Back to Archived Journals » Open Access Journal of Sports Medicine » Volume 13
A Thematic Analysis of Osteopathic Physicians’ Identities and Experiences in North American Professional Sports
Authors Blacha K, Cade A ![]() , Russell T
, Russell T ![]() , Skinner D
, Skinner D ![]()
Received 16 June 2022
Accepted for publication 6 September 2022
Published 15 September 2022 Volume 2022:13 Pages 77—87
DOI https://doi.org/10.2147/OAJSM.S378045
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Andreas Imhoff
Kaitlyn Blacha,1 Andrew Cade,1 Tyler Russell,1 Daniel Skinner2
1Ohio University, Heritage College of Osteopathic Medicine, Dublin, OH, USA; 2Department of Social Medicine, Ohio University, Heritage College of Osteopathic Medicine, Dublin, OH, USA
Correspondence: Daniel Skinner, Email [email protected]
Objective: This interview-based thematic analysis examines the evolving professional identities and practices of osteopathic physicians (DOs) in North American professional sports (baseball, basketball, football, hockey, and soccer) to understand the extent to which DOs employ osteopathic-specific skill sets in their work with player-patients. In addition, the study sought to understand the prevalence of professional bias, interprofessional dynamics between DOs and other health professionals, and other factors such as management.
Methods: This qualitative, interview-based study is grounded in twelve semi-structured interviews with 41% of DOs (all nonsurgical, primary care sports medicine trained) working with North American professional sports teams. Interviews were transcribed and coded to identify key themes and representative quotes.
Results: Findings suggest that DOs believe their training and philosophical orientation positions them well to make important contributions to serving the medical needs of professional sports teams. At the same time, DOs are careful about championing an osteopathically-specific approach to patient care, such as evoking osteopathic principles of care or techniques such as Osteopathic Manipulative Medicine. This is the case for several reasons, the most important of which is a strong drive toward collaboration and collegiality within professional sports medicine teams.
Conclusion: This study finds that in navigating the complexities of osteopathic identity, DOs working in professional sports are proud of their osteopathic orientation and report experiencing little discrimination, but also downplay what has historically distinguished their practice from that of other healthcare professionals. These findings have consequences for how scholars think about emerging professional identities in sports medicine, generally, as well as the fast-growing profession of osteopathic medicine specifically.
Keywords: osteopathic medicine, sports medicine, professional identity, chiropractic
Introduction
Osteopathic medicine is one of two recognized types of medical practice in the United States. Practitioners distinguish themselves from mainstream (or “allopathic”) physicians in a number of ways, but especially through an emphasis on a set of “tenets” and treatment regimens.1 The four principles of osteopathic medicine are based on the philosophy that body systems are related and are dependent on each other for optimal health. The American Osteopathic Association’s official statement of the tenets is comprised of the following:
- The body is a unit; the person is a unit of body, mind, and spirit.
- The body is capable of self-regulation, self-healing, and health maintenance.
- Structure and function are reciprocally interrelated.
- Rational treatment is based upon an understanding of the basic principles of body unity, self-regulation, and the interrelationship of structure and function.1
Also unique to osteopathy is training in Osteopathic Manipulative Medicine (OMM), which is used to diagnose and treat a wide variety of conditions. From the beginning of medical school, osteopathic medical students are taught that philosophically distinct practices and principles will guide their unique approach to treatment as physicians.2
Over recent decades the osteopathic profession has undergone a steady and in many ways dramatic shift in its identity and broader place within American medicine.3,4 With more than a quarter of all medical students now training at osteopathic medical schools,5 and DOs normalized into the larger fabric of American health care, the profession appears to stand on increasingly firm ground, with greater recognition and respect from allopathic physicians.6 At the same time, a question confronts medicine regarding the distinctiveness of osteopathic physicians themselves. They are doing less OMM every year,7,8 and are practicing in mainstream, integrated environments where their osteopathic orientation may not play as prominent a role as it once did when DOs trained in osteopathic-specific residencies and practiced in osteopathic hospitals.9
Because osteopathic principles emphasize the importance of the musculoskeletal system to health and disease, DOs have long held prominent roles in sports medicine. For example, Phogg Allen, Kansas University’s acclaimed basketball coach, was an osteopathic physician who claimed he “won more games at the training table than on the sidelines”.10 Cecil Ferguson was a Major League Baseball (MLB) player who after his career ended trained as an osteopathic physician. A 1942 article called the “Miami osteopath” Ferguson, “a ‘Mr. Fix-It’ of the sports world”, adding that he
patched up some of the game’s greatest stars, including such luminaries as Bob Feller, Carl Hubbell, Gabby Hartnett and Johnny Mize, not to mention scores of top-notchers in other sports.11
Finally, the Detroit Red Wings employed John Finley, DO for over 40 years as their head team physician, beginning in 1953.12 Today, many of the most prominent professional team physicians, some of which were interviewed for this study, hold DO degrees.
