Back to Journals » OncoTargets and Therapy » Volume 12
A temperature-sensitive phase-change hydrogel of topotecan achieves a long-term sustained antitumor effect on retinoblastoma cells
Authors Huo Y, Wang Q, Liu Y, Wang J, Li Q, Li Z ![]() , Dong Y, Huang Y, Wang L
, Dong Y, Huang Y, Wang L
Received 30 April 2019
Accepted for publication 8 July 2019
Published 30 July 2019 Volume 2019:12 Pages 6069—6082
DOI https://doi.org/10.2147/OTT.S214024
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr William C. Cho
Yan Huo,1,2,* Qun Wang,1,* Ying Liu,1 Junyi Wang,1 Qian Li,1 Zongyuan Li,1 Yan Dong,1 Yifei Huang,1 Liqiang Wang1
1Department of Ophthalmology, The 1st Medical Center Of Chinese PLA General Hospital, Beijing 100853, People’s Republic of China; 2The Institutional Animal Care and Use Committee of National Beijing Center for Drug Safety Assessment, Institute of Pharmacology and Toxicology, Academy of Military Medical Sciences, Beijing 100850, People’s Republic of China
*These authors contributed equally to this work
Background: Retinoblastoma (Rb) is one of the most common malignancies among children. Following early diagnosis and prompt treatment, the clinical outcome or prognosis of Rb is promising. However, the prognosis or survival rates of patients with late-stage Rb remain poor. Current therapeutic strategies for advanced Rb mainly involve the use of advanced chemotherapeutic options. However, the efficacy of these strategies is not satisfactory. Therefore, the development of novel strategies to achieve a more effective antitumor effect on late-stage Rb is of crucial importance.
Methods and materials: Topotecan was dissolved in phosphate-buffered saline and prepared into a temperature-sensitive phase-change hydrogel (termed Topo-Gel). Moreover, Topo-Gel was injected into tumor tissues formed by Y79 cells (an Rb cell line) in nude mice to examine the long-term release and long-acting antitumor effect of Topo-Gel on Rb tumors.
Results: Topo-Gel transforms from liquid to a hydrogel at near body temperatures (phase-change temperature [T1/2] was 37.23±0.473 °C), and maintains the slow release of topotecan in Rb tumor tissues. Following the subcutaneous injection of Topo-Gel, the treatment induced long-acting inhibition of tumor growth and relieved the adverse effects associated with topotecan. Topo-Gel, a temperature-sensitive phase-change hydrogel, is a slow-release system that prolongs the presence of topotecan in Rb tissues, and preserves the efficacy of topotecan in the long term.
Conclusion: Preparation of topotecan into a temperature-sensitive phase-change hydrogel achieves a long-term sustained antitumor effect on Rb cells, and may be a useful strategy for the treatment of intraocular Rb.
Keywords: retinoblastoma, temperature-sensitive phase-change hydrogel, slow-release system, long-acting antitumor effect
Introduction
Retinoblastoma (Rb) is one of the most common malignancies among children. Following early diagnosis and prompt treatment, the clinical outcome or prognosis of Rb is promising.1–4 However, the prognosis or survival rates of patients with late-stage Rb remains poor.5–7 Current therapeutic strategies for advanced Rb mainly include the use of advanced chemotherapeutic agents, such as melphalan (Alkeran) or topotecan.8–11 However, the efficacy of these drugs in the treatment of advanced Rb is not satisfactory.12,13 Moreover, Rb occurs in children, and these patients have weaker body functions compared with adults.14,15 The adverse effects of long-term chemotherapy on the health of children cannot be ignored. Of note, the oral or intravenous administration of chemotherapy can lead to the widespread distribution of the drugs to various organs throughout the body. This results in insufficient effective concentrations of the chemotherapeutic drugs in local tumor tissues. Therefore, the preparation of a novel sustained-release formulation of antitumor drugs is of great importance. This approach allows direct intratumoral injection of drugs, which avoids adverse effects or damage to organs of the whole body. In addition, the drugs can exert long-term effects after a single administration, and the approach can improve the compliance of patients receiving antitumor treatment.
Currently, the most commonly used drugs against Rb are carboplatin, etoposide, vincristine, melphalan, or topotecan. Carboplatin, etoposide, and vincristine are widely used in antitumor therapy of Rb, and are administered via intravenous drips.16,17 Melphalan or topotecan can be used to treat Rb via intra-arterial chemotherapy (IAC).8–10 During intra-arterial chemotherapy, melphalan or topotecan is injected into the tumor tissue in the eye via the ophthalmic artery. Injections of melphalan or topotecan are in the form of solutions that could lead to the complete and rapid clearance of tumor tissues. This results in the short duration of the efficacy of drugs, leading to the requirement for multiple or frequent doses. Therefore, it is valuable to investigate and develop new pharmaceutical formulations that can offer the sustained release of drugs in the tumor tissues, and ultimately provide long-term antitumor efficacy of drugs through a single/one-time administration.
Topotecan is easier to dissolve in water compared with melphalan. The establishment of a topotecan formulation can result in the administration of a larger dose of topotecan in a smaller volume versus that of melphalan. In the present study, a temperature-sensitive phase-change hydrogel of topotecan (Topo-Gel) was prepared. Topo-Gel was directly injected into tumor tissues to examine the duration of its antitumor effect on Rb cells.
Materials and methods
Cell culture and agents
The Rb cell line Y79 was purchased from the National Infrastructure of Cell Line Resource, Chinese Academy of Medical Sciences (Beijing, China), an organization possessing typical biological samples of the Chinese government. Cells were cultured in Dulbecco’s modified eagle medium (Thermo Fisher Scientific Corporation, Waltham, MA, USA), supplemented with 20% fetal bovine serum (Thermo Fisher Scientific Corporation, Waltham, MA, USA) in an incubator at 37 °C and 5% CO2. Topotecan (Cat. No.: S1231) was purchased from Selleck Corporation, Houston, Texas, USA.
Preparation of topotecan formulations
The formulations of topotecan were prepared as described by Wang YL et al and Tang ZG et al (2018).18,19 Briefly, topotecan was fully solubilized in phosphate-buffered saline (PBS) to produce a topotecan solution (termed Topo-Sol). Subsequently, Topo-Sol was repeatedly filtrated using a 0.1-μm micron filter, and termed topotecan solution-1 (Topo-Sol-1). A temperature-sensitive phase-change hydrogel of topotecan (termed Topo-Gel) was generated by mixing Topo-Sol with poloxamer 407 (FREDA Corporation, Jinan City, People’s Republic of China). The topotecan in the formulations was examined using liquid chromatograph mass spectrometer/mass spectrometer (LC-MS/MS) methods, as described by Ye et al (2013), Li et al (2010), Holleran et al (2010), and Muenster et al (2008).20–23
For the phase-transition experiments, topotecan was prepared into Topo-Gel and Topo-Gel was incubated at the indicated temperature. To examine the effect of pH on the phase-transition of Topo-Gel, topotecan was diluted using physiological saline at the indicated pH values (6.6, 6.8, 7.0 or 7.2), and fixed with poloxamer 407 to produce the Topo-Gel. Subsequently, Topo-Gel was incubated at the indicated temperature for the phase-transition or in vitro release experiments.
