Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Abnormal Brain Functional Connectivity in Patients with Chronic Obstructive Pulmonary Disease and Correlations with Clinical and Cognitive Parameters
Authors Han KI ![]() , Yeo Y
, Yeo Y ![]() , Jo HJ, Jo MJ, Park Y
, Jo HJ, Jo MJ, Park Y ![]() , Park TS, Jung SJ, Bae JH, Jang SH, Choi J
, Park TS, Jung SJ, Bae JH, Jang SH, Choi J ![]() , Park DW, Kim TH
, Park DW, Kim TH ![]()
Received 23 November 2024
Accepted for publication 26 March 2025
Published 5 April 2025 Volume 2025:20 Pages 971—985
DOI https://doi.org/10.2147/COPD.S505271
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Kyung-Il Han,1,* Yoomi Yeo,2,* Hang Joon Jo,3,4,* Min Ju Jo,5 Yeonkyung Park,6 Tai Sun Park,2 Sung Jun Jung,3,4 Jin Ho Bae,4 Sung-Ho Jang,7 Joonho Choi,8 Dong Woo Park,9 Tae-Hyung Kim2
1Department of Pulmonary and Critical Care Medicine, Asan Medical Center, Seoul, Korea; 2Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Hanyang University Guri Hospital, Hanyang University College of Medicine, Seoul, Korea; 3Department of Physiology, Hanyang University College of Medicine, Seoul, Korea; 4Department of Biomedical Engineering, Graduate School of Biomedical Science and Engineering, Hanyang University, Seoul, Korea; 5Department of Internal Medicine, Myongji St. Mary’s Hospital, Seoul, Korea; 6Department of Internal Medicine, Veterans Health Service Medical Center, Seoul, Korea; 7Department of Rehabilitation, College of Medicine, Hanyang University Guri Hospital, Guri, Korea; 8Department of Psychiatry, College of Medicine, Hanyang University Guri Hospital, Guri, Korea; 9Department of Radiology, College of Medicine, Hanyang University Guri Hospital, Guri, Korea
*These authors contributed equally to this work
Correspondence: Tae-Hyung Kim, Division of Pulmonology and Critical Care Medicine, Department of Internal Medicine, Hanyang University Guri Hospital, Hanyang University College of Medicine, 153, Gyeongchun-ro, Guri-si, Gyeonggi-do, 11923, Korea, Tel +82-31-560-2243, Fax +82-31-553-7369, Email [email protected]
Background: Cognitive impairment is a major comorbidity of chronic obstructive pulmonary disease (COPD), but the underlying mechanisms are not fully understood. In this study, we used resting-state functional magnetic resonance imaging to investigate brain functional connectivity (FC) abnormalities in patients with COPD and explored the correlation between abnormal FC and COPD-related clinical parameters.
Methods: Forty-one patients with COPD, without a definite diagnosis of cognitive impairment or depression, and 30 age- and sex-matched controls were recruited. A total of 184 resting-state functional connectivity (RSFC) maps were generated for all seed points. Welch’s t-test was used to assess differences in RSFC between the COPD and control groups, and the correlation coefficients between RSFC and clinical parameters were calculated.
Results: Patients with COPD had lower scores on the Mini-Mental State Exam (MMSE) and Korean version of the Montreal Cognitive Assessment and higher scores on the Beck Depression Inventory than the control group. Additionally, patients with COPD showed decreased RSFC in the left middle-posterior cingulate cortex, left posterior-dorsal cingulate cortex, and right superior occipital gyrus and increased RSFC in the left superior temporal sulcus, left posterior transverse collateral sulcus, right occipital pole, and right precentral gyrus. The regions showing differences in FC correlated with MMSE score, COPD symptom assessment scales, such as the COPD Assessment Test and modified Medical Research Council Dyspnea Scale, and pulmonary function parameters, including forced expiratory volume in one second and forced vital capacity.
Conclusion: Patients with COPD showed significant differences in FC within specific brain regions that correlated with symptoms, cognition, and lung function.
Keywords: Brain functional magnetic resonance imaging, chronic obstructive pulmonary disease, resting state functional connectivity
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by irreversible airflow limitation and may be accompanied by various comorbidities.1–3 Although COPD primarily affects the lungs, recent research has revealed its potential impact on the brain.4–6 However, comorbid cognitive impairment is frequently dismissed as a typical sign of aging, and delayed detection is common. A diagnosis of even mild cognitive impairment is important because it is associated with worse outcomes and increased health care burden in patients with COPD.7
Various pathophysiologic phenomena in COPD, including hypoxia, hypercapnia, oxidative stress, systemic inflammation, and comorbid cardiovascular diseases, may contribute to the development of cognitive impairment.4 The persistent airflow limitation associated with COPD may lead to arterial oxygen desaturation, which reduces the amount of oxygen supplied to the brain.8 Other studies have shown that hypoxia associated with COPD induces cerebral perfusion decline and neuronal damage.9,10 The prevalence of neuropsychological deficits increased from 27% in COPD patients with mild hypoxemia to 61% in those with severe hypoxemia, suggesting a significant relationship between the degree of hypoxemia and the extent of neuropsychological impairment.11
Different brain imaging techniques have been used to study cognitive impairment in patients with COPD (Table 1).12–27 One effective neuroimaging tool for investigating neuropsychological problems is resting-state functional magnetic resonance imaging (RS-fMRI), which can detect abnormalities in brain function by analyzing functional interactions among different brain regions. Akiyama et al used fMRI to analyze the pathway and localization of dyspnea sensation in the brain, finding that the resistive load required to induce thalamic and cortical activation was significantly lower in patients with COPD than controls.14 Zhang et al demonstrated that patients with COPD exhibit changes in spontaneous brain activity, as observed through RS-fMRI, with reduced activity in certain brain regions and increased activity in others, suggesting potential pathophysiologic changes related to oxygen transport and brain function.17
