")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Activities of Daily Living and Depression in Chinese Elderly of Nursing Homes: A Mediation Analysis
Authors Gao L, Yang J, Liu J , Xin T, Liu Y
Received 25 October 2022
Accepted for publication 19 December 2022
Published 6 January 2023 Volume 2023:16 Pages 29—38
DOI https://doi.org/10.2147/PRBM.S394787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Lunan Gao,1 Jinhong Yang,2 Jiang Liu,1 Tingting Xin,1 Yuxiu Liu1
1School of Nursing, Weifang Medical University, Weifang, People’s Republic of China; 2Department of Oncology, Weifang People’s Hospital, Weifang, People’s Republic of China
Correspondence: Yuxiu Liu, School of Nursing, Weifang Medical University, No. 7166 Baotong Western Street, Weifang, People’s Republic of China, Tel +8618663608162, Email [email protected]
Purpose: This study aimed to explore the role of sleep quality as a mediator in the activities of daily living (ADLs) and depression.
Patients and Methods: Participants (N=645; age≥ 60) were included in six nursing homes in Weifang, Shandong Province, using convenience sampling. Participants completed questionnaires to assess sleep quality, ADLs, and depression. Depression condition was assessed by the Patient Health Questionnaire (PHQ-9), ADLs was assessed by the Barthel Index (BI), and sleep quality was measured by the Pittsburgh Sleep Quality Index (PSQI). Mediation analysis was carried out by SPSS PROCESS.
Results: ADLs (r=0.449, P< 0.01) and sleep quality (r=0.450, P< 0.01) were found to be positively associated with depression among the elderly. Sleep quality plays a significant mediating role in the influence of ADLs on depression in the elderly in nursing homes (Bootstrap 95% CI [0.076, 0.139]), The pathway from ADLs to sleep quality to depression yielded a medium effect size of 20.23%.
Conclusion: ADLs help to explain how sleep quality partly mediates depression among the elderly in nursing homes. It is therefore recommended that timely detection and efficient interventions should focus on promoting physical function and improving sleep quality among the elderly in nursing homes.
Keywords: elderly, nursing home, activities of daily living, depressive symptom, sleep quality
Introduction
Depression is one of the most common problems in the elderly in nursing homes besides chronic illness.1 A meta-analysis indicated that the detection rate of depressive symptoms in nursing homes was 37.49% in China.2 Previous studies have reported that depression is generally associated with both internal and external factors including aging, health status, and one’s physical function among the elderly.3–5 Depression is characterized by negative emotions and less motivation, leading to an inability to perform daily tasks effectively, which is also associated with the declining ADLs of the elderly.6–8 However, the mechanism connecting depressive symptoms and impaired ADLs in the elderly in nursing homes has not been established. Exploring the theoretical mechanisms underlying these variables may help to reduce the emotional burden on the elderly in nursing homes.
Previous studies have found that the rate of depression in the elderly may increase as their ADLs decline.9 A recent study identified that there was a significant correlation between depression and functional disability among the elderly in Nigeria,4 and many cross-sectional studies showed that ADLs impairment had a negative effect on depression among Chinese elderly people.3,10–13 However, the mediating pathways of ADLs and depression remain unclear. Therefore, an important unsolved question for elderly health is the extent to which the negative effect of ADLs on depression might be alleviated by targeting modifiable mediators.
Sleep is an important determinant of health for the elderly and is closely associated with physical fitness. There is a positive correlation between sleep and ADLs impairment in the elderly, and it presents a nonlinear dose-response relationship.14,15 Impaired ADLs is linked to an increased risk of comorbid depression symptoms, and short sleep duration may play a mediating role in this association.16 Poor ADLs are also linked to sleep apnea and sleep-disordered breathing.17 A cross-sectional survey showed that elderly people with ADLs impairments almost always had sleep disturbances.18 In addition, the elderly with impaired ADLs are more likely to have sleep problems.19,20 The elderly with impaired ADLs in nursing homes are more likely to be exposed to noise or the bright light at night than those living in homes or communities which can interfere with initiating or maintaining sleep.20,21
Sleep and depression may be reciprocally related.22,23 Sleep disturbance is a behavior that is strongly associated with depression, which will further aggravate depression.24–26 Two types of sleep disturbance related to depression are sleep duration and insomnia. A cross-sectional study has found a U-shaped relationship between sleep duration and depressive symptoms.27,28 Subjective poor sleep quality manifests in various forms, such as insomnia, feeling fatigued, and sleepy during the day.29 Poor sleep quality, such as insomnia, is now recognized as a critical feature of depression.30 Insomnia has been shown in numerous studies to be an independent predictor of depressive disorders31,32 and suicide.33,34 Poor sleep quality is the most prominent symptom in depressive patients and was formerly regarded as the main secondary manifestation of depression.29 However, many longitudinal studies have identified poor sleep quality as an independent risk factor for the development of emerging or recurrent depression among young, middle‐aged and the elderly.35–37 Evidence was found for a possible causal relationship between insomnia symptoms and depressive symptoms, and subjective well-being.38 Above all, there have been more cross-sectional studies that support the hypothesis that poor sleep quality predicts depression or depressive symptoms. Furthermore, an electroencephalogram (EEG) study established that insomnia was a significant risk factor for depression.39 Sleep disturbance subsequently contributes to negative emotions, especially depression. Sleep disturbance can also have an impact on one’s emotional response and social function.40 A previous study reported that early intervention for patients with sleep disturbances could reduce the incidence of depression.41 But a theoretically meaningful mechanism for connecting sleep and depression in the elderly in nursing homes has not yet been found. Investigating the relationship between these variables may be beneficial in managing the emotional changes of the elderly.