Formed in 1976, the American Osteopathic Academy of Sports Medicine is the oldest osteopathic sports medicine organization. In 1992, osteopathic physicians became eligible to earn additional subspecialty board certification in sports medicine.13 Since then, the profession’s involvement with sports medicine has grown steadily. The 2020 American Association of Medical College’s (AAMC) Physician Specialty Data report indicates that while DOs make up 8.2% of the total active physicians in the United States across all specialties, Sports Medicine is relatively saturated with DOs. Amongst all specialties included in the report, sports medicine had the highest proportion of DOs at 18.9%.14 The American Osteopathic Academy of Sports Medicine publishes two clinically-focused academic journals, and DOs have a notable DO presence on the editorial boards of non-osteopathic sports medicine journals such as the Clinical Journal of Sport Medicine and The Physician and Sportsmedicine. The Academy maintains that an infusion of osteopathic principles and practice in sports medicine could lead to improved performance, a reduction in injuries and recovery time, and better competitive outcomes.13
Despite the long-standing interest and involvement in sports medicine by DOs, the existing literature examining the role of osteopathy is small. Scholars have examined the growing demand for non-physician osteopaths in sports medicine in the United Kingdom, finding a growing demand for osteopathy in sports and that its use increases the chances an athlete can remain fit and return rapidly from injury.15 A survey-based study by Kent et al found that 88% of the surveyed sports medicine physicians used complementary and alternative interventions in their practice.16 Of the 23 different alternatives to allopathic care, chiropractic and osteopathic manipulation was the most frequently reported adjunct to care, suggesting that OMM is prevalent in sports medicine. Within the realm of professional sports medicine, a study by Makhni et al provided a scholarly overview of injury reporting in four major North American professional sports leagues, finding significant variation within the four leagues.17 In that study, however, little attention was paid to the roles played by differently situated health professionals.
Somewhat surprisingly, given the profession’s steady and rapid growth, scholars have not yet examined the role that DOs play within sports medicine specifically. Considering the steady shifts DOs have undergone in their own professional trajectories and developments,6 such an examination is potentially important, not only to osteopathic medicine, but professional sports medicine itself. The present study seeks to understand the significance, if any, of being a DO in sports medicine, and the usefulness of the unique aspects of osteopathic training in treating athletes. Furthermore, beyond actual or potential benefits of the training, this qualitative thematic analysis explores how being a DO is viewed within the realm of professional sports medicine. The high stakes, visibility, and diversity of medical teams within professional sports offers an interesting space in which to assess the meaningfulness and clinical relevance of being a DO as opposed to an MD or other health professional.
Methods
After inviting all 29 of the osteopathic physicians we identified as currently working in North American professional sports medicine to participate in our study, the research team conducted 12 (41%) interviews. Though all major professional sports (baseball, basketball, football, hockey, and soccer) were represented in our study (See Table 1), we were unable, after several attempts, to interview the three osteopathic physicians currently working in women’s professional sports. Our sample set included one woman of the five currently working in the field. Interviews were conducted over a 45-day period, averaged 40 minutes in length and were guided by a semi-structured interview guide designed to better understand osteopathic physicians’ experiences in professional sports (See Appendix 1). The interviews were led by the fourth author with follow up and clarification directed by the other members of the research team. Interviewees were not compensated for their participation. This study received a 45 CFR 46.104(d) Category 2 exemption by the Ohio University Institutional Review Board (21-E-32). All participants provided informed consent and were aware that deidentified responses would be published.
 |
Table 1 Interviewee Affiliations & Years of Experience* |
Interviews were transcribed by a professional transcriptionist and uploaded to the team-coding software platform, Dedoose.18 This study employed thematic analysis, a widely recognized interpretive approach within content analysis that is particularly well-suited for analyzing qualitative texts to better understand thematic emergence.19 The first, second, and third authors coded the interviews to identify excerpts that could, in turn, serve as the basis of thematic analysis. While Neuendorf argues that fully developed codes can minimize research bias,20 we wanted our interpretive lens to arise from the data, and not the other way around. Accordingly, we have followed Cascio et al in establishing initial codes that we expected to arise,21 but then developed the majority of our codebook iteratively during the course of coding (“open coding”).22 Within the context of the present study, we believe this approach serves to minimize bias given this study’s parameters and aims. Our aim, which was to examine the interviews themselves, and not import preconceived notions into the study, required a high degree of openness to new concepts arising during the course of analysis. Code frequencies are reported to provide a sense of the prevalence of different themes within the codebook, but are not intended to serve as quantitative markers within our qualitative study. The team also utilized Dedoose’s memo writing feature to facilitate an iterative exchange of ideas and record insights that arose during coding. Coding was blinded so that each coder could not see other coders’ applications.
Results
Analysis yielded three main findings and a series of smaller findings.
DOs Feel Advantaged in Working with Patient-Players
All interviewees maintained that osteopathic training affords them a distinct advantage as sports physicians. This perceived advantage is a function of their training and an adherence to osteopathic philosophy, supplemented by training in OMM. See Table 2 for code frequencies and Table 3 for quote excerpts.
