Back to Journals » International Medical Case Reports Journal » Volume 15
A Twin Pregnancy of Partial Mole Coexisting with a Normal Fetus: A Case Report
Authors Tolcha FD ![]() , Usman AK, Senbeta HB
, Usman AK, Senbeta HB ![]() , Tadesse TM
, Tadesse TM ![]()
Received 16 February 2022
Accepted for publication 3 June 2022
Published 9 June 2022 Volume 2022:15 Pages 275—280
DOI https://doi.org/10.2147/IMCRJ.S362339
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Professor Ronald Prineas
Fekata Defere Tolcha, Abubeker Kedir Usman, Habtamu Beyene Senbeta, Telila Mesfin Tadesse
Department of Obstetrics and Gynecology, Madda Walabu University, Goba Referral Hospital, Goba, Oromia, Ethiopia
Correspondence: Fekata Defere Tolcha, Email [email protected]
Background: Twin pregnancy with partial hydatidiform mole and a co-existing normal fetus (PHMCF) is a very rare clinical condition. It presents with various complications like preterm labor, pre-eclampsia, hyperthyroidism and fetal anomalies.
Case Presentation: We report the case of a 40-year-old G13P10A2 mother who was referred to our hospital at 28 weeks as a case of twin pregnancy and pre-eclampsia. She had headache, epigastric pain, bilateral leg swelling, and decreased fetal movement for two days. Her physical examination was remarkable for raised blood pressure and uterus larger than gestational age. Ultrasound findings showed honeycomb-like echo suggestive of a molar pregnancy with a co-existing normal fetus. After she was admitted and managed for severe pre-eclampsia, a cesarean section was done to affect the delivery of a male neonate weighing 1400 grams. Histopathology confirmed the diagnosis of a partial mole with no malignant features. In follow-up, the serum β-HCG level normalized by the 7th week.
Conclusion: PHMCF is a rare obstetric condition. Despite these pregnancies having a greater risk of complications, strict follow-up at a tertiary care hospital and timely management of complications can result in good outcomes for both the mother and the fetus.
Keywords: partial mole, twin pregnancy, case report, pre-eclampsia
Introduction
Multifetal gestation is an obstetric condition of two or more fetuses marked by various complications with maternal risks including antepartum hemorrhage, spontaneous abortions, congenital anomalies, intrauterine fetal demise, preterm labor, and preeclampsia.1 Gestational trophoblastic disease is a clinical condition of abnormal trophoblastic cells encompassing a range of benign to malignant conditions. Premalignant conditions include complete mole and partial mole, which may present with vaginal bleeding, hyperemesis gravidarum, pre-eclampsia, hyperthyroidism and large for date uterus.2
If one of the twins is a molar pregnancy with an incidence of 1 in 100,000 pregnancies, the risks of complications are amplified by added risks arising from the partial mole. Regardless of those risks, 40% of patients with complete hydatidiform mole and co-existing normal fetus (CHMCF) result in a live birth.3 Even though singleton molar pregnancies are terminated, twin pregnancies with hydatidiform mole can continue if there are no complications or genetic abnormalities.4
Despite there being life-threatening risks to the mother, expectant management should be a considerable option as shown by our case. The delicate balance between managing complications of the pregnancy and not endangering the fetus is a hard one to maintain. Here, we try to show the concurrent management of PHMCF and arising complications. Even though there are reports of multiple pregnancies co-existing with complete molar mole, we could only find a few reports regarding co-existence with partial mole.5 The recent increment in artificial fertilization is increasingly becoming a culprit for the uptick in cases of PHMCF.6
Case Presentation
We present a 40-year-old Gravida13 Para10 Abortion2 mother who presented with headache, epigastric pain, bilateral leg swelling, epistaxis, and decreased fetal movement for a two-day duration. Her previous pregnancies were uneventful with no prior history of hypertensive diseases in pregnancy or hyperthyroidism reported. Although she had eight home deliveries, there were no twin pregnancies or molar pregnancies. In addition, she had no family history of bleeding diathesis. On the current pregnancy, she had no bleeding, raised blood pressure or any danger signs on the antenatal follow-up she had at 9 weeks. She was referred from a local health center, where the diagnosis of co-existing molar pregnancy was overlooked, with the impression of twin pregnancy and pre-eclampsia.
