Back to Journals » Nature and Science of Sleep » Volume 14
Actigraphy-Based Characteristics of Sleep in Paediatric Cancer Patients in Remission and a Comparison with Their Healthy Peers in the Recovery Stay
Authors Vyhlídal T, Dygrýn J ![]() , Chmelík F
, Chmelík F ![]()
Received 11 May 2022
Accepted for publication 12 August 2022
Published 25 August 2022 Volume 2022:14 Pages 1449—1456
DOI https://doi.org/10.2147/NSS.S374234
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Tomáš Vyhlídal, Jan Dygrýn, František Chmelík
Faculty of Physical Culture, Palacký University Olomouc, Olomouc, Czech Republic
Correspondence: Tomáš Vyhlídal, Email [email protected]
Background: Previous research has demonstrated that paediatric cancer survivors (PCS) have lower sleep quality than their healthy peers. However, the research to date has focused mainly on self-reported data. Therefore, the aim of this cross-sectional study was to characterise selected sleep parameters in PCS using objective monitoring techniques and to compare them with a control group (CG) of their healthy peers during a structured recovery stay. A specific objective was to characterise sleep with respect to gender, age, and cancer type.
Methods: 26 PCS and 38 CG aged 7– 15 years participated in the study. Selected sleep indicators (time in bed, total sleep time, sleep efficiency) were objectively assessed with an Actigraph wGT3X-BT accelerometer for 12 days during the recovery stay.
Results: No significant differences were found between the PCS and CG groups in terms of the selected sleep parameters. The total time in bed was 543.1 min/day in the PCS and 537.2 min/day in the CG (p=0.91). The total sleep time was 455.3 min/day in the PCS and 457.5 min/day in the CG (p=0.57). Sleep efficiency was 85.3% in the PCS and 86.3% in the CG (p=0.36). Sleep efficiency > 85% was achieved by 62% of the PCS (n=16) and 68% of the CG (n=26). There were no significant differences in sleep parameters in terms of variables such as gender, age, or cancer type.
Conclusion: The results of our study suggest that – under the same conditions – the PCS did not differ from their healthy peers in terms of the indicators of time in bed, total sleep time, and sleep efficiency. No significant differences according to age, gender, or cancer type were found.
Keywords: sleep, accelerometry, cancer survivors, children
Introduction
Sleep plays an essential role in the healthy development of children.1–3 The benefits of healthy sleep include, for instance, lower risk of cardiovascular disease, type 2 diabetes, and higher quality of life or enhanced cognitive functioning.2,4–7
Childhood cancer is associated with a wide range of potential adverse treatment consequences.8–10 The disease has a negative impact on the sleep patterns and sleep quality of the children who are treated.11–13 Reduced sleep quality is a significant negative factor affecting the quality of life in this target group even many years after diagnosis and treatment.14–18 Reduced sleep time, increased wakefulness during the night, and reduced sleep efficiency have been demonstrated for almost all types of cancer in childhood.11
Currently, we continue to encounter studies that focus on the subjective assessment of sleep, either by study participants themselves or their parents.18–24 This is despite it being known that objective assessment using an accelerometer provides more consistent and detailed information compared to self-reporting.25
Furthermore, the subjective sleep data provided by respondents and objective instrumental measurements show significant differences.26–28 In addition, published studies often analyse sleep data during the period of patient hospitalisation29–31 and we lack information on patient sleep in the post-treatment periods.
Thus, further studies using objective sleep monitoring are needed in order to understand sleep better in paediatric cancer survivors32,33 and focus on understanding risk factors, which may include gender, age, or cancer type.34
On the basis of these findings, the main aim of this study is to objectively characterise selected sleep parameters in children with cancer in remission and compare them with those of their healthy peers during an organised recovery stay. This stay is unique in terms of providing an environment and duration that are identical for both groups. A specific objective is to characterise sleep parameters in terms of gender, age, and cancer type.
Methods
Design and Participants
Paediatric cancer survivors PCS in remission and their healthy peers – control group (CG) participated in the study. Both groups were in the age range of 7–15 years.
For the PCS, the inclusion criterion of the study was completion of active oncological treatment at the Department of Paediatric Oncology at the University Hospital Brno; all participants had to be in remission ˂ five years after the end of the maintenance phase of treatment and had to have permanent residence in the Czech Republic. The exclusion criterion was a disability or health disadvantage unrelated to the treatment. Because of the large number of cancer types, we decided to divide the diseases into a) haematological malignancy and b) solid tumours. This division is in line with a number of other studies.35,36 We further split the participants by gender and by age. Age categories were divided into primary school age (7–11 years) and secondary school age age (12–15 years).
