Back to Journals » Clinical Ophthalmology » Volume 20
Accuracy of Two Novel Self-Contained Darkroom Refractive Screeners Compared with Cycloplegic Retinoscopy and a Traditional Autorefractor in Schoolchildren
Authors Jiang J ![]() , Yang R
, Yang R ![]() , Guo Y
, Guo Y ![]() , Zhong D, Lu H, Huang H, Chen Y
, Zhong D, Lu H, Huang H, Chen Y ![]() , Han Y, Tao Y
, Han Y, Tao Y ![]() , Chen Q
, Chen Q
Received 22 March 2026
Accepted for publication 19 May 2026
Published 3 June 2026 Volume 2026:20 609736
DOI https://doi.org/10.2147/OPTH.S609736
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Junda Jiang,1,2 Rui Yang,1 Yuqi Guo,1 Dedong Zhong,1 Haiyan Lu,1 Huiyao Huang,1 Yuhao Chen,1 Yun Han,1 Yangxiaolang Tao,1 Qi Chen1
1Visual Science and Optometry Center, The People’s Hospital of Guangxi Zhuang Autonomous Region, Guangxi Key Laboratory of Eye Health, Guangxi Health Commission Key Laboratory of Ophthalmology and Related Systemic Diseases Artificial Intelligence Screening Technology, Institute of Ophthalmic Diseases, Guangxi Academy of Medical Sciences, Nanning, Guangxi, 530022, People’s Republic of China; 2Youjiang Medical University for Nationalities, Baise, Guangxi, 533000, People’s Republic of China
Correspondence: Qi Chen, Visual Science and Optometry Center, The People’s Hospital of Guangxi Zhuang Autonomous Region, Guangxi Key Laboratory of Eye Health, Guangxi Health Commission Key Laboratory of Ophthalmology and Related Systemic Diseases Artificial Intelligence Screening Technology, Institute of Ophthalmic Diseases, Guangxi Academy of Medical Sciences, Nanning, Guangxi, 530022, People’s Republic of China, Email [email protected]
Objective: To evaluate the clinical performance of two novel self-contained darkroom refractive screeners (Columba 300, YD-SX-A) and a traditional tabletop autorefractor (Topcon KR8800) in refractive screening for children and adolescents, using cycloplegic retinoscopy (CR) as the gold standard, and to provide evidence for equipment selection.
Methods: A total of 1354 participants aged 6– 18 years were enrolled from December 2025 to February 2026. Non-cycloplegic measurements were performed sequentially with the three devices, followed by CR after cycloplegia with 0.5% tropicamide. Statistical analyses included Wilcoxon signed-rank test, Bland-Altman analysis, linear regression, and ROC curve analysis.
Results: The prevalence of myopia, hyperopia, and astigmatism measured by CR was 73.2%, 15.0%, and 35.8%, respectively. All three devices showed strong positive correlation with CR in spherical equivalent (SE, r > 0.9), with Topcon KR8800 presenting the optimal correlation and consistency. YD-SX-A had the smallest mean difference in cylinder power with CR. All devices achieved excellent myopia diagnostic efficacy (AUC > 0.95), while Topcon KR8800 was superior in hyperopia and astigmatism diagnosis.
Conclusion: Topcon KR8800 has the highest accuracy for clinical precise screening. Columba 300 and YD-SX-A are portable, rapid, and sensitive for myopia screening, suitable for large-scale preliminary screening. A two-level “initial screening-confirmation” process is recommended for myopia prevention and control in children and adolescents.
Keywords: children and adolescents, refractive screening, self-contained darkroom refractive screener, cycloplegic retinoscopy, diagnostic efficacy, myopia prevention and control
Background
In recent years, myopia has become a global public health problem with a continuously rising incidence.1–3 It is predicted that by 2050, the global myopic population will reach 4.758 billion, accounting for 49.5% of the world’s total population.4 The prevalence of myopia among children and adolescents in China is particularly severe, with an overall myopia rate of 52.7%, including 14.3% in 6-year-old children, 35.6% in primary school students, 71.1% in junior high school students, and as high as 80.5% in senior high school students.5 Myopia not only affects the daily activities, academic performance, and career development of children and adolescents but also may lead to serious complications such as retinal degeneration, glaucoma, and macular degeneration when progressing to high myopia, even resulting in irreversible blindness.6–8 Therefore, large-scale refractive screening, as a key link in myopia prevention and control, is of great significance for early identification of high-risk groups and timely implementation of primary prevention (eg, increasing outdoor activity time) and secondary prevention (eg, low-concentration atropine, orthokeratology intervention).9–14
Cycloplegic retinoscopy (CR) is the “gold standard” for measuring refractive errors, which can obtain the true refractive status by inhibiting ciliary muscle accommodation.15,16 However, CR has limitations such as cumbersome operation, dependence on the expertise of professional optometrists, 30–40 minutes of onset time for cycloplegic agents (eg, tropicamide), and potential adverse reactions such as photophobia and blurred near vision, making it difficult to meet the needs of large-scale population screening in schools and communities.17,18 Non-cycloplegic refraction is reliable for adults but inaccurate for children under 18 years due to strong ciliary muscle accommodation.19,20 Currently, commonly used automatic refraction equipment for screening (eg, Retinomax Autorefractor, Spot Photoscreener, Welch Allyn SureSigh, PlusoptiX Photoscreener) has the advantages of rapidity and convenience,21–24 but their accuracy still needs to be improved due to factors such as strong ciliary muscle accommodation ability of children and adolescents, interference from ambient light during detection, and insufficient portability of equipment.25,26 Existing portable screeners are limited by ambient light interference; the two darkroom devices were selected for their fixed distance and darkroom design to reduce errors. The distribution of medical resources in China is uneven, and primary medical institutions are relatively lacking in professional optometrists and equipment. There is an urgent need for reliable and easy-to-operate novel screening equipment to improve the coverage of refractive screening.
This study included two novel self-contained darkroom refractive screeners: the Columba 300 and the YD-SX-A. Previous studies have confirmed its good consistency and effectiveness in refractive error detection, making it suitable for large-scale population screening.27 Unlike previous autorefractors, both have a fixed detection distance and darkroom environment, which theoretically can reduce light interference and accommodation effects, and are applicable to young children and subjects with poor compliance. This study compared the clinical performance of the two novel devices with the traditional tabletop autorefractor (Topcon KR8800) using CR as the gold standard, aiming to provide an evidence-based basis for the selection of refractive screening equipment for children and adolescents.
