Back to Journals » International Journal of General Medicine » Volume 11
A video depicting resuscitation did not impact upon patients' decision-making
Authors Richardson-Royer C, Naqvi I, Riffel C, Harvey L, Smith D, Ayalew D, Motayar N, Amoateng-Adjepong Y, Manthous CA
Received 24 July 2017
Accepted for publication 18 October 2017
Published 12 February 2018 Volume 2018:11 Pages 73—77
DOI https://doi.org/10.2147/IJGM.S147109
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Supplementary video presented by Richardson-Royer et al
Views: 3162
Caitlin Richardson-Royer,1 Imran Naqvi,1 Christopher Riffel,1 Lawrence Harvey,1 Domonique Smith,1 Dagmawe Ayalew,1 Nasim Motayar,1 Yaw Amoateng-Adjepong,1,2 Constantine A Manthous3
1The Jewish Hospital of Cincinnati, Cincinnati, OH, USA; 2Yale University School of Medicine, New Haven, CT, USA; 3Lawrence & Memorial Hospital, New London, CT, USA
Background: Previous studies have demonstrated that video of and scripted information about cardiopulmonary resuscitation (CPR) can be deployed during clinician–patient end-of-life discussions. Few studies, however, examine whether video adds to verbal information-sharing. We hypothesized that video augments script-only decision-making.
Methods: Patients aged >65 years admitted to hospital wards were randomized to receive evidence-based information (“script”) vs. script plus video of simulated CPR and intubation. Patients’ decisions registered in the hospital record, by hospital discharge were compared for the two groups.
Results: Fifty script-only intervention patients averaging 77.7 years were compared to 50 script+video patients with a mean age of 74.7 years. Eleven of 50 (22%) in each group declined CPR; and an additional three (script) vs. four (script+video) refused intubation for respiratory failure. There were no differences in sex, self-reported health trajectory, functional limitations, length of stay, or mortality associated with decisions.
Conclusion: The rate at which verbally informed hospitalized elders opted out of resuscitation was not impacted by adding a video depiction of CPR.
Keywords: end of life, cardiopulmonary resuscitation, CPR, intubation, mechanical ventilation, autonomy
Introduction
When considering hypothetical scenarios that describe risks, benefits, and alternatives, a majority of elders prefer not to receive cardiopulmonary resuscitation (CPR) or endotracheal intubation/mechanical ventilation.1 Since informed consent is not required for these invasive procedures in the US, CPR and intubation are frequently provided by default2 despite ample opportunity to discern patients’ wishes before CPR.
Accordingly, investigators have tested methods to enhance patient decision-making regarding CPR. Studies have suggested that brief, narrated videos depicting CPR and intubation, deployed during verbal information-sharing, impact decisions of cancer patients,3,4 critically ill surrogates,5 and acutely hospitalized elders nearing end-of-life.6 We hypothesized that video depicting CPR/intubation would impact decisions of non-critically ill, hospitalized elders who receive uniform information regarding risks, benefits, and alternatives of resuscitation.
Methods
This protocol (NCT01878968) was approved by the Institutional Review Board of the Jewish Hospital of Cincinnati, a 350-bed community teaching hospital, where the study was performed. Patients were candidates for the studies if they were >65 years and admitted to the department of medicine hospitalist service. Each morning, a list of patients admitted to the service in the prior 24 hours was generated using the hospital’s electronic medical records. Patients were excluded if they had been admitted or transferred to/from the critical care unit, if they required contact isolation or if they already had a formal order precluding CPR or intubation. Eligible patients were approached for participation by study personnel and included if they provided verbal and formal written consent.
Patients who agreed to participate (Figure 1) were randomized to hear a brief, evidence-based script (Figure S1) with or without viewing a video depicting simulated CPR and mechanical ventilation (Video S1). The formal recorded resuscitation decisions, at discharge, of study patients and those who refused participation were the primary outcome of interest.
