Back to Journals » Infection and Drug Resistance » Volume 19
A Successfully Treated Case of Mycobacterium chelonae Pulmonary Infection and a Literature Review (1990–2025)
Authors Qi B, Wang C, Wei X, Li Y, Li Y, Yao Y, Wei S, Ning S, Du X, Jin Y, Yang R, Chen X, Ge P, Sun B ![]()
Received 5 November 2025
Accepted for publication 17 February 2026
Published 26 May 2026 Volume 2026:19 579282
DOI https://doi.org/10.2147/IDR.S579282
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Bing Qi,1 Chen Wang,2 Xujing Wei,2 Yuexuan Li,3 Yanan Li,2 Yuanrui Yao,2 Shuxin Wei,4 Siming Ning,1 Xiwei Du,1 Yanan Jin,1 Ruixia Yang,1 Xin Chen,1 Peng Ge,1,* Bao Sun1,*
1Department of Clinical Pharmacy, The Second Affiliated Hospital of Xi’an Medical University, Xi’an, Shaanxi, 710038, People’s Republic of China; 2School of Pharmacy, Xi’an Medical University, Xi’an, Shaanxi, 710021, People’s Republic of China; 3School of Medical Technology, Xi’an Medical University, Xi’an, Shaanxi, 710021, People’s Republic of China; 4School of Clinical Medical, Xi’an Medical University, Xi’an, Shaanxi, 710021, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bao Sun, Email [email protected] Peng Ge, Email [email protected]
Objective: This study aims to evaluate the pharmaceutical interventions conducted by clinical pharmacists in the case of a 59-year-old patient diagnosed with lung adenocarcinoma and a suspected infection, focusing on pathogen identification and the formulation of a safe and effective treatment plan.
Methods: Through clinical consultation, pharmacists conducted an evaluation of the patient’s underlying conditions and clinical manifestations, leading to the suspicion of a high probability of Mycobacterium chelonae infection. Consequently, they recommended a treatment regimen in accordance with guidelines for non-tuberculous mycobacterial infections, consisting of azithromycin 0.5 g and moxifloxacin 0.4 g administered orally once daily, accompanied by dynamic monitoring of therapeutic efficacy.
Results: The patient became afebrile by day 3. At day 14, inflammatory markers had normalised, and no clinically significant adverse drug reactions were observed during short-term follow-up.
Conclusion: In this case, PTseq supported early hypothesis generation and timely antimicrobial stewardship. The azithromycin-moxifloxacin regimen was associated with short-term clinical improvement; however, confirmatory microbiologic evidence, susceptibility guidance, and longer follow-up are needed before drawing generalized conclusions.
Keywords: Mycobacterium chelonae, pulmonary infection, PTseq sequencing, literature analysis
Introduction
Mycobacterium chelonae is a species of non-tuberculous mycobacteria (NTM) predominantly associated with skin and soft tissue infections, whereas pulmonary involvement is exceedingly uncommon. Over the past 35 years, sporadic reports have documented its role as an atypical pulmonary pathogen. With the advancement of molecular diagnostic technologies and heightened clinical awareness, understanding of its microbiological characteristics, diagnostic approaches, and therapeutic strategies has steadily improved.1 A review of 16 English-language case reports retrieved from the PubMed database revealed that the majority of affected patients presented with underlying chronic pulmonary disorders.2 Taxonomically, M. chelonae is classified within the Mycobacterium abscessus–chelonae complex, a subgroup of rapidly growing mycobacteria.3 Disseminated disease is rare and generally confined to severely immunocompromised individuals. Notably, M. chelonae demonstrates substantial in vitro resistance to multiple antimycobacterial agents,4 and conventional chemotherapeutic eradication has often proven unsuccessful. Herein, we present a rare case of pulmonary M. chelonae infection in a patient without pre-existing chronic lung disease, which was successfully managed with an oral combination regimen of azithromycin (0.5 g once daily) and moxifloxacin (0.4 g once daily).
