Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 17
A Systematic Review of Research on Guided Access Cavity Preparation Endodontic Treatment: Dentin Preservation Perspectives
Authors Muryani A, Aripin D, Dharsono HDA ![]() , Rajion ZA, Wicaksono S
, Rajion ZA, Wicaksono S ![]()
Received 15 August 2024
Accepted for publication 13 November 2024
Published 22 January 2025 Volume 2025:17 Pages 49—63
DOI https://doi.org/10.2147/CCIDE.S491632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Anna Muryani,1,2 Dudi Aripin,2 Hendra Dian Adhita Dharsono,2 Zainul Ahmad Rajion,3 Satrio Wicaksono4
1Doctoral Programme Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 2Conservative Dentistry Department Faculty of Dentistry, Universitas Padjadjaran, Bandung, West Java, Indonesia; 3Department Oral Maxillofacial Surgery and Oral Diagnosis Kulliyyah of Dentistry International Islamic University Malaysia, Kuantan, Malaysia; 4Faculty of Mechanical and Aerospace Engineering, Institut Teknologi Bandung, Bandung, West Java, Indonesia
Correspondence: Anna Muryani, Gedung Pamitran Unpad, lantai 4 Wing Utara Jl. Prof. Eyckman No. 38 Bandung, Faculty of Medicine, Universitas Padjadjaran, West Java, Indonesia, 40161, Tel +62 896 1997 2132, Email [email protected]
Purpose: Guided access cavity preparation (GACP) is an endodontic procedure utilizing stents, guide sleeves, or dynamic guides to facilitate the proper formation of access cavities. This paper aims to evaluate the significance of research on guided access cavity preparation in endodontic treatment concerning dentin preservation. In the context of dentin preservation, this paper provides a thorough scoping review of a variety of methodologies for evaluating the accuracy of guided access cavity preparation.
Materials and Methods: Article searches were conducted using Tthe keywords ”Guide Access Cavity Preparation” AND “Static Guide OR 3D Printing Template” AND ”Dynamic Guide through digital databases including PubMed, Scopus, Cochrane Library, Science Direct, and Google Scholar. Research articles published in English within the past five years (2019-2024) and in accordance with the PCC (Population, Concept, and Context) framework were also included in the study. Articles from the meta-analysis or systematic review study type, those that were not accessible in full text or in a paid format, and those that did not assess the use of guided endodontics in endodontic surgery were excluded. This scoping review adheres to the Preferred Reporting Items for Systematic Reviews without Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) criteria.
Results: A total of 12 articles were reviewed, encompassing various locations, designs, type, and samples, which demonstrated the use of guided access cavity preparation has significant clinical applications and can provide accurate results in endodontic therapy.