The in vitro release of topotecan from Topo-Gel was examined. Topo-Gel (100 μl) was placed in an EP (eppendorft) tube, incubated at 37 °C for approximately 5 mins. Subsequently, physiological saline (~900 μl) was slowly added, and the solution was incubated at 37 °C. Topo-Gel samples were collected daily for LC-MS/MS, and the in vitro release profile of Topo-Gel was determined based on the sustained presence of topotecan in the hydrogel (topotecan in Topo-Gel can be released into physiological saline).
Release of topotecan from Topo-Gel or clearance of topotecan from tumor tissues injected with Topo-Gel
All animal experiment protocols were approved by the Institutional Animal Care and Use Committee of National Beijing Center for drug safety assessment, Institute of Pharmacology and Toxicology, Academy of Military Medical Sciences, Beijing, China (Certification ID: IACUC-2019–002). All procedures were performed in accordance with the UK Animals (Scientific Procedures) Act of 1986 and associated guidelines. The preparation of samples was performed as described by Wang et al (2018) and Xie et al (2018).18,19 LC-MS/MS experiments were performed, and the curves of sustained topotecan presence in tumor tissues were obtained through calculations as described by Ye et al (2013), Li et al (2010), Holleran et al (2010), and Muenster et al (2008).20–23 Briefly, Y79 cells were cultured and injected into the left hind limb sites of nude mice to form subcutaneous tumors. Following the growth of subcutaneous tumors to a volume of approximately 1,500–2,000 mm3, intratumoral administration (intratumoral injection) experiments were performed. Animals (nude mice) were divided into the following three groups: solvent control injection, Topo-Sol injection, and Topo-Gel injection. Agents were directly injected into subcutaneous tumors in nude mice, and each tumor was injected with approximately 50 μl of liquid. Animals were harvested and tumor tissues were collected. The tissues were milled using liquid nitrogen, and the topotecan in the tissue was extracted using acetonitrile. The amount of topotecan was examined using LC-MS/MS.
In vivo antitumor effects of Topo-Gel on Rb tissues formed by Y79 cells
BALB/c nude mice (thymus-deficient) were purchased from SI-Bei-Fu Corporation, Beijing, China. Y79 cells were injected into nude mice to form subcutaneous tumors.24–26 When the tumor volumes reached 1,000–1,200 mm3, the mice received oral administration of topotecan or an intratumoral injection with topotecan formulations. For the oral administration of topotecan, the mice received a gastrointestinal administration of the indicated dose of topotecan (ie, 3 mg/kg, 2 mg/kg, 1 mg/kg, or 0.5 mg/kg) over the course of 2 days. For the intratumoral injection of topotecan formulations, the solvent control, Topo-Sol, or Topo-Gel was directly injected into the subcutaneous tumors. After 14–20 days, the mice were sacrificed via cervical dislocation, and tumors were harvested. Tumor weights were measured using precision balances, and tumor volumes were calculated as length × width × width/2.
Western blotting
Subcutaneous tumors received an intratumoral injection of Topo-Sol or Topo-Gel. After 2–3 weeks, subcutaneous tumors were harvested and protein samples were extracted. The protein levels of Pro-PARP, cleaved-PARP, and CHEK1, or the phosphorylation of CHEK1 (S296 and S345 points) were determined through Western blotting experiments as described by Liang et al (2017) and Ji et al (2017).27,28
The adverse effects of topotecan formulations on the body health of mice
Nude mice, which were injected with Y79 cells to form subcutaneous tumors, received an oral administration of topotecan, or an intratumoral injection of Topo-Sol or Topo-Gel. After 2–3 weeks of treatment, the body weight, hematological parameters, and mass of the main organs were examined.
Statistical analysis
A statistical analysis was performed through the Bonferroni correction with a two-way analysis of variance using the SPSS Statistics software (IBM Corporation, Armonk, NY, USA). The T1/2 value of the hydrogel was calculated using the Origin software (Version No 6.1; OriginLab Corporation, Northampton, MA, USA). A P<0.05 denoted statistical significance between groups.
Results
Preparation and identification of topotecan solutions
Initially, the characteristics of topotecan formulations were examined using LC-MS/MS. As shown in Figure 1, topotecan can be easily dissolved in PBS to produce a topotecan solution (termed Topo-Sol). The concentration of topotecan in Topo-Sol was >30 mg/ml (30.05±1.25 mg/ml). Subsequently, the uniformity of Topo-Sol and the dissolution of topotecan in Topo-Sol were examined. Topo-Sol was filtered using a 0.1-μm pore size filter to extract potential undissolved topotecan microparticles. As shown in Figure 1A–D, there was no significant difference between the concentrations of topotecan in Topo-Sol and Topo-Sol-1 (Topo-Sol after multiple filtrations using a 0.1-μm aperture). The concentration of topotecan in Topo-Sol-1 was 30.14±1.33 mg/ml (Figure 1D). The results are shown as images from the LC-MS/MS or quantitative analysis. Therefore, it was concluded that the topotecan solution was successfully prepared, and topotecan is fully soluble or highly soluble in PBS.
 |
Figure 1 Concentration of topotecan in the solution. Topotecan was dissolved in PBS to form a solution (termed Topo-Sol). Topo-Sol was filtered using a 0.1-μm pore diameter filter membrane, and the resultant solution was termed Topo-Sol-1. Topotecan was extracted from the solutions using acetonitrile for investigation through LC-MS/MS. The results are shown as images of LC-M/MS for the solvent control (A), Topo-Sol (B), Topo-Sol-1 (C), and concentration of topotecan in the solutions (D). *P<0.05. |
Preparation of topotecan hydrogel and the in vitro release of topotecan from the topotecan hydrogel
Subsequently, the solution of poloxamer 407 dissolved in PBS was prepared at 10 °C. Topo-Sol was added and the poloxamer 407 solution was stirred at 10 °C. The apparent viscosity (η [Pa/s]) of Topo-Gel containing different doses of poloxamer 407 as a function of temperature (°C) was examined to reveal whether the topotecan hydrogel (termed Topo-Gel) could transform from the liquid form to a hydrogel form. In addition, the phase-transition temperature (T1/2) of Topo-Gel was calculated based on the apparent viscosity-temperature curves. As shown in Figure 2 and Table 1, Topo-Gel can transform from a liquid to a hydrogel, and the T1/2 value of Topo-Gel containing 10.0% poloxamer 407 was similar to body temperature. Therefore, a 12.5% concentration of poloxamer 407 was used for the subsequent steps of the experiment. Moreover, there was no significant difference in the T1/2 value of Topo-Gel with a 10.0% concentration of poloxamer 407 at the indicated pH (Figure 3 and Table 2). Topotecan did not alter the phase-transition temperatures of topotecan hydrogel with added poloxamer 407 (Table S1).
