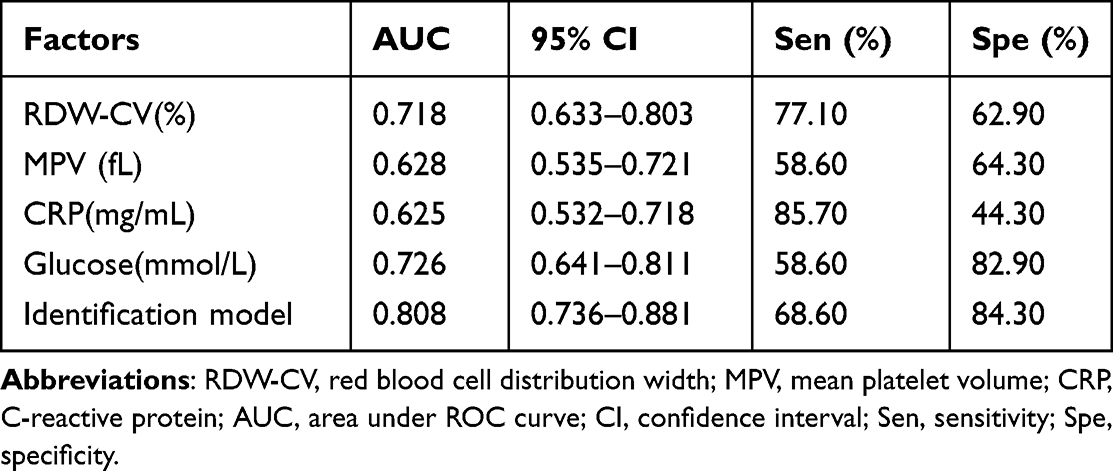 |
Table 5 ROC Analysis of Independent Risk Factors and the Identification Model of TBRIS |
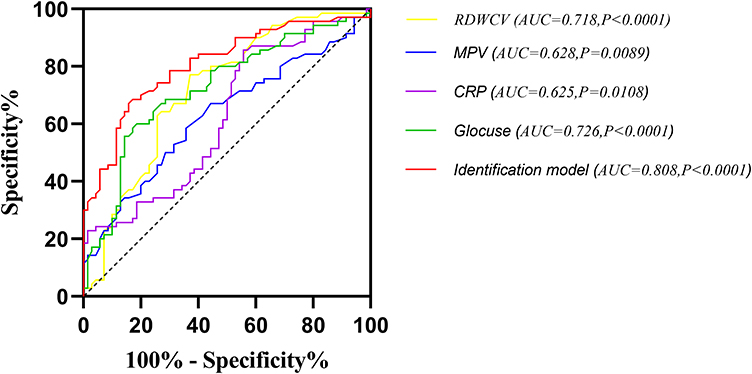 |
Figure 3 The analysis of ROC curve and area under curve. Abbreviations: RDW-CV, red blood cell distribution width; MPV, mean platelet volume; CRP, C-reactive protein. |
Discussion
Stroke is one of the main causes of mortality and long-term physical and cognitive impairment in China.19 In addition to conventional vascular risk factors, such as hypertension, diabetes, long-term smoking and drinking and hyperlipidaemia, recent studies have found that inflammation is closely connected to cerebral infarction.20–22 In clinical terms, tuberculosis is a common chronic inflammatory disease. Although tuberculosis meningitis comprises 1% of the incident cases of tuberculosis, it remains the most serious form of extrapulmonary tuberculosis.1,23 The occurrence of stroke has been reported in up to 57% of TBM patients,3,24 with mortality approximately three times higher in TBM patients with stroke than in patients without stroke.3 In the present study, most TBMRIS patients (82.86%) developed Ischemic stroke within 3 months after the diagnosis of TBM. This finding suggests that TBMRIS was likely to develop during the intensive inflammatory response period that occurred in active TBM patients. This is consistent with the results of previous studies.2,25 In addition, there were 10 (14.29%) patients who were hospitalized for acute Ischemic stroke and who had a confirmed diagnosis of TBMRIS, indicating that measures should be taken to screen out TBM. Significant differences in the Modified Research Council (MRC) grade were also found between the TBMRIS group and TBM group, and the multivariate analysis showed that MRC Grade II was an independent risk factor for TBMRIS. As Anuradha26 found that patients with MRC grade III were more likely to have acute cerebral infarction events, in which TBM patients with conventional vascular risk factors were included, the finding in the present study, in which patients with conventional vascular risk factors were excluded, suggested that ischemic stroke may occur at early stage in patients with TBM without conventional vascular risk factors, indicating that clinicians should pay more attention to the prevention of ischemic stroke from patients with TBM without conventional vascular risk factors.
