Back to Journals » Patient Preference and Adherence » Volume 17
A Systematic Review and Meta-Analysis of the Effectiveness of Adherence Therapy and Its Treatment Duration in Patients with Schizophrenia Spectrum Disorders
Authors Li IH, Hsieh WL ![]() , Liu WI
, Liu WI ![]()
Received 23 December 2022
Accepted for publication 10 March 2023
Published 21 March 2023 Volume 2023:17 Pages 769—780
DOI https://doi.org/10.2147/PPA.S401650
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
I Hsien Li, Wen Ling Hsieh, Wen I Liu
School of Nursing, National Taipei University of Nursing and Health Sciences, Taipei City, Taiwan
Correspondence: Wen I Liu, School of Nursing, National Taipei University of Nursing and Health Sciences, 365, Ming Te Road, Peitou, Taipei City, 112303, Taiwan, Tel +886-2-28227101 Ext 3184, Fax +886-2-28280219, Email [email protected]
Background: Adherence therapy (AT) is an intervention for improving medication adherence of people with schizophrenia spectrum disorders, but no systematic reviews have yet summarized the effectiveness and minimum treatment duration of AT. We here aimed to systematically examine the effectiveness of AT in improving outcomes versus treatment as usual (TAU) and its minimum effective duration for people diagnosed with schizophrenia spectrum disorders.
Patients and Methods: Eligible randomized controlled trials were identified from four databases (Web of Science, PubMed, CINAHL and Cochrane Library) for the period 1 January 2006 to 1 January 2023. Of 1087 retrieved candidate studies, five studies with a total of 726 participants met the inclusion criteria. The search terms consisted of adherence therapy, compliance therapy, schizophrenia, schizoaffective disorder, schizophrenic disorder, medication adherence, and medication compliance (combined with OR and AND). Two investigators independently selected studies, extracted data, and conducted bias risk assessments. Random-effects models were used to analyze the pooled data.
Results: Meta-analysis of the five selected studies showed that AT had a significantly greater positive effects than TAU on psychiatric symptoms, but no significant effects on adherence behaviors and attitudes.
Conclusion: The AT had limited effects in terms of improving the attitudes and behaviors of people with schizophrenia spectrum disorders with respect to medication adherence, but did improve patients’ psychiatric symptoms. The therapy should be performed by trained staff for maximum benefit, and the recommended duration of the intervention is 12 hours.
Keywords: adherence therapy, medication adherence, psychiatric symptoms, motivational interviewing
Introduction
Schizophrenia spectrum disorders are chronic psychiatric disorders that require medical treatment. After the medication is discontinued, patients may also experience recurrent episodes of the disease. Recurrence rates after the discontinuation of antipsychotic medications have been reported to be as high as 77% to >90%,1,2 largely because of medication nonadherence.3,4 Previous studies have reported that 54.5–80% of patients failed to take their medications regularly,5–7 leading to recurrent episodes of psychiatric symptoms and rehospitalization and a consequent increase in the burdens on healthcare professionals and finances.8,9 Studies have shown, however, that the administration of long-acting injectable antipsychotics can stabilize patients and reduce relapses.10 Making use of community-based care then allows them to return from the hospital to the community. The key factor in this step is that they must adhere to their medications to avoid relapses. However, many challenges have been reported in promoting medication adherence among community-dwelling patients.11 From the recovery perspective, it is best if these individuals take their medication voluntarily after they return to the community. Assisting them in taking their medication consistently and regularly to control their symptoms is thus one of the essential functions of mental health care professionals and a critical direction of current mental health policy.12
In clinical practice, patients are generally taught about diseases and medications and then simply expected to adhere to their medication regime. Past research has, however, demonstrated that while health education increases patient knowledge of their disease and treatment, it does not improve medication adherence.13 The reasons for medication nonadherence are complex and can include the lack of a support system, lack of interpersonal relationships with healthcare professionals, and poor insight, coupled with substance abuse behaviors, negative attitudes toward medications, presence of side effects, and cognitive impairment.9,14,15
Many ways to improve medication adherence have been explored. A recent study suggested that an effective strategy to improve medication adherence in psychiatric patients is to merge behavioral and educational approaches.16 This study mainly focused on intervention in the form of adherence therapy (AT). Adherence therapy, developed by Gray et al in 2006, is a short-term intervention based on cognitive behavioral therapy (CBT) and motivational interviewing (MI) methods.17 It consists of six elements: assessment, medication problem-solving, medication timeline, exploring ambivalence, discussing beliefs and concerns about the medication, and using the medication in the future. The key skills for implementing AT are information exchange between the therapist and the client, identification of the discrepancies between the client’s thoughts about the drug and their actual adherence, discussion of the client’s resistance to the drug and treatment, and joint decision-making between the therapist and the client about the appropriate treatment method.17 When a treatment plan is jointly made by the client and the therapist, the client is more likely to adhere to the medication.