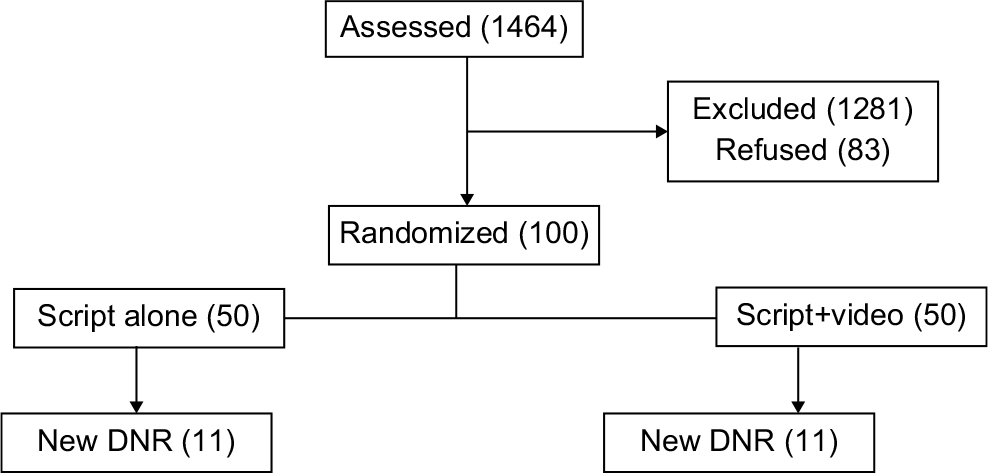 | Figure 1 CONSORT figure for patient entry (DNR = no CPR and/or endotracheal intubation). Abbreviations: DNR, do not resuscitate; CPR, cardiopulmonary resuscitation. |
Demographic, self-reported functional status and health trajectory, resuscitation decisions, and outcomes of the index hospitalization (including intensive care unit transfer, intubation, CPR, mortality, and length of stay) were recorded for all study patients. Outcomes of patients receiving script alone were compared to those of script+video and to non-participants by Z-test for proportions, non-paired Student’s t-tests, and analysis of variance as appropriate. Multiple logistic regression analyses were used to adjust for confounding, and included mechanistically plausible independent variables and those found to differ between groups’ univariate analyses. A P-value of <0.05 signified statistical significance.
Results
Fourteen hundred sixty-four patients were assessed for eligibility between September and December 2014; 1281 did not meet entry criteria, 83 refused, and 100 agreed to participate. This cohort included 53 women and 47 men, 73 Whites, 25 African-Americans, and one Hispanic. The average length of stay was 4.4 days. All patients reported their pre-study understanding of resuscitation prognosis, activities of daily living, instrumental activities of daily living, and 6-month health trajectory (Table 1). Fifty-six (56%) reported no change in their health 6–12 months prior to admission, 18 (18%) reported worsening, and 26 (26%) reported improving. Thirty-one patients (31%) believed that ≥50% of patients survive hospitalization after CPR. Thirty (30%) believed that 70% of patients requiring mechanical ventilation were alive 1 year later.