Previous studies have suggested that atherosclerosis aggravation may be the main cause of stroke in patients with conventional vascular risk factors. Therefore, in TBM patients, it was difficult to determine whether stroke was caused by TBM or atherosclerosis. In our study, patients with conventional vascular risk factors were excluded, reducing the effects of atherosclerosis. The multivariate analysis showed that variations of RDW-CV, MVP, CRP, CSF glucose and MRC Grade II were independent risk factors for TBMRIS, implying that these independent risk factors alone or in combination promoted the development of TBMRIS through different kinds of pathways.
The unveiling of independent risk factors for TBMRIS is an important issue because the pathogenesis that is induced by independent risk factors may influence the choice of management, stroke prognosis, and risk of recurrence. In some previous studies, inflammatory changes in the vessels of the circle of Willis are the most likely reason for vascular complications in tubercular meningitis. Exudative basal meningitis results in vasospasm with or without secondary thrombosis. These changes jeopardize arterial blood flow, causing Ischemic stroke in the early stage of the disease.27,28 However, to date, the underlying pathogenesis of vasospasm in tubercular meningitis-related Ischemic stroke has not been entirely elucidated. First, in the present study, the TBMRIS group had elevated plasma C-reactive protein and lower cerebrospinal fluid glucose than the TMB group, which implies that the immune response to tuberculosis infection may be more intensive in TBMRIS patients than in TMB patients.29,30 Moreover, a lower MPV was also found in the TBMRIS group. As platelets are known to change their structure and function from inactive to active platelets owing to physiologic signals31 and MPV reflects platelet size and activity, increases or decreases in MPV can represent various inflammatory processes and diseases.32 Previous studies have investigated that the MPV is correlated inversely with the C-reactive protein concentration, suggesting that a lower MPV implies a more intensive inflammatory response.33–36 In addition, plasma levels of C-reactive protein are an independent risk factor for vasospasm severity;37,38 the more intensive immune response to a tuberculosis infection may induce a more severe vasospasm in the TBMRIS group.
In addition, in the present study, the TBMRIS group had elevated variation in RDW-CV levels. Previous studies have found that elevated variations in RDW-CV levels are common in TBM patients.39 Elevations in the RDW-CV levels suggests that the patients’ red blood cell life is shortened and red blood cell rupture is increased, so that substances such as hemoglobin and ferrous ions that are released into blood circulation can directly combine with NO to stimulate the generation of oxygen free radicals and ultimately activate a variety of inflammatory factors including C-reactive protein.40 In summary, in the present study, the more intensive immune response to tuberculosis infection in the TBMRIS group may initially induce more active platelet activation, then a more severe vasospasm, with or without thrombosis, and ultimately the development of TBMRIS.
In the present study, the multivariate logistic regression analysis revealed that variations in RDW-CV, MVP, CRP, CSF glucose and MRC Grade II were independent risk factors for TBMRIS, indicating that these parameters could be used as potential biomarkers for TBMRIS. However, these biomarkers are also commonly found in systemic inflammation and other diseases. Considering that the development of TBMRIS may be caused by the combined effects of variation of red blood cell distribution width, mean platelet volume, C-reactive protein, CSF glucose and Modified Research Council Grade II, we calculated the TBMRIS Index (0.529). The area under the ROC curve of the TBMRIS Index was highly accurate (0.808), which suggests that the independent risk factors together promoted the development of TBMRIS, and this also illustrates that the index of TBMRIS equaling to 0.529 had the most power to predict the TBM patients who were at higher risk for TBMRIS.
The strengths of our study were the multicentre enrolment and the study’s comparison with TBM patients without conventional vascular risk factors. Our study also has limitations. Due to the retrospective nature of the study, this study included some uncontrollable settings, and the findings need to be confirmed by future studies with large sample randomized control trials.
Conclusion
In conclusion, our results show that RDW-CV, MVP, CRP, CSF glucose and MRC Grade II are independent risk factors for TBMRIS. These independent risk factors alone or in combination promoted the development of TBMRIS. We found that the more intensive immune response to tuberculosis infection in the TBMRIS group contributed to the initiation of platelet activation and to the development of vasospasm, which are attributed to the pathogenesis of TBMRIS. The identification model established in this study may assist clinicians in identifying TBM patients at high risk of developing TBMRIS. The findings in the present study should be further validated in more prospective larger studies.
Data Sharing Statement
The datasets generated and analyzed in this study will be available by the corresponding authors upon reasonable request.