Adherence therapy emphasizes the use of MI techniques to encourage people to take their medications. A previous study found that therapeutic alliance, insight, and medical social support were the most important factors affecting the medication adherence of community-dwelling patients with schizophrenia spectrum disorders.18 However, the individual’s motivation for medication use is a mediator of medication adherence—that is, when therapeutic alliance, insight, and medical social support cannot be established within a short time, increasing the person’s motivation can effectively improve their medication adherence, thereby preventing disease recurrence.18 A systematic review of the literature showed that AT was able to improve the psychiatric symptoms of people with severe mental illness,19,20 but it did not significantly improve adherence attitudes and behaviors in those with schizophrenia spectrum disorders.20 The trials on which these findings are based, however, did not have sufficient power to detect the effects or whether there was a ceiling effect. Currently, there are no firm conclusions regarding the optimal duration of AT interventions, who should administer them, or the frequency of AT required to effectively facilitate medication adherence by patients. However, further studies have recently discussed the effects of AT in schizophrenia spectrum disorders. The contribution of this review, therefore, is to cover these new articles by performing an updated systematic literature review and meta-analysis to help incorporate any new findings into the body of knowledge.
We conducted a systematic review and meta-analysis of literature published from 2006 to 2023 to reanalyze the effect of AT interventions on psychiatric symptoms, adherence attitudes, and adherence behaviors in people with schizophrenia spectrum disorders. We also evaluated the effect of AT duration and implementation details to provide a reference for clinical professionals. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) structure.
Patients and Methods
We searched the published literature for studies written in English and related to AT-based interventions aiming to improve medication adherence in patients with schizophrenia spectrum disorders. We searched four electronic databases: Web of Science, PubMed, the Cumulative Index to Nursing and Allied Health (CINAHL), and the Cochrane Library. We also examined the bibliographies of the studies we selected. We conducted the search based on the PICO model: (1) Participants: people with schizophrenia spectrum disorders, including schizophrenia and schizoaffective disorders, as defined in the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5); (2) Intervention: AT-based interventions were included; (3) Comparison: the control group should not have received any AT-based intervention but instead may have received the usual treatment, health education, or no intervention at all; and (4) Outcomes: The primary outcome was the relief of psychiatric symptoms, and the secondary outcome was the patients’ attitudes and behaviors toward medication adherence. The keywords we used in this search were [“adherence therapy” OR “compliance therapy”] AND [“schizophrenia” OR “schizoaffective disorder” OR “schizophrenic disorder”] AND [“medication adherence” OR “medication compliance”]. We set the timeframe as 1 January 2006 to 1 January 2023, and we used the term “randomized controlled trial” as a filter. The final selections are shown in Figure 1. The study was registered in the PROSPERO database (registration number CRD42022316815).
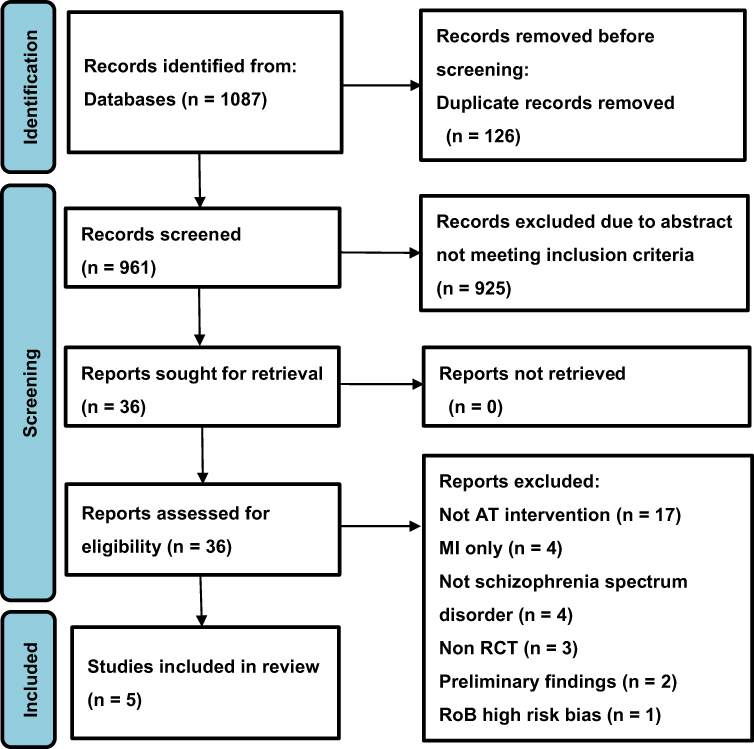 |
Figure 1 Results of the search and screening process. Notes: PRISMA figure adapted from Liberati A, Altman D, Tetzlaff J et al. The PRISMA statement for systematic review and meta-analysis of studies that evaluate health care intervention: explanation and elaboration. Journal of Clinical Epidemiology. 2009; 62(10). Creative Commons.21 |
Inclusion and Exclusion Criteria
The inclusion criteria were that the study had to have been designed as a randomized controlled trial (RCT) involving people aged ≥18 years with schizophrenia spectrum disorders, and it had to have implemented an AT intervention or a combined AT-treatment-as-usual (TAU) intervention. The study results had to include psychiatric symptoms and aspects of medication adherence such as adherence attitudes and behaviors. Studies in which MI was the only intervention or that were considered high risk based on the risk of bias (RoB) tool were excluded.