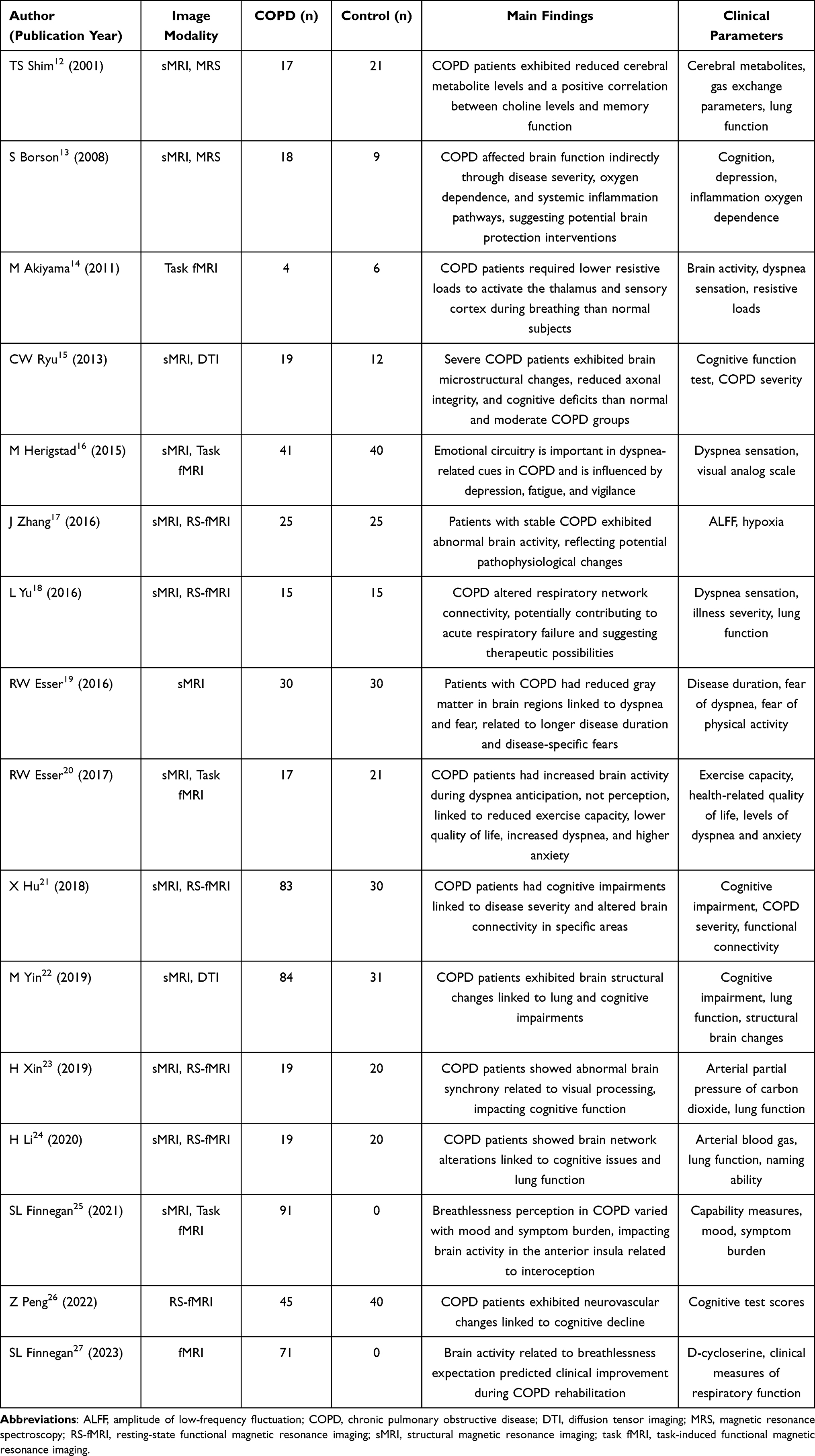 |
Table 1 Relevant Literature Review of Studies Using Brain MRI in COPD Patients |
RS-fMRI offers several advantages over task-based fMRI. It captures the brain’s intrinsic connectivity without requiring specific tasks, making it more accessible for clinical populations with cognitive or physical impairments. Additionally, it allows the identification of potential co-activation patterns through spontaneous neural synchrony, even within a short scan duration. Unlike task-based approaches that are limited to predefined stimuli or tasks, RS-fMRI provides a broader and more comprehensive view of brain network dynamics. Compared to previous research, in our study, we explored the FC between the COPD group and the control group by using a large number of gray-matter regions of interest (ROIs) as seed regions. We identified brain regions showing differences in FC between the COPD and control groups and further conducted an exploratory analysis to examine the correlations between these connectivity differences and key clinical parameters of COPD.
Methods
Participants
Fifty patients with COPD who had no prior diagnosis of cognitive impairment or depression were recruited. Forty-one patients (mean age = 70.6 ± 5.7, male: female ratio = 37:4) were selected as the patient group after excluding 9 patients who had severe brain shrinkage or brain infarction on image review. All patients underwent outpatient clinic follow-up for at least one year before enrollment. In the enrolled patients, COPD was diagnosed based on post-bronchodilator (BD) forced spirometry: a forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) <70% and post-BD FEV1 <80% of the normal value. Thirty participants with no respiratory symptoms or history of respiratory disease who were matched for age and sex (mean age = 68.9 ± 4.7, male: female = 27:3) with the patients were recruited as controls. The exclusion criteria were as follows: 1) overt neuropsychiatric disease, including dementia or major depressive disorder; 2) other lung parenchymal diseases, including interstitial lung disease and bronchiectasis; 3) untreated malignancy; 4) congestive heart failure; and 5) use of immunosuppressive agents.
The study was approved by the Institutional Review Board of the Hanyang University Guri Hospital (IRB No: GURI 2015–05-019), and all participants provided informed consent.
Assessment of Clinical Parameters
For all participants, characteristics such as smoking history and severity of dyspnea measured according to the modified Medical Research Council (mMRC) dyspnea scale were collected.28 The Charlson Comorbidity Index was used to evaluate comorbidities.29 Spirometry was performed according to the standard guidelines of the American Thoracic Society and European Respiratory Society.30 The Mini-Mental State Examination (MMSE) and MoCA-K (Korean version of the Montreal Cognitive Assessment) were used to evaluate cognitive function.31,32 Current quality of life status was measured using the EuroQoL-5D (EQ-5D).33 Beck Depression and Anxiety Inventories (BDI and BAI, respectively) were used to evaluate recent emotional status.34,35 Cerebrovascular risk was measured using the Framingham Risk Score Profile (FSRP).36
For COPD patients, in addition to post-BD spirometry and percutaneous oxygen saturation measurement, their current medical status was verified by their self-reported history of acute exacerbation within the previous year and COPD Assessment Test (CAT) score.37
Imaging Data Acquisition
Anatomical and functional MRI images were acquired for all participants using a 3.0-T MRI system (Philips Ingenia; Koninklijke Philips N.V., Amsterdam, Netherlands). All participants were instructed to close their eyes during the imaging session and were provided with earplugs. Foam pads were used to reduce the impact of head movements. For each individual subject, high-resolution structural whole-brain images were acquired using a T1-weighted MPRAGE pulse sequence (repetition time [TR]=8.4 s, echo time [TE]=4.1 s, flip angle [FA]=8°, 1×1×1 mm3 resolution), and then RS-fMRI data were acquired with a gradient echo-planar pulse sequence (TR=3.0 s, TE=35 ms, FA=90°, 30 slices with 1.72×1.72 mm2 in-plane resolution, and 5 mm slice thickness). Data quality assurance was performed by visual inspection by imaging specialists (Dong Woo Park and Hang Joon Jo) and using the Analysis of Functional NeuroImages (AFNI, https://afni.nimh.nih.gov) software package.38
Image Preprocessing
All imaging data were preprocessed using the AFNI package.39 The effects of physiologic disturbances on RS-fMRI data were reduced by adaptive cyclic physiologic noise modeling.40,41 The remaining effects of nuisance signals, including head-motion interference and hardware-related artifacts, were also corrected using the fast anatomy-based image correction method (fast ANATICOR).38,40,42 Subsequently, spatial smoothing with an isotropic Gaussian kernel (full-width-at-half-maximum = 6 mm) was applied to the RS-fMRI time series.43,44 Using the robust nonlinear warping function (3dQWarp) of the AFNI package, all image data were registered to the N27 brain atlas of the Montreal Neurological Institute and linearly resampled in the 1-mm isocubic grid space.45 All preprocessed data were assessed by AFNI data quality assurance pipelines.46
Functional Connectivity Analysis
A conventional seed-based correlation approach was used to obtain the RSFC maps of each participant. The seed points were placed in a 10 mm-diameter sphere centered on the segmented and labeled area generated by the FreeSurfer software pipeline.47 The seed points for each participant consisted of 184 gray matter regions (150 cortical and 34 subcortical areas), and the seed time series was retrieved by averaging the time series of RS-fMRI voxels overlapping their seed points.47,48 Pearson correlation coefficients were calculated between the seed time series and the time series of all voxels in the RS-fMRI data to produce the RSFC maps, which were then transformed into z-score maps using the Fisher z transformation. Ultimately, there were 184 RSFC maps for all seed points of a topic (13,064 FC maps for all seed points for all 71 subjects).
