Back to Journals » Clinical Ophthalmology » Volume 17
A Systematic Review of Digital Ophthalmoscopes in Medicine
Authors Robles R ![]() , Patel N
, Patel N ![]() , Neag E, Mittal A, Markatia Z, Ameli K, Lin B
, Neag E, Mittal A, Markatia Z, Ameli K, Lin B
Received 6 July 2023
Accepted for publication 22 September 2023
Published 6 October 2023 Volume 2023:17 Pages 2957—2965
DOI https://doi.org/10.2147/OPTH.S423845
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rafael Robles,1 Nikhil Patel,2 Emily Neag,2 Ajay Mittal,3 Zahra Markatia,2 Kambiz Ameli,2 Benjamin Lin2
1Department of Ophthalmology, Virginia Commonwealth University School of Medicine, Richmond, VA, USA; 2Bascom Palmer Eye Institute, University of Miami, Miami, FL, USA; 3Department of Ophthalmology, University of Florida College of Medicine, Gainesville, FL, USA
Correspondence: Benjamin Lin, Bascom Palmer Eye Institute, University of Miami, 900 NW 17th Street, Miami, FL, 33136, USA, Tel +1 305 326-6000, Fax +1 305 326-6000, Email [email protected]
Purpose: Recent advances in telemedicine have led to increased use of digital ophthalmoscopes (DO) in clinical settings. This review aims to assess commercially available DOs, including smartphone (SP), desktop, and handheld ophthalmoscopes, and evaluate their applications.
Methods: A literature review was performed by searching PubMed (pubmed.ncbi.nlm.nih.gov), Web of Science (webofknowledge.com), and Science Direct (sciencedirect.com). All English-language papers that resulted from the search terms “digital ophthalmoscope”, “screening tool”, “glaucoma screening”, “diabetic retinopathy screening”, “cataract screening”, and “papilledema screening” were reviewed. Studies that contained randomized clinical trials with human participants between January 2010 and December 2020 were included. The Risk of Bias in Systematic Reviews (ROBIS) tool was used to assess the methodological quality of each included paper.
Results: Of the 1307 studies identified, 35 met inclusion and exclusion criteria. The ROBIS tool determined that 29/35 studies (82.8%) had a low risk of bias, 3/35 (8.5%) had a moderate risk of bias, and 3/35 (8.5%) had a high risk of bias.
Conclusion: The continued adoption of DOs remains uncertain because of concerns about the image quality for non-mydriatic eyes and the confidence in data captured from the device. Likewise, there is a lack of guidelines for the use of DOs, which makes it difficult for providers to determine the best device for their practice and to ensure appropriate use. Even so, DOs continue to gain acceptance as technology and practice integration improve, especially in underserved areas with limited access to ophthalmologists.
Keywords: fundoscopy, teleophthalmology, diagnostics, screening, referral
Introduction
Three of the leading causes of preventable vision loss worldwide are glaucoma, cataracts, and diabetic retinopathy (DR). A major contributing factor to vision loss due to these conditions is inadequate access to care, leading to late diagnosis and treatment. As of October 2019, it was estimated that more than half of the 3 million Americans with glaucoma were unaware of their condition.1 Cataracts account for one in three cases of blindness and one in six cases of visual impairment, highlighting the need for treatment.2 The increasing prevalence of systemic risk factors in the aging US population is expected to accelerate onset of these ocular manifestations.3,4
Limited access due to geographic barriers, high costs, lack of patient education, and transportation create additional challenges.5–7 Pervasive barriers in urban populations including transportation and physical disability have contributed to a 25% prevalence of undiagnosed diabetic retinopathy.7 Movement of screening and follow-up appointments to teleophthalmology may mitigate these obstacles.5
The limited cadre trained to operate traditional direct ophthalmoscopes and biomicroscopy precludes their use as a screening tool universally. These systems are restricted to ophthalmology clinics and emergency departments. A digital solution can decentralize this, allowing remote providers to monitor screening and refer patients to ophthalmologists when necessary. This article categorizes and reviews the current progress of digital ophthalmoscopy, referred to as computer-aided, handheld-, and smartphone-based devices which digitize available systems of direct ophthalmoscopy.