Selection of Studies
Authors Liu and Li of the present study selected articles that met the inclusion criteria based on their titles and abstracts. When this could not be determined based on title and abstract alone, a full-text search was conducted. When these two authors disagreed about including a study, the third author (Hsieh) was consulted.
Quality Appraisal
The two main authors conducted a quality appraisal using the Risk of Bias 2 tool (RoB 2) in the Cochrane Handbook for Systematic Reviews version 5.1.0.22 The appraisal assessed whether there was any bias in the random assignment process, bias caused by the deviation of the interventions applied to some groups from the originally planned interventions, bias in missing values, bias in outcome measures, or bias in terms of selective reporting of the findings. The appraisal results were categorized into low, medium, or high risk of bias.
Statistical Analysis
We analyzed the continuous data (psychiatric symptoms, adherence attitudes, and adherence behaviors) from the articles we had included in our analysis with random-effects models using Review Manager 5.3 statistical software. We determined the standardized mean differences (SMD) and 95% confidence intervals (95% CI) and categorized effect sizes as small, medium, large, or very large.23 We included the participants’ diagnoses, sample sizes, questionnaires, and measurement time points in our analysis. We conducted a subgroup analysis to test whether the duration (hours) of the AT intervention had any effect on the improvement of psychiatric symptoms. We evaluated study heterogeneity using I2 and presented psychiatric symptoms and adherence attitudes and behaviors in forest plots.
Results
We identified 1087 articles from the four databases, reduced to 961 articles after eliminating duplicates. The title and abstract were then reviewed, eliminating 925 articles, and the remaining 36 articles were selected for a full text assessment. Articles that met the following conditions were excluded: (1) the intervention was not based on AT (n = 17); (2) the intervention involved only MI (n = 4); (3) the participants were not patients with schizophrenia spectrum disorders (n = 4); (4) the study only had a quasi-experimental design (n = 3); (5) the article contained only preliminary findings from a study whose results were later published in full (n = 2); (6) RoB indicated a high risk of bias (n = 1). Once these studies had been excluded, a total of five articles remained. The literature screening process is illustrated as a flowchart (Figure 1).
Study Quality
All five studies were RCTs with clear descriptions showing that the randomized assignment had been conducted by people independent of the research team and that participants had been blinded to treatment allocation.17,24–27 The experimental groups in all five studies received AT interventions, but in three of these AT was the sole intervention and the control group received routine TAU, which may have resulted in a higher risk of performance bias.25–27 Two had a low risk of performance bias because of the nature of the intervention tested.17,24 All of the studies used a rater or assessor blinding process.17,24–27
All five studies used an intention-to-treat analysis approach. Two of them had an attrition rate of 2.5–4.5%.24,27 The rejection rate in the studies ranged from 14% to 40%.17,24–27 Figure 2 summarizes our risk assessments of the five articles, and Figure 3 illustrates our risk assessments in the six areas described above.
 |
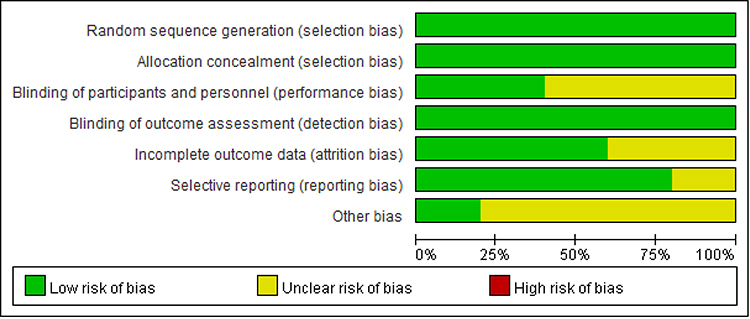 |
Figure 3 Overall risk assessment of the five studies. |
Participants and Study Locations
The five studies were conducted between 2006 and 2019 and involved a total of 726 participants who had been diagnosed with schizophrenia spectrum disorders such as schizophrenia or schizoaffective disorders. The average age of the participants ranged from 28.87 (± 9.54) to 50 (± 9) years old. Three of the studies took place in Asia24,25,27 and the other two were conducted in Europe and the United States.17,26
Characteristics of the Participants
The participants of three of the studies were living in the community at the time of the study.17,24,25 One study involved people who were hospitalized,27 and the fifth one involved people who were hospitalized and then returned to the community during the study period.26 The participants in Chien et al24 consisted of community-dwelling people with a psychiatric symptoms score (PANSS) >60 who were within three years of onset. They had taken oral antipsychotics for at least one month and had been identified by the community psychiatric nurse (CPN) as exhibiting poor medication adherence. In Gray et al,17 the participants had been assessed by a physician as requiring treatment with psychiatric medication. They had also been hospitalized for psychiatric symptoms during the year before the study, had been required to change the type or dosage of the drug they were on, had increased their use of psychiatric services, or had been identified as unstable by the caregiver or medical personnel. Maneesakorn et al25 recruited people who lived in the community. In the study by Schulz et al,26 the participants were hospitalized with severe symptoms, took oral antipsychotics, and had been recommended to receive medication for more than one year after discharge. The participants in von Bormann et al27 were hospitalized because of exacerbated psychiatric symptoms.
