Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 11
A Swedish register-based, long-term inception cohort study of patients with rheumatoid arthritis – results of clinical relevance
Authors Hafström I, Ajeganova S, Andersson MLE ![]() , Bala SV, Bergman S
, Bala SV, Bergman S ![]() , Bremander A
, Bremander A ![]() , Forslind K
, Forslind K ![]() , Malm K, Svensson B
, Malm K, Svensson B ![]()
Received 5 June 2019
Accepted for publication 13 August 2019
Published 9 September 2019 Volume 2019:11 Pages 207—217
DOI https://doi.org/10.2147/OARRR.S218448
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Ingiäld Hafström1, Sofia Ajeganova2,3, Maria LE Andersson4,5, Sidona-Valentina Bala6,7, Stefan Bergman5,8, Ann Bremander4,5,9, Kristina Forslind4,10, Karina Malm5,11, Björn Svensson4
1Division of Gastroenterology and Rheumatology, Department of Medicine Huddinge, Karolinska Institutet, and Rheumatology Unit, Karolinska University Hospital, Stockholm, Sweden; 2Division of Gastroenterology and Rheumatology, Department of Medicine Huddinge, Karolinska Institutet, Stockholm, Sweden; 3Rheumatology Division, Universitair Ziekenhuis Brussel, Vrije Universiteit Brussel, Brussels, Belgium; 4Faculty of Medicine, Department of Clinical Sciences, Rheumatology, Lund University, Lund, Sweden; 5Spenshult Research and Development Center, Halmstad, Sweden; 6Faculty of Medicine, Department of Health Sciences, Lund University, Lund, Sweden; 7Department of Medicine, Section of Rheumatology, Helsingborg’s Hospital, Helsingborg, Sweden; 8Primary Health Care Unit, Department of Public Health and Community Medicine, Institute of Medicine, the Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; 9Department of Regional Health Research, University of Southern Denmark, Odense, Denmark; 10Department of Research and Education, Skånevård Sund, Region Skåne, Helsingborg´s Hospital, Helsingborg, Sweden; 11Rheumatology, Capio Movement, Halmstad, Sweden
Correspondence: Ingiäld Hafström
Rheumatology Unit, R92, Karolinska University Hospital, 141 86 Stockholm, Sweden
Tel +46 73 699 6235
Email [email protected]
Purpose: At the end of the twentieth century, the outcome of rheumatoid arthritis (RA) was shown to be unsatisfactory and new therapeutic strategies were introduced. This initiated a register-based long-term study of early RA, the Better Anti-Rheumatic PharmacOTherapy (BARFOT) study. The aims were to evaluate the disease course and to acquire knowledge for improved care.
Patients and methods: BARFOT is a multicentre observational study of patients with early RA, consecutively included 1992–2006. The patients are followed in daily practice according to a structured protocol for 15 years and data recorded in a web-based register. Also, through linkage of the BARFOT register to national registers we have acquired information on comorbidity and mortality.
Results: In all, 2857 patients have been included and over 80 scientific articles have been published. Phenotypic characteristics at disease onset, i.e. gender, smoking habits and autoantibody profiles have been addressed. The disease course over 15 years was described. Early predictors for persistent disease activity, impaired function, joint damage and co-morbidities have been identified. Treatment strategies have been studied. A randomized sub-study gave strong support for the treatment of recent RA with low-dose prednisolone in combination with disease-modifying anti-rheumatic drug. Furthermore, the impact of lifestyle factors, such as smoking, alcohol consumption, body weight and physical activity has been addressed.
Conclusion: A register-based study like BARFOT has provided a basis for optimal long-term management of patients with RA. In addition, the register has made it possible to perform a diversity of studies of RA addressing various issues of major relevance to the patients.
Keywords: patient reported outcomes, PRO, disease progression, prognostic factors, lifestyle, observational study, registry
Introduction
Toward the end of the twentieth century, it became increasingly realized that rheumatoid arthritis (RA) was a disease with a high incidence of disability and increased mortality, which brought about major efforts to improve treatment. Treatment strategies turned from “go low and slow” to “early and active” with the aim that this would improve the disease course and outcome. This assumption was supported by clinical trials, but nothing was known about long-term efficacy. Therefore, to respond to this important unmet need, we initiated a longitudinal observational study including all available incident RA patients to assess treatment and outcome for several years.
In 1992, these considerations resulted in Better Anti-Rheumatic PharmacOTherapy (BARFOT), a long-term observational cohort study of patients with RA engaging six rheumatology centers in southern Sweden. All data were assembled in a register, which was the first in Sweden to enable regular documentation of different aspects of RA and became the prototype for the national Swedish Rheumatology Quality Register (initially named RAMONA- RA monitoring and assessment), which started in 1995.
Unlike other RA registers, the BARFOT register focused on providing information of clinical importance for the patient. Thus, the BARFOT study pays attention to most facets of the disease, besides measures of disease activity and damage also physical function, pain and quality of life.
Through the start of the BARFOT register, it became possible for the participating rheumatologists to follow the disease course in detail in daily practice and thus make well-founded interventions. The structured data collection admitted studying several aspects of disease outcome and predictors. Also, through linkage of the BARFOT register to different national registers we have been able to add information about comorbidity and mortality. Here, some of the results will be reviewed, particularly those with relevance for clinical practice.
Patients and methods
Patients
The patients were consecutively enrolled in the BARFOT multicentre study during 1992–2006. Inclusion criteria were disease duration of 12 months or less, fulfilling the ACR 1987 classification criteria.1 All patients gave their written informed consent to the study, which was performed in accordance with the Helsinki Declaration. The following ethics committees approved the study: Lund university LU 154-95 and 398-01; Göteborg university Gbg M 45-95 and Ö 282-01; Linköping university Li 123-95 and 01-263; Karolinska Institutet KI 153-95 and 02-075: Stockholm EPN 2011/381-31/4 and 2016/297-31/1, all in Sweden.
The BARFOT protocol
A structured protocol was developed by the collaborating rheumatology units in close co-operation with international experts working with newly proposed outcome measures. The patients were assessed at inclusion and at predefined follow-up visits up to 15 years. Besides the fixed times there was an option for closer registrations if required. All units collected the data in a common database. Treatment decisions were made by the responsible rheumatologist except in limited randomized substudies.
At inclusion, patient characteristics such as age, gender, education, social status, smoking habits (current, previous or never smokers), menopausal age, comorbidity and medication and disease duration were registered.
Information of the regular clinical monitoring and radiographic assessments are given in Table 1.
