Back to Journals » Patient Preference and Adherence » Volume 17
A Theoretical Qualitative Investigation Exploring Illness Perceptions and Decision-Making About COVID-19 in an Ethnically Diverse UK-Based Sample
Authors McDonald S ![]() , Blackie LER
, Blackie LER ![]()
Received 16 September 2022
Accepted for publication 9 December 2022
Published 19 February 2023 Volume 2023:17 Pages 473—489
DOI https://doi.org/10.2147/PPA.S389660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Stephanie McDonald, Laura ER Blackie
School of Psychology, University of Nottingham, Nottingham, UK
Correspondence: Stephanie McDonald, School of Psychology, University of Nottingham, Nottingham, UK, Email [email protected]
Purpose: The primary aim of the present investigation was to explore perceptions, experiences, and decision-making relating to the COVID-19 illness as the UK entered into a phase of “living safely with COVID-19”. A secondary aim was to explore how perceptions around the COVID-19 vaccine might vary by ethnicity.
Participants and Methods: We adopted a qualitative approach with a diverse sample of UK-based participants. One-hundred-and-ninety-three individuals completed an online survey measuring perceptions towards COVID-19 with questions conceptualized through the Common-Sense Model of Self-Regulation.
Results: Through deductive thematic analysis we identified one overarching theme in our data, “The transition back to normal routines”, with four themes illustrating individuals’ perceptions and experiences with COVID-19: 1) “Living with the uncertainty”, 2) “Concern for others”, 3) “The multiple consequences of COVID-19”, and 4) “Sense of control”, with the sub-theme of “Should I vaccinate, should I not vaccinate?”.
Conclusion: Findings from the present investigation provide key insights for understanding how people’s perceptions of COVID-19 during this transition period might impact their decisions and behavior moving forward. Specifically, findings suggest some prevailing concerns around catching the virus, while no strong qualitative evidence for concerns over long COVID were identified in this sample, the responsibility felt by individuals towards taking their own precautionary measures in light of the easing of all national restrictions, and some potential differences in perceptions towards the vaccine between individuals from different ethnic backgrounds.
Keywords: illness perceptions, common-sense model, COVID-19
Introduction
On March 11th 2020, the outbreak of the novel coronavirus SARS-Cov-2 was declared a pandemic by the World Health Organization (WHO). This had a significant impact on people’s lives, the health sector, and the economy worldwide. National restrictions were implemented across the globe to try and tackle the virus. These included a cycle of lockdowns, social distancing, the wearing of face coverings, hand sanitizing, and regular testing against the virus.1 In the United Kingdom (UK) the first lockdown took place between 26th March and 23rd June 2020.2 Following this, government regulations were monitored and adapted according to the progress of the virus, and further local lockdowns in specific regions were implemented throughout 2020–2021. At the time the present research was conducted during July 2021, the UK was entering a phase of “living safely with COVID-19”. This saw the easing of COVID-19 related restrictions, including removing the mandate for face coverings in indoor areas and social distancing measures. This was at a point in time where the majority of adults over the age of 25 years had been offered at least one dose of the COVID-19 vaccine. The UK was one of the first countries in Europe to enter such a phase, and it marked a transition back to normal pre-pandemic routines after over a year of national restrictions that had changed how people worked, lived, and socialized.
Illness perceptions have previously been shown to influence behavioral and emotional responses to a health threat, such as the outbreak of infectious diseases.3–5 Research focusing on individuals’ illness perceptions, and how these may influence decision-making, coping strategies, and health behavior relating to COVID-19 were, by majority, conducted at the earlier stages of the pandemic.4,6–8 At that point in time, the novelty of the virus brought with it uncertainties with regards to the possible impact of the illness on individuals’ health, wellbeing, and daily activities both in the short and longer term. It is not yet known what people’s perceptions and experiences were in relation to the COVID-19 illness as societies phased out of the pandemic, and indeed, what this new “normality” and living with the virus may look like for individuals. It is, therefore, important to explore how individuals may be adjusting to this transition, how perceptions may be changing compared to findings presented in the literature from earlier stages of the COVID-19 pandemic, how illness perceptions may be influencing individuals’ behavior, and to identify areas where support could be targeted moving forward in response to concerns, uncertainties, or potential misconceptions. Findings from this theoretically-driven study involving the collection of data from a diverse UK-based sample, where efforts were made to recruit individuals from different ethnic backgrounds, can provide important insights to inform practice as more and more countries are implementing an exit strategy from the pandemic.
Illness Perceptions and COVID-19
Research suggests that illness perceptions are key factors influencing behavior relating to illness prevention and management, coping, and recovery.9,10 The Common Sense Model of Self-Regulation (CSM) is a dominant theoretical model in the study of illness representations or perceptions.9 According to the CSM, when faced with a health threat, such as the SARS-Cov-2 coronavirus disease (COVID-19), individuals form cognitive representations of the health threat. These consist of the following dimensions: a) the identity of illness (symptoms), b) perceptions of the cause of the illness, c) the consequences of the illness to the individual, d) perceptions of cure or control of the illness by the individual’s actions (personal control) and available treatment (treatment control), and e) beliefs around the timeline of the illness.
In a parallel process, people also form emotional reactions to the health threat, termed emotional representations in the CSM, which may include fear, anger, or distress. Cognitive and emotional illness representations guide the adoption of coping strategies to deal with the health threat and the emotional reactions to the threat. Appraisal of coping strategies and illness outcomes can then lead to a modification of adopted strategies or illness perceptions in a feedback mechanism. As such, the CSM provides a dynamic framework of individuals’ self-management of illness.9 Research suggests that illness perceptions are present both in patient and non-patient populations,3 with findings demonstrating similarity in how healthy individuals and clinical samples cognitively represent an illness.11 Within the context of COVID-19, individuals’ perceptions of illness have been found to be key determinants of uptake and adherence to preventative measures, such as mask wearing, social distancing, and sanitizing, which was particularly significant in the earlier stages of the pandemic,3,4,6 as well as decision-making with regards the COVID-19 vaccine.12
According to the CSM, illness perceptions are considered to be dynamic and evolving over time, often as a result of a process of appraisal of the consequences of coping strategies adopted by the individual.9 The evolution of the illness, outcomes of treatment and general perceptions around the seriousness of illness can also influence individuals’ illness representations.3 A longitudinal study conducted at the earlier stages of the pandemic looking at illness perceptions and how these may evolve over the course of COVID-19, found that over a period of four months, participants rated the virus as having more negative consequences, a longer timeline and a more prevalent identity. Emotional representations, on the other hand, were found to be stable across the two points in time.7 This can have profound implications in terms of how individuals may be impacted by COVID-19. If the emotional reaction to the illness remains stable across time, especially if this reflects more negative affect towards the illness, such emotional perceptions can have a negative impact on the individual’s wellbeing and quality of life. Previous findings also show that illness perceptions can be modified by relevant interventions, and that this can have a positive impact on health-related outcomes and behavior.13–15
Theoretically-driven studies of people’s perceptions and experiences can provide key insights for the development of interventions to target future support and aid towards clarifying potential misconceptions. It is, therefore, important to assess individuals’ perceptions of the illness, especially as nations are evolving away from imposed restrictions, where individual behavior is largely determined by individual decision-making rather than government policy. While some of these dimensions would have been influenced by consistent public health messages (eg, symptoms and timeline), there is still likely to be considerable individual differences in how individuals perceive the salience of these dimensions to their lives. For example, some individuals might be concerned with long COVID, whereas others view the flu-like symptoms as a short-term illness. It is therefore important to examine differences in illness perceptions, because these will likely influence their decisions and behaviors, which is particularly relevant in a time when UK individuals have had autonomy by the government to choose what precautions and measures they take to live with the virus.