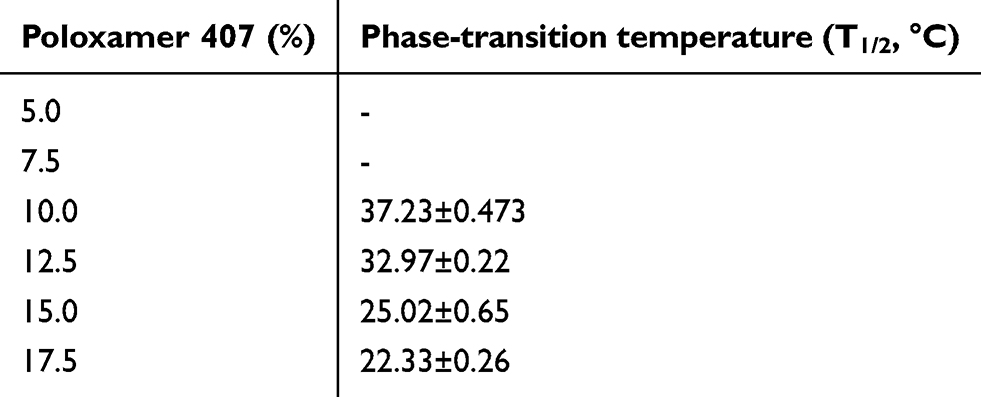 |
Table 1 Phase-transition temperatures of Topotecan hydrogel with indicted Poloxamer 407 |
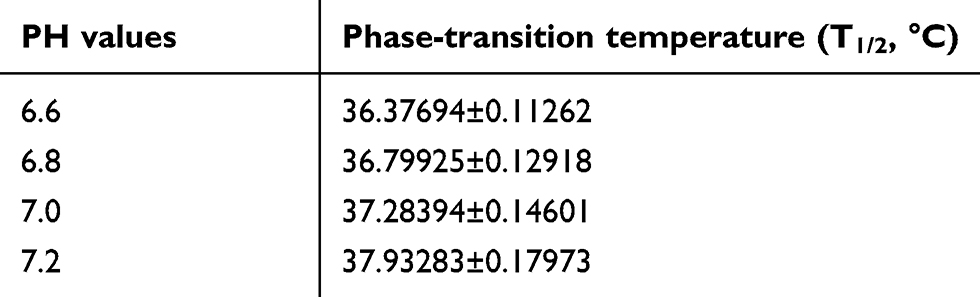 |
Table 2 Phase-transition temperatures of Topo-Gel with 10% Poloxamer 407 at indicated PH-value |
 |
Figure 2 Phase-transition of the topotecan hydrogel with indicated concentration of poloxamer 407. The apparent viscosity (η [Pa/s]) of Topo-Gel containing different doses of poloxamer 407 as a function of temperature (°C) was examined. The apparent viscosity-temperature curves of the topotecan hydrogel with 5% (A), 7.5% (B), 10% (C), 12.5% (D), 15% (E), or 17.5% (F) poloxamer 407 are shown. |
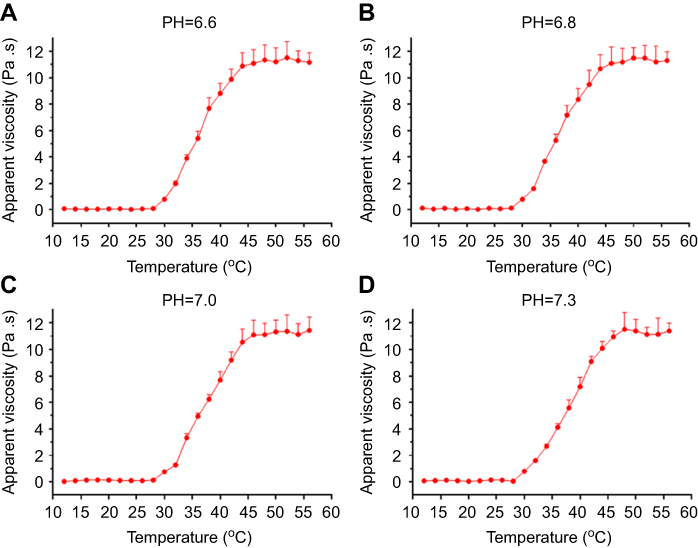 |
Figure 3 Phase-transition of the topotecan hydrogel with 10% poloxamer 407 at indicated pH values. The apparent viscosity (η [Pa/s]) of Topo-Gel containing 10% poloxamer 407 dose as a function of temperature (°C) was examined. The apparent viscosity-temperature curves of the topotecan hydrogel with 10% poloxamer 407 at pH=6.6 (A), pH=6.8 (B), pH=7.0 (C), or pH=7.2 (D) are shown. |
Subsequently, the in vitro release of topotecan from Topo-Gel was determined to examine whether topotecan prepared as Topo-Gel resulted in the slow release of topotecan. As shown in Figure 4, Topo-Gel achieved the long-term sustainability of topotecan. The presence of topotecan was sustained in Topo-Gel for >400 h. The half-life time (t1/2 value) of topotecan release from Topo-Gel was 151.94±19.32 h. Moreover, there was no significant difference in the t1/2 value of topotecan release from Topo-Gel at different pH values (Table 3). Therefore, the preparation of the Topo-Gel formulation achieved the long-term sustainability of topotecan in Topo-Gel.
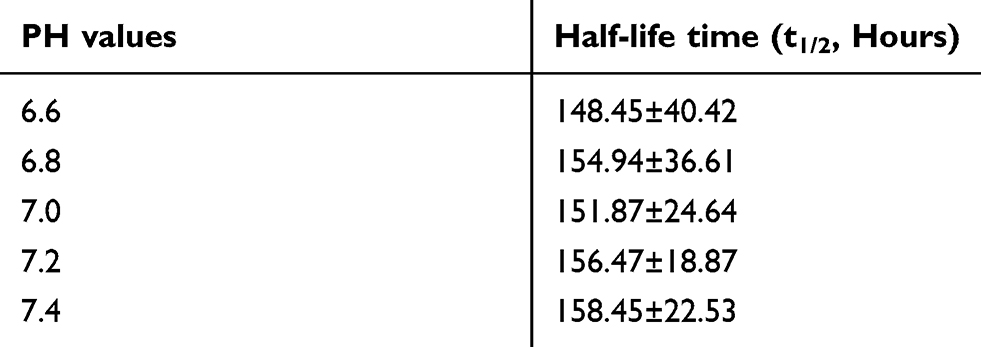 |
Table 3 Half-life time of Topotecan releasing from Topo-Gel at indicate PH-values |
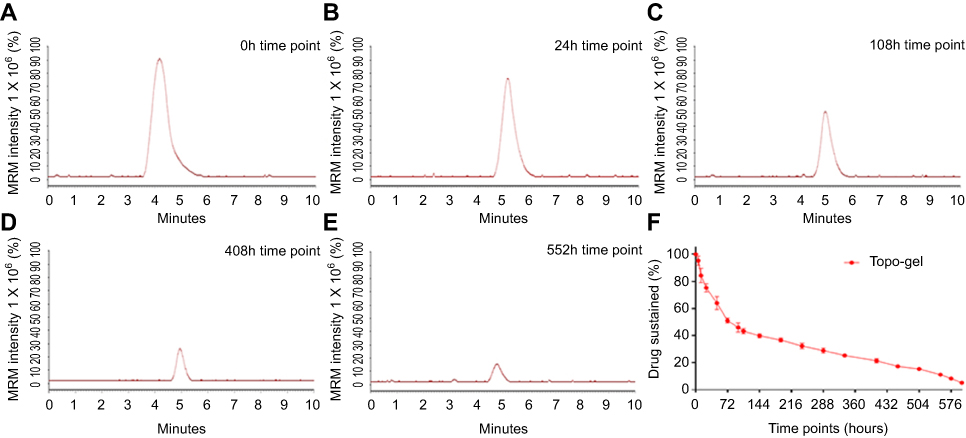 |
Figure 4 In vitro release of topotecan from the hydrogel (Topo-Gel). The in vitro release of topotecan from the hydrogel (Topo-Gel) was examined at indicated time points through LC-MS/MS. The results are shown as images of the LC-MS/MS results (A–E) and the drug-sustaining curve of topotecan in Topo-Gel (F). |
In vivo release of topotecan from tumor tissues injected with topotecan formulations
Subcutaneous tumors were formed by injecting Y79 cells into nude mice to further assess the slow-release of Topo-Gel. Subsequently, topotecan formulations were directly injected into the subcutaneous tumor tissues, and tumors were harvested for LC-MS/MS to examine the sustainability of topotecan. As shown in Figure 5, topotecan was almost completely removed from subcutaneous tumors within 48 h after injection of Topo-Sol. The t1/2 value of topotecan in tumor tissues after injection of Topo-Sol was 10.07±1.10 h. An injection of Topo-Gel resulted in long sustainability or slow release of topotecan in subcutaneous tumor tissues (t1/2 value: 94.07±11.58 h). Following the injection of Topo-Gel, topotecan was detected in tumor tissues, even after 408 h.
