Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Acquired Reactive Perforating Collagenosis Treated with Upadacitinib: A Case Report and Literature Review
Authors Xie B ![]() , Zhang X, Lei X, Zhang Y, Zhang Q, Ye Y
, Zhang X, Lei X, Zhang Y, Zhang Q, Ye Y
Received 2 October 2025
Accepted for publication 25 December 2025
Published 7 January 2026 Volume 2026:19 569903
DOI https://doi.org/10.2147/CCID.S569903
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Bo Xie,* Xiaoyan Zhang,* Xinxin Lei,* Yuting Zhang, Qin Zhang, Yujian Ye
Department of Dermatology, Hangzhou Third People’s Hospital, Hangzhou Third Hospital Affiliated to Zhejiang Chinese Medical University, Hangzhou, 310009, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yujian Ye, Department of Dermatology, Hangzhou Third People’s Hospital, Hangzhou Third Hospital Affiliated to Zhejiang Chinese Medical University, Westlake Road 38, Hangzhou, 310009, People’s Republic of China, Email [email protected]
Abstract: Acquired reactive perforating collagenosis (ARPC) is a rare perforating dermatosis linked to systemic diseases, with unclear pathogenesis and no standardized therapy. We report a 53-year-old male with ARPC who failed conventional treatments but improved rapidly with upadacitinib 15 mg/day for one month, followed by 15 mg every other day. After three months, most lesions resolved, leaving hyperpigmentation and scars. Literature review shows conflicting reports: one case of ARPC improved with upadacitinib, another developed ARPC during upadacitinib treatment for atopic dermatitis. Our findings suggest upadacitinib may be effective for ARPC, especially in pruritic patients, regardless of diabetes status.
Keywords: Janus kinase inhibitor, reactive perforating collagenosis, upadacitinib
Introduction
Acquired reactive perforating collagenosis (ARPC) is a rare subtype of perforating dermatosis characterized by the transepidermal elimination of altered collagen, typically manifesting as umbilicated, hyperkeratotic papules and nodules accompanied by intense pruritus.1 The condition is frequently associated with underlying systemic diseases, including diabetes mellitus, chronic renal failure, thyroid disorders, hepatic dysfunction, malignant neoplasms, and infectious diseases, which are believed to contribute to aberrant collagen metabolism and a compromised cutaneous response to superficial trauma such as scratching.1 The pathogenesis of ARPC remains incompletely elucidated, and no standardized therapeutic guidelines exist. Current management often involves a stepwise approach, beginning with topical corticosteroids and antihistamines, and escalating to phototherapy (eg, ultraviolet B), systemic agents (eg, retinoids, allopurinol, doxycycline), or immunosuppressants (eg, cyclosporine) in refractory cases, albeit with variable and often unsatisfactory efficacy.2
Recently, insights into the role of inflammatory cytokines, particularly T-helper 2 (Th2)-associated pathways involving IL-4, IL-13, and IL-31, have prompted the successful use of dupilumab in some ARPC cases.3,4 Concurrently, the Janus kinase (JAK) inhibitors, such as tofacitinib and baricitinib, have emerged as promising therapeutic options due to their broad anti-inflammatory and antipruritic effects.5,6 Upadacitinib, a selective JAK1 inhibitor, represents a more targeted agent within this class and is approved for several inflammatory conditions, including atopic dermatitis. Its potential application in ARPC, however, remains scarcely explored and is supported by only a single prior case report demonstrating efficacy.7 Intriguingly, a contrasting report describes the development of ARPC in a patient treated with upadacitinib for atopic dermatitis (AD), highlighting the complexity of its role in this disease.8 This duality underscores the need for further evidence to clarify the therapeutic position of upadacitinib relative to other emerging biologic and small-molecule therapies in ARPC.
Herein, we present a case of a 53-year-old male with ARPC who achieved significant clinical improvement with upadacitinib, and we review the pertinent literature to discuss its potential place in the current treatment landscape.
Case Report
A 53-year-old male presented with scattered pruritic papules and nodules on his extremities, which had persisted for 4 months. Prior to visiting our institution, he had received oral antihistamines, thalidomide, and topical mometasone furoate for 3 months, with no significant improvement in symptoms. One month before admission, the cutaneous lesions gradually increased in number, and pruritus exacerbated. The patient denied a history of major systemic diseases or long-term oral medication use.