Materials and Methods
Inclusion Criteria
The eligibility criteria for this review included a systematic search using PubMed, Web of Science, and Science Direct. The included studies estimate the size and direction of the effect of interventions presented as numerical data on an individual study-level basis and with quantitative synthesis (meta-analysis). Additionally, the classification of the type of DO subdivided the category into three groups: desktop-based digital ophthalmic devices, handheld digital ophthalmic devices, and smartphone-based retinal imaging DO in either a mydriatic or non-mydriatic fashion. Ophthalmology patients were defined as those who were diagnosed and treated for an ophthalmic condition at the beginning of the study. Further, we included studies involving participants who had glaucoma, diabetic retinopathy, and cataracts.
Search Strategy and Screening
PubMed, Web of Science, and Science Direct were searched from 2010 to 2020. The search keywords for each database included: “digital ophthalmoscope”, “screening tool”, “glaucoma screening”, “diabetic retinopathy screening”, “cataract screening”, and “papilledema screening.” Studies were limited to randomized clinical trials published between January 2010-December 2020 involving human subjects and written in English (Figure 1).
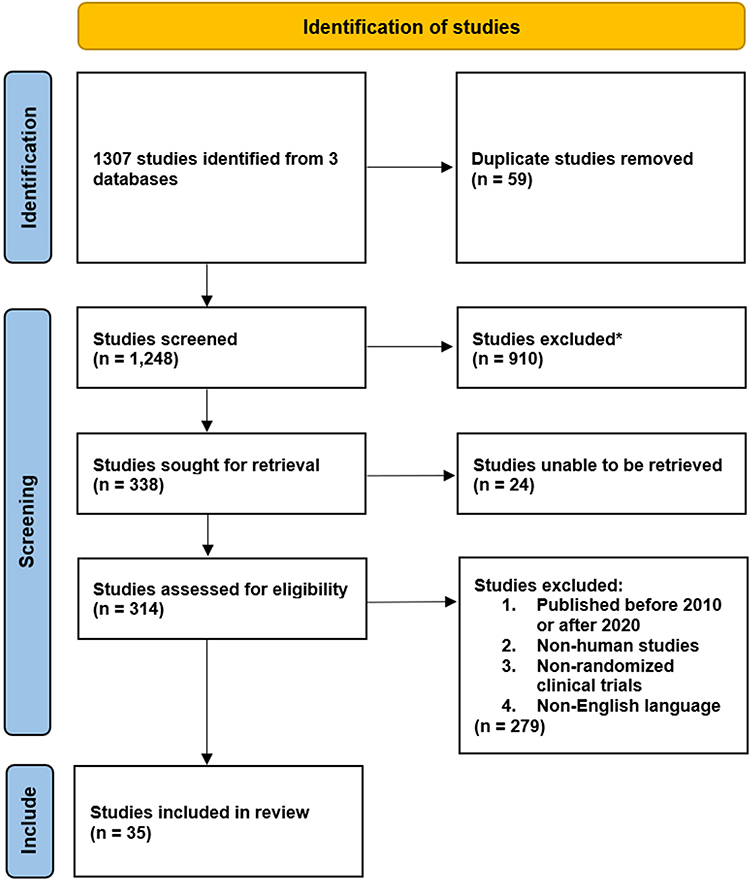 |
Figure 1 PRISMA flow diagram illustrating the study selection process for the systematic review. *Records excluded after manual review by authors determined that studies were not relevant to the current review. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow et al The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons. |
In addition to the literature review database search, relevant studies were reviewed by the coauthors for relevance to the area of focus of the paper. Assessments of the study design, population, intervention, and methodology were completed during the review process.