Clinical Data
A 59-year-old Chinese woman presented with a 2-week history of pronounced fatigue and a 1-day history of fever with chills and dizziness. On examination, temperature was 38.3°C and pulse rate 118 beats/min. Laboratory tests showed: white blood cell count 6.38×10^9/L, neutrophils 84.8%, high-sensitivity C-reactive protein 7.46 mg/L, procalcitonin 1.12 μg/L, and interleukin-6234.7 pg/mL. Gram stain and fungal smear were negative; respiratory nucleic acid assays for influenza A/B, rhinovirus, Mycoplasma pneumoniae, adenovirus and respiratory syncytial virus were negative. Blood culture showed no bacterial growth after 5 days, and bronchoalveolar lavage fluid (BALF) culture yielded only normal respiratory flora. A tuberculosis RNA test was reported as positive; however, the overall clinical-radiologic picture and the subsequent clinical course did not support active tuberculosis. We therefore interpreted this result as possibly reflecting non-viable nucleic acid detection or contamination; confirmatory tuberculosis testing was not available for this report and is acknowledged as a limitation.
Three years earlier, a solitary pulmonary nodule in the left lower lobe was discovered during routine screening and remained stable during follow-up. One year prior, chest computed tomography (CT) revealed an irregular ground-glass nodule in the dorsal segment of the left lower lobe, highly suggestive of invasive adenocarcinoma. The patient underwent single-port laparoscopic left lower lobectomy with mediastinal lymph node dissection, with an uneventful postoperative course. Postoperative adjuvant chemotherapy with pemetrexed and carboplatin was completed in four cycles.
Three months before the current presentation, the patient noticed enlargement of right cervical lymph nodes; biopsy confirmed metastatic lung adenocarcinoma. She subsequently received combination chemotherapy with carboplatin, paclitaxel, and toripalimab. One month prior to presentation, follow-up evaluation indicated immune-related pneumonia, necessitating corticosteroid therapy and temporary suspension of immunotherapy. The second cycle of carboplatin plus paclitaxel chemotherapy was then administered. The current symptoms developed 14 days after the last chemotherapy cycle.