Methods
Participants
A total of 1354 children and adolescents aged 6–18 years who visited the Eye Center of Guangxi Zhuang Autonomous Region People’s Hospital from December 2025 to February 2026 were enrolled, and only data from the right eye were analyzed (n = 1354) to eliminate inter-eye correlation bias.28 The inclusion criteria were the absence of other ocular diseases, such as strabismus, amblyopia, cataracts, or glaucoma (confirmed via slit-lamp examination of the anterior segment and indirect ophthalmoscopy of the fundus). Exclusion criteria: ① Abnormal refractive medium; ② History of ocular surgery; ③ Complicated with nystagmus, aphakia, strabismus, amblyopia, or fundus diseases; ④ Suffering from other systemic diseases; ⑤ Use of orthokeratology lenses within six months; ⑥ Unable to cooperate with the completion of detection; ⑦ Test results exceeding the measurable range of the instrument. The requirement for written informed consent was waived by the Ethics Committee of Guangxi Zhuang Autonomous Region People’s Hospital (No. KY-IIT-2025-217) due to the observational and non-invasive nature of this study. All data were analyzed anonymously, and no identifying information was collected, ensuring participant privacy and confidentiality. This study was conducted in strict accordance with the Declaration of Helsinki.
Detection Instruments
Columba 300 Refractive Screening Instrument with Built-in Darkroom
This equipment is researched, developed, and produced by Changsha Anshikang Medical Technology Co., Ltd., with a core innovation of a built-in integrated closed darkroom cavity structure. Based on infrared red-eye reflection technology, it achieves objective refractive measurement, which can completely shield external light interference through its own darkroom, and simultaneously induce physiological mydriasis to inhibit the ciliary muscle accommodation reflex, effectively reducing the systematic error of refractive measurement in the non-cycloplegic state. The device adopts an arc-shaped ergonomic desktop design that fits the facial features of children, and the core screening tube can be detached separately, taking into account both desktop fixed detection and handheld mobile screening scenarios. The total weight of the device is approximately 2 kg, with a built-in large-capacity fast-charging battery, no need for a fixed external power supply. It can expand the simulated darkroom function with exclusive box accessories, has strong adaptability to strong light detection environments, and can complete standardized measurements without a professional darkroom. Equipped with innovative single-point ranging technology and age-specific iterative AI optical algorithm, the device can effectively avoid measurement interference caused by movement obstruction of young children, completing automatic simultaneous binocular detection within 2–5 seconds, with core optical data collection taking only 0.1 seconds. The built-in algorithm automatically completes 3 consecutive measurements and outputs the average value, meeting the requirements of the “Specifications for Refractive Error Screening of Primary and Secondary School Students”. It is also equipped with an age-appropriate audio-visual attraction module, which can significantly improve the detection cooperation of young children. Non-optometry professionals can operate it independently after simple training, and the maximum daily screening capacity of the device can reach more than 3000 person-times. A single detection can simultaneously obtain 8 categories of core optometric data including myopia, hyperopia, astigmatism, axis, pupil diameter, interpupillary distance, strabismus degree, and refractive medium abnormalities. It can seamlessly adapt to the Anshikang Nebula Eye Health Management System, supporting online establishment of children’s refractive development files and multi-terminal data query, and can generate individual and group refractive development trend analysis reports, providing standardized data support for precise prevention and control of children’s myopia.
YD-SX-A Refractive Screening Instrument with Built-in Darkroom
This equipment is independently researched, developed, and produced by Nanning Gardener Medical Devices Co., Ltd., a domestic refractive screening device with a core innovation of a 1-meter-long cylindrical built-in standardized darkroom structure. Based on infrared red-eye reflection technology and wavefront sensing principle, the device achieves objective refractive measurement. It can shield external light interference through the closed darkroom, induce physiological mydriasis to reduce the basic regulatory tension of the ciliary muscle, and minimize refractive measurement errors in the non-cycloplegic state. The device adopts a lightweight and detachable design, with a total weight of approximately 2 kg and a built-in rechargeable lithium battery. It does not require a fixed operating table, external power supply, or professional darkroom, has no special requirements for the lighting of the detection environment, and has strong scene adaptability. The operation terminal realizes one-key automatic simultaneous binocular detection on a tablet, completing a single-person measurement in 2–5 seconds. The built-in algorithm automatically completes 3 measurements and takes the average value, and the detection standard fully complies with the “Specifications for Refractive Error Screening of Primary and Secondary School Students”. Non-optometry professionals can operate it independently after simple training. A single detection can simultaneously obtain 15 core optometric data including spherical equivalent, sphere, cylinder, axis, and interpupillary distance, supporting wireless transmission and docking with the regional visual health management system, enabling paperless storage and information management of screening data.
Topcon KR8800 Desktop Autorefractor
This equipment is produced by Topcon Corporation of Japan, a classic medical-grade automatic integrated refractive-corneal curvature testing device, and is currently the gold standard reference device for clinical refractive examination and refractive screening of children and adolescents in domestic medical institutions. The core of the device is equipped with Topcon’s exclusive Rotary Prism measurement technology, constructing an optical detection system based on the principle of infrared light source reflection and Scheiner’s four-hole disk precise focusing design. Combined with an automatic fogging fixation system, it can capture a wider range of fundus reflected light through the rotating prism, significantly improving the reliability of refractive data compared with single-point measurement equipment. Meanwhile, it is synchronously equipped with a corneal curvature measurement module, which can accurately distinguish corneal-derived and intraocular-derived astigmatism and complete collaborative correction, reducing the systematic error of refractive measurement in the non-cycloplegic state from the optical principle. The device is an integrated fixed desktop structure with external dimensions of 27.5 cm × 47.5 cm × 45 cm and a net weight of approximately 16 kg. It has no built-in rechargeable battery and only supports external AC power supply, requiring placement on a stable operating table and use in a low-brightness darkroom environment. The device is equipped with a standardized chin rest and forehead rest with an adjustable range of 7 cm, which can strictly fix the subject’s head position and detection distance, eliminate measurement deviations caused by head position deviation and incorrect eye position, and ensure the standardization of detection conditions and the repeatability of results. The operation adopts a sequential monocular measurement mode, with a built-in automatic focusing and measurement program. After precise alignment, the measurement starts automatically. Each eye automatically completes 3 consecutive measurements and outputs the average value, meeting the requirements of the “Specifications for Refractive Error Screening of Primary and Secondary School Students” and automatically prompting remeasurement for abnormal measurement values. It is also equipped with a 5-inch color LCD display that can simultaneously display binocular measurement data, a built-in thermal printer supporting instant printing of test reports, and can realize rapid data transmission and management through USB and RS-232 interfaces. The refractive measurement range of the device: sphere −25 D~+22 D, cylinder 0~±10 D, axis measurement range 0°~180°, minimum measurable pupil diameter 2.0 mm, supporting high-precision step measurement of 0.12 D/0.125 D. It can simultaneously complete the measurement of corneal curvature, pupil diameter, interpupillary distance, and corneal diameter, and is equipped with an infrared reflection function to initially monitor abnormalities of the refractive medium. The landscape fixation target with adjustable two-color brightness can improve the subject’s fixation cooperation. The three instruments are shown in Figure 1.
