Back to Journals » International Journal of Women's Health » Volume 18
A Study of Potential Classes and Trajectories of Psychological Distress in Infertility Patients: A Study Protocol
Authors Liu Y ![]() , Fan J, Wu F, Li B, Yi M, Yu J, Li G, An J, Yan X
, Fan J, Wu F, Li B, Yi M, Yu J, Li G, An J, Yan X
Received 4 March 2026
Accepted for publication 19 May 2026
Published 26 May 2026 Volume 2026:18 606751
DOI https://doi.org/10.2147/IJWH.S606751
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Ying Liu,1,2,* JiHua Fan,3,* FengJuan Wu,4 BingYu Li,2 MiaoMiao Yi,2 JiaYi Yu,2 Guo Li,2 JiaYi An,2 Xin Yan1,2
1Nursing Department, Affiliated Hospital of Zunyi Medical University, Zunyi, Guizhou, 563000, People’s Republic of China; 2Nursing College, Zunyi Medical University, Zunyi, Guizhou, 563000, People’s Republic of China; 3Guangxi Key Laboratory of Special Biomedicine/Advanced Institute for Brain and Intelligence, School of Medicine, Guangxi University, Nanning, 530004, People’s Republic of China; 4Department of Neurology, Lanzhou University Second Hospital, Lanzhou, Gansu, 730030, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xin Yan, Email [email protected]
Background: Infertility as a multi-dimensional stressor, the heavy burden of disease significantly restricts the release of the reproductive potential of this group, and brings physiological and psychological troubles to a large number of women. Moreover, intense and continuous psychological distress will lead to further serious psychological problems and various mental diseases. However, the longitudinal evolution trajectory of psychological distress and its key influencing factors have not been systematically clarified. This study aims to reveal temporal changes in psychological distress among infertility patients, analyze the probability of transformation and the key influencing factors, and provide a theoretical basis and practical guidance for early and precise psychological distress intervention.
Methods: Infertility patients in the gynecological outpatient department of the Affiliated Hospital of Zunyi Medical University from September 2024 to December 2025 were selected as potential study subjects, and the final study subjects were established according to the exclusion criteria. First, potential classes of psychological distress among infertility patients were identified using latent class analysis (LCA), and relevant measures were administered at 3-, 6-, and 12-month intervals after the first data collection from the study subjects. The development trajectory of psychological distress of infertility patients and its correlation analysis were obtained through the data analysis based on latent transition analysis (LTA).
Discussion: Early and accurate management of psychological distress in infertile patients is important to help improve their poor outcomes and increase the fertility rate. The results of this study will provide crucial information to better understand the psychological distress, potential classes, and influencing factors in infertility patients.
Trial Registration: Observational study, not applicable.
Keywords: infertility, psychological distress, latent transition analysis
Background
Infertility is defined as a condition in which a couple who are of childbearing age have been living together for more than 12 months and have had regular sexual intercourse without using any contraceptive measures for a year or more, yet have not been able to conceive successfully, which has been recognized by WHO as the third most serious health problem affecting human beings.1–4 The causes of infertility are diverse. Male infertility may stem from issues such as sperm dysplasia and sexual dysfunction, while female infertility can arise from conditions like pelvic damage and ovulation disorders.1,5,6 Additionally, emotional stress plays a significant role in contributing to infertility.7,8 Women’s emotional stress can be indicated by tubal spasms, anovulation, and vaginismus.9 According to recent studies, approximately 8.8% of women of reproductive age in the United States experienced infertility.10 Infertility is even more alarming in China; the prevalence of infertility has risen sharply, from 7.5% in 2007 to 18.2% in 2020, and currently affects about one in five couples of reproductive age.11 However, infertility is far more than a medical condition—it carries profound emotional and social implications. A long-term longitudinal study has shown that among women with primary or secondary infertility, half suffer from psychological distress, and the probability of such distress is even higher among women with primary infertility.12 Compared with women in the general population, women who have experienced infertility are 1.6 times more likely to suffer from psychological distress.8
Psychological distress is a common mental health problem that results from multiple factors causing an individual to experience unpleasant emotional states.13 It is a sub-health state that lies between normal psychological functioning and mental illness, often involving psychological, social, and spiritual dimensions. The psychological dimension includes depression, anxiety, obsessive-compulsive disorder, stress, and paranoia.10,12,14–18 The social dimension encompasses hostility and isolation.19,20 The spiritual dimension encompasses somatization symptoms and stigma.21–25 Studies have reported that the prevalence of depression in infertile patients is as high as 56%, and in studies of suicidal ideation, about 9.4% of women reported suicidal thoughts or attempts.26,27 Meanwhile, psychological distress problems such as stress, anxiety, stigma, obsessive-compulsive, sleep disturbances, and social isolation were more severe than those of women in general.28–30 In addition, the psychological distress caused by infertility further undermines women’s work efficiency, leading to an increase in absenteeism and missed working hours.31,32 It may also trigger domestic violence incidents and potentially result in marital breakdowns, among other consequences.33–35 In summary, given the complexity and specificity of psychological distress in infertility patients, early and precise identification of their psychological distress and individualized management occupy a crucial position in both clinical practice and the patients’ recovery process.
