Back to Journals » Psychology Research and Behavior Management » Volume 18
A Study on the Effectiveness of Metacognitive Training in Treating Negative Symptoms of Different Subtypes of Schizophrenia
Authors Shen L, Yan J ![]() , Xiao W, Sun L, Du M, He Y
, Xiao W, Sun L, Du M, He Y
Received 21 June 2025
Accepted for publication 17 October 2025
Published 25 October 2025 Volume 2025:18 Pages 2225—2235
DOI https://doi.org/10.2147/PRBM.S548616
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Bao-Liang Zhong
Lijuan Shen,1,* Jing Yan,2,* Weixia Xiao,3 Lixin Sun,3 Mingjun Du,3 Yiqun He3
1Department of Clinical Psychology, the Second Affiliated Hospital of Xinxiang Medical University (Henan Mental Hospital), Xinxiang Key Laboratory of Diagnosis and Treatment Technology of Psychosomatic Diseases, Xinxiang, Henan, People’s Republic of China; 2Peking University Sixth Hospital, Peking University Institute of Mental Health, NHC Key Laboratory of Mental Health (Peking University), National Clinical Research Center for Mental Disorders (Peking University Sixth Hospital), Beijing, People’s Republic of China; 3The Second Affiliated Hospital of Xinxiang Medical University (Henan Mental Hospital), Xinxiang, Henan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lijuan Shen, Department of Clinical Psychology, the Second Affiliated Hospital of Xinxiang Medical University (Henan Mental Hospital), Xinxiang Key Laboratory of Diagnosis and Treatment Technology of Psychosomatic Diseases, Xinxiang, Henan, 453002, People’s Republic of China, Email [email protected] Jing Yan, Peking University Sixth Hospital, Peking University Institute of Mental Health, NHC Key Laboratory of Mental Health (Peking University), National Clinical Research Center for Mental Disorders (Peking University Sixth Hospital), Beijing, People’s Republic of China, Email [email protected]
Purpose: This study aims to investigate the efficacy of metacognitive training (MCT) as an adjunctive treatment strategy for schizophrenia, particularly its impact on negative symptoms and potential mechanisms.
Patients and Methods: This study included a total of 73 inpatients with schizophrenia. 36 patients were in the MCT group and 37 patients were in the control group. Both groups of patients were receiving a single second-generation antipsychotic drug treatment. The MCT group underwent a 4-week MCT program consisting of 8 modules, while the control group received non-cognitive psychological support for the same duration and frequency. The Positive and Negative Syndrome Scale (PANSS) five-factor model and negative symptom two-factor model were used to assess psychiatric symptoms, and the Snyder’s Self-Monitoring Scale (SSMS) and the Personal and Social Performance Scale (PSP) were used as functional evaluation indicators.
Results: After treatment, compared to the control group, the MCT group had significantly lower scores in the PANSS total score (p< 0.001), negative factor (p=0.002), and hostility factor (p=0.046). Further, the PSP score (p< 0.001) and SSMS score (p=0.042) were significantly improved. In the two-factor analysis of negative symptoms, the MCT group showed significant improvements in both diminished expression (DE) symptoms (p< 0.001) and social amotivation (SA) symptoms (p=0.010) after treatment. Multivariate linear regression analysis revealed that changes in the reduction rates of P2 (Conceptual disorganization), N7 (stereotyped thinking), and SA scores had a significant impact on the reduction in DE scores; changes in the reduction rates of P6 (Suspiciousness/persecution) and DE scores had a significant impact on the reduction rate of SA scores (p< 0.05).
Conclusion: MCT can improve the clinical symptoms and functions of patients with schizophrenia, especially in the DE factor characterized by conceptual disorganization and stereotyped thinking, and the SA factor prominent in suspiciousness/persecution symptom. This provides insights for the precise treatment of negative symptoms.
Keywords: metacognitive training, schizophrenia, negative symptoms, diminished expression, social amotivation
Introduction
Schizophrenia is a severe mental illness that typically manifests during adolescence or early adulthood, with a chronic or recurrent course. Patients often have persistent and poorly treated negative symptoms and cognitive impairment, which seriously affects their social function and imposes a heavy burden of disease. At present, more and more research evidence support that negative symptoms occupy a central position in many symptoms of schizophrenia, and 60% of patients have significant and persistent negative symptoms, which usually occur in the early stages of the disease and significantly reduce the ability of patients to perform daily activities. Patients with more prominent negative symptoms often experience worse functional outcomes, including impairments in occupational, household, and recreational functions, which can also lead to more relationship difficulties.1 In treatment-resistant schizophrenia (TRS), which is characterized by the lack of response to two or more antipsychotic medications, patients typically exhibit more severe and frequent negative symptoms. Recent studies have also indicated that the severity of the disease in this subgroup (TRS) may be mediated by the severity of negative symptoms.2 In recent years, there has been a growing demand for more effective treatment for negative symptoms to improve long-term prognosis. However, few medications for negative symptoms have shown substantial benefit. An increasing number of psychosocial and behavioral interventions have been developed and are synergistic with drug therapy to alleviate and treat negative symptoms.3
Metacognition was initially defined as the awareness of cognition, that is, the ability to monitor, evaluate, and regulate cognition itself.4 Subsequently, this definition has been expanded5 and is now considered as a more comprehensive ability to integrate complex representational information of self and others.6 This has led to the development of interventions targeting metacognitive processes, some of which, such as metacognitive training (MCT), were specifically designed for psychosis.7 The theoretical foundation of MCT is to indirectly alleviate psychiatric symptoms and associated distress by addressing cognitive biases, negative emotions, and low self-esteem that may lead to information processing errors at the cognitive level, which play an important role in the occurrence and development of mental illness.8 The aim is to increase patients’ “cognitive insight” and assist them in learning strategies for managing symptoms. In recent years, many studies have verified the feasibility, safety and effectiveness of MCT.9–11 A considerable number of studies have demonstrated that MCT can reduce delusions and positive symptoms, and improve cognitive insight and cognitive biases. However, there are also different conclusions.12–15 There is more controversy regarding the efficacy of MCT in treating negative symptoms. There is a correlation between negative symptoms and impaired ability to process self/other psychological states.5 Based on this finding, low metacognitive levels can predict higher negative symptom scores in the future.16 A recent meta-analysis on the short-term and long-term effects and moderating factors of metacognitive training in disease treatment suggested that MCT is associated with benefits within one year of the intervention. The short-term benefits are improvements in positive symptoms and cognitive biases, while the long-term benefits pertain to self-esteem, negative symptoms, quality of life, happiness, and functionality.17 However, the exact efficacy and mechanism of MCT in the treatment of negative symptoms remain to be studied.
