")
Back to Journals » International Medical Case Reports Journal » Volume 17
Acute Bowel Obstruction Due to Transmural Migration of Gossypiboma: A Case Report
Authors Baset GY , Seyar F, Hussain Pour ZH , Karimi QA
Received 9 January 2024
Accepted for publication 12 March 2024
Published 19 March 2024 Volume 2024:17 Pages 177—180
DOI https://doi.org/10.2147/IMCRJ.S458658
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Ghulam Yahia Baset,1 Farukh Seyar,2 Zaker Hussain Hussain Pour,3 Qurban Ali Karimi4
1Faculty member, Department of Emergency Surgery and Trauma, Kabul University of Medical Science, Ali Abad Teaching Hospital, Kabul, Afghanistan; 2Faculty Member, Department of Abdominal Surgery, Kabul University of Medical Science, Ali Abad Teaching Hospital, Kabul, Afghanistan; 3Faculty Member, Department of Maternal and Child Health, Kabul University of Medical Science, Kabul, Afghanistan; 4Department of Research, Kabul University of Medical Science, Kabul, Afghanistan
Correspondence: Ghulam Yahia Baset, Tel +93783676086, Email [email protected]
Abstract: gossypiboma is used to describe a retained surgical swab in the body after an operation. It remains an unwanted complication of surgical practice that increase morbidity and mortality of the patient and profound medico legal problems. Intra-abdominal gossypiboma can migrate in to the ileum, stomach, colon or bladder without any apparent opening in the wall of these luminal organs. Vigilant sponge counting during procedures and thorough exploration prior to closure of the abdomen, are essential practices to avoid such occurrences. Herein we present a case of gossypiboma in a 26-year old woman that was in the lumen of small bowel and caused acute intestinal obstruction.
Keywords: Gossypiboma, bowel obstruction, transmural migration, surgical swab, cesarean section
Introduction
Gossypiboma, also known as a retained surgical sponge, is a rare but potentially serious complication that arises from surgical procedures. The term “gossypiboma” is derived from the Latin words “gossypium”, meaning cotton, and the Swahili word “boma”, meaning place of concealment.1 It is also referred to by other synonyms such as Gauzoma, Textiloma, Cottonoma, and Muslinoma. Gossypiboma can have significant implications for patient health, leading to increased morbidity and mortality rates. While some cases may remain asymptomatic for an extended period, ranging from years to even several months following the operation, others can present with symptoms as early as 3–12 weeks or as late as 5–7 years post-surgery.2
When a surgical sponge is unintentionally left inside the patient’s body, it acts as a foreign object and can give rise to various complications. Intra-abdominal gossypiboma can cause the formation of abdominal or pelvic abscesses, fistulas, or even migrate through the bowel wall.3 These complications can have a significant impact on the patient’s well-being. In this case study, we report a specific case of a retained surgical sponge that resulted in acute bowel obstruction due to its complete transmural migration into the small bowel. By presenting this case, we aim to highlight the potential risks associated with gossypiboma and emphasize the importance of its timely detection and management.
Case Report
We present the case of a 26-year-old female patient who was admitted to the hospital with a history of abdominal pain persisting for 20 days. The patient reported experiencing colicky abdominal pain, as well as symptoms of nausea, vomiting, and constipation over the past three days. The patient’s medical history revealed a previous cesarean section performed seven months ago. Upon physical examination, there were no significant findings of abdominal distention. However, mild tenderness was observed in the paraumbilical region, and increased bowel sounds were noted. No abnormal findings were detected during the digital rectal examination. Blood tests indicated mild leukocytosis, while a urine examination revealed the presence of white blood cells and epithelial cells. An abdominal and pelvic ultrasound was performed, which revealed fatty liver and cystitis. Additionally, an abdominal X-ray was conducted and revealed the presence of radiopaque material in the abdomen (Figure 1).