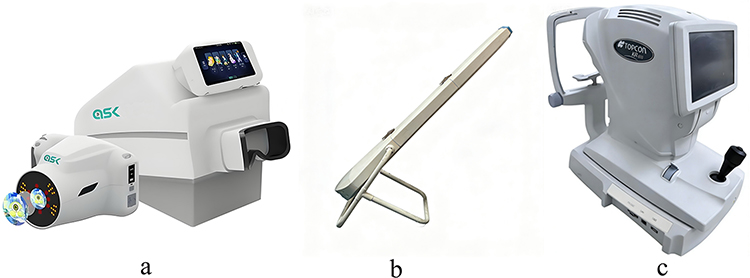 |
Figure 1 The three instruments (a) Columba 300 (b) YD-SX-A (c) Topcon KR8800. |
Detection Methods
Non-Cycloplegic Measurement
All participants underwent refractive error measurement using the following equipment sequentially with undilated pupils (without cycloplegic agents). Each device automatically performed three consecutive measurements, and the average values of spherical power (DS) and cylinder power (DC) were recorded.
Cycloplegia and CR Measurement
Participants eligible for cycloplegia, after excluding those with contraindications such as elevated intraocular pressure or a tendency toward angle-closure glaucoma, signed the informed consent form, and one drop of 0.5% tropicamide (Alcon Laboratories, Inc., Switzerland) was instilled into each eye at 5-minute intervals; 45 minutes later, the cycloplegic effect was confirmed if the pupil dilated to at least 6 mm and the light reflex was absent. CR measurements were performed by optometrists with over five years of experience via retinoscopy with a streak retinoscope (Welch Allyn, Inc., USA), and DS, DC, and cylinder axis were recorded.
Statistical Analysis
Data management: Excel was used to establish a database, with double-entry and verification by two persons. Statistical analyses were performed using SPSS 24.0, GraphPad Prism, and Python. Regarding definitions, the spherical equivalent (SE) was calculated as SE = DS + DC/2; myopia was defined as an SE < −0.5 D, hyperopia as an SE > +2.0 D, and astigmatism as a DC < −0.75 D. Since the data did not follow a normal distribution, non-parametric tests were used. For difference comparisons, the Wilcoxon signed-rank test was utilized to evaluate measurement discrepancies between each device and the CR. Consistency analysis: Bland-Altman method was used to assess the consistency between devices and CR, and the mean difference, 95% limits of agreement (LOA), and coverage rate were calculated. Correlation analysis: Linear regression analysis was used to evaluate the correlation between each device and CR, and Pearson correlation coefficient (r) and coefficient of determination (R2) were calculated. For diagnostic efficacy evaluation, receiver operating characteristic (ROC) curves were generated to calculate the area under the curve (AUC), optimal cutoff value, sensitivity, and specificity. A P value <0.05 was considered statistically significant.
Results
General Characteristics
A total of 1354 participants were enrolled, with an average age of 10.37 ± 3.18 years (range: 6–18 years), including 689 males (50.9%) and 665 females (49.1%). Based on CR as the gold standard, the prevalence of myopia was 73.2% (991 eyes), hyperopia 15.0% (203 eyes), and astigmatism 35.8% (485 eyes). The refractive distribution is shown in Figure 2. SE was mainly concentrated in the range of −3.00~0.00 D. The distribution trends of DS and DC were basically consistent with those of CR, but the measured values of the three devices were slightly biased towards myopia (eg, the average SE of Columba 300 was −2.00 D, and that of CR was −1.55 D).
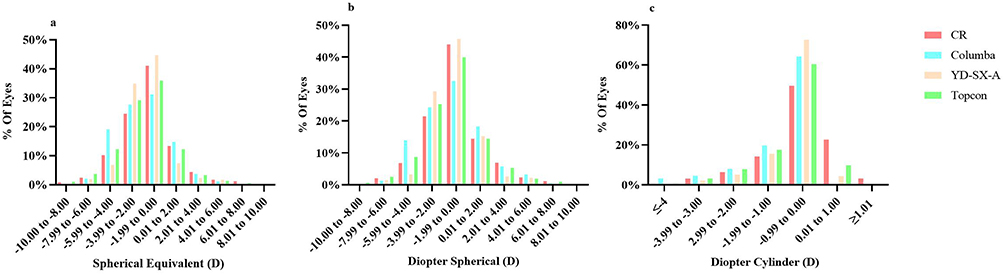 |
Figure 2 Histogram illustrating the distribution of refractive error in diopter (a) SE (b) DS (c) DC. |
Comparison of Differences Between Each Device and CR (Wilcoxon Signed-Rank Test)
All Participants and Myopic Group
As shown in Table 1A, among all participants, there were statistically significant differences in SE and DS among the three devices compared to CR (P < 0.001), and only the DC measurement of YD-SX-A showed no significant difference from CR (P = 0.076). In the myopic group, Columba 300 had significant differences in SE, DS, and DC with CR (P < 0.001); YD-SX-A demonstrated significant differences in SE (P = 0.021) and DS (P < 0.001) from CR, but no difference in DC (P = 0.277); Topcon KR8800 had significant differences in all parameters with CR (P < 0.001).