The patient’s medical history was notable for hypertension of one year’s duration and type 2 diabetes mellitus for 15 years, both managed with stable pharmacological therapy.
PTseq analysis of BALF identified: Mycobacteroides chelonae (62 sequences), Tropheryma whipplei (6 sequences), and human gammaherpesvirus 4 (EBV) (4461 sequences). Upon consultation, clinical pharmacists-considering the patient’s oncologic status and microbiological findings-suspected a high probability of M. chelonae infection. Following relevant NTM treatment guidelines, they recommended oral azithromycin (0.5 g once daily) plus moxifloxacin (0.4 g once daily). After initiation of therapy, the patient’s body temperature normalised by day 3, and at 14-day follow-up all infection markers had normalised (Table 1).
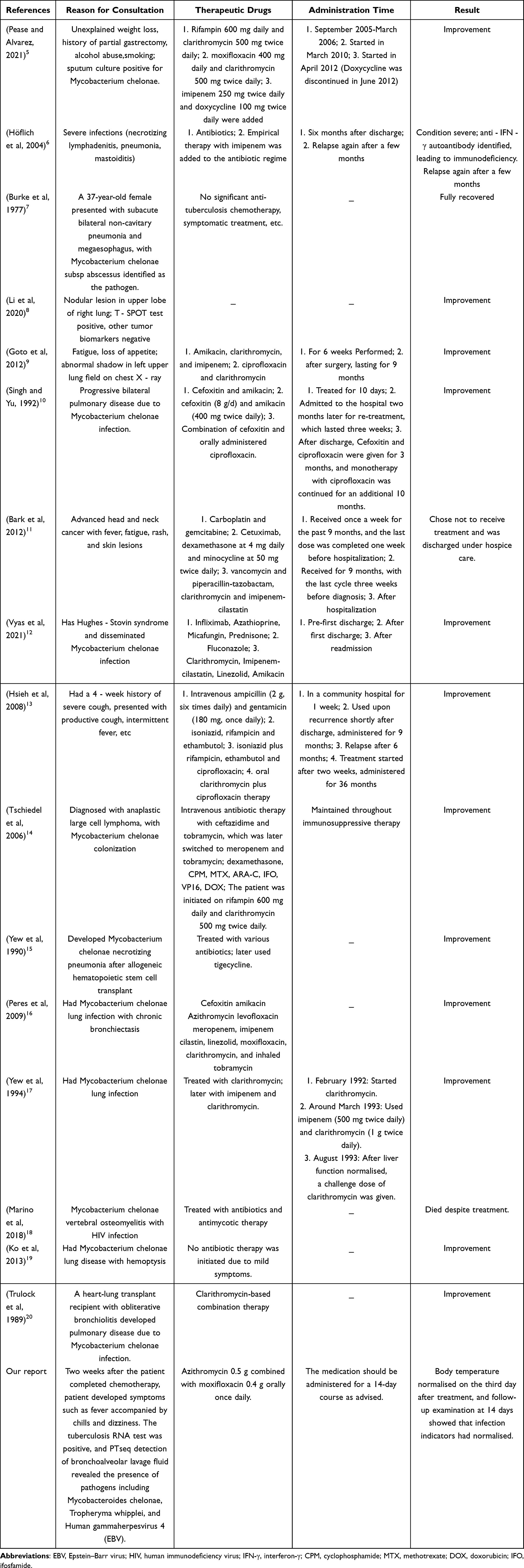 |
Table 1 Conditions for Treatment Recommended by Clinical Pharmacists |
Literature Review
We conducted a comprehensive PubMed search for reports of pulmonary infection caused by Mycobacterium chelonae from January 1, 1990, to December 31, 2025, using combinations of the keywords “Mycobacterium chelonae”, “pulmonary”, “lung”, and “mycobacterium”. Titles/abstracts were screened, followed by full-text assessment. Duplicate records were removed. We included case reports/series that provided patient-level pulmonary involvement with species-level identification of M. chelonae; we excluded non-pulmonary infections, reports with unclear species identification, and studies without sufficient case information. Using these criteria, 16 individual pulmonary cases were identified from 16 published articles.5–20 Including the present case, 17 cases have been reported in the literature within this time window. Due to heterogeneity and incomplete reporting across cases, we summarized patient demographics, clinical presentations, diagnostic approaches, treatment regimens, and outcomes descriptively, without making formal comparative inferences (Table 2).