In conclusion, there have been many studies focusing on the relationship between ADLs and depression in the elderly in nursing homes.4,42 Akosile et al4 reported that significant correlation existed between depression scores and individual quality of life and functional disability domains and between overall QoL and each functional disability domain. Zhao et al42 found that active leisure activities significantly mediated the effect of moderate/severe depressive symptoms on physical function. However, current studies do not examine the role of sleep quality between the two variables among the elderly in nursing homes. Sleep problems are prevalent among the elderly in nursing homes.1 The literatures cited above also provide a theoretical foundation for ADLs and sleep quality on depression. The mediating role of sleep in ADLs and depression deserves quantitative study. We hypothesize that sleep quality would mediate the association between ADLs and depression.
Materials and Methods
Participant and Design
This cross-sectional survey of research data was conducted in six nursing homes in Weifang city, Shandong province in China between August 2021 and January 2022. A total of 672 elderly people with age over 60 years were included in the six nursing homes using convenience sampling. Those who were included in this research met the eligibility criteria: (1) at least 60 years old, (2) verbal consent obtained from each participant, (3) residing in the nursing homes for three months or more. The exclusion criteria were: (1) diagnosed with depression and taking antidepressant drugs; (2) the absence of coma, being unconscious, or having a severe cognitive deficit. Three well-trained postgraduate nursing students distributed questionnaires to the remaining 655 elderly people who fulfilled the inclusion criteria. The questionnaires were completed principally by three trained postgraduate nursing students, who read the items and marked the responses of the elderly on the questionnaires. Although illustrated exhaustively, ten of them refused to join the research because they were tired or uninterested. Ultimately, leaving 645 participants participated in the research with a response rate of 96.0%.
Data Collection
Before the survey, we got in touch with the managers of the six nursing homes and asked about their facilities’ size and the number of the elderly. We obtained permission from the managers of the six nursing homes through telephone, Wechat, or face-to-face interviews. The managers of the six nursing homes helped us to explain the purpose of the survey to the elderly in nursing homes and obtain informed consent from each elderly people. Participants were informed that their participation in this study was entirely voluntary and their anonymity and confidentiality were protected. Each elderly has their own room, and after asking permission, we entered the elderly’s room for a face-to-face interview. Some basic personal information such as age, gender, disease history, and medication history, was obtained through the medical records of the nursing homes.
Measurements
Socio-Demographic Characteristics
The data of resident-level factors were collected using the self-design sheet, including age, gender, marital status, education level, main source of income, number of children, living style of elderly before admission to nursing homes, length of residence, number of chronic diseases, and medicine.
Depression
Depression in the elderly was assessed using the Patient Health Questionnaire (PHQ-9).43 In our study, and Cronbach’s α of the PHQ-9 was 0.916. The critical score was 5, 10, 15, and 20.44 No depression has a score of 0–4. Mild depression has a score of 5–9. Moderate depression has a score of 10–14; and severely severe depression has a score of 15–19 and 20–27 respectively. A score of 5 or higher was regarded as depression.
Sleep Quality
The Pittsburgh Sleep Quality Index (PSQI) was used to assess sleep quality.45 The PSQI is a 17-item scale, with seven components assessing subjective sleep quality, latency, duration, efficiency, disturbance, use of sleep medication, and daytime dysfunction. Participants answered the seven items on a 4-point Likert-type scale. The total score is the sum of the 7 dimensions, with higher scores indicating poorer levels of sleep quality. The rating scale was 0–5 for sleep very good, 6–10 for good sleep quality, and 11–15 for poor sleep quality, and 16–21 for terrible sleep quality.46 Internal consistency was measured using Cronbach’s α (0.837).
Activities of Daily Living (ADLs)
The activities of daily living scale was used to assess the physical function of the elderly using a modified Barthel index (BI).47 The modified BI is a 7-item scale except for one unsuitable item: stairs. The elderly are advised to use the elevator instead of the stairs in nursing homes in China, and we deleted item 10 (walk up and down stairs) in the original scale. To prevent participants from feeling repetitive in their questions, instead of asking items one by one, we combined the bowel and bladder into one question in toileting. The higher the score, the worse the activity of daily living function is. Cronbach’s α coefficient of the scale in this study was 0.970.
Data Analysis
Data analysis were performed using SPSS 23.0 for Windows (IBM Corp., Armonk, NY, USA) software. Descriptive statistics were used to present the demographic characteristics and study variables. Categorical variables and continuous variables were described by frequencies (percentages) and means (standard deviations) respectively. The normality of the data was examined with a quantile-quantile plot (QQ plot). Spearman correlation was used to investigate the correlations of non-normally distributed data. To address the mediating effect of sleep quality between depression and physical function, the bootstrapping procedure in the SPSS PROCESS 3.4 version was performed to present a regression-based mediation analysis.48 ADLs (independent variable), sleep quality (a mediator), and depression symptoms (dependent variable) total scores were used as an observable variable in the mediation model. The direct, indirect, and total effects were calculated using the product of coefficients strategy and tested using the bootstrapping method (N=5000)49. If the 5000 bootstrap 95% bias-corrected confidence intervals (CI) did not cross 0, the indirect effect is significant. The covariates of age, gender, marital status, education level, main source of income, number of children, living style of elderly before admission to nursing homes, length of residence, number of chronic diseases, and medicine were controlled in the mediation model. P<0.05 (two-tailed) was considered statistically significant.