For each seed point, Welch’s t-test was performed to examine group differences in the RSFC map between COPD and control subjects, and the significance threshold for group statistics was set at family-wise-error-corrected P (PFWE) < 0.05, for multiple comparison correction by the clustering technique of the AFNI package.39
Correlation Analysis with Clinical Parameters
RSFC measurements were extracted for all patients with COPD by averaging the z-scores of the voxels within the group difference clusters obtained in the previous step. The correlation coefficients between the RSFC and all clinical parameters were calculated to determine the relationship between the patients’ RSFC and clinical manifestations. To minimize age-related bias, we set age as a covariate and excluded it from all statistical analyses.49 In addition, Bonferroni correction was performed to avoid compromising the statistical accuracy due to excessive correlations (P < 0.05).
Results
Baseline Characteristics
The baseline characteristics of the study population are summarized in Table 2. The COPD group showed mean FEV1 of 49.5% and reported their symptoms as mMRC scale 1.73 and CAT score 16.3, indicating they were in the moderate stage of disease. The mean treatment duration was 70.3 months.
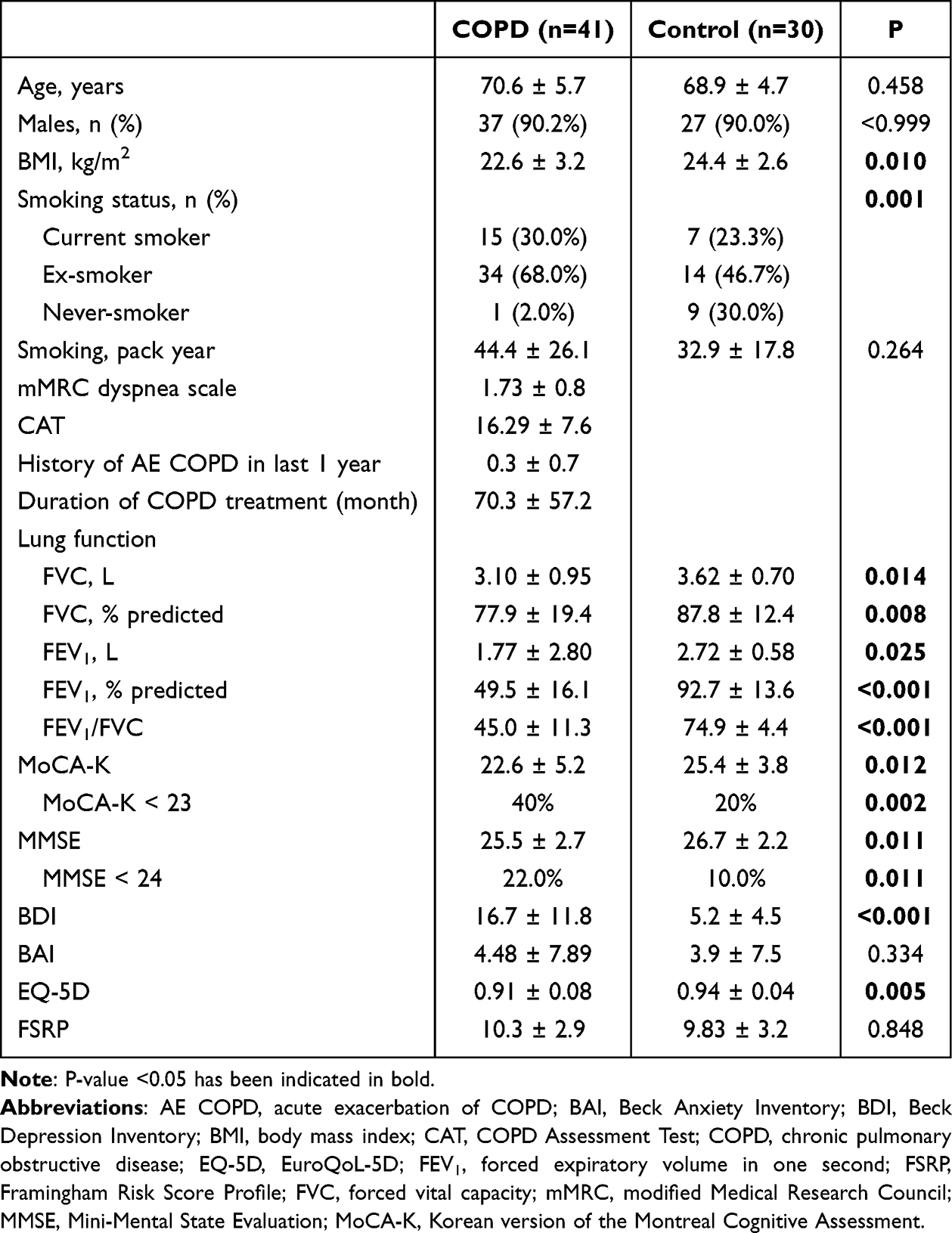 |
Table 2 Baseline Characteristics of the Subjects in Both Groups |
As described in Table 2, there were no significant differences in sex (P > 0.999) and FSRP (P = 0.848) between the COPD and control groups. The COPD group exhibited a lower BMI (22.6 ± 3.2 vs 24.4 ± 2.6 kg/m2, P < 0.010) and significantly reduced lung function, with lower values for FVC, FEV1, and FEV1/FVC (P < 0.05 for all). In terms of cognitive function, the COPD group had lower scores on the MoCA-K (22.6 ± 5.2 vs 25.4 ± 3.8, P = 0.012) and MMSE (25.5 ± 2.7 vs 26.7 ± 2.2, P = 0.011) than the control group. The COPD group also had a higher BDI scores (16.7 ± 11.8 vs 5.2 ± 4.5, P < 0.001), but there was no statistically significant difference in BAI scores (4.5 ± 7.9 vs 3.9 ± 7.5, P = 0.334). Additionally, the COPD group reported a lower EQ-5D score, indicating lower quality of life (0.91 ± 0.08 vs 0.94 ± 0.04, P = 0.005).
Group Differences in RSFC Between the COPD and Control Groups
Of the 184 seed points, 14 showed significant differences between the COPD and control groups (PFWE < 0.05). Table 3 shows the target regions and peak z-values for each of the 14 seed points.