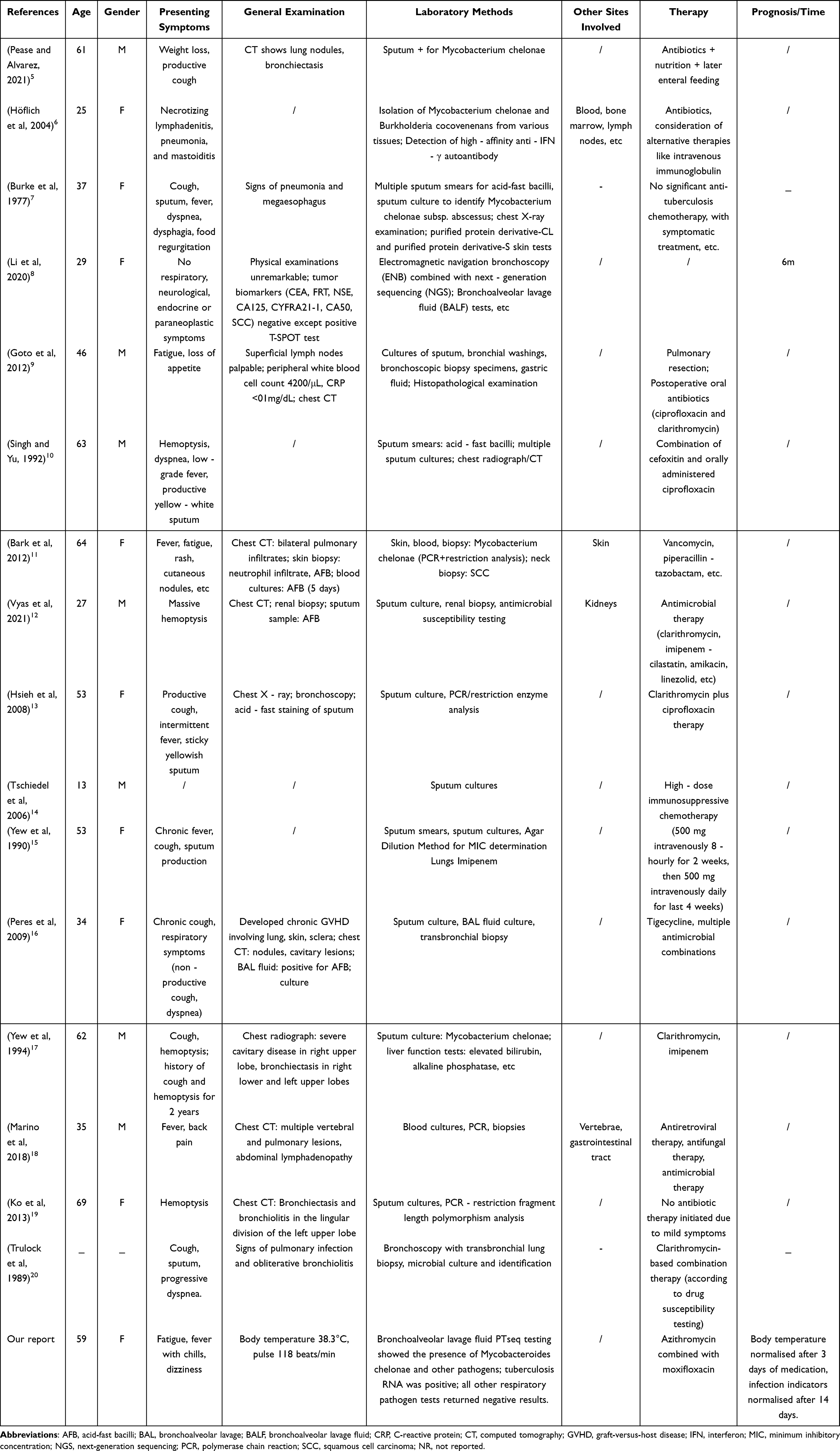 |
Table 2 Clinical Characteristics of Reported Pulmonary Mycobacterium chelonae Cases |
Discussion
Mycobacterium chelonae belongs to the class Actinomycetia, order Mycobacteriales, family Mycobacteriaceae. This polymorphic organism may present as long, slender rods or short, thick rods (0.2–0.5 × 1–6 μm), with occasional coccoid forms of approximately 0.5 μm in diameter also reported. Young colonies (<5 days) demonstrate strong acid-fast staining, which diminishes with prolonged cultivation. On most culture media, colonies are typically smooth, moist, and glossy, appearing within 3–4 days,21 and are nonpigmented or pale creamy yellow. Rough colony morphotypes may develop after approximately three weeks. M. chelonae is widely distributed in environmental reservoirs, including water, soil, dust, and healthcare settings. Human transmission occurs predominantly via environmental exposure, either through aerosol inhalation or via contact with contaminated water/food in the presence of skin breaches.22,23 As an opportunistic pathogen, it frequently causes infections when skin barriers are compromised (eg, surgery, trauma, cosmetic procedures) or when host immunity is impaired. Clinically, cutaneous infections often manifest with localized swelling, erythema, warmth, pain, and purulent discharge. Pulmonary disease presents with features consistent with pneumonia, including persistent cough, chest pain, hemoptysis, and dyspnea. Pulmonary M. chelonae infections are exceedingly rare.24,25 Given the rarity of pulmonary involvement and the necessity of tailoring diagnosis and treatment to the organism’s pathogenic profile, we systematically evaluated the reasons for consultation, therapeutic regimens, treatment duration, and clinical outcomes in the aforementioned cases, extracting essential diagnostic and management data to guide individualized therapeutic recommendations for such infections (see Table 1).