Results
Demographic Characteristics
A total of 645 old adults in nursing homes participated in the research, with an average age of 77.43±9.96 years. A majority of respondents were female 350 (54.3%). The score of PHQ-9 was (4.63±5.97), PSQI was (7.92±5.16), and ADLs was (6.00±5.79). More information is shown in Table 1.
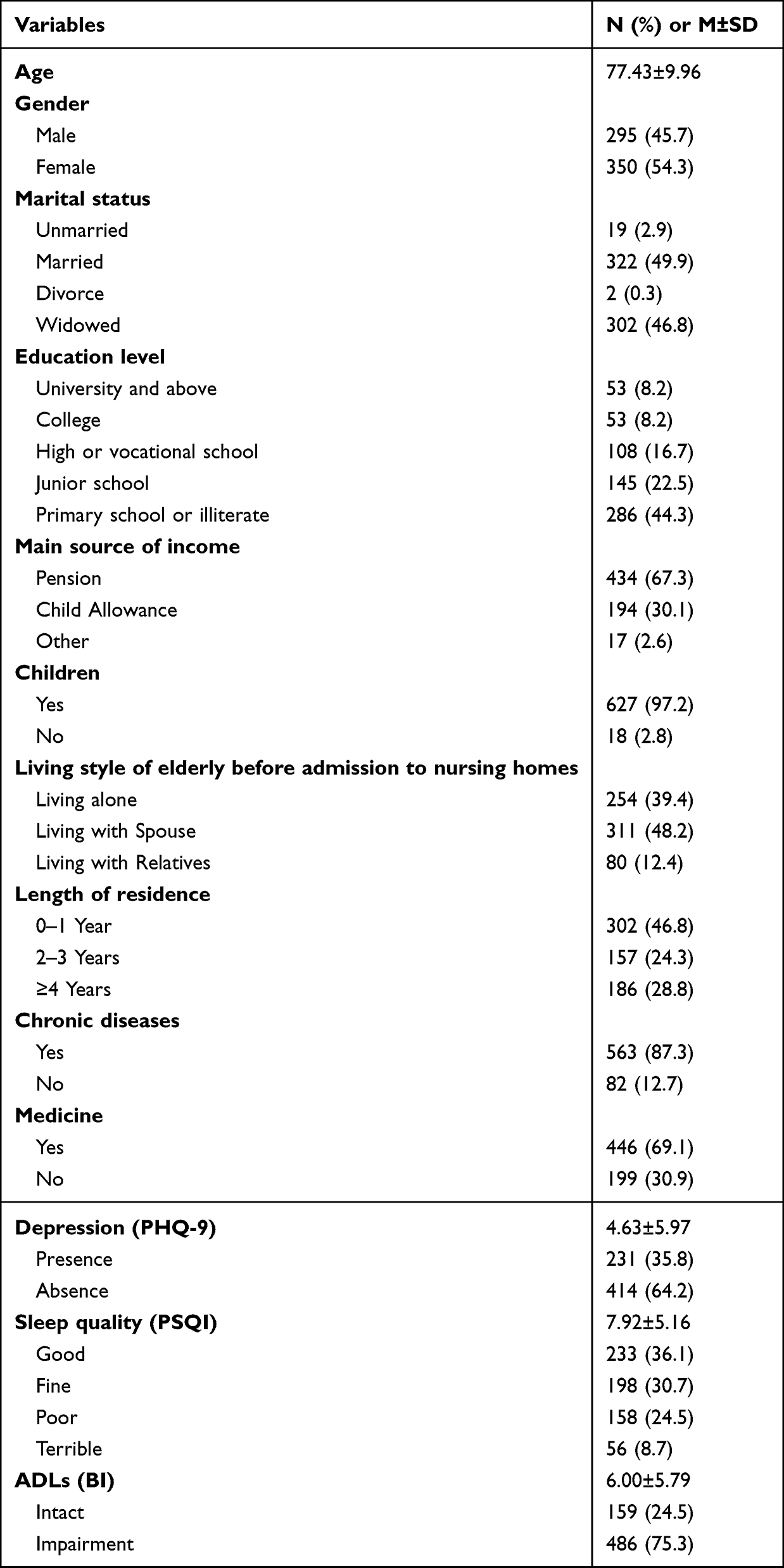 |
Table 1 Demographic Characteristics (N = 645) |
Correlations Between Variables
Depression was positively correlated with ADLs (r=0.449, P<0.01) and sleep quality (r=0.450, P<0.01), and negatively correlated with length of residence (r=−0.232, P<0.01), marital status (r=−0.096, P<0.05), and age (r=−0.138, P<0.01). Sleep quality was significantly correlated with age (r=0.117, P<0.01). ADLs was significantly correlated with the main source of income (r=−0.084, P<0.05). The detail is shown in Table 2.
 |
Table 2 Bivariate Correlations Among Depression, Sleep Quality, ADLs (r) |
Sleep Quality as a Mediator Between Depression and ADLs
The following variables were entered into the models as covariates: age, gender, education level, marital status, and main source of income, length of residence, living style of elderly before admission to nursing homes, number of chronic diseases and medicine, number of children. The regression analysis showed that ADLs and sleep quality could directly predicted depression (β=0.418, P<0.01; β=0.306, P<0.01). The detail is shown in Table 3.