Conclusion: Article searches were conducted using the keywords “Guide Access Cavity Preparation” AND ‘Static Guide OR 3D Printing Template’ AND” Dynamic Guide through digital databases including PubMed, Scopus, Cochrane Library, Science Direct, and Google Scholar. Research articles published in English within the past five years (2019– 2024) and in accordance with the PCC (Population, Concept, and Context) framework were also included in the study. Articles from the meta-analysis or systematic review study type, those that were not accessible in full text or in a paid format, and those that did not assess the use of guided endodontics in endodontic surgery were excluded. This scoping review adheres to the Preferred Reporting Items for Systematic Reviews without Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) criteria. Studies show that advanced technologies in guided access cavity preparation endodontic treatment can improve dentin preservation, improve accuracy and predictability, particularly for root canal anomalies and difficult teeth, but clinicians must consider limitations and clinical applications. Clinicians must evaluate the limitations and clinical applications of guided endodontic access prior to its implementation.
Keywords: guided endodontic access, GEA, guided access cavity preparation, GACP, static guided endodontic access, SGEA, dynamic guide endodontic access, DGEA, preservation dentin
Introduction
Guided access cavity preparation (GACP) is a technique used in endodontic treatment that involves the use of stents or guide sleeves or dynamic guide to assist in the accurate and precise preparation of access cavities.1,2 The guided access cavity preparation has gained attention and popularity in recent years due to advancements in cone-beam computed tomography and three-dimensional rapid prototyping manufacturing technology. This technique allows for more conservative access cavity preparation, decreased chair time, and reduced risk of iatrogenic damage.3,4 Preserving tooth structure is a fundamental principle in minimally invasive endodontics.5–12
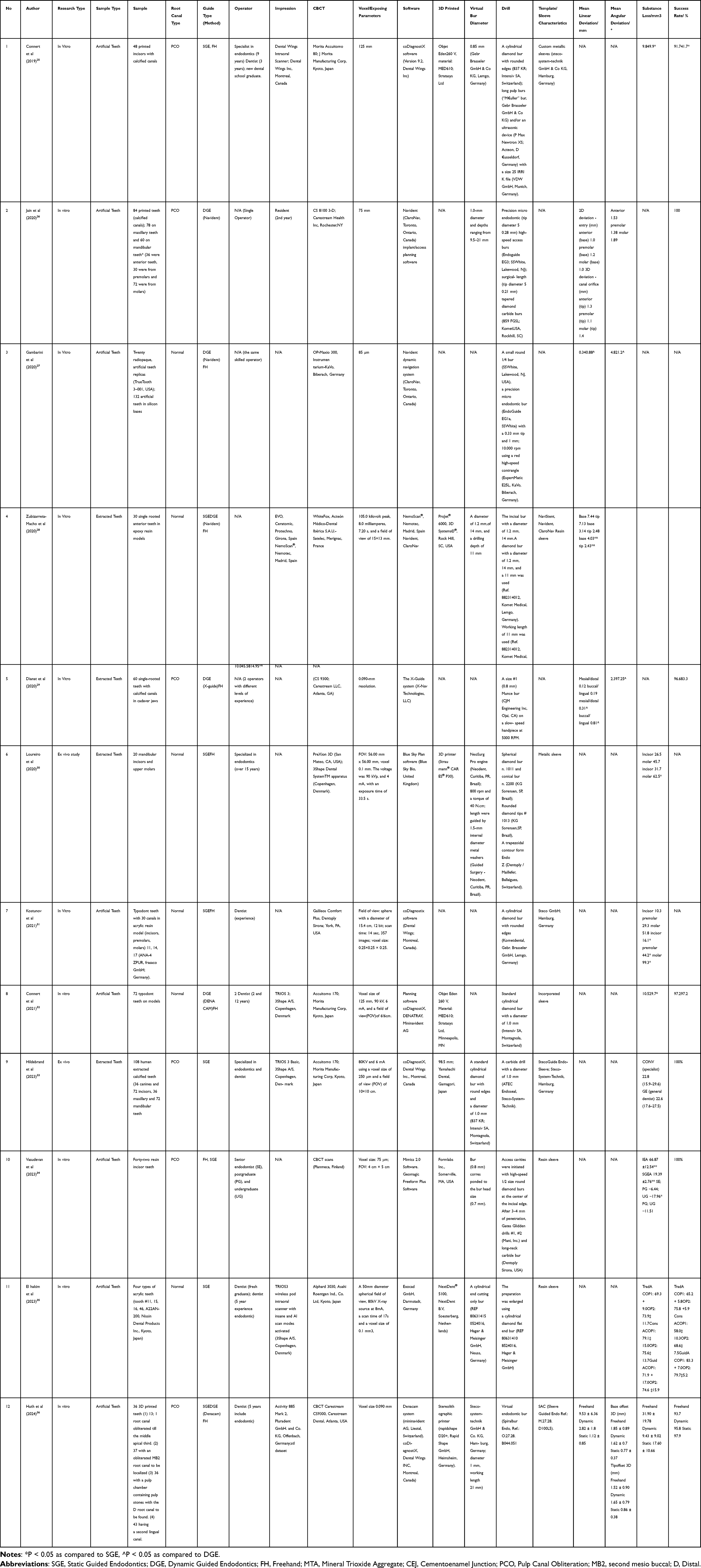 |
Table 1 Data Extraction on Experimental Studies |
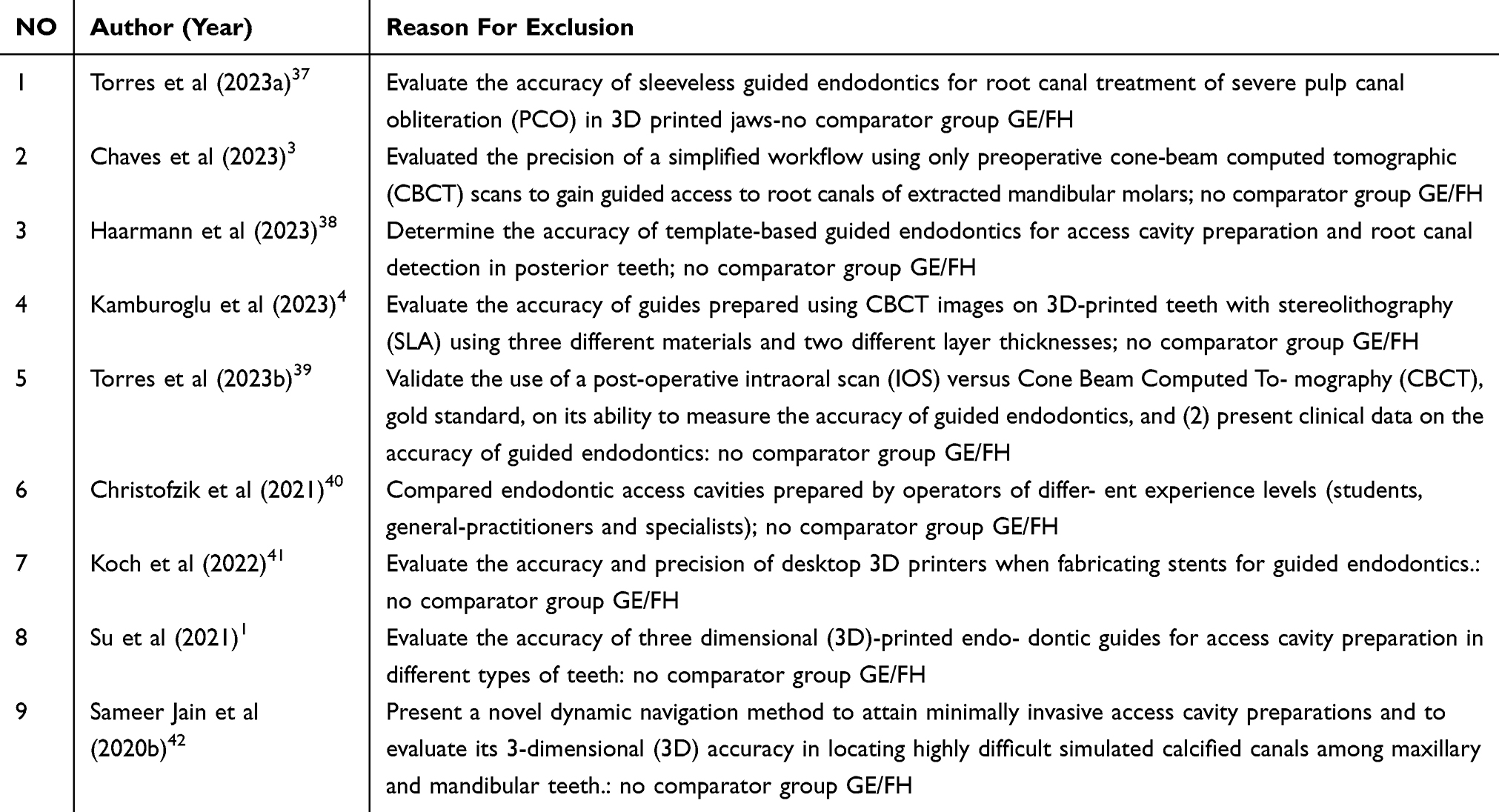 |
Table 2 Excluded Studies with Reason for Exclusion |
Minimally invasive endodontic access opening preparation techniques using guided access have shown promising outcomes in various clinical scenarios. These include cases of pulp canal calcification, dens evaginatus, anomalous teeth. The guided endodontics technique has been compared to conventional methods using models in numerous pioneering studies.2,13–19 Successful applications of guided endodontics in clinical practice, such as cavity preparation, root canal localization, have been demonstrated in recent clinical case reports.3,20,21
Preserving tooth structure is now the main goal of endodontic, restorative, and contemporary dentistry techniques.2,13–19 Minimally invasive endodontics maximizes the preservation of natural tooth structure by reducing the amount of preparation required for the access cavity, the prepared apical size, and the taper of prepared canals.22 Cone beam computed tomography, operating microscopes, and ultrasonic instruments are examples of sophisticated endodontic instruments that have made this therapeutic paradigm change possible. Aiming to create access points that maintain as much healthy tooth structure as feasible, the term “minimally invasive endodontic access cavities” refers to this process.22,23 In this scoping review, we aim to examine the current research on guided access cavity preparation techniques that prioritize the preservation of dentin aspects, clinical applications, accuracy, and limitations of guided access cavity preparation in achieving minimally invasive endodontic outcomes.