The Role of Ethnicity in Shaping Perceptions and Decision-Making in Relation to the COVID-19 Vaccine
The COVID-19 vaccine is currently advised by medical organizations to offer the most effective means of protecting individuals from the virus.16 However, the effectiveness of vaccination programs is largely determined by uptake in the population. Vaccine hesitancy is characterized by an individual refusing or delaying getting vaccinated despite it being readily available to them.17 Within the UK, studies have found that hesitancy towards the COVID-19 vaccine is more prevalent in ethnic minority communities.18–20 Research in UK samples has found higher hesitancy towards the COVID-19 vaccine among individuals from Black ethnic backgrounds, followed by individuals from Asian ethnic backgrounds.19,21 It is particularly important to understand why this might be the case given that ethnic minorities living in the UK have been disproportionately affected by COVID-1922 both in terms of illness severity and socio-economic impact. Although this was not the primary question in this study, we did recruit a diverse UK sample and our questions asked about treatment control, potentially giving us qualitative insights from individuals to explore if and how vaccine hesitancy was expressed within the context of the CSM.
Research into factors contributing towards COVID-19 vaccine hesitancy in the UK have included lack of trust towards the vaccine and worry around side effects and longer term effects of the vaccine.19,21 However, understanding the causes of vaccine hesitancy is a complex issue. It is important to consider vaccine hesitancy within the broader social context, where distrust in the UK medical system among individuals from ethnic minority communities, and particularly people of Black ethnic background, have shown to be influenced by experiences of racial discrimination.23 Within the context of health care, experiences of discrimination and distrust in the medical system can contribute to lower uptake of preventative health services, including immunization.23–28 Recent evidence from the USA demonstrates that there is considerable variability within COVID-19 vaccine hesitancy; while many individuals from Black ethnic backgrounds did not feel hesitant towards taking the vaccine, vaccine hesitancy was greater for individuals from Black ethnic communities whom had experienced the death of a close friend or family member or whom had experienced discrimination from the police or courts.29 Instances of historical betrayals against ethnic minority groups (eg, Windrush, Tuskegee, Brexit) have been linked with lower trust in government and law enforcement, especially in ethnic minority communities.30–32 Findings also suggest that lack of trust affecting health decisions in ethnic minority communities is not just focused on luck of trust in the apparatus of the state, but also lack of trust in other individuals within their communities, outgroups, and the political process.32
Given the impact of vaccine hesitancy upon the health of individuals and the longer term management of the virus and the pandemic, it is important to explore whether differences in views and experiences around the vaccine remain prevalent in ethnic minority communities. A secondary aim of the present investigation was, therefore, to explore individuals’ perceptions towards treatment control. Perceptions around treatment map onto the treatment control dimension of the CSM. Within the context of COVID-19, treatment control was conceptualized as perceptions towards the COVID-19 vaccine. As such, the approach taken in this study was to explore whether responses relating to this dimension of the CSM varied by ethnicity.
Timing and Nature of Present Investigation
The majority of studies investigating perceptions around COVID-19 have been published at the earlier stages of the pandemic, providing useful insights into people’s experiences and health-related beliefs. It is also important to capture perceptions as nations are progressing towards a new stage in the pandemic, characterized by the easing of restrictions. Even in the summer of 2022 cases of COVID-19 infections have increased exponentially, reinforcing the need to understand how individuals perceive the COVID-19 virus after immunization. Exploring illness representations and decision processes will provide key insights into any misconceptions, and areas where interventions can be targeted to support individuals into this gradual process of further change in the pandemic, and in the absence of government-related policy around precautionary measures in guiding behavior.
The present investigation adopted a theoretically-based qualitative approach to the study of illness perceptions, experiences, and decision-making relating to the COVID-19 illness. Studies exploring perceptions around COVID-19 have primarily been conducted within the context of a quantitative theoretical framework, adopting measures such as the Brief or Revised Illness Perception Questionnaire.5–7 A key strength of the present investigation is the adoption of a qualitative research design along with recruitment of a diverse sample of individuals from different ethnic backgrounds. This is in line with previous research exploring experiences, perceptions, and decision-making in the health domain which has the potential to gain in-depth insights into these experiences.33 Doing so, will enable us to gain an in-depth understanding into these processes, above and beyond the knowledge that standardized scales may be able to provide. Given the novelty of this virus, and indeed the current pandemic, this research will offer insights into the perspective of the individual.
Materials and Methods
Participants
Data from 193 individuals were analyzed. Participants were recruited through PROLIFIC, a platform used to recruit participants for online research studies. Recruitment strategy involved recruiting individuals who lived in the United Kingdom at the time of the research and were between the ages of 25–60 years. The rationale for this age restriction was, first, the research was conducted at a time when national COVID-19 restrictions were beginning to be lifted in July 2021 and at a time where the majority of individuals over the age of 25 had already been offered their first dose of the COVID-19 vaccine. Second, the upper age limit reflects the fact that guidance available in the National Health Service placed individuals over the age of 60 as a vulnerable population to COVID-19.34 To enable the inclusion of a diverse and representative sample with varied experiences and perceptions in our study we set a criterion within PROLIFIC to include individuals from diverse ethnic backgrounds. Individuals received monetary reward for taking part in the study, as per the terms and conditions of the recruitment platform.
Participants’ ages ranged from 25–60 years (Mage = 33.4 years; SD = 7.6). Thirty-three percent of our sample identified as White, 30.4% identified as Black, Caribbean, Black British, 22.6% as Asian and Asian British, 9.7% of Mixed ethnic backgrounds, 2.5% of participants self-identifying as other ethnic groups, and 1.5% not disclosing their ethnic background. Seventy-seven percent of participants identified as female, 23% as male, and fewer than 1% as non-binary.
Within the context of COVID-19 it can be challenging to strictly classify individuals in terms of patient versus non-patient status. This can depend on whether individuals had a positive COVID-19 test, whether they experienced symptoms, as well as the severity and variability of symptoms between individuals, and whether they were in need of medical treatment. The first criterion being particularly challenging to establish as tests only became widely available after the initial states of the pandemic. Therefore, given the nature of the COVID-19 disease and how individuals came to be diagnosed with having contracted the virus, the following measures were included in the survey to gain information around participants’ experiences with COVID-19: whether participants had a positive COVID-19 test since the start of the pandemic, whether they were required to self-isolate at any point during the pandemic either due to a positive test or someone in their immediate environment receiving a positive test, and whether they needed medical treatment for COVID-19.
Thirteen percent of participants reported having received a positive COVID-19 test over the course of the pandemic, with 62% reporting that they had knowledge of others in their immediate environment. Forty-two percent of participants reported that they had to self-isolate at some point during the pandemic due to the experience of COVID-19 related symptoms, or due to themselves or others in their immediate environment receiving a positive test. Given the unpredictable and cyclical nature of the COVID-19 virus, the inclusion of a wider sample of participants with varying experiences can provide important insights into perceptions and insights into supporting individuals towards the final stages of the COVID-19 pandemic and towards a move towards normality or, indeed, a new version of normality. Also, given the variability in experience and that most people were impacted through self-isolation, we did not employ a patient vs non-patient distinction but analyzed data from the whole sample together. Seventy-nine percent of our sample reported having received at least one dose of the COVID-19 vaccine, 59% had received two doses, and 21% reported not having vaccinated.
Materials and Procedure
The study received ethical approval from the School of Psychology Ethics Committee at the University of Nottingham (Reference: F1289, F1297) and informed consent was obtained from participants prior to taking part in the study. The study complied with the principles set out in the Declaration of Helsinki.35 Data was collected via Qualtrics, an online survey software, between 23rd and 27th July 2021. The study was advertised through PROLIFIC together with an anonymous link to the survey. This contained the participant information sheet and consent statement, followed by the survey questions which were displayed once participants provided consent to taking part.
Survey Questions
Demographic Variables
Participants were asked to report their age and gender. We also asked participants to report their ethnic origin on the basis of pre-defined ethnic categories used in UK government surveys.