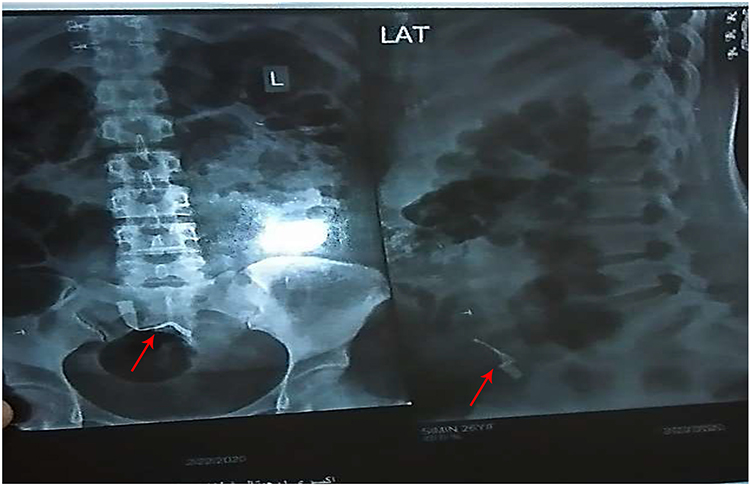 |
Figure 1 Abdominal X-ray(red arrow) showing the presence of radiopaque material(abdominal compress) in the abdomen. |
Based on the clinical findings, the patient underwent an exploratory laparotomy. During the operation, a distended loop of the small bowel was identified. By carefully manipulating the small bowel, a firm loop of ileum located 70cm away from the ileocecal valve was discovered. The distal intestine appeared normal in size, with only a small pointed serosal scratch observed on the wall of the affected loop. An incision was made over the loop, revealing a surgical sponge lodged within it (Figure 2). The sponge was carefully removed, and the bowel was repaired.
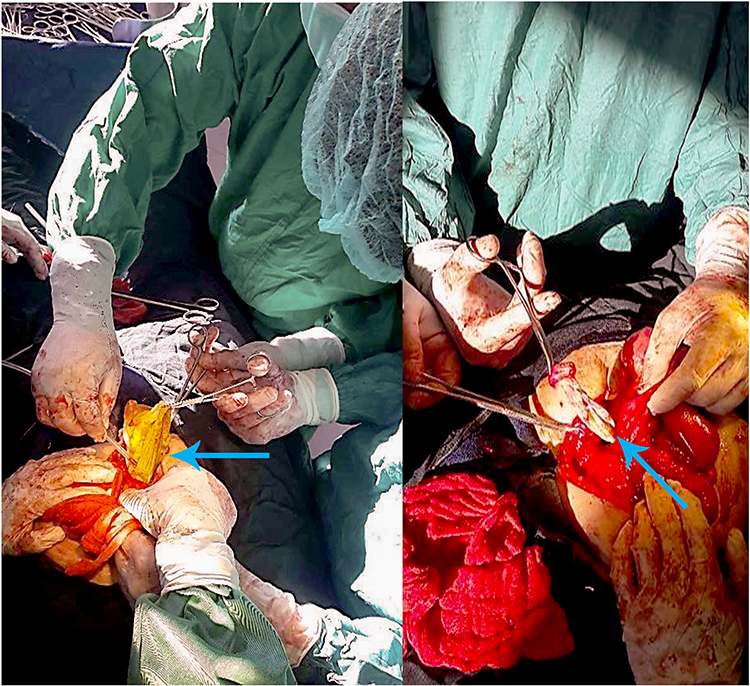 |
Figure 2 Intraoperative photograph(Blue arrow) showing the surgical sponge lodged within the loop of the ileum. |
Following the surgery, the patient’s post-operative course was uneventful. She was discharged from the hospital after six days and remained in good health during the eight-month follow-up period. This case highlights the importance of considering gossypiboma, or retained surgical sponges, as a potential cause of abdominal symptoms in patients with a history of previous surgery. Timely detection and intervention, such as exploratory laparotomy, are crucial in preventing complications and ensuring favorable patient outcomes.