Materials and Methods
Research Question
The research question formulated using the PCC (Population, Concept, and Context) framework was: A comparative evaluation of guided endodontic (static and dynamic navigation systems) versus freehand in the preparation of endodontic access cavities, focusing on the preservation of tooth structure in permanent human teeth.
Search Strategy
The study focused on access cavity endodontic treatment of anterior or posterior teeth using guided endodontic techniques. Articles were screened following PRISMA-ScR guidelines. (Figure 1). Independent authors conducted a scoping review search to identify all articles published up to the end of June 2024 in three databases: PubMed, Cochrane Library, Science Direct, and Google Scholar.
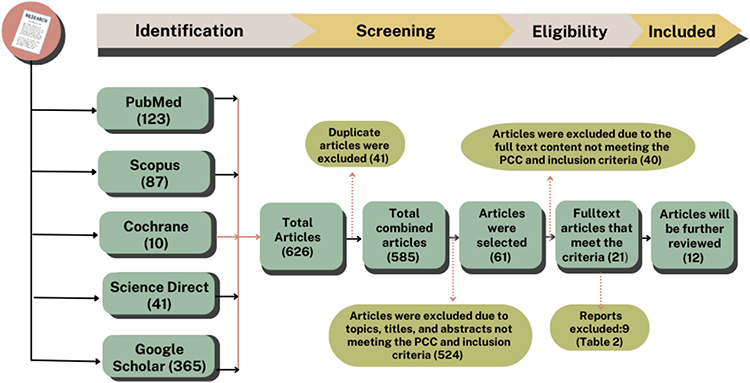 |
Figure 1 PRISMA Flow Diagram for the Selection of Studies in the Scoping Review. Notes: PRISMA Flow Diagram depicting the study selection procedure for the systematic review. It specifies the quantity of records identified by database searches and alternative methods, the screening procedure, and the number of studies incorporated in the review. |
Studies Selection
The study utilized digital databases and Boolean Operators to conduct a comprehensive literature search on guided endodontic access cavity preparation, focusing on its accuracy compared to conventional techniques. Key terms used included “Guide Access Cavity Preparation”, “Static Guide”, “3D Printing Template”, and “Dynamic Guide”, based on limited discourse and understanding of the technique. The study analyzed research published between 2019-Juni 2024 on access cavity preparation non-surgical root canal therapy for anterior and posterior teeth. Post-removal, retreatment, surgical-guided endodontic procedures, gray literature, reviews, case reports, and commentaries or narratives were also excluded.
Data Extraction
The articles were sifted for duplicates and relevance, and then analyzed using established criteria, with inclusion in data extraction Table 1 limited to individuals meeting specified criteria. The Joanna Briggs Institute’s guidelines were employed to evaluate the methodological quality of the selected articles using a self-designed criteria checklist.24 Each full-text article was evaluated for a variety of bias domains, such as angulation, accuracy, time consumed, sample size calculation, randomization, and image acquisition using CBCT. The articles were categorized into low, moderate, and high levels of evidence by the scoring system. An article was classified as having a “low” risk of bias if all domains were rated low, and a “high” risk was ascribed if any domain was rated high. “Unclear” articles had at least one domain that was rated as such. Disagreements among authors were resolved through consultation with a third reviewer.
Results
A literature search was conducted using keywords on four databases, resulting in a total of 626 articles. As a result, 12 papers were selected for further evaluation, whereas 614 articles were discarded since they did not meet the PCC and inclusion criteria. The article screening method is illustrated in Figure 1 and Table 2 of the research procedure steps in the execution diagram, utilizing the PRISMA-ScR framework. The twelve papers that were evaluated were then recorded in a data extraction table, specifically referred to as Table 1. The data extraction table provides a concise summary of the data, encompassing details such as the names of the researchers, the years of the studies, the titles of the research, the places where the studies took place, the designs of the studies, the samples used, and the conclusions of the research.
Table 1 presents the main discoveries derived from twelve research publications that focus on guided access cavity preparation. Sample types in these research articles are used as varied: artificial teeth were used in 8 articles (67%), and extracted teeth were used in 4 articles (33%), represented in Table 1. Different guided endodontic access cavity preparations were used: static guide was used in 8 articles (31%), dynamic guide was used in 6 articles (23%), and freehand was used in 12 article (46%) represented in Table 1. Different types of research on guided access cavity preparations were used: in vitro was used in 10 articles (83%) and ex vivo was used in 2 articles (17%), represented in Table 1. Different types of sample root canals were used: normal tooth was used in 6 article (50%), and pulp canal obliteration or calcification was used in 6 articles (50%). The operators in these researches had a range of competence skill levels, including undergraduate general dentist was used in 1 article (8%), fresh graduate general dentist was used in 1 article (8%), general dentist was used in 5 articles (38%), and senior specialist in endodontic was used in 6 articles (46%) represented in Table 1.