On admission, her blood pressure was 186/100, her pulse rate was 136 and her respiratory rate was 20. On abdominal examination, she had 36 weeks sized gravid uterus with fetal heartbeat of 136 and grade 2 bilateral pitting edema. On the admission blood tests, hematocrit was 32.8% with O+ blood type. Serum β-HCG was found to be 215,400 IU/L, thyroid stimulating hormone was 0.05 IU/mL, urinalysis showed +1 proteinuria, other investigations (Renal function test, Liver function test, Complete blood count, and Chest X-ray) were all normal. With the impression of twin pregnancy complicated by pre-eclampsia with severity features and hyperthyroidism, the patient was managed for pre-eclampsia and a biophysical profile was done daily. Ultrasonography revealed two fetal sacs whereby twin A was a breech, alive twin with aggregate gestational age (AGA) of 28+6 weeks with the normal-appearing placenta as seen in (Figure 1). The other sac was filled with cystic spaces and snowstorm appearance, hinting towards a molar pregnancy (Figure 2).
 |
Figure 1 Ultrasound images showing fetal head and a normal placenta next to the molar tissue. |
 |
Figure 2 Ultrasound image showing the snow storm appearance of the molar tissue. |
We managed our patient expectantly for a week with daily biophysical profile, dexamethasone injections for fetal lung maturity, magnesium sulphate and anti-hypertensive for pre-eclampsia. After one week, a cesarean section was done for indication of twin pregnancy plus Twin A breech to affect the delivery of a 1.4 kg male neonate with Apgar score of 7 and 9 in the 1st and 5th minute, respectively. The grape-like vesicles, separate from the normal appearing placenta, were evacuated manually (Figure 3). There was intraoperative bleeding while removing the molar tissue. Initial evaluation of the neonate revealed no congenital abnormalities and he was admitted to the neonatal intensive care unit with a diagnosis of very low birth weight and discharged after attaining adequate weight. Although, the histopathology result showed a partial mole with variable-sized dilated chorionic villi with focal trophoblastic proliferation and multiple vascular proliferation seen, there were no malignant features. Post-operative hematocrit was 18.8% for which the patient was transfused with one unit of whole blood. The patient was discharged from our side on the 16th day after advice on subsequent follow-up. The level of β-HCG was determined to be normal on the 2nd follow-up at 7 weeks as illustrated in (Table 1). On this visit, the mother had no new compliant with normal blood pressure and TSH levels. In addition, the infant’s interpretation of growth curves adjusted for gestational age showed adequate growth.
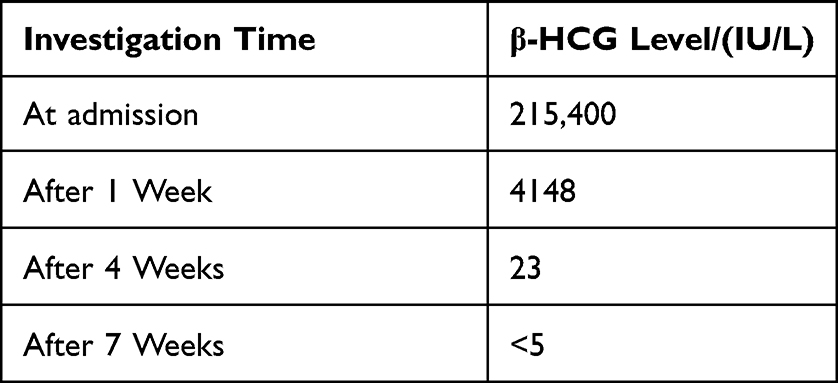 |
Table 1 Serum Beta Human Chorionic Gonadotropin (HCG) Decrement |
 |
Figure 3 A post-operative picture showing the normal placenta with the vesicles of the partial mole. |
Discussion
Twin pregnancy of hydatidiform mole coexisting with a live fetus is a rare entity. A normal fetus with a normal placenta can occur with either complete hydatidiform (CHMCF) or partial hydatidiform mole (PHMCF). The major risk factors for these pregnancies are extreme maternal ages (<15 years and >35 years) and previous molar pregnancy.4,7 Even though all types of molar pregnancies have a higher risk of maternal complication and fetal abnormalities compared to normal pregnancies, PHMCF has a lower risk of maternal complication.8,9 PHMCF occurs with an incidence of 0.005%–0.01% of all pregnancies despite being on the rise due to artificial fertilization. Antepartum bleeding, preterm labor, pre-eclampsia with severity features, thyrotoxicosis, and intrauterine fetal demise can occur in molar pregnancy.10
Multifetal gestations have a higher risk of pre-eclampsia, preterm delivery, and poor neonatal outcomes. PHMCF with the add-on effect of a molar component will contribute to early and exacerbated presentation of these complications.11 In our case, the patient had pre-eclampsia with severity features and hyperthyroidism, which could have been amplified by the presence of molar tissue.
