Back to Journals » International Journal of General Medicine » Volume 18
A Visualized Nomogram to Predict the Risk of Acute Ischemic Stroke Among Patients With Cervical Artery Dissection
Authors Li C, Guan J ![]() , Zhao Q
, Zhao Q ![]() , Li J
, Li J ![]() , Wang Y, Zhao K
, Wang Y, Zhao K
Received 3 December 2024
Accepted for publication 4 March 2025
Published 19 March 2025 Volume 2025:18 Pages 1569—1580
DOI https://doi.org/10.2147/IJGM.S507043
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Changyu Li, Jincheng Guan, Qingshi Zhao, Jiahua Li, Yuying Wang, Kui Zhao
Department of Neurology, People’s Hospital of Longhua, Shenzhen, People’s Republic of China
Correspondence: Jincheng Guan, Department of Neurology, People’s Hospital of Longhua, 38 Jinglong Construction Road, Shenzhen, 518109, People’s Republic of China, Email [email protected]
Background: Acute ischemic stroke (AIS) is a significant global health concern, with cervical artery dissection (CAD) being a notable yet frequently overlooked cause, particularly in young adults. Despite advancements in imaging technologies, there remains a deficiency in effective methodologies for the prompt identification of AIS attributable to CAD. This research aims to create a predictive model combining clinical, imaging, and laboratory data to improve risk stratification and guide timely interventions.
Methods: Between 2019 and 2024, patients diagnosed with CAD were enrolled in the study. Nomogram models were constructed utilizing a two-step methodological approach. Initially, the least absolute shrinkage and selection operator (LASSO) regression analysis was utilized to improve variable selection. Subsequently, logistic regression analysis was conducted to develop an estimation model using the significant indicators identified by the LASSO. The model’s accuracy was evaluated using the application of receiver operating characteristic (ROC) curves, calibration curves, decision curve analyses, and clinical impact curves. The model underwent internal validation through bootstrap resampling with 1,000 iterations.
Results: In the cohort of 102 patients, 75 individuals with CAD experienced had an acute ischemic stroke. This cohort was characterized by a significantly older median age (42 years vs 51 years, p=0.041) and a comparable proportion of males (78.7% vs 74.1%,p=0.825). The analysis identified hyperlipidemia (aOR=0.19, 95% CI=0.040– 0.893, p=0.036), lumen occlusion (aOR=5.41, 95% CI=1.236– 23.648, p=0.025), a lower lymphocyte-to-monocyte ratio (LMR) (aOR=0.68, 95% CI=0.476– 0.797, p=0.038), and higher systemic immune-inflammation index (SII) (aOR=1.01, 95% CI=1.001– 1.016, p=0.026) are independent factors linked to ischemic stroke in CAD patients. The predictive model showed strong performance with an AUC of 0.870 (95% CI=0.789– 0.950) under the ROC curve. Decision curve analysis (DCA) indicated that the constructed nomogram was clinically applicable, with a risk threshold ranging from 9% to 95%.
Conclusion: This study developed a dynamic and visualized nomogram model for the precise prediction of stroke risk in patients with CAD, exhibiting robust performance, calibration, and clinical utility. Future multi-center studies are anticipated to further substantiate its clinical applicability.
Keywords: cervical artery dissection, acute ischemic stroke, nomogram model, predictive model
Introduction
AIS is a significant neurological disorder that continues to be a major global health concern due to its high rates of morbidity and mortality. CAD is a critical and frequently underestimated etiology of AIS. CAD involves the compromise of the structural integrity of the cervical or intracranial arterial wall, allowing blood to penetrate between the medial layers, potentially resulting in luminal narrowing or occlusion.1 CAD has emerged as one of the predominant causes of AIS in young adults,2,3 accounting for approximately 20% of acute ischemic strokes in individuals aged 18 to 45 years.4
CAD primarily encompasses internal cervical artery dissection (ICAD) and vertebral artery dissection (VAD), with annual incidence rates of approximately 2.5 to 3 per 100,000 for ICAD and 1 to 1.5 per 100,000 for VAD.5 The incidence of stroke resulting from CAD is approximately 1.2 per 100,000 individuals.6 Although advancements in imaging techniques have enhanced the detection rate and diagnostic precision of CAD, there remains a deficiency in rapid and effective methods for identifying acute ischemic stroke (AIS) attributable to CAD and for facilitating risk stratification.7 This study aims to create a reliable predictive model to evaluate AIS risk in CAD patients. By thoroughly integrating patients’ clinical characteristics, imaging findings, medical history, laboratory test results, and additional relevant factors, the study aims to establish a comprehensive and precise model. This model is intended to assist clinicians in promptly identifying high-risk patients and implementing effective interventions.