Characteristics of Interventions
The experimental groups in all five studies received AT as the intervention, while the control groups received TAU.17,24–27 The control group in one of the studies received health education in addition to TAU.17 Table 1 shows the content of the routine treatment in each study. The core content of the AT interventions in all five studies included assessing the patient’s thoughts about the treatment, current problems with drug use (side-effect management), solving the patients’ medication problems (side effects or forgetting to take medications), medication timeline, assisting the patients in reviewing their history of past illnesses and drug treatment experiences, exploring their ambivalence about taking medications (perceived benefits and risks of taking or not taking medication), evaluating their opinions concerning medication use (whether there is need to take medication if symptoms are relieved, whether taking medication is considered unnatural), discussing concerns about medication use and educating them on the importance of taking medication regularly to achieve their life goals (wanting to work, wanting to get married when symptoms stabilize).17,24–27 The AT interventions in all five studies were implemented to improve psychiatric symptoms and adherence attitudes,17,24–27 and in three of the studies they were also used to improve adherence behaviors.17,24,26
 |
Table 1 Summary of the Five Selected Studies |
Individual Measures and Outcomes
In four of the studies, trained nursing professionals such as community psychiatric nurses, nurse therapists, and mental health nurses administered the AT.24–27 One study included psychologists and psychiatrists in addition to nursing staff.17
One study used the Brief Psychiatric Rating Scale (BPRS)17 and the remaining four used the Positive and Negative Syndrome Scale (PANSS) to measure effectiveness.24–27 Medical staff assigned the scores. The higher the score in either scale, the more severe were the psychiatric symptoms. In terms of the scales for determining adherence attitudes, Chien et al used the Insight and Treatment Attitudes Questionnaire (ITAQ),24 and Gray et al used the Schedule for the Assessment of Insight – Compliance (SAI-C).17 The other three studies used the Drug Attitude Inventory (DAI-30).25–27 To determine adherence behaviors, Chien et al used the Adherence Rating Scale (ARS),24 Gray et al used the Medication Adherence Questionnaire (MAQ),17 and Schulz et al used the Medication Adherence Rating Scale (MARS).25 The scores of all the above scales are continuous, with higher scores indicating better attitudes or behaviors towards medication adherence.
The results of three of the studies showed improvement in psychiatric symptoms,24–26 while those of the other two did not.17,27 Two of the studies revealed improvements in the participants’ adherence attitudes,24,25 but the other three studies did not show significant improvements.17,26,27 In addition, one study found significant improvement in adherence behaviors,24 whereas two of the others did not find any significant improvement.17,26 The remaining two studies did not investigate this aspect (Table 1).
In the study by Schulz et al,26 the participants already had a good attitude toward taking medication and were willing to receive treatment (thus the intervention had no significant effect on adherence behaviors), but the AT group did exhibit significant improvements in psychiatric symptoms relative to the TAU group. Two of the other studies found that the effect of AT and health education on medication adherence was not significant,17,27 but suggested that this may have been attributable to an insufficient amount of time having been devoted to the intervention. Brief descriptions are shown in Table 1.
Pooled Treatment Effect of at versus TAU on Psychiatric Symptoms
The random-effects model of the participants’ psychiatric symptoms (Figure 4) found that the SMD for AT was −0.69 (95% CI: −1.33 to −0.05) compared to the control group. The Z score for total effect size of the intervention was 2.12 (p = 0.03). There was substantial heterogeneity in the data (I2 = 92%). This indicates that AT can effectively reduce psychiatric symptoms compared to TAU.