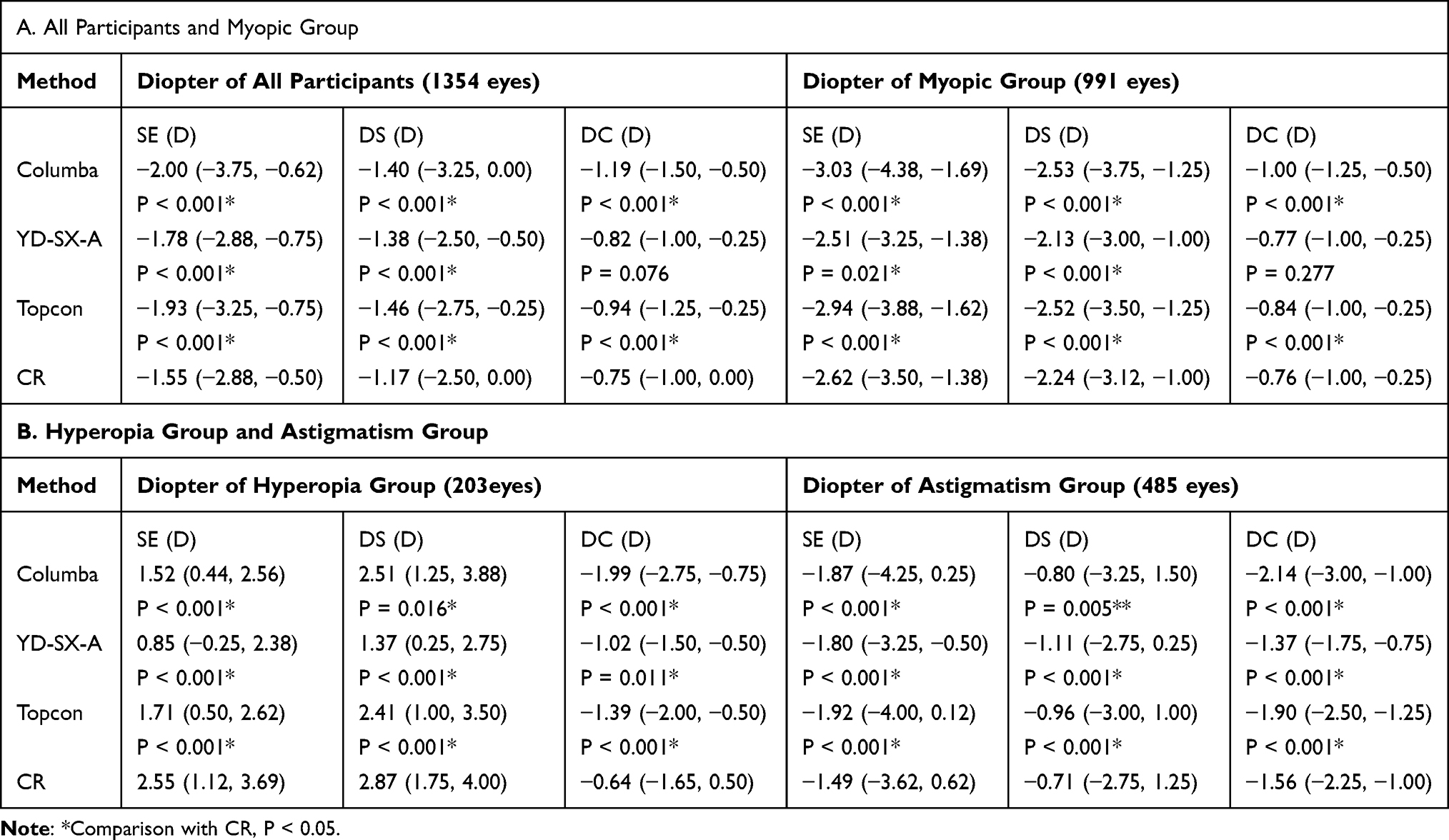 |
Table 1 Data Distribution of All Devices in Different Groups [D, M (P25, P75)] |
Hyperopia Group and Astigmatism Group
As shown in Table 1B, in the hyperopia group, the three devices had significant differences in SE, DS, and DC with CR (P < 0.05), notably, the difference in DS for the Columba 300 was marginally significant (P = 0.016); in the astigmatism group, all devices showed significant differences in SE, DS, and DC from CR (P < 0.001), but YD-SX-A exhibited the smallest mean difference in DC (mean difference −0.19 D).
Bland-Altman Consistency Analysis
Bland-Altman consistency analysis of all participants demonstrated that the Topcon KR8800 exhibited the optimal SE consistency with CR (Table 2), with a mean difference of −0.387 D, a 95% LOA of [−1.880, 1.106] D, an LOA width of only 2.986 D, and a coverage rate of 95.7%; the Columba 300 had an SE mean difference of −0.454 D, a 95% LOA of [−2.367, 1.459] D, and a coverage rate of 94.3%; and the YD-SX-A had an SE mean difference of −0.238 D, but the widest 95% LOA width (4.452 D) and a coverage rate of 94.2%. In terms of DC consistency, the YD-SX-A had the smallest mean difference with CR (−0.072 D) and a coverage rate of 94.2%. The consistency scatter plots for each device compared with CR are presented in Figures 3–5. The measured values from the Topcon KR8800 were more closely clustered around the CR values, exhibiting the lowest degree of dispersion; whereas the dispersion for the Columba 300 and YD-SX-A increased slightly within the high refractive error range (SE < −5.0 D).
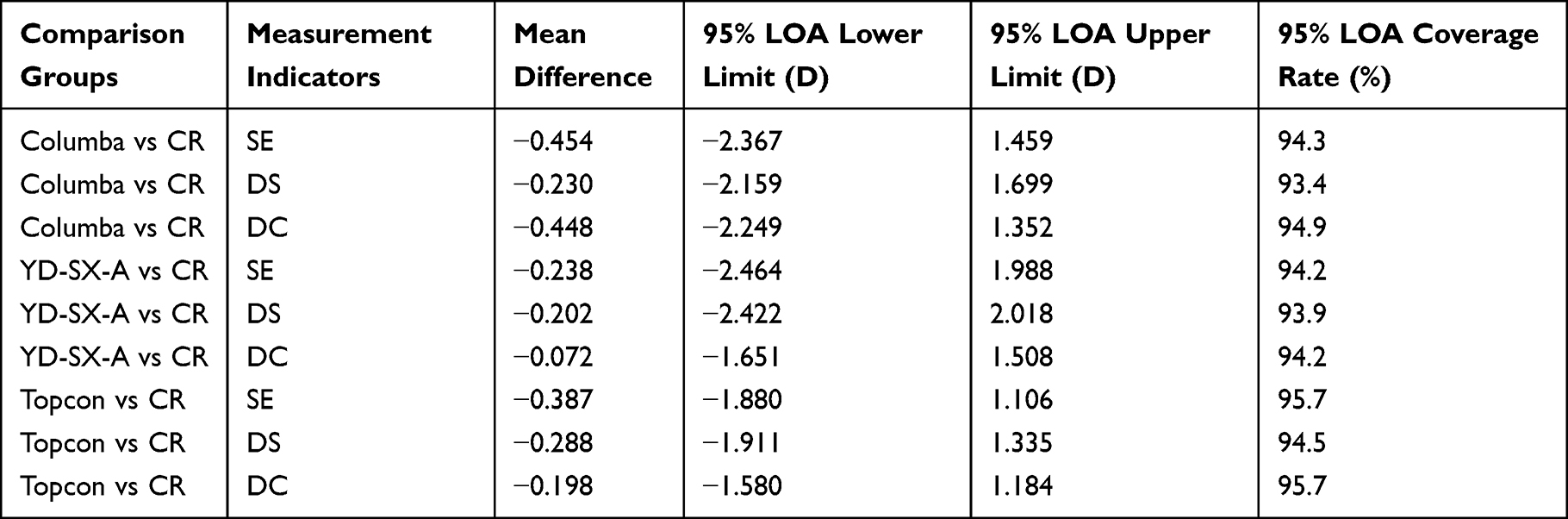 |
Table 2 Bland-Altman Agreement Analysis Results (All Participants) |
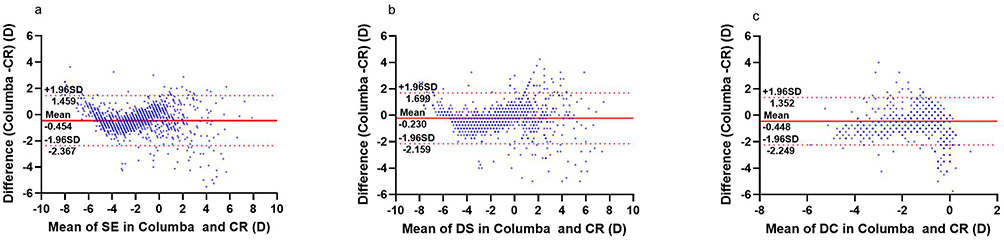 |
Figure 3 Bland–Altman plots of the Columba vs CR (a) SE (b) DS (c) DC. |
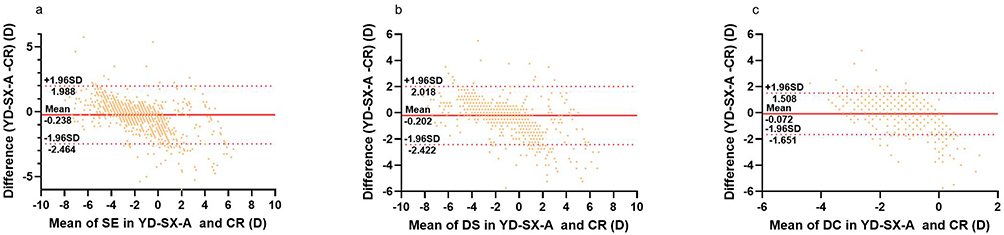 |
Figure 4 Bland–Altman plots of the YD-SX-A vs CR (a) SE (b) DS (c) DC. |
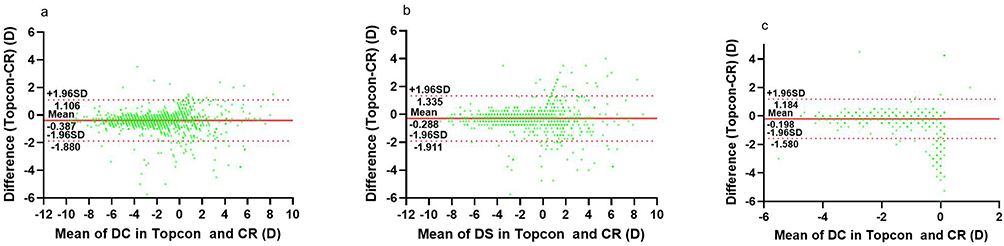 |
Figure 5 Bland–Altman plots of the Topcon vs CR (a) SE (b) DS (c) DC. |