Experience with COVID-19
Participants were asked whether they had a positive result from a COVID-19 test since the start of the pandemic (ie, March 2020), whether they had previously received medical treatment for COVID-19, whether anyone in their close social environment received a positive test result and whether they had to self-isolate at any stage during the pandemic as a result of being a close contact of someone who had tested positive. Participants were also asked to report whether they had received the COVID-19 vaccine, either one or two doses. Participants responded to all these questions with either a yes or no option.
Perceptions Around the COVID-19 Illness
A number of open-ended questions were included in the survey to capture participants’ perceptions and experiences with COVID-19. Questions were framed around the dimensions of the CSM, as measured by the Brief Illness Perception Questionnaire.36 This is a validated measure of illness representations as conceptualized in the CSM framework. Each question was developed to capture a separate dimension. To capture the experiences of individuals who previously contracted COVID-19, as measured by a positive COVID-19 test, as well as those who had not been infected with the virus, the questions were adapted so that they could be answered by all participants, whether they had experience with the illness or not. For example, to investigate perceptions around personal control over COVID-19 two variations of questions were developed: “To what extent have you experienced any symptoms relating to COVID-19?” (displayed for participants with a previous positive test result) and the equivalent question “If you were to catch COVID-19 at this point in time, to what extent do you think you would experience any symptoms relating to this?” (displayed for individuals with no previous positive test result).
Remaining questions included views and experiences with the COVID-19 vaccine, the practical and emotional impact that contracting the virus had or would have on the individual, perceived level of control over catching and managing the illness, perceptions around timeline, and concerns about COVID-19 at a stage in the pandemic when restrictions and social distancing measures were easing. The full list of survey questions is presented in Table 1.
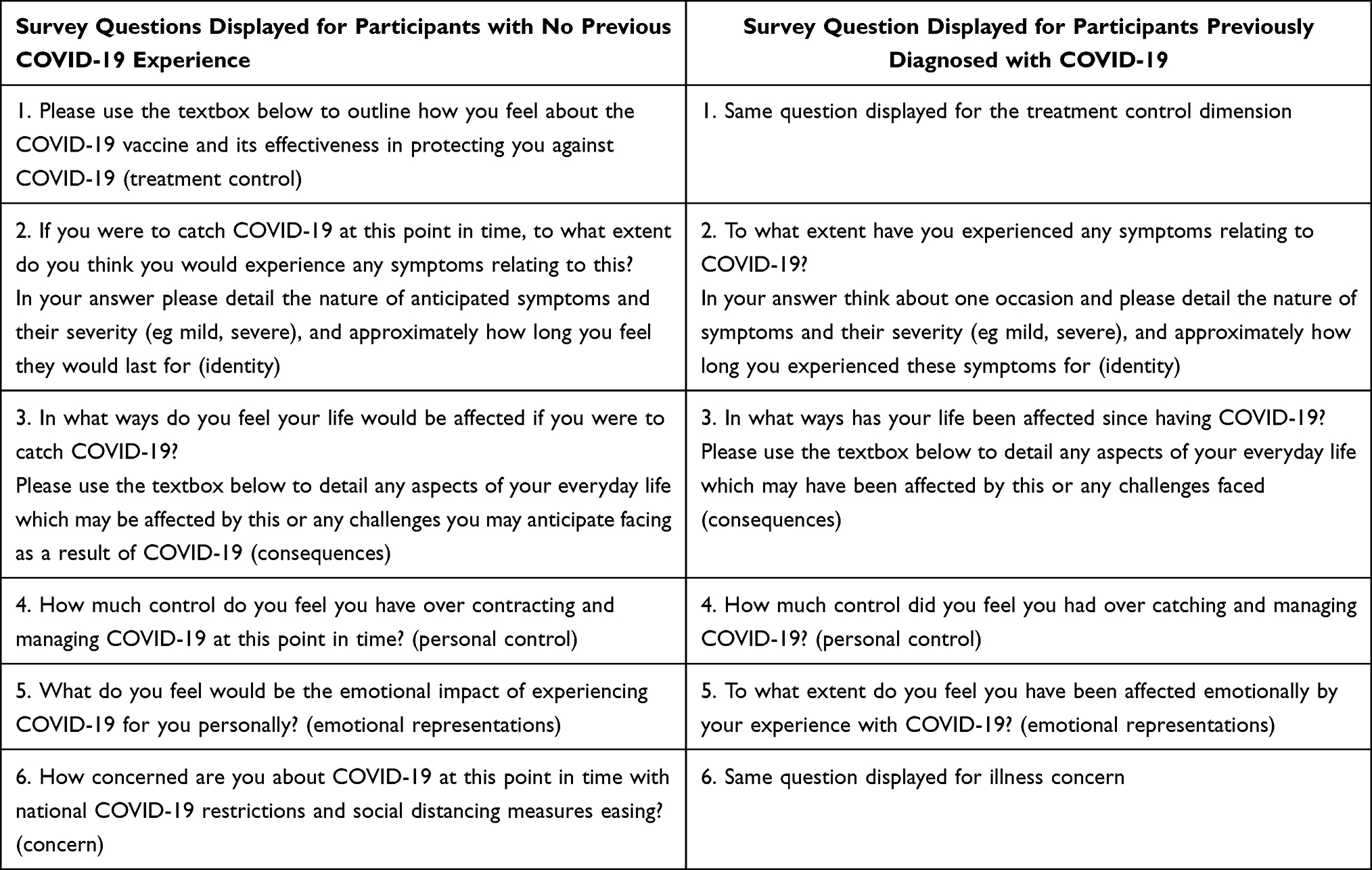 |
Table 1 Survey Questions |
Analysis
Data were analyzed by means of deductive thematic analysis. The aim of thematic analysis is to identify patterns of ideas prevalent across the dataset that address the study’s research question(s). Deductive thematic analysis often involves analysis driven by a theory or existing literature on the topic under investigation. In the present study we used the dimensions of the CSM to structure our survey schedule so as to capture key aspects of individuals’ perceptions and experiences with a particular health issue and to drive the analysis. This approach has been adopted in previous research.37 We therefore initially coded participants’ responses within each CSM dimension, but we reviewed and collapsed codes into broader themes where there was considerable conceptual overlap in themes, in line with the principles of thematic analysis, to arrive at a parsimonious theme structure of the prevalent ideas across the data set.
The data was exported in Microsoft Excel for coding. We adopted the six analytic steps outlined by Braun and Clarke (Braun & Clarke, 2006) to develop a thematic map of individuals’ perceptions and experiences with COVID-19 as we move towards the final stages of this pandemic.
- Data familiarization: This first step involved repeatedly reading through the entire dataset to gain familiarity with the data and to identity any initial ideas that were related to our research question and the broader CSM dimensions that guided our initial coding and analysis.
- Data coding: involved identifying extracts from participants’ responses which were relevant to our research question and generating initial codes for those extracts. Coding was done at the semantic level, whereby codes reflected a summary of surface level meanings in participants’ responses. We adopted a realist/essential standpoint, where the focus of the analysis is on participants’ experiences and the meanings in those experiences. Initial coding was generated for each CSM dimension separately. This process, together with step 1, was undertaken by both authors, where for some questions coding was done explicitly by one of the authors and for the remaining questions codes were generated by both authors. To address our main research question looking at participants’ illness perceptions and experiences, coding was undertaken across all participants’ responses for each survey question with the exception of the question relating to the treatment control dimension. To address our secondary research question, exploring whether perceptions around the COVID-19 vaccine differ between individuals from different ethnic backgrounds, coding for this particular research question was undertaken separately for each of the following groups of data a) responses of individuals with Black ethnic background b) responses of individuals with Asian ethnic background, and c) responses of individuals with White ethnic background. Given the small percentage of participants who identified as mixed or multiple ethnic groups or other ethnic group in our sample, these responses were excluded from the analysis of this question. Views on the COVID-19 vaccine are, therefore, presented separately in our thematic structure for each group of responses for vaccine perceptions only. Once initial coding was completed across the dataset, codes were collated, whereby duplicate codes or codes which represented the same underlying idea but phrased differently were adapted to produce a resulting list of codes, each representing a unique idea in our dataset in relation to our research questions. Whilst initial coding involved generating codes for each of the survey questions used in the analysis, to then generate our initial set of themes (step 3), we collated and combined all codes from questions in the survey focusing on perceptions around COVID-19. To address our secondary research question and capture views around the COVID-19 vaccine, collated codes were generated separately for each aforementioned group of data.