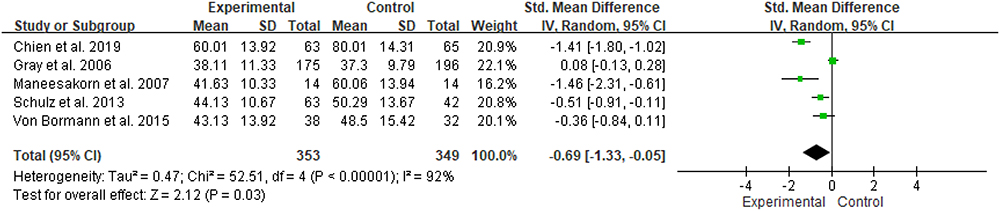 |
Figure 4 The effects of AT and TAU on psychiatric symptoms.17,24–27 |
Pooled Treatment Effect of at versus TAU on Adherence Attitudes
The random-effects model of the participants’ adherence attitudes (Figure 5) found that, compared to the control group, the SMD for the intervention was 0.25 (95% CI: −0.00 to 0.51). The Z score for the total effect size was 1.95 (p = 0.05). There was substantial heterogeneity in the data (I2 = 55%). These results suggest that receiving an AT intervention would not improve patients’ attitudes towards medication adherence.
 |
Figure 5 The effects of AT and TAU on medication adherence attitudes.17,24–27 |
Pooled Treatment Effect of at versus TAU on Adherence Behaviors
The random-effects model of the participants’ adherence behaviors (Figure 6) found that, in comparison with the control group, the SMD for AT in terms of improving adherence behaviors was 0.36 (95% CI: −0.41 to 1.13) and the Z score of the total effective size was 0.92 (p = 0.36). The heterogeneity of the data was high (I2 = 94%). This suggested that receiving an AT intervention would not improve patients’ behaviors in terms of medication adherence.
 |
Figure 6 The effects of AT and TAU on medication adherence behaviors.17,24,26 |
Subgroup Analysis
Because of the high heterogeneity of the data, we conducted a subgroup analysis to examine the effect of the total duration of the AT intervention on the participants’ medication adherence behaviors (Figure 7). One of the studies had a total of 12 h of intervention,24 and two of the others had minimum durations of 2 h 40 min and maximum durations of 7 h 36 min.17,26 We therefore used 12 h as the cut-off point. The SMD for the study with = 12 h of intervention was 1.19 (95% CI: 0.81–1.56) and the Z score of the total effect size was 6.18 (p < 0.00001). The SMD for the studies with <12 h of intervention was −0.08 (95% CI: −0.26 to 0.10) and the Z score of the total effective size was 0.91 (p = 0.36).
 |
Figure 7 Subgroup analysis by intervention duration.17,24,26 |
Discussion
In this study, we compared the effects of AT and TAU in terms of improving psychiatric symptoms, medication adherence attitudes, and medication adherence behaviors of people with schizophrenia spectrum disorders in a systematic review and meta-analysis. We also examined the effect of AT duration and implementation details on the effectiveness of the intervention. We found that while the effects of AT were limited in terms of improving medication adherence attitudes and behaviors relative to routine care, it did improve psychiatric symptoms. These findings are similar to those of previous studies.20,28
In terms of the effectiveness of the AT intervention in improving psychiatric symptoms, the Z score for the total effect size of the intervention was 2.12, which indicates a medium-to-large effect.23 The high degree of heterogeneity in the data appears to be due to inter-study differences in the scales used to determine the participants’ adherence attitudes and behaviors. Some were patient self-report scales while others were observational scales. The timing of scales application also differed. These factors led to a high degree of heterogeneity when the data were pooled across clinical practices. Many different scales are available for measuring medication adherence and the psychiatric symptoms of patients with schizophrenia spectrum disorders. Because medication adherence is a complex issue, its measurement could be affected by the patient’s education level and symptoms if only self-report scales are used. If drug concentrations are measured directly using the patient’s blood and urine samples, this both incurs a higher cost of testing and may lead patients to experience anxiety even to the point that they need to take medications prior to testing.29 It is thus difficult to identify one approach that can truly reflect a patient’s medication adherence. Although the results of this study showed that AT was able to improve the psychiatric symptoms of a group of participants, we suggest that, in addition to measurement scales, objective observations should be included in future studies for the thorough evaluation of medication adherence. The results of one of the studies24 compared with the others suggested that clinical benefit (effect size) increased with length and number of AT sessions and magnitude of intervention doses at each session. However, this study did not indicate what minimum dose is required for AT to be effective.24 The participants in this Hong Kong study received the intervention once every two weeks, two hours per session, for a total of six sessions, so each participant had 12 hours of intervention.24 Our analysis suggests that 12 hours of intervention was more effective than shorter durations for improving medication adherence behaviors in people with schizophrenia spectrum disorders.