Negative symptoms possess a complex internal structure. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V) distinguishes two substructures of negative symptoms: amotivation (including avolition, asociality and anhedonia) and diminished expression (including blunted affect and alogia). Currently, numerous studies have conducted factor analysis based on the PANSS scale, distinguishing negative symptoms into two factors: diminished expression (DE) and social amotivation (SA), and demonstrating that the PANSS scale can clearly differentiate between the two.18–20 The diminished expression factor include: Lack of spontaneity and flow of conversation (N6), Poor rapport (N3), Blunted affect (N1), Motor retardation (G7); and the social amotivation factor include: Passive/apathetic social withdrawal (N4), Active social avoidance (G16), Emotional withdrawal (N2). There are significant differences in clinical phenotypes between these two factors (subgroups) of negative symptoms, including pre-morbid functioning, clinical course, functional outcome, disorder symptoms, social cognition, gender, and ethnicity.21 This suggests that there are differences in the neural mechanisms underlying the two sets of symptoms, and different therapeutic targets may be required.
To investigate the precise efficacy of MCT on different clinical symptom clusters in patients with schizophrenia, especially its impact on different subtypes of negative symptoms and the potential mechanisms involved, this study employs MCT as an adjunctive treatment strategy for patients in the acute phase. Utilizing a two-factor structural model for negative symptoms19,20 and a five-factor structural model of the PANSS based on a large-scale multi-ethnic sample20 (to better align the measurement dimensions of symptoms with the psychopathological symptoms themselves), this study analyzes the improvement effects of MCT on clinical symptoms, psychological and social functions in patients with schizophrenia, particularly on different subtypes of negative symptoms. This study aims to provide further evidence for the clinical application of MCT and offer insights into treatment strategies for negative symptoms.
Materials and Methods
Participants
Inpatients from the Henan Mental Hospital were recruited between March 1, 2013 and July 1, 2013. Patients who met inclusion criteria were referred by each ward on a weekly basis. Patients were assigned to the MCT group and the control group according to the order in which the cases were submitted (for example, the first patient was assigned to the MCT group, the second to the control group, and so on). The grouping for each round was completed on the seventh day of the start of enrollment, with 3–10 patients in each group (if the enrollment for that round was less than 3 patients per group, the enrollment period could be extended to 10 days; otherwise, the enrollment for that round would be abandoned).
Inclusion criteria: 1. Aged 16–60 years; 2. Diagnosed with schizophrenia according to the DSM-IV; 3. Patients should be able to complete a one-hour training course; 4. Estimated that patients can complete 4 weeks of group therapy during hospitalization (the average length of hospital stay for inpatients is approximately 45 days); 5. Subjects and/or guardians fully understand and comprehend the research content of this trial, sign the informed consent form. For voluntary hospitalization, the consent form is generally signed by the patient himself, while for involuntary hospitalization, it needs to be signed by the patient’s guardian. Exclusion criteria: 1. History of brain organic diseases such as brain injury and dementia; 2. Individuals with intellectual disabilities (Raven’s Standard Progressive Matrices score greater than level 3); 3. Individuals with substance dependence. Dropout criteria: 1. Subjects withdraw their informed consent; 2. Completing the psychological treatment module ≤3 times (out of a total of 8 sessions); 3. Patients exhibiting impulsive, aggressive, and self-injurious or suicidal behaviors during the treatment process. Based on the preliminary exploratory research data,22 the MCT group showed a significant difference with a calculated effect size of 0.64. Using a two-independent-samples t-test, the significance level was set at 0.05, the statistical power was set at 80%, and a two-tailed test was conducted. The calculation was performed using G*Power software. A dropout rate of 20% was reserved for dropouts, with 50 participants included in each group. Finally, this study collected a total of 38 patients in the MCT group and 39 in the control group. After excluding patients with incomplete data, 36 patients in the MCT group and 37 in the control group were ultimately included in the data analysis.
The MCT group received MCT treatment twice a week, with one module per session lasting approximately 45–60 minutes. One cycle of the study was completed in 4 weeks. This form was chosen based on the suggestions of the MCT author.23 The control group received clinical psychological care twice a week, with each session lasting approximately 45–60 minutes, providing non-cognitive psychological support and counseling. Meanwhile, both groups of patients were treated with an antipsychotic monotherapy.
In accordance with the Declaration of Helsinki, the protocol involving human participants was reviewed and approved by the Ethics Committee of the Second Affiliated Hospital of Xinxiang Medical University (Project Number: SYJS2022057). After fully understanding the objectives and methods of the study, all participants signed the informed consent form.
Assessment and Procedure
Senior psychiatrists assessed and recruited patients, and researchers verified them according to inclusion and exclusion criteria. The included patients completed the signing of informed consent forms and the assessment of scales.
Participants used the following scales for evaluation:
A Self-Designed General Questionnaire
It collects general information such as gender, age, education level, family history, as well as detailed medical history including disease duration, age of onset, number of recurrences and hospitalizations, and medication status.
Positive and Negative Syndrome Scale (PANSS)
The PANSS24 scale is a widely used clinical assessment scale that evaluates the clinical symptoms and symptom severity of schizophrenia patients through 30 symptom items.
Five-Factor PANSS Model
Positive factor: P1, G9, P6, P3, P5;
Negative factor: N2, N4, N6, N3, N1, G16, G7;
Cognitive/disorganization factor: P2, G11, N7, N5, G13, G5, G15;
Depression/anxiety factor: G2, G3, G6, G4, G1;
Hostility factor: P7, G8, G14, P4.
Two-Factor Structure of Negative Symptoms
Diminished expression (DE): N6, N3, N1, G7;
Social amotivation (SA): N4, G16, N2.
Snyder’s Self-Monitoring Scale (SSMS)
This25 scale consists of 25 questions, with scores ranging from 0 to 25. Each question is answered with a score of 1 if the answer matches the given response, otherwise no score is given. A higher score indicates a higher level of self-monitoring. Self-monitoring ability reflects an individual’s psychological tendency to pay attention to environmental cues and self-behavior in social interactions, as well as their ability to regulate self-expression.