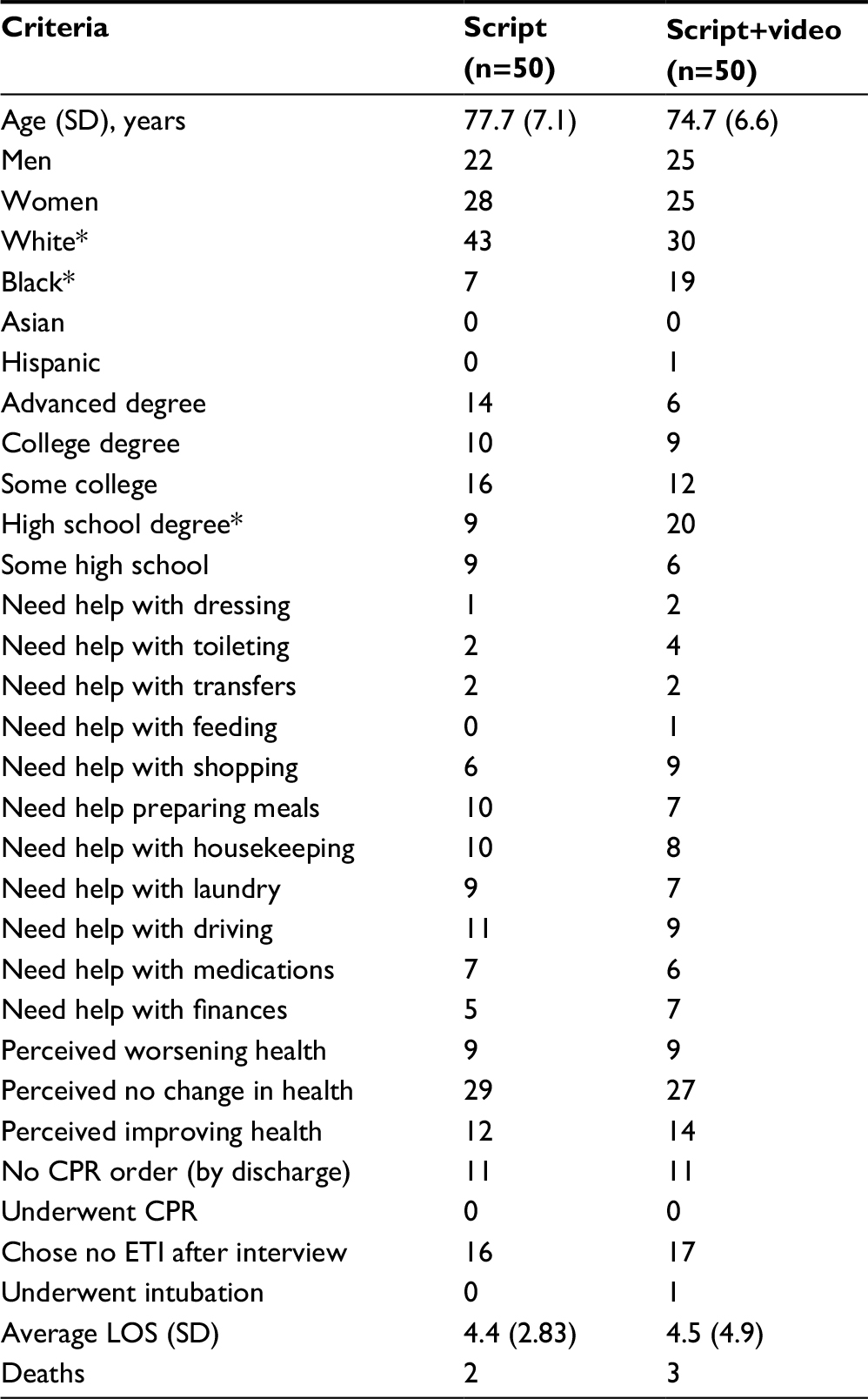 | Table 1 Characteristics and resuscitation decisions of patients randomized to script alone vs. script+video Note: *Statistically significant difference (P<0.05). Abbreviations: CPR, cardiopulmonary resuscitation; ETI, endotracheal intubation; LOS, length of stay. |
Fifty patients who received the script-only intervention averaging 77.7 years were compared to 50 patients with average age 75.7 years, randomized to script+video. There were no differences in sex, self-reported 6-month health trajectory, or baseline understanding of CPR and intubation. There was no difference in patients refusing CPR or intubation in the script-only group (11/50, 22%) compared with the script+video group (11/50, 22%). No enrolled patients received CPR during admission, only one was intubated and similar numbers did not survive admission (two script vs. three script+video). When study patients were compared to 83 patients who declined participation, study patients were six times more likely (22/100 vs. 3/83) to have opted out of CPR and/or intubation.