Rapidly growing mycobacteria (RGM) are environmental nontuberculous mycobacteria (NTM) that typically form visible colonies on solid media within approximately 7 days. Clinically important RGM include the Mycobacterium abscessus complex (subsp. abscessus, massiliense, and bolletii), Mycobacterium chelonae, and the Mycobacterium fortuitum group.26 Importantly, M. abscessus complex and M. chelonae are distinct species with different clinical spectra and antimicrobial resistance patterns; for example, inducible macrolide resistance mediated byerm (41) is common in M. abscessus subsp. abscessus but is typically absent in M. chelonae.3,26 Therefore, species-level confirmation by culture-based identification and, when feasible, antimicrobial susceptibility testing remain essential to guide management.23,27,28
Non-tuberculous mycobacterial pulmonary disease (NTM-PD) is diagnosed by integrating compatible clinical symptoms and radiologic findings with microbiologic evidence, as outlined in commonly used ATS/IDSA criteria and subsequent updates (eg, repeated positive sputum cultures, or a positive bronchoalveolar lavage culture/biopsy with compatible pathology, together with exclusion of alternative diagnoses).23,27,28 Importantly, detection of NTM nucleic acids alone cannot reliably distinguish colonization from true disease; therefore, sequencing results should be interpreted within the overall clinical context and in conjunction with imaging, AFB smear/culture, and definitive species identification.23,27,28 In this setting, metagenomic sequencing/PTseq can support early hypothesis generation and facilitate antimicrobial stewardship, but it should be regarded as an adjunct tool and does not replace standard confirmation or susceptibility-guided management.27–29 In addition, the clinical PTseq report did not provide assay reporting thresholds, negative-control results, or predefined quantitative cutoffs; therefore, the reported sequence counts were treated as semi-quantitative signals, and contamination or detection of non-viable nucleic acids cannot be excluded. Accordingly, we have framed the present case as a probable pulmonary M. chelonae infection with short-term clinical response, while acknowledging that classical microbiologic confirmation and longer follow-up would strengthen diagnostic certainty and treatment assessment.23,27,28
This report has several limitations inherent to a single-case description and a literature-based synthesis of published reports.30 Firstly, the predominance of cases from specific medical institutions introduces potential referral bias, thereby affecting the generalizability of findings. Secondly, missing critical information—such as environmental exposure history, immune status indicators, and detailed underlying disease trajectories—limits in-depth analysis of infection mechanisms and risk factors. Additionally, heterogeneity in specimen collection and diagnostic protocols over time and across institutions,31,32 compounded by technological limitations before the year 2000, may have led to underdiagnosis or misclassification.33 Other potentially influential factors—including prior NTM infection history, interspecies microbial interactions, and host genetic polymorphisms affecting antibiotic metabolism—remain unexplored and could impact both infection risk assessment and optimal therapeutic strategies.
To address these gaps, future investigations should adopt multicenter prospective designs to expand sample sizes, enhance data completeness (including standardized environmental exposure histories and longitudinal immune monitoring), and implement refined analytical methods such as metagenomic sequencing for detailed strain typing. Such approaches would facilitate a clearer understanding of M. chelonae infection characteristics and support optimization of management strategies.29
Conclusions
We report a rare case of probable pulmonary Mycobacterium chelonae infection in a patient with lung adenocarcinoma, in whom BALF PTseq supported early hypothesis generation and antimicrobial stewardship.
The azithromycin-moxifloxacin regimen was associated with short-term clinical improvement without significant adverse events in this immunocompromised patient. Given the lack of classic microbiologic confirmation and limited follow-up, this report should not be interpreted as evidence of definitive cure or as a basis for generalized treatment recommendations. Future studies incorporating confirmatory culture/species identification, susceptibility testing and longer follow-up are needed.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding authors (Bao Sun and Peng Ge) on reasonable request.
Ethics Approval and Consent to Participate
Written informed consent was provided by the patient for the publication of the case details. Details of the case can be published without institutional approval. According to the institutional policies of The Second Affiliated Hospital of Xi’an Medical University, formal ethical approval is not required for the publication of a single anonymised case report. Written informed consent for publication of the clinical details was obtained from the patient.
Consent for Publication
Written informed consent for publication was obtained from the patient.
Acknowledgments
We would like to thank the patient and the multidisciplinary clinical team for their contributions to this report.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by Shaanxi Pharmaceutical Association Project for High-Quality Development of Hospital Pharmacy (Grant No. XM-2024-1-1-7).