We also compared the details of the AT implementation given in three of the studies. The intervention in the Hong Kong study was administered by trained community psychiatric nurses.24 The phenomenon of deinstitutionalization has brought people with psychiatric disorders back into the community; these patients who return to the community must begin looking for work, returning to school, and reconnecting and interacting with others. As part of this process, they must also live with their mental illness and learn to deal with their stress and control their emotions. AT interventions in the five articles included in this study were implemented mostly by nursing professionals.17,24–27 Previous studies have shown that community psychiatric nurses play a crucial role in managing people who receive involuntary treatments.30 Some patients may still have some disease symptoms, so they may lack self-confidence and experience social isolation or even stigmatization,31 which may hinder their recovery and increase their difficulty in staying in the community. In Chien et al, community psychiatric nurses established relationships with their patients with a nonjudgmental attitude,24 to allow the patients to engage in the three processes involved in MI: focusing, evoking, and planning.32 The use of motivational communication skills can help the patient to find reasons to make positive changes without the necessity for persuasion. When a patient resists the change process, the nurse-led AT approach can provide a comprehensive understanding of why they are not adhering to their medication, based on the nurses’ familiarity with the patient and the patient’s trust in the therapeutic interpersonal relationship. A good therapeutic alliance helps people to adhere to medications, as shown by one qualitative study.33 In terms of further exploration of the mechanism by which AT can relieve psychiatric symptoms, AT intervention core skills discussed in these articles include expressing empathy, exploring patients’ strengths and barriers to adherence, developing discrepancies between client’s beliefs and evidence, use of timeline techniques to help patients think about their life experience with non-adherence (eg, stopping medication can lead to worsened psychiatric symptoms, perhaps even hospitalization), and exploring patients’ ambivalence about taking medication.17,24–27 When patients develop medication adherence, their psychiatric symptoms can be relieved. In one of the other studies, the AT intervention was conducted by nursing staff, with each participant receiving an average of only 7.24 sessions (standard deviation [SD] = 1.09; range: 5–9) of therapy, which had an average duration of 42 min (SD = 12.96; range: 17–92).26 Thus, both the number of sessions was smaller and their duration was shorter. In Gray et al, the project team included nursing staff, psychologists, and psychiatrists, and it was not clear whether the nursing staff conducted the AT intervention independently or in conjunction with other healthcare professionals.17
Because the participants in the Chien et al study24 were living with their families in the community, the implementation of the AT targeted not only them, but also their family members. While the goal of targeting the patients was to improve their motivation to take medication, that of targeting their family members was to understand their thoughts and feelings concerning the patient’s medication. The AT intervention strengthened family members’ support for the patient taking the medication and also used CBT homework assignments to record the patient’s behaviors, reasoning, and circumstances with respect to taking or not taking their medication every week. Once people with schizophrenia spectrum disorders return to the community after being discharged from the hospital, they live with their families. Therefore, their medication adherence behaviors are profoundly affected by both their own views and those of their family. Some patients do not take their medicine after returning home because they experience stigma or a lack of support from their family.9 The support of surrounding family members and friends can help patients to achieve medication adherence.15,34 Chien et al included the main caregivers in the patients’ families in their study,24 and concluded that understanding the feelings and views of a patient’s family members’ concerning their medication can help to improve their medication adherence while living in the community.
In addition, the Chien et al study24 excluded people who were given long-acting injectable antipsychotics. Based on their inclusion criteria, the participants of that study had not suffered from the symptoms of their disease for a long time and their cognitive function was still healthy, which could be a determining factor contributing to the effectiveness of the intervention. Previous research has found that a high proportion of people with substance abuse issues are unable to adhere to medications.35 Thus, studies excluding people with such issues may be subject to selection bias.
In terms of pharmacological strategies, long-acting injectable antipsychotics can indeed help some patients,10 but a portion of community-dwelling psychiatric patients primarily take oral medicine. At present, technological interventions such as reminders, support messages, social support engagement, data feedback, and psychoeducation are used as top-down strategies to remind patients with mental illness to take their medicine, in order to achieve medication adherence.36 From the recovery perspective, it is preferable that patients’ intrinsic motivation can be triggered to reduce their nonadherence.
A limitation of this study is that in the articles17,24,26 included, participants had more positive medication attitudes; therefore, they exhibited better medication adherence, this may explain AT has a ceiling effect on their medication attitudes and behaviors. In addition, those who were involved with substances and those in need of assistance due to non-adherence were not recruited.25,27 A systematic literature review showed that other nonpharmacological approaches that emphasize educational and behavioral strategies and include one-on-one interventions targeting the patient‘s diagnosis, symptoms, and medicines can promote medication adherence in people with psychiatric conditions.16 In addition to CBT, AT incorporates MI techniques and behavioral strategies. These intervention strategies enable patients with schizophrenia in relatively stable communities to achieve medication adherence before crises occur. This approach thus achieves the goal of maintaining community mental health, abides by community mental health principles, and empowers patients. Based on our findings, AT can significantly improve psychiatric symptoms compared to TAU. We therefore suggest that clinical professionals use AT as an adjunct intervention.
Implications for Mental Health Nurses
The results of this study show that AT could effectively improve the psychiatric symptoms of people with schizophrenia spectrum disorders. We recommend that AT be conducted by the assigned staff to help establish a therapeutic relationship with the patient. The recommended AT duration is 12 hours. It is also desirable to include the patient’s caregivers or co-residents in the intervention to maximize its effect in promoting medication adherence.