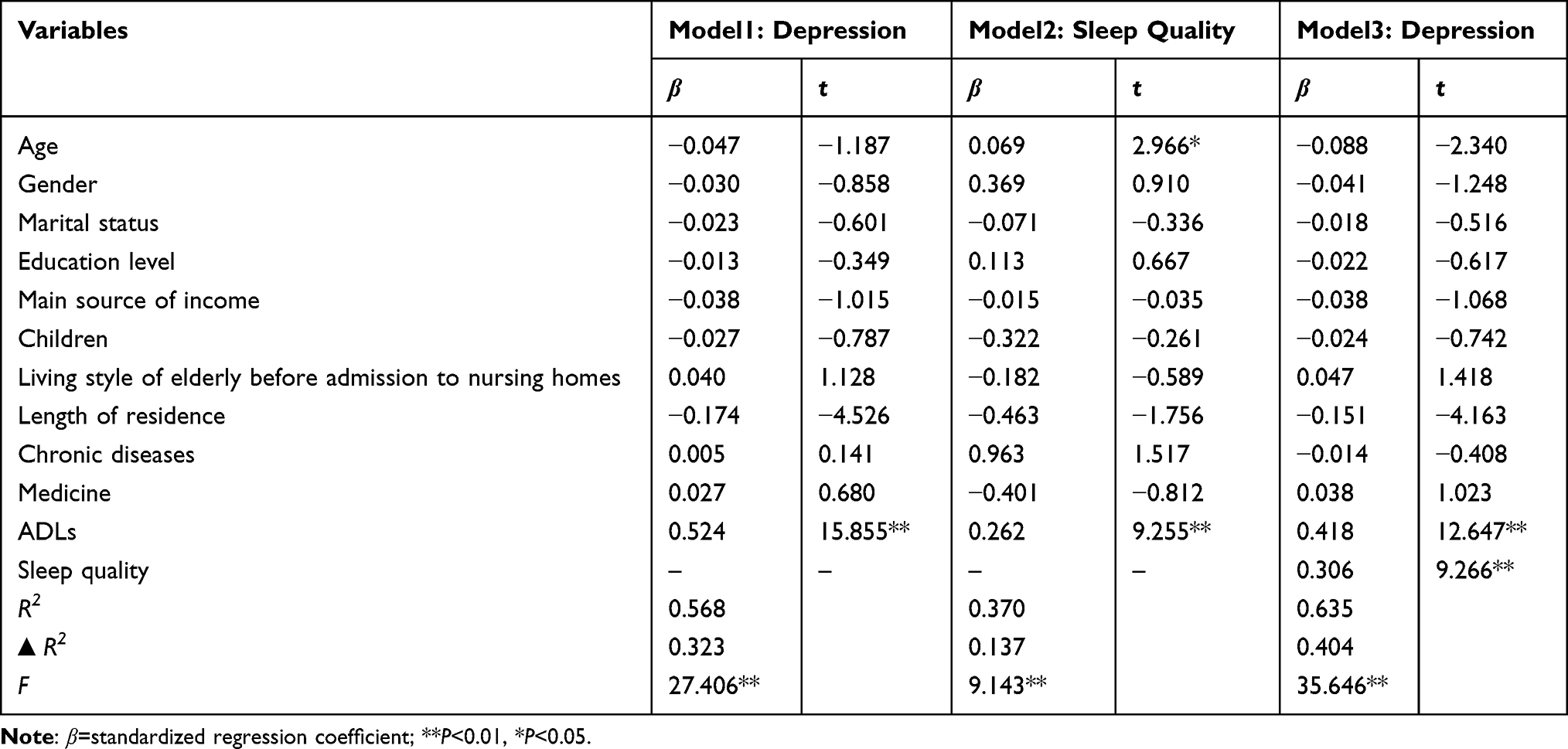 |
Table 3 The Indirect Effects of Physical Function on Depressive Symptoms by Sleep Quality |
As shown in Table 4, the direct effect of ADLs on depression was 0.418 (95% CI [0.311, 0.425]). A significant indirect effect of ADLs on depression through sleep quality was 0.106 (95% CI [0.076, 0.139]). The whole model explained that 20.23% of the effects of ADLs on depression were mediated through sleep quality in the elderly in nursing homes. The mediation model is shown in Figure 1.
 |
Table 4 Total and Direct Indirect Effects of Depressive Symptoms on Physical Function by Sleep Quality |
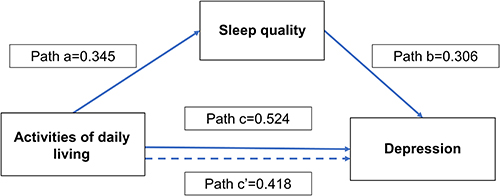 |
Figure 1 Mediation model: Associations among ADL, sleep quality, and depression. |
Discussion
Impaired ADLs (75.3%) and poor sleep quality (33.2%) are highly prevalent in the elderly in nursing homes in China and are correlated with depression (r=0.449, P<0.01; r=0.450, P<0.01). ADLs and sleep quality were found to be positively associated with depression among the elderly in nursing homes. The present study firstly examined sleep quality as a possible mediator of the mechanisms between ADLs and depression among Chinese elderly in nursing homes. Furthermore, these findings confirmed that the elderly with high levels of self-care dependence and poor sleep quality tend to have depression.