Disclosure
The authors declare no competing interests in this work.
References
1. Adjemian J, Olivier KN, Seitz AE, et al. Spatial clusters of nontuberculous mycobacterial lung disease in the United States. Am J Respir Crit Care Med. 2012;186(6):553–11. doi:10.1164/rccm.201205-0913OC
2. Prevots DR, Marras TK. Epidemiology of human pulmonary infection with nontuberculous mycobacteria: a review. Clin Chest Med. 2015;36(1):13–34. doi:10.1016/j.ccm.2014.10.002
3. Johansen MD, Herrmann JL, Kremer L. Non-tuberculous mycobacteria and the rise of Mycobacterium abscessus. Nat Rev Microbiol. 2020;18(7):392–407. doi:10.1038/s41579-020-0331-1
4. Nessar R, Cambau E, Reyrat JM, et al. Mycobacterium abscessus: a new antibiotic nightmare. J Antimicrob Chemother. 2012;67(4):810–818. doi:10.1093/jac/dkr578
5. Pease C, Alvarez GG. A case of relapsed Mycobacterium chelonae pulmonary infection presenting with severe weight loss and treated with a combination of antibiotic therapy and percutaneous feeding. J Clin Tuberc Other Mycobact Dis. 2021;22:100209. doi:10.1016/j.jctube.2020.100209
6. Hoflich C, Sabat R, Rosseau S, et al. Naturally occurring anti-IFN-gamma autoantibody and severe infections with Mycobacterium cheloneae and Burkholderia cocovenenans. Blood. 2004;103(2):673–675. doi:10.1182/blood-2003-04-1065
7. Burke DS, Ullian RB. Megaesophagus and pneumonia associated with Mycobacterium chelonei. A case report and a literature review. Am Rev Respir Dis. 1977;116(6):1101–1107. doi:10.1164/arrd.1977.116.6.1101
8. Y L, Zang Y, Wang Y, et al. Peripheral pulmonary nodule diagnosed as mycobacterium chelonae using electromagnetic navigation bronchoscopy combined with next generation sequencing: a case report. Am J Transl Res. 2020;12(7):4066–4073.
9. Goto T, Hamaguchi R, Maeshima A, et al. Pulmonary resection for mycobacterium chelonae infection. Ann Thorac Cardiovasc Surg. 2012;18(2):128–131. doi:10.5761/atcs.cr.11.01689
10. Singh N, Yu VL. Successful treatment of pulmonary infection due to Mycobacterium chelonae: case report and review. Clin Infect Dis. 1992;14(1):156–161. doi:10.1093/clinids/14.1.156
11. Bark CM, Traboulsi RS, Honda K, et al. Disseminated Mycobacterium chelonae infection in a patient receiving an epidermal growth factor receptor inhibitor for advanced head and neck cancer. J Clin Microbiol. 2012;50(1):194–195. doi:10.1128/JCM.05399-11
12. Vyas V, Bryant SM, Shah A, et al. Disseminated Mycobacterium chelonae infection with Hughes-Stovin syndrome. Proc. 2021;34(5):595–596. doi:10.1080/08998280.2021.1918817
13. Hsieh HC, Lu PL, Chen TC, et al. Mycobacterium chelonae empyema in an immunocompetent patient. J Med Microbiol. 2008;57(Pt 5):664–667. doi:10.1099/jmm.0.47574-0
14. Tschiedel E, Grasemann H, Ratjen F. Mycobacterium chelonae in a CF patient with anaplastic large cell lymphoma. J Cyst Fibros. 2006;5(2):133–136. doi:10.1016/j.jcf.2005.11.004
15. Yew WW, Kwan SY, Wong PC, et al. Ofloxacin and imipenem in the treatment of Mycobacterium fortuitum and Mycobacterium chelonae lung infections. Tubercle. 1990;71(2):131–133. doi:10.1016/0041-3879(90)90009-W
16. Peres E, Khaled Y, Krijanovski O I, et al. Mycobacterium chelonae necrotizing pneumonia after allogeneic hematopoietic stem cell transplant: report of clinical response to treatment with tigecycline. Transpl Infect Dis. 2009;11(1):57–63. doi:10.1111/j.1399-3062.2008.00351.x