Studies have shown that psychological intervention can alleviate psychological distress and increase the pregnancy rate.36–38 However, research related to the psychological distress of patients with infertility is confronting a series of formidable challenges: firstly, extant studies tend to focus on the overall impact of anxiety and depression on psychological distress in infertility patients, and anxiety and depression as a part of psychological distress cannot be measured comprehensively.12,39,40 Secondly, the large individual differences and the existence of large heterogeneity lead to different emotional support needs by infertility patients. Finally, high-intensity and continuous psychological distress can lead to the further aggravation of psychological problems and trigger various types of psychological disorders, and there is a lack of longitudinal studies on the developmental pattern of psychological distress in infertility patients.40
In conclusion, it is important to explore longitudinal studies on the developmental patterns of psychological distress in infertility patients with a human-centred approach, to provide early and precise management of psychological distress, and thus to improve the poor outcomes and fertility of infertility patients.
Methods/Design
Study Aim
The objectives of this study are as follows in two phases (Figure 1):
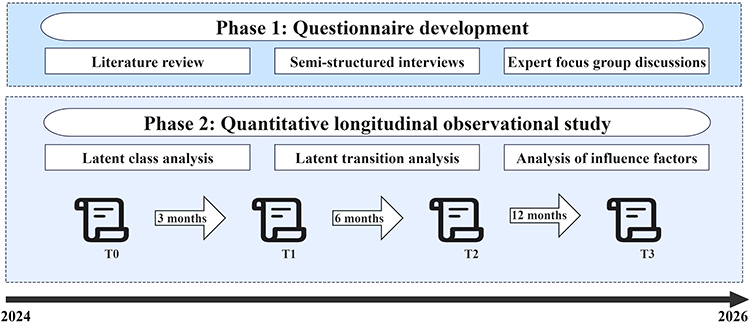 |
Figure 1 Research contents. |
Phase 1: Identify psychological distress dimensions and develop the questionnaire
- Through literature review, extract the psychological, social, and mental distress experiences of infertile patients, and initially summarize the core dimensions;
- Through semi-structured interviews, supplement and optimize the above dimensions and related social demographic indicators;
- Through expert focus group discussions, finally determine the structure of psychological distress dimensions. Subsequently, based on the identified dimensions, match existing mature scales to form the final questionnaire for investigating the psychological distress of infertile patients.
Phase 2: quantitative longitudinal observational study
- Evaluate the potential class of psychological distress in infertile patients;
- Evaluate the change of the latent classes over time (transformation) and influencing factors of psychological distress in infertile patients;
Study Design
This protocol describes an observational study consisting of two parts (subprojects).
As the first part, a literature review, semi-structured interviews and expert focus group discussions will be conducted within six months to develop a questionnaire for investigating the psychological distress of infertile patients.
As the second part, a quantitative longitudinal observational study will be conducted at three measurement points (month 3, month 6, and month 12) within 12 months. This is an example of an LTA for two time points. u11-u15 represent the 5 psychological disturbances at time point 1, and u21-u25 represent those at time point 2 (Figure 2).