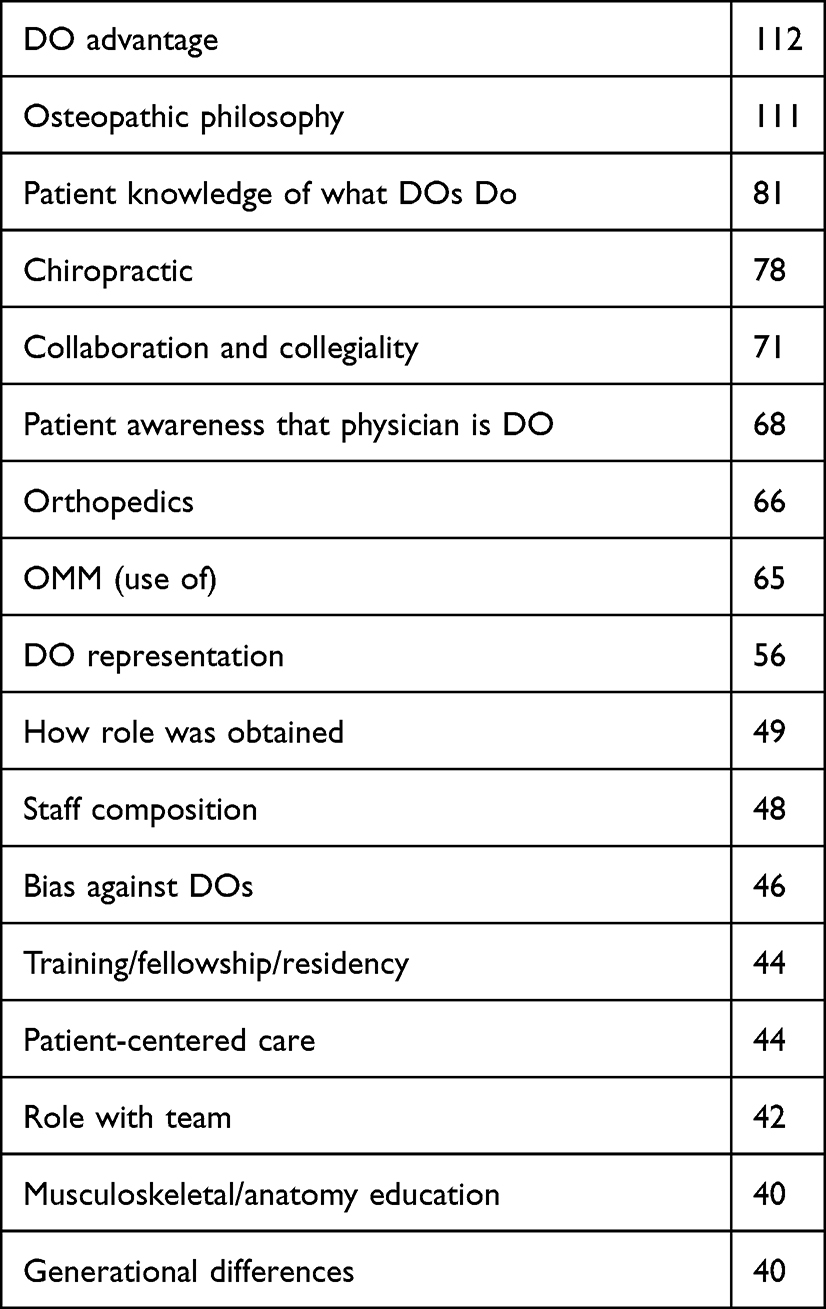 |
Table 2 Code Frequencies (> 40 Applications) |
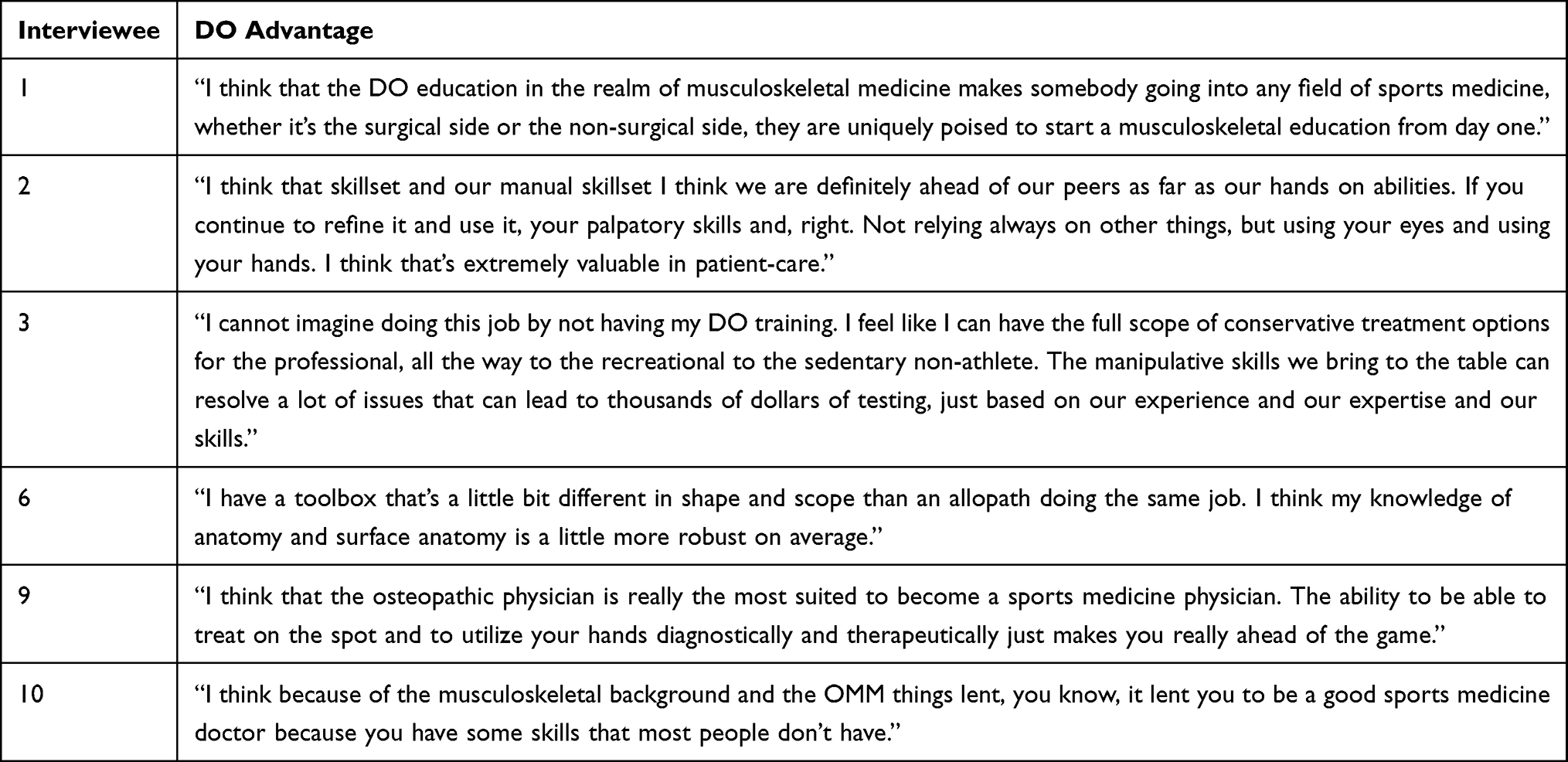 |
Table 3 Excerpts Asserting DO Advantage in Professional Sports |
The code co-occurrences of DO Advantage and Musculoskeletal/Anatomy Education provide conceptual insight into the basis of this perceived advantage (see Table 4). Multiple respondents offered that osteopathic medical education provided them with extensive musculoskeletal and anatomical training that some thought provided them an advantage in comparison to their allopathic and other health team colleagues. Interviewee 9 explained,