Materials and Methods
Patient Selection
Patients diagnosed with CAD and admitted to Shenzhen Longhua District People’s Hospital from 2019 to 2024 were enrolled.CAD was initially diagnosed via computed tomography angiography (CTA) and confirmed using digital subtraction angiography (DSA) or high-resolution magnetic resonance imaging (HR-MRI). Confirmed CAD was diagnosed based on imaging criteria, which required the presence of at least one of the following indicators:8(a) DSA showing intimal flaps or double lumen signs. Magnetic resonance angiography (MRA) and magnetic resonance imaging (MRI) can identify intimal flaps or double lumen signs.Skilled clinicians are able to identify these features clearly on ultrasound or CTA.Thickened vascular intima and atherosclerotic plaque formation were excluded,9 and all AIS cases were confirmed via MRI. The link between CAD and AIS was confirmed, with HR-MRI or CTA imaging identifying the dissected artery as the sole vessel responsible for AIS.The diagnostic criteria for ischemic stroke associated with CAD are as follows:8 (1) Acute onset of symptoms. (2) Presence of focal neurological deficits, such as unilateral facial or limb weakness or numbness, and speech disorders, with some cases presenting comprehensive neurological deficits. (3) The duration of symptoms and signs is not limited (when imaging shows a responsible lesion) or it lasts for more than 24 h (when a responsible lesion is absent). (4) Exclusion of non-vascular etiologies. (5) Head CT or MRI ruling out cerebral hemorrhage. (6) The ischemic stroke is linked to the presence of CAD.
Furthermore, cardiogenic stroke was ruled out in all patients through comprehensive cardiac assessments. The diagnoses of AIS and CAD were evaluated by two seasoned neurologists and radiologists.Patients were categorized into ischemic stroke and non-ischemic stroke cohorts based on the occurrence of a stroke. Data were extracted from electronic medical records and management databases aimed at quality improvement. The Ethics Committee of Shenzhen Longhua District People’s Hospital approved the study.
Data Collection
We gathered demographic and clinical data from patients, encompassing variables such as age, gender, and medical history, which includes conditions such as hypertension, diabetes mellitus, prior incidents of stroke or transient ischemic attack (TIA), hyperlipidemia, trauma, and head or neck pain. Additionally, we collected information on lifestyle factors, specifically smoking and alcohol consumption habits.
The laboratory data collected comprised baseline systolic (SBP) and diastolic blood pressure (DBP), fasting blood glucose levels at the time of admission, and counts of white blood cells (WBC), neutrophils (N), lymphocytes (L), monocytes (M), and platelets (PLT). Additionally, levels of C-reactive protein (CRP), D-dimer, hemoglobin A1c (HbA1c), total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), uric acid (UA), creatinine (Cr), and homocysteine (Hcy) were measured. The neutrophil-to-lymphocyte ratio (NLR) was determined by dividing the neutrophil count by the lymphocyte count.The lymphocyte-to-monocyte ratio (LMR) was determined by dividing the lymphocyte count by the monocyte count. Similarly, the platelet-to-lymphocyte ratio (PLR) was calculated by dividing the platelet count by the lymphocyte count.10 The systemic inflammation response index (SIRI) and the systemic immune-inflammation index (SII) were defined as follows: SIRI is calculated as the product of neutrophil and monocyte counts divided by lymphocyte counts, and SII is calculated as the product of platelet and neutrophil counts divided by lymphocyte counts.11,12
Statistical Analysis
Statistical analyses were performed using SPSS version 26.0 (IBM Corporation, Armonk, NY, USA) and R software version 4.2.0. A clinical comparison was conducted between cohorts of patients with ischemic stroke and those without, with the normality of continuous variables assessed via the Shapiro–Wilk test. For data exhibiting normal distribution, the t-test was employed, and results were expressed as mean ± standard deviation (SD). For data not conforming to a normal distribution, the Mann–Whitney U-test was utilized, with results reported as median and interquartile range (IQR).Categorical information was analyzed using either Pearson’s chi-squared test or Fisher’s exact test. Missing data were imputed using the missForest algorithm.