The best initial modality used to screen and diagnose is an ultrasound, which, if performed in the early second trimester, has a detection rate ranging from 43% to 68%.12 The ultra-sonographic appearance of a partial hydatidiform mole has been described as being honeycomb-like echogenic tissue with multi-cystic areas in the first trimester and as a “snowstorm” appearance in the second trimester. Although it can sometimes miss congenital malformations, ultrasound will aid in screening for congenital anomalies as these pregnancies are fraught with various abnormalities.13 Histopathologic findings can differentiate between complete and partial moles with focal trophoblastic hyperplasia and fetal parts or cells indicating partial mole.4
Management plan differs based on the time of diagnosis. If diagnosed earlier, patients are advised and options are discussed with the mother. However, as many of these pregnancies arise due to infertility treatment, some women may wish to continue the pregnancy despite the risks. If diagnosed later in pregnancy, managing teams may find it difficult to decide whether to continue or terminate it. Given that maternal and fetal conditions are monitored strictly, continuing the pregnancy should be considered.14 Cesarean section is the best mode of delivery owing to the risk of metastasis of trophoblastic cells by uterine contraction if delivery is through spontaneous vaginal delivery.15
Follow-up is crucial as there is a risk of disease progression. Higher β-HCG levels and termination due to complications were associated with the development of gestational trophoblastic disease.16 Even though there is a possibility that PHMCF may persist as a gestational trophoblastic disease, which is 4%, the risk is higher for CHMCF (12%–20%).17 Hence, differentiating between CHM and PHM is of paramount importance as follow-up durations are tailored based on this. Although patients with CHMCF are followed for 6–12 months post-normalization of β-HCG, patients with PHMCF are observed for only 4 weeks.18
Conclusion
In conclusion, in twin pregnancy of hydatidiform mole and a co-existing normal fetus, priority should be given to ensuring maternal safety as there are grave maternal consequences. If the mother opts to continue with the pregnancy despite advice, we recommend she be transferred to a tertiary care setting with a thorough evaluation and strict follow-up in advance anticipation of complications. If complications arise and fetal lung maturity is confirmed, we advise the delivery of these pregnancies. In addition, pregnancy should be terminated if maternal condition worsens or fetal anomalies which are incompatible with life are confirmed.
Data Sharing Statement
A copy of the case clinical information, informed consent form, and images are available for review from the corresponding author upon request by the editor of this Journal.
Ethical Approval
There is no ethical concern for this case report as there was neither a data set analysis nor a management for research purposes only. Hence, institutional approval is not required for our case report.
Consent
Written informed consent was obtained from the patient for publication of her condition and accompanying images. A copy of the written consent form is available to the editor of this journal.
Funding
We received no funding for our case report.
Disclosure
We declare that there is no conflict of interest in our case report.
References
1. Fishman DA, Padilla LA, Keh P, Cohen L, Frederiksen M, Lurain JR. Management of Twin Pregnancies Consisting of a Complete Hydatidiform Mole and Normal Fetus. Obstetrics Gynecology. 1997;7844(97):546–550.
2. Tsakiridis I, Giouleka S, Kalogiannidis I, Mamopoulos A, Athanasiadis A, Dagklis T. Diagnosis and Management of Gestational Trophoblastic Disease: a Comparative Review of National and International Guidelines. Obstet Gynecol Surv. 2020;75(12):747–756. doi:10.1097/OGX.0000000000000848
3. Sebire NJ, Foskett M, Paradinas FJ, et al. Outcome of twin pregnancies with complete hydatidiform mole and healthy co-twin Diagnosis of vascular graft infections with antibodies against staphylococcal slime antigens For personal use. Lancet. 2002;359:2165–2166. doi:10.1016/S0140-6736(02)09085-2
4. Ngan HYS, Seckl MJ, Berkowitz RS, et al. Update on the diagnosis and management of gestational trophoblastic disease. Int j Gynecol Obstetrics. 2018;143:79–85. doi:10.1002/ijgo.12615
5. Sharon NZ, Maymon R, Melcer Y, Jauniaux E. Obstetric outcomes of twin pregnancies presenting with a complete hydatidiform mole and coexistent normal fetus: a systematic review and meta-analysis. BJOG. 2020;127:1450–1457. doi:10.1111/1471-0528.16283
6. Cheng-juan SZ, You-ping HAO, Song YU, Ling F, Wu Qing-qing LI. Twin pregnancy and partial hydatidiform mole following in vitro fertilization and embryos transfer: a novel case of placental mosaicism. Chin Med J. 2012;125(24):4517–4519.