… I just think we know our musculoskeletal system better than allopathically trained physicians. You know your kinesiology, you understand your biomechanics, and so I think that the osteopathic physician is really the most suited to become a sports medicine physician. The ability to be able to treat on the spot and to utilize your hands diagnostically and therapeutically just makes you really ahead of the game.
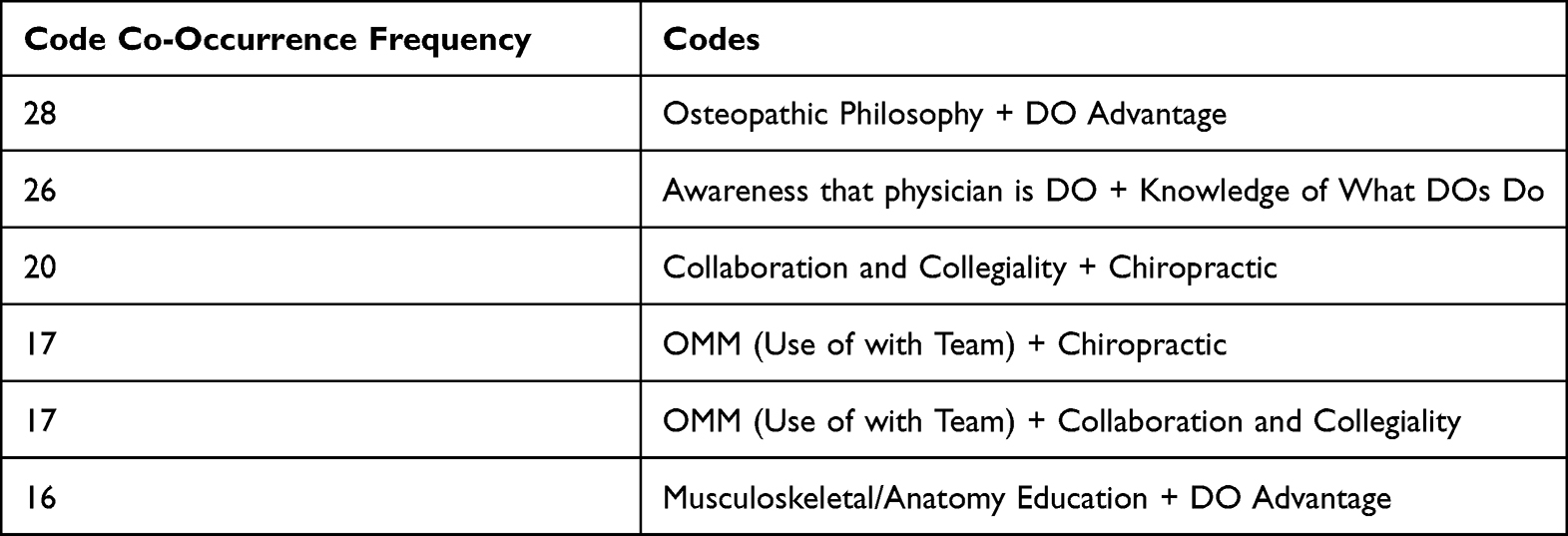 |
Table 4 Top Five Code Co-Occurrences (> 15) |
Interviewee 5 shared a similar perceived advantage in his work with NFL players. He stated,
these are big giant people and there’s definitely been a few cases where really, really good palpatory skills were helpful in figuring out what’s going on with someone whether it was a neck or a spine issue or something like that.