The score of PHQ-9 was (4.63±5.97), PSQI was (7.92±5.16), and ADLs was (6.00±5.79). The mean scores of PHQ-9, ADLs, and PSQI in this study were higher than those in previous studies of community-dwelling elderly,50 indicating that the elderly in nursing homes may have poorer ADLs and be more likely to suffer from depression.
In this study, we found that depression was significantly related to ADLs (β=0.524, P<0.01). The regression coefficient of ADLs on depression is statistically significant, with an effect size of 0.418 (95% CI [0.311, 0.425]). Previous studies have reported that impaired ADLs may be a risk factor for depression in the elderly.7 Impaired ADLs in later life reduces the range of activities of the elderly and reduces their opportunities to contact and communicate with the outside world, making them prone to loneliness and disrupting their sense of control over life and other psychological states, leading older people to experience low self-esteem and self-worth.51,52 Besides, impairments in ADLs are associated with a lower quality of life and lack of social activity, which are in turn associated with the development of depression symptoms.53 However, the mechanism is not well understood at present. Identifying potential pathways could not only shed light on the effects of impaired ADLs in the elderly on depressive symptoms, but also on the depression and suicide tendency of the elderly with poor physical health.54
Our study found that sleep quality was also significantly associated with depression (β=0.306, P<0.01). An epidemiological survey has confirmed the association between sleep disturbance and depressive episodes, which was frequently reported to co-occur in a majority of patients.55 According to Krystal et al,56 both sleep disturbances and problems appeared to increase the risk of the occurrence and recurrence of major depression and other psychiatric disorders. Together, sleep quality may influence depressive symptoms. The elderly who sleep too long or too short may have lower sleep efficiency and a higher degree of sleep fragmentation, and are more likely to self-report fatigue, lack of energy in daily life, and depression.1,21,54 The relationship between the two variables needs to be further verified.
In this study, we confirmed that sleep quality was significantly associated with ADLs (β=0.262, P<0.01). Karakurt P and Ünsal A57 believed that adequate sleep could restore physical fitness, and high physical fitness was positively proportional to high ADLs, but may be inversely proportional to depression. Besides, the mechanisms of neurobiological and psychological factors might account for the association of physical activity and sleep quality,58 for example, the thermoregulatory hypotheses and the hypothesis of energy conservation and body restoration.59 Kubala et al60 reported that higher-intensity activity was associated with better sleep quality among middle- to older-aged adults. Collectively, this research supported the theory that more physical activities might be beneficial to sleep quality, and sleep quality is an important intermediate variable between depression and ADLs to some extent.
In conclusion, our cross-sectional results are broadly consistent with previous findings. The regression coefficient of ADLs on depression was statistically significant (β=0.418, t=12.647, P<0.01), when ADLs and sleep quality were both included in the regression analysis together. While sleep quality in the elderly in nursing homes significantly and positively predicted depression (β=0.306, t=9.266, P<0.01) with a mediating effect value of 0.106 and Bootstrap 95% CI (0.076–0.139) for the mediating effect of sleep quality. It could be explained that ADLs could directly predict depression and also play a predictive role through sleep quality. Additionally, as shown in Table 4, the pathway from ADLs to sleep quality to depression yielded a medium effect size of 20.23%, which is consistent with previous studies in the elderly.61–63 The latest cross-sectional study verified that sleep health mediated 20% of the effect of physical activity on depression in the US.63 Another longitudinal analysis in Finland confirmed that physical activity was associated with fewer sleep problems and depressive symptoms in adulthood.61 Similarly, Cahuas et al62 found that physical activity and quality sleep can help teenagers reduce depressive symptoms. Horwath et al64 reported that in “old-old” (aged 80 and older) long-term care facilities residents, moderate dependency in ADLs, sleep disturbances were significantly associated with higher prevalence of depression. Our study found that sleep quality partly mediated the relationship between ADLs and depression among the elderly in nursing homes.
Some notable implications can be provided for clinical practice. Our results confirmed that sleep quality partially mediated the association between ADLs and depression in the elderly in nursing homes. We suggest that the elderly in nursing homes with comorbid impaired physical function and sleep disorders may experience more negative emotion or depression than those only with impaired physical function. Therefore, improving sleep quality may be helpful for the management of the elderly with depression. Sleep quality should be routinely assessed in nursing homes, especially for elderly with depression and impaired ADLs. These findings are very important to take into consideration when integrating interventions into the management of disability and depression. Interventions should address improving sleep quality among the elderly as well as providing them with functional support through health education.
Some limitations in the current study should be noted. Firstly, the cross-sectional study could just reveal a section of these variables in nursing homes, suggesting that subsequent studies should carry out corresponding longitudinal studies on depression in nursing homes. Many studies have reported a reciprocal relationship between sleep and depression and impaired physical function. A reverse mediation (sleep-ADLs-depressive symptoms or sleep-depressive symptoms-ADLs) may also be made. Second, convenient sampling was used which can result in selection bias. Last, the elderly who participated in our study in nursing homes may be more frail and feel lonelier than community- or home-dwelling older people. Thus, the generalizability of our results to other settings should be cautious.