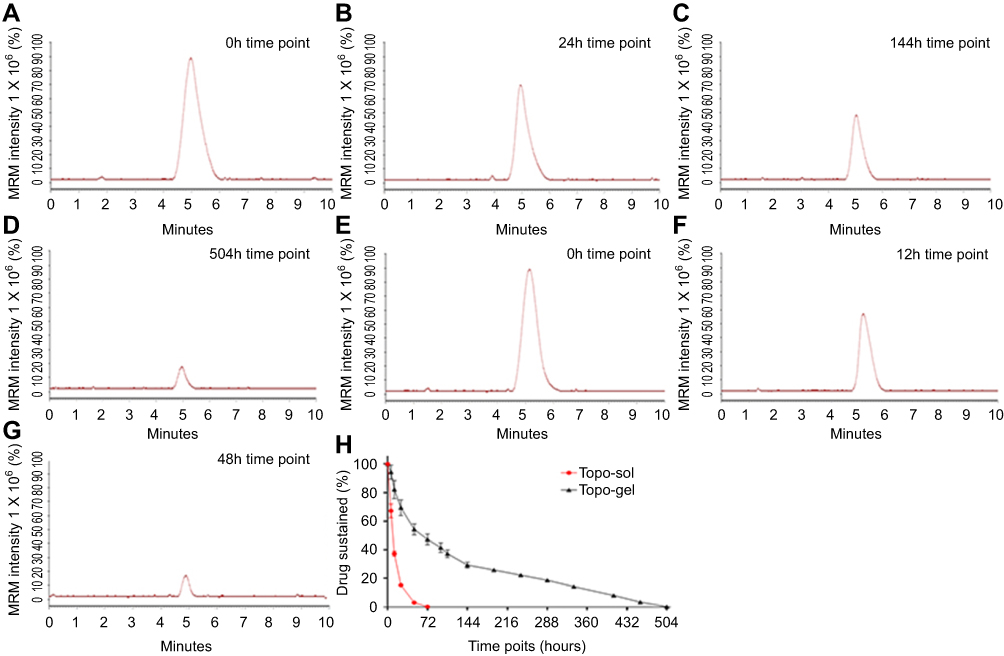 |
Figure 5 In vivo release of topotecan from tumor tissues injected with topotecan formulations. Y79 cells were injected into nude mice to form subcutaneous tumors. Topotecan formulations (Topo-Gel, Topo-Sol) were injected into tumor tissues. At each time point, subcutaneous tumors were harvested for investigation through LC-MS/MS. The results are shown as images of the LC-MS/MS results (A–G) from the Topo-Gel injection group (A–D) or Topo-Sol group (E–G), and the drug-sustaining curve of topotecan in tumor tissues (H). |
The concentration of topotecan in the blood of nude mice after intratumoral injection of the topotecan formulations was also examined. As shown in Figure 6, after injection of Topo-Sol, topotecan was rapidly cleared from the tumor tissue, and its blood concentration peaked at the 12-h time point (Figure 6). After injection of Topo-Gel, the clearance of topotecan from the tumor tissues was extremely slow, and its concentration in the blood was constantly low (Figure 6). Notably, topotecan was detected in the blood >400 h after injection (Figure 6). The peak concentration of topotecan after an intratumoral injection of Topo-Sol was almost 72.85-fold higher than the peak concentration of topotecan after an intratumoral injection of Topo-Gel. Therefore, the preparation of topotecan into Topo-Gel achieved the long sustainability of topotecan in tumor tissues.
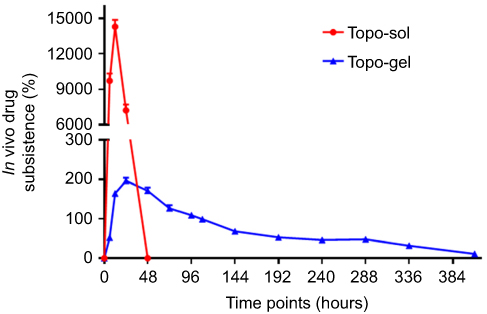 |
Figure 6 In vivo release of topotecan from tumor tissues injected with topotecan formulations – measurement of the concentration of topotecan in the blood. Y79 cells were injected into nude mice to form subcutaneous tumors. Topotecan formulations (Topo-Gel, Topo-Sol) were injected into tumor tissues. At each time point, blood was harvested for investigation through LC-MS/MS. The results are shown as the concentration curve of topotecan in the blood of nude mice. n=10 for each group at each time point. |
Injection of Topo-Gel induced the long-acting antitumor effect of topotecan
The aforementioned results showed that an injection of Topo-Gel could induce the long sustainability or slow release of topotecan. Topotecan formulations were injected into subcutaneous tumors to further examine whether an injection of Topo-Gel could achieve the long-acting feature of topotecan. As shown in Figure 7, a single injection of Topo-Sol did not inhibit the subcutaneous growth of Y79 cells in nude mice. In contrast, a single injection of Topo-Gel significantly inhibited the subcutaneous growth of Y79 cells in nude mice. Moreover, the results of the Western blotting analysis showed that, unlike Top-Sol, a single injection of Topo-Gel enhanced the cleavage of PARP. Unlike Topo-Sol, an injection of Topo-Gel induced the phosphorylation of CHEK1 at the S296 or S345 residue (Figure 8). Therefore, the direct injection of Topo-Gel into tumor tissues achieved the long-acting antitumor effect of topotecan.