Personal and Social Performance Scale (PSP)
This26 scale measures overall performance in terms of social function and personal abilities. By quantifying patients’ performance in daily life, social interaction, self-care, and symptom control, it is used for rehabilitation assessment and treatment effect monitoring of patients with schizophrenia and other severe mental disorders. The scale adopts a grading scoring system, typically ranging from 1 to 100 points, with higher scores indicating better personal and social performance.
Re-assessment of PANSS, SSMS, and PSP were also administered within one week after the end of treatment. The rating scale was evaluated by experienced senior psychiatrists, and the raters underwent consistency training.
Interventions
All patients received conventional treatment (monotherapy with second-generation antipsychotic medication). Patients in both the MCT group and the control group underwent 8 sessions of treatment over 4 weeks. The therapists were all psychologists or psychiatrists with long-term experience in treating schizophrenia spectrum disorders and had experience in group courses. Each treatment session in the MCT group is presented through a set of slides, including the core theories, practical examples and matching exercises corresponding to the current module, to help patients perceive their cognitive distortions and correct cognitive biases through example exercises. The specific operation is as follows: In each class, the therapist will first explain common prejudices in the module through slides; illustrate the correlation between these cognitive prejudices and mental illnesses with cases from daily life; conduct group discussions with a large number of practice cases in the course to address these prejudices; and finally, distribute homework practice sheets at the end of the course. Homework can be completed with the help of an auxiliary tool: a yellow card (containing three basic questions: 1. What is the evidence? 2. Are there different opinions? 3. Even if it seems like. Am I overreacting? This card is for patients to use when necessary, such as when they feel offended. It aims to prompt patients to rethink before engaging in inappropriate behavior). In addition, during non-treatment periods, patients can obtain necessary support through the red card (which contains the name, phone number, and affiliation of the person who can be contacted in case of emergency). Before each session, the therapist will assess the patient’s response to the treatment module by checking their homework. The MCT course consisted of 8 modules, each exploring a single cognitive bias27 (Table 1). The control group also received non-cognitive psychological support and counseling through slides, including lectures on mental illness-related knowledge, emotional management, and relaxation therapy.
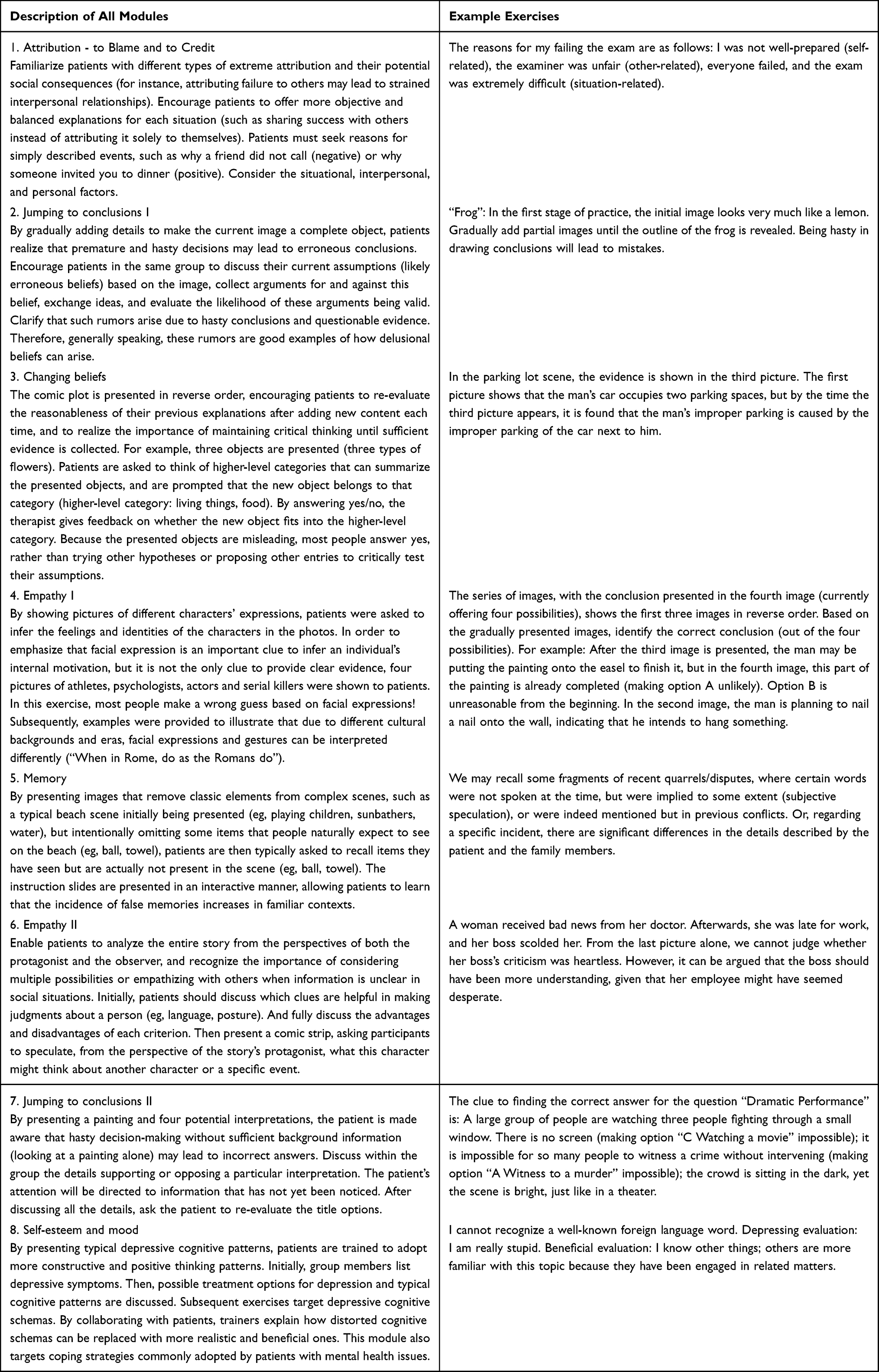 |
Table 1 The Main Content and Objectives of Each MCT Module |
Statistical Analysis
Data statistical analysis was conducted using SPSS 27.0. Measurement data conforming to a normal distribution were expressed as mean ± standard deviation (xˉ±s), and t-tests were used for inter-group comparisons. Data not conforming to a normal distribution were expressed as M (Q1, Q3), and Mann–Whitney U-tests were used for inter-group comparisons. Enumeration data were expressed as the number of cases, and chi-square tests were used for inter-group comparisons. In correlation analysis, Pearson correlation analysis was used for data that conform to a normal distribution, while Spearman correlation analysis was used for data that do not conform to a normal distribution. Multiple linear regression analysis was employed to evaluate the influencing factors of the change in negative symptom reduction rate. The reduction rate is expressed as: (baseline score - post-treatment score)/baseline score. All statistical analyses were considered statistically significant with a two-tailed p-value < 0.05.