Result evaluation quality of the selected articles included among the 12 studies analyzed, two study incorporated all three techniques,28,36 whereas the remaining studies compared Guided Endodontic Access (SGEA or/and DGEA), compared FHA (Freehand Access) for access cavity preparation endodontic treatment.25–27,29–35 All studies assessed image acquisition using CBCT, and SGEA, after which the dynamic navigation system was employed for real-time access cavity preparation.25–36 The loss of tooth substance was comparatively evaluated across four studies that assessed angulation.27–29,36 Five studies analyzed accuracy and time taken, demonstrating that guided endodontic exhibited increased accuracy, reduced angulation variations, and shorter time requirements compared to the free-hand approach represented in Table 1.26,27,29,32,36
Six studies compared SGEA and the freehand technique, showing that SGEA had greater accuracy and less tooth substance loss related to angulation variations.25,30,31,33–35 Four studies compared DGEA and FHA, with SGEA again demonstrating superior accuracy and minimized tooth substance loss compared to the freehand technique.26,27,29,32 In comparison to both static-guided endodontics and the freehand technique, DGEA demonstrated better accuracy and reduced tooth substance loss in relation to angulation variations in two studies.28,36
The evaluation of randomisation, sample size calculation, image acquisition via CBCT, angulation, accuracy, and time taken was performed in the full-text articles to assess the risk of bias. The scoring of the level of evidence for the five included articles was tabulated, with the overall risk of bias assessment summarized in Figures 2 and 3. Three articles exhibited a low risk of bias, while 9 articles demonstrated a high risk of bias due to the lack of evaluation of key parameters.25,26,28,31–35 The study by Connert et al (2019) did not report data on randomisation, sample size calculation, angulation, accuracy, and time taken.25 Sameer D Jain et al (2020) had unclear sample size calculation and did not assess angulation.26 Zubizarreta-Macho et al (2020) conducted a comparative evaluation but lacked information on sample size calculation, accuracy, and time taken.28 Loureiro et al (2020) did not mention key domains of randomisation, sample size calculation, angulation, and accuracy.30 Kostunov et al (2020) also omitted data on sample size calculation, angulation, and time taken.31 Connert et al (2021) failed to report on randomisation, sample size calculation, and angulation.32 Hildebrand et al (2023) and Vasudevan et al (2023) lacked clarity in randomisation and did not assess angulation and accuracy.33,34 El Hakim et al (2023) did not mention data on randomisation, sample size calculation, angulation, and time taken. Consequently, these nine studies were categorized as having a high risk of bias.35
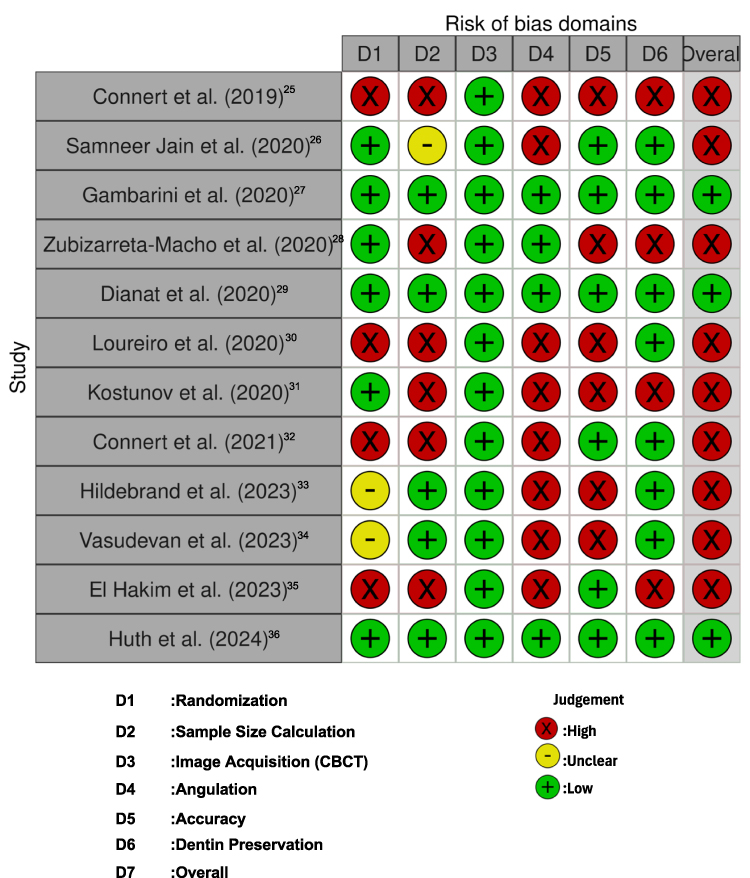 |
Figure 2 Risk of bias assessment “Traffic Light” summary plot. |
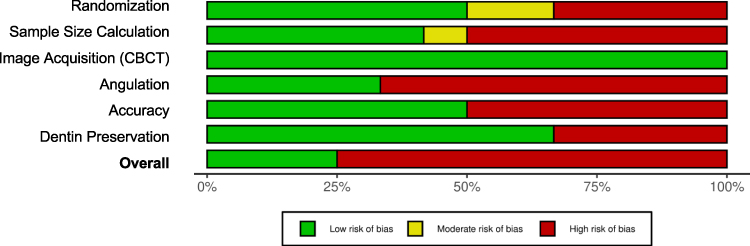 |
Figure 3 Risk of bias assessment graph. |
Discussion
The conventional approach to access cavity preparation compromises the structural integrity and stability of the tooth, with a typical reduction of 63% in relative cuspal stiffness due to the loss of marginal ridge integrity.28,43 Preserving enamel and dentin during this process enhances the tooth’s biomechanical response to occlusal loading, while increased coronal wear leads to higher stress concentrations at the cervical region. The pericervical dentin is subjected to increased stress as the access cavity is expanded. The tooth’s internal morphology, deformability, and fracture resistance are compromised as a result of the excessive removal of this dentin during endodontic therapy.44,45 The disproportionate loss of tooth structure can be mitigated through the use of magnification; however, cavities accessible by free-hand are frequently encountered.42,46–49
Guided Access Cavity Preparation (GACP) is a method that efficiently controls cavity preparations, reducing dentin loss, prioritizing the preservation of healthy tooth structure, and ensuring excellent access while retaining biomechanical integrity.1,15,25 It corresponds with contemporary dentistry’s minimum invasive techniques.5,23,50 Guided access cavity preparation is a method in endodontic treatment that offers precise and accurate preparation, particularly in complex cases like calcified canals or anatomical variations. It contributes to more conservative dentistry by using 3D CBCT images to optimize root canal identification.13,14,16,19,30,51–53 Advancements in rapid prototyping manufacturing technology and cone-beam computed tomography have made guided endodontics possible. Two methodologies, SGE and DGEA, have shown significant interest in improving precision, reducing surgery time, and patient satisfaction.2,19,36,54,55 Traditional methods were effective in locating canals in only 41.7% of cases in 2019, while guided approaches were successful in 91.7%.25 3D printing technology can generate models with internal root anatomy, enhancing precision and minimizing iatrogenic errors.2,19,25,53,54,56,57
SGEA that employs a preset access drill route derived from cone beam computed tomography (CBCT) and transmitted to a rigid template has been developed as a result of advancements in 3D printing and surface scanning. This CBCT-based splint guidance safeguards healthy tooth structure and minimizes iatrogenic errors. A printed template with sleeves is improved by precise pre-operative planning using 3D CBCT images, which enables the precise localization of the root canal. Connert et al (2019) reported an average substance loss of 9.8 mm and a missed canal prevalence of 8.3%. Conventional access cavity preparation resulted in five times more substance loss than static guided preparation. Additionally, 3D printed root canals were accurately identified in 91.7% of guided endodontic cases, as opposed to 41.7% of normal cases. Nevertheless, the time and expenses that are associated with this process increase.25
Volumetric tooth substance loss during dental operations has been greatly decreased since the advent of DGEA. DGEA reduces iatrogenic mistakes, improves visualization of dental tissues while maintaining tooth structure, and enables real-time modifications to the access cavity direction. DNS improves accuracy and dependability over the FHA approach by exhibiting fewer linear and angular deviations as well as a small decrease in dentinal thickness.26, 29, 62, 63 huth (2024) claims that there was a difference in angle deviation between the three methods (p < 0.0001). The FHA technique had the largest deviation (9.53 ± 6.36°), followed by DGEA (2.82 ± 1.8°). SGEA was the most accurate (1.12 ± 0.85°). The operating method had the strongest effect on accuracy (ηP² = 0.524), followed by tooth type** (ηP² = 0.364) and operator skill (ηP² = 0.08). There was no significant difference in bur base and tip localization among the three techniques. In terms of tooth substance loss, the FHA method caused the most damage (p < 0.001), while DGEA preserved the most (p < 0.0001). For operating time (time taken), freehand was the quickest, followed by SGEA, with DGEA taking the longest.28,36,58
Zehnder et al (2016) reported an average angular deviation of 1.81°. Using a 1.5 mm implant bur, they observed coronal deviations between 0.16–0.21 mm and apical deviations from 0.17–0.47 mm. In the maxillary teeth, FHA cavities led to double the material loss and showed poorer trajectory accuracy compared to DGE.59 Buchgreitz et al (2019) found that optimal trajectory was achieved in 75% of dynamically navigated cases, compared to 40% in static guided cases. DGE further reduced the risk of perforation, successfully identifying root canals in 96.6% of cases without perforation. Additionally, Dianat et al (2020) noted that DGE improved the efficiency of access cavity preparation, completing it in an average of 4 minutes (maximum of 7 minutes), while the FHA group required 7 to 19 minutes.29
The results show that GEA techniques are more accurate and protect more tooth material than FHA methods. Although freehand is faster, it is less precise and causes more tooth damage. This suggests that GEA© is better for procedures where accuracy is important.