Outcomes
The reported outcomes included comparing manufacturing companies, price, field of view (FOV), and size among the different DOs. Furthermore, the DOs were compared using cup-to-disc (c/d) ratios, kappa (κ) coefficient for interrater image quality, accuracy, and ophthalmic disease detection sensitivity. When more than one review included the same studies, the review that reported the most complete presentation of the results was selected for inclusion in the overview.
Assessment of Methodological Quality
We assessed the methodological quality of each included study using the Risk of Bias In Systematic Reviews (ROBIS) tool. Two review authors (AM and NP) independently performed quality assessments. Disagreements regarding the overall assessments were resolved through discussion, with a third reviewer as the final arbitrator (RR). The rationale behind assessments was documented. We calculated the measures of agreement and reliability between raters for each ROBIS domain.
Data Synthesis
We stratified the included systematic reviews by type of pathology assessed (glaucoma, diabetic retinopathy, cataracts), type of DO, and type of analysis (with or without meta-analysis). When a meta-analysis was performed, we reported pooled estimates using the models and measures of effect reported by systematic review authors with 95% confidence intervals (CIs). These measures included the sensitivity and specificity of each device for detecting various outcomes. Further, a κ-coefficient statistical analysis, which measures the degree of interrater agreement between variables, was recorded from the studies identified for this review and was included when possible. No additional statistical analyses were performed.
Results
Results of the Literature Search
We obtained a total of 1307 citations through database searches. Following the application of the inclusion and exclusion criteria, 35 published studies were included in the analysis. They contained data on diabetic retinopathy, glaucoma, cataracts, functionality, and comparison reports related to digital ophthalmoscopes.
Methodological Quality
Using the ROBIS tool, 29/35 studies (82.8%) had a low risk of bias, 3/35 (8.5%) had a moderate risk of bias, and 3/35 (8.5%) had a high risk of bias across all the ROBIS domains. These include study eligibility criteria, identification and selection of studies, data collection and appraisal, and synthesis and findings.
Digital Ophthalmoscope Use in Screening for Ophthalmic Disease
Smartphone-Based Retinal Imaging in Diabetic Retinopathy
With respect to diabetic retinopathy, Karakaya et al8 compared the ability of various smartphone-based retinal cameras, including iExaminer (Welch Allyn; Skaneateles Falls, NY, USA), D-EYE (D-EYE Srl; Padova, Italy), Peek Retina (Nesta, London, UK), and iNview (Volk Optical Inc.; Mentor, OH, USA) (Table 1). Data on the sensitivity and specificity of each device for detecting DR were used as comparative metrics (Table 2). Russo et al9 utilized the International Clinical Diabetic Retinopathy Disease Severity scale10 to compare DR grading agreement between a slit-lamp biomicroscope and D-EYE, a digital retinal camera magnetically attached to an iPhone 5 (Apple Inc.; Cupertino, CA, USA). The latter showed greater sensitivity to lens transparency and pupil diameter with a higher portion of images deemed ungradeable. However, the D-Eye’s 8 megapixel camera, offers approximately 150 pixels per retinal degree which exceeds the standard benchmark resolution set by the United Kingdom’s National Health Service for effective detection of retinopathy (6 megapixels and 30 pixels per degree).11 Prathiba et al12 tested the ability of a non-mydriatic fundus on phone (FOP) smartphone-based nonmydriatic retinal imaging camera (FOP NM-10; Remedio Innovative Solutions Pvt. Ltd, Bangalore, India) to detect sight-threatening diabetic retinopathy (STDR). A sensitivity of 88% and 82% was determined by two graders, respectively, with a high specificity of 99% to detect STDR when compared with a Zeiss FF450 desktop mydriatic fundus camera (Zeiss; Jena, Germany). Several studies used the κ-coefficient between graders to assess overall image quality (Table 2).
 |
Table 1 Comparison of Digital Ophthalmoscopes and Classification |
 |
Table 2 Comparison of Digital Ophthalmoscope in Various Ocular Pathologies |
Computer-Aided & Handheld Non-Mydriatic Imaging in Diabetic Retinopathy
Malerbi et al13 revealed agreement as a screening tool regarding the classification of diabetic retinopathy for observation or referral when comparing binocular indirect ophthalmoscopy (BIO) to telemedicine protocols using a Canon CR-s Digital Retinal Camera (Canon Medical Systems; Amstelveen, Netherlands) for DR screening. However, there was poor agreement in terms of actual classifiation of DR. This disagreement was thought to be due to the limitations of BIO in detecting minor changes, like microaneurysms,neovascularization, or macular edema.