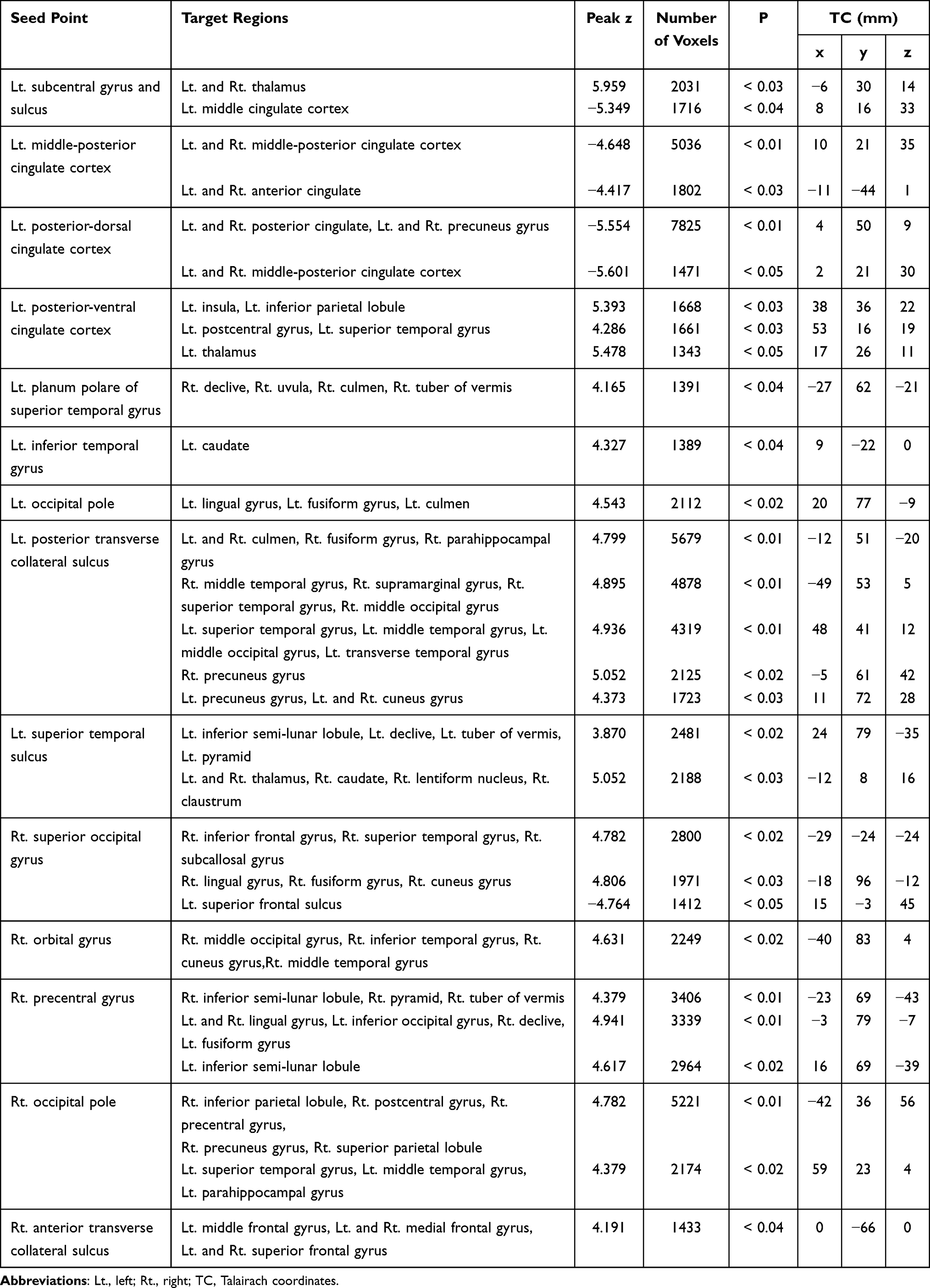 |
Table 3 Detailed Brain Regions and Values for the All Resting-State Functional Connectivity (RSFC) Maps With Group Differences |
Figure 1 illustrates the seven major seed points showing differences in RSFC with an uncorrected P-value < 0.05 between the COPD and control groups. Compared to controls, patients with COPD showed decreased RSFC for seed points in the left middle-posterior cingulate cortex (pMCC), left posterior-dorsal cingulate cortex (dPCC), and right superior occipital gyrus (SOG). In contrast, patients with COPD showed increased RSFC compared to controls in the left superior temporal sulcus, left posterior transverse collateral sulcus (ptCS), right occipital pole, and right precentral gyrus.
 |
Figure 1 Functional connectivity differences in COPD and healthy control groups. The green dots in the panel “Seed Keys” represent the seed regions for RSFC analyses, which are the left middle posterior cingulate cortex (A), left posterior cingulate cortex (B), right superior occipital gyrus (C), left superior temporal sulcus (D), left posterior transverse collateral sulcus (E), right occipital pol; (F), and right precentral gyrus (G). Panels A to G present the seed locations in the voxel space, as shown in the panel “Seed Keys”, and the significant group differences (FWE-corrected P<0.05) in their RSFC between patients with COPD and NC subjects. The clusters colored in cyan to dark blue are the target regions where the degrees of RSFC in the COPD group were lower than those in the NC group (COPD < NC), specifically the middle posterior cingulate cortex (A and B), and the left superior frontal sulcus (C). The clusters colored in yellow to red are regions where the COPD group had higher degrees of RSFC compared to the NC group (COPD > NC), specifically the right thalamus (D), right precuneus gyrus (E), left superior temporal gyrus (F), and left inferior semi-lunar lobule (G). Abbreviations: COPD, chronic obstructive pulmonary disease; NC, healthy control; RSFC, resting-state functional connectivity. |
For better understanding, we reorganized the increased or decreased FC in the patient group and the intra- or inter-hemispheric distributions of connectivity and compared them with the control group (Figure 2). Figure 2A illustrates the overall RSFC that was increased or decreased. Increased RSFC was found at 12 seed points in the patient group (Figure 2B). Decreases in RSFC, including in the cingulate cortex, were observed at four seed points (Figure 2C), and the decreased RSFC map was found in left intra-hemispheric connectivity (Figure 2D). The majority of RSFC changes were located in the temporal and occipital lobes, and increased RSFCs were only observed in right hemispheric connectivity (Figure 2E). In inter-hemispheric connectivity, increased or decreased RSFC changes were observed (Figure 2F).