Conclusion
This study showed that depression and poor sleep quality were prevalent among the elderly in nursing homes in China. Furthermore, our study firstly established the mediation model that sleep quality partly mediated the relationship between ADLs and depression among the elderly in nursing homes. These findings help to understand the mechanism and role of ADLs and sleep quality on depression in the elderly in nursing homes. Therefore, we recommend that timely detection and efficient interventions focusing on promoting physical function and improving sleep quality among the elderly in nursing homes may be crucial in improving elderly’s psychological state and other health outcomes.
Ethical Considerations
This study was conducted after Medical Ethics Committee of Weifang Medical University approval (approval number: 2019SL076). All participants were informed of the study content, and verbal informed consent was obtained from themselves or their guardians, which was approved by Weifang Medical University. Before the survey, we obtained permission from the management of each nursing homes, and all participants were told about the purpose of the survey. This study complied with the Declaration of Helsinki.
Acknowledgments
We would like to gratefully acknowledge the elderly who participated in this study.
Funding
1This study was supported by the Youth Grant of the National Natural Science Foundation of China (No.71804129). 2Research on Optimization Path and Management Strategy of Intelligent Aged Care Service in Urban Community under the Mode of “Internet+Aged Care” of Shandong Province Soft Science Research Program” (2022RKY07010).
Disclosure
All authors in this study declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Kim DE, Yoon JY. Factors that influence sleep among residents in long-term care facilities. Int J Environ Res Public Health. 2020;17(6):1889.
2. Zhong YZ, Gao J, Bai DX, et al. A meta-analysis of detection rate of depressive symptoms among the elderly in pension institutions in China. Chin Ment Health J. 2020;34(12):1006–1015.
3. Wang X, Shang S, Yang H, et al. Associations of psychological distress with positive psychological variables and activities of daily living among stroke patients: a cross-sectional study. BMC Psychiatry. 2019;19(1):381. doi:10.1186/s12888-019-2368-0
4. Akosile CO, Mgbeojedo UG, Maruf FA, Okoye EC, Umeonwuka IC, Ogunniyi A. Depression, functional disability and quality of life among Nigerian older adults: prevalences and relationships. Arch Gerontol Geriatr. 2018;74:39–43. doi:10.1016/j.archger.2017.08.011
5. Liang CE, Zhan T, Li XM, et al. Studying on the influence of physical health on the depressive suicidal tendencies of the elderly mediated by social relations. Chin Health Serv Manage. 2020;37(06):472–476.
6. Matos Queirós A, von Gunten A, Martins M, Wellens NIH, Verloo H. The forgotten psychopathology of depressed long-term care facility residents: a call for evidence-based practice. Dement Geriatr Cogn Dis Extra. 2021;11(1):38–44. doi:10.1159/000514118
7. Kong LN, Zhang N, Yuan C, Yu ZY, Yuan W, Zhang GL. Relationship of social support and health-related quality of life among migrant older adults: the mediating role of psychological resilience. Geriatr Nurs. 2021;42(1):1–7. doi:10.1016/j.gerinurse.2020.10.019
8. Song D, Zhou J, Ma J, et al. Sleep disturbance mediates the relationship between depressive symptoms and cognitive function in older adults with mild cognitive impairment. Geriatr Nurs. 2021;42(5):1019–1023. doi:10.1016/j.gerinurse.2021.06.004
9. Kvæl LAH, Bergland A, Telenius EW. Associations between physical function and depression in nursing home residents with mild and moderate dementia: a cross-sectional study. BMJ open. 2017;7(7):e016875. doi:10.1136/bmjopen-2017-016875
10. Kimball SM, Mirhosseini N, Rucklidge J. Database analysis of depression and anxiety in a community sample-response to a micronutrient intervention. Nutrients. 2018;10(2). doi:10.3390/nu10020152
11. Yang Y. How does functional disability affect depressive symptoms in late life? The role of perceived social support and psychological resources. J Health Soc Behav. 2006;47(4):355–372. doi:10.1177/002214650604700404
12. Tang X, Qi S, Zhang H, Wang Z. Prevalence of depressive symptoms and its related factors among China’s older adults in 2016. J Affect Disord. 2021;292:95–101. doi:10.1016/j.jad.2021.04.041
13. Deng Y, Paul DR. The relationships between depressive symptoms, functional health status, physical activity, and the availability of recreational facilities: a rural-urban comparison in middle-aged and older Chinese adults. Int J Behav Med. 2018;25(3):322–330. doi:10.1007/s12529-018-9714-3
14. Chien MY, Chen HC. Poor sleep quality is independently associated with physical disability in older adults. J Clin Sleep Med. 2015;11(3):225–232. doi:10.5664/jcsm.4532
15. Sun Y, Lyu YB, Zhong WF, et al. Association between sleep duration and activity of daily living in the elderly aged 65 years and older in China. Natl Med J China. 2022;102(02):108–113.
16. Liu JK, Li S, Lin J, et al. The comorbid relationship between activities of daily living and symptoms of depression and anxiety in the elderly. Chin J Prev Cont Chron Dis. 2022;30(04):251–255.