Discussion
The retention of surgical sponges in the peritoneal cavity is an infrequent but avoidable medical error. The reported incidence of gossypiboma, or retained surgical sponges, varies between 1 in 100 and 1 in 3000 for all surgical interventions and between 1 in 1000 and 1 in 1500 for intra-abdominal operations.1 Several factors contribute to the retention of sponges, including emergency surgery, unexpected changes in the surgical procedure, disorganization, hurried sponge counts, long operations, unstable patient condition, inexperienced staff, inadequate staff numbers, and obesity.1 Gossypiboma can elicit two types of body responses: exudative or septic fibrosis. Complications of gossypiboma include adhesion formation, fistula formation, abscess formation, and transmural migration. The retained foreign body causes pressure necrosis of the bowel wall and can partially or completely migrate into the bowel lumen. Subsequently, the perforation created can close spontaneously after migration is complete.2 Patients with gossypiboma often present with symptoms such as abdominal pain, anorexia, nausea, vomiting, and weight loss, which can result from obstruction or a malabsorptive-type syndrome caused by intra-abdominal bacterial overgrowth or multiple intestinal fistulas.4 Plain abdominal radiography can aid in diagnosis when a radiopaque marker of the retained surgical sponge is visible. However, this imaging method may not be effective when markers are disintegrated or fragmented over time. Ultrasonography can detect retained surgical sponges, which appear echogenic and create delineated acoustic shadows. Additionally, computed tomography (CT) scans may reveal spongiform gas bubbles and a low-density mass with prominent and prolonged rim enhancement, suggestive of a retained surgical sponge.5 In our patient’s case, the presence of a radiopaque marker on the surgical sponge allowed for diagnosis through plain radiography. Surgical exploration remains the preferred treatment for gossypiboma. However, in certain cases, surgical intervention may not be necessary as spontaneous migration can occur, leading to the expulsion of the foreign material through the anus during defecation. Percutaneous approaches are applicable for the removal of readily accessible foreign bodies but are not suitable for intra-abdominal foreign bodies. Laparoscopic methods have also been employed to remove gossypiboma.6 To prevent the retention of foreign bodies inside patients, three essential measures should be implemented. First, meticulous counting of all surgical materials should be performed. Second, thorough exploration of the surgical site at the conclusion of procedures is crucial. Lastly, the routine use of surgical textile materials that have a radiopaque marker can enhance visibility and aid in the detection of retained surgical sponges.7
Conclusion
Gossypiboma is an avoidable complication resulting from the retention of surgical sponges inside the peritoneal cavity. Vigilant sponge counting, thorough exploration of the surgical site, and the use of radiopaque markers on surgical textile materials are key measures to prevent such occurrences. By implementing these preventive measures and raising awareness among healthcare professionals, we can enhance patient safety and minimize the risks associated with gossypiboma.
Ethical Approval
This case report is exempt from ethical approval as determined by the ethical review board at our institution, given the nature of the article.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this article and the accompanying image. A copy of the written consent is available for review by the editor-in-chief of this journal upon request.
Acknowledgment
The authors would like to express their sincere gratitude to the patient’s guardians for providing consent to include the case details and photographs in this publication. Their cooperation and willingness to share the information have been invaluable in contributing to the medical literature and advancing patient care.
Funding
No specific funding was received for this case report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Lata I, Kumar D, Sahu S. Gossypiboma: a rare cause of acute abdomen: a case report and review of literature. Int J Crit Illn Inj Sci. 2011;1(2):157–160. doi:10.4103/2229-5151.84805
2. Agrawal H, Gupta N, Krishengowda U, Gupta AK, Naskar D, Durga CK. Transmural migration of a gossypiboma: a rare cause of acute abdomen. Indian J Surg. 2018;80(1):84–86. doi:10.1007/s12262-017-1660-9
3. Khan HS, Ahmed M. Gossypiboma as a Cause of Intestinal Obstruction. J Coll Physicians Surg Pak. 2014;24(3):188–189.
4. Biswas RS, Ghosh SG. Gossypiboma and surgeon: current medicolegal perspectives. Indian J Surg. 2018;80(4):318–322.
5. Sarkar M, Ghosh K. Spontaneous transmural migration of a retained surgical mop into the small intestinal lumen, causing sub-acute intestinal obstruction: a case report. TAJ. 2006;19(1):34–37.
6. Umana J. Gossypiboma and Its Implication: case Series. J West Afr Coll Surg. 2012;2(2):95–105.
7. Gencosmanoglu R, Inceoglu R. An unusual case of small bowel obstruction: gossypiboma - case report. BMG Surg. 2003;3:6.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.