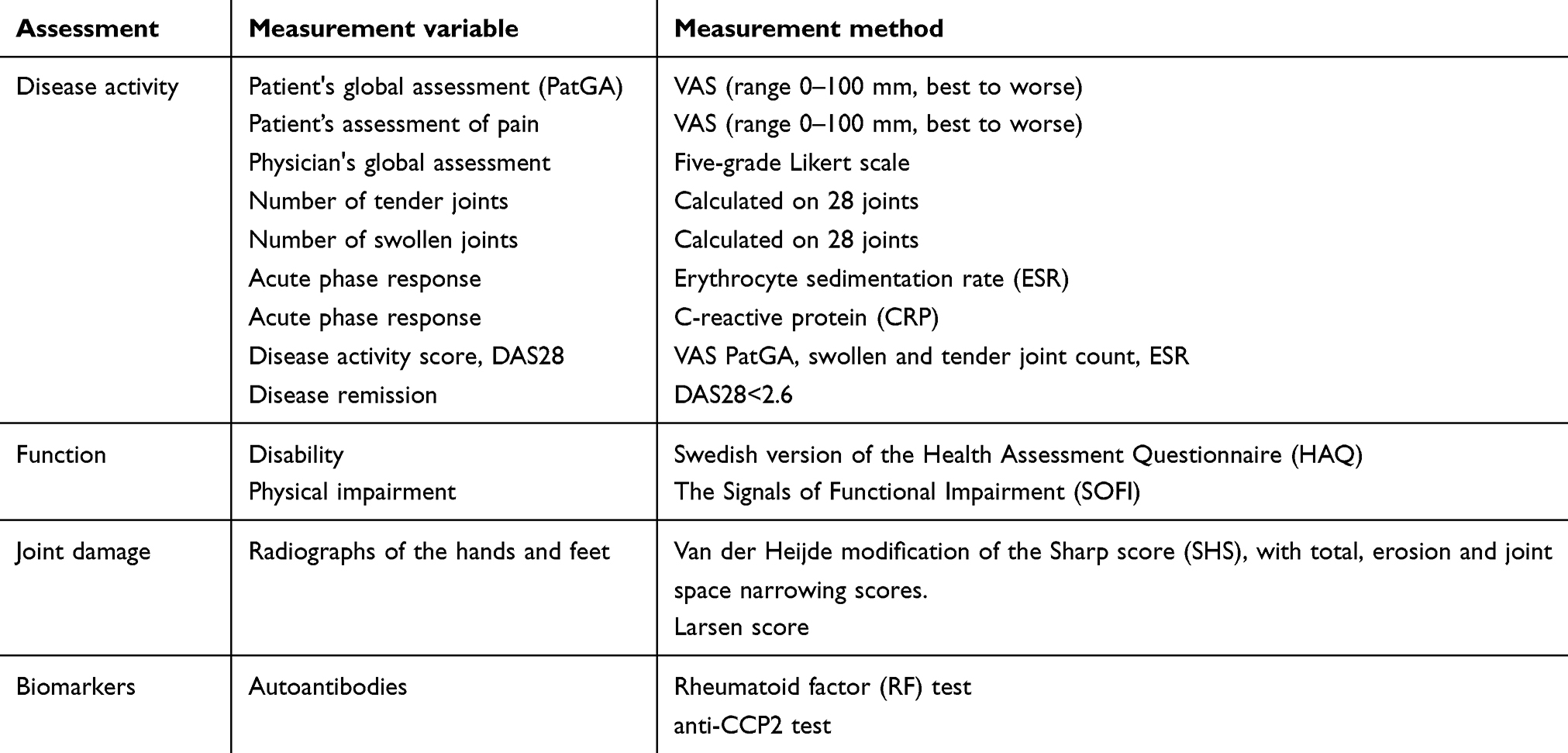 |
Table 1 Clinical, laboratory and radiographic assessments according to the BARFOT protocol |
Biomarkers
At all predefined visits, serum samples were biobanked until analyzed. Among later analyses are anti-cyclic citrullinated peptide (anti-CCP2) antibodies (Euro-Diagnostica, Malmö, Sweden) and anti-carbamylated protein antibodies (anti-CarP) (in-house ELISA, Leiden).
Data enrichment by questionnaires
In 2010 and 2017, questionnaires were sent to all patients remaining in the study (2102 and 1542, respectively), with questions concerning lifestyle factors, such as smoking, alcohol habits, diet and physical activity, as well as pain, health-related quality of life and comorbidity.
Data enrichment by register linkage
To secure information about comorbidities and mortality, linkage of the BARFOT register to national health registers, such as the National Patient Register, including data on hospital discharges, and Cause of Death Register, has been performed. Comparisons with the general population have been made through linkage with the national demographic registers in Sweden.
Major results
Disease onset
From 1992 to 2006, a total of 2837 patients were included. Patient and disease characteristics at baseline are shown in Table 2.