Smartphone-Based Retinal Imaging in Glaucoma
Russo et al14 compared smartphone ophthalmoscopy using a D-EYE adapter on an iPhone 5s (Apple Inc.; Cupertino, CA, USA) with slit-lamp indirect biomicroscopy to assess undilated vertical cup-to-disc ratio (VCDR) (Figure 2). D-EYE identification of optic nerve was feasible in 104 of 107 eyes, and two masked glaucoma specialists deemed the modalities to have significant grading agreement in 73.4% of cases (κ = 0.63, p < 0.001). A low-cost molded plastic adapter was manufactured and clipped over a Samsung Galaxy SIII smartphone (Samsung Electronics Co.; Seoul, South Korea) in the 2014 Giardini et al16 glaucoma screening cohort, which yielded no significant difference in VCDR between dilated Digital Retinal Camera (DRS+, Haag Streit CenterVue, Italy) footage and smartphone-acquired footage (p = 0.98). In a follow-up assessment of the Nakuru Eye Disease Cohort study of primary open-angle glaucoma incidence, amongst other diseases, Bastawrous et al15 used Peak Retina, a prism adapter, over a Samsung SIII GT-I9300 smartphone (Samsung Electronics Co.; Seoul, South Korea) to image optic nerve heads. No discernable difference was noted between mydriatic photographs taken with a lay photographer using Peek Retina when compared to an experienced retinal photographer. The results showed that the image quality obtained with the smartphone adapter allowed for effective glaucomatous disc grading17 (Table 2).
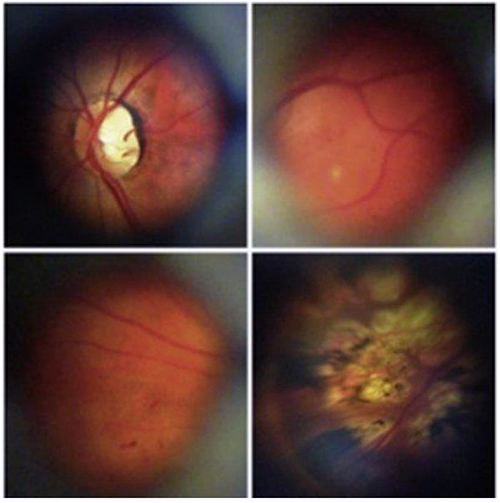 |
Figure 2 Representative retinal images of no apparent diabetic retinopathy (top left), mild nonproliferative diabetic retinopathy (top right), moderate nonproliferative diabetic retinopathy (bottom left), and panretinal photocoagulation scars in proliferative diabetic retinopathy (bottom right). Notes: Reprinted from AmJ Ophthalmol, volume 159(2), Russo A, Morescalchi F, Costagliola C, Delcassi L, Semeraro F. Comparison of smartphone ophthalmoscopy with slit-lamp biomicroscopy for grading diabetic retinopathy. 360–364.e1, Copyright 2015, with permission from Elsevier.9 |
Computer-Aided Imaging in Glaucoma
Issac et al17 reported the application of adaptive threshold-based fundus processing for glaucoma screening. This threshold-based method functions in lieu of cumbersome manual segmentation of optic disc and cup with color intensity discernment to generate a binary image. After initial fundus imaging with a Welch Allyn PanOptic Ophthalmoscope (Welch Allyn; Skaneateles Falls, NY, USA), optic cup segmentation was done by green channel histogram, followed by “ISNT” feature selection20 including c/d ratio, neuroretinal rim (NRR) area, and blood vessel area. Sixty-seven images rendered with Artificial Neural Network and Support Vector Machine classifiers obtained a diagnostic accuracy of 94.1%, specificity of 90%, and sensitivity of 100%. Alternative computer aided diagnostics include superpixel segmentation and vessel kinking for optic cup boundary detection are also becoming implemented for detection of glaucomatous discs.21
Smartphone-Based Retinal Imaging in Cataracts
A study by Dickson et al18 utilized a D-EYE DO to analyze the presence of abnormalities, VCDR, and optic nerve size and color compared to the results of BIO. Three D-EYE examiners reviewed the videos for fundus abnormalities, optic-disc characteristics and c/d ratios. The results showed no statistical difference between the D-EYE and BIO mean c/d ratios. The study concluded that the D-EYE could reliably be used clinically to detect abnormalities and measure the c/d ratio, including in some patients with cataracts. Also, a study from 2017 used a 20D Volk Spherical lens (Volk Optical Inc.; Mentor, OH, USA) and a smartphone to examine the anterior segment and fundus. The results showed that the diagnostic technique was suitable for photo documentation and could successfully identify various diseases, including cataracts, in the patient populations19 (Table 2).