Construction and Evaluation of Models
The least absolute shrinkage and selection operator (LASSO) regression analysis serves as a method for both shrinkage and variable selection within linear regression models. By imposing constraints on model parameters, LASSO analysis minimizes estimation inaccuracies for a specified quantitative response. This approach results in certain regression coefficients (RCs) being reduced to zero, thereby excluding the corresponding variables from the model. Conversely, variables with RCs greater than zero are retained, indicating a strong association with the response variable. Subsequently, employing a −2log-likelihood approach and a binomial family, the LASSO method performs a 10-fold K cross-validation to centralize and normalize pertinent variables before selecting those with optimal lambda values. The multicollinearity among variable combinations was assessed using variance inflation factors and the condition index. Variables deemed significant in the LASSO analysis were utilized to conduct a univariate logistic regression analysis. Variables exhibiting a P-value of less than 0.05 in the univariate logistic regression analysis were then incorporated into the multivariate logistic regression analysis.13 A multivariate logistic regression analysis was conducted to identify independent factors associated with ischemic stroke in patients with CAD. Odds ratios (OR) with 95% confidence intervals (CI) were calculated for each endpoint to provide estimates. Subsequently, significant indicators identified from the analysis were utilized for the construction of a nomogram. Each variable included in the nomogram was assigned a weighted score, and the cumulative score of all variables was used to evaluate the risk of ischemic stroke in patients with CAD. This evaluation was based on a function relating the total score to the probability of the outcome. Ultimately, a conventional nomogram was developed using the “rms” package in R. The receiver operating characteristic (ROC) curves were utilized to assess the predictive accuracy of the model. To investigate the concordance between observed events and predicted outcomes, a calibration curve was constructed. Internal validation of the model was conducted using bootstrap resampling with 1,000 iterations. Decision curve analysis (DCA) was applied to quantify the net benefit across a range of threshold probabilities, thereby further evaluating the utility of the aforementioned nomograms.14,15 Additionally, the Clinical Impact Curve (CIC) was employed to appraise the clinical applicability of the prediction model. Finally, the “DynNom” package in R was utilized to construct dynamic nomogram models for predicting the risk of ischemic stroke in patients with CAD. Statistical significance was determined by a two-tailed P-value threshold of 0.05.
Result
Baseline Characteristics of Patients
The study enrolled 102 patients, who were then divided into non-ischemic and ischemic stroke cohorts. Of these patients, 73.2% were allocated to the ischemic stroke group. This cohort was characterized by a significantly older median age (42 years vs 51 years, p=0.041) and a lower prevalence of hyperlipidemia (8.0% vs 25.9%, p=0.04). Regarding imaging characteristics, patients in the ischemic stroke cohort demonstrated a higher incidence of lumen occlusions (37.3% vs 11.1%, p=0.022) and a lower incidence of dissecting aneurysms (6.7% vs 40.7%, p<0.001). Laboratory analysis revealed that ischemic stroke patients had significantly elevated median white blood cell (8.81 vs 6.23, p=0.010) and neutrophil counts (5.84 vs 3.87, p=0.007) compared to non-ischemic stroke patients.Lymphocyte counts were notably reduced in the ischemic stroke group compared to the control group (median 1.32 vs 1.87, p=0.001).Furthermore, the ischemic stroke cohort exhibited elevated median values of the NLR (4.46 vs 2.14, p<0.001) and PLR (167.84 vs 119.51, p=0.006), alongside reduced LMR values (2.60 vs 4.28, p<0.001), relative to the non-ischemic stroke cohort.Simultaneously, the SIRI (median 2.81 vs 0.18, p<0.001) and the SII (median 1215.88 vs 366.30, p<0.001), both indicators of inflammatory response, exhibited significantly elevated levels in the ischemic stroke cohort, as presented in Table 1.
 |
Table 1 A Comparative Analysis of the Characteristics Between the Non-Ischemic Stroke Cohort and the Ischemic Stroke Cohort |
Prediction Model Development
According to the positivity rate of our data, we selected lambda. min for analysis. Using lambda. min =0.054, we filtered the following variables, namely, age, hyperlipidemia, history of head and neck pain, lumen occlusion, intraluminal thrombus, baseline DBP, lymphocytes, LMR, SII (Figure 1). We conducted an analysis of 41 variables related to AIS employing the LASSO method. The analysis utilized lambda. min = 0.054 [log (lambda. min) = −1.286] and lambda.1se = 0.138 [log(lambda.1se) = −0.860]. Based on the positivity rate of our dataset, we opted for lambda. min for further analysis. Utilizing lambda. min = 0.054, we identified and retained the following variables: age, hyperlipidemia, history of head and neck pain, lumen occlusion, intraluminal thrombus, baseline DBP, lymphocyte count, LMR, and SII, as illustrated in Figure 1.