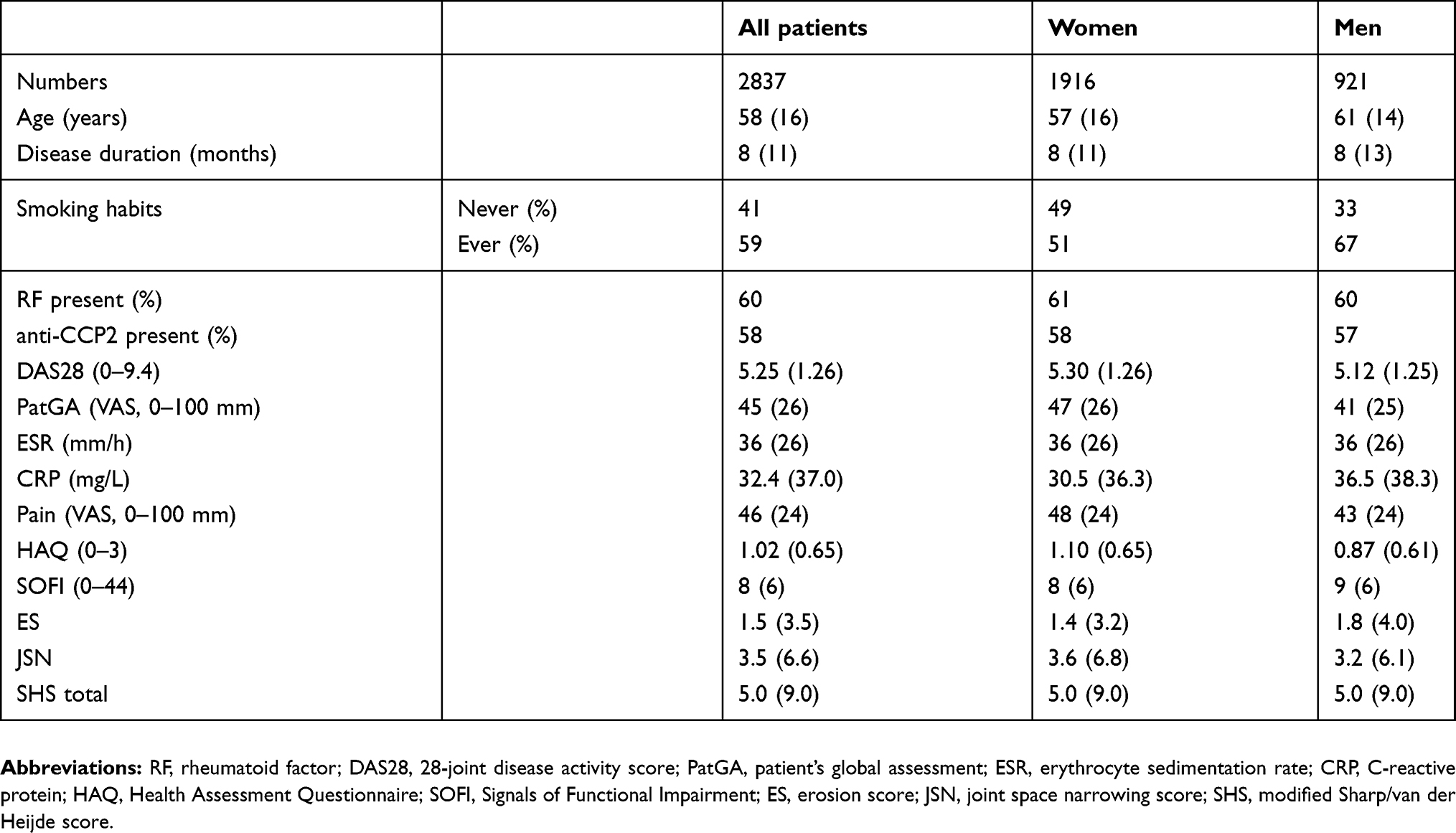 |
Table 2 Characteristics of the patients at inclusion divided by gender |
Role of autoantibodies
The BARFOT studies have investigated the role of autoantibodies for the clinical profile of the disease. Thus, the most recent study revealed that the proportion of patients with a positive test for rheumatoid factor (RF), anti-CCP2 and anti-CarP was lower in patients with a higher age at disease onset.2 An increasing number of these autoantibodies at onset was associated with younger age, current smoking and higher erythrocyte sedimentation rate (ESR).3
Moreover, ACPA (CCP2) was found to be associated with osteopenia in the femoral neck and/or Ward´s triangle at disease onset, independently of inflammation.4
The presentation of RA has changed
To examine if the presentation of RA had changed over the years, we compared patients with a disease onset 1992–1999 with those included 2000–2006. Patients included in the 2000s were older, had a shorter mean disease duration at inclusion, were more often RF positive, had higher disease activity score (DAS28), disability measured by Health Assessment Questionnaire (HAQ), pain measured by VAS pain and patient’s global assessment (PatGA) as well as a higher total van der Heijde modification of the Sharp score, the latter mainly dependent on a higher joint space narrowing score.5 The proportion of smokers were higher in 1996, 29%, than in 2004, 20%.6
At inclusion, the patients addressed their beliefs about the cause of their RA. Thirty percent of the patients reported some possible causal event, most frequently infection, linked to a seasonal trend in the onset of RA.7 The role of infections as possible triggers was also suggested by a two-cohort study, which showed that onset of RA in the Swedish patients was more frequent in winter than in other seasons, in contrast to the Dutch cohort.8
Living with RA
Remission
The goal for treatment in RA is remission. Since several sets of criteria for remission have been proposed, we tried to find the most appropriate criterion for long-term studies. To that end, we studied the frequency of achieved remission defined by three commonly used sets of criteria in 700 patients included in BARFOT during the 1990s and followed for 8 years.9 Remission was determined by DAS28 remission criterion (DAS28 Cr), the Simplified Disease Activity Index criterion (SDAI Cr)10 and the Boolean-based ACR/EULAR remission criteria (Boolean Cr).11 Remission at all follow-up visits, i.e. sustained remission, was infrequent, most common by the DAS28 Cr, 14%, followed by the SDAI Cr, 5%, and the Boolean Cr, 3%. Progression of radiographic joint damage was least pronounced in patients with sustained remission, independently of criterion used. Sustained remission was also associated with improved function, irrespective of criteria.9
Persistently active disease
Patients who did not achieve DAS28 Cr remission at any visit up to 8 years were defined as having persistently active disease which afflicted as many as 37% (43% women vs. 25% men).12 These patients had significantly worse PatGA, pain, HAQ and radiological damage compared to the non-persistent group.
Living with persistent disease
An interview study focused on the life situation of ten patients with persistent disease. Living with persistent RA was revealed as an existence dominated by painful symptoms, radical changes and limitations in life, a continual struggle to cope with life and to master the illness, and a dependency on those who are close by and the world around.13 This qualitative study nicely conforms with the quantitative data described above and is a further argument for great attention and improved care for this group of patients with a severe disease course.
Pain
Pain in patients with RA is the most common and troublesome complaint, which causes functional impairment and reduced quality of life. The 2010 postal questionnaire addressed among other things also pain. As many as 34% of the responders reported chronic wide-spread pain, more often women, a pain related to DAS28 and HAQ, and less distinctly to acute phase reactants, i.e., ESR and C-reactive protein.14
In another study, unacceptable pain, i.e. pain VAS 40 mm or more, was present in 34% of the patients after 15 years. Of these, 33% were in remission suggesting that many patients had pain not directly related to inflammation.15
Physical function and disability
In most patients, physical function assessed by HAQ improves during treatment with disease-modifying anti-rheumatic drugs (DMARDs). However, after 8 years, the patients with persistently active disease had significantly higher frequency of disability (HAQ≥1.0) than the rest of the patients (52% vs. 18%).12 Furthermore, we have recently shown that improvement in physical function does not always follow a reduction in disease activity, suggesting that impaired physical function may also depend on other factors.16 The Signals of Functional Impairment performance test measuring hand, shoulder/arm and lower extremity function was shown to be a valuable complement to self-reported function.17
Comorbidities
RA is associated with an enhanced risk of cardiovascular disease (CVD) and mortality. Whether prompt control of the inflammatory process after disease onset could improve CVD and mortality outcome was studied in patients recruited 1993–1999 and followed until 2010. Incident CVD morbidity and mortality data were obtained through register linkage. In summary, we found that a better control of inflammation during the critical first 2 years of disease resulted in cardiovascular and survival benefits. Predictive factors for morbidity and mortality differed by age at disease onset, suggesting a need for age stratification in the evaluation of CVD and mortality risks in early RA.18
Disease course in patients with disease onset in the 1990s and in the 2000s
In 1999, biologic DMARDs were introduced in Sweden, which inspired us to compare the disease course in patients included before and after this change in treatment options. Over 5 as well as 8 years, the DAS28 decreased significantly more in patients included in the 2000s compared with those included in the 1990s. Of interest, there was no significant difference in improvement in pain or HAQ between the groups, despite the treatment differences.5,16
Gender differences
In several of the BARFOT studies, women were found to suffer a more severe disease course than men. In the cohort included in the 1990s, women had compared with men, higher DAS28 and HAQ, both at inclusion and after 2 years.19 After 2 years, 28% of the women and 40% of the men were in DAS28 remission.19 After 5 years, the remission rates were 31% for women and 52% for men.20 Of the women, only 10% achieved sustained remission over 8 years compared to 23% of the men.9
Even though women had higher DAS28, HAQ and VAS pain at all visits up to 5 and 8 years compared to men, the radiological scores did not differ between genders at any timepoint.21,22
Also, when comparing the patients included in the 1990s with those included in the 2000s the gender differences were significant. At the 5-year follow-up, the remission rate had increased in the group included in the 2000s (women 42% vs. men 64%).5
Prediction of disease outcome
The disease course and outcome of RA may vary from spontaneous remission to a persistently active disabling disease. Since treatment options today are manifold with varying toxicity, the key issue in early management of RA is adequate prediction of the long-term outcome.