17. Sandberg O, Franklin KA, Bucht G, Gustafson Y. Sleep apnea, delirium, depressed mood, cognition, and ADL ability after stroke. J Am Geriatr Soc. 2001;49(4):391–397. doi:10.1046/j.1532-5415.2001.49081.x
18. Xie LQ, Yang BX, Liao YH, et al. Sleep disturbance in older adults with or without mild cognitive impairment and its associated factors residing in rural area, China. J Geriatr Psychiatry Neurol. 2021;34(6):632–641. doi:10.1177/0891988720964249
19. Çavuşoğlu Ç, Deniz O, Tuna Doğrul R, et al. Frailty is associated with poor sleep quality in the oldest old. Turk J Med Sci. 2021;51(2):540–546. doi:10.3906/sag-2001-168
20. Okoye SM, Szanton SL, Perrin NA, et al. Objectively measured sleep and physical function: associations in low-income older adults with disabilities. Sleep Health. 2021;7(6):735–741. doi:10.1016/j.sleh.2021.09.001
21. Gulia KK, Kumar VM. Sleep disorders in the elderly: a growing challenge. Psychogeriatrics. 2018;18(3):155–165. doi:10.1111/psyg.12319
22. Ouyang P, Sun W. Depression and sleep duration: findings from middle-aged and elderly people in China. Public Health. 2019;166:148–154. doi:10.1016/j.puhe.2018.10.007
23. Chung KH, Li CY, Kuo SY, Sithole T, Liu WW, Chung MH. Risk of psychiatric disorders in patients with chronic insomnia and sedative-hypnotic prescription: a nationwide population-based follow-up study. J Clin Sleep Med. 2015;11(5):543–551. doi:10.5664/jcsm.4700
24. Iranpour S, Kheirabadi GR, Esmaillzadeh A, Heidari-Beni M, Maracy MR. Association between sleep quality and postpartum depression. J Res Med Sci. 2016;21:110. doi:10.4103/1735-1995.193500
25. Steiger A, Pawlowski M. Depression and sleep. Int J Mol Sci. 2019;20(3):607. doi:10.3390/ijms20030607
26. Nishitani N, Kawasaki Y, Sakakibara H. Insomnia affects future development of depression in workers: a 6-year cohort study. Nagoya J Med Sci. 2019;81(4):637–645. doi:10.18999/nagjms.81.4.637
27. Shen L, Jia GY, Li JY, Zhang SY, Sun HH, Xue ZQ. A study on the relationship between pain, sleep and depression among the elderly in China—based on the 2018 China health and retirement longitudinal study. Chin Prev Med. 2022;2022;1–6.
28. Zhang XF, Liu F, Liu WP. Relationship between sleep duration and depressive symptoms in middle-aged and elderly people in four provinces of China. Chin J Epidemiol. 2021;42(11):1955–1961.
29. Fang H, Tu S, Sheng J, Shao A. Depression in sleep disturbance: a review on a bidirectional relationship, mechanisms and treatment. J Cell Mol Med. 2019;23(4):2324–2332. doi:10.1111/jcmm.14170
30. Dinis J, Bragança M. Quality of sleep and depression in college students: a systematic review. Sleep Sci. 2018;11(4):290–301. doi:10.5935/1984-0063.20180045
31. Riemann D. Does effective management of sleep disorders reduce depressive symptoms and the risk of depression? Drugs. 2009;69(Suppl 2):43–64. doi:10.2165/11531130-000000000-00000
32. Riemann D, Voderholzer U. Primary insomnia: a risk factor to develop depression? J Affect Disord. 2003;76(1–3):255–259. doi:10.1016/S0165-0327(02)00072-1
33. Bernert RA, Turvey CL, Conwell Y, Joiner TE Jr. Association of poor subjective sleep quality with risk for death by suicide during a 10-year period: a longitudinal, population-based study of late life. JAMA psychiatry. 2014;71(10):1129–1137. doi:10.1001/jamapsychiatry.2014.1126
34. Bjørngaard JH, Bjerkeset O, Romundstad P, Gunnell D. Sleeping problems and suicide in 75,000 Norwegian adults: a 20 year follow-up of the HUNT I study. Sleep. 2011;34(9):1155–1159. doi:10.5665/SLEEP.1228
35. Lauer CJ, Schreiber W, Holsboer F, Krieg JC. In quest of identifying vulnerability markers for psychiatric disorders by all-night polysomnography. Arch Gen Psychiatry. 1995;52(2):145–153. doi:10.1001/archpsyc.1995.03950140063009
36. Jaussent I, Bouyer J, Ancelin ML, et al. Insomnia and daytime sleepiness are risk factors for depressive symptoms in the elderly. Sleep. 2011;34(8):1103–1110. doi:10.5665/SLEEP.1170
37. Chang PP, Ford DE, Mead LA, Cooper-Patrick L, Klag MJ. Insomnia in young men and subsequent depression. The Johns Hopkins precursors study. Am J Epidemiol. 1997;146(2):105–114. doi:10.1093/oxfordjournals.aje.a009241
38. Lane JM, Jones SE, Dashti HS, et al. Biological and clinical insights from genetics of insomnia symptoms. Nat Genet. 2019;51(3):387–393. doi:10.1038/s41588-019-0361-7
39. Wang YQ, Li R, Zhang MQ, Zhang Z, Qu WM, Huang ZL. The neurobiological mechanisms and treatments of REM sleep disturbances in depression. Curr Neuropharmacol. 2015;13(4):543–553. doi:10.2174/1570159X13666150310002540
40. Liu R, Shao W, Lai JK, Zhou L, Ren M, Sun N. Identification of comprehensive geriatric assessment-based risk factors for insomnia in elderly Chinese hospitalized patients. Aging Med. 2021;4(1):26–34. doi:10.1002/agm2.12146
41. Her J, Cho MK. Effect of aromatherapy on sleep quality of adults and elderly people: a systematic literature review and meta-analysis. Complement Ther Med. 2021;60:102739. doi:10.1016/j.ctim.2021.102739
42. Zhao M, Wang Y, Wang S, Yang Y, Li M, Wang K. Association between depression severity and physical function among Chinese nursing home residents: the mediating role of different types of leisure activities. Int J Environ Res Public Health. 2022;19(6):3543.