For the CG, the research inclusion criterion was defined as age 7–15 years and permanent residence in the Czech Republic. The exclusion criterion was having undergone active cancer treatment and another type of disability or health disadvantage.
Recruitment of Participants
The total numbers of participants approached to join the research study who met the criteria for PCS and CG were 32 and 44, respectively. For the PCS group, four participants were not interested in participating in the research survey. The data of two participants could not be evaluated because they did not wear the device for the minimum period. For the CG, six participants were not interested in participating in the research. Thus, in total, data was evaluated for 26 PCS and 38 CG. On the basis of the inclusion and exclusion criteria of the research study, the legal guardians of potential participants were approached by the main organiser of the recovery stay, the KRTEK Children’s Oncology Foundation. The legal guardians of the participants were addressed two weeks prior to the implementation of the research investigation.
Data Collection
The data collection took place between 19 and 30 August 2018 and lasted 12 days. The data was collected during a recovery stay organised by the KRTEK Children’s Oncology Foundation for PCS treated at the Department of Paediatric Oncology of the University Hospital Brno in the period from 18 August to 31 August 2018. These recovery stays are of an integrative nature and are attended by both PCS and their healthy peers (CG). The uniqueness of the data collection in the PCS and CG is mainly seen in the fact that the data collection took place during the recovery stay. As a result, both groups were able to follow the same daily routine (same wake-up time, same daily activities, same bedtime, same diet). Consent of the legal guardians was required for participation in the study. The study was approved by the Ethics Committee of the Faculty of Physical Culture of Palacký University in Olomouc under the reference number 48/2018.
Sleep Monitoring
An ActiGraph wGT3X-BT (ActiGraph, Pensacola, FL, USA) accelerometer was attached to the non-dominant wrist of the participants on the first day of the recovery stay. The participants were instructed to wear the device on their non-dominant wrist for 12 consecutive days, except for when swimming and bathing. The device was initialised to collect accelerations at 100 Hz using the Actilife software (ActiGraph, Pensacola, FL, USA). Next, the raw accelerometer data was processed using the R package GGIR (v2.1–0, https://cran.r-project.org/web/packages/GGIR/).34 We consider this length of monitoring to be unique, as objectively assessed sleep parameters often range from three to five days.29,30 The measuring device was distributed to the participants on the first day of the recovery stay. The Body Mass Index (BMI) was calculated by dividing the child’s weight (kg) by height (m) squared. The participants’ body weight and height were measured on the first day of the recovery stay using a TanitaTM calibrated digital scale (UM-075 type; Tanita Corporation, Tokyo, Japan) and the Leicester height measure.
Sleep Assessment
Indicators for assessing sleep duration and quality were determined as “Time in bed” (Difference between onset and waking time), “Total sleep time” (actual sleep time of the participant), and “Sleep efficiency” (calculated as: [Total sleep time/Time in bed]*100).37,38 The National Sleep Foundation’s sleep duration recommendation for healthy populations is set for the School-age group: 6–13 years 9 to 11 hours of sleep and for the Teenagers group: 14–17 years 8 to 10 hours.39 The “Sleep efficiency” indicator shows the ratio between the time spent in bed and the time for which a given participant actually sleeps. This indicator is the most commonly used measure to objectively assess sleep quality40 and can provide essential information about the health status of an individual.41 Sleep efficiency ≥ 85% is an indicator of good sleep quality.42
Statistical Analysis
The characteristics of the study sample are presented using descriptive statistics (median and interquartile range). To compare the study groups (age, gender, type of oncologic disease), the Mann–Whitney U-test was used. The level of statistical significance was set at α=0.05. The effect size coefficients were interpreted as follows: 0.2 ≤ d < 0.5 – small effect size, 0.5 ≤ d < 0.8 – medium effect size, and d ≥ 0.8 – large effect size.
Results
In Table 1 we present the basic descriptive characteristics of the PCS and CG research population. We found no significant differences between the study groups (PCS and CG) in either boys (age: p = 0.91, body height: p = 0.56, body weight: p = 0.31, BMI: p = 0.45) or girls (age: p = 0.74, body height: p = 0.91, body weight: p = 0.85, BMI: p = 0.87).