To address this, we performed a series of studies to find early predictors of later radiological damage. Thus, antifilaggrin (which equals anti-CCP1),23,24 serum cartilage oligomeric matrix protein ,25 survivin (a proto-oncogene),26 and hand bone loss by digital X-ray radiogrammetry ,27 independently predicted radiological progression after a disease course of 2 and 5 years. We could confirm that anti-CCP2 is a most reliable laboratory predictor of radiological damage.28 The combination of anti-CCP2 with anti-CarP autoantibodies proved to have additional predictive potency.29 However, in our nested randomized study, RF and anti-CCP2 did not predict progressive joint damage in patients treated with prednisolone in combination with DMARDs.30
However, it is at least equally important to find predictors of the clinical course of RA. In a study over 8 years we found that as many as 37% of the patients suffered a persistently active disease which was independently predicted at onset by female gender, current smoking and disease activity and absence of remission at 6 months.12 In a collaboration work involving three European RA cohorts, we found that the presence of RF at disease onset was associated with an increased overall mortality, especially deaths related to neoplasm and respiratory disease, while anti-CCP2 was associated with an increase in cardiovascular deaths.31
Lifestyle factors and disease outcome
Lifestyle factors like smoking, alcohol consumption, body weight and physical activity influence not only cardiovascular health but may also have impact on the disease course and outcome of RA.
Smoking
To assess the effects of smoking on disease outcome, 1787 patients, of which 23% of the women and 24% of the men were current smokers, were studied over the first year of the disease. Smoking status was not associated with disease activity at inclusion, but after 1 year smokers had higher disease activity assessed by DAS28 and lower remission rate compared with previous smokers and non-smokers, despite more DMARD treatment during the first 3 months.6 In the year 2010, the change in smoking habits and its influence on disease activity was assessed by a postal survey. The proportion of smokers had decreased to 17% 6–14 years after diagnosis. However, smoking cessation after the onset of RA did not influence disease activity.32
Current smoking was, in a nested control study over the first 2 years of the disease, found to be associated with subsequent development of severe extra-articular RA, most frequently interstitial lung disease and pleuritis. In addition, current smoking was associated with high disease activity, disability and positive RF.33
The influence of smoking on joint damage was addressed in a six-cohort multinational study. In this study, smokers had more severe joint damage on radiographs of hands and feet 1, 2 and 5 years after diagnosis compared to non-smokers. However, this effect was lost when adjusting for anti-CCP2 positivity. This indicates that the effect of smoking on joint damage could be mediated via the effect of ACPA.34
In a follow-up study, with data on three autoantibodies, RF, anti-CCP2 and anti-CarP, smoking was associated with concurrent presence of two or three autoantibodies rather than anti-CCP2 alone. This implies that smoking is a risk factor for breaking tolerance to multiple autoantigens in RA.35
Given the negative effects of smoking on RA described above, we further studied if second-hand exposure to tobacco smoke affected disease activity in patients who had never smoked. No association was found between second-hand exposure and disease activity.36
Alcohol consumption
In 2010, 1238 BARFOT patients answered the questionnaire about alcohol consumption. Of all, 67% were non-hazardous drinkers and 21% were classified as hazardous drinkers.37 Alcohol consumption in women, but not in men, was associated with lower self-reported disease activity and better health-related quality of life than non-drinkers. Current smoking emerged as an independent negative prognostic factor for reported disease activity, which might have counteracted the immunosuppressive effect of alcohol.37
The role of alcohol consumption in RA is complex. On the one hand, alcohol may lower the risk for getting RA,38 and reduce inflammation in established RA,39 on the other hand, alcohol may enhance hepatotoxicity of DMARDs. Discussions regarding alcohol consumption are thus important to make patients aware of its interactions with medication.
What about changes in alcohol habits after diagnosis in our patients? Based on the questionnaire of 2010 it was found that 6% of the patients had stopped drinking. By qualitative content analyses, we found that patients who stopped drinking were older, had lower health-related quality of life, more pain and fatigue and worse physical function compared with those who continued drinking.40 The reasons for stopping drinking alcohol varied but was most often illness. Another reason was a desire to improve health and well-being and, less frequently, the patients referred to work and solidarity with family members.40
Body weight
In 1596 patients from the BARFOT cohort, 13% of the patients were obese at disease onset (body mass index [BMI] ≥30 kg/m2) and 16% in the survey 9 years later.41 Obesity was independently associated with higher disease activity, worse HAQ score, more pain and worse PatGA both at disease onset and at the time of the survey. Also, obesity was independently associated with important comorbidities, such as hypertension, diabetes mellitus and chronic pulmonary disease.41
Interestingly, if the cutoff for obesity was set to ≥28 kg/m2,42 the associations to disease severity gave similar results.41 This implies that unfavorable body composition could be more accurately detected by redefining BMI cutoffs in RA. Further, a higher waist circumference was also associated with a worse disease outcome and could be used in the RA population besides BMI to aid in the prediction of the disease prognosis.41
Physical activity
According to the 2010 questionnaire, 65% of the BARFOT patients met the WHO recommendations for health-enhancing physical activity, women to a larger extent than men,43 virtually the same as in a non-rheumatoid population in Sweden. Meeting recommended levels of physical activity could not be predicted by function or pain at disease onset, which makes it important to recommend a healthy lifestyle along the course of the disease.