7. Tsakiridis I, Mamopoulos A, Kalogiannidis I, Dagklis T, Aggelidou S, Athanasiadis A. Coexisting normal pregnancy with complete mole: a rare case report with successful pregnancy outcome. J Obstet Gynaecol. 2021;5:1–3. doi:10.1080/01443615.2020.1845636
8. Matsui H, Suzuka K, Iitsuka Y, Seki S, Sekiya S. Hydatidiform mole coexistent with a twin live fetus: a national collaborative study in Japan. Int J Gynecol Obstet. 2000;70(3):A135–A136. doi:10.1016/s0020-7292(00
9. Shazly SAEM, Ali MK, Abdel Badee AY, Alsokkary ABA, Khodary MM, Mostafa NAE. Twin pregnancy with complete hydatidiform mole and coexisting fetus following ovulation induction with a non-prescribed clomiphene citrate regimen: a case report. J Med Case Rep. 2012;6:1–5. doi:10.1186/1752-1947-6-95
10. Rathod S, Rani R, John LB, Samal SK. Successful outcome of twin gestation with partial mole and co-existing live fetus: a case report. J Clin Diagnostic Res. 2015;9(8):QD01–QD02. doi:10.7860/JCDR/2015/13038.6268
11. Sibai BM, Hauth J, Caritis S, et al. Hypertensive disorders in twin versus singleton gestations. Am J Obstet Gynecol. 2000;182(4):938–942. doi:10.1067/mob.2000.104439
12. Imafuku H, Miyahara Y, Ebina Y, Yamada H. Ultrasound and MRI findings of twin pregnancies with complete hydatidiform mole and coexisting normal fetus: two case reports. Kobe J Med Sci. 2018;64(1):E1–E5.
13. Zeng C, Chen Y, Zhao L, Wan B. Partial hydatidiform mole and coexistent live fetus: a case report and review of the literature. Open Med. 2020;14(1):843–847. doi:10.1515/med-2019-0098
14. Chu W, Chapman J, Persons DL, Fan F. Twin Pregnancy With Partial Hydatidiform Mole and coexistent fetus. Arch Pathol Lab Med. 2004;128(11):1305–1306. doi:10.5858/2004-128-1305-TPWPHM
15. Lin M, Chen J, Liao B, He Z, Lin S, Luo Y. When a vesicular placenta meets a live fetus: case report of twin pregnancy with a partial hydatidiform mole. BMC Pregnancy Childbirth. 2021;21(1):1–9. doi:10.1186/s12884-021-04160-2
16. Lin LH, Maestá I, Braga A, et al. Gynecologic Oncology Multiple pregnancies with complete mole and coexisting normal fetus in North and South America: a retrospective multicenter cohort and literature review. Gynecol Oncol. 2017;145(1):88–95. doi:10.1016/j.ygyno.2017.01.021
17. Dolapcioglu K, Gungoren A, Hakverdi S, Hakverdi AU, Egilmez E. Twin pregnancy with a complete hydatidiform mole and co-existent live fetus: two case reports and review of the literature. Arch Gynecol Obstet. 2009;279(3):431–436. doi:10.1007/s00404-008-0737-x
18. Gajewska M, Zygula A, Wielgos M, Szewczyk G. Twin pregnancy with a partial hydatidiform mole and a coexistent live fetus. Diagnostic and therapeutic dilemmas. A case report and the review of literature. Ginekol Pol. 2020;91(10):589–593. doi:10.5603/GP.a2020.0109
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Umbilical Artery Thrombosis After Selective Termination in Dichorionic Diamniotic Twin Pregnancy: A Case Report
Liu H, Zeng Z, Liao H, Hu Q, Yu H
International Journal of Women's Health 2023, 15:1327-1332
Published Date: 10 August 2023