Discussion
This study demonstrates that hospitalized elders who were willing to participate in this study of end-of-life decision-making, opted out of CPR at the same rate (22%) whether or not they viewed a video depicting CPR and endotracheal intubation. While the video is not likely to harm efforts at informed consent for CPR, substantive, evidence-based, information-sharing may be the “effective” ingredient that could differentiate this from previous studies.1,3–6
Between 1992 and 2005, 433,985 Medicare beneficiaries underwent CPR in US hospitals.7 While roughly half may survive the initial cardiac arrest, many initial survivors go on to prolonged hospitalization including critical illness and only 18% (overall) survive to hospital discharge. Since survival of alive discharges at 1 year averages 59%,8 overall survival at 1 year following CPR is 10.6%. Not all of these patients are functionally independent and many have long-term (e.g., neurologic and other) sequelae. Outcomes following intubation are also not good. A landmark 2005 study estimated that more than 377,000 patients aged ≥65 are mechanically ventilated each year.9 Of these, 25%–30% do not survive hospitalization and more than half of survivors are discharged to nursing homes, many with substantial physical and mental disabilities.10 These complex prognostic data must be considered in the context of specific patient health trajectory and values.
Withholding CPR requires informed consent from the patient; however if patients do not receive information and understand outcomes and prognosis of CPR, they are unable to provide informed consent. There is abundant evidence to suggest that many (if not a majority) of informed patients opt out.1–6 In a cohort of 371 non-hospitalized elderly patients (>60 years), 41% opted for CPR before receiving information about it, which dropped to 22% after receiving prognostic statistics.1
Volandes et al4 randomized 50 patients with malignant brain tumors to receive either verbal narrative about CPR or narrative+video. “After the verbal description, 25.9% of participants preferred life-prolonging care, 51.9% basic care, and 22.2% comfort care. In the video arm, no participants preferred life-prolonging care, 4.4% preferred basic care, 91.3% preferred comfort care, and 4.4% were uncertain.”3 These results were reproduced in a cohort of 150 patients with advanced cancer; 48% of script-only patients opted for CPR while only 20% who received script+video opted for CPR.4 In a small study of 23 surrogate decision-makers of critically ill patients, script+video nearly doubled (41% vs. 22%) the rate at which surrogates opted out for their loved one.5 The same 3-minute video was deployed in a recent prospective randomized study of 150 elders with prognosis <1 year. Sixty-four percent of patients “treated” with video-assisted decision support opted out of CPR compared to only 32% receiving routine care.6 Our study differs in examining responses of acutely ill, hospitalized, non-terminally ill elders. Since ours was a heterogeneous group with varying prognosis, it is not surprising that the opt-out rate was substantially lower. Moreover, while our video included similar content, it was not professionally produced. So our findings suggest that either video (categorically) does not enhance decision-making or that the proprietary video used by Volandes et al adds, where our home-grown version (that includes similar content) does not. Interestingly, we demonstrated identical opt-out rates (22%) in a pilot when we used the proprietary video.11 We believe our data suggest that if verbal information-sharing is sufficient, the exact script or use of video is less consequential than systematic, early engagement of patients in shared decision-making. A recent review highlights paucity of studies to demonstrate definitive ideal approaches to these discussions, but concluded that “the most promising interventions involved structured discussion at the time of acute admission to hospital and review by specialist teams at the point of an acute deterioration” based largely on the results of one small study.12,13 Our observations support this conclusion, confirming that patients are willing to consider and make proactive, informed choices about their “code status.”12,13
There are several limitations in our study. Firstly, the sample sizes were small and there were few in-hospital deaths, cardiopulmonary arrests or respiratory failure requiring endotracheal intubation. Secondly, many patients refused to participate in this study. Recruitment bias could overestimate the observed results if patients who preferred resuscitation systematically refused participation. Thirdly, our study does not necessarily demonstrate that the specific videos/script affected these results. We do not know what conversations occurred between patients who did not participate and their physicians. So, our result reflects the impact of a systematic, uniform discussion about resuscitations rather than the specific impact of a script. Finally, end-of-life choices vary substantially among demographic groups, and while the study cohort is somewhat diverse, results represent choices at one hospital, in one city, in one region of the US that is not representative of all cities/regions/countries.