It is important and recommended to make patients aware of the influence of lifestyle on RA. Based on the 2017 questionnaire it was found that, according to the patients’ recall, smoking had been discussed with 25% of the patients, alcohol consumption with 17%, diet with 23% and physical activity with 49%. Although these figures are higher than previously reported, there is a need for further improvement to comply with the EULAR recommendations of patient-centered standards of care.
Treatment with low-dose prednisolone
An important but controversial topic in the treatment of early RA is use of prednisolone, which gave rise to our randomized prednisolone study.44 A total of 250 patients were randomized to 7.5 mg prednisolone daily or no prednisolone for 2 years at the start of their first DMARD. We found that the prednisolone-group had lower joint damage progression and higher remission rate than the non-prednisolone group and the frequency of adverse effects was small. A follow-up study demonstrated that remission after 2 years with prednisolone was associated with reduced joint destruction also after 4 years.45 In a further study, we concluded that the inhibition of progression of joint destruction by prednisolone might depend on decreased activity of matrix metalloproteinases as well as impaired osteoclast activation.46
Prednisolone in this low dose had no or minor effects on bone density.47 Measurement of bone-markers revealed that the suppressive effect on bone synthesis exerted by prednisolone was counteracted by the ability of prednisolone to hamper the inflammatory mediated increase in bone resorption.48
Concerning cardiovascular risks, treatment with low-dose prednisolone did not influence the thickness or endothelial function of the carotid intima after 5 years.49 After 10 years, the incidence of ischaemic coronary artery events was similar in the two treatment groups, whereas the long-term risk for incident cerebrovascular events was somewhat higher in the prednisolone group.50
Discussion
The primary goal of the BARFOT study was to create a basis for improved treatment of patients with RA. The information acquired by the register served as guidance to clinical practice, primarily with regard to tailored anti-inflammatory treatment. In addition, the structured protocol allowed further studies, which have contributed to increase the knowledge of this complex disease.
RA has been recognized as a separate disease entity but is indeed a multi-faceted disease, in which the identification of novel RA-related autoantibodies has made it possible to distinguish subphenotypes.51 The present studies, including the recent multi-national cohort studies, suggest that the magnitude of immune response at disease onset influences the clinical presentation of the disease and may have implications for diagnosis and prognosis of RA at different ages.2,3 The data also support the hypothesis of a pathophysiological role of ACPA in systemic bone loss.4
Although infections with periodontal pathogens and Epstein-Barr virus have been shown to induce autoimmunity and ACPA-production,52 the prevalence and possible pathogenetic role of common viral infections in the pathogenesis of RA has not yet been established. Many patients believe that an infection might be a possible causal event, linked to onset of RA in the winter season.7 However, this could not be verified in our dual cohort study, in which joint destruction over time did not differ between patients with disease onset in winter or summer.8
A key focus of the BARFOT studies has been to increase knowledge about the disease course from the patient’s perspective. We have shown that despite improved treatment options, a high proportion of patients suffer from a persistently active disease, pain, disability and impaired health over many years after disease onset. Pain emerged as the major complaint, frequently unacceptable, and not always linked to active disease but also present in remission, stressing the need of improved pain assessment and treatment.
There is agreement concerning the importance of achieving remission, but various remission definitions exist.53 The DAS28 remission criterion, used in BARFOT, identified more patients in sustained remission than did the other applied criteria with no difference in degree of joint damage and disability.9 This suggests that this criterion may cause fewer misclassifications and may therefore be used in long-term cohort studies until more accurate criteria are available.
Despite modern treatment strategies, many of the BARFOT patients had a persistently active disease.12 Importantly, several recent studies similarly report a substantial proportion of patients with persistent disease activity in spite of currently available effective treatment options.54 This emphasizes the importance of very early and persistent management and care of the patients.
The BARFOT studies stress the fact that pain in RA is a major distress causing impaired function and is associated with increased risk of poor outcome,14,15 and it also contributes to the global burden of the disease.55 In addition to inflammation, pain may also be due to other causes. These observations imply that the origin of pain in patients with RA should be identified and adequate treatment given, which has been emphasized in the recent EULAR recommendations for pain management.56
Like pain, function did not improve in all patients following a satisfactory reduction in disease activity.16 This is in line with other reports, reviewed in Norton et al.57 It is thus vital to be aware of the fact that functional impairment as well as pain may have causes other than inflammation and therefore may remain also following successful control of the inflammation.
The higher risk of CVD seen in patients with RA is not fully explained be traditional CVD risk factors,58 moreover also inflammation plays a role. Thus, inflammatory cytokines in RA stimulate plaques formation and rupture in CVD.59 The role of inflammation for CVD is supported in our studies in which prompt control of inflammation during the critical first 2 years of disease resulted in cardiovascular and survival benefits providing a rationale for our treatment approach to prevent CV in patients with RA.18
Our data suggest that RA is more serious in women than in men.12 However, Sokka et al reasoned that this gender difference is valid only for patients with more limited disease activity reflecting “considerable differences in the measures between genders”.60 In accordance with that report, the observation of a significant overrepresentation of women among patients with long-standing active disease indicates true worse outcome as to components included in the disease activity measures but not radiologic destruction.21,22
Lifestyle factors like smoking influenced disease severity and development of extra-articular disease, while obesity was associated with high disease activity and comorbidities.
Among lifestyle factors, cigarette smoking is established to increase severity and comorbidity in RA. In addition, during the last years obesity and low physical activity have also been found to affect the disease negatively.61–65 All these factors are potentially intervenable, and consequently smoking cessation, weight control and physical activity have been included in the EULAR recommendation for management of early arthritis.66
Reliable predictors of the disease course and outcome are of paramount importance for treatment precision. We have detected predictors for persistently active disease, joint damage and comorbidities. Some of these have been performed as joint studies with other groups, while in others linkage was done with national health registers.
Through the year’s rheumatologists have tried to identify predictors of the future course of early RA. On a group level, we and others have found baseline variables predicting clinical as well as radiological outcome. However, to our knowledge, no single predictor or prediction model has been proven to identify the disease course in an individual patient. Accordingly, a recent literature review found that “No predictors were identified reliably predicting clinical response to methotrexate after 3–6 months in the individual patient: clinical predictors were weak”.67 Furthermore, despite much research, a significant number of patients in the present era of biologic DMARDs yet develop refractory disease.68 Consequently, there is still an urgent need for improved early prediction of disease outcomes. We will now focus on the immune response to joint specific proteins by identification of unique peptides which can be recognized by antibodies by a specific pathogenic or regulatory function.