Physical examination revealed scattered 3–8 mm red papules and nodules on the extensor surfaces of the extremities, distributed diffusely without fusion. The lesions were firm on palpation, with umbilicated depressions and keratotic plugs observed at the top of some papules (Figure 1A). The photographs at 1 month and 3 months post-treatment are depicted in Figure 1B and C, respectively. Hematoxylin & Eosin staining (Figure 2A) and Van Gieson staining (Figure 2B) demonstrated degenerated eosinophilic collagen bundles in the upper dermis penetrating the epidermis—consistent with a “perforating phenomenon”—accompanied by perilesional infiltration of lymphocytes and histiocytes. Based on the typical clinical manifestations and histopathological features, a diagnosis of ARPC was confirmed.
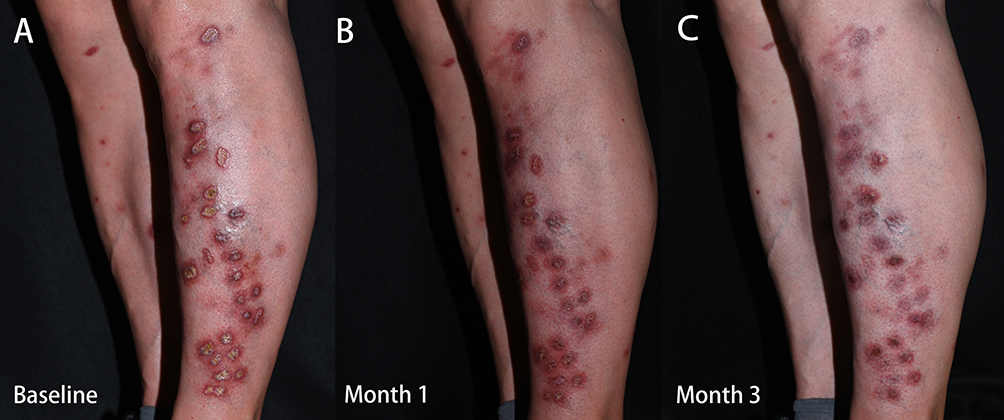 |
Figure 1 Clinical Photograph of ARPC. (A) Erythematous papules and nodules on both lower extremities at baseline, with umbilicated depressions and keratotic plugs observed on the top of some papules. (B) 1 months after upadacitinib administration. (C) 3 months after upadacitinib administration. Abbreviation: ARPC, acquired reactive perforating collagenosis. |
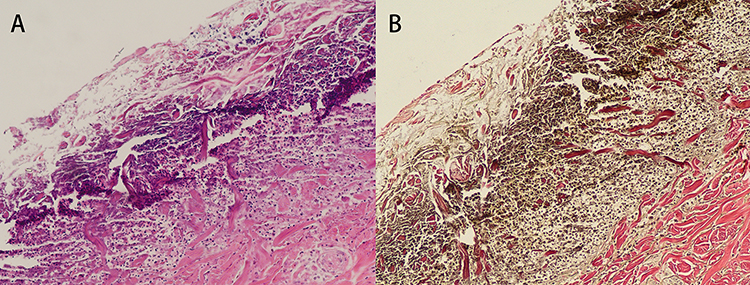 |
Figure 2 Pathological Examination. (A) Hematoxylin & Eosin staining. (B) Van Gieson staining. Pathological examination exhibited the entire process of scattered red collagen fibers migrating from the dermis to the epidermis. |
The patient was initiated on upadacitinib 15 mg once daily, with no other concurrent medications. After 1 month of treatment, pruritus resolved rapidly, and the nodules gradually flattened (Figure 1B). The dose of upadacitinib was then reduced to 15 mg every other day for maintenance. By the 3-month follow-up, most umbilicated central lesions had resolved, leaving only post-inflammatory hyperpigmentation and focal scars (Figure 1C).