Results
General Features
The MCT group ultimately included 36 patients, while the control group included 37 patients. There were no significant differences between the two groups in terms of age, gender, family history, onset age, disease duration, recurrence frequency, and hospitalization frequency. The number of years of education for patients in the MCT group was significantly higher than that in the control group (p=0.027). After 4 weeks of treatment, there was no significant difference in the medication dosages used by the two groups of patients (Table 2).
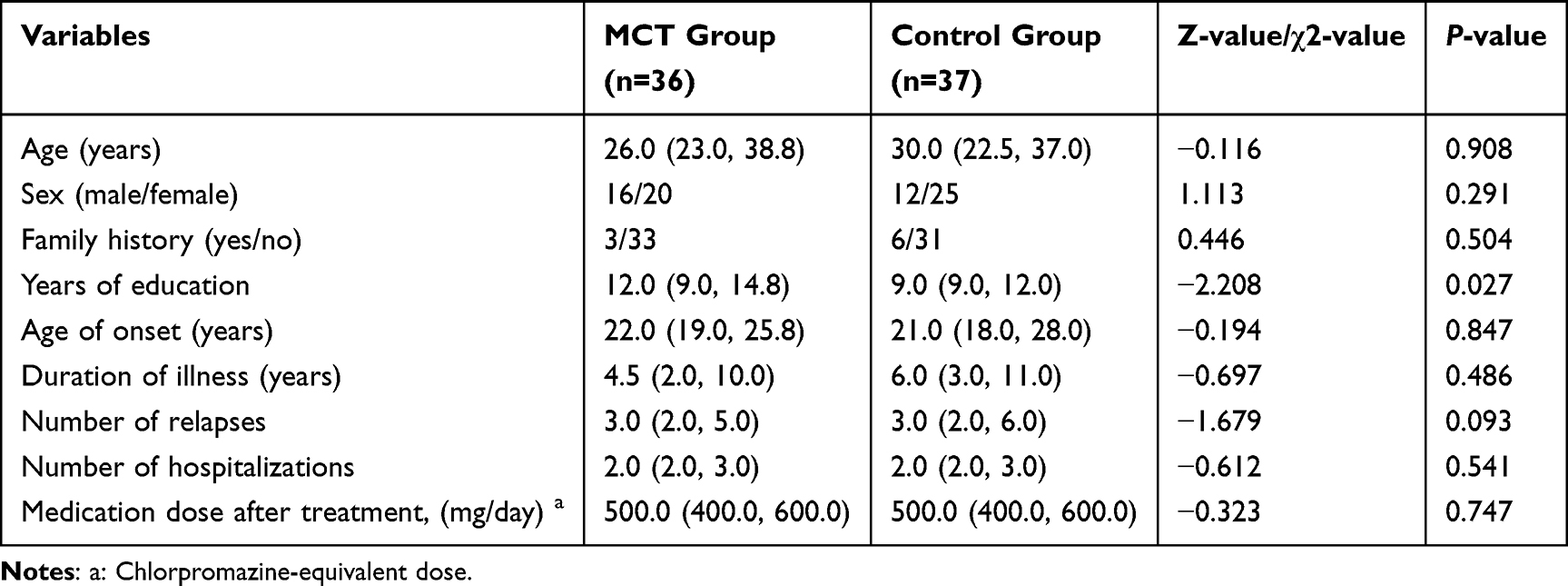 |
Table 2 General Information Comparison |
Comparison of Clinical Assessments
At baseline, there were no significant differences in the PANSS total score, positive, negative, depression/anxiety, and hostility factors among the five factors of PANSS, as well as the PSP score and Snyder score between the two groups. After treatment (4 weeks), both groups showed improvements in various scores. The MCT group scored significantly lower than the control group in the PANSS total score (p<0.001), as well as in the negative factor (p=0.002), and hostility factor (p=0.046) scores. The positive factor score showed a downward trend, but there was no significant difference. Meanwhile, the PSP score (p<0.001) and SSMS score (p=0.042) were significantly higher in the MCT group compared to the control group (Table 3).