 |
Figure 1 Variable selection by the LASSO binary logistic regression model. (A) coefficients profile plot was constructed against the log(lambda) sequence. Nine variables with nonzero coefficients were selected by deriving the optimal lambda. (B) Following verification of the optimal parameter (lambda) in the LASSO model, we plotted the partial likelihood deviance (binomial deviance) curve versus log(lambda) and drew dotted vertical lines based on 1 standard error criteria. |
Univariable and Multivariable Logistic Regression Analyses for Futile Recanalization
Table 2 presents the results of univariable and multivariable logistic regression analyses aimed at identifying independent factors associated with ischemic stroke in patients with CAD. The analysis revealed that hyperlipidemia (aOR = 0.19, 95% CI]= 0.040–0.893, p = 0.036), lumen occlusion (aOR = 5.41, 95% CI = 1.236–23.648, p = 0.025), lower LMR (aOR = 0.68, 95% CI = 0.476–0.797, p = 0.038), and higher SII (aOR = 1.01, 95% CI = 1.001–1.016, p = 0.026) were independently associated with ischemic stroke in the context of CAD (Table 2). The multivariate logistic regression model demonstrated an absence of collinearity issues, as evidenced by variance inflation factors ranging from 1.021 to 1.490 (Table 3).
 |
Table 2 Univariate and Multivariate Logistic Regression Analysis for Ischemic Stroke With CAD |
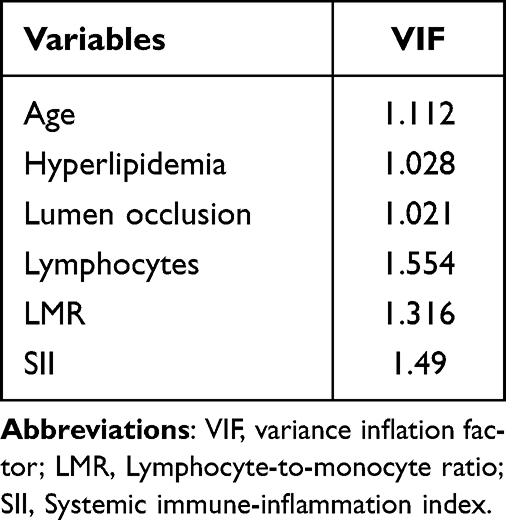 |
Table 3 Multicollinearity Assessment |
Predictive Model Construction
A predictive nomogram model was developed utilizing the previously mentioned stand-alone ischemic stroke indicators (Figure 2). Furthermore, a dynamic nomograph was constructed based on a network platform to enhance accessibility for clinicians and researchers. This tool is available online at https://ais-with-cad.shinyapps.io/DynNomapp/. By inputting individual patient variables on the website, clinicians and researchers can efficiently determine the risk of AIS in patients with CAD.
 |
Figure 2 Development of a novel nomogram for predicting the individual risk of AIS among patients with CAD via a multivariate logistic regression analysis. |
Prediction Model Assessment and Validation
The analysis of the ROC curve for the predictive model demonstrated an AUC of 0.870, with a 95% CI ranging from 0.789 to 0.950. The model exhibited a sensitivity of 90.7% and a specificity of 74.1% (Figure 3A). Internal validation was conducted using bootstrap resampling performed 1,000 times, resulting in an AUC of 0.860 (95% CI: 0.755−0.936) (Figure 3B).
 |
Figure 3 ROC curve of the prediction model(A) and the ROC of the internal validation of the prediction model(B). |
The calibration curve of the prediction model closely aligned with the ideal diagonal line, indicating strong concordance between the estimated and actual values. The model demonstrated a mean squared error of 0.032 (refer to Figure 4A). Internal validation was conducted using bootstrap resampling with 1000 iterations, resulting in a mean squared error of 0.044 (Figure 4B).