Discussion
Pathologically, ARPC is characterized by the trans-epidermal extrusion of collagen fibers. Clinically, it typically presents as umbilicated hyperkeratotic papules, often accompanied by intractable pruritus. In our patient, the initial presentation consisted of firm, erythematous, 3–8 mm papules and nodules with central keratotic plugs and classic umbilication, distributed symmetrically on the extensor surfaces of the limbs. The pruritus was severe and refractory to conventional antipruritics. While the etiology and pathogenesis of ARPC remain incompletely elucidated, accumulating evidence links it to abnormal cutaneous wound repair and dysregulated collagen metabolism. Additionally, ARPC frequently occurs as a secondary phenomenon in patients with systemic diseases, such as diabetes mellitus and chronic renal failure.3 To date, no specific treatment is indicated for ARPC. The significant pitfall of current therapies (including ultraviolet B phototherapy, antihistamines, and systemic agents like allopurinol or retinoids) is their unpredictable and often modest efficacy, particularly against the debilitating pruritus. This therapeutic void underscores the critical need to explore targeted, pathogenesis-oriented treatments for refractory cases.2
It is currently believed that ARPC is a response to trauma. Pruritus-induced scratching or friction may disrupt normal collagen metabolism—a mechanism that also explains the association between ARPC and systemic diseases (particularly diabetes mellitus and chronic kidney disease).1 Inflammatory factor dysregulation is another key feature of ARPC, involving abnormal expression of transforming growth factor-β, extracellular matrix proteins,9 receptors for advanced glycation end products,10 and IL-31.4 In recent years, studies have further implicated T helper 2 (Th2)-associated cytokines (eg, IL-4 and IL-13) in ARPC pathogenesis, leading to the successful use of dupilumab (a monoclonal antibody targeting IL-4/IL-13 receptors) in ARPC treatment.3
Moreover, the JAK inhibitors tofacitinib5 and baricitinib6 have also demonstrated efficacy in ARPC, likely attributed to their broad anti-inflammatory and antipruritic properties. Upadacitinib is a selective JAK1 inhibitor that has been approved by the US Food and Drug Administration for the treatment of rheumatoid arthritis, psoriatic arthritis, AD, etc.11 Theoretically, its safety profile is linked to its JAK1 selectivity, which may offer a better benefit-risk ratio compared to broader JAK inhibitors; however, class-related risks including serious infections, herpes zoster reactivation, laboratory abnormalities (eg, neutropenia, lipid elevation), and other adverse events necessitate pre-treatment screening and ongoing monitoring.12 However, its application in ARPC remains rarely reported. Prior to our case, only Ding et al7 described a case of ARPC treated with upadacitinib. In contrast, Morrison et al8 reported the development of ARPC in a patient receiving upadacitinib for AD—raising questions about the consistency of upadacitinib’s effects in ARPC.
A detailed comparison of these cases reveals critical nuances. Ding et al7 treated a 63-year-old male with ARPC secondary to diabetes mellitus with upadacitinib 15 mg daily for 3 months, followed by 15 mg every other day for maintenance; significant improvements in pruritus and cutaneous lesions were observed. In our case, the patient received upadacitinib 15 mg daily for only 1 month, followed by 15 mg every other day, and still achieved favorable outcomes by the 3-month follow-up (Figure 1C). The therapeutic response in our patient was notably rapid. Pruritus subsided within the first week of treatment. By the 1-month follow-up, the nodules had significantly flattened, and the keratotic plugs had been shed. The resolution progressed to near-complete clearance by 3 months, leaving only post-inflammatory hyperpigmentation and superficial scars. A key distinction between the two cases is that our patient had no underlying systemic diseases (eg, diabetes mellitus or chronic kidney disease), which may have enabled earlier dose reduction without compromising efficacy, suggesting that the absence of systemic metabolic comorbidity might predict a more favorable treatment response.
Notably, Morrison et al8 reported a case of a 37-year-old male patient who developed ARPC after 8 weeks of upadacitinib treatment for AD, and the ARPC gradually resolved 2–3 weeks after drug discontinuation. This AD patient showed no response to either dupilumab or upadacitinib, whereas cyclosporine treatment yielded therapeutic effects. This paradoxical case highlights the complex, dual role JAK-STAT signaling may play in different inflammatory skin contexts. It suggests that in certain individuals, inhibiting specific immune pathways might inadvertently disrupt skin immune homeostasis in a way that predisposes to or unmasks ARPC. This finding may suggest that Th2-type inflammation might play a minor role in the pathogenesis of AD in this patient, and it may also indirectly imply that pruritus and Th2-type inflammation could be associated with the therapeutic efficacy in ARPC. Therefore, the efficacy of upadacitinib may depend on the dominant inflammatory drivers in a given patient’s ARPC, explaining its therapeutic success in some and its potential to induce the condition in others.
Conclusion
Our case, combined with the existing literature, confirms that upadacitinib is a viable therapeutic option for ARPC—particularly in patients with prominent pruritus, regardless of the presence or absence of underlying diabetes mellitus. Further large-scale studies are needed to validate its efficacy and safety in ARPC and to clarify the mechanisms underlying its variable effects.