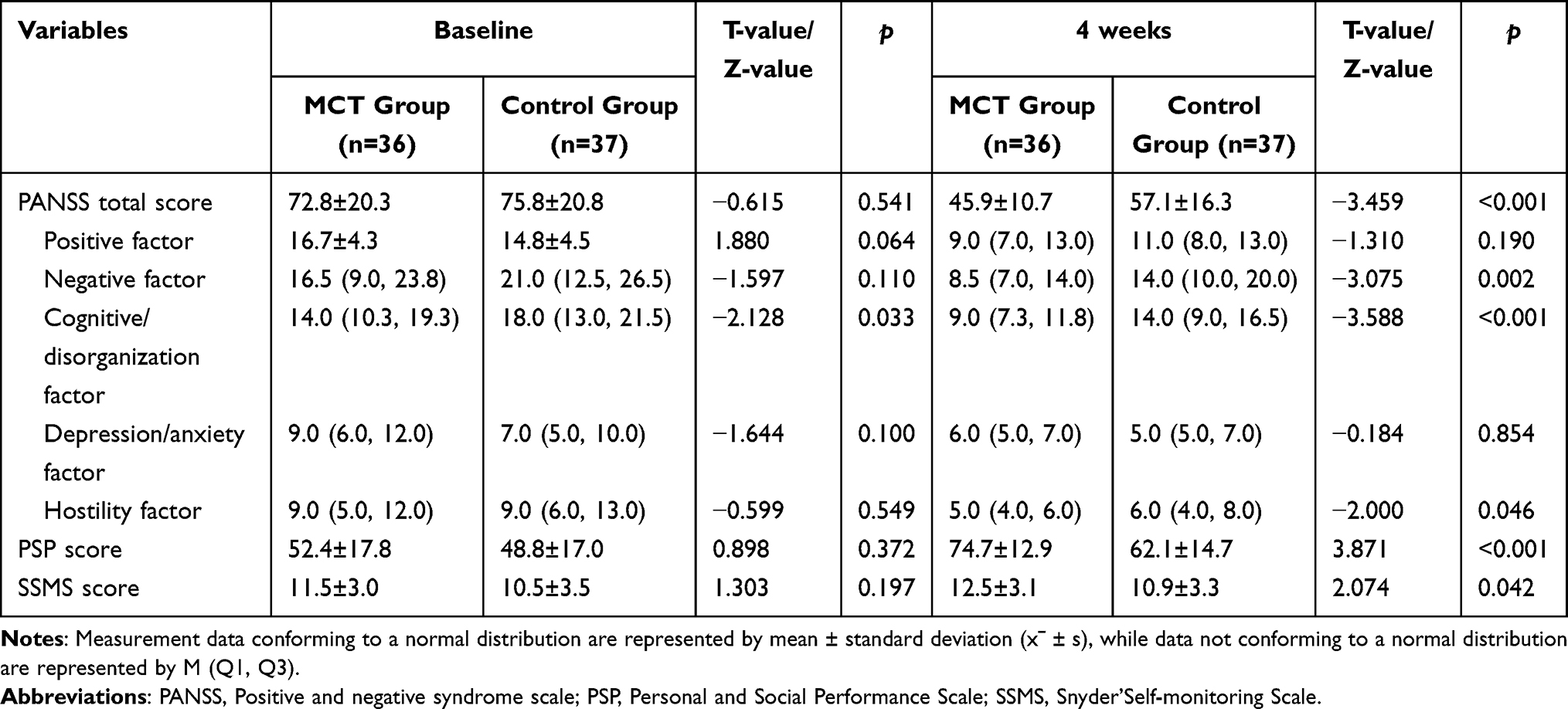 |
Table 3 Clinical Assessment Before and After Treatment |
Comparison of Negative Symptoms
At baseline, there was no significant difference in the two factors of negative symptoms between the two groups. After treatment, compared to the control group, the MCT group showed significant improvements in both DE symptoms (p<0.001) and SA symptoms (p=0.010) of negative symptoms (Table 4).
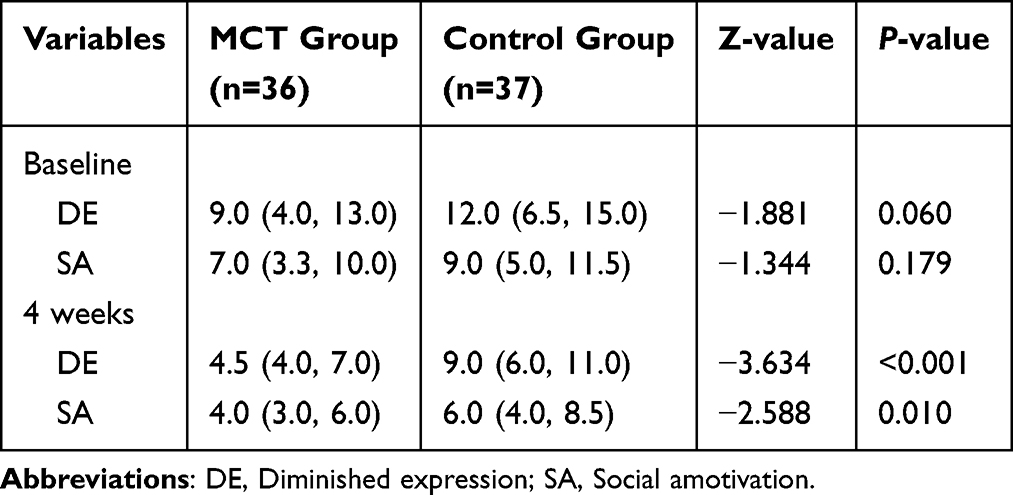 |
Table 4 Comparison of Two Factors of Negative Symptoms Before and After Treatment |
Correlation Analysis of the Two-Factor Reduction Rate of Negative Symptoms
MCT treatment primarily focuses on training aimed at cognitive biases. Therefore, a correlation analysis was conducted between the DE and SA score reduction rates in the MCT group and the score reduction rates of positive factors (P1, G9, P6, P3, P5) and cognitive/disorganization factors (P2, G11, N7, N5, G13, G5, G15). After normality testing, the SA and P1 score reduction rates conformed to a normal distribution, and Pearson correlation analysis was used; the remaining indicators did not conform to a normal distribution, and Spearman correlation analysis was employed. The strength of the correlation was indicated by the correlation coefficient. It was found that there was a significant positive correlation between the DE score reduction rate and the score reduction rates of SA, P1, P3, P2, G11, N7, N5, and G13 (p<0.05); there was also a significant positive correlation between the SA score reduction rate and the score reduction rates of DE, P1, P6, P3, P2, N5, and G13 (p<0.05) (Supplementary Table 1).
Using the DE score reduction rate and SA score reduction rate as dependent variables, respectively, and selecting meaningful item score reduction rates as independent variables through correlation analysis, we substituted them into the multiple linear regression equation. The results showed that changes in the score reduction rates of P2, N7, and SA had a significant impact on the DE score reduction rate (p<0.05); changes in the score reduction rate of P6 and DE had a significant impact on the SA score reduction rate (p<0.05) (Table 5).