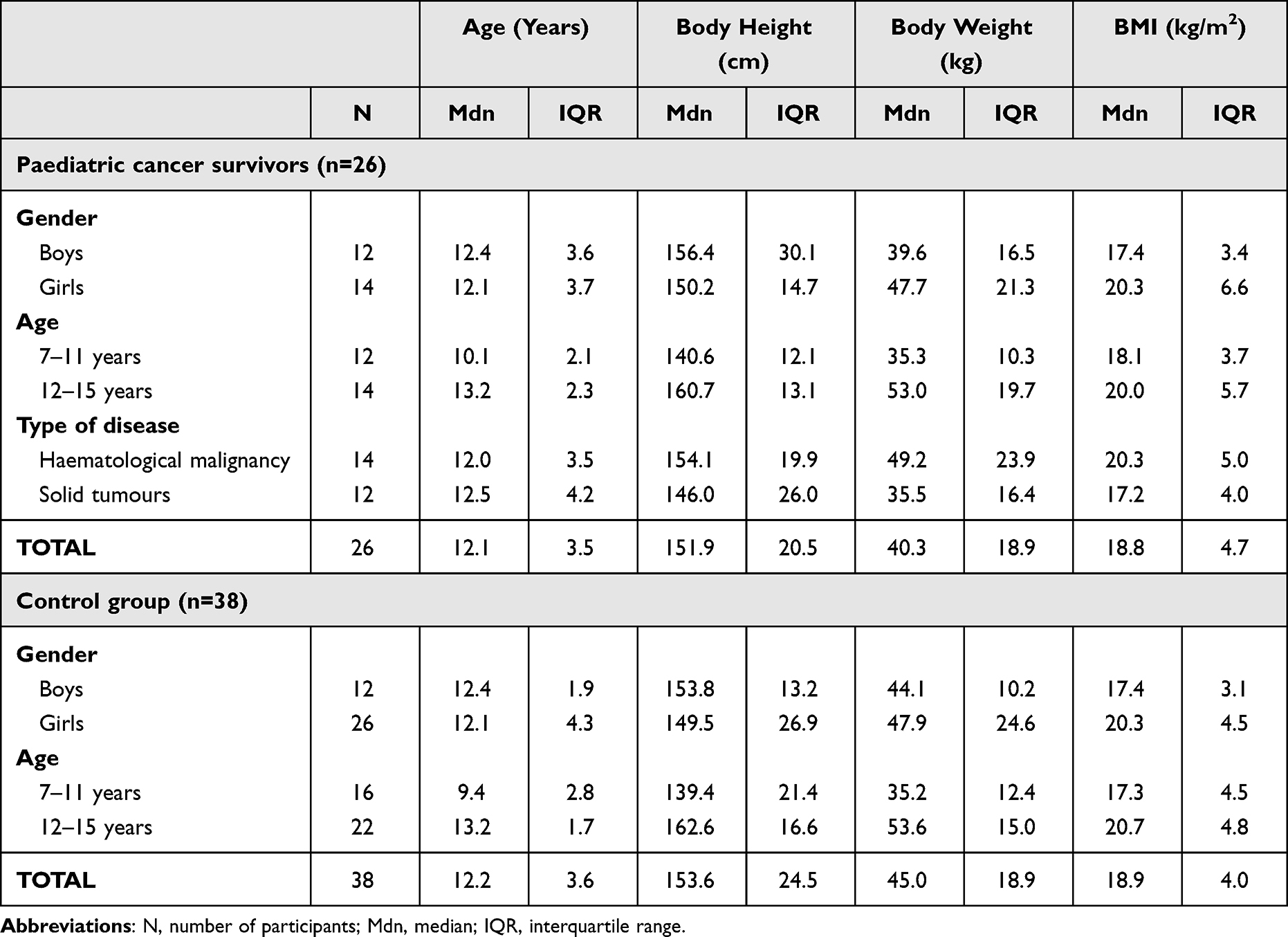 |
Table 1 Descriptive Characteristics of the Paediatric Cancer Survivors and Control Group |
The overview of selected actigraphy-based sleep characteristics of the PCS and CG are presented in Table 2. No significant differences were found between the groups (PCS, CG). The total time in bed was 543.1 min/day in the PCS (CG 537.2 min/day). The total sleep time in the PCS was 455.3 min/day (CG 457.5 min/day). Sleep efficiency in the PCS was 85.3% (CG 86.3%). Sleep efficiency >85% was achieved by 62% of the PCS and 68% of the CG.
