Back to Journals » Breast Cancer: Targets and Therapy » Volume 10
A single-nucleotide polymorphism of the beta 2-adrenergic receptor gene can predict pathological complete response to taxane- and platinum-based neoadjuvant chemotherapy in breast cancer
Authors Du Y, Yan T, Zhou L ![]() , Yin W, Lu J
, Yin W, Lu J ![]()
Received 29 September 2018
Accepted for publication 6 November 2018
Published 27 November 2018 Volume 2018:10 Pages 201—206
DOI https://doi.org/10.2147/BCTT.S189197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Yueyao Du,* Tingting Yan,* Liheng Zhou, Wenjin Yin, Jinsong Lu
Department of Breast Surgery, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai 200127, China
*These authors contributed equally to this work
Background: Germline genetic polymorphisms in certain genes are associated with the response to anthracycline- and taxane-based neoadjuvant chemotherapy in breast cancer (BC). This translational study aims to evaluate the potential role of rs1042713 in the beta 2-adrenergic receptor (ADRB2) gene in predicting pathological complete responses (pCRs) to taxane- and platinum-based neoadjuvant chemotherapy in locally advanced breast cancer (LABC).
Materials and methods: The distribution frequencies of rs1042713 were genotyped in LABC patients who received taxane- and platinum-based neoadjuvant chemotherapy. Associations between tumor-relevant biomarkers, genotypes and pCRs were evaluated using Student’s t-test for continuous variables and Chi-square or Fisher’s exact test for categorical variables. For univariate analysis, the relationship between the rs1042713 polymorphism and pCR was analyzed by Chi-square or Fisher’s exact test. The modified ORs with their 95% CIs were calculated by a multivariate logistic regression analysis to explore the association between genotype and pCR.
Results: There was a significant correlation of the rs1042713 genotype with estrogen receptor (ER) status (P=0.008). Significant differences were detected in the rs1042713 genotypes of pCR and non-pCR patients (P=0.046). The pCR rate was 18.2% in patients with ADRB2 rs1042713 AA genotypes and 38.7% in AG+GG genotypes. Women carrying the AG+GG (OR=2.91, 95% CI: 1.02–8.29, P=0.046) genotype had a higher pCR rate than those with the AA genotype.
Conclusion: rs1042713, which is located in the ADRB2 gene, could predict pCR to taxane- and platinum-based neoadjuvant chemotherapy in LABC. This finding suggests that rs1042713 could play a potential role as a predictive marker in clinical settings.
Keywords: beta 2-adrenergic receptor gene, locally advanced breast cancer, neoadjuvant chemotherapy, pathological complete response, polymorphism
Introduction
Neoadjuvant chemotherapy is a widely accepted treatment modality in women with newly diagnosed early breast cancer (BC), especially in locally advanced breast cancer (LABC).1,2 Neoadjuvant chemotherapy helps reduce tumor volume, thus enabling more patients to receive breast-conserving surgery. In addition, it offers the opportunity to assess tumor response in the resection specimen.3 Pathological complete response (pCR) is defined as the absence of invasive cancer. Previous studies have demonstrated that pCR after neoadjuvant chemotherapy is associated with better long-term survival.4–6 Among women who receive neoadjuvant chemotherapy, the clinical response rate is up to 70%, but only ~15%–30% of patients achieve pCR.1,2,7 Novel predictive biomarkers that can predict tumor response prior to the initiation of chemotherapy are valuable in making individualized treatment decisions and maximizing efficacy in cancer patients. Germline genetic polymorphisms include minor changes in DNA sequences that can modify the structure, expression or activity of the proteins encoded by genes.8 Previous research has demonstrated that germline genetic polymorphisms located in WT1, IGF1R, MDM2 and CD24 genes are associated with a response to anthracycline- and taxane-based neoadjuvant chemotherapy in BC.3,9–11
ADRB2 is localized to the 5q32 chromosomal region. The encoded protein, the beta 2-adrenergic receptor, is a member of the G protein-coupled receptor superfamily.12 The association between polymorphisms in the ADRB2 genes and the risk of several diseases has been previously studied. Different polymorphic forms, point mutations, and/or downregulation of this gene are associated with nocturnal asthma, obesity, and type 2 diabetes.12–15 Huang et al demonstrated that the presence of the 27Glu (rs1042714) mutation in ADRB2 or the 64Arg mutation in ADRB3 (rs4994) was associated with a decreased risk for BC, especially when both mutations were present.16 rs1042713 is an A/G single-nucleotide variation at nucleotide position 46 in the ADRB2 gene (AGA to GGA). The mutation substitutes the 16th amino acid of the translated protein chain from arginine to glycine. It is still unclear whether this polymorphism in the ADRB2 gene has a predictive role in response to neoadjuvant chemotherapy in LABC.