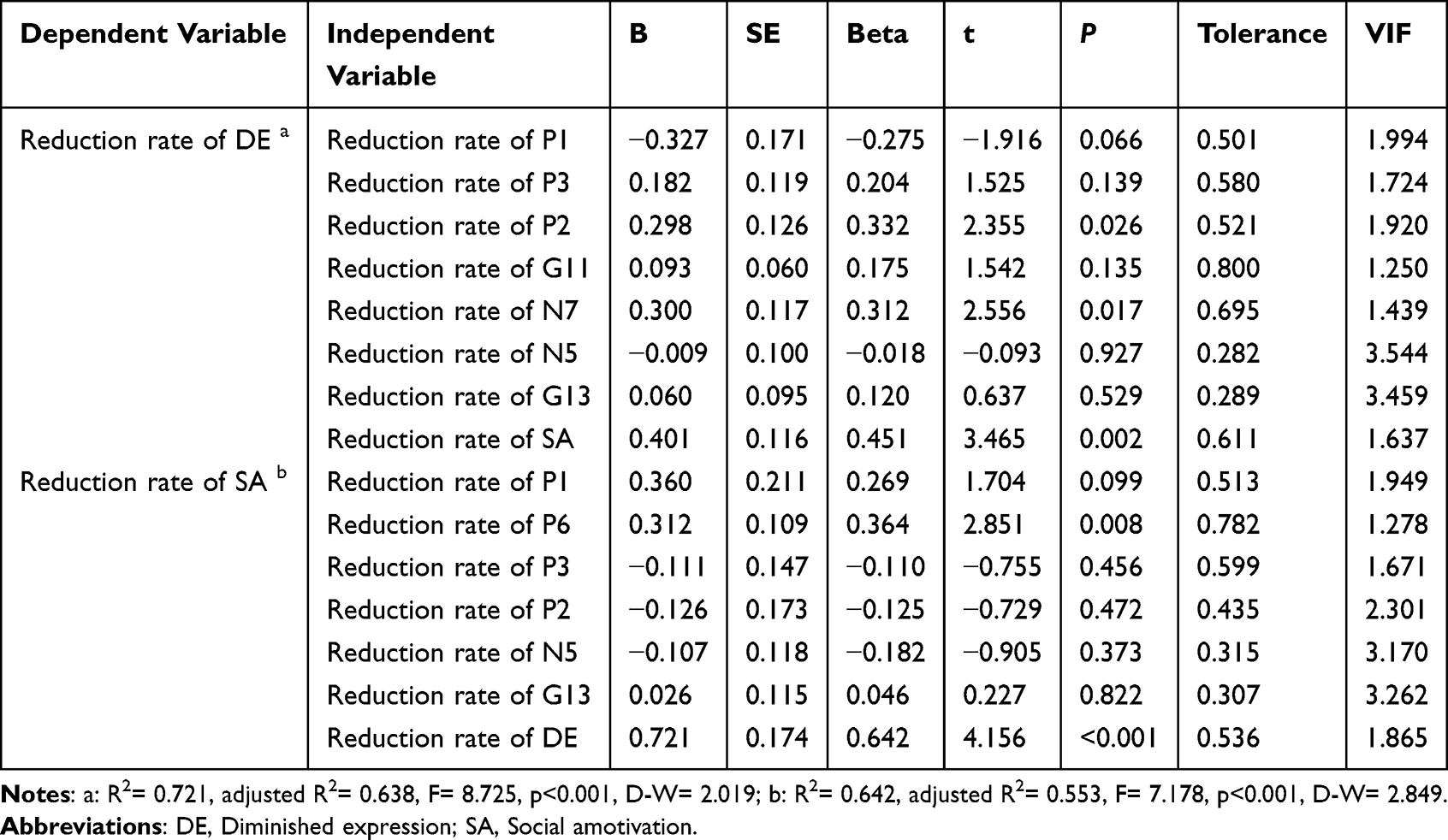 |
Table 5 Multiple Linear Regression Analysis of the Reduction Rate of Two Factors in Negative Symptoms |
Discussion
This study is the first to employed a more precise classification model based on the PANSS scale to explore the efficacy of MCT in treating different types of clinical symptoms in patients with schizophrenia, and further elucidated the efficacy and possible mechanism of MCT in treating different subtypes of negative symptoms. The current study found that MCT significantly improved overall psychiatric symptoms, negative symptoms, and hostile symptoms, and significantly enhanced patients’ self-monitoring ability and personal and social functioning. MCT significantly improved both factors of diminished expression (DE) and social amotivation (SA) in negative symptoms. This is related to the improvement of conceptual disorganization and stereotyped thinking symptoms in the DE factor, as well as the improvement of suspiciousness/persecution symptoms in the SA factor.
Previous studies have found that after MCT treatment, the overall psychiatric symptoms (PANSS total score) of schizophrenia patients significantly improve.28,29 To enhance the precision of measuring psychiatric symptoms, this study further categorized the PANSS scale into five factors based on previous research evidence: positive factors, negative factors, cognitive/disorganization factors, depressive/anxiety factors, and hostile factors. To our knowledge, this is the first time to use the refined PANSS scale classification to assess the effectiveness of MCT on symptoms in patients with schizophrenia. This study found that MCT significantly improved negative symptoms and hostile symptoms. There was a noticeable trend towards improvement in positive symptoms. It is suggested that MCT can be used in targeted treatment for negative symptoms, and significant improvement in hostile symptoms may reduce patients’ clinical risks, which is more conducive to clinical management and home care, providing a basis for a good prognosis of the disease. At the same time, it was found that the patients’ self-monitoring ability, as well as their personal and social functions, significantly improved, indicating that the patients had become more prosocial. Their attention to environmental cues and regulation of self-expression could promote better social functioning. This may be due to the therapeutic benefits of MCT on cognitive biases being transferred to psychosocial functioning and insight into the disease.11 It is more conducive to patients’ integration into society, addressing challenges in the workplace, and improving work outcomes.30
A large number of previous studies have demonstrated the validity of the two-factor structure of negative symptoms.31–33 The two-factor structure is associated with different clinical symptom clusters in schizophrenia, and behavioral and neuroimaging research support the possibility of different underlying mechanisms.32 It is proposed that different treatment strategies may be required. The current study further explored the efficacy and potential mechanisms of MCT on different subtypes of negative symptoms. It was found that MCT, as an adjunctive therapy for patients with schizophrenia, significantly improved negative symptoms in two subtypes: diminished expression (DE) and social amotivation (SA), with potentially more pronounced improvement in symptoms of DE. Related to the improvement of the DE factor are the improvements in symptoms of conceptual disorganization (P2) and stereotyped thinking (N7), as well as the improvement of the SA factor. Related to the improvement of the SA factor are the improvements in symptoms of suspiciousness/persecution (P6), as well as the DE factor. This provides evidence for the effectiveness of MCT in treating different subtypes of negative symptoms. Previous research on the underlying mechanisms of alogia has indicated that reduced expression is associated with limited cognitive resources. Generating speech in social situations requires a high degree of cognitive processing. When cognitive resources are limited, patients’ speech output may decrease. Furthermore, aphasia is associated with poor language fluency, such as the ability to control retrieval34 and semantic memory.35 Current research has reversely verified the role of cognitive correction (improving conceptual disorganization and stereotyped thinking symptoms) in treating the negative symptom subtype of DE. Neurocognitive research suggests that motivational disorders are associated with abnormalities in various reward processing, including certain aspects of impairments in reinforcement learning, reward prediction, and prediction error processing.36 Patients with schizophrenia can be reluctant to make efforts to obtain rewards. The underlying psychological mechanism that may cause this motivational disorder is believed to be related to negative experiences that lead to patients’ negative expectations about their ability to successfully complete goal-oriented tasks, namely defeatist beliefs and negative expectations.37 Therefore, we believe that MCT exerts an indirect therapeutic effect on the negative symptom subtype of SA by improving symptom of suspiciousness/persecution (negative thinking patterns about one’s own situation). However, the improvements of these two subtypes are to some extent interrelated. On the one hand, the two dimensions of symptoms may not be completely independent, but there is a certain degree of overlap between them. For example, some studies have found that reduced motivation is not only the basis of the SA factor but also the basis of all negative symptoms, including DE.38 On the other hand, the scope and structural clarity of the PANSS item set may play a role. For instance, the assessment of N2 and N6 relies on observable external behaviors, which can lead to ambiguity in the output results.