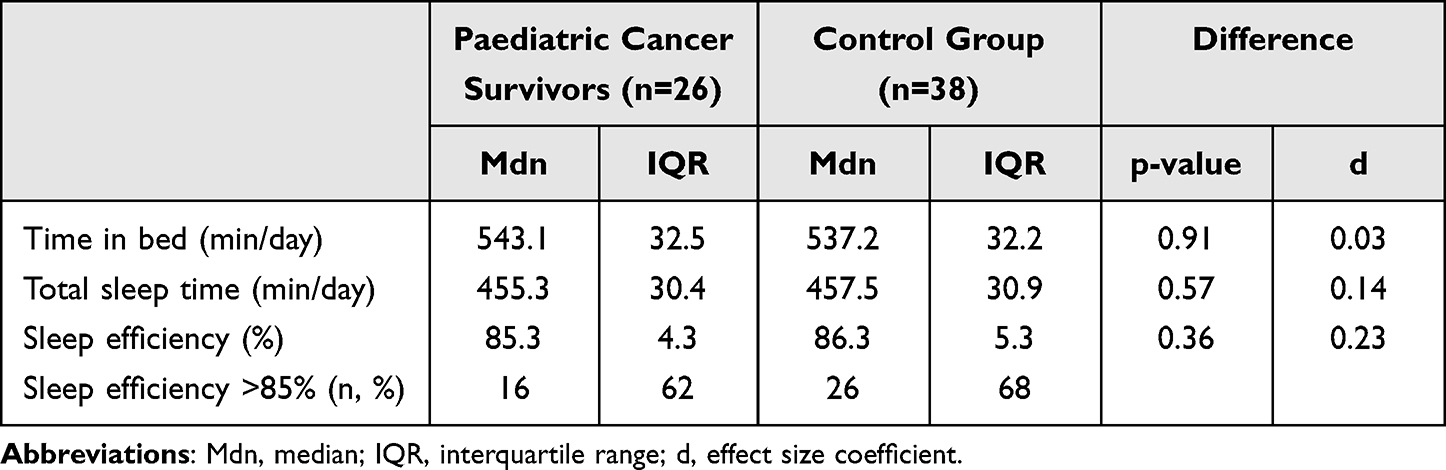 |
Table 2 Overview of Selected Sleep Parameters |
An overview of selected sleep parameters of the target and control groups according to age, sex, and type of cancer is presented in Table 3. There were no significant differences between the PCS and CG in terms of the individual parameters.
 |
Table 3 Overview of Selected Sleep Parameters by Gender, Age, and Type of Cancer |
Discussion
The main finding of this study was that the PCS and CG did not differ significantly in terms of the selected sleep parameters.
For comparison, we were unable to identify a study that objectively characterised selected sleep parameters in PCS and their healthy peers in a recovery stay setting that was the same for all participants. Objectively measured sleep indicators are most commonly found in the hospital setting during hospitalisation.29–31 Here, the measurements are often between two and five days. The study by Nunes et al31 for example, points out that the hospital environment and the period of hospitalisation are very specific and these sleep indicators cannot be generalised to other settings. The aforementioned study also supports other research investigations and points to the need to focus on other types of environments for this target group.
Similarly to our research, no significant differences in terms of gender, age, or cancer type were found in other studies either.31,43 Comparable objectively measured results were obtained in the study by Russell et al43 in survivors of acute lymphoblastic leukaemia and their healthy peers/siblings. Here again, no significant differences in selected sleep parameters between PCS and CG were confirmed. These results are also consistent with the previously published study by Greenfeld et al.44
The factor of age did not prove to be significant in our results, which is in line with the study by Kocevska et al28 who reported that gender differences in sleep parameters are only observable from adulthood onwards. Adult females spend a longer time in bed compared to males, but have lower sleep efficiency.
Compared to recommendations for a healthy paediatric population,39 we must mention that neither PCS nor CG achieve the established sleep recommendation for optimal support of their health.
Although a number of studies have pointed to impaired sleep quality in PCS, objective measurements of sleep parameters suggest that even after the completion of paediatric cancer treatment, these patients are able to match their healthy peers in remission. However, this finding needs to be confirmed by further studies and should be a standard part of treatment (not just an adjunct), as also pointed out by Merz and Tomfohr-Madsen.45
The main strength of this study is the objectively measured selected sleep parameters in a recovery stay setting in which the same conditions (daily routine, diet, accommodation) were set for both groups. Also, the length of the research investigation is unique compared to other available studies.