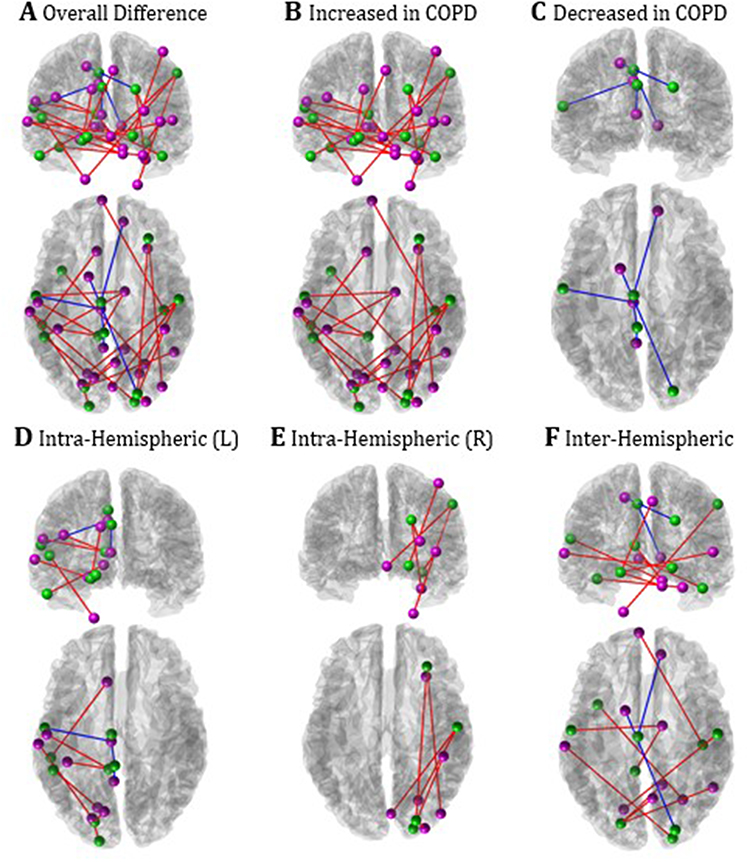 |
Figure 2 Spatial characteristics of group differences in RSFC between the COPD and control groups. Green dots indicate the centroids of the seed regions, and purple dots indicate those of the target regions showing the significant group difference between COPD and control groups. The blue lines show that the COPD group had lower RSFC between the seed point and target region than the control group. In contrast, the red lines indicate that the COPD group had a higher RSFC between the seed point and target region than the control group. For detailed explanations, please refer to the Results and Discussion sections of the main text. (A) Overall difference, (B) Increased RSFC in COPD, (C) Decreased RSFC in COPD, (D) RSFC changes in left intra-hemispheric area. (E) RSFC changes in right intra-hemispheric area. (F) RSFC changes in inter-hemispheric area. Abbreviations: COPD, chronic obstructive pulmonary disease; L, left; R, right; RSFC, resting-state functional connectivity. |
Correlation of Regional RSFC and Clinical Parameters
Figures 3, 4 and Table 4 demonstrate the correlations between RSFC and clinical parameters associated with COPD. The RSFCs of the right precentral gyrus (PrCG) and left inferior semi-lunar lobule (ISLL) (Figure 3A and C) were positively correlated with mMRC dyspnea scale (r = 0.5097, P = 0.0035)(Figure 4A) and CAT scores (r = 0.422, P = 0.03)(Figure 4C). The FC between the left superior frontal sulcus (SFS) and right superior occipital gyrus (SOG) (Figure 3B) negatively correlated with the MMSE score (r = −0.4615, P = 0.0155)(Figure 4B). The FC between the left ptCS and right precuneus gyrus (PreCG) (Figure 3C and E) exhibited a negative correlation with the CAT score (r = −0.422, P = 0.044) (Figure 4C) and showed positive correlations with FEV1% (r = 0.4774, P = 0.008) (Figure 4D) and FVC% (r = 0.5637, P = 0.0005) (Figure 4E). A similar trend was observed in the FC of the cingulate cortex. The FC between the left posterior cingulate cortex (PCC) and middle posterior cingulate cortex (pMCC) (Figure 3C) showed a negative correlation with the CAT score (r = −0.4263, P = 0.027) (Figure 4C), whereas the FC between the left posterior dorsal cingulate cortex (dPCC) and pMCC (Figure 3D) showed positive correlations with FEV1% (r = 0.4068, P = 0.0415) (Figure 4D) and FVC% (r = 0.4048, P = 0.0435) (Figure 4E). The FC between the left superior temporal sulcus (STS) and thalamus (THA) (r = −0.4371, P = 0.0215) (Figure 3E) and between the right occipital pole (OP) and left superior temporal gyrus (STG) (r = −0.4498, P = 0.016) (Figure 3E) were negatively correlated with FVC% (Figure 4E). No correlation was observed between RSFC and clinical parameters such as MoCA-K, mood assessments (BDI and BAI), or quality of life-related variable (EQ-5D) or cardiovascular risk factors(FSRP).
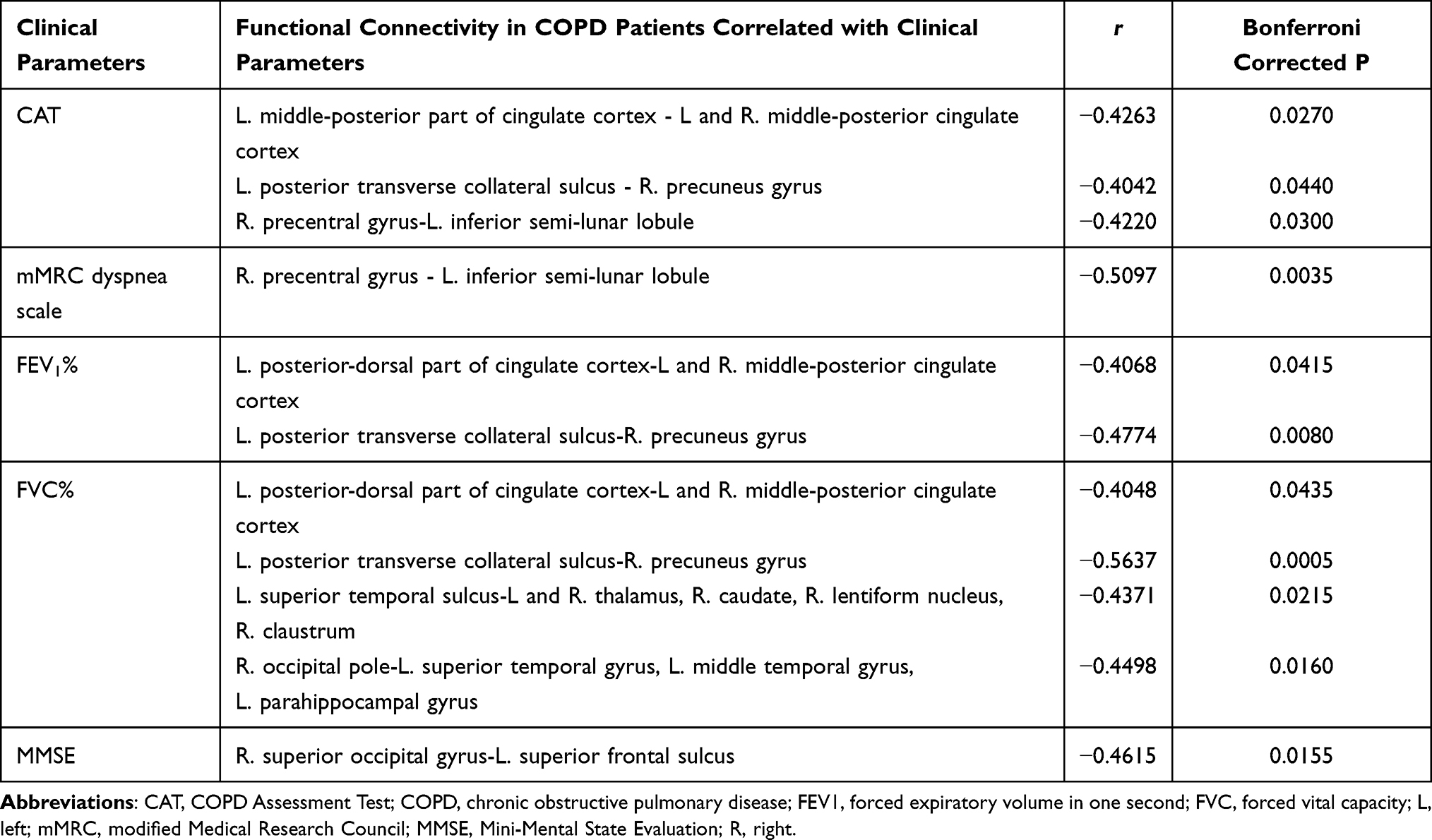 |
Table 4 Correlation of Functional Connectivity and Clinical Parameters in COPD Patients |
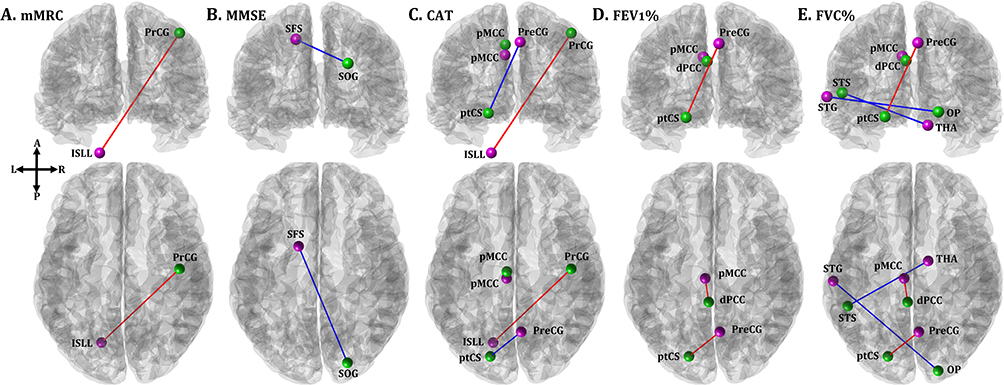 |