Discussion
Limitations of Digital Ophthalmoscopes
As of yet, there are limited repositories available to compare commercially available DO systems. The standard of retinal imaging involves using a desktop mydriatic fundus camera. However, these desktop-based DOs have drawbacks such as being cumbersome, confined to office settings, technician-dependent, and costly.12,22 The 3nethra device (Forus, Bangalore) is the most affordable option within this category, whereas Optos Daytona (Optos PLC; Dunfermline, UK) provides the best FOV (45°–200°) (Table 1). Although not considered the standard of care, handheld non-mydriatic DOs offer certain advantages, such as being lightweight, portable, and suitable for dilated and non-dilated patients.23
Numerous studies have evaluated handheld cameras for detecting diabetic retinopathy with relatively high sensitivities and specificities.24–26 Nevertheless, these devices have their own sets of limitations, such as the need for consistent manual alignment to maintain focus, and issues with light reflexes on the condensing lens.12,27 The most affordable option among direct ophthalmoscopes is the handheld PanOptic, while the Versacam provides the best FOV (45°) (Table 1 and 2).
Emerging smartphone-based DOs present another viable alternative. Their compact size makes them lightweight, ergonomically friendly, and easily transportable.14 They do not require dilation and necessitate minimal training, making them ideal for non-specialists and telemedicine in rural areas.12,22,24 Multiple aforementioned studies have found the D-EYE smartphone reliable in examining DR, glaucoma, cataracts, and even hypertensive emergencies. The Peek Retina is the most inexpensive in this group, while the 20D Volk lens paired with a smartphone offers the best FOV (60°). Among smartphone-based DO options, we recommend using a 20D Volk lens paired with a smartphone for fundus photography, given its wide FOV, affordability, and versatility (Table 1).
Overall, DOs are portable, cost-effective, facilitate collaboration, and are user-friendly.28,29 Still, some existing fundus cameras have a limited FOV, necessitate frequent pupillary dilation, and require skilled operators to produce montage images.30 Enhancements in optical designs are needed to expand the FOV further and improve image quality. Encouragingly, research has demonstrated that DOs offer an improved FOV compared with traditional ophthalmoscopes without mydriasis. This could be further enhanced by utilizing 3D imaging or software that intelligently stitches multiple images together, enabling the capture of different regions of the peripheral retina.31
Device Training & Ophthalmologist Workload
Many studies have emphasized the significance of proper training and the time required to acquire the skills necessary to capture high-quality retinal images or videos effectively. Despite sufficient practice, challenges with focusing and dealing with bothersome lens reflections may arise.27 Consequently, the quality of the captured images and the accuracy of the test results could potentially fail to identify underlying pathologies.