The smaller sample size of the PCS may be a limitation of the study. Another limitation was the use of the objective method of actigraphy, which, compared to polysomnography, does not allow the analysis of other sleep disorders (such as sleep breathing disorders, parasomnia or sleep movement disorders) that may affect sleep quality. It is also important to mention that actigraphy provides information about the presumed sleep based on the analysis of the patient’s movements, whereas only polysomnography indicates as objectively as possible that the patient is asleep and what the structure of his sleep is. Not using supplementary tools such as self-reported sleep diary or missing data on anxiety-depressive symptoms may also have posed a limitation to our findings.
Conclusions
The results of our study suggest that under the same conditions the PCS do not differ from their healthy peers in terms of time in bed, total sleep time, and sleep efficiency. No significant differences were found in terms of age, gender, or cancer type.
As sleep is one of the important pillars of a healthy lifestyle, by examining it, we can draw conclusions and recommendations that may lead to systematic support for the target group and to the mitigation or prevention of late effects of treatment.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Palacký University Olomouc (No. 48/2018).
Consent to Participate
Informed consent was obtained from legal guardians.
Funding
This study was funded by Internal grant of Palacký University Olomouc (IGA_FTK_2020_013).
Disclosure
The authors declare no competing interests.
References
1. Schlieber M, Han J. The role of sleep in young children’s development: a review. J Genet Psychol. 2021;182(4):205–217. doi:10.1080/00221325.2021.1908218
2. Paruthi S, Brooks LJ, D’Ambrosio C, et al. Consensus statement of the american academy of sleep medicine on the recommended amount of sleep for healthy children: methodology and discussion. J Clin Sleep Med. 2016;12(11):1549–1561. doi:10.5664/jcsm.6288
3. Bisogni S, Chiarini I, Giusti F, et al. Impact of hospitalization on the sleep patterns of newborns, infants and toddlers admitted to a pediatric ward: a cross-sectional study. Minerva Pediatr. 2015;67(3):209–217. PMID: 25297322.
4. Belmon LS, van Stralen MM, Busch V, Hamsen IA, Chinapaw MJM. What are the determinants of children’s sleep behavior? A systematic review of longitudinal studies. Sleep Med Rev. 2019;43:60–70. doi:10.1016/j.smrv.2018.09.007
5. Chaput J, Gray CE, Poitras VJ, et al. Sleep and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. 2016;41(June):S266–S282. doi:10.1139/apnm-2015-0627
6. Meltzer LJ, Williamson AA, Mindell JA. Pediatric sleep health: it matters, and so does how we define it. Sleep Med Rev. 2021;57:101425. doi:10.1016/j.smrv.2021.101425
7. Short MA, Blunden S, Rigney G, et al. Cognition and objectively measured sleep duration in children: a systematic review and meta-analysis. Sleep Heal. 2018;4(3):292–300. doi:10.1016/j.sleh.2018.02.004
8. Rueegg CS, Kriemler S, Zuercher SJ, et al. A partially supervised physical activity program for adult and adolescent survivors of childhood cancer (SURfit): study design of a randomized controlled trial [NCT02730767]. BMC Cancer. 2017;17(1). doi:10.1186/s12885-017-3801-8
9. Gendron É, Caru M, Léveillé P, et al. The effect of cardiorespiratory fitness and physical activity levels on cognitive functions in survivors of childhood acute lymphoblastic leukemia. Pediatr Hematol Oncol. 2020;37(7):582–598. doi:10.1080/08880018.2020.1767737
10. Kaushik P, Sharma S, Shah N, Kutty PK, Ghildiyal R. Sleep disturbances and childhood cancer- A tertiary care experience. Pediatr Hematol Oncol J. 2022;7(3):103–107. doi:10.1016/j.phoj.2022.05.001