Figure 3 The RSFC maps showing high correlations between the RSFC and clinical scores in the COPD group. The panels (A–E) show the RSFC maps indicating high correlations (P<0.05) between the RSFC and clinical scores in the COPD group. The green dots indicate the positions of the seed points, whereas the purple dots indicate the target regions. The red lines represent positive correlations between each clinical score and RSFC, while the blue lines represent negative correlations. Abbreviations: CAT, COPD Assessment Test; COPD, chronic obstructive pulmonary disease; dPCC, posterior dorsal cingulate cortex; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; ISLL, inferior semi-lunar lobule; MMSE, Mini-Mental State Examination; mMRC, modified Medical Research Council dyspnea scale; OP, occipital pole; pMCC, middle posterior cingulate cortex; PrCG, precentral gyrus; PreCG, precuneus gyrus; ptCS, posterior transverse collateral sulcus; RSFC, resting-state functional connectivity; SFS, superior frontal sulcus; SOG, superior occipital gyrus; STG, superior temporal gyrus; STS, superior temporal gyrus; THA, thalamus. |
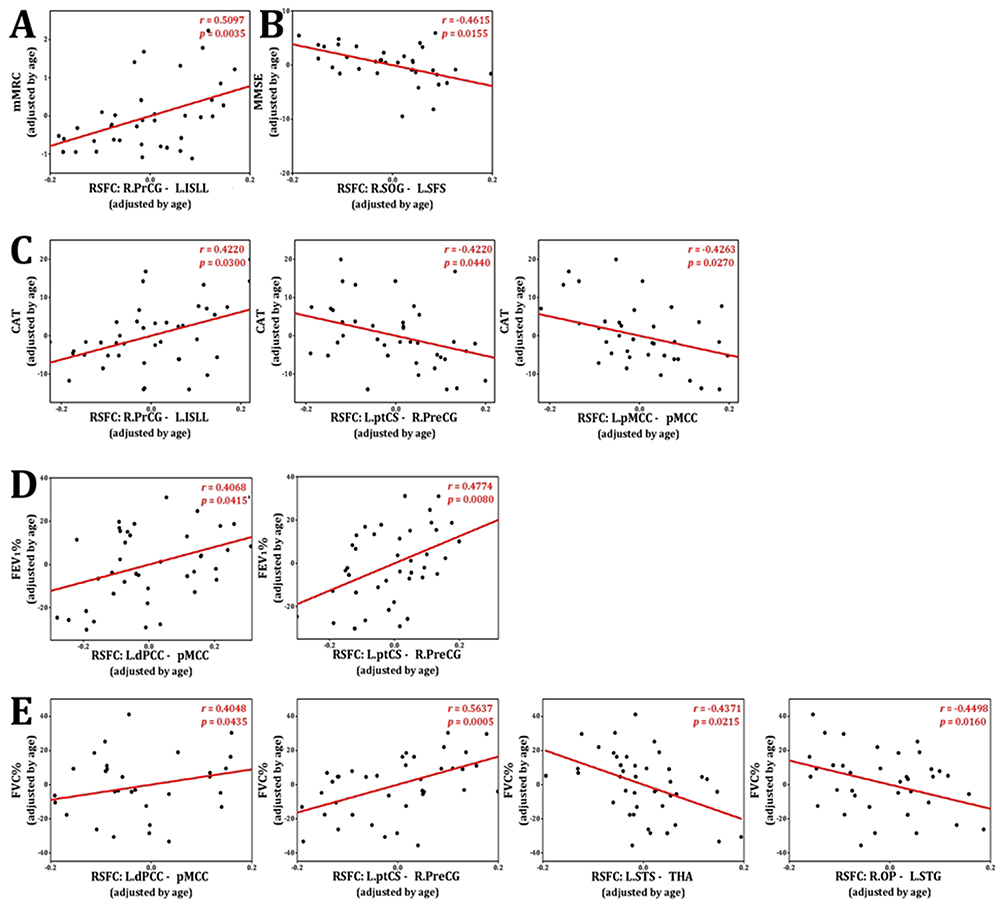 |
Figure 4 Correlations of RSFCs and clinical scores. (A) Correlation of modified Medical Research Council dyspnea scale (mMRC) and resting-state functional connectivity (RSFC) between right precentral gyrus (R.PrCS) and left inferior semi-lunar lobule (L.ISLL) (r = 0.5097, P = 0.0035); (B) Correlation of Mini-Mental State Evaluation (MMSE) and RSFC between right superior occipital gyrus (R.SOG) and left superior frontal gyrus (L.SFS) (r = −0.4615, P = 0.0155); (C) Correlation of COPD Assessment Test (CAT) and RSFC in three different regions (first panel, R.PrCS and L.ISLL (r = 0.4220, P = 0.03); second panel, left posterior transverse collateral sulcus (L.ptCS) and right precuneus gyrus (R.PreCG) (r = −0.4220, P = 0.044); and third panel, left middle posterior cingulate cortex (L.pMCC) and middle posterior cingulate cortex (pMCC) (r = −0.4263, P = 0.027); (D) Correlation of forced expiratory volume 1 (FEV1%) and RSFC in two different regions (first panel, left posterior dorsal cingulate gyrus (L.dPCC) and mPCC (r = 0.4068, P = 0.0415) and second panel, L.ptCS and R.PreCG (r= 0.4774, P = 0.008); (E) Correlation of forced vital capacity (FVC%) and RSFC in four different regions (first panel, left posterior dorsal cingulate gyrus (L.dPCC) and pMCC (r = 0.4048, P = 0.0435), second panel, L.ptCS and R.PreCG (r = 0.5637, P = 0.0005), third panel, left superior temporal sulcus (L.STS) and thalamus (THA) (r=−0.4371, P = 0.0215) and fourth panel, right occipital pole (R.OP) and left superior temporal gyrus (L.STG) (r = −0.4498, P = 0.0160). |
Discussion
In this study, we used RS-fMRI to measure RSFC in COPD patients without diagnosed cognitive impairment or depression and in healthy controls. We compared the RSFC between the two groups and examined the correlations between COPD-related clinical variables (such as lung function) and cognitive or mood indices with the RSFC in specific brain regions that differed from the control group. This study aimed to identify how COPD affects brain function by analyzing these differences and their correlations with major COPD-related clinical variables.
Several previous studies have assessed specific brain changes in COPD using brain MRI (Table 1). Wang et al assessed intrinsic brain activity in patients with COPD using the amplitude of the low-frequency fluctuation method, revealing lower cognitive function scores in patients than in healthy controls, along with abnormal intrinsic brain activity in the precuneus, PCC, and brainstem.50 Finnegan et al used task-induced fMRI to demonstrate that changes in cognition and emotion related to dyspnea experienced by patients with COPD induce alterations in brain activity in the anterior insula or emotional centers.25 Previous studies using various fMRI techniques to explore different brain regions in patients have identified significant changes; however, no consistent conclusions have been reached.