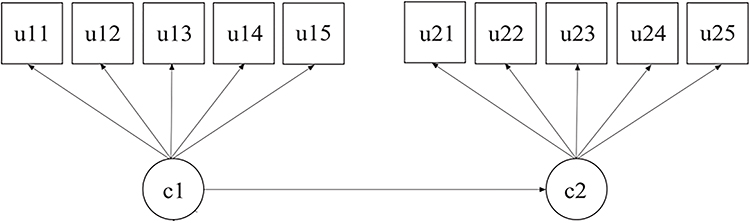 |
Figure 2 LTA model diagram. |
As the third part, the final formed scale was used for a pilot testing to examine the comprehensibility, acceptability, and completion time of the questionnaire, evaluate the response distribution of each item (identifying low-variability items), test the stability of the data collection process, and provide a basis for optimizing the formal survey process.
Study Setting
This research will be conducted at the Affiliated Hospital of Zunyi Medical University in Zunyi City, Guizhou Province. This is a tertiary general hospital with 2800 beds, and its annual outpatient volume exceeds 2 million visits. An average of 200 to 300 infertility patients are seen each month in the Obstetrics and Gynecology and Reproductive Center outpatient clinics, which provides the required sample size for this study.
Participants and Eligibility Criteria
Infertility patients attending the outpatient clinic of the Affiliated Hospital of Zunyi Medical University between September 2024 and December 2025 will be selected as potential study subjects using a consecutive enrollment method, and the final participants will be determined based on the inclusion and exclusion criteria. All the follow-up visits will be completed by December 2026.
Inclusion Criteria
① Patients diagnosed with infertility by outpatient physicians: ② Age is 18–40 years old; ③ Vital signs are stable, able to understand and cooperate with the investigation. ④ Voluntary participation in this study.
Exclusion Criteria
① serious insufficiency of the heart, liver, kidney, and other organs and suffering from malignant tumors; ② serious aphasia and cognitive dysfunction; ③ being involved in other research topics.
Study Instruments
General Demographic Data
The general demographic data of the research subjects, including names, ages, educational levels, family incomes, etc, were collected by the researchers through the design of a general data questionnaire.
Distress Thermometer (DT)
The Distress Thermometer (DT) is used to assess patients’ psychological distress. It consists of a single-item scale ranging from 0 (no distress) to 10 (extreme distress) and a 34-item Problem List (PL), which is divided into five subcategories: physical, emotional, family, practical, and spiritual/religious. The current measurement evaluation of the psychological distress thermometer indicates that a cut-off point of 4 yields the best sensitivity and specificity, and in the present study, a score of DT ≥ 4 was considered to be significantly psychologically distressing. The Chinese version of the DT has demonstrated high test-retest reliability (r = 0.800, p < 0.01).41
Self-Rating Depression Scale (SDS)
The SDS is used to assess depressive symptoms.36 This scale consists of 20 items and employs a 4-point Likert scale for scoring, ranging from 1 (almost never or rarely) to 4 (most of the time). The total score is used to evaluate the severity of depressive symptoms.
Beck Depression Inventory (BDI)
This scale is a 21-item self-report scale used to measure the presence and severity of depression.42 Each item is scored from 0 to 3; the total score ranges from 0 to 63 and is calculated by adding up the scores of each item. Depression was defined as a score of more than 16.
Infertility Stigma Scale (ISS)
The ISS is used to assess patients’ sense of stigma. This scale consists of 4 factors (self-deprecation, social withdrawal, public stigma, and family stigma) and 27 items. The Cronbach’s alpha coefficient, split-half coefficient, and test-retest correlation coefficient of the entire scale are 0.94, 0.90, and 0.91, respectively, demonstrating good reliability.43
Penn State Worry Questionnaire (PSWQ)
PSWQ is a measure of worry phenomena and has been demonstrated to be valid in cross-cultural populations. PSWQ has 16 items, and each item is rated on a scale from 1 (“not at all typical of me”) to 5 (“very typical of me”). The Chinese version of PSWQ and its factors evidenced good internal consistency and both convergent and discriminant validity.44
Data Collection
Two uniformly trained researchers identified potential subjects based on inclusion and exclusion criteria. First, one researcher guided the participants in groups to a quiet room in the clinic where they could talk and collect information. Another researcher introduced and explained the main purpose, significance, and implementation of the study to the study participants on a one-on-one basis and signed an informed consent form with the consent of the study participants. At the same time, the subjects completed the baseline data collection in the outpatient classroom, and the whole process was expected to take about 1 hour. After the completion of the baseline data, the researcher will conduct the subsequent 3 surveys and instruct them to fill in the online form at the corresponding time points. After the completion of data collection, the collected data were saved in the background and extracted into an Excel file. When all the data collection was completed, two researchers independently extracted and entered the data, cross-checked the data, and negotiated to resolve any differences. This study commits to adhering to privacy protection principles and strictly keeping the information of the participants confidential. Moreover, participants cannot view each other’s answers.