 |
Figure 4 Calibration curves of the prediction model(A) and the calibration curves of the internal validation of the prediction model(B). |
The DCA of the model indicates that, for risk thresholds ranging from 9% to 95%, the decision curve surpasses both the “none” and “all” lines. This suggests that the model yields a higher net benefit compared to extreme cases across a broad threshold range, thereby demonstrating clinical utility within this interval (Figure 5A). The clinical impact curve demonstrated that when the risk threshold exceeded 70%, the number of subjects closely corresponded to the number of individuals classified as high risk (ie, the true positive cases) (refer to Figure 5B). These findings collectively suggest that the prediction model developed in this study exhibits substantial clinical utility.
 |
Figure 5 DCA (A) and the clinical impact curve (B)of the prediction model. |
Discussion
In this study, we developed and validated a predictive nomogram that incorporates demographic, clinical, and laboratory data to assess the individualized risk of stroke in patients with CAD. To address the common issues of overfitting and skewed indicator distributions associated with traditional logistic regression analysis, we employed LASSO regression to evaluate potential associated variables. We conducted a further evaluation of the estimated results by refining the regression coefficients through the application of the LASSO technique. Subsequently, we employed multivariate analysis to identify independent predictors, which facilitated the development of a nomogram. In addition, we developed a visualized nomogram that allows every clinical worker to easily assess the risk of AIS in patients with CAD (Figure 6).
 |
Figure 6 The example diagram of the visualized nomogram model. |
A nomogram serves as a robust and practical tool for estimation, generating probabilities of various clinical events by integrating diverse prognostic and determinant data, and evaluating individual risk through the amalgamation of multiple significant event indicators.16 Nomograms are a critical resource for synthesizing biological and clinical findings, playing a pivotal role in the advancement of personalized therapy. Additionally, they feature an intuitive digital interface that enhances prognosis prediction and supports clinical decision-making.13
The constructed nomogram model incorporated four variables: hyperlipidemia, lumen occlusion, LMR, and SII. The model demonstrated strong discriminative capacity, accurate calibration, and significant clinical utility.
Our study unexpectedly discovered that patients with CAD who had a history of hyperlipidemia exhibited a reduced risk of developing stroke. The protective mechanism of hyperlipidemia in patients with CAD against stroke is not fully understood. However, existing literature suggests several potential factors. Firstly, the role of lipids in vascular wall repair: hyperlipidemia may contribute to the repair of damaged arterial walls by increasing blood cholesterol and lipoprotein levels, thereby providing essential materials for arterial wall repair.For instance, cholesterol may play a role in the repair of endothelial cells, thereby mitigating endothelial dysfunction and consequently decreasing the likelihood of thrombosis. Some studies have suggested that elevated cholesterol levels might lower the risk of further extension or rupture of arterial dissection by enhancing the stability of the vessel wall. Furthermore, individuals with obesity may possess a greater ability to withstand external impacts to the neck, whereas those with lower body mass may exhibit increased vulnerability of the cervical blood vessels; however, a comprehensive etiological analysis is lacking. Finally, patients diagnosed with hyperlipidemia are typically managed with statin therapy, which possesses anti-inflammatory and antioxidant properties and enhances endothelial function. The administration of statins may indirectly mitigate the risk of stroke in individuals with CAD. While hyperlipidemia might, in certain instances, confer a protective effect against the incidence of dissection stroke, it should not be misconstrued as a protective factor. For individuals at risk of developing hyperlipidemia, it is advisable to regulate blood lipid levels through appropriate dietary and lifestyle modifications to minimize potential health risks.
This study demonstrated that patients with CAD exhibiting lumen occlusion are at an increased risk for AIS, indicating that lumen occlusion is a significant risk factor for poor prognosis in CAD patients.17 The development of a mural hematoma and the subsequent enlargement of the dissected arterial lumen occlusion adversely affect local hemodynamics, leading to impaired blood flow dynamics. These changes result in extended arterial dissection segments, substantial energy loss in blood flow, reduced blood flow velocity, and a state of low shear force. Such conditions facilitate secondary thrombosis and exacerbate lumen stenosis, thereby perpetuating a detrimental cycle of ischemia in distal brain tissues.18 Consequently, the administration of antithrombotic therapy in patients with vascular occlusion due to CAD may be beneficial in preventing AIS.