 |
Figure 7 Investigation of the long-acting antitumor effects of the topotecan formulations in the Rb subcutaneous tumor model. Y79 cells were injected into nude mice to form subcutaneous tumors. A single injection of solvent control (PBS), blank hydrogel (PBS with 10% poloxamer 407), or topotecan formulations (Topo-Gel, Topo-Sol) was performed into tumor tissues. After 3–4 weeks of growth, tumors were harvested, and tumor volumes and weights were calculated. The results are shown as (A) tumor images, (B) tumor volumes, (C) inhibition rates from tumor volumes, (D) tumor weights, and (E) inhibition rates from tumor weights. *P<0.05. |
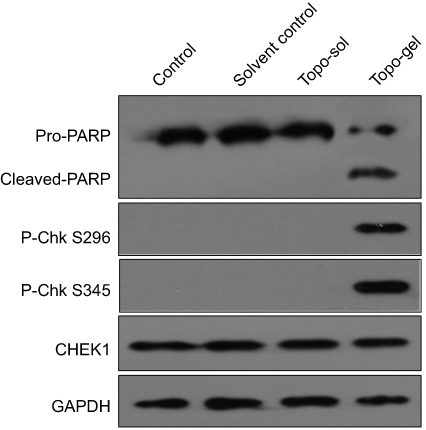 |
Figure 8 Investigation of the long-acting antitumor effect of topotecan formulations in the Rb subcutaneous tumor model through Western blotting. Y79 cells were injected into nude mice to form subcutaneous tumors. A single injection of solvent control (PBS), blank hydrogel (PBS with 10% poloxamer 407), or topotecan formulations (Topo-Gel, Topo-Sol) was performed into tumor tissues. After 3–4 weeks of growth, tumors were harvested, and the levels of PARP cleavage and expression/ phosphorylation of CHEK1 were examined through Western blotting. |
Topo-Gel reduces the adverse effects of topotecan on the health of mice
An injection of Topo-Gel can induce a high concentration of topotecan in tumor tissues and a low concentration of topotecan in the organs of nude mice. Therefore, the body weight, hematological parameters, and mass of the main organs were examined to reveal the adverse effects of topotecan formulations. As shown in Figure 9, an oral administration of 3 mg/kg, 2 mg/kg, or 1 mg/kg of topotecan significantly inhibited the subcutaneous growth of Y79 cells in nude mice. The antitumor effect observed after oral administration of a 3 mg/kg topotecan is similar to that reported after a single intratumoral injection of Topo-Gel (Figure 9). Meanwhile, the antitumor effect observed after the oral administration of 2 mg/kg or 1 mg/kg topotecan was weaker than that reported after a single intratumoral injection of Topo-Gel (Figure 9). The oral administration of 0.5 mg/kg topotecan could not inhibit the subcutaneous growth of Y79 cells in nude mice (Figure 9). Moreover, the oral administration of topotecan can cause serious damage to the bodily health of nude mice, leading to a decrease in hematological parameters, weight loss, and weight loss in major organs (Tables 4 and 5, and Figure 10). It is worth noting that the oral administration of topotecan caused these effects in a dose (0.5 mg/kg) without antitumor activity. The injection of Topo-Sol did not exert a significant antitumor effect, and did not affect the hematological parameters, body weight, and weights of major organs (Tables 4 and 5, and Figure 10). A single intratumoral injection of Topo-Gel exerted a similar antitumor effect to that observed following the oral administration of 3 mg/kg topotecan. However, the injury induced in mice was significantly less than that noted after the oral administration of each dose of topotecan (Tables 4 and 5, and Figure 10). The results are displayed as a data Table (Tables 4 and 5) or a heat map drawn from the data (Figure 10). Therefore, it was concluded that Topo-Gel reduces the adverse effects of topotecan on the health of mice.
 |
Table 4 The effect of Toptecan on nude mice’s hematological parameters |
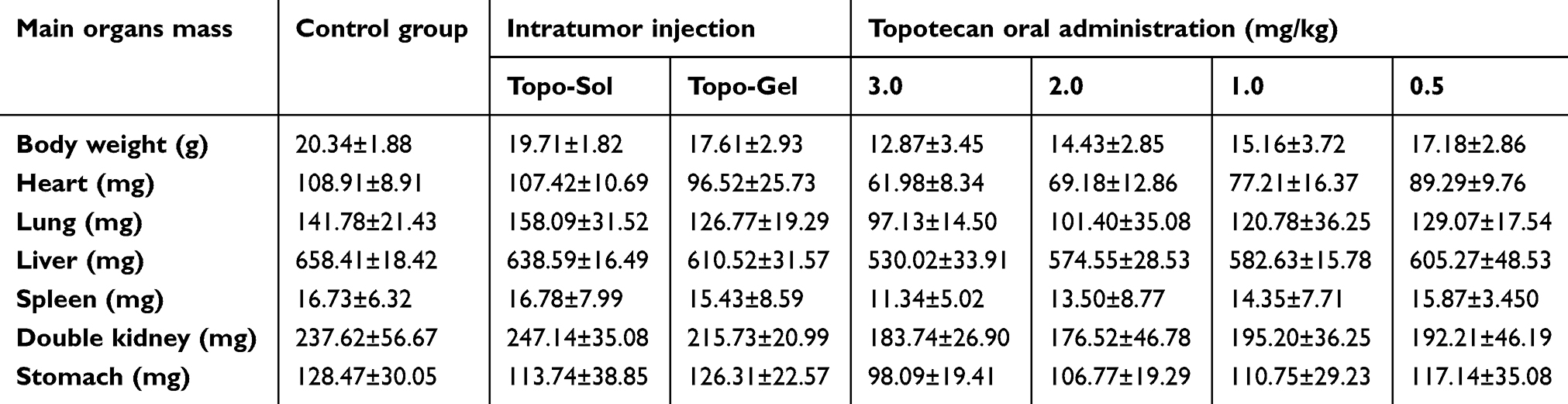 |
Table 5 The effect of Toptecan on nude mice’s body weight and main organs mass |
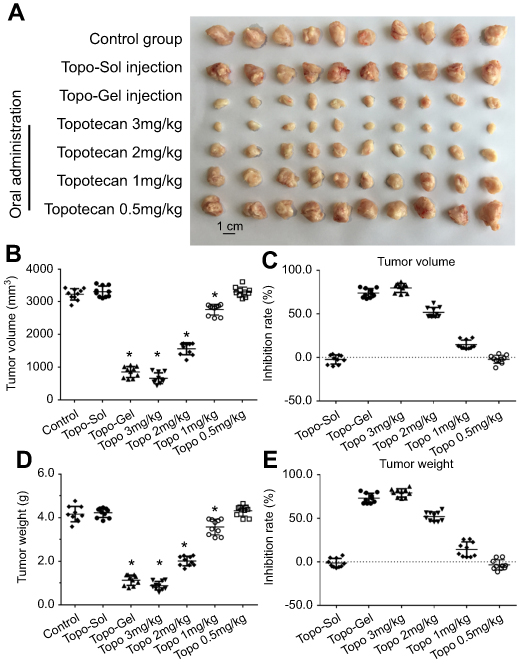 |
Figure 9 Investigation of the long-acting antitumor effect of topotecan formulations in the Rb subcutaneous tumor model. Y79 cells were injected into nude mice to form subcutaneous tumors. A single injection of topotecan formulations (Topo-Gel, Topo-Sol) was injected into tumor tissues. Alternatively, nude mice received oral administration of topotecan (3 m/kg, 2 mg/kg, 1 mg/kg, or 0.5 mg/kg) once per 2 days. After 3–4 weeks of growth, tumors were harvested, and tumor volumes or tumor weights were calculated. The results are shown as (A) tumor images, (B) tumor volumes, (C) inhibition rates according to tumor volumes, (D) tumor weights, and (E) inhibition rates according tumor weights. *P<0.05 Topo-Gel versus solvent control; *P<0.05 oral administration of topotecan versus solvent control. |
 |
Figure 10 The effect of topotecan on the hematological parameters, body weight, and mass of the main organs of nude mice (Tables 4 and 5). The inhibition rates in each group were calculated and shown as a heat map. |
Discussion
Chemotherapy continues to be the mainstay for the treatment of Rb.29,30 However, the current strategies for the administration of these drugs are not satisfactory. In this study, topotecan was prepared as a hydrogel that can be transformed from a liquid into a hydrogel at body temperature. Topotecan exhibits better solubility compared with melphalan, allowing topotecan formulations to deliver a larger amount of the drug in a smaller volume. In the present study, topotecan formulations (Topo-Sol or Topo-Gel) yielded a high dose of topotecan (almost 30 mg/ml). Topo-Gel, which is in liquid form at room temperature, can be directly injected into the tumor tissue to ensure precise drug administration. Moreover, at the body temperature of an animal, Topo-Gel can be sustained in the tumor tissues for a long time in the form of a hydrogel. Topotecan can be slowly released from Topo-Gel into tumor tissues via dissolution of the hydrogel by the cells, and exerts its long-term antitumor effect via a single administration.