Conclusion
We found that while the effects of AT were limited in terms of improving the attitudes and behaviors of people with schizophrenia spectrum disorders toward medication adherence, the intervention did improve their psychiatric symptoms. In clinical practice, assigning trained staff to competently administer AT can foster a therapeutic relationship and deliver unique, personalized care. The recommended duration of the intervention is 12 hours. Considering a patient’s specific situation can help to increase their motivation to change and make AT a more effective approach.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kishi T, Ikuta T, Matsui Y, et al. Effect of discontinuation v. maintenance of antipsychotic medication on relapse rates in patients with remitted/stable first-episode psychosis: a meta-analysis. Psychol Med. 2019;49(5):772–779. doi:10.1017/S0033291718001393
2. Zipursky RB, Menezes NM, Streiner DL. Risk of symptom recurrence with medication discontinuation in first-episode psychosis: a systematic review. Schizophr Res. 2014;152(2–3):408–414. doi:10.1016/j.schres.2013.08.001
3. Lauriello J. Prevalence and impact of relapse in patients with schizophrenia. J Clin Psychiatry. 2020;81(2):2. doi:10.4088/JCP.MS19053BR1C
4. Tham XC, Xie H, Chng CM, Seah XY, Lopez V, Klainin-Yobas P. Factors affecting medication adherence among adults with schizophrenia: a literature review. Arch Psychiatr Nurs. 2016;30(6):797–809. doi:10.1016/j.apnu.2016.07.007
5. Abdel-Baki A, Ouellet-Plamondon C, Malla A. Pharmacotherapy challenges in patients with first-episode psychosis. J Affect Disord. 2012;138(Suppl):S3–14. doi:10.1016/j.jad.2012.02.029
6. Haddad PM, Brain C, Scott J. Nonadherence with antipsychotic medication in schizophrenia: challenges and management strategies. Patient Relat Outcome Meas. 2014;5:43–62. doi:10.2147/PROM.S42735
7. Häge A, Weymann L, Bliznak L, Märker V, Mechler K, Dittmann RW. Non-adherence to psychotropic medication among adolescents - A systematic review of the literature. Z Kinder Jugendpsychiatr Psychother. 2018;46(1):69–78. doi:10.1024/1422-4917/a000505
8. Novick D, Haro JM, Suarez D, Perez V, Dittmann RW, Haddad PM. Predictors and clinical consequences of non-adherence with antipsychotic medication in the outpatient treatment of schizophrenia. Psychiatry Res. 2010;176(2–3):109–113. doi:10.1016/j.psychres.2009.05.004
9. Semahegn A, Torpey K, Manu A, Assefa N, Tesfaye G, Ankomah A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: a systematic review and meta-analysis. Syst Rev. 2020;9(1):17. doi:10.1186/s13643-020-1274-3
10. Bartoli F, Cavaleri D, Callovini T, et al. Comparing 1-year effectiveness and acceptability of once-monthly paliperidone palmitate and aripiprazole monohydrate for schizophrenia spectrum disorders: findings from the STAR network depot study. Psychiatry Res. 2022;309:114405. doi:10.1016/j.psychres.2022.114405
11. Chan SW, Li Z, Klainin-Yobas P, Ting S, Chan MF, Eu PF. Effectiveness of a peer-led self-management programme for people with schizophrenia: protocol for a randomized controlled trial. J Adv Nurs. 2014;70(6):1425–1435. doi:10.1111/jan.12306
12. Olivares JM, Sermon J, Hemels M, Schreiner A. Definitions and drivers of relapse in patients with schizophrenia: a systematic literature review. Ann Gen Psychiatry. 2013;12(1):32. doi:10.1186/1744-859X-12-32
13. Gray R, Wykes T, Gournay K. From compliance to concordance: a review of the literature on interventions to enhance compliance with antipsychotic medication. J Psychiatr Ment Health Nurs. 2002;9(3):277–284. doi:10.1046/j.1365-2850.2002.00474.x
14. Velligan DI, Sajatovic M, Hatch A, Kramata P, Docherty JP. Why do psychiatric patients stop antipsychotic medication? A systematic review of reasons for nonadherence to medication in patients with serious mental illness. Patient Prefer Adherence. 2017;11:449–468. doi:10.2147/PPA.S124658
15. Wade M, Tai S, Awenat Y, Haddock G. A systematic review of service-user reasons for adherence and nonadherence to neuroleptic medication in psychosis. Clin Psychol Rev. 2017;51:75–95. doi:10.1016/j.cpr.2016.10.009
16. Loots E, Goossens E, Vanwesemael T, Morrens M, Van Rompaey B, Dilles T. Interventions to improve medication adherence in patients with schizophrenia or bipolar disorders: a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18:19. doi:10.3390/ijerph181910213