The clinical message from the randomized studies of treatment with low-dose prednisolone in combination with synthetic DMARDs was that low-dose prednisolone may be recommended for at least 2 years to patients with recent onset RA. This recommendation is in line with that of the 2019 update of the Swedish Society for Rheumatology RA treatment guidelines. Furthermore, a recent “Systematic Review of International Guidelines and Consensus Statements” reports that most current recommendations of glucocorticoid use in RA are similar to those proposed by our group.69
To conclude, long-term observational studies on RA like BARFOT may serve the dual purpose of providing a basis for optimal long-term management of the patient and of creating a platform for a diversity of studies of the disease which otherwise would have been difficult or impossible to achieve.
Acknowledgments
We thank all the members of the BARFOT study group. The study was funded by grants from the Swedish Rheumatism Association and the Foundation for Assistance to Disabled People in Skåne, Sweden.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Arnett FC, Edworthy SM, Bloch DA, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31(3):315–324. doi:10.102/art.1780310302
2. Boeters DM, Mangnus L, Ajeganova S, et al. The prevalence of ACPA is lower in rheumatoid arthritis patients with an older age of onset but the composition of the ACPA response appears identical. Arthritis Res Ther. 2017;19(1):115. doi:10.1186/s13075-017-1324-y
3. Derksen VF, Ajeganova S, Trouw LA, et al. Rheumatoid arthritis phenotype at presentation differs depending on the number of autoantibodies present. Ann Rheum Dis. 2017;76(4):716–720. doi:10.1136/annrheumdis-2016-209794
4. Hafstrom I, Ajeganova S, Forslind K, Svensson B. Anti-citrullinated protein antibodies are associated with osteopenia but not with pain at diagnosis of rheumatoid arthritis: data from the BARFOT cohort. Arthritis Res Ther. 2019;21(1):45. doi:10.1186/s13075-019-1833-y
5. Andersson ML, Forslind K, Hafstrom I. Comparing five year out-come in two cohorts of patients with early rheumatoid arthritis - A BARFOT Study. Open Rheumatol J. 2015;9:8–15. doi:10.2174/1874312901409010008
6. Soderlin MK, Petersson IF, Bergman S, Svensson B, Group BS. Smoking at onset of rheumatoid arthritis (RA) and its effect on disease activity and functional status: experiences from BARFOT, a long-term observational study on early RA. Scand J Rheumatol. 2011;40(4):249–255. doi:10.3109/03009742.2010.541495
7. Soderlin MK, Bergsten U, Svensson B, Group BS. Patient-reported events preceding the onset of rheumatoid arthritis: possible clues to aetiology. Musculoskeletal Care. 2011;9(1):25–31. doi:10.1002/msc.193
8. de Rooy DP, Andersson ML, Knevel R, Huizinga TW, Svensson B, van der Helm-van Mil AH. Does the season at symptom onset influence the long-term severity of radiographic joint destruction in rheumatoid arthritis? Ann Rheum Dis. 2012;71(12):2055–2056. doi:10.1136/annrheumdis-2012-201565
9. Svensson B, Andersson ML, Bala SV, Forslind K, Hafstrom I, Group BS. Long-term sustained remission in a cohort study of patients with rheumatoid arthritis: choice of remission criteria. BMJ Open. 2013;3(9):e003554. doi:10.1136/bmjopen-2013-003554
10. Smolen JS, Breedveld FC, Schiff MH, et al. A simplified disease activity index for rheumatoid arthritis for use in clinical practice. Rheumatology (Oxford). 2003;42(2):244–257. doi:10.1093/rheumatology/keg072
11. Felson DT, Smolen JS, Wells G, et al. American College of Rheumatology/European League against Rheumatism provisional definition of remission in rheumatoid arthritis for clinical trials. Ann Rheum Dis. 2011;70(3):404–413. doi:10.1136/ard.2011.149765
12. Svensson B, Andersson M, Forslind K, Ajeganova S, Hafstrom I. Group BS. Persistently active disease is common in patients with rheumatoid arthritis, particularly in women: a long-term inception cohort study. Scand J Rheumatol. 2016;45(6):448–455. doi:10.3109/03009742.2016.1147595
13. Bala SV, Samuelson K, Hagell P, et al. Living with persistent rheumatoid arthritis: a BARFOT study. J Clin Nurs. 2017;26(17–18):2646–2656. doi:10.1111/jocn.13691
14. Andersson ML, Svensson B, Bergman S. Chronic widespread pain in patients with rheumatoid arthritis and the relation between pain and disease activity measures over the first 5 years. J Rheumatol. 2013;40(12):1977–1985. doi:10.3899/jrheum.130493
15. Andersson MLE, Forslind K, Svensson B. Prevalence of unacceptable pain in patients with long-standing RA. Ann Rheum Dis. 2017;76(Suppl 2):812–813.
16. Andersson MLE, Forslind K, Hafstrom I, Group BS. Patients with early rheumatoid arthritis in the 2000s have equal disability and pain despite less disease activity compared with the 1990s: data from the BARFOT study over 8 years. J Rheumatol. 2017;44(6):723–731. doi:10.3899/jrheum.161235
17. Bremander A, Forslind K, Eberhardt K, Andersson MLE. Importance of measuring hand and foot function over the disease course in rheumatoid arthritis: an eight-year follow-up study. Arthritis Care Res (Hoboken). 2019;71(2):166–172.
18. Ajeganova S, Andersson ML, Frostegard J, Hafstrom I. Disease factors in early rheumatoid arthritis are associated with differential risks for cardiovascular events and mortality depending on age at onset: a 10-year observational cohort study. J Rheumatol. 2013;40(12):1958–1966. doi:10.3899/jrheum.130365
19. Tengstrand B, Ahlmen M, Hafstrom I. The influence of sex on rheumatoid arthritis: a prospective study of onset and outcome after 2 years. J Rheumatol. 2004;31(2):214–222.
20. Forslind K, Hafstrom I, Ahlmen M, Svensson B, Group BS. Sex: a major predictor of remission in early rheumatoid arthritis? Ann Rheum Dis. 2007;66(1):46–52. doi:10.1136/ard.2006.056937
21. Ahlmen M, Svensson B, Albertsson K, Forslind K, Hafstrom I, Group BS. Influence of gender on assessments of disease activity and function in early rheumatoid arthritis in relation to radiographic joint damage. Ann Rheum Dis. 2010;69(1):230–233. doi:10.1136/ard.2008.102244
22. Hafstrom I, Bala V, Albertsson K, Forslind K, Svensson B, Group BS. Joint destruction in early rheumatoid arthritis over 8 years is similar in women and men despite apparently higher disease activity and poorer function in women. Ann Rheum Dis. 2011;70(4):709–710. doi:10.1136/ard.2010.135343
23. Forslind K, Vincent C, Serre G, Svensson B. Antifilaggrin autoantibodies in early rheumatoid arthritis. Scand J Rheumatol. 2000;29(5):320–322.