Topotecan, which functions as a topoisomerase I inhibitor, is often used as a DNA damage-inducing treatment.31,32 In cancer cells, topotecan can also be used as a therapeutic strategy for recurrent cisplatin-resistant tumors (eg, ovarian cancer).33,34 In the present study, topotecan was rapidly cleared from tumor tissues after a single injection of Topo-Sol, whereas topotecan was detected in tumor tissues for a long time after a single injection of Topo-Gel. Unlike Topo-Sol, an injection of Topo-Gel induced the activation of apoptotic or DNA damage-related pathways, including cleavage of PARP or phosphorylation of CHEK1.35 Moreover, the adverse effects of topotecan (ie, low blood counts, nausea, vomiting, diarrhea, or fatigue) limit the use of topotecan. The present results showed that, when an equal antitumor effect was achieved via the oral administration of topotecan or injection of Topo-Gel, the observed toxicity in nude mice of the former group was much more serious. Therefore, the development of the Topo-Gel induced the slow release or long-acting effects of topotecan in tumor tissues, and improved the adverse effects caused by topotecan. Moreover, it is difficult to establish immunodeficient animals and corresponding tumor models in large animals (eg, beagle dogs). Immunodeficient mice are a common model for oncological research. However, their size is insufficient to establish tumor tissue in the mouse eye. Thus, a subcutaneous tumor model in nude mice is established, and drugs are injected into solid tumors. In vivo imaging of small animals can reflect the growth of tumor tissue in vivo.36–40 In order to inject drug preparations into solid tumor tissues, we established a subcutaneous tumor model. The results fully demonstrated the antitumor effect of the drug. Subcutaneous tumors are easy to observe and can reflect the antitumor effect of drugs by measuring tumor volume and weight.
Currently, various image-guided interventional strategies enable precise drug delivery in tumor tissues.41–44 For tumor tissues with large vascular invasion, transcatheter arterial chemoembolization can be used to mix lipiodol with antitumor drugs for injection into the tumor tissue through the large blood vessels. This approach results in tumor vascular occlusion and antitumor effects.45–47 For tumor tissues without large vascular invasion, the drug can be injected into the tumor tissue through a puncture under the guidance of computed tomography.48,49 The Topo-Gel prepared in this study can be used for the long-acting and sustained release of drugs, as well as the embolization of tumor blood vessels. Poloxamer, a polymer material used in the preparation of Topo-Gel, is a pharmaceutical excipient approved by the Chinese Pharmacopoeia (the fourth part of Chinese Pharmacopoeia [2015 Version], page 531–532,). It can be used in injections, emulsifiers, etc., and it has a good safety profile. In addition, poloxamer can be biodegraded without posing a potential risk to the health of the patient (eg, polymer residue in the organs of the patient). Interestingly, Taich et al (2016) prepared a sustained-release hydrogel of topotecan using another material, namely poly(ε-caprolactone)-poly(ethyleneglycol)-poly(ε-caprolactone).50 Majumder et al (2018) designed a multicompartment hydrogel that can facilitate the time-resolved delivery feature of combination therapy on glioblastoma. Furthermore, Li et al produced a systematic summary and introduction for the design of hydrogels targeting controlled drug delivery.51,52 Meng et al prepared a temperature-sensitive phase-change hydrogel of tamoxifen achieving long sustainability of agru in tumor tissues and a long-acting antitumor effect.48,53 Studies are warranted to examine the differences between hydrogels prepared using different materials.
Conclusion
Topo-Gel, a temperature-sensitive phase-change hydrogel, is a slow-release system allowing the long-term sustainability of topotecan in Rb tissues and preserving the efficacy of topotecan in the long term.
Abbreviations
Rb, Retinoblastoma; PARP, poly ADP-ribose polymerase; CHEK1, checkpoint kinase 1; TACE, transcatheter arterial chemoembolization; CT, Computed Tomography.
Acknowledgments
This work was supported by direct grants from the Chinese Government: National Key R&D Program of China (Project No: 2017YFA0103204), National Natural Science Foundation of China (Grant No. 81770887), and National Natural Science Foundation of China (Grant No. 81670830). These funding sources or funding bodies had no role in the design of this study and will not have any role during its execution, analyses, interpretation of the data, or decision to submit the results. We thank Dr. Xioajie Xu in Department of Medical Molecular Biology, Beijing Institute of Biotechnology, Collaborative Innovation Center for Cancer Medicine, Beijing100850, China for her help and advice.