As more areas facing eye specialist shortages begin to employ DOs, specialists may be inundated with images for review. Integrating artificial intelligence and machine learning to analyze captured images is a viable solution to alleviate this burden.32 Further research is required to develop effective training guidelines for user-friendly ophthalmoscopes to ensure the capture and analysis of high-quality data that can be accurately assessed efficiently with machine learning algorithms.
Privacy Concerns
Some of the significant concerns regarding the use of DOs are privacy and security risks related to online storage and transfer of captured images or videos.33,34 One study on health information technology demonstrated that some patients refused to participate because of perceived privacy and security risks.33 Similarly, another study highlighted how clinicians fear data loss and confidentiality risks.34 DO developers should follow HIPAA guidelines, remove any protected health information, and encrypt their data on secure applications, private networks, or third-party management software.35
Limitations of the Review Process
The search was limited to articles written between 2010 and 2020 and written in English, possibly introducing bias and concerns of applicability in non-English populations. Our search included three databases, potentially overlooking the pertinent studies available in other databases. Our inclusion criteria focused on predetermined ophthalmic conditions which excludes other relevant DO analyses. Future research should address these limitations to provide a more robust understanding of the effectiveness of digital ophthalmoscopy in various ophthalmic conditions.
Conclusion
Digital ophthalmoscopy methods offer novel algorithms to optimize anterior and posterior segment evaluation. Such systems may augment current access to care by providing more affordable and accessible diagnostic tools for remote communities with limited specialists. This systematic review suggests effectiveness of DOs in evaluating diabetic retinopathy, glaucoma, and cataracts with respect to traditional ophthalmoscopy. Integrating this imaging with geo-tagging could also enable further database creation that can help improve resource allocation in worldwide screening programs. With ongoing development, the ability for DOs to handle non- mydriatic photography and media opacities will likely continue to improve. Given the challenges inherent in providing high quality ophthalmic care in rural or otherwise underserved communities, the ongoing improvement of DO technologies should be a priority.
Acknowledgments
The authors have no individuals or organizations to acknowledge in relation to this study.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. American Academy of Ophthalmology. Undiagnosed Glaucoma — a pressing U.S. Problem; 2019. Available from: https://www.aao.org/eyenet/academy-live/detail/undiagnosed-glaucoma-pressing-u-s-problem.
2. Khairallah M, Kahloun R, Bourne R, et al. Number of people blind or visually impaired by cataract worldwide and in world regions, 1990 to 2010. Invest Ophthalmol Vis Sci. 2015;56(11):6762–6769. doi:10.1167/iovs.15-17201
3. Salongcay RP, Silva PS. The role of teleophthalmology in the management of diabetic retinopathy. Asia Pac J Ophthalmol Phila Pa. 2018;7(1):17–21. doi:10.22608/APO.2017479
4. Kovarik JJ, Eller AW, Willard LA, Ding J, Johnston JM, Waxman EL. Prevalence of undiagnosed diabetic retinopathy among inpatients with diabetes: the diabetic retinopathy inpatient study (DRIPS). BMJ Open Diabetes Res Care. 2016;4(1):e000164. doi:10.1136/bmjdrc-2015-000164