Quality Control
- The screening process will strictly follow the inclusion and exclusion criteria, and informed consent will be signed before completing the questionnaire.
- Before conducting the formal study, researchers will receive standardized training to ensure the objectivity and accuracy of the survey data.
- Before conducting the survey, the researchers will introduce the content of the questionnaire and the precautions to the participants. To ensure that the participants understand the content, the researcher will explain it in a consistent language and avoid the use of leading words.
- The questionnaire must be filled out completely, without omitting anything. The questionnaire will be checked immediately after completion to ensure the completeness of the information and the accuracy of the responses, and will be verified and corrected if necessary.
- The data obtained will be double-entered and checked to ensure the accuracy of the data.
Sample Size and Calculation
Based on the prevalence of infertility (18.2%), the sample size calculation formula for a cross-sectional study was adopted n=Z2α/2×p×(1−p)/d2, with a 95% confidence level (Z = 1.96) and a 5% allowable error (d=0.05). The required sample size was calculated to be n = 229. Taking into account a 30% dropout rate during the follow-up process, the final sample size was determined to be n = 229 / (1–0.3) ≈ 327.
Statistical Analysis Methods
The social demographic data of the patients were described, analyzed, and preprocessed using SPSS 27.0 software. LCA and LTA were conducted using Mplus 8.3. Firstly, DT, SDS, BDI, ISS, and PSWQ will be included as different psychological distress dimensions in the LCA model to identify different subtypes of psychological distress. The LCA process included model parameterization, parameter estimation, model evaluation, latent classification, and result interpretation. Then, based on the results of the LCA model, we will use the LTA model to study how individuals transition between potential classes at different time points. LTA is an extension of longitudinal data LCA. LTA uses transformation matrices to depict its stability from a probabilistic perspective by describing the unchanged probability of an individual belonging to a certain potential class. It also describes its development trend through transformation probabilities to obtain the development trajectory. The Akaike information criterion (AIC), Bayesian information criterion (BIC), and sample-corrected Bayesian information criterion (aBIC) were used to evaluate the fit of the LTA model, the accuracy of class division was evaluated using Entropy, and the differences in model fit were compared using the likelihood ratio test [Lo-Mendell-Rubin (LMR)] and the bootstrap likelihood ratio test (BLRT). Finally, a multivariate logistic regression analysis was conducted to determine the influencing factors of psychological distress in infertile patients. Here, the latent class of psychological distress in infertile patients was taken as the dependent variable, and relevant covariates were included based on the theoretical framework.
Discussion
Despite the general consensus on the psychological distress caused by infertility, there is still a lack of understanding of the types of psychological distress presented by infertility patients after diagnosis and their dynamic patterns of evolution. In particular, there is a lack of in-depth exploration of how the categories of psychological distress change over time, how they affect treatment compliance and outcomes, and the underlying driving mechanisms.
This study focuses on filling several key gaps in the current research field. Firstly, through systematic literature review and in-depth qualitative research, it comprehensively captures the subjective experiences of psychological distress among infertile patients and the contextual factors they are exposed to. Based on this, LCA was applied to accurately identify potential classes of psychological distress in infertility patients, and to deeply reveal the differentiated needs characteristics of patients in different psychological distress subgroups. This research approach aims to provide a solid scientific basis for developing highly personalized and precise psychological support intervention measures, thereby enhancing the effectiveness and targeting of psychological support.
Secondly, this study adopts a longitudinal research design to dynamically track the evolution process of psychological distress classes in infertile patients, and deeply explore the possible transformation patterns and internal mechanisms that may occur at different time points. This design helps to reveal the time-dependent characteristics of psychological distress development and provides a new perspective for understanding the dynamic changes of psychological distress.