Linear Regression and Correlation Analysis
As shown in Figure 6, all three devices demonstrated a strong positive correlation between their measurements and the CR reference standard for SE (r > 0.9): the Topcon KR8800 yielded an r value of 0.9528, an R2 of 0.9079, and a regression equation of Y = 0.330 + 0.970X (exhibiting the slope closest to 1 and the smallest intercept); the Columba 300 produced an r of 0.9210, an R2 of 0.8515, and a regression equation of Y = 0.398 + 0.972X; the YD-SX-A showed an r of 0.9023, an R2 of 0.8142, and a regression equation of Y = 0.577 + 1.190X (where a slope >1 suggests potential overestimation at higher refractive errors).
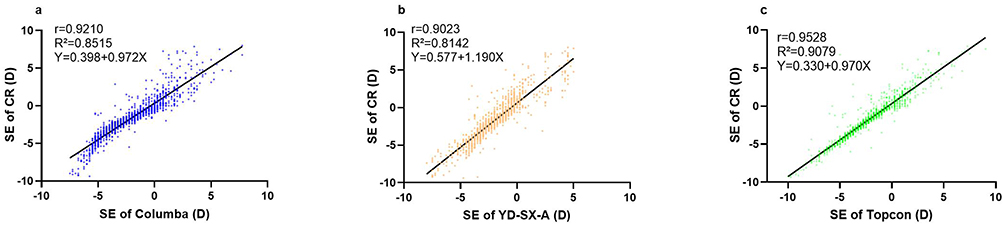 |
Figure 6 SE correlation between Screening Instruments and CR (a) Columba (b) YD-SX-A (c) Topcon. |
ROC Curve and Diagnostic Efficacy
As shown in Table 3, all three devices demonstrated excellent diagnostic accuracy for diagnosing myopia (AUC > 0.95): the Topcon KR8800 exhibited the highest sensitivity (98.1%) with an optimal cutoff value of −0.875 D, while the Columba 300 and YD-SX-A showed sensitivities of 93.0% and 95.6%, and specificities of 89.3% and 82.6%, respectively. For hyperopia diagnosis, the Topcon KR8800 achieved an AUC of 0.963 and a sensitivity of 93.1%, performing significantly better than the Columba 300 (AUC = 0.957, sensitivity = 86.7%) and YD-SX-A (AUC = 0.940, sensitivity = 84.2%), while specificities were similar among the three devices (ranging from 89.8% to 91.8%). In astigmatism diagnosis, Topcon KR8800 had an AUC of 0.986, a sensitivity of 98.2%, and a specificity of 91.0%, which was significantly superior to Columba 300 (AUC = 0.854, sensitivity = 68.9%) and YD-SX-A (AUC = 0.852, sensitivity = 71.0%). The ROC curves of each device are shown in Figure 7. The curve for the Topcon KR8800 was closer to the upper-left corner, indicating optimal diagnostic performance; whereas the curves for the Columba 300 and YD-SX-A were similar in myopia diagnosis, they exhibited considerable divergence in astigmatism diagnosis.
