")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Acute Genital Ulcers in a Woman Secondary to COVID-19 Infection: A Case Report
Authors Zhang J , Wang D , Chen M, Li J , Huang W
Received 18 October 2023
Accepted for publication 18 December 2023
Published 5 January 2024 Volume 2024:17 Pages 31—34
DOI https://doi.org/10.2147/CCID.S445296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Anne-Claire Fougerousse
Jia Zhang,1,* Danni Wang,1,* Mingjing Chen,1 Jiajun Li,2 Wenxiang Huang1
1Department of Geriatrics, the First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Infectious Diseases, the First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenxiang Huang, Department of Geriatrics, the First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China, Tel +86 13883533808, Email [email protected]
Abstract: Acute genital ulcers (AGU) have been associated with various pathogens, such as Epstein–Barr virus (EBV) and cytomegalovirus (CMV). However, cases of AGU associated with coronavirus disease 2019 (COVID-19) are rare, and this disease significantly impairs human quality of life. In this case, we report a 37-year-old woman who presented with a five-day history of a painful genital ulcer and fever. A month earlier, she had experienced a COVID-19 infection that resolved without medical therapy. Physical examination revealed that multiple asymmetric ulcers presented on labia minora covered with whitish exudates. The patient, without any high-risk sexual behavior, or a personal or family history of autoimmune disorders or inflammatory bowel disease, was diagnosed with COVID-19-related AGU after ruling out other infectious and immune diseases. Following a two-week treatment of oral prednisone, her vulvar edema, ulcers, and fever improved significantly. This case suggests that AGU may be triggered by a COVID-19 infection.
Keywords: COVID-19, SARS-CoV-2, acute genital ulcers, fever
Introduction
Acute genital ulcers (AGU), also known as Lipschütz ulcers, aphthous ulcers, or acquired genital ulceration, are characterized by acute, painful vulvar aphthous ulcers and typically occur in nonsexually active adolescent females.1,2 These ulcers, either singular or multiple, manifest as deep, sharply demarcated lesions with fibrinous coatings or greyish exudate.3,4 They frequently appear on the labia minora but also affect other regions, such as the labia majora and the perineal area.3 Affected patients often exhibit flu-like symptoms, including fever, fatigue, and lymphadenitis.4 The diagnosis of AGU is established by exclusion of other diseases.5–7 Although the etiology of AGU remains to be fully elucidated, it has been associated with various pathogens, including Epstein–Barr virus (EBV) and cytomegalovirus (CMV).4 In this paper, we report a rare case of a 37-year-old woman with exquisitely painful genital ulcers and persistent fever, which were attributed to COVID-19 infection after ruling out other common etiologies, thus highlighting the potential connection between AGU and COVID-19.
Case Presentation
A 37-year-old woman presented to our hospital with a 5-day history of exquisitely painful genital ulcers and persistent fever (38.5°C) on February 24, 2023. Over the previous month, she experienced a COVID-19 infection confirmed by a nasopharyngeal swab polymerase chain reaction. She referred to mild symptoms including fever, sore throat, and cough, which improved significantly within a week without medical intervention. She denied engaging in any recent high-risk sexual behavior. Additionally, she reported no history of autoimmune disorders or inflammatory bowel disease in herself or her family. Physical examination revealed multiple asymmetric ulcers with necrotic bases on the labia minora, which were covered in whitish exudates and exhibited well-demarcated borders (Figure 1A). No similar lesions existed elsewhere. Laboratory tests indicated a low lymphocyte count of 0.9 × 10^9/L (normal range: 1.10–3.20) and a reduced percentage of lymphocytes at 10.5% (normal range: 20–50). The erythrocyte sedimentation rate was elevated at 84 mm/h (normal range: 2–26), and the C-reactive protein level was above normal at 13.9 mg/L (normal range: 0–8). After ruling out other common triggers such as herpes simplex virus, syphilis, EBV, human immunodeficiency virus, and CMV—all of which yielded negative serologic test outcomes—a diagnosis of AGU secondary to COVID-19 was established. Treatment with oral prednisone 20mg daily was initiated, the patient’s fever subsided within 24 h, and vulvar edema and ulcers improved markedly (Figure 1B) after 14 days of therapy. At a 3-month follow-up, the patient remained asymptomatic.