Abbreviations
ARPC, acquired reactive perforating collagenosis; AD, atopic dermatitis; Th2, T helper 2; JAK, Janus kinase.
Ethics and Consent Statement
The written informed consent was obtained from the patient for the publication of the case details and images. This case report was conducted in accordance with the Declaration of Helsinki (as revised in 2013, Fortaleza, Brazil) and approved by the Ethics Committee of Hangzhou Third People’s Hospital (Approval No. 2025KA277).
Funding
This work was supported by National Natural Science Foundation of China (82303998).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu J, Zhao P, Zhang X, et al. Acquired reactive perforating collagenosis triggered by trauma with eosinophilia: a case report and literature review. Front Med Lausanne. 2024;11:1415545. doi:10.3389/fmed.2024.1415545
2. Karpouzis A, Giatromanolaki A, Sivridis E, et al. Acquired reactive perforating collagenosis: current status. J Dermatol. 2010;37(7):585–5. doi:10.1111/j.1346-8138.2010.00918.x
3. Liu B, Wu Y, Wu X, et al. Dupilumab improve acquired reactive perforating collagenosis characterized by type 2 inflammation. Front Immunol. 2023;14:1240262. doi:10.3389/fimmu.2023.1240262
4. Oikawa A, Muramatsu K, Watanabe K, et al. Successful nemolizumab treatment of refractory acquired reactive perforating collagenosis in a diabetic patient. Cureus. 2025;17(7):e88884. doi:10.7759/cureus.88884
5. Yuan R, Zhou G, Liu H. Tofacitinib for treatment of acquired reactive perforating collagenosis. JAMA Dermatol. 2025;161(4):446. doi:10.1001/jamadermatol.2024.6280
6. Zheng J, Ding Y, Chen Y, et al. Effectiveness of baricitinib in acquired reactive perforating collagenosis: a case report. Front Immunol. 2024;15:1388274. doi:10.3389/fimmu.2024.1388274
7. Ding W, Wang Y, Song L, et al. A potential new treatment with upadacitinib for acquired reactive perforating collagenosis. JAAD Case Rep. 2024;48:112–114. doi:10.1016/j.jdcr.2024.04.017
8. Morrison E, Low SE, Ngan K. A unique case of reactive perforating collagenosis secondary to upadacitinib treatment of severe atopic eczema. Clin Exp Dermatol. 2025;50(7):1452–1453. doi:10.1093/ced/llaf122
9. Gambichler T, Birkner L, Stücker M, et al. Up-regulation of transforming growth factor-beta3 and extracellular matrix proteins in acquired reactive perforating collagenosis. J Am Acad Dermatol. 2009;60(3):463–469. doi:10.1016/j.jaad.2008.06.006
10. Akoglu G, Sungu N, Karaismailoglu E, et al. Expression of the receptor for advanced glycation end products in acquired reactive perforating collagenosis. Indian J Dermatol Venereol Leprol. 2017;83(4):432–435. doi:10.4103/ijdvl.IJDVL_113_16
11. Roskoski R. Properties of FDA-approved small molecule protein kinase inhibitors: a 2024 update. Pharmacol Res. 2025;217:107804. doi:10.1016/j.phrs.2025.107804
12. Schwartz DM, Kanno Y, Villarino A, et al. JAK inhibition as a therapeutic strategy for immune and inflammatory diseases. Nat Rev Drug Discov. 2017;16(12):843–862. doi:10.1038/nrd.2017.201
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Upadacitinib Therapy in Adolescent Severe Alopecia Areata: A Case Series and Narrative Review
Gao Y, Zhu C, Jin H
Clinical, Cosmetic and Investigational Dermatology 2025, 18:2141-2148
Published Date: 3 September 2025
A Real-World Study of Upadacitinib in Anti-TNF Refractory Crohn’s Disease: Effectiveness, Persistence, and Safety
Fang Y, Zhou L, Li L, Zhang L, Zhu N, Hu J, Liu Q, Wu J, Zhang P, Mei Q, Han W
Journal of Inflammation Research 2026, 19:591249
Published Date: 5 May 2026
A Successful Outcome of Upadacitinib Therapy in a Patient with Genital Erosive Fixed Drug Eruption: A Case Report
Li C, Wang X, Li X, Xu M, Kong S, Tao X, Liu W, Wan H
Clinical, Cosmetic and Investigational Dermatology 2026, 19:615233
Published Date: 17 June 2026