")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Acquired Digital Fibrokeratoma: A Report of Five Cases and Review of the Literature
Authors Wang X, Zhang D , Lin Q , Niu C, Fan H, Zhang M, Yuan X, Ma W
Received 15 November 2023
Accepted for publication 22 January 2024
Published 30 January 2024 Volume 2024:17 Pages 247—252
DOI https://doi.org/10.2147/CCID.S447798
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Xing Wang,* Dong Zhang,* Qingxia Lin, Changying Niu, Huiping Fan, Mogen Zhang, Xiangfeng Yuan, Weiyuan Ma
Department of Dermatology, Affiliated Hospital of Weifang Medical University, Weifang, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiangfeng Yuan; Weiyuan Ma, Department of Dermatology, Affiliated Hospital of Weifang Medical University, Weifang, People’s Republic of China, Tel +86-536-3081272, Email [email protected]; [email protected]
Abstract: Acquired digital fibrokeratoma (ADF) is rare in clinical practice and is easily misdiagnosed. Herein, 5 cases of patients (3 males and 2 females) with ADF are reported. The mean age at onset was 42.6 years, and the mean disease duration was 3 years. Four patients had ADF on the hands, and 1 patient had ADF on the foot. The clinical manifestations were all solitary, skin-colored papules, with a firm texture and smooth surface, protruding from the skin surface. In 3 patients, ADF manifested as columnar protrusions, and in 2 patients, ADF manifested as dome-shaped protrusions. For all 5 patients, the diameters of the lesions were < 1 cm. Clinically, all 5 patients were misdiagnosed (ie, eccrine poroma (EP), common warts, rudimentary polydactyly, pyogenic granuloma (PG), and acral fibroma). All cases of ADF were confirmed by histopathology. The histopathological manifestations of ADF were as follows: finger-like protrusions on the skin surface; collagen fiber bundles running vertically to the epidermis seen in the dermis; and thick red-stained collagen fibers connected with the normal dermal connective tissue below. All 5 patients underwent surgical resection; the distance between the incision margin and the edge of the tumor was 2– 3 mm, and the surgical depth was the deep dermis. No recurrence was observed in more than half a year of follow-up after surgery.
Keywords: acquired digital fibrokeratoma, clinical manifestation, histopathology, surgical resection
Introduction
Acquired digital fibrokeratoma (ADF) is a rare benign tumor of fibrous tissue,1 and the cause is still unclear. The clinical manifestation of ADF is a single hemispherical or columnar nodule with a hard texture protruding from the skin surface, and histopathology manifestations include thickened and interwoven collagen fiber bundles running vertically with the epidermis seen in the dermis. ADF is rare in clinical practice and is easily misdiagnosed. To increase dermatologists’ understanding of ADF, herein, the clinical manifestations and histopathology of 5 patients with ADF are presented, and the diagnosis, differential diagnosis, and treatment methods are discussed through a literature review (Table 1).
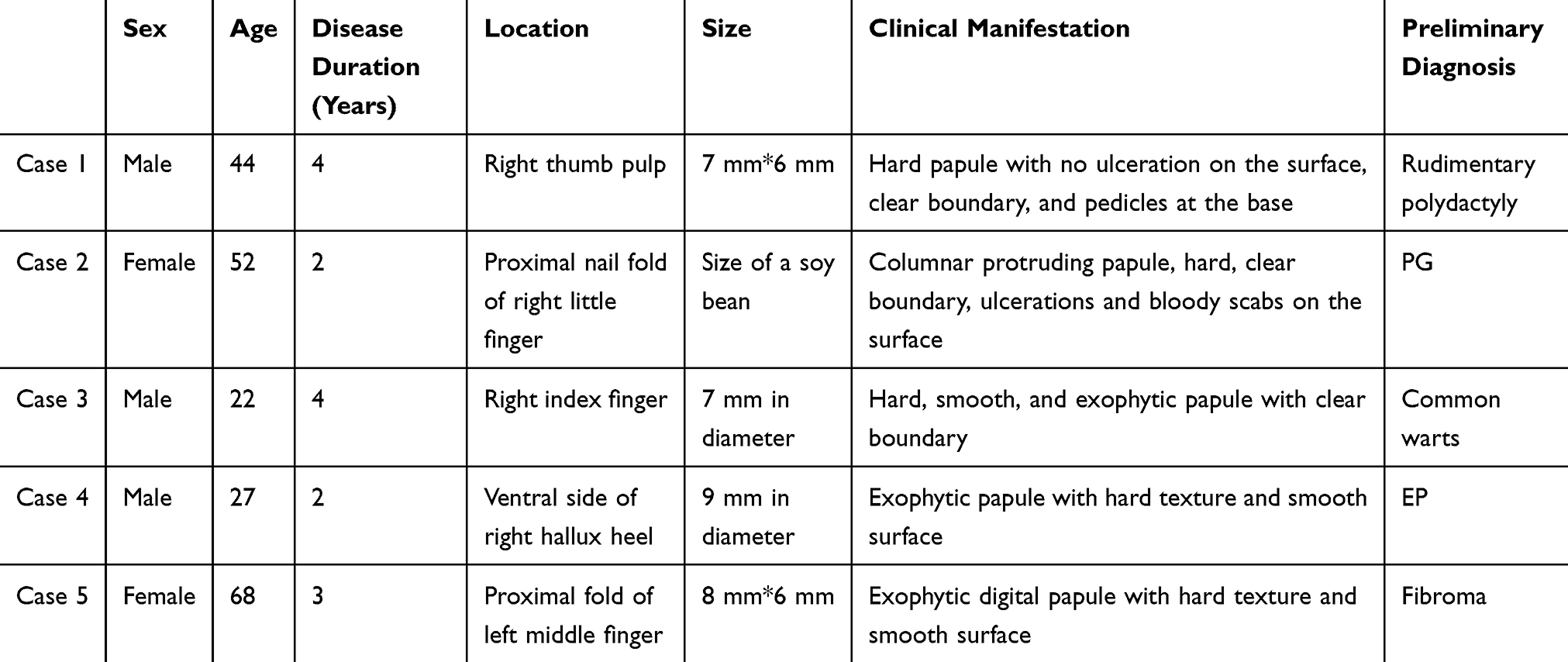 |
Table 1 Clinical Information of the Five ADF Patients |
Case Presentation
Case 1