- Initial search for themes: this stage involved grouping conceptually similar codes into potential themes. We started with a set of deductive themes but we reviewed the conceptual overlap in ideas across themes after coding per theme. Thematic analysis strives for themes with clear and distinct boundaries, therefore we revised our theme structure to reduce themes from CSM dimensions into broader and more meaningful themes in this stage.
- Reviewing themes: this step involved checking that each theme in our final thematic map captured the ideas represented in the coded extracts and that all themes worked in relation to the dataset. Steps 3 and 4 were completed by the first author for consistency.
- Defining and naming themes: this step involved re-examining the final set of themes and the coded data to identity core conceptual ideas captured by each theme. This process enabled us to generate names for our themes. Both authors were involved in this step.
- Producing the report: selecting appropriate quotations across the dataset to illustrate how the conceptual ideas encapsulated within each of our themes were represented in the data. This step was completed by the first author.
Results
One overarching theme was identified in the data, addressing our primary question of exploring illness perceptions on COVID-19 across the dataset: “The transition back to normal routines”, with four themes, illustrating individuals’ perceptions and experiences with COVID-19: 1) “Living with the uncertainty”, 2) “Concern for others”, 3) “The multiple consequences of COVID-19”, and 3) “Sense of control”. In addressing our secondary question on potential qualitative differences in views and experiences with the COVID-19 vaccine among individuals from different ethnic backgrounds, we developed a subtheme within the “Sense of control” theme: “Should I vaccinate, should I not vaccine?”. Each theme is presented below, together with supporting quotations from participants’ responses. Quotations reflect participants’ exact responses; no grammatical changes have been made by the authors.
The Transition Back to Normal Routines
This overarching theme captures people’s views and concerns with the COVID-19 virus, and how they make meaning of a significant change in the context of the pandemic through their experiences of psychological and physical adjustment in this process.
Living with the Uncertainty
This theme reflects how UK individuals saw society as progressing towards the final stages of the pandemic, yet the threat of the virus still loomed. The prospect of catching COVID-19 was still worrying to individuals. Although responses ranged from no concerns around COVID-19 to high levels of concern, there was a general sense of worry in our sample around exposure to the virus. Some participants felt, due to its high transmissibility, catching the virus was inevitable, given it is still possible to contract it even if fully immunized. As one participant noted,
I feel little control. Although I am vaccinated, numbers of cases are on the rise and as I am yet to get covid-19, I feel like a sitting duck waiting to get it. I do feel safer having been double vaccinated but I do still feel nervous… (Participant 130)
Some concerns were centered around uncertainty with regards to how the virus may manifest, with individuals who identified as vulnerable or with pre-existing medical conditions expressing concerns around the impact the virus could potentially have on these conditions, or potential severity of COVID-19 related symptoms as a result of these health issues. Even in those without any underlying health conditions, there were some concerns around the possibility of experiencing more severe symptoms of the illness and uncertainty with regards to longer term effects of the virus on the individual’s health. For example, one participant reported
Covid is still out there, and no one can be certain how it affects my health (short and long term) until I catch it (Participant 70)
whilst another noted
I think the symptoms would be mild to moderate. I worry that I would feel quite unwell and not be able to do my day to day activities for up to 2 weeks. I worry that I might be affected longer term with fatigue. (Participant 157)
In addition to concerns around their personal health, some participants also raised concerns that COVID-19 is still highly transmissible, with easing of restrictive measures likely leading to further spread of the virus and a rise in positive cases. For a number of individuals, the anticipated impact would be the return of restrictions and possible lockdowns, resembling earlier stages of the pandemic. This reflects perceptions around the cyclical nature of the virus and highlighting the unpredictability of the virus as perceived by participants at these later stages in the pandemic, leading to uncertainty around a move towards normality. For example, one participant commented
I am worried that more people will catch it and that we will go back into a lockdown. However I do believe that we need to get back to “normal” at some point (Participant 17)
Concern for Others
The notion of concern and responsibility towards others was prevalent across our dataset, often more so than concerns around one’s own health. Participants wrote about feeling worried, anxious, even guilty of the prospect of passing the virus onto loved ones and others who may be more vulnerable to the effects of the virus. For example, one participant commented
Emotionally stressing about catching or even potentially to pass it on to others. Also stressful thinking about vulnerable family members getting it (Participant 159)
Others commented how easing of restrictions may put those who are unvaccinated at risk, such as young persons who at the time were below the recommended age for having the vaccine or individuals who could not have the vaccine due to other health-related issues. One participant noted,
Very concerned [with the easing of restrictions] - I’m worried that it’ll result in even more covid mutations that might not be affected by the vaccine. I’m also very aware that there are people who cannot get vaccinated (e.g. They’re immuno-compromised), and they are incredibly at risk right now. (Participant 85)
Some individuals also commented that the easing of restrictions was unfair on individuals as well as those who may have less control over coming into contact with others, for example due to the nature of their work, and thus are at a potentially higher risk of infection. As one participant commented,
I think it’s wrong to have eased restrictions, at the very least reduced the mask-wearing policy. I feel that it’s unfair on people who have less control e.g. shop workers, health workers, public transport workers on who they come into contact with. I’m expecting a third fourth wave. (Participant 72)
Participants also talked about the impact on significant others if they were to contract the virus. Specifically, some individuals reported that this would be a source of worry as, depending on the nature and severity of symptoms, they would have to rely on others for everyday tasks or caretaking for their young children. They feared that this would put an additional burden on loved ones, whilst the individual recovered and self-isolated to prevent spreading the virus to family members. For example, as one participant reported
Isolating myself can affect my life in a massive way. It means I have to have people to depend on to supply basic necessities. It will affect people who depend on me as well since they will be cut off. It affects general morale and well-being. (Participant 74)
The Multiple Consequences of COVID-19
This theme captures participants’ lived and anticipated experiences of the COVID-19 illness and the impact on their everyday lives and wellbeing, including perceptions around how the virus will manifest if individuals were to contract it.
In considering potential impact of contracting COVID-19 on everyday life, a number of participants anticipated either no impact or short-term minimal impact. Reporting on anticipated symptoms associated with the virus, the majority of participants reported that they expected symptoms to be mild to moderate, and relatively short-lived. Some expressed the belief that COVID-19 symptoms would resemble that of a cold or flu, potentially in a more severe form. For example, one individual noted
I would expect to develop some flu-like symptoms- mild to moderate fever, sneezing, mild-moderate headache, mild to moderate body ache, tiredness, cough. I surely wouldn’t expect anything severe. (Participant 169)
Some participants anticipated that some symptoms, such as shortness of breath and tiredness, may in fact persist for longer. Some participants who commented on more prolonged or severe symptoms was often due to other health conditions. For example, one participant reported
Severely. I have numerous high risk health condition and no doubt in my mind I would struggle. And would struggle to recover (Participant 178)
A minority of participants reported that they either experienced or would anticipate experiencing more severe symptoms for a longer period of time. Those who did report negative anticipated consequences expressed concerns around potential long term effects of COVID-19 on their health, such as their fitness levels and ability to exercise. As one participant commented,
I used to run but I now find this harder to do my chest gets tight quickly and I need to come home and have a sit down to get my breath back (Participant 141)
whilst another reported
Getting up and completing simple tasks would be much harder than usual as I would only be able to exert little energy. I would constantly feel weak too, therefore my full-time job would be very tough. I would feel tired all the time so wouldn’t be able to work much. Overall this would affect my everyday life majorly. (Participant 63)
Overall, although some participants expressed concerns over the possibility of longer term effects of COVID-19 on their health, beliefs around the experience of long COVID, in terms of how the majority of participants spoke about anticipated symptoms of COVID-19, were not prevalent in our sample.