Author contributions
All authors made substantial contributions to the design and conception, acquisition, analysis or interpretation of data. All authors took part in either drafting or revising the manuscript. At the same time, authors gave final approval of the version to be published; and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brennan RC, Qaddoumi I, Mao S, et al. Ocular salvage and vision preservation using a topotecan-based regimen for advanced intraocular retinoblastoma. J Clin Oncol. 2017;35:72–77. doi:10.1200/JCO.2016.69.2996
2. Friedrich MJ. Retinoblastoma therapy delivers power of chemotherapy with surgical precision. JAMA. 2011;305:2276–2278. doi:10.1001/jama.2011.778
3. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. doi:10.3322/caac.21492
4. Munier FL, Gaillard MC, Stathopoulos C. Anterior chamber chemotherapy in retinoblastoma-necessary but not sufficient for aqueous seeding control. JAMA Ophthalmol. 2018;136:596–597. doi:10.1001/jamaophthalmol.2018.0630
5. Chu WK, Law KS, Chan SO, et al. Antagonists of growth hormone-releasing hormone receptor induce apoptosis specifically in retinoblastoma cells. Proc Natl Acad Sci USA. 2016;113:14396–14401. doi:10.1073/pnas.1617427113
6. Zhang MG, Lee JY, Gallo RA, et al. Therapeutic targeting of oncogenic transcription factors by natural products in eye cancer. Pharmacol Res. 2018;129:365–374. doi:10.1016/j.phrs.2017.11.033
7. Roskoski R
8. Francis JH, Abramson DH, Ji X, et al. Risk of extraocular extension in eyes with retinoblastoma receiving intravitreous chemotherapy. JAMA Ophthalmol. 2017;135:1426–1429. doi:10.1001/jamaophthalmol.2017.4600
9. Berry JL, Bechtold M, Shah S, et al. Not all seeds are created equal: seed classification is predictive of outcomes in retinoblastoma. Ophthalmology. 2017;124:1817–1825. doi:10.1016/j.ophtha.2017.05.034
10. Saengwimol D, Rojanaporn D, Chaitankar V, et al. A three-dimensional organoid model recapitulates tumorigenic aspects and drug responses of advanced human retinoblastoma. Sci Rep. 2018;8:15664. doi:10.1038/s41598-018-34037-y
11. Qu W, Meng B, Yu Y, Wang S. Folic acid-conjugated mesoporous silica nanoparticles for enhanced therapeutic efficacy of topotecan in retina cancers. Int J Nanomedicine. 2018;13:4379–4389. doi:10.2147/IJN.S142668
12. Committee for the National Registry of Retinoblastoma. The National Registry of Retinoblastoma in Japan (1983–2014). Jpn J Ophthalmol. 2018;62:409–423. doi:10.1007/s10384-018-0597-2
13. Ramírez-Ortiz MA, Lansingh VC, Eckert KA, et al. Systematic review of the current status of programs and general knowledge of diagnosis and management of retinoblastoma. Bol Med Hosp Infant Mex. 2017;74:41–54. doi:10.1016/j.bmhimx.2016.08.002
14. Akella SS, Francis JH, Knezevic A, et al. Growth patterns of survivors of retinoblastoma treated with ophthalmic artery chemosurgery. PLoS One. 2018;13:e0197052. doi:10.1371/journal.pone.0197052
15. Rowlands MA, Mondesire-Crump I, Levin A, et al. Total retinal detachments due to retinoblastoma: outcomes following intra-arterial chemotherapy/ophthalmic artery chemosurgery. PLoS One. 2018;13:e0195395. doi:10.1371/journal.pone.0195395
16. Zhu X, Xue L, Yao Y, et al. The FoxM1-ABCC4 axis mediates carboplatin resistance in human retinoblastoma Y-79 cells. Acta Biochim Biophys Sin (Shanghai). 2018;50:914–920. doi:10.1093/abbs/gmy080
17. He H, Lee C, Kim JK. UHRF1 depletion sensitizes retinoblastoma cells to chemotherapeutic drugs via downregulation of XRCC4. Cell Death Dis. 2018;9(2):164. doi:10.1038/s41419-018-1111-y
18. Wang YL, Tang ZG. A novel long-sustaining system of apatinib for long-term inhibition of the proliferation of hepatocellular carcinoma cells. Onco Targets Ther. 2018;11:8529–8541. doi:10.2147/OTT.S188209
19. Xie H, Tian S, Yu H, et al. A new apatinib microcrystal formulation enhances the effect of radiofrequency ablation treatment on hepatocellular carcinoma. Onco Targets Ther. 2018;11:3257–3265. doi:10.2147/OTT.S165000
20. Ye L, Shi J, Wan S, et al. Development and validation of a liquid chromatography-tandem mass spectrometry method for topotecan determination in beagle dog plasma and its application in a bioequivalence study. Biomed Chromatogr. 2013;27:1532–1539. doi:10.1002/bmc.2956
21. Li N, Singh P, Mandrell KM, Lai Y. Improved extrapolation of hepatobiliary clearance from in vitro sandwich cultured rat hepatocytes through absolute quantification of hepatobiliary transporters. Mol Pharm. 2010;7:630–641. doi:10.1021/mp9001574
22. Holleran JL, Parise RA, Yellow-Duke AE, et al. Liquid chromatography-tandem mass spectrometric assay for the quantitation in human plasma of the novel indenoisoquinoline topoisomerase I inhibitors, NSC 743400 and NSC 725776. J Pharm Biomed Anal. 2010;52:714–720. doi:10.1016/j.jpba.2010.02.020
23. Muenster U, Grieshop B, Ickenroth K, Gnoth MJ. Characterization of substrates and inhibitors for the in vitro assessment of Bcrp mediated drug-drug interactions. Pharm Res. 2008;25:2320–2326. doi:10.1007/s11095-008-9632-1
24. An L, Li DD, Chu HX, et al. Terfenadine combined with epirubicin impedes the chemo-resistant human non-small cell lung cancer both in vitro and in vivo through EMT and Notch reversal. Pharmacol Res. 2017;124:105–115. doi:10.1016/j.phrs.2017.07.021
25. Jia H, Yang Q, Wang T, et al. Rhamnetin induces sensitization of hepatocellular carcinoma cells to a small molecular kinase inhibitor or chemotherapeutic agents. Biochim Biophys Acta. 2016;1860:1417–1430. doi:10.1016/j.bbagen.2016.04.007
26. Wang L, Zhao L, Jia X, et al. Aminophenols increase proliferation of thyroid tumor cells by inducing the transcription factor activity of estrogen receptor α. Biomed Pharmacother. 2019;109:621–628. doi:10.1016/j.biopha.2018.10.168
27. Liang Y, Xu X, Wang T, et al. The EGFR/miR-338-3p/EYA2 axis controls breast tumor growth and lung metastasis. Cell Death Dis. 2017;8:e2928. doi:10.1038/cddis.2017.518
28. Ji Q, Xu X, Li L, et al. miR-216a inhibits osteosarcoma cell proliferation, invasion and metastasis by targeting CDK14. Cell Death Dis. 2017;8:e3103. doi:10.1038/cddis.2017.518
29. Maheshwari A, Finger PT. Cancers of the eye. Cancer Metastasis Rev. 2018;37(4):677–690. doi:10.1007/s10555-018-9762-9
30. Aitken JF, Youlden DR, Moore AS, et al. Assessing the feasibility and validity of the Toronto Childhood Cancer Stage Guidelines: a population-based registry study. Lancet Child Adolesc Health. 2018;2:173–179. doi:10.1016/S2352-4642(18)30023-3
31. Shah N, Mohammad AS, Saralkar P, et al. Investigational chemotherapy and novel pharmacokinetic mechanisms for the treatment of breast cancer brain metastases. Pharmacol Res. 2018;132:47–68. doi:10.1016/j.phrs.2018.03.021
32. Zhang GN, Zhang YK, Wang YJ, et al. Modulating the function of ATP-binding cassette subfamily G member 2 (ABCG2) with inhibitor cabozantinib. Pharmacol Res. 2017;119:89–98. doi:10.1016/j.phrs.2017.01.024
33. Poveda A, Del Campo JM, Ray-Coquard I, et al. Phase II randomized study of PM01183 versus topotecan in patients with platinum-resistant/refractory advanced ovarian cancer. Ann Oncol. 2017;28:1280–1287. doi:10.1093/annonc/mdx111
34. Liu NF, Chen YQ, Hu JL, et al. Role and timing of second-line therapies for patients with recurrent platinum-resistant ovarian epithelial cancer. Eur J Gynaecol Oncol. 2017;38:266–270.