DO Identity is Secondary to Collegiality and Collaboration
DO identity arose often within the context of medical teams, especially as concerns the relationship between DOs and chiropractors, orthopedists, and the use of OMM. In this area, Use of OMM and Chiropractic co-occurred 17 times, and Collaboration & Collegiality and Chiropractic 20 times.
Despite being champions of OMM and osteopathic philosophy, DOs reported rarely advocating for the use of more OMM in team care. Interviewees valued OMM, but it did not play a central role in their work in professional sports. Interviewee 1 explained that OMM was “not a regular occurrence”, adding that “by the time a lot of patients come to me, they’ve been in physical therapy.” Interviewee 11, who worked with NHL and MLS teams noted that “I think OMM is always sort of, obviously, in the back of my mind … there’s definitely times where I think like, oh, this person might benefit from OMM.” Yet, just moments later, this physician clarified that they “did not do any OMM with the teams.” Interviewee 4 explained that the lack of OMM in his work with an NBA team was due to a division of labor that he felt was necessary to avoid sending mixed messages to players. Specifically, he explained that he did not want to confuse players, leading them to ask “why are you doing what [the team chiropractor] does? You are supposed to take care of my athlete’s foot.” In Interviewee 4ʹs view, chiropractic and OMM were similar enough to not warrant risking unclear messaging between players and the team’s medical staff.
Interviewees offered several different reasons for their muted approach to osteopathic techniques and approaches. First, we heard from Interviewee 3 about a need to present a unified message to players (and sometimes their agents), to “make sure they hear a consistent message from the same physicians” with the assumption that a different care philosophy, such as that which guides osteopathy, might complicate that messaging. Second, interviewees shared a sense that high pressure situations (such as playoffs) did not afford time for adhering to the tenets of osteopathic medicine such as self-regulation, self-healing, and health maintenance. As Interviewee 6 explained,
when the stakes are higher, if someone’s got sinus pressure in the preseason, I tell them, ‘Rub some dirt on it, and give it a couple of weeks, and you don’t get any antibiotics’. If you’re in game five of the second round of the playoffs, I’m getting my prescription pad out just like anybody else would, because the cost of the error of being wrong on delay in treatment becomes unnecessarily high in that circumstance.
Third, some junior members of care teams shared their sense that propriety and hierarchy required that they wait to champion osteopathic-specific treatments. For example, Interviewee 11 was hesitant to assert her commitment to osteopathic philosophy during her sports medicine fellowship, where, in contrast to her DO-predominant residency, “most everyone that I came in contact with was an MD.” She added,
I think if I’d had been there for longer, or if I wasn’t necessarily in training, and just trying to learn the basics in general, then I probably would have made that more of a thing.
And finally, we encountered a sense by some that chiropractors were just as good at manipulation as DOs. Interviewee 10, who works in Major League Baseball, told us,
there are certain things that our sports chiropractor does that I don’t do [like active release technique]. I do some myofascial things and some muscle energy type things. But he’s actually really good at it. And so, he’s also a DNS [Dynamic Neuromuscular Stabilization] certified instructor. So, for some of those things, I will send [players] over to him because he does it better than I do, you know. It’s that simple.
Regarding patient-player distinctions between OMM and chiropractic, Interviewee 10 also explained,
No. I think it’s more of, ‘Oh, you do manual therapy or you do manipulation,’ you know. I don’t think the player from their point of view–they just want someone that can do it. They don’t really care. And a number of them have, especially the high-level ones, they have a DO or chiropractor that they work with in off season very regularly. So, it’s very common to see that.
For this physician, DOs were regarded by patient-players as being trained in manipulation, but the distinction between chiropractic and osteopathic manipulation was rarely made clear.
In other cases, however, interviewees reported deferring to team chiropractors for manipulation despite the fact that they felt that their osteopathic training positioned them to do a qualitatively different or superior manipulation. Accordingly, OMM (Use of with Team) was closely aligned with Collaboration and Collegiality (17 code co-occurrences). For example, Interviewee 1 noted,
We have a pretty well-established chiropractic college in the area, and so there’s quite a few chiropractors. It’s not uncommon for a patient to quote-unquote ‘have a chiropractor’, so they have somebody that they see regularly.