The impact of COVID-19 was also captured through participants’ narrative around disruptions to everyday activities as a result of contracting the virus, in terms of inability to travel, caretaker responsibilities, and impact on work patterns and income if the individual were to either self-isolate or need to take leave of absence from work. The most significant impact of COVID-19 for participants was the emotional cost of having to self-isolate and how this would impact interactions with loved ones and mental wellbeing. For example, one participant commented
My mental health would suffer having to isolate, since I would not be able to spend time with my loved ones… (Participant 38).
Similarly, another participant mentioned
I have a very busy household with three young children so I think if I were to catch the virus. My general day to day chores and activities would be massive decreased plus my interaction with my children if they were to test negative, I wouldn’t be going around them which would massively upset me but would be essential for their safety. I would also not be able to work so financial impact so they added worry of that. (Participant 16)
Some participants also expressed feeling anxious about returning to normal activities and social situations following COVID-19. As one participant reported,
Everyday life has changed drastically. Can’t go anywhere without a face mask, emotionally a bit distressing having to think of being careful around people and thinking twice before going to events and places with lots of places as things start to open up. When feeling a bit under the weather or even if I come across a family and friend who is feeling under the weather the first thought to cross my mind is covid. (Participant 159)
In thinking about the timeline of COVID-19, some participants reported that they would expect the virus to continue to pose a threat in the shorter term (ie, within the next few years), with some responses reflecting a longer timeline. Some responses included beliefs around a more permanent presence of COVID-19 in our lives, such that the virus is here to stay and this is something that as a society we need to adjust to, learn to live with and manage through, for example, immunization programs, resembling strategies involved in managing seasonal flu.
Sense of Control
Although the majority of individuals who took part in this study had received, at the time, at least one dose of the COVID-19 vaccine, general concern about the virus was prevalent in our sample, and for many people the COVID-19 pandemic was far from over.
Responses ranged from participants feeling that they had a good sense of control over the virus to feelings of having no control over catching and managing the virus. A number of participants expressed that they continued to take precautionary measures against COVID-19, even in contexts where this was no longer mandated by government policy, to prevent catching or spreading the virus to other people. This often took the form of wearing face coverings in public places, maintaining social distance when in the presence of other people, and hand sanitizing regularly. These actions offered individuals some level of control in protecting themselves and others from infection as well as controlling for a further rise in positive cases and a risk to prolonging the pandemic, whilst acknowledging that these measures should continue to reflect a collective effort towards tackling COVID-19. For example, one participant reported
Although we don’t have total control, we can manage in some ways by being cautious. Remembering to sanitize/ wash our hands before touching our face, before eating, after coming from outside. Wearing a face mask and trying to maintain social distance. All this could certainly help us from contracting the infection to some extent. (Participant 169)
Participants expressed that they still acted cautiously, such as avoiding crowded places or being careful in social interactions and maintaining a healthy lifestyle. Responses also reflected beliefs that being themselves vaccinated as well as others in their immediate social environment gave individuals some hope of protection against COVID-19. For example, one individual commented
I think I have a high control now I’m double vaccinated and most of my friends/family are too… (Participant 139)
Participants who reported lower levels of perceived control over the virus often attributed this to a number of factors. Some felt that catching the virus was out of their control, expressing concerns and anger towards government management of the pandemic and decision-making with regards the lifting of restrictions, as they felt that this was either too soon in the pandemic or still posing a risk to vulnerable and unvaccinated individuals. Some responses reflected a belief that some precautionary measures should be kept in place by government, such as the use of facial coverings and social distancing measures, even if other restrictions are being lifted in a process of moving society towards “normal living” with the virus. For example, one participant reported
I am fairly concerned because cases are rising but there are no safety measures in place. I believe the government should have kept the little restrictions that were in place (masks and distancing) until cases calmed down. (Participant 24)
Some expressed that the easing of restrictions would have an impact on other people’s actions more generally, such that it could potentially encourage others to be less careful about COVID-19. Some participants expressed that they felt they had to follow these actions as others may not be taking precautionary measures, thus increasing the risk of infection for the individual as well as others. Some comments from participants include
I don’t think people understand that the vaccination programme won’t eradicate COVID-19. While I see most people trying their best to distance and maintain hygiene measures anyway, the pace of infection means that it only takes a small number of people to infect a whole community. I don’t trust some people to think of their family and communities, and stick to self-isolation guidance if they are pinged (Participant 32)
demonstrating lack of trust in individuals’ actions, and
I am concerned, particularly with the spread of the delta variant, that the easing of restrictions is ill-conceived. I think it will encourage people to act recklessly and unnecessarily increase risk of infection for everyone. (Participant 71)
Similarly, another participant commented
Having an underlying illness does cause me to worry as far as Covid-19 is concerned, and there are people not wearing masks and not using ‘commonsense’ as the government tells everybody to use. (Participant 53)
Others felt that complete lifting of restrictions would make it challenging for individuals to protect themselves in certain contexts and feeling less confident in these situations, such as when using public transport, frequent interactions with other people due to the nature of their work, thus, acknowledging that this pandemic is far from over yet. For example, one participant noted,
… this is a public health issue, we all must work together … hard to assure that i will not contract COVID-19 when I see large groups of people gathering outside and inside of pubs and in the streets without masks, and without being fully vaccinated. These same people then go on public transportation as well without masks or socially distancing. So I feel very little control over managing the spread of COVID-19 (Participant 83)
Others welcomed the easing of restrictions, as COVID-19 is something that we as a society need to learn to live with and manage, as it would not be feasible to remain in prolonged isolation.
I am not very concerned about covid19 as it is something we will have to live with, we need to start treating covid like flu (Participant 95)
Should I Vaccinate, Should I Not Vaccinate?
To address our secondary, more exploratory question around potential differences in how the vaccine was perceived across different ethnic groups in our sample, responses were coded separately for each of the following groups of data: responses from participants from Asian ethnic backgrounds, responses from participants from Black ethnic backgrounds, and responses from participants from White ethnic backgrounds. Through coding participants’ responses, we started to notice that whilst the ideas identified in the data were similarly expressed in all groups, some ideas, particularly those reflecting more reservation around the effectiveness of the vaccine, were more prevalent in some groups. Here we first present the positive perceptions and experiences with the COVID-19 vaccine that were shared across individuals from different ethnicities.