11. Orsey AD, Wakefield DB, Cloutier MM. Physical activity (PA) and sleep among children and adolescents with cancer. Pediatr Blood Cancer. 2013;60(11):1908–1913. doi:10.1002/pbc.24641
12. Stavinoha PL, Olsthoorn IM, Swartz MC, et al. Non-pharmacological sleep interventions for pediatric cancer patients and survivors: a systematic review protocol. Syst Rev. 2021;10(1):1–7. doi:10.1186/s13643-021-01724-3
13. Oswald KA, Richard A, Hodges E, Heinrich KP. Sleep and neurobehavioral functioning in survivors of pediatric cancer. Sleep Med. 2021;78:153–159. doi:10.1016/j.sleep.2020.12.026
14. Walter LM, Nixon GM, Davey MJ, Downie PA, Horne RSC. Sleep and fatigue in pediatric oncology: a review of the literature. Sleep Med Rev. 2015;24:71–82. doi:10.1016/j.smrv.2015.01.001
15. Steur LMH, Kolk RHE, Mooij F, et al. The prevalence and risk factors of sleep problems in pediatric oncology: its effect on quality of life during and after cancer treatment. Expert Rev Qual Life Cancer Care. 2016;1(2):153–171. doi:10.1080/23809000.2016.1168265
16. Zhou ES, Recklitis CJ. Insomnia in adult survivors of childhood cancer: a report from project REACH. Support Care Cancer. 2014;22(11):3061–3069. doi:10.1007/s00520-014-2316-y
17. Daniel L, Kazak AE, Li Y, et al. Relationship between sleep problems and psychological outcomes in adolescent and young adult cancer survivors and controls. Support Care Cancer. 2016;24(2):539–546. doi:10.1007/s00520-015-2798-2
18. Sheikh IN, Roth M, Stavinoha PL. Prevalence of sleep disturbances in pediatric cancer patients and their diagnosis and management. Children. 2021;8(12):1100. doi:10.3390/children8121100
19. Daniel LC, Aggarwal R, Schwartz LA. Sleep in adolescents and young adults in the year after cancer treatment. J Adolesc Young Adult Oncol. 2017;6(4):560–567. doi:10.1089/jayao.2017.0006
20. Daniel LC, Meltzer LJ, Gross JY, Flannery JL, Forrest CB, Barakat LP. Sleep practices in pediatric cancer patients: indirect effects on sleep disturbances and symptom burden. Psychooncology. 2021;30(6):910–918. doi:10.1002/pon.5669
21. Momayyezi M, Fallahzadeh H, Farzaneh FF, Momayyezi M. Sleep quality and disturbances in children and adolescents with cancers: a cross-sectional study. Int J Pediatr. 2018;6(4):7529–7542. doi:10.22038/ijp.2018.28729.2509
22. Kim H, Zhou ES, Chevalier L, et al. Parental behaviors, emotions at bedtime, and sleep disturbances in children with cancer. J Pediatr Psychol. 2020;45(5):550–560. doi:10.1093/jpepsy/jsaa018
23. Ince D, Demirağ B, Karapınar TH, et al. Assessment of sleep in pediatric cancer patients. Turk J Pediatr. 2017;59(4):379–386. doi:10.24953/turkjped.2017.04.003
24. Soheilipour F, Faranoush M, Jolfaei AG, Tafreshi RI, Kashaninasab F. Evaluating sleep habits and related factors in childhood cancer survivors: a cross‐sectional study. Iran J Pediatr Hematol Oncol. 2022;12(2):122–133. doi:10.18502/ijpho.v12i2.9077
25. Smith MT, McCrae CS, Cheung J, et al. Erratum: use of actigraphy for the evaluation of sleep disorders and circadian rhythm sleep-wake disorders: an American Academy of Sleep Medicine systematic review, meta-analysis, and GRADE assessment (Journal of Clinical Sleep Medicine (2019)14:7(1209–123). J Clin Sleep Med. 2019;15(3):531. doi:10.5664/jcsm.7702
26. Tremaine RB, Dorrian J, Blunden S. Subjective and objective sleep in children and adolescents: measurement, age, and gender differences. Sleep Biol Rhythms. 2010;8(4):229–238. doi:10.1111/j.1479-8425.2010.00452.x
27. Lubas MM, Szklo-Coxe M, Mandrell BN, et al. Concordance between self-reported sleep and actigraphy-assessed sleep in adult survivors of childhood cancer: the impact of psychological and neurocognitive late effects. Support Care Cancer. 2022;30(2):1159–1168. doi:10.1007/s00520-021-06498-x