DOs Feel That Being a DO is Not Particularly Known or Occupationally Relevant, and There is Little Discrimination
There was consensus among Interviewees that patient-players rarely know what makes DOs different and do not seem to even notice the letters “DO” after their name. Interviewee 9, who worked in basketball explained,
I’d be working on one of them before the game, and other players would stick their head in and, ‘Oh, hey, Doc, I didn’t know you were a chiropractor.’ And I said, ‘Well … ’ so I’d go through the educational process with them. And then, as they began to see that I was treating them during their preseason physicals, and I was interpreting their lab work and setting them up for their electrodiagnostics and so forth, then they came to view me more as really their primary care physician on the team.
Interviewee 1 offered an exception, noting,
I’ve had to explain it to a couple of players, and it was kind of initiated just because they asked–it was more recognizing that the letters behind my name were different than they had seen elsewhere.
This physician offered a “funny anecdotal story” about a soccer player who “was having some back and musculoskeletal stuff”, so I did some osteopathic manipulation, and he kind of quipped, “Are you trained to do this?” [Laughs] And so we have continually razzed him about that for the past two years.”
In addition, interviewees reported little bias against DOs within these professional contexts. In only one case did an interviewee express concern, not from management, but from an agent. Interviewee 8 explained,
There have been some positives and some negatives with that. We actually had one assistant general manager who used to be a player agent, and the environment for agents now is ‘best of everything–you need the best care. You need the best access. You need the best of everything’. And he, frankly, had concerns about that … it came up that, ‘Shouldn’t a medical director be an MD?’ Because he wasn’t as familiar with the DO, and he just wanted the marquee. He thought it looked better on the marquee, to be frank. But fortunately, my tenure and service … pushed that conversation aside …
In addition to the question of MD and other health professional bias against DOs, instances of “DO bias against MDs” are usually related to the question of DOs feeling advantaged in sports medicine because of their training. For example, as Interviewee 2 put it,
I think our training and our extra skillset helps us to just be better physicians and I believe strongly in our philosophy … But if you’re a good physician, you’re a good physician, whether you’re an MD or DO or whatever other initials you want to put after your name.
Interviewees report their sense that management often appears to not even be aware that their medical staff include DOs, and if they are aware, it is of little importance. As Interviewee 9 noted,
The organization themselves, I don’t think that they knew that I had osteopathic training. I think what they were made aware of is that I was a new breed of physician, and that I was sports medicine trained.
As Interviewee 4 explained,
To be very honest, I don’t know that even the administration, the owners and the management, really knew the difference between a DO and MD at that time. I think they just knew the kind of services and care we gave was excellent and that’s all they were really caring about.
MDs, of course, do know the difference between DOs and MDs, but even here, apropos of the discussion above, collegiality overrules difference. As one physician, working with a football team, noted,
it’s definitely not a we/them thing at all. It’s very much, you know, what’s your role and how we all fit in together. So, it definitely isn’t like, ‘Oh, those guys, oh, no, no.’ It’s none of that. It’s very collegial.
Though all interviewees reported finding OMM a useful skill, several reported never using it in their capacity as members of team medical staff.
Discussion
Understanding Perceived DO Advantage
DOs believe their osteopathic training puts them at an advantage in working with patient-players is unsurprising in sports medicine, where training is heavily focused on the musculoskeletal system. What is somewhat more surprising given the importance of osteopathy itself to the DOs we interviewed is that they reported rarely championing osteopathic techniques within care teams, evoking instead osteopathic “philosophies”, “principles”, and “tenets.” This qualitative, interview-based study provides a revealing snapshot of a profession in transition. While the past 25 years or so have seen rapid growth in the osteopathic profession, with DOs fully licensed in all 50 states and increasingly recognized as equivalent to MDs in training and practice, a paradoxical outcome of this legitimacy is a decrease, or at least tamping, of osteopathic identity itself. Our interviewees made clear that being a team physician is a tremendous honor that they must treat with care. One of the ways they care for this work is through assimilation, which requires participation in a team-based care philosophy and division of labor that may not allow for osteopathic-specific treatment such as OMM. This point echoes something we heard from several physicians, namely that it was important that they be seen in their position as physicians, not merely OMM technicians.
Champions of osteopathic philosophy are likely to find this downplaying of OMM disappointing, of course. Osteopathic medicine continues to undergo a repositioning of its aims in light of the move to a single accreditation system for US medical residencies, which also brought with it the end of most osteopathic-specific residencies, and other traditional mainstays of distinctiveness. The snapshot of professional sports this qualitative study offers suggests that pressures within multidisciplinary healthcare teams and cultures present another challenge to those for whom osteopathic distinctiveness is important. And yet, our data also remind us that the effect of these pressures is mixed, as the lack of discrimination and bias that DOs report is likely to be far more important to DOs than osteopathic distinctiveness. All indications are that DOs are respected members of the medical teams on which they serve.
While one anecdote revealed that agents and players tend to question DOs’ presence on medical teams based on the assumption that DOs graduated from less prestigious institutions, the majority of interviewees reported no such bias. Of course, this apparent lack of discrimination has a two-sided effect in that our interviewees also made clear that management, as well as their medical staff colleagues, not only did not see the presence of DOs as a negative, but did not seem to think of that presence at all. There was a sense among many of our interviewees that patient-players and even colleagues are sometimes altogether unaware that they are DOs. However, interviewees did offer that when, usually over some time, patient-players and colleagues did come to understand the unique aspects of their skillset, these physicians were able to employ osteopathic-specific techniques. For example, Interviewee 10, stated that when he started with the team “the manipulation thing became a big thing once people realized you could do it. When they have seen me work on some people, like, a low back or even a shoulder, and I do some manual medicine on it, all of a sudden they can throw or they can get their catcher’s crouch, they are amazed because they are like, “How did you do that?” The question, of course, is whether these physicians had enough time as team physicians to reach this point.