Finally, this study intends to combine the multivariate Logistic regression analysis method to systematically analyze the multidimensional factors that influence the probability of class transformation of psychological distress in infertile patients, including individual characteristics, environmental factors, etc. Through quantitative analysis, the specific impact direction and degree of each factor on the class transformation will be clarified, providing theoretical support and practical guidance for formulating more precise and effective psychological intervention strategies in clinical practice, and thereby promoting the innovation and development of psychological support methods and contents for infertility.
A comprehensive understanding of the changing process of the potential classes of psychological distress in infertility over time is important for developing personalized psychological intervention plans that meet the unique needs of infertile patients. By deeply understanding the characteristics and needs of patients in different potential classes, we can develop more targeted psychological support strategies to improve patients’ coping ability and psychological resilience, which in turn will enhance patients’ treatment experience, reduce the dropout rate, and promote the care of psychological distress in infertility from “empirical comfort” to a new stage of “evidence-based, precise, and relational orientation”. From a broader practical perspective, revealing the mechanism of psychological distress transformation helps encourage patients to actively seek psychological support and medical services, promotes the formation of a supportive medical environment, and ultimately improves the physical and mental rehabilitation outcomes and quality of life of patients. Notably, due to social biases and traditional expectations of male roles, the psychological stress caused by male infertility has also not received the attention it deserves.45,46 Future research could also focus on its unique patterns of psychological distress, such as shame, social withdrawal, or performance anxiety, in order to promote intervention measures for both spouses and to eliminate the stigmatization associated with infertility, as infertility is a shared challenge for couples.
Abbreviations
LCA, Latent class analysis; LTA, Latent transition analysis; WHO, World Health Organization.
Ethics and Consent to Participate
The research protocol and questionnaire was approved by the Institutional Ethical Review Board at the Affiliated Hospital of Zunyi Medical University (KLL-2024-498) in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Author Contributions
Study design: Ying Liu, JiHua Fan, Xin Yan. Data collection: FengJuan Wu, BingYu li, Guo Li, JiaYi An. Data analysis: Ying Liu, MiaoMiao Yi, JiaYi Yu. Manuscript writing: Ying Liu, JiHua Fan, Xin Yan. Ying Liu and JiHua Fan contributed equally to this work and share first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was supported by a grant from the Zunyi Science and Technology and Big Data Bureau, Guizhou Province, China (Zun Shi Ke He HZ Zi (2023) No. 290).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Faso C. Infertility. Prim Care. 2025;52(2):307–8. doi:10.1016/j.pop.2025.01.004
2. Carson SA, Kallen AN. Diagnosis and management of infertility: a review. JAMA. 2021;326(1):65–76. doi:10.1001/jama.2021.4788
3. World Health Organization. Infertility Prevalence Estimates: 1990–2021. 2023.
4. Practice Committee of the American Society for Reproductive Medicine, American Society for Reproductive Medicine. Definition of infertility: a committee opinion. Fertil Sterility. 2023;120(6):1170. doi:10.1016/S0015-0282(23)01971-4
5. Eisenberg ML, Esteves SC, Lamb DJ, et al. Male infertility. Nat Rev Dis Primers. 2023;9(1):49. doi:10.1038/s41572-023-00459-w
6. Phillips K, Olanrewaju RA, Omole F. Infertility: evaluation and Management. Am Fam Physician. 2023;107(6):623–630.
7. Negris O, Lawson A, Brown D, et al. Emotional stress and reproduction: what do fertility patients believe? J Assist Reprod Genet. 2021;38(4):877–887. doi:10.1007/s10815-021-02079-3
8. Nik Hazlina NH, Norhayati MN, Shaiful Bahari I, et al. Worldwide prevalence, risk factors and psychological impact of infertility among women: a systematic review and meta-analysis. BMJ Open. 2022;12(3):e057132. doi:10.1136/bmjopen-2021-057132
9. Vander Borght M, Wyns C. Fertility and infertility: definition and epidemiology. Clin Biochem. 2018;62:2–10. doi:10.1016/j.clinbiochem.2018.03.012