Participants who spoke more favorably towards the vaccine often acknowledged that even though the vaccine may not offer the individual full protection against contracting the virus, it was nevertheless effective in protecting the individual against severity of the illness, in terms of the experience of severe symptoms, hospitalization, and death from COVID-19. Participants also expressed confidence in the vaccine in protecting against the spread of the virus, offering some control in managing the pandemic; having being vaccinated further enabled a return to normal life and the ability to carry out activities, such as travelling, and feeling safer in carrying out such tasks. For example, as one participant reported,
I feel so happy and grateful to have received both doses of the vaccine. Although I know it does not completely stop me catching the virus, I feel confident that if I do get the virus, it won’t affect me as badly and that I am less likely to pass it on to others. (Participant 130)
Some comments also reflected beliefs around relevance of the vaccine primarily for individuals who may be more vulnerable to the effects of the illness. As one participant stated,
The benefits are not clear. I understand that it reduces illness and hospitalization. I don’t think it is a necessity for a healthy young person without pre-existing medical conditions. However, I choose to take it as it protects other vulnerable people in the community. (Participant 37)
Now, we compare responses across the three groups of participants on their concerns around the COVID-19 vaccine. While all groups reported concerns with effectiveness of the vaccine in protecting individuals against the onset of the COVID-19 illness, concerns with regards to the potential side effects or longer term effects of the vaccine, and mistrust in the vaccine, upon careful consideration of the codes developed in the analyses, we observed higher instances and more elaborate accounts reflecting these concerns in responses from participants from Black ethnic backgrounds, as shown in Table 2. We, therefore, made the decision to proceed with the analysis with counting the number of instances for this theme (ie, number of codes in the dataset relevant to this theme) within each group, in order to get a sense of the nature of the differences between groups. Number of instances of a code did not reflect number of individual participants. Rather, counts were per occurrence such that one participant, for example, could mention a number of related ideas. In the next paragraph, we present a qualitative narrative of these concerns with supporting evidence, and where appropriate, we highlight the differences between groups in terms of the frequencies of codes in each of these areas (as per Table 2).
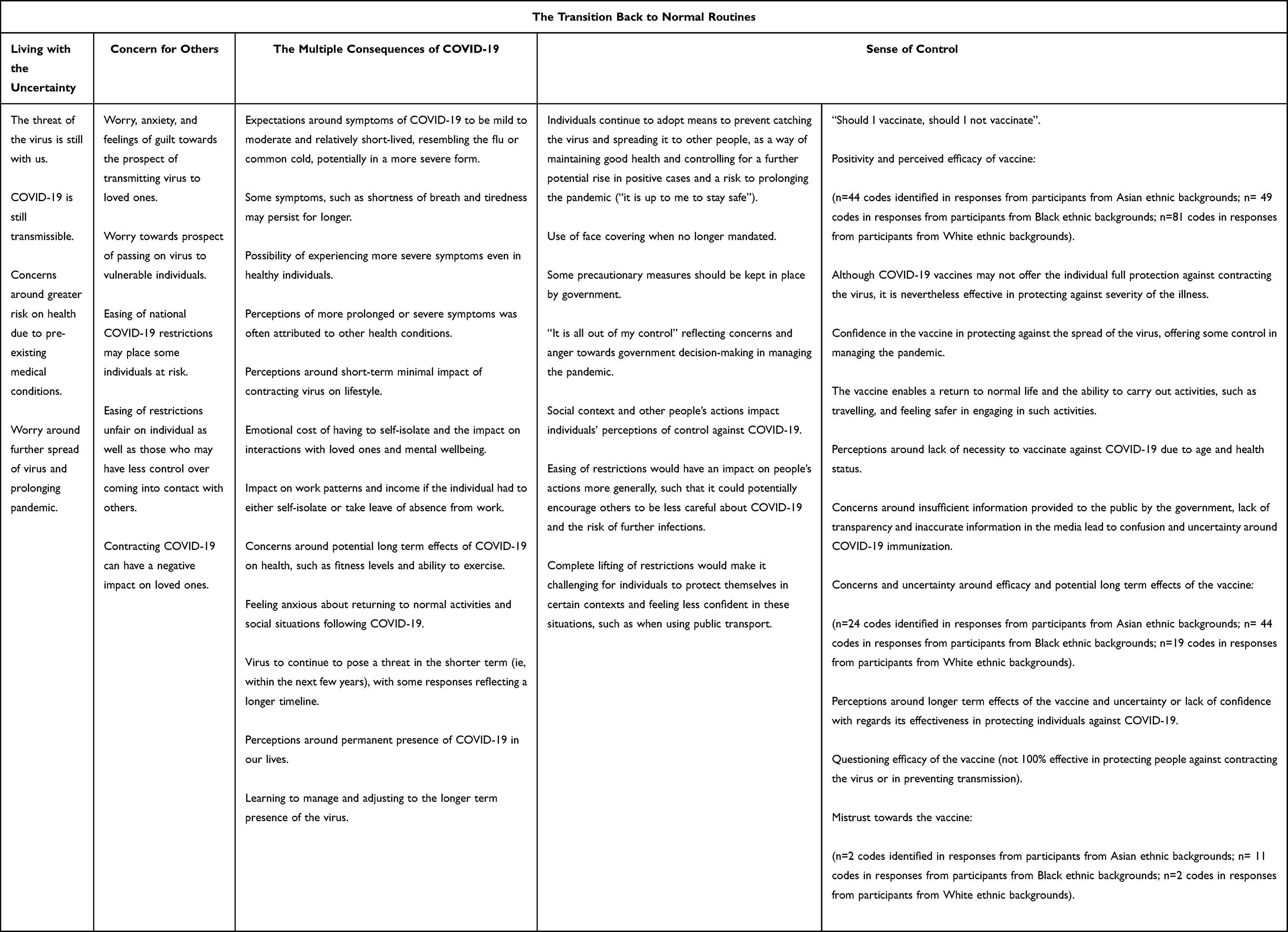 |
Table 2 Themes Developed in the Thematic Analysis with Collated Codes for Each Theme |
Participants from all groups expressed concerns around the potential longer term effects of the vaccine and uncertainty about its effectiveness in protecting individuals against COVID-19 and against potential new variants of the virus. Most individuals across the different groups who questioned the efficacy of the vaccine did so on the grounds that the vaccine was not perceived to be 100% effective in protecting people against contracting the virus or in preventing transmission. Some people commented that there is still a chance to catch the virus and experience illness from COVID-19 even whilst vaccinated. For example, one participant commented
Although I have had the vaccine, I’m still unsure about it as people have been double jabbed but still manage to get covid… (Participant 96)
Participants across all groups also commented negatively with regards information provided by the government around the vaccine and more generally how the vaccine was depicted in the media. More specifically, concerns around insufficient information provided to the public by the government, lack of transparency and inaccurate information in the media led to confusion and uncertainties around COVID-19 immunization. One participant reported
There are so many unknowns surrounding the Covid 19 vaccines, and I feel the government is not transparent enough with details to help me make that decision to get the vaccine anytime soon. I do believe the vaccines are productive but for me, the risks outweigh the benefit at this time. (Participant 93)
However, there were some differences between groups. As seen in Table 2, there was a higher prevalence of concerns around efficacy and potential long term effects of the vaccine among responses from participants from Black ethnic backgrounds. Participants from Black ethnic backgrounds also expressed more mistrust towards the vaccine in particular in comparison to individuals of Asian and White ethnic backgrounds. This reflected perceptions around the timeline of vaccine production coupled with insufficient vigorous testing of the vaccine. Some responses include
The vaccine doesn’t stop you from getting covid only from death. I also don’t think it’s that effective against newer strains. I’m hesitant about the vaccine because I don’t think extensive testing has been done on its effects of menstruating women. I also believe the health care system has a racial bias and in some cases just blatant racism and ignorance so I will be waiting to see the long term effects on those demographics. (Participant 33)
Similarly, another individual commented
I think it’s a joke, I don’t trust the science behind it. I think we are very hasty and that these vaccines need longer clinical trials. Efficacy is questionable and the government aren’t very open about the few who have suffered terrible sometimes permanent side effects. It’s necessary to get the economy back up and running. But I would prefer better more consistent behavioural changes in order for businesses to run and for individuals to continue social distancing. (Participant 121)
Discussion
The central aim of the present investigation was to obtain a comprehensive account of illness perceptions and decision-making in relation to COVID-19 in a diverse sample of participants through the lens of the Common-Sense Model of Self-Regulation. A secondary aim of this study was to examine perceptions towards treatment control in relation to the COVID-19 vaccine among individuals from different ethnic backgrounds. Findings from this theoretically-driven qualitative investigation offer key insights that enable the recommendations of interventions around managing the virus and supporting individuals as societies enter what appear to be the final stages in the COVID-19 pandemic, reflecting a “learning to live with the virus” approach. Key findings are discussed below, together with implications for practice.