A 44-year-old man had a light red papule develop on the pulp of his right thumb 4 years prior, and he had no subjective symptoms. Over the past four years, the papule gradually increased to 7 mm*6 mm, with a firm texture, clear boundary, smooth surface, contracted base, and a collar-shaped bulge at the periphery (Figure 1a). No similar skin lesions were found in other parts of the patient’s body, and a systemic examination was normal. The patient was previously healthy and had no family history. He denied any history of local trauma.
 |
Figure 1 Clinical ADF manifestations (five patients in a, b, c, d, and e). |
The preliminary clinical diagnosis was rudimentary polydactyly. During surgery, the skin was incised 3 mm from the edge of the tumor to the deep dermis, and the tumor was completely removed. The histopathological manifestations were as follows: under a low-magnification microscope, the tumor had finger-like protrusions; under a high-magnification microscope, the epidermis was thickened, fibroblasts in the dermis were thickened, and collagen fiber bundles were thickened and stained red, running roughly perpendicular to the epidermis. Minor inflammatory cell infiltration was observed between the proliferative fiber bundles, with dilated and hyperplastic capillaries (Figures 2a and b). The final diagnosis was ADF, and no recurrence was observed in the 10-month follow-up after surgery.
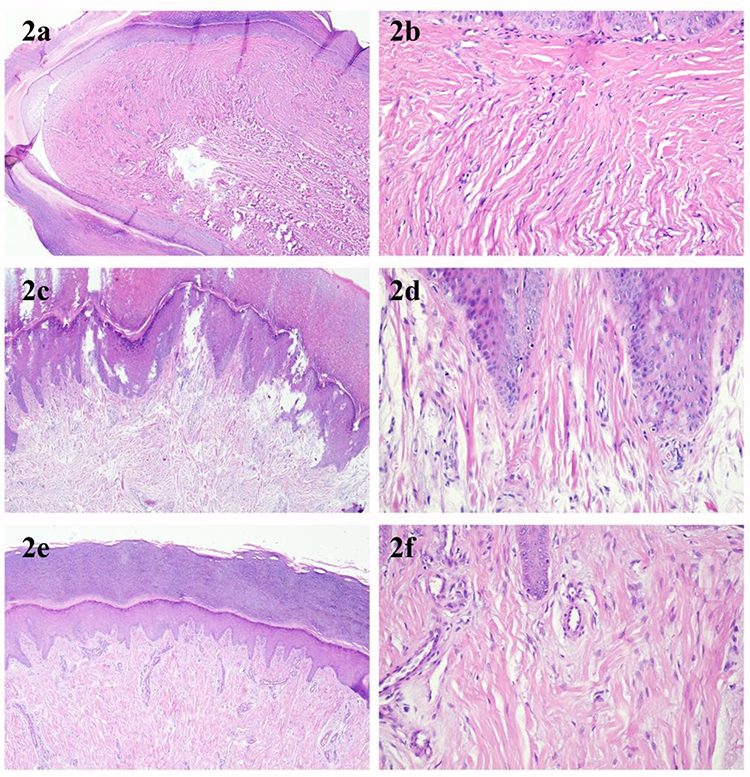 |
Figure 2 Histopathological manifestations of ADF (a) Case 1, with digital papules visible (40x); (b) Case 1, thickened and red-stained collagen bundles arranged perpendicular to the epidermis and increased capillaries (200x); (c) Case 2, obvious hyperkeratosis and epidermal thickening (40x); (d) Case 2, collagen fiber bundles arranged perpendicular to the epidermis seen in the dermis, with obvious thickening and red staining (200x); (e) Case 3, tumor was flat and dome-shaped (40x); (f) Case 3, fewer fibroblasts in the dermis and hyperplastic collagen arranged perpendicular to the skin surface (200x). |
Case 2
A 52-year-old female had a single skin-colored papule, the size of a miliary grain, develop on the proximal nail fold of the little finger of her right hand 2 years prior, and she did not have subjective symptoms. Over the past 2 years, the tumor slowly increased to the size of a soybean grain and became a columnar protrusion, with a firm texture, clear boundary, and ulceration and bloody scabs on the surface (Figure 1b). No similar skin lesions were found in other parts of the body, and a systemic examination was normal. The patient was previously healthy and had no family history. She denied any history of trauma before the onset of illness. The preliminary clinical diagnosis was pyogenic granuloma (PG). The tumor was completely removed, with a 3-mm margin around the tumor, and then sent for a histopathological examination. The histopathological manifestations were similar to those in Case 1 (Figures 2c and d). The final diagnosis was ADF, and no recurrence was observed in the 1-year follow-up after surgery.
Case 3