10. Centers for Disease Control and Prevention.
11. Qiao J, Wang Y, Li X, et al. A Lancet Commission on 70 years of women’s reproductive, maternal, newborn, child, and adolescent health in China. Lancet. 2021;397(10293):2497–2536. doi:10.1016/S0140-6736(20)32708-2
12. Bagade T, Thapaliya K, Breuer E, et al. Investigating the association between infertility and psychological distress using Australian Longitudinal Study on Women’s Health (ALSWH). Sci Rep. 2022;12(1):10808. doi:10.1038/s41598-022-15064-2
13. Abu-Odah H, Molassiotis A, Zhao IY, et al. Psychological distress and associated factors among Palestinian advanced cancer patients: a cross-sectional study. Front Psychol. 2022;13:1061327. doi:10.3389/fpsyg.2022.1061327
14. Fernandez RS, Crivelli L, Guimet NM, et al. Psychological distress associated with COVID-19 quarantine: latent profile analysis, outcome prediction and mediation analysis. J Affect Disord. 2020;277:75–84. doi:10.1016/j.jad.2020.07.133
15. Simionescu G, Doroftei B, Maftei R, et al. The complex relationship between infertility and psychological distress (Review). Exp Ther Med. 2021;21(4):306. doi:10.3892/etm.2021.9737
16. Omani-Samani R, Ghaheri A, Navid B, et al. Prevalence of generalized anxiety disorder and its related factors among infertile patients in Iran: a cross-sectional study. Health Qual Life Outcomes. 2018;16(1):129. doi:10.1186/s12955-018-0956-1
17. Maroufizadeh S, Navid B, Omani-Samani R, et al. The effects of depression, anxiety and stress symptoms on the clinical pregnancy rate in women undergoing IVF treatment. BMC Res Notes. 2019;12(1):256. doi:10.1186/s13104-019-4294-0
18. Song D, Jiang W, Hu S, et al. Identification of psychological symptom clusters and their influencing factors in women undergoing assisted reproductive technology in China: a cross-sectional study. Int J Womens Health. 2024;16:1493–1504. doi:10.2147/IJWH.S468644
19. Nakkas C, Annen H, Brand S. Psychological distress and coping in military cadre candidates. Neuropsychiatr Dis Treat. 2016;12:2237–2243. doi:10.2147/NDT.S113220
20. Wright J, Duchesne C, Sabourin S, et al. Psychosocial distress and infertility: men and women respond differently. Fertil Sterility. 1991;55(1):100. doi:10.1016/S0015-0282(16)54067-9
21. Scocco P, Preti A, Totaro S, et al. Stigma and psychological distress in suicide survivors. J Psychosom Res. 2017;94:39–46. doi:10.1016/j.jpsychores.2016.12.016
22. Yokota R, Okuhara T, Okada H, Goto E, Sakakibara K, Kiuchi T. Association between stigma and anxiety, depression, and psychological distress among Japanese women undergoing infertility treatment. Healthcare. 2022;10(7):1300.
23. Peterson B, Taubman-Ben-Ari O, Chiu B, et al. Infertility stigma and openness with others are related to depressive symptoms and meaning in life in men and women diagnosed with infertility. Reprod Health. 2025;22(1):7. doi:10.1186/s12978-025-01951-0
24. Oti-Boadi M, Oppong Asante K. Psychological health and religious coping of Ghanaian women with infertility. Biopsychosoc Med. 2017;11(1):20–27. doi:10.1186/s13030-017-0105-9
25. Cattaneo Della Volta MF, Vallone F, Dolce P, et al. Psychological health conditions of ART treated infertile couples: a 4-years prospective study. Front Psychol. 2025;16:1616754. doi:10.3389/fpsyg.2025.1616754
26. Pasch LA, Holley SR, Bleil ME, et al. Addressing the needs of fertility treatment patients and their partners: are they informed of and do they receive mental health services? Fertil Steril. 2016;106(1):209–215.e2. doi:10.1016/j.fertnstert.2016.03.006
27. Shani C, Yelena S, Reut BK, et al. Suicidal risk among infertile women undergoing in-vitro fertilization: incidence and risk factors. Psychiatry Res. 2016;240:53–59. doi:10.1016/j.psychres.2016.04.003
28. Salari N, Babajani F, Hosseinian-Far A, et al. Global prevalence of major depressive disorder, generalized anxiety, stress, and depression among infertile women: a systematic review and meta-analysis. Arch Gynecol Obstet. 2024;309(5):1833–1846. doi:10.1007/s00404-024-07444-y