The current study employs the PANSS five-factor and negative symptom two-factor models to investigate the precise efficacy of MCT as an adjunctive therapy for psychiatric symptoms, and further explores the distinct mechanisms and potential treatment strategies of the negative symptom two-factor model. However, the study has certain limitations. Firstly, the sample size is relatively small, and the educational levels of the two patient groups were not matched, making it difficult to clearly determine the significance of MCT’s efficacy on cognitive/disorganization factors. Furthermore, the study observed a relatively obvious trend in the improvement of positive factors by MCT. However, we believe that the limited sample size prevented the results from showing significant differences. In the future, the sample size could be further expanded for more in-depth research. Secondly, the negative symptom assessment scale used in the study is relatively simple, with limited differentiation and targeted treatment guidance for negative symptoms. In the future, other negative symptom assessment tools could be introduced to facilitate more detailed differentiation of symptoms, delve deeper into the mechanism of action of MCT, and provide clearer guidance for the selection of clinical treatment strategies.
Conclusion
This study is the first to utilize the PANSS five-factor model and the negative symptoms two-factor model for precise classification of schizophrenia symptoms, aiming to evaluate the effectiveness of MCT as an adjunctive treatment strategy for schizophrenia. MCT significantly improved overall psychiatric symptoms, negative symptoms, and hostile symptoms, while also significantly enhancing patients’ self-monitoring abilities as well as their personal and social functioning. Additionally, MCT could effectively improve the two subtypes of negative symptoms: diminished expression and social amotivation, especially in the diminished expression factor characterized by conceptual disorganization and stereotyped thinking, and the social amotivation factor prominent in suspiciousness/persecution symptom. This study further provides evidence for the application of MCT in the adjuvant treatment of schizophrenia and offers insights into the more precise treatment of negative symptoms with MCT.
Acknowledgments
This work was supported by the Second Affiliated Hospital of Xinxiang Medical University Application of Metacognitive Training Technique in Psychiatric Rehabilitation (No. SYJS2022057) and the Open Project of Psychiatry and Neuroscience Discipline of Second Affiliated Hospital of Xinxiang Medical University (No. XYEFYJSSJ-2024-12).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Marder SR, Umbricht D. Negative symptoms in schizophrenia: newly emerging measurements, pathways, and treatments. Schizophr Res. 2023;258:71–77. doi:10.1016/j.schres.2023.07.010
2. Saleh Y, Jarratt-Barnham I, Petitet P, Fernandez-Egea E, Manohar SG, Husain M. Negative symptoms and cognitive impairment are associated with distinct motivational deficits in treatment resistant schizophrenia. Mol Psychiatry. 2023;28(11):4831–4841. doi:10.1038/s41380-023-02232-7
3. Cella M, Roberts S, Pillny M, et al. Psychosocial and behavioural interventions for the negative symptoms of schizophrenia: a systematic review of efficacy meta-analyses. Br J Psychiatry. 2023;223(1):321–331. doi:10.1192/bjp.2023.21
4. Flavell JH. Metacognition and cognitive monitoring: a new area of cognitive–developmental inquiry. Am Psychologist. 1979;34(10):906–911. doi:10.1037/0003-066X.34.10.906
5. Swanson L, Schwannauer M, Bird T, et al. Metacognitive training modified for negative symptoms: a feasibility study. Clin Psychol Psychother. 2022;29(3):1068–1079. doi:10.1002/cpp.2692
6. Lysaker PH, Minor KS, Lysaker JT, et al. Metacognitive function and fragmentation in schizophrenia: relationship to cognition, self-experience and developing treatments. Schizophrenia Res. 2020;19:100142. doi:10.1016/j.scog.2019.100142
7. Steffen Moritz TSW, Woodward TS. Metacognitive training in schizophrenia: from basic research to knowledge translation and intervention. Curr Opin Psychiatry. 2007;20(6):619–625. doi:10.1097/YCO.0b013e3282f0b8ed
8. Pos K, Meijer CJ, Verkerk O, Ackema O, Krabbendam L, de Haan L. Metacognitive training in patients recovering from a first psychosis: an experience sampling study testing treatment effects. Eur Arch Psychiatry Clin Neurosci. 2018;268(1):57–64. doi:10.1007/s00406-017-0833-7
9. Philipp R, Kriston L, Lanio J, et al. Effectiveness of metacognitive interventions for mental disorders in adults-A systematic review and meta-analysis (METACOG). Clin Psychol Psychother. 2019;26(2):227–240. doi:10.1002/cpp.2345
10. Ochoa S, Lopez-Carrilero R, Barrigon ML, et al. Randomized control trial to assess the efficacy of metacognitive training compared with a psycho-educational group in people with a recent-onset psychosis. Psychol Med. 2017;47(9):1573–1584. doi:10.1017/S0033291716003421
11. Melville G, Hoffman M, Pollock A, Kurtz MM. Do metacognitive therapies for schizophrenia-spectrum disorders work? A meta-analytic investigation. Psychol Med. 2024;54(8):1510–1518. doi:10.1017/S0033291724000564
12. Liu YC, Tang CC, Hung TT, Tsai PC, Lin MF. The efficacy of metacognitive training for delusions in patients with schizophrenia: a meta-analysis of randomized controlled trials informs evidence-based practice. Worldviews Evid Based Nurs. 2018;15(2):130–139. doi:10.1111/wvn.12282