The overarching theme from our analysis “The transition back to normal routines” captured that many individuals still had worries and concerns about COVID-19 despite the transition in the UK government’s policy to remove all national restrictions. In this discussion, we will draw out some of the key findings from our thematic analysis that we feel have significance for understanding how people’s perceptions of COVID-19 during this transition period might impact their decisions and behavior moving forward. Specifically, we will address the impact of three issues in turn: (1) limited concerns around developing long COVID in our sample, as captured in the way participants spoke about anticipated symptoms relating to COVID-19, 2) individuals’ perceptions towards taking their own precautionary measures in light of the easing of all national restrictions, and 3) differences between individuals from different ethnic backgrounds in their perceptions towards the COVID-19 vaccine.
First, we identified that most individuals in our sample reported that they expected the symptoms of COVID-19 to be mild and short-lived with few long-term health consequences. Of course, there were some exceptions to this, particularly among individuals with underlying health conditions or those with loved ones who were considered vulnerable. Yet, it is also notable that many individuals were reporting worries and concerns with catching COVID-19 as national restrictions eased, but there was less concern that it would manifest as more than cold or flu-like symptoms over the short-term. It is worth noting that the data was collected from a sample where the majority of people had had their first vaccination dose, and therefore it may indicate the trust and confidence many individuals had (with the exceptions noted above) in vaccination as a first-line of defense. However, while research shows vaccination is effective in reducing symptom severity and hospitalization,38 little is currently known on how vaccination mitigates the risk of long COVID. There are some inconsistencies in the research into long COVID with some studies in the UK reporting the vaccine to be more effective in reducing the risk of the long-duration of symptoms38 and other studies in the US reporting lower rates of vaccine efficacy in reducing risk of long COVID symptoms.39 These differences and gaps in knowledge may have implications for the decisions and behaviors individuals choose to engage in to protect themselves from the virus. However, as we discuss next, social norms and other concerns may override individuals’ tendencies to take precautionary behavioral measures.
Second, many participants discussed how they were continuing to take precautionary measures for themselves, such as adhering to social distancing and mask-wearing in crowded indoor spaces, despite many participants also saying they felt that the symptoms and health impact of COVID-19 would be short-lived. This has coincided more recently with recommendations from UK public health officials urging individuals to take these precautions as COVID-19 cases had surged in the summer months of June and July in 2022. However, while this is recommended health guidance, there are many reasons individuals may not follow this in a time where the choice of precaution taken lies on the individual’s own shoulders. Specifically, people’s health behaviors are heavily influenced by social norms, and their read on what is socially acceptable derived from other people’s behavior in similar contexts.40 The influence of social norms and conformity processes have been demonstrated early on in the COVID-19 pandemic when cases were high and vaccinations were not readily available to the public. Specifically, in one study researchers coded mask wearing data from public webcams across seven major cities in the UK, US, and Ireland in the autumn of 2020.41 They found that mask wearing behavior varied significantly, and a key factor was the level of mask wearing of others in the immediate area. This research is impactful in highlighting the role of social norms in a global crisis, because it was deduced from naturalistic methods, rather than self-report methods that could be subject to social desirability biases. To be clear, we are not advocating for a re-instatement of national restrictions, especially given the costs to mental health that have been documented in the literature from such policies,42 rather we are pointing to a psychological explanation for why individuals may remain concerned about COVID-19, yet may not take precautionary steps to reduce their personal risks.
Third, we noticed some differences between individuals from different ethnic groups in their perceptions towards the COVID-19 vaccine. As evidenced in our frequency counts for this theme (Table 2), participants from Black ethnic backgrounds questioned the efficacy of the vaccine to a greater extent and displayed greater mistrust in the vaccine compared to individuals from White and Asian ethnic backgrounds. This finding is consistent with some research from the UK showing concerns and hesitancy towards the uptake of the COVID-19 vaccine among individuals from ethnic minority groups,19,20 and importantly, it indicates that UK government health officials might need to engage with this and re-consider whether their one-size-fits-all approach to health messaging through the pandemic (eg, Prime Minister’s “Get Boosted Now” speech on 12 December 2021) addresses the unique health concerns from individuals in ethnic minority groups.
We provide two cautionary notes with regard to the implications of these potential differences in perceptions of the COVID-19 vaccine. First, our study was not designed primarily with this important question in mind, rather we recruited a diverse sample and had some broad questions on treatment control that could be used to gain some insight into this topic. However, if our study had asked about vaccine hesitancy directly, then we might have seen no differences, or a more diverse and elaborated set of responses that could speak to this important question more comprehensively than can our current data set. Second, and related to this first point, our qualitative analysis did not provide comprehensive and rich insight into the reasons why individuals reported greater concerns towards the vaccine. Drawing from existing UK research, one possibility is that individuals in some ethnic groups have lower faith in UK public health systems. For example, findings show significantly lower reports of trust in the NHS and towards NHS staff from individuals from Black ethnic backgrounds compared to individuals from White ethnic backgrounds.32 Yet, recent research, although in the USA, has shown that there is considerable variability in COVID-19 hesitancy, and a number of participants from Black ethnic backgrounds reported no hesitancy.29 This suggests that future research is needed to understand individuals’ responses to precautionary measures, such as vaccines, within a pandemic context while taking into account the broader social context that may influence individuals’ perceptions and reactions to the healthcare system.
Conclusion
Findings from the present investigation provide key insights into understanding how people’s perceptions of COVID-19 may impact their decisions and behavior moving forward during a period of transition back to normal routines. The results suggest prevailing concerns around catching the virus, while no strong qualitative evidence for concerns with long COVID in this sample, and some potential differences between individuals from different ethnic backgrounds regarding perceptions towards the vaccine that require further targeted investigation.
Acknowledgments
The authors would like to thank Professor Eamonn Ferguson for his helpful comments on an earlier draft of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organisation. Coronavirus disease (COVID-19). Available from: https://www.who.int/health-topics/coronavirus#tab=tab_1.
2. Institure for Government. Timeline of UK government coronavirus lockdowns and restrictions; 2022. Available from: https://www.instituteforgovernment.org.uk/charts/uk-government-coronavirus-lockdowns.