Osteopathic Identity and Orthopedic Surgery
Several interviewees evoked the rise of orthopedic surgery as a factor shaping the roles and identities of DOs within professional sports medicine. Several interviewees offered the strong and growing presence of orthopedic surgeons in professional sports as a rationale for the comparatively low representation of DOs in professional sports (29 of the total 703 physicians we identified are DOs). Though more DOs are seeking out and successfully gaining entrance into orthopedic surgery residencies and fellowships, orthopedic surgery remains an MD dominated field, with 2021 National Resident Matching Program data indicating that 107/866 (12%) residency spots were filled by DOs. As recently as 2018, that number was 4/738 (0.4%), which suggests a rapid increase in DO acceptance to these programs.23 Underlying these trends is a shift in team composition itself, as several interviewees noted that even twenty years ago many teams’ medical staff were led by generalists. Today, however, primary care and internal medicine have largely given way to orthopedic surgeons in professional sports medical staff.
We did not identify any DO-trained orthopedic surgeons in professional sports, though we did interview two DOs that work at an orthopedic practice. A snapshot of the representation within the broader physician population can be gleaned by assessing the AAMC’s Physician Specialty Data Report. According to the AAMC, in 2019 8.2% of the physicians in the United States were DOs, while only 5.6% of orthopedic surgeons were DOs.14 The combination of DOs being underrepresented in both professional sports medicine and the dominant speciality within it, orthopedic surgery, explains some of our findings and simultaneously raises new questions.
This low ratio of DOs in professional sports poses a question: where will osteopathic physicians stand within professional sports in the future? Interviewee 3, a DO working in professional hockey offered,
I think a lot of teams center the team physician from the orthopedic perspective, whereas we were very fortunate to set it up from the primary care sports medicine perspective, with orthopedic support. Generally, I think a lot of teams start with a strong orthopedic surgeon who then builds a team. So, they may not recognize the value of osteopathic training.
The fact that DOs are not only a minority within professional sports medicine, but disproportionately represented given the ratio of DOs-to-MDs in practice, may explain why DOs are willing to set aside their unique skill set and prioritize assimilation within the majority group of MD orthopedic surgeons.
Osteopathic Manipulation and Chiropractic
As we have explained, the ubiquity of chiropractors on medical teams within professional sports, and players’ familiarity with chiropractors generally, means that osteopathic physicians must be thoughtful in how they assert themselves vis-á-vis manipulation. Osteopathic manipulation and chiropractic are, of course, distinct approaches, which means that many DOs see this conflation as a category mistake. But again, our interviews suggest a pragmatic concern with collegiality and uniformity in messaging when working with players often overrules any temptation DOs may have in asserting their particular and unique skill set. In some cases, chiropractic and OMM were presented by interviewees as complementary, with chiropractors referring player-patients to DOs when chiropractors recognized an opportunity to leverage the osteopathic approach. The same complement existed on the part of DOs, who reported referring player-patients to team chiropractors when the DO believed that chiropractic would provide superior care. This kind of collegiality is not surprising, of course, but we find it noteworthy, especially given that OMM is a central part of osteopathic training and, for many DOs, including those whom we interviewed, an important part of their medical skillset.
This qualitative study is not without limitations. The small sample size of 12 physician interviews provides only a snapshot of the complicated world of osteopathic identity in professional sports. In the future, larger sample sizes could provide more information and a more nuanced picture of DO experience. As we have noted, however, the total sample of osteopathic physicians working within professional sports is itself small, making the focus of this study inherently narrow. Finally, as is the case with all small-sample qualitative studies, findings may not be applicable to all osteopathic physicians. As the osteopathic medical profession itself is rapidly growing and changing, it is also likely that the findings reported here will need to be updated from time to time.
Conclusion
While this qualitative study draws on a small sample of DOs working with teams in North American professional sports, the consensus views shared by interviewees provide a snapshot of a unique professional crossroads for osteopathic medicine. The DO identity has long been double-edged, seeking legitimacy and recognition from mainstream medical professionals and institutions, on the one hand, but asserting difference and distinction, on the other. This study confirms that in navigating the complexities of osteopathic identity, osteopathic physicians working in professional sports have veered toward assimilation, downplaying what has historically distinguished them from not only other medical professionals, but non-medical health professionals such as chiropractors as well. While the near-absence of bias towards DOs is of course something the profession will celebrate, the absence of this bias appears to have been achieved by downplaying what is historically distinctive about osteopathic medicine itself. This is in spite of the fact that some DOs appear to harbor bias against their MD counterparts, a view that appears to be rooted in the perceived “DO advantage” we documented. In these regards, osteopathic physicians’ experiences within professional sports appear to be similar to the contemporary experience of DO students in medical school, those applying for residencies under the new dual MD-DO accreditation system, and also generally to the broader profession. Though some DOs steeped in osteopathic history and philosophy may find these results disappointing, the results do suggest a future in which DOs may be increasingly a part of the medical mainstream in professional sports medicine and beyond.