17. Gray R, Leese M, Bindman J, et al. Adherence therapy for people with schizophrenia. European multicentre randomised controlled trial. Br J Psychiatry. 2006;189:508–514. doi:10.1192/bjp.bp.105.019489
18. Hsieh WL, Lee SK, Chien WT, Liu WI, Lai CY, Liu CY. Mediating effect of the motivation for medication use on disease management and medication adherence among community-dwelling patients with schizophrenia. Patient Prefer Adherence. 2019;13:1877–1887. doi:10.2147/PPA.S218553
19. Wong-Anuchit C, Chantamit OPC, Schneider JK, Mills AC. Motivational interviewing-based compliance/adherence therapy interventions to improve psychiatric symptoms of people with severe mental illness: meta-analysis. J Am Psychiatr Nurses Assoc. 2019;25(2):122–133. doi:10.1177/1078390318761790
20. Gray R, Bressington D, Ivanecka A, et al. Is adherence therapy an effective adjunct treatment for patients with schizophrenia spectrum disorders? A systematic review and meta-analysis. BMC Psychiatry. 2016;16:90. doi:10.1186/s12888-016-0801-1
21. Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for systematic review and meta-analysis of studies that evaluate health care intervention: explanation and elaboration. J Clin Epidemiol. 2009;62:10. doi:10.1016/j.jclinepi.2009.06.006
22. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
23. Rosenthal JA. Qualitative descriptors of strength of association and effect size. J Soc Serv Res. 1996;21(4):37–59. doi:10.1300/J079v21n04_02
24. Chien WT, Cheung EFC, Mui JHC, Gray R, Ip G. Adherence therapy for schizophrenia: a randomised controlled trial. Hong Kong Med J. 2019;2(1):4–9.
25. Maneesakorn S, Robson D, Gournay K, Gray R. An RCT of adherence therapy for people with schizophrenia in Chiang Mai, Thailand. J Clin Nurs. 2007;16(7):1302–1312. doi:10.1111/j.1365-2702.2007.01786.x
26. Schulz M, Gray R, Spiekermann A, Abderhalden C, Behrens J, Driessen M. Adherence therapy following an acute episode of schizophrenia: a multi-centre randomised controlled trial. Schizophr Res. 2013;146(1–3):59–63. doi:10.1016/j.schres.2013.01.028
27. von Bormann S, Robson D, Gray R. Adherence therapy following acute exacerbation of schizophrenia: a randomised controlled trial in Thailand. Int J Soc Psychiatry. 2015;61(1):3–9. doi:10.1177/0020764014529099
28. Zomahoun HTV, Guénette L, Grégoire JP, et al. Effectiveness of motivational interviewing interventions on medication adherence in adults with chronic diseases: a systematic review and meta-analysis. Int J Epidemiol. 2017;46(2):589–602. doi:10.1093/ije/dyw273
29. Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int. 2015;2015:1–12. doi:10.1155/2015/217047
30. Heslop B, Wynaden D, Tohotoa J, Heslop K. Mental health nurses’ contributions to community mental health care: an Australian study. Int J Ment Health Nurs. 2016;25(5):426–433. doi:10.1111/inm.12225
31. Alyahya NM, Munro I, Moss C. The experience of psychosis and recovery from consumers’ perspectives: an integrative literature review. J Psychiatr Ment Health Nurs. 2022;29(1):99–115. doi:10.1111/jpm.12696
32. Miller WR, Rose GS. Toward a theory of motivational interviewing. Am Psychol. 2009;64(6):527–537. doi:10.1037/a0016830
33. Clifford L, Crabb S, Turnbull D, Hahn L, Galletly C. A qualitative study of medication adherence amongst people with schizophrenia. Arch Psychiatr Nurs. 2020;34(4):194–199. doi:10.1016/j.apnu.2020.06.002
34. Salzmann-Erikson M, Sjödin M. A narrative meta-synthesis of how people with schizophrenia experience facilitators and barriers in using antipsychotic medication: implications for healthcare professionals. Int J Nurs Stud. 2018;85:7–18. doi:10.1016/j.ijnurstu.2018.05.003
35. Leclerc E, Noto C, Bressan RA, Brietzke E. Determinants of adherence to treatment in first-episode psychosis: a comprehensive review. Rev Bras Psiquiatr. 2015;37(2):168–176. doi:10.1590/1516-4446-2014-1539
36. Steinkamp JM, Goldblatt N, Borodovsky JT, et al. Technological interventions for medication adherence in adult mental health and substance use disorders: a systematic review. JMIR Mental Health. 2019;6(3):e12493. doi:10.2196/12493
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Telephone-Based Brief Motivational Interviewing on Self-Management, Medication Adherence, and Glycemic Control in Patients with Uncontrolled Type 2 Diabetes Mellitus in a Rural Community in Thailand
Sawaengsri N, Maneesriwongul W, Schorr EN, Wangpitipanit S
Patient Preference and Adherence 2023, 17:2085-2096
Published Date: 24 August 2023