Limitation
The study highlights the clinical benefits of guided endodontics. It helps locate root canals more precisely and reduces damage to the tooth structure. However, the guided techniques take longer than freehand. The study has some limitations, such as using an in vitro model, limited tooth variety, and possible lack of training with the DGE. These factors may affect the results, and more research is needed to confirm the findings. This study shows that DGE is more accurate and causes less tooth damage than freehand methods. While FHA is faster, GEA techniques are better for preserving tooth material. Further clinical studies are needed to confirm these results in real-world settings. Using 3D-printed teeth for research seems useful and could improve future studies.36,58,60,61
The accuracy of guided access cavity preparation has been validated through pre-clinical studies, demonstrating its reliability compared to traditional methods. Gambarini et al (2020) reported that the DGEA exhibited significantly greater precision than FHA techniques. Specifically, the DGEA group achieved a mean angulation deviation of 4.8°, whereas the FHA group recorded a substantially higher deviation of 21.2°. Similarly, the horizontal deviation, measured as the maximum distance from the desired position, was markedly lower for the DGEA group at 0.34 mm, compared to 0.88 mm in the FHA group. These findings suggest that the application of DNS enhances the benefits of ultra-conservative access cavities by minimizing the risk of iatrogenic damage to critical crown structures, while also reducing procedural risks, associated costs, and challenges in tissue removal and root canal examination.27
Zubizarreta-Macho et al (2020) further investigated the precision of guided systems, comparing SGEA and DGEA with the free-hand approach. Their results revealed that DGEA provided superior accuracy, with mean deviations of 3.14 mm at the base and 2.48 mm at the tip, alongside an angulation error of 5.58°. In contrast, SGEA exhibited higher deviations, with 7.44 mm at the base, 7.13 mm at the tip, and an angulation error of 10.04°. The FHA method displayed the highest angulation error at 14.95°, along with deviations of 4.03 mm at the base and 2.43 mm at the tip. The study concluded that DGEA offered the most precise endodontic access cavities among the three methods, as demonstrated by lower deviation angles and reduced horizontal deviation at both the coronal entry point and apical endpoint.62
Together, these findings highlight the advantages of guided endodontic techniques, particularly dynamic systems, in achieving more accurate and predictable outcomes compared to free-hand methods. The use of dynamic navigation not only enhances precision but also contributes to better preservation of dental structures and improved clinical efficiency.
Jain et al (2020) explored the use of a technologically advanced system incorporating optical guidance, computer assistance, and 3D navigation. Their system demonstrated efficient performance, achieving a mean horizontal deviation of 0.9 mm and a 3D divergence of 1.3 mm, with an average angular variation of 1.7°.26 This technology proved effective for accessing difficult, calcified canals. Similarly, Dianat et al (2020) focused on comparing the DNS and FHA approaches. The DNS method exhibited superior efficiency, identifying root canals in 96.6% of cases compared to 83.3% for the FHA group.29 Additionally, the DNS approach minimized tooth structure loss and reduced procedure time, emphasizing the significance of endodontist-led access cavity preparation. Kostunov et al31 (2020) evaluated guided versus conventional endodontics. While conventional methods located 100% of root canals, guided techniques achieved a 93.3% success rate. However, guided endodontics preserved more tooth structure, with incisors losing only 10.3 ± 1.1 mm³ of material. Despite these benefits, the guided approach involved higher radiation exposure, increased perforation risk, and greater costs, alongside challenges in removing dead tissue and inspecting canals. Similarly, Su et al (2021) examined the precision of guided access cavities. Their study revealed that 23 out of 117 cavities were initially inaccessible, though all were eventually accessed following canal negotiation. The study reported minimal deviations, with average linear deviations of 0.13 ± 0.21 mm at the coronal position and 0.46 ± 0.4 mm at the apical position, along with an angular deviation of 2.8 ± 2.6°. Notably, anterior teeth and premolars displayed better coronal precision than molars. The use of 3D-printed guides ensured precise access cavity preparation.1
All four studies highlight advancements in guided endodontics and related technologies, emphasizing improved accuracy and preservation of tooth structure. Jain et al (2020) and Su et al (2021) both underscore the precision of new systems, though Su’s study notes some initial accessibility challenges. Dianat et al (2020) and Kostunov et al (2020) provide valuable insights into the efficiency of different approaches, with Dianat emphasizing clinical effectiveness and Kostunov discussing trade-offs such as cost and radiation exposure. Together, these studies underline the evolving landscape of endodontic technologies, balancing precision with clinical practicality.1,26,31,58
While guided endodontics offers precision, tissue conservation, and improved canal detection, it presents several challenges. Restricted mouth openings, especially in posterior teeth, can limit the use of templates, as noted by Gambarini et al (2020). The inflexible nature of templates also restricts the clinician’s ability to modify the access axis during treatment. Additionally, template planning and manufacturing are time-consuming and labor-intensive processes.27