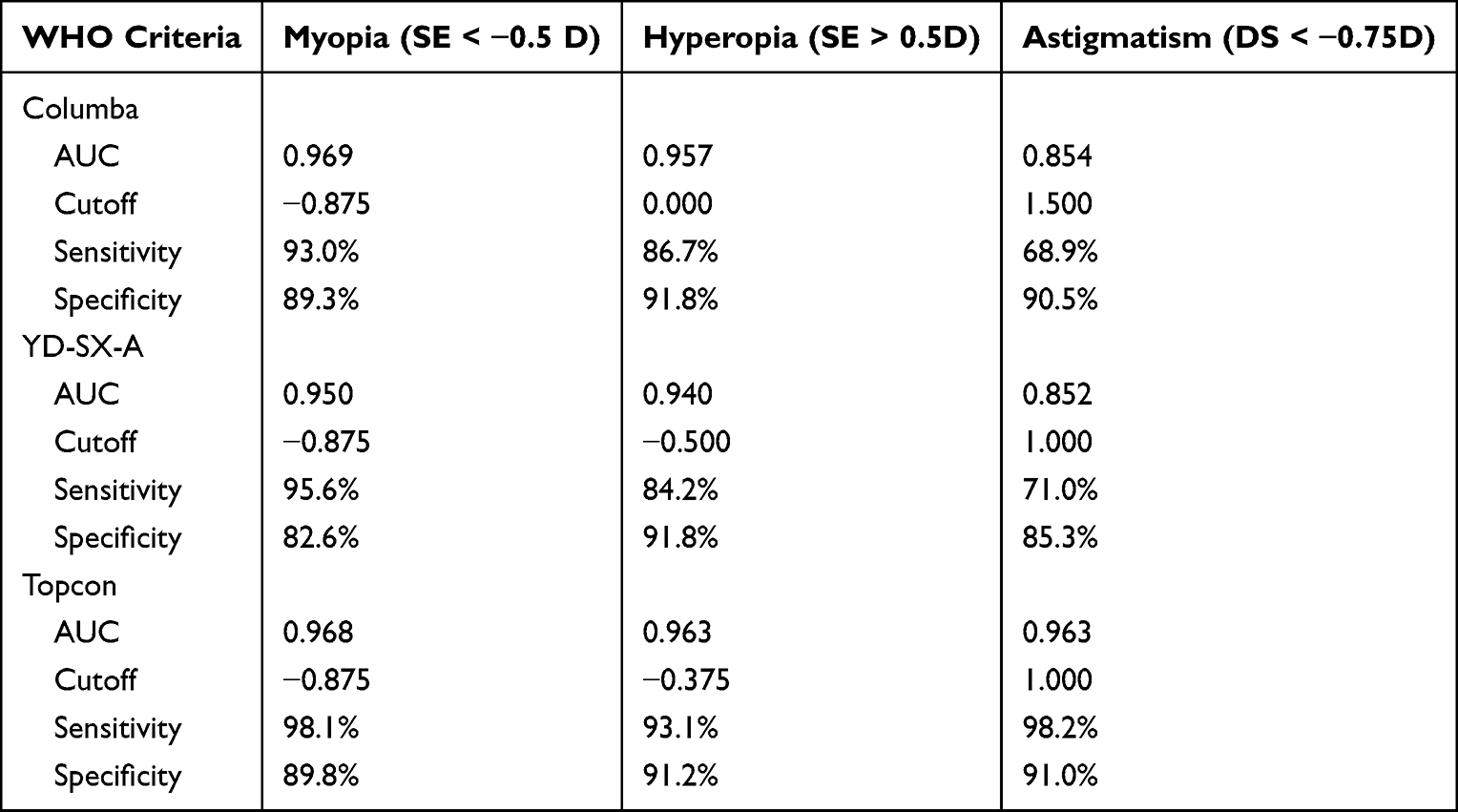 |
Table 3 Refractive Error Detection: Sensitivity/Specificity Comparison (ROC-Derived Cutoffs) |
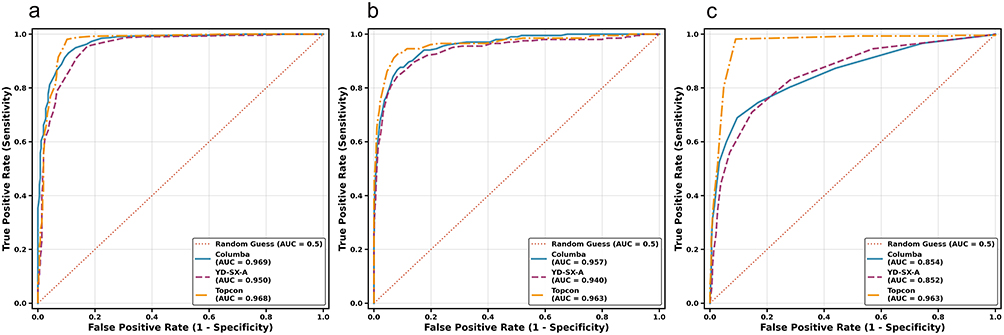 |
Figure 7 ROC Curve Comparison of Different Instruments vs CR (a) Myopia (b) Hyperopia (c) Astigmatism. |
Discussion
This study systematically evaluated the performance of two novel self-contained darkroom refractive screeners (Columba 300, YD-SX-A) and a traditional tabletop autorefractor (Topcon KR8800) in refractive screening of children and adolescents aged 6–18 years using CR as the gold standard. The results showed that all three devices have clinical application value, but there are significant differences in consistency, correlation, and diagnostic efficacy. The analysis is carried out below in combination with data and existing studies.
The Wilcoxon signed-rank test showed that there were statistically significant differences in SE and DS between the three devices and CR (P < 0.001), and only the DC of YD-SX-A had no significant difference from CR in all participants and the myopic group (P = 0.076 and P = 0.277). According to research,27 the inherent difference between refractive screeners and CR is mainly due to the strong ciliary muscle accommodation ability of children and adolescents, and even the darkroom environment cannot completely eliminate accommodation interference. The DC stability of YD-SX-A is better, which may be related to its 1-meter long darkroom design that allows sufficient pupil dilation (diameter > 6 mm) and reduces the interference of corneal reflection and lens accommodation on cylinder power measurement. This suggests that it can provide more reliable cylinder power reference values in preliminary astigmatism screening and is suitable as a preferred tool for astigmatism screening in primary medical institutions.
Bland-Altman analysis showed that Topcon KR8800 had the narrowest LOA width for SE measurement (2.986 D) and a coverage rate of 95.7%, which was significantly superior to the two novel devices. This is consistent with the high stability characteristics of Topcon series autorefractors in children and adolescents screening reported by Di Wang et al29,30 Topcon KR8800 is based on the double pinhole imaging principle, scans the 180° meridian focus through infrared, has a better inhibitory effect on accommodation, and is equipped with corneal curvature measurement function, which can reduce errors through collaborative correction of corneal astigmatism and intraocular astigmatism.31 Therefore, it performs excellently in precise detection and is suitable as a reference for clinical diagnosis (eg, trial lens reference before glasses fitting). The LOA widths of Columba 300 and YD-SX-A are slightly wider (3.826 D, 4.452 D), but the coverage rate of over 94% still meets the needs of large-scale screening. The increased dispersion of the two in the high refractive error range (SE < −5.0 D) may be related to the thinning of the retinal pigment epithelium in children with high myopia and weakened reflection signals, leading to a decrease in the accuracy of infrared imaging algorithms.32,33 In the future, it is necessary to optimize the measurement model for high myopia population (eg, adding retinal signal enhancement algorithms).