3. Dias Neto D, Nunes da Silva A, Roberto MS, et al. Illness perceptions of COVID-19 in Europe: predictors, impacts and temporal evolution. Front Psychol. 2021;12:1–11. doi:10.3389/fpsyg.2021.640955
4. Dixon D, Den Daas C, Hubbard G, Johnston M. Using behavioural theory to understand adherence to behaviours that reduce transmission of COVID-19; evidence from the CHARIS representative national study. Br J Health Psychol. 2022;27(1):116–135. doi:10.1111/bjhp.12533
5. Skapinakis P, Bellos S, Oikonomou A, et al. Depression and its relationship with coping strategies and illness perceptions during the COVID-19 lockdown in Greece: a cross-sectional survey of the population. Depress Res Treat. 2020. doi:10.1155/2020/3158954
6. Chong YY, Chien WT, Cheng HY, et al. The role of illness perceptions, coping, and self-efficacy on adherence to precautionary measures for COVID-19. Int J Environ Res Public Health. 2020;17(18):6540. doi:10.3390/IJERPH17186540
7. Shiloh S, Peleg S, Nudelman G. Making sense of COVID-19: a longitudinal investigation of the initial stages of developing illness representations. Psychol Health. 2021. doi:10.1080/08870446.2021.1925670
8. Figueiras MJ, Dias Neto D, Maroco J, Kern de Castro E. Is my risk lower than yours? The role of compared risk, illness perceptions, and self-efficacy as determinants of perceived risk for COVID-19. Heal Risk Soc. 2022;24(1–2):54–66. doi:10.1080/13698575.2022.2031911
9. Leventhal H, Phillips LA, Burns E. The Common-Sense Model of Self-Regulation (CSM): a dynamic framework for understanding illness self-management. J Behav Med. 2016;39(6):935–946. doi:10.1007/s10865-016-9782-2
10. Dempster M, Howell D, McCorry NK. Illness perceptions and coping in physical health conditions: a meta-analysis. J Psychosom Res. 2015;79(6):506–513. doi:10.1016/J.JPSYCHORES.2015.10.006
11. Figueiras MJ, Alves NC. Psychology and Health Lay perceptions of serious illnesses: an adapted version of the Revised Illness Perception Questionnaire (IPQ-R) for healthy people. Psychol Health. 2007. doi:10.1080/14768320600774462
12. Vollmann M, Salewski C. To get vaccinated, or not to get vaccinated, that is the question: illness representations about covid-19 and perceptions about covid-19 vaccination as predictors of covid-19 vaccination willingness among young adults in the Netherlands. Vaccines. 2021;9(9). doi:10.3390/vaccines9090941
13. Chan VWY, Kong APS, Lau JTF, Mak WWS, Cameron LD, Mo PKH. An intervention to change illness representations and self-care of individuals with type 2 diabetes: a randomized controlled trial. Psychosom Med. 2021;83(1):71–84. doi:10.1097/PSY.0000000000000883
14. Figueiras MJ, Maroco J, Monteiro R, Caeiro R, Dias Neto D. Randomized controlled trial of an intervention to change cardiac misconceptions in myocardial infarction patients. Psychol Health Med. 2017;22(3):255–265. doi:10.1080/13548506.2016.1153677
15. Petrie KJ, Cameron LD, Ellis CJ, Buick D, Weinman J. Changing illness perceptions after myocardial infarction: an early intervention randomized controlled trial. Psychosom Med. 2002;64(4):580–586. doi:10.1097/00006842-200207000-00007
16. World Health Organization. Coronavirus disease (COVID-19): vaccines; 2020. Available from: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-vaccines.
17. MacDonald NE, Eskola J, Liang X, et al. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33(34):4161–4164. doi:10.1016/J.VACCINE.2015.04.036
18. Scientific Advisory Group for Emergencies. Factors influencing COVID-19 vaccine uptake among minority ethnic groups, 17 December 2020 - GOV.UK; 2020. Available from: https://www.gov.uk/government/publications/factors-influencing-covid-19-vaccine-uptake-among-minority-ethnic-groups-17-december-2020.
19. Iyengar KP, Vaishya R, Jain VK, Ish P. BAME community hesitancy in the UK for COVID-19 vaccine: suggested solutions. Postgrad Med J. 2022;98(e2):e134–e135. doi:10.1136/POSTGRADMEDJ-2021-139957
20. Ekezie W, Czyznikowska BM, Rohit S, et al. The views of ethnic minority and vulnerable communities towards participation in COVID-19 vaccine trials. J Public Health. 2021;43(2):e258–e260. doi:10.1093/PUBMED/FDAA196
21. Robertson E, Reeve KS, Niedzwiedz CL, et al. Predictors of COVID-19 vaccine hesitancy in the UK Household Longitudinal Study. Brain Beh Immun. 2021;94:41–50. doi:10.1101/2020.12.27.20248899
22. UK Government. COVID-19: review of disparities in risks and outcomes - GOV.UK. Available from: https://www.gov.uk/government/publications/covid-19-review-of-disparities-in-risks-and-outcomes.; 2020.
23. Quinn SC, Jamison A, Freimuth VS, An J, Hancock GR, Musa D. Exploring racial influences on flu vaccine attitudes and behavior: results of a national survey of White and African American adults. Vaccine. 2017;35(8):1167–1174. doi:10.1016/J.VACCINE.2016.12.046
24. Musa D, Schulz R, Harris R, Silverman M, Thomas SB. Trust in the health care system and the use of preventive health services by older black and white adults. Am J Public Health. 2009;99(7):1293–1299. doi:10.2105/AJPH.2007.123927
25. Birkhäuer J, Gaab J, Kossowsky J, et al. Trust in the health care professional and health outcome: a meta-analysis. PLoS One. 2017;12(2). doi:10.1371/JOURNAL.PONE.0170988
26. Gille F, Smith S, Mays N. Why public trust in health care systems matters and deserves greater research attention. J Health Serv Res Policy. 2015;20(1):62–64. doi:10.1177/1355819614543161
27. Sullivan LS. Trust, risk, and race in American medicine. Hastings Cent Rep. 2020;50(1):18–26. doi:10.1002/HAST.1080
28. Schwei RJ, Kadunc K, Nguyen AL, Jacobs EA. Impact of sociodemographic factors and previous interactions with the health care system on institutional trust in three racial/ethnic groups. Patient Educ Couns. 2014;96(3):333–338. doi:10.1016/J.PEC.2014.06.003
29. Willis DE, Andersen JA, Montgomery BEE, et al. COVID-19 vaccine hesitancy and experiences of discrimination among black adults. J Racial Ethn Heal Disparities. 2022;1–10. doi:10.1007/S40615-022-01290-X/TABLES/3
30. Park J. Historical origins of the Tuskegee experiment: the dilemma of public health in the United States. Uisahak. 2017;26(3):545–578. doi:10.13081/KJMH.2017.26.545
31. Williams W. Windrush lessons learned review: independent review by Wendy Williams. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/876336/6.5577_HO_Windrush_Lessons_Learned_Review_LoResFinal.pdf.
32. Ferguson E, Dawe-Lane E, Khan Z, et al. Trust and distrust: identifying recruitment targets for ethnic minority blood donors. Transfus Med. 2022;32(4):276–287. doi:10.1111/TME.12867
33. McDonald S, Ferguson E, Hagger M, Je Foss A, King AJ. Patient Preference and Adherence Dovepress A theory-driven qualitative study exploring issues relating to adherence to topical glaucoma medications. Patient Prefer Adhere. 2019. doi:10.2147/PPA.S174922
34. National Health Service. Who is at high risk from coronavirus (COVID-19) - NHS. Available from: https://www.nhs.uk/conditions/coronavirus-covid-19/people-at-higher-risk/who-is-at-high-risk-from-coronavirus/.
35. World Medical Association. Declaration of Helsinki: ethical principles for medical research involving human subjects. J Am Coll Dent. 2013;81(3):14–18. doi:10.1093/acprof:
36. Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–637. doi:10.1016/J.JPSYCHORES.2005.10.020
37. McDonald S, Ferguson E, Hagger MS, Foss AJE, King AJ. A theory-driven qualitative study exploring issues relating to adherence to topical glaucoma medications. Patient Prefer Adherence. 2019;13:819–828. doi:10.2147/PPA.S174922
38. Antonelli M, Penfold RS, Merino J, et al. Risk factors and disease profile of post-vaccination SARS-CoV-2 infection in UK users of the COVID Symptom Study app: a prospective, community-based, nested, case-control study. Lancet Infect Dis. 2022;22(1):43–55. doi:10.1016/S1473-3099(21)00460-6
39. Al-Aly Z, Bowe B, Xie Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat Med. 2022;28(7):1461–1467. doi:10.1038/s41591-022-01840-0
40. Cialdini RB, Goldstein NJ. SOCIAL INFLUENCE: compliance and conformity. Annu Rev Psychol. 2004;55:591–621. doi:10.1146/annurev.psych.55.090902.142015
41. Woodcock A, Wesley Schultz P. The role of conformity in mask-wearing during COVID-19. PLoS One. 2021;16(12):e0261321. doi:10.1371/JOURNAL.PONE.0261321
42. Rossi R, Socci V, Talevi D, et al. COVID-19 pandemic and lockdown measures impact on mental health among the general population in Italy. Front Psychiatry. 2020;11:7–12. doi:10.3389/fpsyt.2020.00790
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.