Discussion
AGU, first identified by Lipschütz in 1913, mainly affects non-sexually active adolescent females and is characterized by the sudden onset of intense, painful, yet self-resolving vulvar aphthous ulcers.1,2,4,8 These ulcers often present with systemic infection symptoms and are associated with various pathogens, such as EBV, CMV, and influenza virus.4 The differential diagnoses for AGU encompass sexually transmitted infections, such as Treponema pallidum, herpes simplex virus, and Human Immunodeficiency Virus, as well as non-infectious conditions including Crohn’s disease, Behçet’s disease, erosive lichen planus, bullous disorders, localized trauma, and tumors.4,9 The characteristics of AGU and its differential diagnoses of Behcet’s disease, Crohn’s disease, and erosive lichen planus are shown in Table 1.
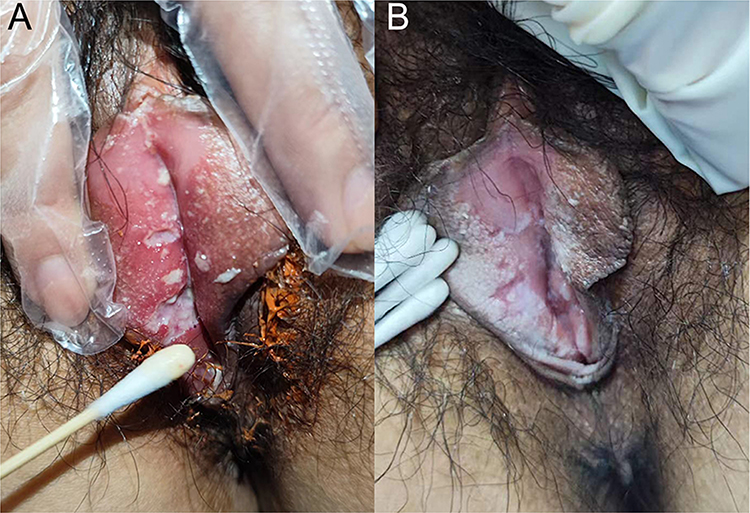 |
Figure 1 (A) Necrotic and fibrinous genital ulcers. (B) Follow-up image after 14 days of therapy demonstrating a resolving ulcerated lesion and vulvar edema. |
 |
Table 1 Characteristics of Acute Genital Ulcers, Behcet’s Disease, Crohn’s Disease, and Erosive Lichen Planus |
In this case, the patient exhibited sudden, painful ulcers on the labia minora, accompanied by fever. Laboratory tests targeting etiologies commonly associated with differential diagnoses of AGU yielded negative results. Considering the medical history, which indicated a COVID-19 infection 1 month earlier, the patient was diagnosed with AGU secondary to COVID-19 in accordance with the diagnostic criteria.4 Recently, five reported cases also highlighted the association between AGU and COVID-19.12–16 Of these, four were diagnosed with COVID-19 before the onset of genital ulcers, whereas one case was diagnosed 12 days after vulvar ulcers appeared. Notably, all cases presented flu-like symptoms alongside genital ulcers. Laboratory tests failed to reveal any positive findings for other potential causes of vaginal ulcers, leading to the final diagnosis of COVID-19-associated ulcers.12–16 The mechanism in these cases may be a dysregulation of the immune system accompanied by cytokine activation due to systemic illness. The fact that the SARS-CoV-2 virus triggers a systemic autoimmune inflammatory response, impacting multiple organ systems, may explain the connection between the development of genital ulcers and COVID-19 infection.16
Treatment for AGU includes pain management, anti-inflammatory medication, and corticosteroid therapy.4 While corticosteroid therapy remains controversial, a systematic review suggests that systemic corticosteroids may prolong the disease’s duration.5 However, a retrospective analysis of 26 patients with AGU indicates that corticosteroid therapy effectively resolves acute flare-ups and prevents AGU recurrences.17 Furthermore, given that four other reported cases of COVID-19-associated AGU have successfully utilized corticosteroid therapy with favorable outcomes,12,13,15,16 oral prednisone was administered to this patient, leading to the resolution of lesions within 2 weeks without any subsequent recurrences. Given the current context of the COVID-19 pandemic, we suggest clinicians adopt a low threshold for suspicion when evaluating AGU. Notably, for the rapid alleviation of symptoms related to COVID-19-associated AGU, oral steroid therapy continues to play a vital role in management.
Conclusion
In conclusion, we report a rare case to describe the potential relationship between the development of AGU and COVID-19 infection. Currently, the global COVID-19 pandemic remains far from over, clinicians should be alert to the presence of genital ulcers accompanied by flu-like symptoms in a clinical setting, and consider the possibility of COVID-19 infection as a potential trigger. Such recognition may prevent patients from delaying treatment, and timely and effective steroid therapy after diagnosis can avoid unnecessary interventions and alleviate patient distress.