Compared to the control group, participants in the COPD group had a significant decrease in RSFC in the cingulate cortex (between the left PCC and pMCC, and the left dPCC and pMCC), which is associated with memory, self-awareness, and decision-making. The PCC is a key component of the default mode network (DMN), and abnormal activity in the DMN has been linked to the development and progression of mood disorders, including depression. This finding is consistent with prior research; Hu et al previously described reduced activity in six brain regions associated with the DMN, including the PCC and hippocampus, in patients with COPD.21 Furthermore, considering that the RSFC between the left dPCC and the pMCC decreases as FEV1% and also FVC% decrease, it is possible to suggest that the progression of COPD may influence specific brain FC and that this connection may be inversely related to the severity of the COPD.
A noteworthy observation in our study was that compared with the control group, the COPD group exhibited increased RSFC in the PrCG, which is involved in motor function. It is also interesting to note that there was a positive correlation between clinical parameters, such as the mMRC dyspnea scale and CAT scores, and the PrCG – ISLL RSFC, which differs from previous research. Yu et al reported a decrease in FC in the motor cortex at rest and during inspiratory loading in patients with COPD.18 In their study, seven key seed points were selected from the brain network associated with the respiratory muscles, including regions in the motor cortex, somatosensory cortex, brainstem, and cerebellum, to compare FC using RS-fMRI. Our study differs methodologically from the aforementioned study in that it analyzed a broader range of brain regions rather than being restricted to areas associated with specific functions. Although we cannot precisely explain the mechanism of the change in this region, we suspect that persistent and recurrent hyperventilation in response to airflow limitation in the patient could result in chronic hyperventilation, resulting in increased RSFC in the motor cortex.
FVC% was negatively correlated with the change in RSFC between the STG and OP, the main regions of the visual pathway. Xin et al analyzed regional homogeneity based on RS-fMRI in patients with COPD and healthy controls and found reduced regional homogeneity in brain areas associated with visual processing pathways in the patients. This suggests a potential link between the pathophysiological mechanisms of COPD and the brain’s visual processing pathways, which is consistent with the findings of related research.23
Esser et al reported that the anticipation of dyspnea increases activation in emotion-related brain areas in patients with moderate-to-severe COPD, as observed using fMRI. However, our study did not find correlations between RSFC and mood assessments such as BDI and BAI. Further research is needed to clarify the correlation between COPD and the brain areas related to emotion processing.20
Our study had several limitations. First, the interpretation of FC between seed and target regions is not straightforward. Many aspects of the functioning of specific areas of the brain remain unclear, and a statistically significant difference in RSFC may not fully explain the significance of that connection in the broader functional context. Second, our study was cross-sectional; therefore, it cannot capture changes in RSFC over the prolonged course of COPD progression. The causal factors through which COPD impairs cognitive function and affects emotions are not well established.
Despite these limitations, our study has significant value in complementing existing research on brain structural changes in COPD patients with cognitive impairment. Specifically, while other studies have focused on analyzing FC in brain regions with significant structural changes identified through previous research or morphometry, our study provides a comprehensive analysis of the entire brain. Additionally, while our study confirmed some similarities in FC changes found in previous research, it also presented the unique finding of increased RSFC in the PrCG, highlighting the need for further research in this area. Furthermore, certain areas such as the connection between the right SOG and left SFS, which showed a negative correlation with the MMSE score, require further validation through subsequent studies.
Conclusions
In summary, we investigated the FC in the brains of patients with COPD and compared them with healthy controls. Many statistically significant differences were found in specific brain regions, including those in the cingulate cortex and precentral gyrus, and also showed a significant correlation with clinical parameters, including respiratory symptoms and lung function. Further research is required to support this theoretical background, and this study may offer significant help to better understand the relationship between COPD and brain function.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval Statement
This study followed the principles outlined in the Declaration of Helsinki and was conducted with the approval of the Institutional Review Board of the Hanyang University Guri Hospital (IRB No: GURI 2015-05-019).
Patient Consent Statement
All participants provided informed consent.
Permission to Reproduce Material from Other Sources
An unauthorized version of the Korean MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Clinical Trial Registration
This clinical trial was not registered in a clinical trial registry.
Funding
HJJ and JHB were supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2022R1A2C1092667), and the Intramural Research Grant of Hanyang University (No. 202200000003365).
Disclosure
The authors declare that they have no relevant conflicts of interest for this study.
References
1. Halpin DMG, Criner GJ, Papi A. et al. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease. The 2020 GOLD science committee report on COVID-19 and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2021;203(1):24–36. doi:10.1164/rccm.202009-3533SO
2. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
3. Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2163–2196. doi:10.1016/S0140-6736(12)61729-2
4. Siraj RA. Comorbid Cognitive Impairment in Chronic Obstructive Pulmonary Disease (COPD): current understanding, risk factors, implications for clinical practice, and suggested interventions. Medicina. 2023;59(4). doi:10.3390/medicina59040732
5. Hansen KK, Hilberg O, Jensen HI, Løkke A, Farver-Vestergaard I. The association between cognitive functions and psychological factors in patients with severe COPD. Int J Chron Obstruct Pulmon Dis. 2023;18:2065–2078. doi:10.2147/COPD.S426897
6. De Luca SN, Chan SMH, Dobric A, et al. Cigarette smoke-induced pulmonary impairment is associated with social recognition memory impairments and alterations in microglial profiles within the suprachiasmatic nucleus of the hypothalamus. Brain Behav Immun. 2023;109:292–307. doi:10.1016/j.bbi.2023.02.005
7. Chang SS, Chen S, McAvay GJ, Tinetti ME. Effect of coexisting chronic obstructive pulmonary disease and cognitive impairment on health outcomes in older adults. J Am Geriatr Soc. 2012;60(10):1839–1846. doi:10.1111/j.1532-5415.2012.04171.x
8. Andrianopoulos V, Gloeckl R, Vogiatzis I, Kenn K. Cognitive impairment in COPD: should cognitive evaluation be part of respiratory assessment? Breathe. 2017;13(1):e1–e9. doi:10.1183/20734735.001417
9. Dodd JW, Getov SV, Jones PW. Cognitive function in COPD. Eur Respir J. 2010;35(4):913–922. doi:10.1183/09031936.00125109
10. Ortapamuk H, Naldoken S. Brain perfusion abnormalities in chronic obstructive pulmonary disease: comparison with cognitive impairment. Ann Nucl Med. 2006;20(2):99–106. doi:10.1007/BF02985621
11. Grant I, Prigatano GP, Heaton RK, McSweeny AJ, Wright EC, Adams KM. Progressive neuropsychologic impairment and hypoxemia. Relationship in chronic obstructive pulmonary disease. Arch Gen Psychiatry. 1987;44(11):999–1006. doi:10.1001/archpsyc.1987.01800230079013
12. Shim TS, Lee JH, Kim SY, et al. Cerebral metabolic abnormalities in COPD patients detected by localized proton magnetic resonance spectroscopy. Chest. 2001;120(5):1506–1513. doi:10.1378/chest.120.5.1506
13. Borson S, Scanlan J, Friedman S, et al. Modeling the impact of COPD on the brain. Int J Chron Obstruct Pulmon Dis. 2008;3(3):429–434. doi:10.2147/COPD.S2066
14. Akiyama M, Suzuki J, Nakamura Y, et al. Analysis of activation process of dyspnea sensation in CNS in patients with COPD measured by fMRI. Eur Respir J. 2011;38(Suppl 55):p4612.