5. Saleem SM, Pasquale LR, Sidoti PA, Tsai JC. Virtual ophthalmology: telemedicine in a COVID-19 Era. Am J Ophthalmol. 2020;216:237–242. doi:10.1016/j.ajo.2020.04.029
6. Maa AY, Wojciechowski B, Hunt KJ, et al. Early experience with Technology-Based Eye Care Services (TECS): a novel ophthalmologic telemedicine initiative. Ophthalmology. 2017;124(4):539–546. doi:10.1016/j.ophtha.2016.11.037
7. Ramchandran RS, Yilmaz S, Greaux E, Dozier A. Patient perceived value of teleophthalmology in an urban, low-income US population with diabetes. PLoS One. 2020;15(1):e0225300. doi:10.1371/journal.pone.0225300
8. Karakaya M, Hacisoftaoglu RE. Comparison of smartphone-based retinal imaging systems for diabetic retinopathy detection using deep learning. BMC Bioinform. 2020;21(4):259. doi:10.1186/s12859-020-03587-2
9. Russo A, Morescalchi F, Costagliola C, Delcassi L, Semeraro F. Comparison of smartphone ophthalmoscopy with slit-lamp biomicroscopy for grading diabetic retinopathy. Am J Ophthalmol. 2015;159(2):360–364.e1. doi:10.1016/j.ajo.2014.11.008
10. Wilkinson CP, Ferris FL, Klein RE, et al. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology. 2003;110:1677–1682. doi:10.1016/S0161-6420(03)00475-5
11. Denniston AK, Lee AY, Lee CS, et al. United Kingdom Diabetic Retinopathy Electronic Medical Record (UK DR EMR) users group: report 4, real-world data on the impact of deprivation on the presentation of diabetic eye disease at hospital services. Br J Ophthalmol. 2019;103(6):837–843. PMID: 30269098; PMCID: PMC6582816. doi:10.1136/bjophthalmol-2018-312568
12. Prathiba V, Rajalakshmi R, Arulmalar S, et al. Accuracy of the smartphone-based nonmydriatic retinal camera in the detection of sight-threatening diabetic retinopathy. Indian J Ophthalmol. 2020;68(Suppl 1):S42. doi:10.4103/ijo.IJO_1937_19
13. Malerbi FK, Morales PH, Farah ME, et al. Comparison between binocular indirect ophthalmoscopy and digital retinography for diabetic retinopathy screening: the multicenter Brazilian type 1 diabetes study. Diabetol Metab Syndr. 2015;7(1):116. doi:10.1186/s13098-015-0110-8
14. Russo A, Mapham W, Turano R, et al. Comparison of smartphone ophthalmoscopy with slit-lamp biomicroscopy for grading vertical cup-to-disc ratio. J Glaucoma. 2016;25(9):e777. doi:10.1097/IJG.0000000000000499
15. Bastawrous A, Giardini ME, Bolster NM, et al. Clinical validation of a smartphone-based adapter for optic disc imaging in Kenya. JAMA Ophthalmol. 2016;134(2):151–158. PMID: 26606110; PMCID: PMC5321504. doi:10.1001/jamaophthalmol.2015.4625
16. Giardini ME, Livingstone IAT, Jordan S, et al. A smartphone based ophthalmoscope. Annu Int Conf IEEE Eng Med Biol Soc IEEE Eng Med Biol Soc Annu Int Conf. 2014;2014:2177–2180. doi:10.1109/EMBC.2014.6944049
17. Issac A, Partha Sarathi M, Dutta MK. An adaptive threshold based image processing technique for improved glaucoma detection and classification. Comput Methods Programs Biomed. 2015;122(2):229–244. doi:10.1016/j.cmpb.2015.08.002
18. Dickson D, Fouzdar-Jain S, MacDonald C, et al. Comparison study of funduscopic exam of pediatric patients using the D-EYE method and conventional indirect ophthalmoscopic methods. Open J Ophthalmol. 2017;7(3):145–152. doi:10.4236/ojoph.2017.73020
19. Furdova A, Furdova A, Krcmery V. Our experience with smartphone and spherical lens for the eye fundus examination during humanitarian project in Africa. Int J Ophthalmol. 2017;10(1):157–160. doi:10.18240/ijo.2017.01.25