24. Forslind K, Vincent C, Serre G, Svensson B. Antifilaggrin antibodies in early rheumatoid arthritis may predict radiological progression. Scand J Rheumatol. 2001;30(4):221–224.
25. Andersson ML, Svensson B, Petersson IF, et al. Early increase in serum-COMP is associated with joint damage progression over the first five years in patients with rheumatoid arthritis. BMC Musculoskelet Disord. 2013;14:229. doi:10.1186/1471-2474-14-229
26. Svensson B, Hafstrom I, Forslind K, Albertsson K, Tarkowski A, Bokarewa M. Increased expression of proto-oncogene survivin predicts joint destruction and persistent disease activity in early rheumatoid arthritis. Ann Med. 2010;42(1):45–54. doi:10.3109/07853890903376280
27. Forslind K, Kalvesten J, Hafstrom I, Svensson B, Group BS. Does digital X-ray radiogrammetry have a role in identifying patients at increased risk for joint destruction in early rheumatoid arthritis? Arthritis Res Ther. 2012;14(5):R219. doi:10.1186/ar4058
28. Forslind K, Ahlmen M, Eberhardt K, Hafstrom I, Svensson B, Group BS. Prediction of radiological outcome in early rheumatoid arthritis in clinical practice: role of antibodies to citrullinated peptides (anti-CCP). Ann Rheum Dis. 2004;63(9):1090–1095. doi:10.1136/ard.2003.014233
29. Ajeganova S, van Steenbergen HW, Verheul MK, et al. The association between anti-carbamylated protein (anti-CarP) antibodies and radiographic progression in early rheumatoid arthritis: a study exploring replication and the added value to ACPA and rheumatoid factor. Ann Rheum Dis. 2017;76(1):112–118. doi:10.1136/annrheumdis-2015-208870
30. Hafstrom I, Engvall IL, Ronnelid J, Boonen A, van der Heijde D, Svensson B. Rheumatoid factor and anti-CCP do not predict progressive joint damage in patients with early rheumatoid arthritis treated with prednisolone: a randomised study. BMJ Open. 2014;4(7):e005246. doi:10.1136/bmjopen-2014-005246
31. Ajeganova S, Humphreys JH, Verheul MK, et al. Anticitrullinated protein antibodies and rheumatoid factor are associated with increased mortality but with different causes of death in patients with rheumatoid arthritis: a longitudinal study in three European cohorts. Ann Rheum Dis. 2016;75(11):1924–1932. doi:10.1136/annrheumdis-2015-208579
32. Andersson ML, Bergman S, Soderlin MK. The effect of stopping smoking on disease activity in Rheumatoid Arthritis (RA). Data from BARFOT, a Multicenter Study of Early RA. Open Rheumatol J. 2012;6:303–309. doi:10.2174/1874312901206010303
33. Nyhall-Wahlin BM, Petersson IF, Nilsson JA, Jacobsson LT, Turesson C. Group BS. High disease activity disability burden and smoking predict severe extra-articular manifestations in early rheumatoid arthritis. Rheumatology (Oxford). 2009;48(4):416–420. doi:10.1093/rheumatology/kep004
34. de Rooy DP, van Nies JA, Kapetanovic MC, et al. Smoking as a risk factor for the radiological severity of rheumatoid arthritis: a study on six cohorts. Ann Rheum Dis. 2014;73(7):1384–1387. doi:10.1136/annrheumdis-2013-203940
35. van Wesemael TJ, Ajeganova S, Humphreys J, et al. Smoking is associated with the concurrent presence of multiple autoantibodies in rheumatoid arthritis rather than with anti-citrullinated protein antibodies per se: a multicenter cohort study. Arthritis Res Ther. 2016;18(1):285. doi:10.1186/s13075-016-1177-9
36. Soderlin MK, Andersson M, Bergman S, Group BS. Second-hand exposure to tobacco smoke and its effect on disease activity in Swedish rheumatoid arthritis patients. Data from BARFOT, a multicenter study of RA. Clin Exp Rheumatol. 2013;31(1):122–124.
37. Bergman S, Symeonidou S, Andersson ML, Soderlin MK, Group BS. Alcohol consumption is associated with lower self-reported disease activity and better health-related quality of life in female rheumatoid arthritis patients in Sweden: data from BARFOT, a multicenter study on early RA. BMC Musculoskelet Disord. 2013;14:218. doi:10.1186/1471-2474-14-218
38. Kallberg H, Jacobsen S, Bengtsson C, et al. Alcohol consumption is associated with decreased risk of rheumatoid arthritis: results from two Scandinavian case-control studies. Ann Rheum Dis. 2009;68(2):222–227. doi:10.1136/ard.2007.086314
39. Maxwell JR, Gowers IR, Moore DJ, Wilson AG. Alcohol consumption is inversely associated with risk and severity of rheumatoid arthritis. Rheumatology (Oxford). 2010;49(11):2140–2146. doi:10.1093/rheumatology/keq202
40. Larsson I, Andersson MLE, Group BS. Reasons to stop drinking alcohol among patients with rheumatoid arthritis in Sweden: a mixed-methods study. BMJ Open. 2018;8(12):e024367. doi:10.1136/bmjopen-2018-024367
41. Ajeganova S, ML A, Hafstrom I, Group BS. Association of obesity with worse disease severity in rheumatoid arthritis as well as with comorbidities: a long-term followup from disease onset. Arthritis Care Res (Hoboken). 2013;65(1):78–87. doi:10.1002/acr.21710
42. Stavropoulos-Kalinoglou A, Metsios GS, Koutedakis Y, et al. Redefining overweight and obesity in rheumatoid arthritis patients. Ann Rheum Dis. 2007;66(10):1316–1321. doi:10.1136/ard.2006.060319
43. Malm K, Bergman S, Andersson M, Bremander A, Group BS. Predictors of severe self-reported disability in RA in a long-term follow-up study. Disabil Rehabil. 2015;37(8):686–691. doi:10.3109/09638288.2014.939773
44. Svensson B, Boonen A, Albertsson K, van der Heijde D, Keller C, Hafstrom I. Low-dose prednisolone in addition to the initial disease-modifying antirheumatic drug in patients with early active rheumatoid arthritis reduces joint destruction and increases the remission rate: a two-year randomized trial. Arthritis Rheum. 2005;52(11):3360–3370. doi:10.1002/art.21298
45. Hafstrom I, Albertsson K, Boonen A, van der Heijde D, Landewé R, Svensson B. Remission achieved after 2 years treatment with low-dose prednisolone in addition to disease-modifying anti-rheumatic drugs in early rheumatoid arthritis is associated with reduced joint destruction still present after 4 years: an open 2-year continuation study. Ann Rheum Dis. 2009;68(4):508–513. doi:10.1136/ard.2008.087833
46. Engvall IL, Svensson B, Boonen A, van der Heijde D, Lerner UH, Hafström I. Low-dose prednisolone in early rheumatoid arthritis inhibits collagen type I degradation by matrix metalloproteinases as assessed by serum 1CTP–a possible mechanism for specific inhibition of radiological destruction. Rheumatology (Oxford). 2013;52(4):733–742. doi:10.1093/rheumatology/kes369
47. Engvall IL, Brismar K, Hafstrom I, Tengstrand B. Treatment with low-dose prednisolone is associated with altered body composition but no difference in bone mineral density in rheumatoid arthritis patients: a controlled cross-sectional study. Scand J Rheumatol. 2011;40(3):161–168. doi:10.3109/03009742.2010.523012
48. Engvall IL, Svensson B, Tengstrand B, Brismar K, Hafstrom I, Better Anti-Rheumatic Farmac OTSG. Impact of low-dose prednisolone on bone synthesis and resorption in early rheumatoid arthritis: experiences from a two-year randomized study. Arthritis Res Ther. 2008;10(6):R128. doi:10.1186/ar2542
49. Hafstrom I, Rohani M, Deneberg S, Wornert M, Jogestrand T, Frostegard J. Effects of low-dose prednisolone on endothelial function, atherosclerosis, and traditional risk factors for atherosclerosis in patients with rheumatoid arthritis–a randomized study. J Rheumatol. 2007;34(9):1810–1816.