Another limitation GE stated Hildebrand et al (2023) reported that guided methods required more radiographs than conventional techniques, increasing radiation exposure. The need for CBCT imaging, though essential for detecting complex root morphologies and pathologies, introduces higher radiation doses compared to conventional radiography.33 Vasudevan et al (2023) also highlighted that static guided access (SGEA) achieved 100% canal success but was challenging to apply in patients with limited mouth opening, affecting posterior regions.34
Another issue lies in operator training. El Hakim et al (2023) noted that experienced operators performed better in freehand techniques, though non-restrictive guides reduced the dependency on experience. Moreover, the cost and availability of CBCT equipment and rapid prototyping technology pose barriers to widespread adoption. Despite these limitations, dynamic navigation offers flexibility to overcome some template constraints, though clinical studies are needed to validate these systems further. Guided endodontics is a promising technique, but it requires further refinement in areas such as operator training, template design, accessibility in posterior regions, and the balance between radiographic requirements and patient safety.35
Recent studies highlight the potential of guided endodontics to enhance access cavity preparation, minimize tooth substance removal, and improve treatment accuracy, regardless of the operator’s experience. Future research should prioritize the refinement of nonrestrictive guide designs to overcome limitations found in static templates, such as restricted lateral movements during drilling and challenges when accessing posterior teeth.33,35 Additionally, assessing the real-time applicability of dynamic navigation systems in clinical environments is crucial, particularly for complex cases involving calcified or narrow-root canals.32,63 Another important focus is the advancement of affordable and accessible 3D printing technologies, which could make guided endodontics more practical for everyday dental procedures.26 Furthermore, long-term clinical studies are necessary to confirm the effectiveness of guided approaches, particularly in maintaining the structural resilience of treated teeth and minimizing procedural errors over time.25,62
The development of guided endodontics offers exciting potential, but there are still areas that require further exploration. One key aspect is the application of dynamic navigation systems in clinical practice to validate their reliability and reduce variability caused by different operator skill levels, especially when working on calcified or posterior canals.34 Additionally, further improvements in minimally invasive access designs and their influence on the structural integrity and fracture resistance of treated teeth should be explored through longitudinal studies.
While integrating dynamic and static navigation systems has enhanced precision and reduced material loss, several challenges persist. Research is needed to assess the impact of DGEA on preserving tooth integrity, particularly in cases with complex anatomy or calcified canals.29,36 It is also essential to streamline guided systems by reducing the time and costs associated with intraoral scanning and guide production.27,29 Additionally, understanding how operator experience influences outcomes will aid in the development of standardized training programs, ensuring consistency across both static and dynamic navigation methods.27,36 Comparative clinical trials are needed to evaluate the clinical benefits of ultraconservative access cavities and their impact on long-term tooth durability, balancing the advantages of minimal invasiveness with effective cleaning.11 Finally, the integration of DNS with technologies such as augmented reality or artificial intelligence could further enhance decision-making and precision during endodontic procedures.29 In conclusion, guided access cavity preparation endodontic treatment using advanced technologies has shown great potential in improving the accuracy and predictability of endodontic therapy. Research shows that guided access cavity preparation endodontic treatment can improve dentin preservation and endodontic therapy accuracy. It is useful for root canal anomalies and difficult teeth, reducing unnecessary tooth removal and preventing complications. However, it is crucial for clinicians to consider its limitations and clinical applications before incorporating it.
Acknowledgments
We are grateful to all promoters, The Doctoral Programme Faculty of Medicine, Universitas Padjadjaran Indonesia, The Conservative Dentistry Department Faculty of Dentistry Universitas Padjadjaran Indonesia, The Department Oral Maxillofacial Surgery and Oral Diagnosis Kulliyyah of Dentistry International Islamic University Malaysia, The Faculty of Mechanical and Aerospace Engineering Institut Teknologi Bandung Indonesia, and Research Funder, Direktorat Riset dan Pengabdian Masyarakat Universitas Padjadjaran (DRPM UNPAD).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Su Y, Chen C, Lin C, et al. Guided endodontics: accuracy of access cavity preparation and discrimination of angular and linear deviation on canal accessing ability—an ex vivo study. BMC Oral Health. 2021;21(1):1–9. doi:10.1186/s12903-021-01936-y
2. Ribeiro D, Reis E, Marques JA, Falacho RI, Palma PJ. Guided endodontics: static vs. dynamic computer-aided techniques—a literature review. J Pers Med. 2022;12(9). doi:10.3390/jpm12091516
3. Chaves GS, Silva JA, Capeletti LR, et al. Guided access cavity preparation using a new simplified digital workflow. J Endod. 2023;49(1):89–95. doi:10.1016/j.joen.2022.11.004
4. Kamburoğlu K, Sönmez G, Koç C, Yılmaz F, Tunç O, Isayev A. Access cavity preparation and localization of root canals using guides in 3D-printed teeth with calcified root canals: an in vitro CBCT study. Diagnostics. 2023;13(13):2215. doi:10.3390/diagnostics13132215
5. Silva EJNL, De-Deus G, Souza EM, et al. Present status and future directions – minimal endodontic access cavities. Int Endod J. 2022;55(S3):531–587. doi:10.1111/iej.13696
6. Mohamed H, Ahmed A, Gutmann JL. Education for Prevention: A Viable Pathway for Minimal Endodontic Treatment Intervention. Endod Pract Today. 2015; 9: 283–285.