29. Foti FL, Karner-Hutuleac A, Maftei A. The value of motherhood and psychological distress among infertile women: the mediating role of coping strategies. Front Public Health. 2023;11:1024438. doi:10.3389/fpubh.2023.1024438
30. Rooney KL, Domar AD. The relationship between stress and infertility. Dialogues Clin Neurosci. 2018;20(1):41–47. doi:10.31887/DCNS.2018.20.1/klrooney
31. Payne N, Seenan S, van den Akker O. Experiences and psychological distress of fertility treatment and employment. J Psychosom Obstet Gynaecol. 2019;40(2):156–165. doi:10.1080/0167482X.2018.1460351
32. Gremillet L, Netter A, Sari-Minodier I, et al. Endometriosis, infertility and occupational life: women’s plea for recognition. BMC Womens Health. 2023;23(1):29. doi:10.1186/s12905-023-02183-9
33. Stellar C, Garcia-Moreno C, Temmerman M, et al. A systematic review and narrative report of the relationship between infertility, subfertility, and intimate partner violence. Int J Gynaecol Obstet. 2016;133(1):3–8. doi:10.1016/j.ijgo.2015.08.012
34. Wang K, Li J, Zhang JX, Zhang L, Yu J, Jiang P. Psychological characteristics and marital quality of infertile women registered for in vitro fertilization-intracytoplasmic sperm injection in China. Fertil Steril. 2007;87(4):792–798. doi:10.1016/j.fertnstert.2006.07.1534
35. Dube L, Nkosi-Mafutha N, Balsom AA, et al. Infertility-related distress and clinical targets for psychotherapy: a qualitative study. BMJ Open. 2021;11(11):e050373. doi:10.1136/bmjopen-2021-050373
36. Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi:10.1016/S0033-3182(71)71479-0
37. Katyal N, Poulsen CM, Knudsen UB, et al. The association between psychosocial interventions and fertility treatment outcome: a systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2021;259:125–132. doi:10.1016/j.ejogrb.2021.02.012
38. Ying L, Wu LH, Loke AY. The effects of psychosocial interventions on the mental health, pregnancy rates, and marital function of infertile couples undergoing in vitro fertilization: a systematic review. J Assist Reprod Genet. 2016;33(6):689–701. doi:10.1007/s10815-016-0690-8
39. Cao D, Bai C, Zhang G. Psychological distress among infertility patients: a network analysis. Front Psychol. 2022;13:906226. doi:10.3389/fpsyg.2022.906226
40. Hecht LM, Joseph-Mofford G, Iacobelli R, et al. Anxiety, depression, and infertility-specific distress among women with female factor infertility. J Health Psychol. 2024:13591053241235092. doi:10.1177/13591053241235092
41. Tang L, Zhang Y-N, Pang Y, et al. Validation and reliability of distress thermometer in Chinese cancer patients. Chin J Cancer Res. 2011;23(1):54–58. doi:10.1007/s11670-011-0054-y
42. Beck AT, Steer RA, Ball R, Ranieri WF. Comparison of beck depression Inventories-IA and-II in psychiatric outpatients. J Pers Assess. 1996;67(3):588–597. doi:10.1207/s15327752jpa6703_13
43. Fu B, Qin N, Cheng L, et al. Development and validation of an Infertility Stigma Scale for Chinese women. J Psychosom Res. 2015;79(1):69–75. doi:10.1016/j.jpsychores.2014.11.014
44. Zhong J, Wang C, Li J, et al. Penn State Worry Questionnaire: structure and psychometric properties of the Chinese version. J Zhejiang Univ Sci B. 2009;10(3):211–218. doi:10.1631/jzus.B0820189
45. Barone B, Amicuzi U, Tammaro S, et al. Male infertility: a comprehensive review of urological causes and contemporary management. J Clin Med. 2026;15(1):397. doi:10.3390/jcm15010397
46. Napolitano L, Barone B, Crocetto F, Capece M, La Rocca R. The COVID-19 pandemic: is it a wolf consuming fertility? Int J Fertil Steril. 2020;14(2):159–160.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychological Distress, Dyadic Coping, and Quality of Life in Infertile Clients Undergoing Assisted Reproductive Technology in China: A Single-Center, Cross-Sectional Study
Bai J, Zheng J, Dong Y, Wang K, Cheng C, Jiang H
Journal of Multidisciplinary Healthcare 2022, 15:2715-2723
Published Date: 29 November 2022