13. Briki M, Monnin J, Haffen E, et al. Metacognitive training for schizophrenia: a multicentre randomised controlled trial. Schizophr Res. 2014;157(1–3):99–106. doi:10.1016/j.schres.2014.06.005
14. Birules I, Lopez-Carrilero R, Cuadras D, et al. Cognitive insight in first-episode psychosis: changes during metacognitive training. J Pers Med. 2020;10(4):253. doi:10.3390/jpm10040253
15. Sauve G, Lavigne KM, Pochiet G, Brodeur MB, Lepage M. Efficacy of psychological interventions targeting cognitive biases in schizophrenia: a systematic review and meta-analysis. Clin Psychol Rev. 2020;78:101854. doi:10.1016/j.cpr.2020.101854
16. Lysaker PH, Kukla M, Dubreucq J, et al. Metacognitive deficits predict future levels of negative symptoms in schizophrenia controlling for neurocognition, affect recognition, and self-expectation of goal attainment. Schizophr Res. 2015;168(1–2):267–272. doi:10.1016/j.schres.2015.06.015
17. Penney D, Sauve G, Mendelson D, Thibaudeau E, Moritz S, Lepage M. Immediate and sustained outcomes and moderators associated with metacognitive training for psychosis: a systematic review and meta-analysis. JAMA Psychiatry. 2022;79(5):417–429. doi:10.1001/jamapsychiatry.2022.0277
18. Liemburg E, Castelein S, Stewart R, et al. Two subdomains of negative symptoms in psychotic disorders: established and confirmed in two large cohorts. J Psychiatr Res. 2013;47(6):718–725. doi:10.1016/j.jpsychires.2013.01.024
19. Kaliuzhna M, Kirschner M, Carruzzo F, et al. Clinical, behavioural and neural validation of the PANSS amotivation factor. Schizophr Res. 2020;220:38–45. doi:10.1016/j.schres.2020.04.018
20. Lim K, Peh OH, Yang Z, et al. Large-scale evaluation of the Positive and Negative Syndrome Scale (PANSS) symptom architecture in schizophrenia. Asian J Psychiatr. 2021;62:102732. doi:10.1016/j.ajp.2021.102732
21. Strauss GP, Horan WP, Kirkpatrick B, et al. Deconstructing negative symptoms of schizophrenia: avolition-apathy and diminished expression clusters predict clinical presentation and functional outcome. J Psychiatr Res. 2013;47(6):783–790. doi:10.1016/j.jpsychires.2013.01.015
22. Moritz S, Veckenstedt R, Randjbar S, Vitzthum F, Woodward TS. Antipsychotic treatment beyond antipsychotics: metacognitive intervention for schizophrenia patients improves delusional symptoms. Psychologic Med. 2011;41:1823–1832. doi:10.1017/S0033291710002618
23. Moritz S, Woodward TS, Burlon M. Metacognitive skill training for patients with schizophrenia (MCT), manual. VanHam Campus Verlag Hamburg. 2005.
24. Kay SR, Opler LA, Fiszbein A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–276. doi:10.1093/schbul/13.2.261
25. Snyder M. Self-monitoring of expressive behavior. J personal soc psycholog. 1974;30:526–537. doi:10.1037/h0037039
26. Chiu E-C, Hung T-M, Huang C-M, Lee S-C, Hsieh C-L. Responsiveness of the personal and social performance scale in patients with schizophrenia. Psychiatry Res. 2018;260:338–342. doi:10.1016/j.psychres.2017.11.053
27. Moritz S, Andreou C, Schneider BC, et al. Sowing the seeds of doubt: a narrative review on metacognitive training in schizophrenia. Clin Psychol Rev. 2014;34(4):358–366. doi:10.1016/j.cpr.2014.04.004
28. Moritz S, Balzan RP, Menon M, et al. Two decades of metacognitive training for psychosis: successes, setbacks, and innovations. Expert Rev Neurother. 2025;25(5):579–590. doi:10.1080/14737175.2025.2483204
29. Fekete Z, Vass E, Balajthy R, et al. Efficacy of metacognitive training on symptom severity, neurocognition and social cognition in patients with schizophrenia: a single-blind randomized controlled trial. Scand J Psychol. 2022;63(4):321–333. doi:10.1111/sjop.12811
30. Zalzala A, Fiszdon JM, Moritz S, et al. Metacognitive training to improve insight and work outcome in schizophrenia. J Nerv Ment Dis. 2022;210(9):655–658. doi:10.1097/NMD.0000000000001512
31. Bucci P, Galderisi S. Categorizing and assessing negative symptoms. Curr Opin Psychiatry. 2017;30(3):201–208. doi:10.1097/YCO.0000000000000322
32. Kaiser S, Lyne J, Agartz I, Clarke M, Morch-Johnsen L, Faerden A. Individual negative symptoms and domains - relevance for assessment, pathomechanisms and treatment. Schizophr Res. 2017;186:39–45. doi:10.1016/j.schres.2016.07.013
33. Kaliuzhna M, Kirschner M, Carruzzo F, et al. How far to go in deconstructing negative symptoms? Behavioural and neural level evidence for the amotivation domain. Schizophr Res. 2021;236:41–47. doi:10.1016/j.schres.2021.08.007
34. Docherty AR, Berenbaum H, Kerns JG. Alogia and formal thought disorder: differential patterns of verbal fluency task performance. J Psychiatr Res. 2011;45(10):1352–1357. doi:10.1016/j.jpsychires.2011.04.004
35. Sumiyoshi C, Sumiyoshi T, Nohara S, et al. Disorganization of semantic memory underlies alogia in schizophrenia: an analysis of verbal fluency performance in Japanese subjects. Schizophr Res. 2005;74(1):91–100. doi:10.1016/j.schres.2004.05.011
36. Strauss GP, Waltz JA, Gold JM. A review of reward processing and motivational impairment in schizophrenia. Schizophr Bull. 2014;40(Suppl 2):S107–16. doi:10.1093/schbul/sbt197
37. Couture SM, Blanchard JJ, Bennett ME. Negative expectancy appraisals and defeatist performance beliefs and negative symptoms of schizophrenia. Psychiatry Res. 2011;189(1):43–48. doi:10.1016/j.psychres.2011.05.032
38. Foussias G, Remington G. Negative symptoms in schizophrenia: avolition and Occam’s razor. Schizophr Bull. 2010;36(2):359–369. doi:10.1093/schbul/sbn094
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.