35. Kim MK, James J, Annunziata CM. Topotecan synergizes with CHEK1 (CHK1) inhibitor to induce apoptosis in ovarian cancer cells. BMC Cancer. 2015;15:196. doi:10.1186/s12885-015-1584-3
36. Ji Q, Xu X, Kang L, et al. Hematopoietic PBX-interacting protein mediates cartilage degeneration during the pathogenesis of osteoarthritis. Nat Commun. 2019;10(1):313. doi:10.1038/s41467-018-08277-5
37. Li L, Liang Y, Kang L, et al. Transcriptional regulation of the warburg effect in cancer by SIX1. Cancer Cell. 2018;33(3):368–385.e7. doi:10.1016/j.ccell.2018.01.010
38. Shao Z, Li Y, Dai W, et al. ETS-1 induces Sorafenib-resistance in hepatocellular carcinoma cells via regulating transcription factor activity of PXR. Pharmacol Res. 2018;135:188–200. doi:10.1016/j.phrs.2018.08.003
39. Zhang Y, Li D, Jiang Q, et al. Novel ADAM-17 inhibitor ZLDI-8 enhances the in vitro and in vivo chemotherapeutic effects of Sorafenib on hepatocellular carcinoma cells. Cell Death Dis. 2018;9(7):743. doi:10.1038/s41419-018-1111-y
40. Feng F, Jiang Q, Cao S, et al. Pregnane X receptor mediates sorafenib resistance in advanced hepatocellular carcinoma. Biochim Biophys Acta Gen Subj. 2018;1862(4):1017–1030. doi:10.1016/j.bbagen.2018.01.011
41. Yoon SM, Ryoo BY, Lee SJ, et al. Efficacy and safety of transarterial chemoembolization plus external beam radiotherapy vs sorafenib in hepatocellular carcinoma with macroscopic vascular invasion: a randomized clinical trial. JAMA Oncol. 2018;4:661–669. doi:10.1001/jamaoncol.2017.5847
42. Park CG, Hartl CA, Schmid D, Carmona EM, Kim HJ, Goldberg MS. Extended release of perioperative immunotherapy prevents tumor recurrence and eliminates metastases. Sci Transl Med. 2018;10:eaar1916. doi:10.1126/scitranslmed.aao4496
43. Feng F, Jiang Q, Jia H, et al. Which is the best combination of TACE and Sorafenib for advanced hepatocellular carcinoma treatment? A systematic review and network meta-analysis. Pharmacol Res. 2018;135:89–101. doi:10.1016/j.phrs.2018.06.021
44. Xie H, Yu H, Tian S, et al. What is the best combination treatment with transarterial chemoembolization of unresectable hepatocellular carcinoma? A systematic review and network meta-analysis. Oncotarget. 2017;8:100508–100523. doi:10.18632/oncotarget.20119
45. Ni JY, Sun HL, Chen YT, et al. Drug-eluting bead transarterial chemoembolization in the treatment for unresectable soft tissue sarcoma refractory to systemic chemotherapy: a preliminary evaluation of efficacy and safety. J Cancer Res Clin Oncol. 2018;144:157–163. doi:10.1007/s00432-017-2530-3
46. Hartrumpf KJ, Marquardt S, Werncke T, et al. Quality of life in patients undergoing repetitive TACE for the treatment of intermediate stage HCC. J Cancer Res Clin Oncol. 2018;144(10):1991–1999. doi:10.1007/s00432-018-2704-7
47. Hyun MH, Lee YS, Kim JH, et al. Hepatic resection compared to chemoembolization in intermediate- to advanced-stage hepatocellular carcinoma: a meta-analysis of high-quality studies. Hepatology. 2018;68:977–993. doi:10.1002/hep.29883
48. Takayasu K, Arii S, Sakamoto M, et al. Impact of resection and ablation for single hypovascular hepatocellular carcinoma ≤2 cm analysed with propensity score weighting. Liver Int. 2018;38:484–493. doi:10.1111/liv.13670
49. Wang J, Wei Y, Fei YR, et al. Preparation of mixed monoterpenes edge activated PEGylated transfersomes to improve the in vivo transdermal delivery efficiency of sinomenine hydrochloride. Int J Pharm. 2017;533:266–274. doi:10.1016/j.ijpharm.2017.09.059
50. Taich P, Moretton MA, Del Sole MJ, et al. Sustained-release hydrogels of topotecan for retinoblastoma. Colloids Surf B. 2016;146:624–631. doi:10.1016/j.colsurfb.2016.07.001
51. Majumder P, Baxa U, Walsh STR, Schneider JP. Design of a multicompartment hydrogel that facilitates time-resolved delivery of combination therapy and synergized killing of glioblastoma. Angew Chem Int Ed Engl. 2018;57:15040–15044. doi:10.1002/anie.201806483
52. Li J, Mooney DJ. Designing hydrogels for controlled drug delivery. Nat Rev Mater. 2016;1:16071. doi:10.1038/natrevmats.2016.71
53. Meng D, Lei H, Zheng X, et al. A temperature-sensitive phase-change hydrogel of tamoxifen achieves the long-acting antitumor activation on breast cancer cells. Onco Targets Ther. 2019;12:3919–3931. doi:10.2147/OTT.S201421
Supplementary material
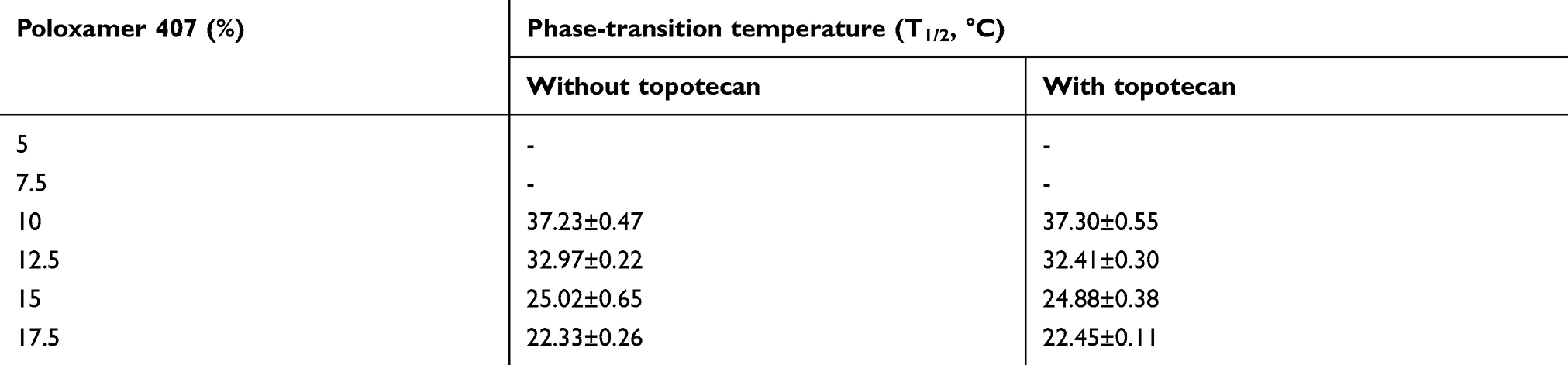 |
Table S1 Topotecan did not alter the phase-transition temperatures of Topotecan hydrogel with indicted Poloxamer 407 |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.