7. Murdoch-Kinch CA, McLean ME. Minimally invasive dentistry. J Am Dental Assoc. 2003;134(1):87–95. doi:10.14219/jada.archive.2003.0021
8. Gutmann J. Minimally invasive dentistry (endodontics). J Conserv Dent. 2013;16(4):282–283. doi:10.4103/0972-0707.114342
9. Silva EJNL, Pinto KP, Ferreira CM, et al. Current Status on Minimal Access Cavity Preparations: A Critical Analysis and a Proposal for a Universal Nomenclature. Vol. 53. Blackwell Publishing Ltd; 2020. doi:10.1111/iej.13391
10. Banerjee A. The CONTEMPORARY PRACTICE OF MINIMALLY INVASIVE DENTistry. Faculty Dent J. 2015;6(2):78–85. doi:10.1308/204268515x14174408396163
11. Gambarini G, Galli M, Morese A, et al. Digital design of minimally invasive endodontic access cavity. Appl Sci. 2020;10(10). doi:10.3390/app10103513
12. Celikten B, Koohnavard M, Oncu A, Sevimay FS, Orhan AI, Orhan K. A new perspective on minimally invasive endodontics: a systematic review. Biotechnol Biotechnol Equip. 2021;35(1):1758–1767. doi:10.1080/13102818.2021.2014966
13. Shah PK, Zhang Q, Chong BS. Get smart - technological innovations in endodontics. part 1: 3d imaging, 3d treatment planning and guided endodontics. Dent Update. 2021;48(6):479–484. doi:10.12968/DENU.2021.48.6.479
14. Chong BS, Dhesi M, Makdissi J. Computer-aided dynamic navigation: a novel method for guided endodontics. Quintessence Int. 2019;50(3):196–202. doi:10.3290/j.qi.a41921
15. Nayak A, Jain PK, Kankar PK, Jain N. Computer-aided design–based guided endodontic: a novel approach for root canal access cavity preparation. Proc Inst Mech Eng H. 2018;232(8):787–795. doi:10.1177/0954411918788104
16. Khademi JA, Trudeau M, Narayana P, Rabi RM, Baerg SD. Image-guided endodontics: the role of the endodontic triad. Dent Today. 2016;35(8).
17. Clark D, Khademi J. Modern molar endodontic access and directed dentin conservation. Dent Clin North Am. 2010;54(2):249–273. doi:10.1016/j.cden.2010.01.001
18. Leontiev W, Connert T, Weiger R, Dagassan-Berndt D, Krastl G, Magni E. Guided endodontics: three-dimensional planning and template-aided preparation of endodontic access cavities. J Visual Exp. 2022;2022(183):183. doi:10.3791/63781
19. Kinariwala N. Guided Endodontics. First. Kinariwala N, ed.. Springer International Publishing;2021. doi:10.1007/978-3-030-55281-7
20. Ambu E, Gori B, Marruganti C, et al. Influence of calcified canals localization on the accuracy of guided endodontic therapy: a case series study. Dent J. 2023;11(8):1–12. doi:10.3390/dj11080183
21. Yan Wang HL, Liu Y, Zheng TJ, Tang YP, Liu R, Liu R. Three-dimensional inlay-guided endodontics applied in variant root canals: a case report and review of literature. World J Clin Cases. 2021;9(36):11425–11436. doi:10.12998/wjcc.v9.i36.11425
22. da Silva DP, Silva IMR, Falcão LF, Falcão DF, Ferraz MÂAL, Falcão CAM. Penetration degree of sealer in artificial lateral canal after passive ultrasonic irrigation with EDTA for different times. Acta odontologica latinoamericana. 2019;32(2):51–56.
23. Marvaniya J, Agarwal K, Mehta DN, Parmar N, Shyamal R, Patel J. Minimal invasive endodontics: a comprehensive narrative review. Cureus. 2022;14(6). doi:10.7759/cureus.25984
24. JBI. Checklist for systematic reviews and research syntheses. The Joanna Briggs Institute. http://joannabriggs.org/research/critical-appraisal-tools.htmlwww.joannabriggs.org%0Awww.joannabriggs.org.
25. Connert T, Krug R, Eggmann F, et al. Guided endodontics versus conventional access cavity preparation: a comparative study on substance loss using 3-dimensional–printed teeth. J Endod. 2019;45(3):327–331. doi:10.1016/j.joen.2018.11.006
26. Jain SD, Saunders MW, Carrico CK, Jadhav A, Deeb JG, Myers GL. Dynamically navigated versus freehand access cavity preparation: a comparative study on substance loss using simulated calcified canals. J Endod. 2020;46(11):1745–1751. doi:10.1016/j.joen.2020.07.032
27. Gambarini G, Galli M, Morese A, et al. Precision of dynamic navigation to perform endodontic ultraconservative access cavities: a preliminary in vitro analysis. J Endod. 2020;46(9):1286–1290. doi:10.1016/j.joen.2020.05.022
28. Zubizarreta-Macho Á, Muñoz A de PAP, Deglow ERERER, Agustín-Panadero R, Álvarez JMJMJMJM. Accuracy of computer-aided dynamic navigation compared to computer-aided static procedure for endodontic access cavities: an in vitro study. J Clin Med. 2020;9(1):129. doi:10.3390/jcm9010129
29. Dianat O, Nosrat A, Tordik PA, et al. Accuracy and efficiency of a dynamic navigation system for locating calcified canals. J Endod. 2020;46(11):1719–1725. doi:10.1016/j.joen.2020.07.014
30. Loureiro MAZ, Elias MRA, Capeletti LR, et al. Guided endodontics: volume of dental tissue removed by guided access cavity preparation—an ex vivo study. J Endod. 2020;46(12):1907–1912. doi:10.1016/j.joen.2020.09.008
31. Kostunov J, Rammelsberg P, Klotz ALL, Zenthöfer A, Schwindling FS. Minimization of tooth substance removal in normally calcified teeth using guided endodontics: an in vitro pilot study. J Endod. 2020;47(2):286–290. doi:10.1016/j.joen.2020.10.025
32. Connert T, Leontiev W, Dagassan-Berndt D, et al. Real-time guided endodontics with a miniaturized dynamic navigation system versus conventional freehand endodontic access cavity preparation: substance loss and procedure time. J Endod. 2021;47(10):1651–1656. doi:10.1016/j.joen.2021.07.012
33. Hildebrand H, Leontiev W, Krastl G, et al. Guided endodontics versus conventional access cavity preparation: an ex vivo comparative study of substance loss. BMC Oral Health. 2023;23(1):1–8. doi:10.1186/s12903-023-03436-7
34. Vasudevan A, Sundar S, Surendran S, Natanasabapathy V. Tooth substance loss after incisal endodontic access and novel single-tooth template-guided endodontic access in three-dimensional printed resin incisors with simulated pulp canal calcification: a comparative in vitro study. J Conserv Dent. 2023;26(3):258–264. doi:10.4103/jcd.jcd_3_23