17. Yew W W, Chau C H, Lee J, et al. Cholestatic hepatitis in a patient who received clarithromycin therapy for a Mycobacterium chelonae lung infection. Clin Infect Dis. 1994;18(6):1025–1026. doi:10.1093/clinids/18.6.1025
18. Marino A, Caltabiano E, Zagami A, et al. Rapid emergence of cryptococcal fungemia, Mycobacterium chelonae vertebral osteomyelitis and gastro intestinal stromal tumor in a young HIV late presenter: a case report. BMC Infect Dis. 2018;18(1):693. doi:10.1186/s12879-018-3573-z
19. Ko Y, Kim W, Shin B S, et al. Nontuberculous mycobacterial lung disease caused by mycobacterium chelonae: a case report. Tuberc Respir Dis. 2013;74(4):191–194. doi:10.4046/trd.2013.74.4.191
20. Trulock E P, Bolman R M, Genton R. Pulmonary disease caused by Mycobacterium chelonae in a heart-lung transplant recipient with obliterative bronchiolitis. Am Rev Respir Dis. 1989;140(3):802–805. doi:10.1164/ajrccm/140.3.802
21. Springer B, Stockman L, Teschner K, et al. Two-laboratory collaborative study on identification of mycobacteria: molecular versus phenotypic methods. J Clin Microbiol. 1996;34(2):296–303. doi:10.1128/jcm.34.2.296-303.1996
22. Falkinham J O. 3rd Environmental sources of nontuberculous mycobacteria. Clin Chest Med. 2015;36(1):35–41. doi:10.1016/j.ccm.2014.10.003
23. Griffith D E, Aksamit T, Brown-Elliott B A, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367–416. doi:10.1164/rccm.200604-571ST
24. Esther CR, Esserman DA, Gilligan P, et al. Chronic Mycobacterium abscessus infection and lung function decline in cystic fibrosis. J Cyst Fibros. 2010;9(2):117–123. doi:10.1016/j.jcf.2009.12.001
25. Saxena S, Spaink HP, Forn-Cuni G. Drug resistance in nontuberculous mycobacteria: mechanisms and models. Biology. 2021;10(2). doi:10.3390/biology10020096
26. Brown-Elliott B A, Philley J V. Rapidly growing mycobacteria. Microbiol Spectr. 2017;5(1). doi:10.1128/microbiolspec.TNMI7-0027-2016
27. Daley C L, Iaccarino J M, Lange C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA clinical practice guideline. Clin Infect Dis. 2020;71(4):e1–e36. doi:10.1093/cid/ciaa241
28. Haworth C S, Banks J, Capstick T, et al. British Thoracic Society guidelines for the management of non-tuberculous mycobacterial pulmonary disease (NTM-PD). Thorax. 2017;72(Suppl 2):ii1–ii64. doi:10.1136/thoraxjnl-2017-210927
29. Forbes J D, Knox N C, Peterson C L, et al. Highlighting clinical metagenomics for enhanced diagnostic decision-making: a step towards wider implementation. Comput Struct Biotechnol J. 2018;16:108–120. doi:10.1016/j.csbj.2018.02.006
30. Euser A M, Zoccali C, Jager K J, et al. Cohort studies: prospective versus retrospective. Nephron Clin Pract. 2009;113(3):c214–7. doi:10.1159/000235241
31. Griffith D E, Aksamit T R. Understanding nontuberculous mycobacterial lung disease: it’s been a long time coming. F1000Res. 2016;5:2797. doi:10.12688/f1000research.9272.1
32. Nadkarni M A, Martin F E, Jacques N A, et al. Determination of bacterial load by real-time PCR using a broad-range (universal) probe and primers set. Microbiology. 2002;148(Pt 1):257–266. doi:10.1099/00221287-148-1-257
33. Tortoli E. Microbiological features and clinical relevance of new species of the genus Mycobacterium. Clin Microbiol Rev. 2014;27(4):727–752. doi:10.1128/CMR.00035-14
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.