Ethical Approval
This project fully considered and protected the rights and interests of the study objects. It meets the criteria of Ethical Review Committee. The Medical Ethics Committee of The First Affiliated Hospital of Guangxi Medical University has approved the protocol.
Informed Consent
The written informed consent was waivered because of the retrospective nature of our study.
Acknowledgments
We would like to thank Prof. Li for her guidance on statistical methods. We are grateful for the advice and discussions with our colleagues Junli Liang and Jinyu Liang as well as the anonymous reviewers.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by National Natural Science Foundation of China (NSFC 82260243); the Foundation of National Key R&D Program of China (2018YFC 1311300); and Guangxi Medical and Health and Appropriate Technology Development and Promotion Application Project (Nos. S2021101 and. S2020013).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Thwaites GE, van Toorn RS, Choeman J. tubercular meningitis: more questions, still too few answers. Lancet Neurol. 2013;12:999–1010. doi:10.1016/S1474-4422(13)70168-6
2. Kalita J, Misra UK, Nair PP. Predictors of stroke and its significance in the outcome of tubercular meningitis. J Stroke Cerebrovasc Dis. 2009;18:251–258. doi:10.1016/j.jstrokecerebrovasdis.2008.11.007
3. Misra UK, Kalita J, Maurya PK. Stroke in tubercular meningitis. J Neurol Sci. 2011;303:22–30. doi:10.1016/j.jns.2010.12.015
4. Chan KH, Cheung RT, Fong CY, Tsang KL, Mak SL, Ho SL. Clinical relevance of hydrocephalus as a presenting feature of tubercular meningitis. Qjm. 2003;96:643–648. doi:10.1093/qjmed/hcg108
5. Teoh R, Humphries MJ, Chan JC, Ng HK, O’Mahony G. Internuclear ophthalmoplegia in tubercular meningitis. Tubercle. 1989;70:61–64. doi:10.1016/0041-3879(89)90067-6
6. Ozateş M, Kemaloglu S, Gürkan F, Ozkan U, Hoşoglu SS, Imşek MM. CT of the brain in tubercular meningitis. A review of 289 patients. Acta Radiol. 2000;41:13–17. doi:10.1258/rsmacta.41.1.13
7. Bernaerts A, Vanhoenacker FM, Parizel PM, et al. Tuberculosis of the central nervous system: overview of neuroradiological findings. Eur Radiol. 2003;13:1876–1890. doi:10.1007/s00330-002-1608-7
8. Ranjan P, Kalita J, Misra UK. Serial study of clinical and CT changes in tubercular meningitis. Neuroradiology. 2003;45:277–282. doi:10.1007/s00234-003-0958-4
9. Chan KH, Cheung RT, Lee R, Mak SL, Ho SL. Cerebral infarcts complicating tubercular meningitis. Cerebrovasc Dis. 2005;19:391–395. doi:10.1159/000085568
10. Koh SB, Kim BJ, Park MH, Yu SW, Park KW, Lee DH. Clinical and laboratory characteristics of cerebral infarction in tubercular meningitis: a comparative study. J Clin Neurosci. 2007;14:1073–1077. doi:10.1016/j.jocn.2006.07.014
11. Kono T, Ohtsuki T, Hosomi N, et al. Cancer-associated ischemic stroke is associated with elevated D-dimer and fibrin degradation product levels in acute ischemic stroke with advanced cancer. Geriatr Gerontol Int. 2012;12:468–474. doi:10.1111/j.1447-0594.2011.00796.x
12. Bang OY, Seok JM, Kim SG, et al. Ischemic stroke and cancer: stroke severely impacts cancer patients, while cancer increases the number of strokes. J Clin Neurol. 2011;7:53–59. doi:10.3988/jcn.2011.7.2.53
13. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50:e344–e418. doi:10.1161/STR.0000000000000211
14. Adams HP, Adams RJ, Brott T, et al. Guidelines for the early management of patients with ischemic stroke: a scientific statement from the Stroke Council of the American Stroke Association. Stroke. 2003;34:1056–1083. doi:10.1161/01.STR.0000064841.47697.22
15. Draznin B, Aroda VR, Bakris G, et al. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2022. Diabetes Care. 2022;45:S17–s38.
16. Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2019;73:e285–e350.
17. Marais S, Thwaites G, Schoeman JF, et al. Tubercular meningitis: a uniform case definition for use in clinical research. Lancet Infect Dis. 2010;10:803–812.
18. Wasay M, Farooq S, Khowaja ZA, et al. Cerebral infarction and tuberculoma in central nervous system tuberculosis: frequency and prognostic implications. J Neurol Neurosurg Psychiatry. 2014;85:1260–1264.