A 22-year-old male patient had a skin-colored papule, the size of a miliary grain, appear on the distal knuckle of his right index finger 4 years prior, but there was no pain or itching. Over 4 years, the papule gradually increased to 7 mm in diameter, with a firm texture, clear boundary, and smooth surface (Figure 1c). No similar skin lesions were found in other parts of the patient’s body, and a systemic examination was normal. The patient was previously healthy and had no family history. He denied any history of local trauma. The preliminary clinical diagnosis was common warts, and surgical resection was performed. Intraoperatively, the tumor was completely removed, with a 2-mm margin around the tumor. Based on histopathology (Figures 2e and f), the final diagnosis was ADF. No recurrence was observed in the 1-year follow-up after surgery.
Case 4
A 27-year-old man had a single skin-colored papule, the size of a rice grain, appear on the ventral side of the right big toe 2 years prior, with occasional mild pain. The lesion gradually increased to 9 mm in diameter, protruding from the skin surface with a hard texture, smooth surface and pedicle-shaped base (Figure 1d). The patient was previously healthy, with no family history or trauma history. The preliminary clinical diagnosis was eccrine poroma (EP), and the tumor was completely removed, with a 3-mm margin. Histopathological examination results were consistent with ADF. No recurrence was observed in the 6-month follow-up after surgery.
Case 5
A 68-year-old female had a single skin-colored papule, the size of a miliary grain, appear in the proximal fold of the left middle finger 3 years prior, and she did not have subjective symptoms. The lesion gradually increased to 8 mm * 6 mm, with a hard texture and smooth surface (Figure 1e). The patient was previously healthy, with no family history or trauma history. The preliminary clinical diagnosis was digital fibrokeratoma, and the tumor was completely removed, with a 2-mm margin. Histopathological manifestations were consistent with ADF. No recurrence was observed in the 6-month follow-up after surgery.
Discussion
ADF, also known as acral fibrokeratoma (AF), was first reported by Bart et al in 1968. Clinically, ADF is more common in males than in females, with an average age at onset of 40 years, and it is likely to occur in digits,2 especially digit joints.3 ADF skin lesions often manifest as solitary normal-skin color or pink papules or nodules, with a firm texture and hemispherical or finger-like shape. The protruding skin surfaces exhibit exophytic growth, the base can be contracted, and collar-shaped bulges can be seen on the periphery.4 ADF is slow-growing, without any subjective symptoms, and there is no evidence of spontaneous resolution. ADF lesions are usually less than 1 cm in diameter; ADF lesions with a diameter >1 cm are called giant ADFs.5 Choi6 and Ali et al7 reported large ADFs of 2.5 cm×1.6 cm×1.4 cm and 1.6 cm×1.2 cm, respectively. In most cases, ADF involves a solitary lesion. Frydman et al8 reported a case of ADF mostly on the plantar side of the foot. For the patients in this study, the mean age was 42.6 years, which is approximately the same as that reported in the literature. However, the ages of 2 patients were 22 and 27 years, far younger than average age at onset of ADF, indicating that clinicians should not ignore ADF in the young population so as to avoid misdiagnosis or missed diagnosis. The skin lesions of patients in this study all occurred on the fingers and toes and were all solitary. In Case 1, there was a collar-shaped bulge at the surrounding skin and a contraction ring at the base; the skin lesion was very typical.