20. Jonas JB, Budde WM, Lang P. Neuroretinal rim width ratios in morphological glaucoma diagnosis. Br J Ophthalmol. 1998;82(12):1366–1371. PMID: 9930265; PMCID: PMC1722465. doi:10.1136/bjo.82.12.1366
21. Ávila FJ, Bueno JM, Remón L. Superpixel-based optic nerve head segmentation method of fundus images for glaucoma assessment. Diagnostics. 2022;12(12):3210. PMID: 36553217; PMCID: PMC9777478. doi:10.3390/diagnostics12123210
22. Kyari F, Gilbert C. Agreement in measurement of optic cup-to-disc ratio with stereo biomicroscope funduscopy and digital image analysis: results from the Nigeria national blindness and visual impairment survey. Ophthalmic Epidemiol. 2017;24(1):57–62. doi:10.1080/09286586.2016.1254806
23. Zhang W, Nicholas P, Schuman SG, et al. Screening for diabetic retinopathy using a portable, noncontact, nonmydriatic handheld retinal camera. J Diabetes Sci Technol. 2017;11(1):128–134. doi:10.1177/1932296816658902
24. Kortüm K, Müller M, Hirneiß C, et al. Smart eye data: Entwicklung eines Fundaments für medizinische Forschung mittels Smart-DataApplikationen [Smart eye data: development of a foundation for medical research using Smart Data applications]. Ophthalmol Z Dtsch Ophthalmol Ges. 2016;113(6):469–477. German. doi:10.1007/s00347-016-0272-2
25. Keel S, Scheetz J, Holloway E, et al. Utilisation and perceptions towards smart device visual acuity assessment in Australia: a mixed methods approach. BMJ Open. 2019;9(3):e024266. doi:10.1136/bmjopen-2018-024266
26. Choudhri AF, Chatterjee AR, Javan R, Radvany MG, Shih G. Security issues for mobile medical imaging: a primer. RadioGraphics. 2015;35(6):1814–1824. doi:10.1148/rg.2015140039
27. Shanmugam MP. Video indirect ophthalmoscopy using a hand-held video camera. Indian J Ophthalmol. 2011;59(1):53–55. doi:10.4103/0301-4738.73718
28. Muiesan ML, Salvetti M, Paini A, et al. Ocular fundus photography with a smartphone device in acute hypertension. J Hypertens. 2017;35(8):1660–1665. doi:10.1097/HJH.0000000000001354
29. Wu Y, Wei Z, Yao H, et al. TeleOph: a secure real-time teleophthalmology system. IEEE Trans Inf Technol Biomed. 2010;14(5):1259–1266. doi:10.1109/TITB.2010.2058124
30. Toslak D, Liu C, Alam M Nur and Yao X. (2018). Near-infrared light-guided miniaturized indirect ophthalmoscopy for nonmydriatic wide-field fundus photography. Opt. Lett., 43(11), 2551 10.1364/OL.43.002551
31. Mamtora S, Sandinha MT, Ajith A, Song A, Steel DHW. Smart phone ophthalmoscopy: a potential replacement for the direct ophthalmoscope. Eye. 2018;32(11):1766–1771. doi:10.1038/s41433-018-0177-1
32. Ting DSW, Pasquale LR, Peng L, et al. Artificial intelligence and deep learning in ophthalmology. Br J Ophthalmol. 2019;103(2):167–175. doi:10.1136/bjophthalmol-2018-313173
33. Zheng K, Abraham J, Novak LL, Reynolds TL, Gettinger A. A survey of the literature on unintended consequences associated with health information technology: 2014–2015. Yearb Med Inform. 2016;(1):13–29. doi:10.15265/IY-2016-036
34. Dabasia PL, Edgar DF, Garway-Heath DF, Lawrenson JG. A survey of current and anticipated use of standard and specialist equipment by UK optometrists. Ophthalmic Physiol Opt. 2014;34(5):592–613. doi:10.1111/opo.12150
35. Aanensen DM, Huntley DM, Feil EJ, al-Own F, Spratt BG. EpiCollect: linking smartphones to web applications for epidemiology, ecology and community data collection. PLoS One. 2009;4(9):e6968. doi:10.1371/journal.pone.0006968
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Ultra-Widefield Imaging as a Teleophthalmology Screening Tool for Ocular Pathology
Ahmad TR, Situ WA, Chan NT, Keenan JD, Stewart JM
Clinical Ophthalmology 2023, 17:3225-3234
Published Date: 30 October 2023