28. Kocevska D, Lysen TS, Dotinga A, et al. Sleep characteristics across the lifespan in 1.1 million people from the Netherlands, United Kingdom and United States: a systematic review and meta-analysis. Nat Hum Behav. 2021;5(1):113–122. doi:10.1038/s41562-020-00965-x
29. Hinds PS, Hockenberry M, Rai SN, et al. Nocturnal awakenings, sleep environment interruptions, and fatigue in hospitalized children with cancer. Oncol Nurs Forum. 2007;34(2):397–402. doi:10.1188/07.ONF.393-402
30. Linder LA, Christian BJ. Nighttime sleep disruptions, the hospital care environment, and symptoms in elementary school-age children with cancer. Oncol Nurs Forum. 2012;39:553–561. doi:10.1188/12.ONF.553-561
31. Nunes MDR, Nascimento LC, Fernandes AM, et al. Pain, sleep patterns and health-related quality of life in paediatric patients with cancer. Eur J Cancer Care (Engl). 2019;28(4):1–10. doi:10.1111/ecc.13029
32. Matricciani L, Paquet C, Galland B, Short M, Olds T. Children’s sleep and health: a meta-review. Sleep Med Rev. 2019;46:136–150. doi:10.1016/j.smrv.2019.04.011
33. Ha L, Mizrahi D, Wakefield CE, Cohn RJ, Simar D, Signorelli C. The use of activity trackers in interventions for childhood cancer patients and survivors: a systematic review. J Adolesc Young Adult Oncol. 2021;10(1):1–14. doi:10.1089/jayao.2020.0099
34. Daniel LC, van Litsenburg RRL, Rogers VE, et al. A call to action for expanded sleep research in pediatric oncology: a position paper on behalf of the International Psycho-Oncology Society Pediatrics Special Interest Group. Psychooncology. 2020;29(3):465–474. doi:10.1002/pon.5242
35. Rehorst-Kleinlugtenbelt LB, Bekkering WP, van der Torre P, van der Net J, Takken T. Physical activity level objectively measured by accelerometery in children undergoing cancer treatment at home and in a hospital setting: a pilot study. Pediatr Hematol Oncol J. 2019;4(4):82–88. doi:10.1016/j.phoj.2019.12.004
36. Koçak Ü, Rolston KVI, Mullen CA. Fever and neutropenia in children with solid tumors is similar in severity and outcome to that in children with leukemia. Support Care Cancer. 2002;10(1):58–64. doi:10.1007/s005200100277
37. Migueles JH, Rowlands AV, Huber F, Sabia S, van Hees VT. GGIR: a research community–driven open source R package for generating physical activity and sleep outcomes from multi-day raw accelerometer data. J Meas Phys Behav. 2019;2(3):188–196. doi:10.1123/jmpb.2018-0063
38. Shrivastava D, Jung S, Saadat M, Sirohi R, Crewson K. How to interpret the results of a sleep study. J Community Hosp Intern Med Perspect. 2014;4(5):24983. doi:10.3402/jchimp.v4.24983
39. Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s updated sleep duration recommendations: final report. Sleep Heal. 2015;1(4):233–243. doi:10.1016/j.sleh.2015.10.004
40. Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. J Clin Sleep Med. 2012;8(5):597–619. doi:10.5664/jcsm.2172
41. Jung DW, Lee YJ, Jeong DU, Park KS. New predictors of sleep efficiency. Chronobiol Int. 2017;34(1):93–104. doi:10.1080/07420528.2016.1241802
42. Ohayon M, Wickwire EM, Hirshkowitz M, et al. National Sleep Foundation’s sleep quality recommendations: first report. Sleep Heal. 2017;3(1):6–19. doi:10.1016/j.sleh.2016.11.006
43. Russell KB, Merz EL, Reynolds K, Schulte F, Tomfohr-Madsen L. Sleep disturbances in survivors of pediatric acute lymphoblastic leukemia and their siblings. J Pediatr Psychol. 2020;45(7):707–716. doi:10.1093/jpepsy/jsaa043
44. Greenfeld M, Constantini S, Tauman R, Sivan Y. Sleep disturbances in children recovered from central nervous system neoplasms. J Pediatr. 2011;159(2):268–272.e1. doi:10.1016/j.jpeds.2011.01.030
45. Merz EL, Tomfohr-Madsen L. Sleep disruption in pediatric cancer survivors: conceptual framework and opportunities for clinical assessment and behavioral treatment. Am J Lifestyle Med. 2018;12(4):311–323. doi:10.1177/1559827616681725
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.