Acknowledgment
The authors would like to thank the three anonymous peer reviewers and OAJSM editor for providing helpful feedback that greatly improved the manuscript. The authors are also appreciative to the Office of Research and Grants at Ohio University's Heritage College of Osteopathic Medicine for providing generous support for this open access publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Osteopathic Association (AOA). Tenets of osteopathic medicine. Available from: https://osteopathic.org/about/leadership/aoa-governance-documents/tenets-of-osteopathic-medicine/.
2. Cotton A. Osteopathic principles in the modern world. Intl J Osteo Med. 2013;16(1):17–24. doi:10.1016/j.ijosm.2012.10.002
3. Phillips AR. Professional identity in osteopathy: a scoping review of peer-reviewed primary osteopathic research. Int J Osteopath Med. 2022;2022. doi:10.1016/j.ijosm.2022.06.005
4. Skinner D, Esber T, Walkowski S. Evocations of osteopathy’s founder and questions for contemporary osteopathic professional identity: a thematic analysis. Int J Osteopath Med. 2022. doi:10.1016/j.ijosm.2022.08.001
5. American Osteopathic Association. 2022 report tracks increased growth in the osteopathic profession. Available from: https://osteopathic.org/about/aoa-statistics/#:~:text=The%20osteopathic%20medical%20profession%20is,choosing%20to%20pursue%20osteopathic%20medicine.
6. Gevitz N. The DOs: Osteopathic Medicine in America.
7. Shannon SC, Teitelbaum HS. The status and future of osteopathic medical education in the United States. Acad Med. 2009;84(6):707–711. doi:10.1097/ACM.0b013e3181a43be8
8. Shubrook JH, Dooley J. Effects of a structured curriculum in osteopathic manipulative treatment (OMT) on osteopathic structural examinations and use of OMT for hospitalized patients. J Am Osteopath Assoc. 2000;100(9):554–558.
9. Gimpel J, Belanger S, Knebl J, et al. United States osteopathic medical regulatory summit: consensus, recommendations, and next steps in defining osteopathic distinctiveness. J Osteo Med. 2020;120(1):35–44. doi:10.7556/jaoa.2020.005
10. Johnson SM. Phog: The Most Influential Man in Basketball. Lincoln: University of Nebraska Press; 2016:259.
11. Oliver W. Dixie Sports huddle, Asheville (North Carolina) Citizen-Times, June 20, 1942: 10, quote in Jeff Findley, “Cecil Ferguson”, American Society for Baseball Research. Available from: https://sabr.org/bioproj/person/cecil-ferguson.
12. The DO. In memoriam: John Finley, DO, Detroit Red Wings physician; 2022. Available from https://thedo.osteopathic.org/2017/04/in-memoriam-john-finley-do-revered-detroit-red-wings-physician/.
13. American Osteopathic Academy of Sports Medicine (AOASM). Board certification: the future of sports medicine. Available from: https://www.aoasm.org/page/Board_Certification.
14. American Association of Medical Colleges (AAMC). Active physicians with a doctor of osteopathic medicine (DO) degree by specialty; 2019. Available from: https://www.aamc.org/data-reports/workforce/interactive-data/active-physicians-doctor-osteopathic-medicine-do-degree-specialty-2019.
15. Betser J, Cook S. The developing role of osteopaths in sport. SportEX Med. 2009;42:7–12.
16. Kent JB, Tanabe KO, Muthusubramanian A, Statuta SM, MacKnight JM. Complementary and alternative medicine prescribing practices among sports medicine providers. Altern Ther Health Med. 2020;26(5):28–32.
17. Makhni EC, Buza JA, Byram I, et al. Sports reporting: a comprehensive review of the medical literature regarding North American professional sports. Phys Sportsmed. 2014;42(2):154–162. doi:10.3810/psm.2014.05.2067
18. Dedoose Version 9.0.17. Los Angeles, CA: SocioCultural Research Consultants, LLC; 2021.
19. Peterson BL. Thematic analysis/interpretive thematic analysis. In: Matthes J, Davis CS, Potter RF, editors. The International Encyclopedia of Communication Research Methods. Wiley-Blackwell; 2017.
20. Neuendorf KA. The Content Analysis Guidebook. Thousand Oaks, CA: Sage Publications; 2002.
21. Cascio MA, Lee E, Vaudrin N, Freedman DA. A team-based approach to open coding: considerations for creating intercoder consensus. Field Methods. 2019;31(2):116–130. doi:10.1177/1525822X19838237
22. Charmaz K. Constructionism and the grounded theory. In: Holstein AJ, Gubrium JF, editors. Handbook of Constructionist Research. The Guilford Press; 2008:397–412.
23. National Resident Matching Program. Results and data: 2021 main residency match; 2021. Available from: https://www.nrmp.org/wp-content/uploads/2021/05/MRM-Results_and-Data_2021.pdf.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.