Our study unexpectedly identified that the association between the LMR and the SII in peripheral blood samples, and ischemic stroke in patients with CAD, has been previously documented in a limited number of relevant articles both domestically and internationally. These specific and rapidly measurable biomarkers have the potential to enhance the diagnostic accuracy for AIS attributable to CAD. Inflammation plays a crucial role in the development of CAD and stroke,19–21 with white blood cells such as neutrophils, lymphocytes, and monocytes influencing the inflammatory response in diverse ways.22–24 Neutrophils trigger inflammation by releasing mediators that contribute to brain injury, while monocytes worsen inflammation and thrombosis through interactions with platelets and endothelial cells.25 Conversely, lymphocytes exhibit a suppressive effect on inflammation.7,26 The lymphocyte-to-monocyte ratio (LMR) is a composite marker indicating the absolute counts of blood lymphocytes and monocytes, whereas the SII reflects the absolute counts of neutrophils, monocytes, and platelets in the blood.These cellular components could be pivotal in the development of AIS and CAD amid inflammatory processes.19,20
Previous research has identified inflammation as a contributing factor to the progression of AIS. Studies focusing on leukocytes have highlighted inflammatory markers, such as the NLR and the LMR, as being associated with patient prognosis in AIS.27,28 Specifically, a lower NLR and an elevated LMR are indicative of favorable clinical outcomes in AIS patients.29 Furthermore, LMR has been linked to poor prognosis across a range of malignancies, as well as cardiovascular and cerebrovascular diseases.22,30–33 Monocytes, distinct from lymphocytes, serve as crucial immune regulators and are implicated in secondary injury following an acute ischemic event.34
Previous retrospective studies have found that a higher proportion of monocytes after a stroke independently predicts poor prognosis at three months.The SII is a novel inflammatory marker providing a more comprehensive assessment of inflammation than NLR or LMR, as it simultaneously reflects three factors, unlike NLR and LMR, which consider only two.According to a previous study,35 it was demonstrated for the first time that both SIRI and SII are independently associated with ineffective recanalization in patients undergoing endovascular therapy.
However, this research has specific limitations.Firstly, it employs a retrospective design with a limited sample size derived from a single center, which may not adequately represent the broader patient population.The study heavily relies on the precision and comprehensiveness of the extracted data, introducing potential biases in selection. Secondly, this study’s cross-sectional design inherently limits causal inference and temporal assessment of risk factors. As both CAD severity and stroke diagnosis were evaluated during the same hospitalization, our model reflects disease co-occurrence rather than longitudinal prediction. Despite this limitation, we believe our predictive model offers valuable clinical insights and potential value:0.1.Early Stroke Recognition:For patients hospitalized with CAD who exhibit subtle/atypical stroke symptoms, the model could aid clinicians in prioritizing neurological evaluation and imaging. 2.Risk Stratification:Identifying CAD patients with concurrent stroke may guide acute management (eg, antithrombotic therapy optimization) and secondary prevention strategies. Future prospective studies with pre-CAD baseline data and post-discharge follow-up are needed to validate true predictive utility. In addition, the study focused solely on analyzing patient blood samples collected at admission, without examining changes in inflammatory markers over time.Future studies should evaluate how fluctuations in inflammatory markers influence stroke risk in CAD patients.Finally, our model currently lacks external validation.The dataset comprising patients with CAD was sourced exclusively from a single hospital.Despite demonstrating robust internal validation, the model’s validation was conducted using data from the same institution, rather than incorporating data from multiple centers.Consequently, the generalizability of the predictive model requires further assessment in patient populations from other institutions.
Conclusion
Our research showed that the dynamic visual nomogram model effectively predicts stroke risk in CAD patients.Moreover, our predictive model demonstrated good discriminative performance, enhanced calibration, and clinical benefits, which help choose clinical treatment methods.The increasing number of multi-center studies will facilitate the clinical application of our model.
Ethics Approval and Informed Consent
This study protocol was reviewed and approved by the Institutional Research Ethic Committee of Shenzhen Longhua District People’s Hospital, approval number [2024088-01]. All participants wrote informed consent. We followed the guidelines outlined in the Declaration of Helsinki.