Consent
Formal written consent for the publication of case details and associated images was obtained from the patient. Institutional approval was not required for publishing these case details.
Acknowledgments
We would like to thank the patient for participating in our study.
Funding
This work was supported by the Natural Science Foundation of Chongqing, China CSTC, cstc2019jcyj-msxmX0829.
Disclosure
We declare that no authors of our work have conflicts of interest.
References
1. Huppert JS, Gerber MA, Deitch HR, et al. Vulvar Ulcers in Young Females: a Manifestation of Aphthosis. J Pediatric Adolescent Gynecol. 2006;19(3):195–204. doi:10.1016/j.jpag.2006.02.006
2. Farhi D, Wendling J, Molinari E, et al. Non-sexually related acute genital ulcers in 13 pubertal girls: a clinical and microbiological study. Arch Dermatol. 2009;145(1):38–45. doi:10.1001/archdermatol.2008.519
3. Huppert JS. Lipschutz ulcers: evaluation and management of acute genital ulcers in women. Dermatologic Therapy. 2010;23(5):533–540. doi:10.1111/j.1529-8019.2010.01356.x
4. Sadoghi B, Stary G, Wolf P, et al. Ulcus vulvae acutum Lipschütz: a systematic literature review and a diagnostic and therapeutic algorithm. J Eur Acad Dermatol Venereol. 2020;34(7):1432–1439. doi:10.1111/jdv.16161
5. Vismara SA, Lava SAG, Kottanattu L, et al. Lipschütz’s acute vulvar ulcer: a systematic review. Eur J Pediatr. 2020;179(10):1559–1567. doi:10.1007/s00431-020-03647-y
6. Schindler Leal AA, Piccinato CA, Beck APA, et al. Acute genital ulcers: keep Lipschütz ulcer in mind. Arch Gynecol Obstet. 2018;298(5):927–931. doi:10.1007/s00404-018-4866-6
7. Falkenhain-López D, Agud-Dios M, Ortiz-Romero PL, et al. COVID-19-related acute genital ulcers. J Eur Acad Dermatol Venereol. 2020;34(11):e655–e656. doi:10.1111/jdv.16740
8. Lehman JS, Bruce AJ, Wetter DA, et al. Reactive nonsexually related acute genital ulcers: review of cases evaluated at Mayo Clinic. J Am Acad Dermatol. 2010;63(1):44–51. doi:10.1016/j.jaad.2009.08.038
9. Gall R, Navarro-Fernandez IN. Lichen Planus Erosive Form. Treasure Island (FL): StatPearls Publishing; 2023.
10. Barret M, de Parades V, Battistella M, et al. Crohn’s disease of the vulva. J Crohn’s Colitis. 2014;8(7):563–570. doi:10.1016/j.crohns.2013.10.009
11. Mauskar M. Erosive Lichen Planus. Obstetrics Gynecol Clin North Am. 2017;44(3):407–420. doi:10.1016/j.ogc.2017.04.004
12. Falkenhain-López D, Agud-Dios M, Ortiz-Romero PL, et al. COVID-19-related acute genital ulcers. Venereology. 2020;34(11):e655.
13. Christl J, Alaniz VI, Appiah L, et al. Vulvar Aphthous Ulcer in an Adolescent With COVID-19. J Pediatr Adolesc Gynecol. 2021;34(3):418–420. doi:10.1016/j.jpag.2021.02.098
14. Schmitt TM, Devries J, Ohns MJ. Lipschutz Ulcers in an Adolescent After Sars-CoV-2 Infection. J Pediatric Health Care. 2023;37(1):63–66. doi:10.1016/j.pedhc.2022.09.005
15. Jacyntho CM, Lacerda MI, Carvalho MS, et al. COVID-19 related acute genital ulcer: a case report. Einstein. 2022;20.
16. Fotiadou C, Lazaridou E, Apalla Z. Vulvar Aphthous Ulcer in an Adolescent Girl Suffering From COVID-19 Infection. Dermatol Practical Conceptual. 2023;e2023054. doi:10.5826/dpc.1301a54
17. Dixit S, Bradford J, Fischer G. Management of nonsexually acquired genital ulceration using oral and topical corticosteroids followed by doxycycline prophylaxis. J Am Acad Dermatol. 2013;68(5):797–802. doi:10.1016/j.jaad.2012.10.014
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.