43. Levis B, Benedetti A, Thombs BD. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ. 2019;365:l1476. doi:10.1136/bmj.l1476
44. Smarr KL, Keefer AL. Measures of depression and depressive symptoms. Arthritis Care Res. 2020;72(Suppl S10):608–629. doi:10.1002/acr.24191
45. Wang Y, Xiao H, Zhang X, Wang L. The role of active coping in the relationship between learning burnout and sleep quality among college students in China. Front Psychol. 2020;11:647. doi:10.3389/fpsyg.2020.00647
46. Doi Y, Minowa M, Uchiyama M, et al. Psychometric assessment of subjective sleep quality using the Japanese version of the Pittsburgh Sleep Quality Index (PSQI-J) in psychiatric disordered and control subjects. Psychiatry Res. 2000;97(2–3):165–172. doi:10.1016/S0165-1781(00)00232-8
47. Pashmdarfard M, Azad A. Assessment tools to evaluate Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL) in older adults: a systematic review. Med J Islam Repub Iran. 2020;34:33. doi:10.34171/mjiri.34.33
48. Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instrum Comput. 2004;36(4):717–731. doi:10.3758/BF03206553
49. Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–1182. doi:10.1037/0022-3514.51.6.1173
50. Wang F, Liu S, Zhang Q, et al. Prevalence of depression in older nursing home residents in high and low altitude regions: a comparative study. Front Psychiatry. 2021;12:669234. doi:10.3389/fpsyt.2021.669234
51. Tiong WW, Yap P, Huat Koh GC, Phoon Fong N, Luo N. Prevalence and risk factors of depression in the elderly nursing home residents in Singapore. Aging Ment Health. 2013;17(6):724–731. doi:10.1080/13607863.2013.775638
52. Jongenelis K, Pot AM, Eisses AM, Beekman AT, Kluiter H, Ribbe MW. Prevalence and risk indicators of depression in elderly nursing home patients: the AGED study. J Affect Disord. 2004;83(2–3):135–142. doi:10.1016/j.jad.2004.06.001
53. Vest MT, Murphy TE, Araujo KL, Pisani MA. Disability in activities of daily living, depression, and quality of life among older medical ICU survivors: a prospective cohort study. Health Qual Life Outcomes. 2011;9:9. doi:10.1186/1477-7525-9-9
54. Webb CA, Cui R, Titus C, Fiske A, Nadorff MR. Sleep disturbance, activities of daily living, and depressive symptoms among older adults. Clin Gerontol. 2018;41(2):172–180. doi:10.1080/07317115.2017.1408733
55. Ohayon MM, Caulet M, Lemoine P. Comorbidity of mental and insomnia disorders in the general population. Compr Psychiatry. 1998;39(4):185–197. doi:10.1016/S0010-440X(98)90059-1
56. Krystal AD, Thakur M, Roth T. Sleep disturbance in psychiatric disorders: effects on function and quality of life in mood disorders, alcoholism, and schizophrenia. Ann Clin Psychiatry. 2008;20(1):39–46. doi:10.1080/10401230701844661
57. Karakurt P, Ünsal A. Fatigue, anxiety and depression levels, activities of daily living of patients with chronic obstructive pulmonary disease. Int J Nurs Pract. 2013;19(2):221–231. doi:10.1111/ijn.12055
58. Briguglio M, Vitale JA, Galentino R, et al. Healthy Eating, Physical Activity, and Sleep Hygiene (HEPAS) as the winning triad for sustaining physical and mental health in patients at risk for or with neuropsychiatric disorders: considerations for clinical practice. Neuropsychiatr Dis Treat. 2020;16:55–70. doi:10.2147/NDT.S229206
59. Oliveira L, Silva AOD, Santos M, Ritti-Dias RM, Diniz PRB. Exercise or physical activity: which is more strongly associated with the perception of sleep quality by adolescents? Rev Paul Pediatr. 2018;36(3):322–328. doi:10.1590/1984-0462/;2018;36;3;00014
60. Kubala AG, Buysse DJ, Brindle RC, et al. The association between physical activity and a composite measure of sleep health. Sleep Breath. 2020;24(3):1207–1214. doi:10.1007/s11325-019-02007-x
61. Kaseva K, Dobewall H, Yang X, et al. Physical activity, sleep, and symptoms of depression in adults—testing for mediation. Med Sci Sports Exerc. 2019;51(6):1162–1168. doi:10.1249/MSS.0000000000001896
62. Cahuas A, He Z, Zhang Z, Chen W. Relationship of physical activity and sleep with depression in college students. J Am Coll Health. 2020;68(5):557–564. doi:10.1080/07448481.2019.1583653
63. Barham WT, Buysse DJ, Kline CE, Kubala AG, Brindle RC. Sleep health mediates the relationship between physical activity and depression symptoms. Sleep Breath. 2021;26(3):1–9.
64. Horwath U, Szczerbińska K. Determinants of late-life depression in residents of long-term care facility. Pol Merkur Lekarski. 2017;43(257):213–219.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.