50. Ajeganova S, Svensson B, Hafstrom I, Group BS. Low-dose prednisolone treatment of early rheumatoid arthritis and late cardiovascular outcome and survival: 10-year follow-up of a 2-year randomised trial. BMJ Open. 2014;4(4):e004259. doi:10.1136/bmjopen-2013-004259
51. McGonagle D, Watad A, Savic S. Mechanistic immunological based classification of rheumatoid arthritis. Autoimmun Rev. 2018;17(11):1115–1123. doi:10.1016/j.autrev.2018.06.001
52. Sakkas LI, Daoussis D, Liossis SN, Bogdanos DP. The infectious basis of ACPA-positive rheumatoid arthritis. Front Microbiol. 2017;8:1853. doi:10.3389/fmicb.2017.01853
53. Gul HL, Ferreira JF, Emery P. Remission in rheumatoid arthritis: is it all the same? Expert Rev Clin Pharmacol. 2015;8(5):575–586. doi:10.1586/17512433.2015.1061429
54. Buch MH. Defining refractory rheumatoid arthritis. Ann Rheum Dis. 2018;77(7):966–969. doi:10.1136/annrheumdis-2017-212862
55. Minnock P, FitzGerald O, Bresnihan B. Women with established rheumatoid arthritis perceive pain as the predominant impairment of health status. Rheumatology (Oxford). 2003;42(8):995–1000.
56. Geenen R, Overman CL, Christensen R, et al. EULAR recommendations for the health professional’s approach to pain management in inflammatory arthritis and osteoarthritis. Ann Rheum Dis. 2018;77(6):797–807. doi:10.1136/annrheumdis-2017-212662
57. Norton S, Fu B, Scott DL, et al. Health Assessment Questionnaire disability progression in early rheumatoid arthritis: systematic review and analysis of two inception cohorts. Semin Arthritis Rheum. 2014;44(2):131–144. doi:10.1016/j.semarthrit.2014.05.003
58. Solomon DH, Karlson EW, Rimm EB, et al. Cardiovascular morbidity and mortality in women diagnosed with rheumatoid arthritis. Circulation. 2003;107(9):1303–1307. doi:10.1161/01.cir.0000054612.26458.b2
59. Fragoulis GE, Panayotidis I, Nikiphorou E. Cardiovascular risk in rheumatoid arthritis and mechanistic links: from pathophysiology to treatment. Curr Vasc Pharmacol. 2019;17. doi:10.2174/1570161117666190619143842.
60. Sokka T, Toloza S, Cutolo M, et al. Women, men, and rheumatoid arthritis: analyses of disease activity, disease characteristics, and treatments in the QUEST-RA study. Arthritis Res Ther. 2009;11(1):R7. doi:10.1186/ar2684
61. Papadopoulos NG, Alamanos Y, Voulgari PV, Epagelis EK, Tsifetaki N, Drosos AA. Does cigarette smoking influence disease expression, activity and severity in early rheumatoid arthritis patients? Clin Exp Rheumatol. 2005;23(6):861–866.
62. Vittecoq O, Richard L, Banse C, Lequerre T. The impact of smoking on rheumatoid arthritis outcomes. Joint Bone Spine. 2018;85(2):135–138. doi:10.1016/j.jbspin.2017.12.004
63. Levitsky A, Brismar K, Hafstrom I, et al. Obesity is a strong predictor of worse clinical outcomes and treatment responses in early rheumatoid arthritis: results from the SWEFOT trial. RMD Open. 2017;3(2):e000458. doi:10.1136/rmdopen-2016-000391
64. Liu Y, Hazlewood GS, Kaplan GG, Eksteen B, Barnabe C. Impact of obesity on remission and disease activity in rheumatoid arthritis: a systematic review and meta-analysis. Arthritis Care Res (Hoboken). 2017;69(2):157–165. doi:10.1002/acr.22932
65. Sokka T, Hakkinen A. Poor physical fitness and performance as predictors of mortality in normal populations and patients with rheumatic and other diseases. Clin Exp Rheumatol. 2008;26(5 Suppl 51):S14–20.
66. Combe B, Landewe R, Daien CI, et al. 2016 update of the EULAR recommendations for the management of early arthritis. Ann Rheum Dis. 2017;76(6):948–959. doi:10.1136/annrheumdis-2016-210602
67. Roodenrijs NMT, van der Goes MC, Welsing PMJ, et al. Is prediction of clinical response to methotrexate in individual rheumatoid arthritis patients possible? A systematic literature review. Joint Bone Spine. 2019:
68. Becede M, Alasti F, Gessl I, et al. Risk profiling for a refractory course of rheumatoid arthritis. Semin Arthritis Rheum. 2019:
69. Palmowski Y, Buttgereit T, Dejaco C, et al. “Official View” on glucocorticoids in rheumatoid arthritis: a systematic review of international guidelines and consensus statements. Arthritis Care Res (Hoboken). 2017;69(8):1134–1141. doi:10.1002/acr.23185
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.