Linear regression showed that all three devices had a strong positive correlation with CR in SE (r > 0.9), among which Topcon KR8800 had R2 = 0.9079, and the regression equation slope (0.970) was closest to 1 and the intercept (0.330 D) was the smallest, indicating that it can best explain the variance in CR measurements. The high correlation of Topcon KR8800 enables it not only to be used for screening but also to provide reliable refractive error change data for clinical treatment (eg, evaluation of low-concentration atropine efficacy).34 The regression equation of Columba 300 (Y = 0.398+0.972X) shows a systematic underestimation of about 0.4 D; the regression equation of YD-SX-A is Y = 0.577+1.190X, with a slope (1.190) >1, suggesting underestimation in low refractive error and overestimation in high refractive error.
ROC curve analysis showed that all three devices had excellent diagnostic accuracy in myopia diagnosis (AUC > 0.95), and the optimal cutoff value (−0.875 D) was slightly lower than the clinical standard (−0.50 D). The myopia sensitivity of Topcon KR8800 reached 98.1%, with a missed diagnosis rate of only 1.9%, making it suitable as a precise screening tool; the sensitivities of Columba 300 and YD-SX-A were >93%, and although their specificities were slightly lower (82.6%~89.3%), considering that large-scale screening needs to prioritize sensitivity (reducing missed diagnoses), the two still have application value, such as annual school screening.
In hyperopia diagnosis, the sensitivity of Topcon KR8800 (93.1%) was significantly superior to the novel devices. The reason may be that the ciliary muscle accommodation of hyperopic children is more active, and the darkroom environment cannot completely inhibit accommodation.19 It is suggested that hyperopia screening should be combined with cycloplegia or multiple measurements (eg, performing two measurements at 5-minute intervals and taking the average value). In astigmatism diagnosis, the AUC of Topcon KR8800 was 0.986, which was significantly superior to Columba 300 (68.9%) and YD-SX-A (71.0%). This is related to the fact that the two novel devices lack corneal curvature measurement and only rely on red reflex to analyze astigmatism. It is recommended that subjects with abnormal astigmatism (DC < −0.75 D) need to be further confirmed by Topcon or CR to avoid astigmatism missed diagnosis caused by equipment errors.
As self-contained darkroom portable devices, Columba 300 and YD-SX-A have operational advantages incomparable to traditional tabletop instruments, and can effectively make up for the shortage of primary medical resources:4 Portability: YD-SX-A is foldable for storage (weight <3 kg), and Columba 300 has a volume only 1/3 of that of traditional tabletop devices, both supporting battery power supply (battery life > 8 hours), suitable for remote areas or mobile screening (eg, rural schools); Child-friendliness: The dynamic audio-visual module of Columba 300 and the simple operation process of YD-SX-A; Efficiency: Binocular measurement can be completed in 2–5 seconds, and more than 3000 people can be screened per day, which is more than 10 times the efficiency of CR, suitable for large-scale population screening.
Combined with China’s myopia prevention and control system of “primary screening - upper-level confirmation”, the two novel devices can be used as primary screening tools (eg, initial school screening), and abnormal cases are referred to secondary hospitals for confirmation through Topcon KR8800 or CR, forming a closed-loop management of “initial screening - confirmation - intervention”. For example, YD-SX-A can quickly identify high-risk myopic children (eg, SE < −0.875 D) in community screening and synchronize data to the regional medical platform, providing a basis for subsequent interventions (eg, increasing outdoor activities).
This study has the following limitations: Single-center design: The samples were limited to Guangxi region, which may have geographical bias (eg, differences in refractive characteristics between children in southern and northern China). In the future, multi-center studies (covering eastern, central, and western regions) are needed to verify the results; Insufficient age stratification: The device performance was not analyzed by age subgroups (6–8 years, 9–12years, 13–18 years), and differences in accommodation ability of children of different ages may affect the results; Lack of post-mydriasis comparison: The difference between novel devices and CR after mydriasis was not compared, so the synergistic effect of darkroom environment and cycloplegia cannot be clarified; No biological parameters included: Ocular axial length, corneal curvature, pupil size and other parameters were not combined, making it difficult to comprehensively evaluate the predictive value of the device for myopia progression.
Future research can focus on the following directions: Optimizing the algorithms of novel devices (eg, adding age stratification models); Conducting performance evaluation of novel devices after mydriasis; Establishing a “refractive error - ocular axis” combined screening model by combining ocular axial length to improve the prediction accuracy of myopia progression risk.
Conclusion
Topcon KR8800 has the highest accuracy and stability in refractive measurement of children and adolescents, making it suitable for precise clinical screening and diagnostic reference. Columba 300 and YD-SX-A, with their advantages of portability, rapidity, and high myopia screening efficacy (sensitivity > 93%), are applicable for large-scale population preliminary screening, especially for school-aged children with poor compliance and primary care settings with limited resources. In clinical practice, a two-level process of “initial screening - confirmation” should be adopted: novel darkroom devices are preferred for large-scale initial screening, and abnormal cases are further confirmed by Topcon KR8800 or CR to achieve early detection and precise intervention of refractive errors, thereby facilitating myopia prevention and control in children and adolescents.