15. Ryu CW, Jahng GH, Choi CW, et al. Microstructural change of the brain in chronic obstructive pulmonary disease: a voxel-based investigation by MRI. COPD. 2013;10(3):357–366. doi:10.3109/15412555.2012.752808
16. Herigstad M, Hayen A, Evans E, et al. Dyspnea-related cues engage the prefrontal cortex: evidence from functional brain imaging in COPD. Chest. 2015;148(4):953–961. doi:10.1378/chest.15-0416
17. Zhang J, Chen J, Yu Q, et al. Alteration of spontaneous brain activity in COPD patients. Int J Chron Obstruct Pulmon Dis. 2016;11:1713–1719. doi:10.2147/COPD.S110089
18. Yu L, De Mazancourt M, Hess A, et al. Functional connectivity and information flow of the respiratory neural network in chronic obstructive pulmonary disease. Hum Brain Mapp. 2016;37(8):2736–2754. doi:10.1002/hbm.23205
19. Esser RW, Stoeckel MC, Kirsten A, et al. Structural brain changes in patients with COPD. Chest. 2016;149(2):426–434. doi:10.1378/chest.15-0027
20. Esser RW, Stoeckel MC, Kirsten A, et al. Brain activation during perception and anticipation of dyspnea in chronic obstructive pulmonary disease. Front Physiol. 2017;8:617. doi:10.3389/fphys.2017.00617
21. Hu X, Wang H, Tu Y, et al. Alterations of the default mode network and cognitive impairments in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2018;13:519–528. doi:10.2147/COPD.S146870
22. Yin M, Wang H, Hu X, Li X, Fei G, Yu Y. Patterns of brain structural alteration in COPD with different levels of pulmonary function impairment and its association with cognitive deficits. BMC Pulm Med. 2019;19(1):203. doi:10.1186/s12890-019-0955-y
23. Xin H, Li H, Yu H, et al. Disrupted resting-state spontaneous neural activity in stable COPD. Int J Chron Obstruct Pulmon Dis. 2019;14:499–508. doi:10.2147/COPD.S190671
24. Li H, Xin H, Yu J, et al. Abnormal intrinsic functional hubs and connectivity in stable patients with COPD: a resting-state MRI study. Brain Imaging Behav. 2020;14(2):573–585. doi:10.1007/s11682-019-00130-7
25. Finnegan SL, Harrison OK, Harmer CJ, et al. Breathlessness in COPD: linking symptom clusters with brain activity. Eur Respir J. 2021;58(5):2004099. doi:10.1183/13993003.04099-2020
26. Peng Z, Zhang HT, Wang G, et al. Cerebral neurovascular alterations in stable chronic obstructive pulmonary disease: a preliminary fMRI study. PeerJ. 2022;10:e14249.
27. Finnegan SL, Browning M, Duff E, et al. Brain activity measured by functional brain imaging predicts breathlessness improvement during pulmonary rehabilitation. Thorax. 2023;78(9):852–859. doi:10.1136/thorax-2022-218754
28. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. doi:10.1136/thx.54.7.581
29. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
30. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
31. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
32. Kang YJS, Park KHY, Lee BC. “A reliability validity, and normative study of the Korean-Montreal Cognitive Assessment (K-MoCA) as an instrument for screening of vascular cognitive impairment (VCI)”. The Korean Journal of Clinical Psychology. 2009;28(2):549–562. doi:10.15842/kjcp.2009.28.2.013
33. Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53–72. doi:10.1016/0168-8510(96)00822-6
34. Fydrich T, Dowdall D, Chambless DL. Reliability and validity of the Beck Anxiety Inventory. Journal of Anxiety Disorders. 1992;6(1):55–61. doi:10.1016/0887-6185(92)90026-4
35. Richter P, Werner J, Heerlein A, Kraus A, Sauer H. On the validity of the Beck Depression Inventory: a review. Psychopathology. 1998;31(3):160–168. doi:10.1159/000066239
36. Kannel WB, McGee D, Gordon T. A general cardiovascular risk profile: the Framingham Study. Am j Cardiol. 1976;38(1):46–51. doi:10.1016/0002-9149(76)90061-8
37. Jones P, Harding G, Berry P, Wiklund I, Chen W, Leidy NK. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
38. Jo HJ, Reynolds RC, Gotts SJ, et al. Fast detection and reduction of local transient artifacts in resting-state fMRI. Comput Biol Med. 2020;120:103742. doi:10.1016/j.compbiomed.2020.103742
39. Cox RW. AFNI: software for analysis and visualization of functional magnetic resonance neuroimages. Comput Biomed Res. 1996;29(3):162–173. doi:10.1006/cbmr.1996.0014
40. Beall EB. Adaptive cyclic physiologic noise modeling and correction in functional MRI. J Neurosci Methods. 2010;187(2):216–228. doi:10.1016/j.jneumeth.2010.01.013
41. Shin W, Koenig KA, Lowe MJ. A comprehensive investigation of physiologic noise modeling in resting state fMRI; time shifted cardiac noise in EPI and its removal without external physiologic signal measures. Neuroimage. 2022;254:119136. doi:10.1016/j.neuroimage.2022.119136
42. Jo HJ, Saad ZS, Simmons WK, Milbury LA, Cox RW. Mapping sources of correlation in resting state FMRI, with artifact detection and removal. Neuroimage. 2010;52(2):571–582. doi:10.1016/j.neuroimage.2010.04.246
43. Jo HJ, Gotts SJ, Reynolds RC, et al. Effective preprocessing procedures virtually eliminate distance-dependent motion artifacts in resting state FMRI. J Appl Math. 2013;2013:1–9. doi:10.1155/2013/935154
44. Gotts SJ, Jo HJ, Wallace GL, Saad ZS, Cox RW, Martin A. Two distinct forms of functional lateralization in the human brain. Proc Natl Acad Sci U S A. 2013;110(36):E3435–44. doi:10.1073/pnas.1302581110
45. Holmes CJ, Hoge R, Collins L, Woods R, Toga AW, Evans AC. Enhancement of MR images using registration for signal averaging. J Comput Assist Tomogr. 1998;22(2):324–333. doi:10.1097/00004728-199803000-00032
46. Reynolds RC, Taylor PA, Glen DR. Quality control practices in FMRI analysis: philosophy, methods and examples using AFNI. Front Neurosci. 2022;16:1073800. doi:10.3389/fnins.2022.1073800
47. Fischl B, Salat DH, Busa E, et al. Whole brain segmentation: automated labeling of neuroanatomical structures in the human brain. Neuron. 2002;33(3):341–355. doi:10.1016/S0896-6273(02)00569-X
48. Fischl B, van der Kouwe A, Destrieux C, et al. Automatically parcellating the human cerebral cortex. Cereb Cortex. 2004;14(1):11–22. doi:10.1093/cercor/bhg087
49. Varangis E, Habeck CG, Razlighi QR, Stern Y. The effect of aging on resting state connectivity of predefined networks in the brain. Front Aging Neurosci. 2019;11:234. doi:10.3389/fnagi.2019.00234
50. Wang W, Li H, Peng D, et al. Abnormal intrinsic brain activities in stable patients with COPD: a resting-state functional MRI study. Neuropsychiatr Dis Treat. 2018;14:2763–2772. doi:10.2147/NDT.S180325
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.