Conclusion
Our study suggests that if engaged early during hospital admission, with or without video assistance, a substantial proportion of hospitalized, non-critically ill elders opt out of CPR and intubation. Similar patients who were not uniformly engaged, opted out far less often. The interventions deployed in this study are practical, take little time to administer, and may serve as a useful complement for discussions with hospitalized patients about CPR/intubation. Our study confirms what previous surveys have suggested: that when informed of risks, benefits, and alternatives of CPR and intubation many patients opt out.1 Our study provides a simple, reproducible methodology that may promote patient autonomy through enhanced information-sharing.
Disclosure
The authors report no conflicts of interest in this work.
References
Murphy DJ, Burrows D, Santilli S, et al. The influence of the probability of survival on patients’ preferences regarding cardiopulmonary resuscitation. N Engl J Med. 1994;330(8):545–549. | ||
Mirza A, Kad R, Ellison NM. Cardiopulmonary resuscitation is not addressed in the admitting medical records for the majority of patients who undergo CPR in the hospital. Am J Hosp Palliat Care. 2005;22(1):20–25. | ||
El-Jawahri A, Podgurski LM, Eichler AF, et al. Use of video to facilitate end-of-life discussions with patients with cancer: a randomized controlled trial. J Clin Oncol. 2010;28(2):305–310. | ||
Volandes AE, Paasche-Orlow MK, Mitchell SL, et al. Randomized controlled trial of a video decision support tool for cardiopulmonary resuscitation decision making in advanced cancer. J Clin Oncol. 2013;31(3):380–386. | ||
McCannon JB, O’Donell J, Thompson BT, et al. Augmenting communication and decision making in the intensive care unit with a cardiopulmonary resuscitation video decision support tool: a temporal intervention study. J Palliat Med. 2012;15(12):1382–1387. | ||