19. Tu WJ, Qiu HC, Zhang Y, et al. Lower serum retinoic acid level for prediction of higher risk of mortality in ischemic stroke. Neurology. 2019;92:e1678–e87.
20. Zheng J, Liao Y, Xu Y, Mo Z. Icariin attenuates Ischemic stroke through suppressing inflammation mediated by endoplasmic reticulum stress signalling pathway in rats. Clin Exp Pharmacol Physiol. 2022;49:719–730.
21. Zhou YX, Li WC, Xia SH, et al. Predictive value of the systemic immune inflammation index for adverse outcomes in patients with acute Ischemic stroke. Front Neurol. 2022;13:836595.
22. Oh SE, Parikh NS. Recent advances in the impact of infection and inflammation on stroke risk and outcomes. Curr Neurol Neurosci Rep. 2022;22:161–170.
23. Méchaï F, Bouchaud O. Tubercular meningitis: challenges in diagnosis and management. Rev Neurol (Paris). 2019;175:451–457.
24. Chatterjee D, Radotra BD, Vasishta RK, Sharma K. Vascular complications of tubercular meningitis: an autopsy study. Neurol India. 2015;63:926–932.
25. Misra UK, Kalita J, Kumar M, Neyaz Z. Hypovolemia due to cerebral salt wasting may contribute to stroke in tubercular meningitis. Qjm. 2018;111:455–460.
26. Anuradha HK, Garg RK, Agarwal A, et al. Predictors of stroke in patients of tubercular meningitis and its effect on the outcome. Qjm. 2010;103:671–678.
27. Springer P, Swanevelder S, van Toorn R, van Rensburg AJ, Schoeman J. Cerebral infarction and neurodevelopmental outcome in childhood tubercular meningitis. Eur J Paediatr Neurol. 2009;13:343–349.
28. Lammie GA, Hewlett RH, Schoeman JF, Donald PR. Tubercular cerebrovascular disease: a review. J Infect. 2009;59:156–166.
29. Elkind MS, Carty CL, O’Meara ES, et al. Hospitalization for infection and risk of acute ischemic stroke: the Cardiovascular Health Study. Stroke. 2011;42:1851–1856.
30. Sproston NR, Ashworth JJ. Role of C-reactive protein at sites of inflammation and infection. Front Immunol. 2018;9:754.
31. Shah B, Valdes V, Nardi MA, Hu L, Schrem E, Berger JS. Mean platelet volume reproducibility and association with platelet activity and anti-platelet therapy. Platelets. 2014;25:188–192.
32. Korniluk A, Koper-Lenkiewicz OM, Kamińska J, Kemona H, Dymicka-Piekarska V. Mean Platelet Volume (MPV): new perspectives for an old marker in the course and prognosis of inflammatory conditions. Mediators Inflamm. 2019;2019:9213074.
33. Ball S, Dennis JA, Bedanie G, Nugent K. Relation between mean platelet volume and C-reactive protein. Proceedings. 2020;33:163–168.
34. Unal M. Platelet mass index is increased in psoriasis. A possible link between psoriasis and atherosclerosis. Arch Med Sci Atheroscler Dis. 2016;1:e145–e9.
35. Yildirim Cetin G, Gul O, Kesici-Metin F, Gokalp İ, Sayarlıoglu M. Evaluation of the mean platelet volume and red cell distribution width in FMF: are they related to subclinical inflammation or not? Int J Chronic Dis. 2014;2014:127426.
36. Zareifar S, Farahmand Far MR, Golfeshan F, Cohan N. Changes in platelet count and mean platelet volume during infectious and inflammatory disease and their correlation with ESR and CRP. J Clin Lab Anal. 2014;28:245–248.
37. Liu X, Zhao N, Zeng K, et al. Effects of nimodipine combined with betahistine on CRP and other inflammatory cytokines and vascular endothelial function in patients with hypertensive cerebral vasospasm. Clin Hemorheol Microcirc. 2020;75:279–289.
38. Zhang W, Sun L, Ma L, Li Z. Clinical significance of changes in IL-6, CRP and S100 in serum and NO in cerebrospinal fluid in subarachnoid hemorrhage and prognosis. Exp Ther Med. 2018;16:816–820.
39. Mukherjee A, Kaeley N, Dhar M, Kumar S, Bhushan B. Prevalence, characteristics, and predictors of tuberculosis associated anemia. J Family Med Prim Care. 2019;8:2445–2449.
40. Munakomi S. Coanda effect-another entity in “vasospasm mimics” lists. World Neurosurg. 2019;126:679.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.