Acknowledgments
We extend our gratitude to our research group at the Department of Neurology, Shenzhen Longhua District People’s Hospital, China, for their invaluable assistance and support in the conduct of this study.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Engelter ST, Traenka C, Lyrer P. Dissection of Cervical and Cerebral Arteries. Curr Neurol Neurosci Rep. 2017;17(8):59. doi:10.1007/s11910-017-0769-3
2. Blum CA, Yaghi S. cervical artery dissection: a review of the epidemiology, pathophysiology, treatment, and outcome. Arch Neurosci. 2015;2(4):e26670. doi:10.5812/archneurosci.26670
3. Debette S, Leys D. Cervical-artery dissections: predisposing factors, diagnosis, and outcome. Lancet Neurol. 2009;8(7):668–678. doi:10.1016/S1474-4422(09)70084-5
4. Ekker MS, Boot EM, Singhal AB, et al. Epidemiology, aetiology, and management of ischaemic stroke in young adults. Lancet Neurol. 2018;17(9):790–801. doi:10.1016/S1474-4422(18)30233-3
5. Keser Z, Meschia JF, Lanzino G. Craniocervical artery dissections: a concise review for clinicians. Mayo Clin Proc. 2022;97(4):777–783. doi:10.1016/j.mayocp.2022.02.007
6. Ranjbar M, Badihian N, Yazdi M, et al. “Incidence, characteristics and prognosis of cervical artery dissection-induced ischemic stroke in central Iran”. BMC Neurol. 2022;22(1):227. doi:10.1186/s12883-022-02754-7
7. Yang Y, Sun G, Diao S, et al. Diagnostic performances of neutrophil to lymphocyte ratio and lymphocyte to monocyte ratio in acute ischemic stroke caused by cervicocranial arterial dissection. J Clin Lab Analysis. 2020;34(12):e23515. doi:10.1002/jcla.23515
8. Mehdi E, Aralasmak A, Toprak H, et al. Craniocervical dissections: radiologic findings, pitfalls, mimicking diseases: a pictorial review. Curr Med Imaging Rev. 2018;14(2):207–222. doi:10.2174/1573405613666170403102235
9. Chen W-T, Chang F-C, Huang H-C, et al. Total and differential leukocyte counts in ischemic stroke caused by vertebrobasilar artery dissection. J Neurol Sci. 2019;404:101–105. doi:10.1016/j.jns.2019.07.022
10. Lecouffe NE, Kappelhof M, Treurniet KM, et al. A randomized trial of intravenous alteplase before endovascular treatment for stroke. N Engl J Med. 2021;385(20):1833–1844. doi:10.1056/NEJMoa2107727
11. Guan J, Wang Q, Hu J, et al. Nomogram-based prediction of the futile recanalization risk among acute ischemic stroke patients before and after endovascular therapy: a retrospective study. Neuropsychiatr Dis Treat. 2023;19:879–894. doi:10.2147/NDT.S400463
12. Zi W, Qiu Z, Li F, et al. Effect of endovascular treatment alone vs intravenous alteplase plus endovascular treatment on functional independence in patients with acute ischemic stroke. JAMA. 2021;325(3):234–243. doi:10.1001/jama.2020.23523
13. Yang P, Zhang Y, Zhang L, et al. Endovascular thrombectomy with or without intravenous alteplase in acute stroke. N Engl J Med. 2020;382(21):1981–1993. doi:10.1056/NEJMoa2001123
14. Bala F, Beland B, Mistry E, et al. Endovascular treatment of acute ischemic stroke in patients with pre-morbid disability: a meta-analysis. J Neurointerv Surg. 2023;15(4):343–349. doi:10.1136/neurintsurg-2021-018573
15. Zhao H, Bai X, Li W, et al. Influence of pre-stroke dependency on safety and efficacy of endovascular therapy: a systematic review and meta-analysis. Front Neurol. 2022;13:956958. doi:10.3389/fneur.2022.956958
16. Adams HP, Jr. BBH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. definitions for use in a multicenter clinical trial. TOAST. trial of org 10172 in acute stroke treatment. Stroke. 1993;24(1):35–41. doi:10.1161/01.STR.24.1.35
17. Traenka C, Grond-Ginsbach C, Goeggel SB, et al. Artery occlusion independently predicts unfavorable outcome in cervical artery dissection. Neurology. 2020;94(2):e170–e180. doi:10.1212/WNL.0000000000008654