35. Elhakim A, Hwang J, Kim S, Kim E, Kang S. Three-dimensional accuracy of endodontic access preparations using novel nonrestrictive static guides: a laboratory study. Aust Endodontic J. 2023;49(3):631–640. doi:10.1111/aej.12792
36. Huth KC, Borkowski L, Liebermann A, et al. Comparing accuracy in guided endodontics: dynamic real-time navigation, static guides, and manual approaches for access cavity preparation – an in vitro study using 3D printed teeth. Clin Oral Investig. 2024;28(4):1–9. doi:10.1007/s00784-024-05603-8
37. Torres A, Dierickx M, Coucke W, Pedano MS, Lambrechts P, Jacobs R. In vitro study on the accuracy of sleeveless guided endodontics and treatment of a complex upper lateral incisor. J Dent. 2023:131. doi:10.1016/j.jdent.2023.104466
38. Haarmann B, Leontiev W, Magni E. Accuracy of guided endodontics in posterior teeth. Appl Sci. 2023:
39. Torres A, Dierickx M, Coucke W, Pedano MS, Lambrechts P, Jacobs R. Ex-vivo and in-vivo validation of a novel measuring protocol for guided endodontics. J Dent. 2023:135. doi:10.1016/j.jdent.2023.104566
40. Christofzik DW, Glandorf P, Conrad J, Fawzy El-Sayed KM, Größner-Schreiber B, Dörfer CE. 2D radiographs, cone-beam computed tomography and 3D CBCT- based planning software in access cavity preparation: a single blinded randomised controlled in vitro study. Aust Endod J. 2022;48(2):283–296. doi:10.1111/aej.12566
41. Koch GK, Gharib H, Liao P, Liu H Guided access cavity preparation using cost-effective 3D printers. J Endod. 2022;48(7):909–913. doi:10.1016/j.joen.2022.04.005
42. Jain SD, Carrico CK, Bermanis I. 3-dimensional accuracy of dynamic navigation technology in locating calcified canals. J Endod. 2020;46(6):839–845. doi:10.1016/j.joen.2020.03.014
43. Reeh ES, Messer HH, Douglas WH. Reduction in tooth stiffness as a result of endodontic and restorative procedures. J Endod. 1989;15(11):512–516. doi:10.1016/S0099-2399(89)80191-8
44. Jiang Q, Huang Y, Tu XR, Li Z, He Y, Yang X. Biomechanical properties of first maxillary molars with different endodontic cavities: a finite element analysis. J Endod. 2018;44(8):1283–1288. doi:10.1016/j.joen.2018.04.004
45. Wang X, Wang W, Wang D, et al. The effects of different endodontic cavities on the fracture resistance of endodontically treated mandibular first molars-a three-dimensional finite element analysis. 2022.
46. Lang H, Korkmaz Y, Schneider K, Raab WHM. Impact of endodontic treatments on the rigidity of the root. J Dent Res. 2006;85(4):364–368. doi:10.1177/154405910608500416
47. Kishen A, Kumar GV, Chen NN. Stress-strain response in human dentine: rethinking fracture predilection in postcore restored teeth. Dental Traumatol. 2004;20(2):90–100. doi:10.1111/j.1600-4469.2004.00250.x
48. Ramachandran P, PradeepKumar AR, Ravishankar P, Kishen A. In vivo strain alterations in mandibular molars after root canal treatment procedures. J Endod. 2020;46(12):1849–1855. doi:10.1016/j.joen.2020.07.021
49. Huynh N, Li FC, Friedman S, Kishen A. Biomechanical effects of bonding pericervical dentin in maxillary premolars. J Endod. 2018;44(4):659–664. doi:10.1016/j.joen.2018.01.002
50. Hudon C, Danish A, Lambert M, et al. Reconciling validity and challenges of patient comfort and understanding: guidelines to patient-oriented questionnaires. Health Expectations. 2022;25(5):2147–2154. doi:10.1111/hex.13373
51. Rabi RM, Baerg SD. Image-Guided Endodontics: The Role of the Endodontic Triad. Contin Edu; 35(8):94
52. Lima TO, de Oliveira Rocha A, Menezes Dos Anjos L, et al. A global overview of guided endodontics: a bibliometric analysis. J Endod. 2024;50:10–16. doi:10.1016/j.joen.2023.10.002;.
53. Loureiro MAZ, Silva JA, Chaves GS, Capeletti LR, Estrela C, Decurcio DA. Guided endodontics: the impact of new technologies on complex case solution. Aust Endodontic J. 2021;47(3):664–671. doi:10.1111/aej.12498
54. Gt D, Saxena P, Gupta S. Static vs. dynamic navigation for endodontic microsurgery - A comparative review. J Oral Biol Craniofac Res. 2022;12(4):410–412. doi:10.1016/j.jobcr.2022.04.010
55. Tang W, Jiang H. Comparison of static and dynamic navigation in root-end resection performed by experienced and inexperienced operators: an in vitro study. J Endod. 2023; 49(3):294–300. doi:10.1016/j.joen.2022.11.016.
56. Block MS, Emery RW. Static or dynamic navigation for implant placement - choosing the method of guidance. J Oral Maxillofacial Surg. 2016;74(2):269–277. doi:10.1016/j.joms.2015.09.022
57. Moreno-Rabié C, Torres A, Lambrechts P, Jacobs R. Clinical applications, accuracy and limitations of guided endodontics: a systematic review. Int Endod J. 2020;53(2):214–231. doi:10.1111/iej.13216
58. Dianat O, Gupta S, Price JB, Mostoufi B. Guided endodontic access in a maxillary molar using a dynamic navigation system. J Endod. 2021;47(4):658–662. doi:10.1016/j.joen.2020.09.019
59. Zehnder MS, Connert T, Weiger R, Krastl G, Kühl S. Guided endodontics: accuracy of a novel method for guided access cavity preparation and root canal location. Int Endod J. 2016;49(10):966–972. doi:10.1111/iej.12544
60. Krastl G, Zehnder MS, Connert T, Weiger R, Kühl S. Guided Endodontics: a novel treatment approach for teeth with pulp canal calcification and apical pathology. Dental Traumatol. 2016;32(3):240–246. doi:10.1111/edt.12235
61. Buchgreitz J, Buchgreitz M, Bjørndal L. Guided root canal preparation using cone beam computed tomography and optical surface scans – an observational study of pulp space obliteration and drill path depth in 50 patients. Int Endod J. 2019;52(5):559–568. doi:10.1111/iej.13038
62. Guzmán AM, Deglow ER, Zubizarreta-Macho Á, Agustín-Panadero R, Montero SH. Accuracy of computer-aided dynamic navigation compared to computer-aided static navigation for dental implant placement: an in vitro study. J Clin Med. 2019;8(12). doi:10.3390/jcm8122123
63. Zubizarreta-Macho Á, Castaño SV, Montiel-Company JM, Mena-álvarez J. Effect of computer-aided navigation techniques on the accuracy of endodontic access cavities: a systematic review and meta-analysis. Biology. 2021;10(3). doi:10.3390/biology10030212
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.