Funding
This study was supported by Guangxi Health Commission Self-funded Scientific Research Project (No. Z-A20220135) and Guangxi Clinical Ophthalmic Research Center (No. Guike AD19245193).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wu P-C, Huang H-M, Yu H-J, et al. Epidemiology of Myopia. Asia Pac J Ophthalmol. 2016;5(6):386–12. doi:10.1097/APO.0000000000000236
2. Zhang X, Zhou Y, Wang Y, et al. Trend of myopia through different interventions from 2010 to 2050: findings from Eastern Chinese student surveillance study. Front Med. 2023;9:1069649. doi:10.3389/fmed.2022.1069649
3. Grzybowski A, Kanclerz P, Tsubota K, et al. A review on the epidemiology of myopia in school children worldwide. BMC Ophthalmol. 2020;20(1):27. doi:10.1186/s12886-019-1220-0
4. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
5. Tang W, Tan T, Lin J, et al. Developmental characteristics and control effects of myopia and eye diseases in children and adolescents: a school-based retrospective cohort study in Southwest China. BMJ Open. 2024;14(9):e083051. doi:10.1136/bmjopen-2023-083051
6. Ziemssen F, Lagrèze W, Voykov B. [Secondary diseases in high myopia]. Ophthalmologe. 2017;114(1):30–43. German. doi:10.1007/s00347-016-0390-x
7. Koo EB, Gilbert AL, Vanderveen DK. Treatment of amblyopia and amblyopia risk factors based on current evidence. Semin Ophthalmol. 2016;32(1):1–7. doi:10.1080/08820538.2016.1228408
8. Pascual M, Huang J, Maguire MG, et al. Risk factors for amblyopia in the vision in preschoolers study. Ophthalmology. 2013;121(3):622–9.e1. doi:10.1016/j.ophtha.2013.08.040
9. Atowa UC, Wajuihian SO, Hansraj R. A review of paediatric vision screening protocols and guidelines. Int J Ophthalmol. 2019;12(7):1194–1201. doi:10.18240/ijo.2019.07.22
10. Nottingham Chaplin PK, Baldonado K, Hutchinson A, et al. Vision and eye health: moving into the digital age with instrument-based vision screening. NASN Sch Nurse. 2015;30(3):154–160. doi:10.1177/1942602X15581054
11. Morgan IG, French AN, Ashby RS, et al. The epidemics of myopia: aetiology and prevention. Prog Retin Eye Res. 2017;62:134–149. doi:10.1016/j.preteyeres.2017.09.004
12. Walline JJ, Lindsley K, Vedula SS, et al. Interventions to slow progression of myopia in children. Cochrane Database Syst Rev. 2011;(12):CD004916. doi:10.1002/14651858.CD004916.pub3
13. Zheng -N-N, Tan K-W. The synergistic efficacy and safety of combined low-concentration atropine and orthokeratology for slowing the progression of myopia: a meta-analysis. Ophthalmic Physiol Opt. 2022;42(6):1214–1226. doi:10.1111/opo.13029
14. González-Méijome JM, Faria-Ribeiro MA, Lopes-Ferreira DP, et al. Changes in peripheral refractive profile after orthokeratology for different degrees of myopia. Curr Eye Res. 2015;41(2):199–207. doi:10.3109/02713683.2015.1009634
15. Morgan IG, Iribarren R, Fotouhi A, et al. Cycloplegic refraction is the gold standard for epidemiological studies. Acta Ophthalmol. 2015;93(6):581–585. doi:10.1111/aos.12642
16. Safir A. Retinoscopy. Int Ophthalmol Clin. 1971;11(1):115–129. doi:10.1097/00004397-197101110-00008
17. Yazdani N, Sadeghi R, Momeni-Moghaddam H, et al. Comparison of cyclopentolate versus tropicamide cycloplegia: a systematic review and meta-analysis. J Optom. 2017;11(3):135–143. doi:10.1016/j.optom.2017.09.001
18. Contreras-Salinas H, Orozco-Ceja V, Romero-López MS, et al. Ocular cyclopentolate: a mini review concerning its benefits and risks. Clin Ophthalmol. 2022;16:3753–3762. doi:10.2147/OPTH.S388982
19. Lu C, Miao Y, Yao X, et al. Socioeconomic disparities and green space associated with myopia among Chinese school-aged students: a population-based cohort study. J Glob Health. 2024;14:04140. doi:10.7189/jogh.14.04140
20. Sanfilippo PG, Chu B-S, Bigault O, et al. What is the appropriate age cut-off for cycloplegia in refraction? Acta Ophthalmol. 2014;92(6):e458–e62. doi:10.1111/aos.12388
21. Paff T, Oudesluys-Murphy AM, Wolterbeek R, et al. Screening for refractive errors in children: the plusoptiX S08 and the Retinomax K-plus2 performed by a lay screener compared to cycloplegic retinoscopy. JAAPOS. 2010;14(6):478–483.
22. O’Hara MA. Instrument-based pediatric vision screening. Curr Opin Ophthalmol. 2016;27(5):398–401. doi:10.1097/ICU.0000000000000289
23. Garry GA, Donahue SP. Validation of Spot screening device for amblyopia risk factors. JAAPOS. 2014;18(5):476–480.
24. Arnold RW, Armitage MD. Performance of four new photoscreeners on pediatric patients with high risk amblyopia. J Pediatr Ophthalmol Strabismus. 2014;51(1):46–52. doi:10.3928/01913913-20131223-02
25. Tuncer I, Zengin MO, Karahan E. Comparison of the Retinomax hand-held autorefractor versus table-top autorefractor and retinoscopy. Int J Ophthalmol. 2014;7(3):491–495. doi:10.3980/j.issn.2222-3959.2014.03.19
26. Tsuneyoshi Y, Negishi K, Tsubota K. Importance of accommodation and eye dominance for measuring objective refractions. Am J Ophthalmol. 2017;177:69–76. doi:10.1016/j.ajo.2017.02.013
27. Wei X, Li L, Jiang L, et al. Comparison of the new self-contained darkroom refractive screener versus table-top autorefractor and cycloplegia retinoscopy in detecting refractive error. BMC Ophthalmol. 2023;23(1):487. doi:10.1186/s12886-023-03231-6
28. Pesudovs K, Weisinger HS. A comparison of autorefractor performance. Optom Vis Sci. 2004;81(7):554–558. doi:10.1002/j.1538-9235.2004.tb01830.x
29. Wang D, Jin N, Pei R-X, et al. Comparison between two autorefractor performances in large scale vision screening in Chinese school age children. Int J Ophthalmol. 2020;13(10):1660–1666. doi:10.18240/ijo.2020.10.22
30. Su T, Min X, Liu S, et al. [Accuracy of three common optometry methods in examination of refraction in juveniles]. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2016;41(2):174–181. Chinese. doi:10.11817/j.issn.1672-7347.2016.02.010
31. Wang X, Dong J, Wu Q. Comparison of anterior corneal curvature measurements using a galilei dual scheimpflug analyzer and topcon auto kerato-refractometer. J Ophthalmol. 2014;2014:140628. doi:10.1155/2014/140628
32. Chung YW. Myopia: a review of current concepts, association with nonophthalmological conditions, and treatment strategy in children and adolescents. Clin Exp Pediatr. 2025;68(8):554–565. doi:10.3345/cep.2025.00115
33. Yuan W, Xu X, Zhao F. Trends and hot spots in research related to aqueous humor from 2014 to 2023: a bibliometric analysis. Heliyon. 2024;10(13):e33990. doi:10.1016/j.heliyon.2024.e33990
34. Chen H, Pan Z, Liu X, et al. Posterior eye curvature as a biomarker for differentiating pathologic myopia from high myopia. Am J Ophthalmol. 2025;275:88–98. doi:10.1016/j.ajo.2025.03.024
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.