18. Lyu Q, Tian X, Ding Y, et al. Evaluation of carotid plaque rupture and neovascularization by contrast-enhanced ultrasound imaging: an exploratory study based on histopathology. Transl Stroke Res. 2020;12(1):49–56. doi:10.1007/s12975-020-00825-w
19. Robertson JJ, Koyfman A. Cervical artery dissections: a review. J Emergency Med. 2016;51(5):508–518. doi:10.1016/j.jemermed.2015.10.044
20. Vidale S, Consoli A, Arnaboldi M, et al. Postischemic inflammation in acute stroke. J Clin Neurol. 2017;13(1):1–9. doi:10.3988/jcn.2017.13.1.1
21. Pelz JO, Harms K, Metze M, et al. Spontaneous cervical artery dissection is accompanied by a hypercoagulable state and simultaneous inflammatory condition. J Neurol. 2017;265(2):308–314. doi:10.1007/s00415-017-8696-4
22. Ren H, Liu X, Wang L, et al. Lymphocyte-to-monocyte ratio: a novel predictor of the prognosis of acute ischemic stroke. J Stroke Cerebrovasc Dis. 2017;26(11):2595–2602. doi:10.1016/j.jstrokecerebrovasdis.2017.06.019
23. Song Q, Pan R, Jin Y, et al. Lymphocyte-to-monocyte ratio and risk of hemorrhagic transformation in patients with acute ischemic stroke. Neurol Sci. 2020;41(9):2511–2520. doi:10.1007/s10072-020-04355-z
24. Herz J, Sabellek P, Lane TE, et al. Role of neutrophils in exacerbation of brain injury after focal cerebral ischemia in hyperlipidemic mice. Stroke. 2015;46(10):2916–2925. doi:10.1161/STROKEAHA.115.010620
25. Guan J, Wang Q, Zhao Q. Lymphocyte to monocyte ratio is independently associated with futile recanalization in acute ischemic stroke after endovascular therapy. Neuropsychiatr Dis Treat. 2023;19:2585–2596. doi:10.2147/NDT.S434225
26. Lux D, Alakbarzade V, Bridge L, et al. The association of neutrophil-lymphocyte ratio and lymphocyte-monocyte ratio with 3-month clinical outcome after mechanical thrombectomy following stroke. J Neuroinflammation. 2020;17(1):60. doi:10.1186/s12974-020-01739-y
27. Switonska M, Slomka A, Korbal P, et al. Association of neutrophil-to-lymphocyte ratio and lymphocyte-to-monocyte ratio with treatment modalities of acute ischaemic stroke: a pilot study. Medicina. 2019;55(7):342. doi:10.3390/medicina55070342
28. Park MG, Kim MK, Chae SH, et al. Lymphocyte-to-monocyte ratio on day 7 is associated with outcomes in acute ischemic stroke. Neurol Sci. 2018;39(2):243–249. doi:10.1007/s10072-017-3163-7
29. Wang L, Song Q, Wang C, et al. Neutrophil to lymphocyte ratio predicts poor outcomes after acute ischemic stroke: a cohort study and systematic review. J Neurol Sci. 2019;406:116445. doi:10.1016/j.jns.2019.116445
30. Qi H, Wang D, Deng X, et al. Lymphocyte-to-monocyte ratio is an independent predictor for neurological deterioration and 90-day mortality in spontaneous intracerebral hemorrhage. Med Sci Monit. 2018;24:9282–9291. doi:10.12659/MSM.911645
31. Zhu J-Y, Liu -C-C, Wang L, et al. Peripheral blood lymphocyte-to-monocyte ratio as a prognostic factor in advanced epithelial ovarian cancer: a multicenter retrospective study. J Cancer. 2017;8(5):737–743. doi:10.7150/jca.17668
32. Gong S, Gao X, Xu F, et al. Association of lymphocyte to monocyte ratio with severity of coronary artery disease. Medicine. 2018;97(43):e12813. doi:10.1097/MD.0000000000012813
33. Cananzi FCM, Minerva EM, Samà L. Preoperative monocyte‐to‐lymphocyte ratio predicts recurrence in gastrointestinal stromal tumors. J Surg Oncol. 2018;119(1):12–20. doi:10.1002/jso.25290
34. Lattanzi S, Norata D, Divani AA, et al. Systemic inflammatory response index and futile recanalization in patients with ischemic stroke undergoing endovascular treatment. Brain Sci. 2021;11(9):1164. doi:10.3390/brainsci11091164
35. Yi HJ, Sung JH, Lee DH. Systemic inflammation response index and systemic immune-inflammation index are associated with clinical outcomes in patients treated with mechanical thrombectomy for large artery occlusion. World Neurosurg. 2021;153:e282–e289. doi:10.1016/j.wneu.2021.06.113
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.