The cause of ADF is still unclear. The results of some studies have suggested that trauma and repeated stimulation may be inducers of ADF9 and that coagulation factor XIIIa may be involved in ADF development.10 Patients in this study denied a history of local trauma, had no abnormal coagulation function test results, and had no history of XIIIa abnormalities such as hemophilia or a family history of genetic disorders. Therefore, the causes of ADF in this study were unknown. Other studies have found that the pathogenesis of some ADFs is related to medications. Qiao et al11 reported the occurrence of ADF after the oral delivery of cyclosporine A for 6 years after kidney transplantation; gingival hyperplasia and ADF of the left big toe developed 2 years after the oral delivery of cyclosporine A, and both gingival hyperplasia and ADF partially resolved 1 month after the discontinuation of cyclosporine A, suggesting that cyclosporine A may be associated with the pathogenesis of ADF.
Clinically, ADF is easily misdiagnosed as other skin diseases,12 including cutaneous horns, PG, common warts, EP, cellular digital fibroma, superficial acral fibromyxoma, accessory digit, infantile digital fibromatosis, and dermatofibroma/ fibrous histiocytoma. Cutaneous horns mostly occur after benign skin diseases, precancerous lesions or malignant tumors and often occur in exposed areas of the skin, and they manifest as keratotic skin lesions. PG is a benign capillary hemangioma that is likely to occur after local trauma and manifests as a solitary red pedicled polypoid papule that is fast-growing, brittle and very easily bleeds. Common warts are commonly benign proliferations of the skin and mucous membrane caused by human papillomavirus (HPV) infection, and the skin lesions are exophytic hemispherical papules with a rough surface and verrucous hyperplasia. EP is a benign skin tumor originating from the sweat ducts within the epidermis, often occurs on the palmoplantar skin, especially the lateral plantar margins of the feet, and may present as red papules and nodules, with surface ulcerations and scabs occurring in some patients. Cellular digital fibroma is a unique CD34 positive benign fibrous lesion characterized by slow growth, usually asymptomatic, erythematous or fleshy, small (usually less than 5 mm) solitary papules located on the dorsal, lateral, or ventral sides of the fingers, or on the nail folds of the toes. Superficial acral fibromyxoma is a benign fibromyxoid tumor that typically appears in the form of painless nodules after trauma in the area below or around the nail. The most common form of accessory digit is a partially developed, non functional replicated little finger connected to the ulnar edge of the hand. Infantile digital fibromatosis, also known as Reye tumor, is a rare, asymptomatic, benign nodular proliferation of fibrous tissue, which occurs almost exclusively in the dorsolateral region of the fingers and toes. Dermatofibroma/ Fibrous histiocytoma is a common benign proliferative disease of the skin and soft tissue, characterized by round or oval shaped solid papules or nodules, ranging from brown to reddish brown in color. The 5 patients in this case study were all clinically misdiagnosed with other diseases, indicating that clinicians are not familiar with ADF and that the misdiagnosis rate is high. For exophytic lesions on the fingers and toes, attention should be paid to the differential diagnosis, and a histopathological examination should be performed.
Histopathological examinations have important value in the diagnosis of ADF. Under a low-magnification microscope, ADF manifests as finger-like papules on the skin surface, and the epidermis could exhibit different degrees of hyperplasia. Under a high-magnification microscope, collagen fiber bundles running vertically to the epidermis can be seen in the dermis, and these bundles are obviously thickened, red, and connected with the underlying dermal connective tissue, with varying fibroblast proliferation.13 Kint et al14 classified ADF into three types based on the clinical and histopathological features: type I (many collagen fiber bundles accompanied by a large amount of capillary hyperplasia), type II (many collagen bundles accompanied by obvious keratinization of the epidermis), and type III (flat to dome-shaped tumor with few cellular components). Leo L. Wang et al15 reported a case which histopathology was consistent with an acquired digital fibrokeratoma with changes of a pleomorphic fibroma. Lesional cells were negative for CD34, Rb, and p53, and were positive for FXIIIa. They introduced the pleomorphic acquired digital fibrokeratoma as a novel clinicopathologic entity. In this study, cases 1, 4, and 5 were consistent with the characteristics of type I ADF, case 2 was consistent with the characteristics of type II ADF, and case 3 was consistent with the characteristics of type III ADF.