El-Jawahri A, Mitchell SL, Paeche-Orlow MK, et al. A randomized controlled trial of a CPR and intubation video decision support tool for hospitalized patients. J Gen Intern Med. 2015;30(8):1071–1080. | ||
Ehlenbach WJ, Barnato AE, Curtis JR, et al. Epidemiology of in-hospital cardiopulmonary resuscitation in the elderly. N Engl J Med. 2009;361(1): 22–31. | ||
Chan PS, Nallamouthu BK, Krumholz HM, et al. Long-term outcomes in elderly survivors of in-hospital cardiac arrest. N Engl J Med. 2013;368(11):1019–1026. | ||
Wunsch H, Linde-Zwirble WT, Angus DC, Hartman ME, Milbrandt EB, Kahn JM. The epidemiology of mechanical ventilation use in the United States. Crit Care Med. 2010;38(10):1947–1953. | ||
Barnato AE, Albert SM, Angus DC, Lave JR, Degenholtz HB. Disability among elderly survivors of mechanical ventilation. Am J Respir Crit Care Med. 2011;183(8):1037–1042. | ||
Naqvi I, Richardson-Royer CM, Riffel C, Harvey L, Manthous CA. A prospective randomized trial of informed consent for cardiopulmonary resuscitation. Am J Respir Crit Care Med. 2014;189: A3623. | ||
Nicolasora N, Pannala R, Mountantonakis S, et al. If asked, hospitalized patients will choose whether to receive life-sustaining therapies. J Hosp Med. 2006;1(3):161–167. | ||
Field RA, Fritz Z, Baker A, Grove A, Perkins GD. Systematic review of interventions to improve appropriate use and outcomes associated with do-not-attempt-cardiopulmonary-resuscitation decisions. Resuscitation. 2014;85(11):1418–1431. |
Supplementary material
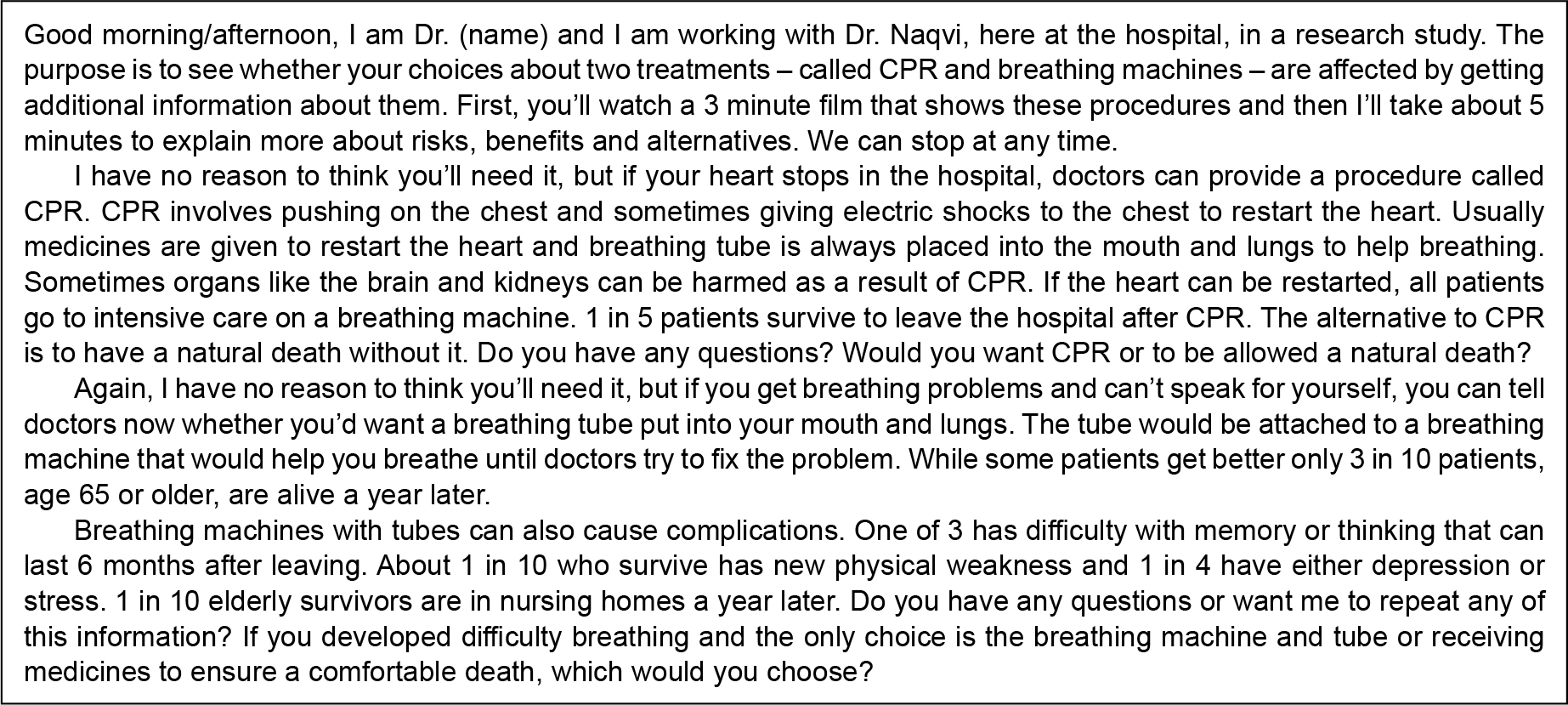 | Figure S1 Scripted intervention. Note: Scripted intervention delivered to intervention groups in both pilot and final study. This script was analyzed using a web-based readability tool which indicates it is at between the 7th and 8th grade levels by the Coleman Liau and Automated Readability Indices. Abbreviation: CPR, cardiopulmonary resuscitation. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.