Conclusion
For the treatment of ADF, surgical resection is the primary option, but CO2 laser or liquid nitrogen cryotherapy can also be used. During surgery, the base of the tumor must be completely removed to prevent recurrence.
Consent Statement
The patient had given written informed consent for the publication of his clinical details and accompanying images. This study was approved by the institutional review board of Affiliated Hospital of Weifang Medical University with the approval code of wyfy-2023-ky-193, and informed consent was obtained from all study subjects.
Funding
Research reported in this publication was supported by Doctoral Startup Fund of Affiliated Hospital of Weifang Medical University (No. 2021BKQ02), Technology Development Project of Affiliated Hospital of Weifang Medical University (WYFYKY-HX202201) and Weifang Science and Technology Development Project (2021YX034).
Disclosure
Xing Wang and Dong Zhang are co-first authors for this study. The authors have no conflicts of interest to declare for this work.
References
1. Shih S, Khachemoune A. Acquired digital fibrokeratoma: review of its clinical and dermoscopic features and differential diagnosis. Int J Dermatol. 2019;58(2):151–158. doi:10.1111/ijd.14046
2. Palaniappan V, Sadhasivamohan A, Sankarapandian J, Karthikeyan K. Acquired fibrokeratoma: a retrospective study in a Tertiary Centre in South India. Indian J Dermatol. 2022;67(3):312. doi:10.4103/ijd.ijd_239_22
3. Moon SH, Cho SH, Lee JD, et al. A case of acquired giant digital fibrokeratoma. J Clin Investigat Dermatol. 2016;4(2):2.
4. Lencastre A, Richert B. Flat-pan nail-wide acquired epiungual fibrokeratoma: report of 4 cases. Skin Appendage Disord. 2019;5(2):111–113. doi:10.1159/000491582
5. Mir MA, Vathulya M, Mahakalkar S, Manohar N. Acquired periungual fibrokeratoma looks like a supernumerary digit: an uncommon soft tissue tumor. J Cutan Aesthet Surg. 2020;13(3):261–263. doi:10.4103/JCAS.JCAS_2_20
6. Choi JH, Jung SY, Chun JS, et al. Giant acquired digital fibrokeratoma occurring on the left great toe. Ann Dermatol. 2011;23(1):64–66. doi:10.5021/ad.2011.23.1.64
7. Ali M, Mbah CA, Alwadiya A, Nur MM, Sunderamoorthy D. Giant fibrokeratoma, a rare soft tissue tumor presenting like an accessory digit, a case report and review of literature. Int J Surg Case Rep. 2015;10:187–190. doi:10.1016/j.ijscr.2015.03.041
8. Frydman AF, Mercer SE, Kleinerman R, Yanofsky VR, Birge MB. Acquired fibrokeratoma presenting as multiple plantar nodules. Dermatol Online J. 2010;16(10):5.
9. Jahan N, Ashwini PK, Chethana SG, Betkerur J, Shastry V. Horn on the Nail: acquired Ungual Fibrokeratoma. J Cutan Aesthet Surg. 2021;14(1):121–124. doi:10.4103/JCAS.JCAS_71_19
10. Tabka M, Litaiem N. Acquired digital fibrokeratoma. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
11. Qiao J, Liu YH, Fang K. Acquired digital fibrokeratoma associated with ciclosporin treatment. Clin Exp Dermatol. 2009;34(2):257–259. doi:10.1111/j.1365-2230.2008.02808.x
12. Garg S, Sandhu J, Kaur A, Punia RPS. Acquired digital fibrokeratoma. J Clin Aesthet Dermatol. 2019;12(5):17–18.
13. Fetsch JF, Laskin WB, Miettinen M. Superficial acral fibromyxoma: a clinicopathologic and immunohistochemical analysis of 37 cases of a distinctive soft tissue tumor with a predilection for the fingers and toes. Hum Pathol. 2001;32(7):704–714. doi:10.1053/hupa.2001.25903
14. Kint A, Baran R, De Keyser H. Acquired (digital) fibrokeratoma. J Am Acad Dermatol. 1985;12(5 Pt 1):816–821. doi:10.1016/S0190-9622(85)70101-6
15. Wang LL, Abbott JJ, Jiang AJ, Hannah C, Rubin AI. Pleomorphic acquired digital fibrokeratoma: a novel clinicopathologic entity. J Cutan Pathol. 2023;50(2):131–133. doi:10.1111/cup.14320
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.