ADRB2 is one of the target genes of the microRNA (miRNA) let-7 family.17 It has been reported that resistance to paclitaxel and cisplatin is partly mediated by miRNA let-7.18 We hypothesized that rs1042713 in the ADRB2 gene could predict response to taxane- and platinum-based neoadjuvant chemotherapy in BC. In this translational study, we identified the single-nucleotide polymorphism (SNP) in the rs1042713 mutation from participants of two prospective studies in which patients received weekly paclitaxel and cisplatin as neoadjuvant chemotherapy.
Materials and methods
Study populations
From October 2013 until November 2016, 130 patients with LABC were recruited for this study. The inclusion criteria were females between the ages of 18 and 70 years with histologically confirmed but untreated large operable BC (T size ≥2 cm and N0-2). Patients who suffered from other malignancies were excluded. Other inclusion and exclusion criteria have been described elsewhere.19 Patients enrolled in this study were participants from two open-label, prospective trials (SHPD001 and SHPD002). All participants from the two trials who were willing to take part in this study and provide informed consent were enrolled in this study. SHPD001 (NCT02199418) was a Phase II study evaluating weekly treatment with paclitaxel in combination with cisplatin as neoadjuvant therapy for LABC patients. SHPD002 (NCT0222199) is a prospective, randomized, open-label study comparing preoperative weekly treatment with paclitaxel and cisplatin with or without endocrine therapy in patients with operable hormone receptor-positive and triple-negative LABC. In these two trials, patients were scheduled to receive intravenous weekly infusions of 80 mg/m2 paclitaxel on day 1 for 16 weeks and 25 mg/m2 cisplatin on days 1, 8 and 15, every 28 days. Patients with HER2-positive cancer were allowed to use concomitant trastuzumab on a weekly basis. Written informed consent was obtained from each subject. For each subject, a 5 mL peripheral blood sample was collected and stored at –80°C. DNA was extracted from the peripheral blood samples of all subjects using Qiagen DNA blood kits (Qiagen NV, Venlo, the Netherlands) according to the manufacturer’s protocol. This study was approved by the ethics committee of Renji Hospital, Shanghai Jiao Tong University. This study was conducted in accordance with the Declaration of Helsinki. Among the 130 patients in this study, 97 (74.6%) were estrogen receptor (ER)-positive and 33 (25.4%) were ER-negative.
Histopathologic response
pCR was evaluated in surgical specimens following chemotherapy and defined as the absence of invasive cancer in the breast, with or without residual noninvasive intraductal carcinoma. All cases with residual invasive cancer of any size were classified as non-pCR.
Selection of SNP in ADRB2 gene
SNPs of the ADRB2 gene were surveyed in the NCBI-dbSNP (www.ncbi.nlm.nih.gov/SNP/) and Hapmap (www.hapmap.org) databases. These databases have genotyped a large number of SNPs in different populations and have provided a set of tag SNPs (tSNPs) representing evolutionally linked genetic variants.20 Using the SNPbrowser™ v4.0 software developed by ABI Company, we selected one tSNP (rs1042713) from the exon of the ADRB2 gene.
SNP genotyping
SNP genotyping was performed at Shanghai Bene-gene Biotechnology Co., Ltd. (Shanghai, China), using the MassARRAY system (Sequenom, San Diego CA, USA) by matrix-assisted laser desorption ionization-time of flight (MALDI-TOF) mass spectrometry. Detailed information on the primer is shown in Table 1.
 | Table 1 Detailed information of primers in the study Abbreviation: SNP, single-nucleotide polymorphism. |
Statistical analyses
Genotype distributions were tested for adherence to the Hardy–Weinberg equilibrium (HWE). Associations between tumor-relevant biomarkers, genotype and pCR were evaluated using Student’s t-test for continuous variables and Chi-square or Fisher’s exact test for categorical variables. The relationship between the rs1042713 polymorphism and pCR was analyzed by Chi-square or Fisher’s exact test. Modified ORs with 95% CIs were calculated by univariate and multivariate logistic regression analyses to explore the association between genotype and pCR. All statistical analyses were conducted with Stata 14.0 (StataCorp LP, College Station, TX, USA).
Results
Associations of genotype with clinicopathologic parameters
The genotypic distribution for rs1042713 was tested for deviation from HWE and showed no deviation (data not shown). There was a correlation between the rs1042713 genotypes and the clinicopathologic parameters of primary BC. There was a significant correlation between the codominant model of the rs1042713 genotype and ER status (P=0.008). In ER-positive BC, more women carried the AA genotype than the AG and GG genotypes, whereas in ER-negative BC, more women carried the AG genotype than the AA and GG genotypes. There were no significant correlations between the rs1042713 genotype and other clinicopathologic features, including age, menstrual status, PR and HER2 status. The detailed associations between the rs1042713 genotype and ER are shown in Table 2.
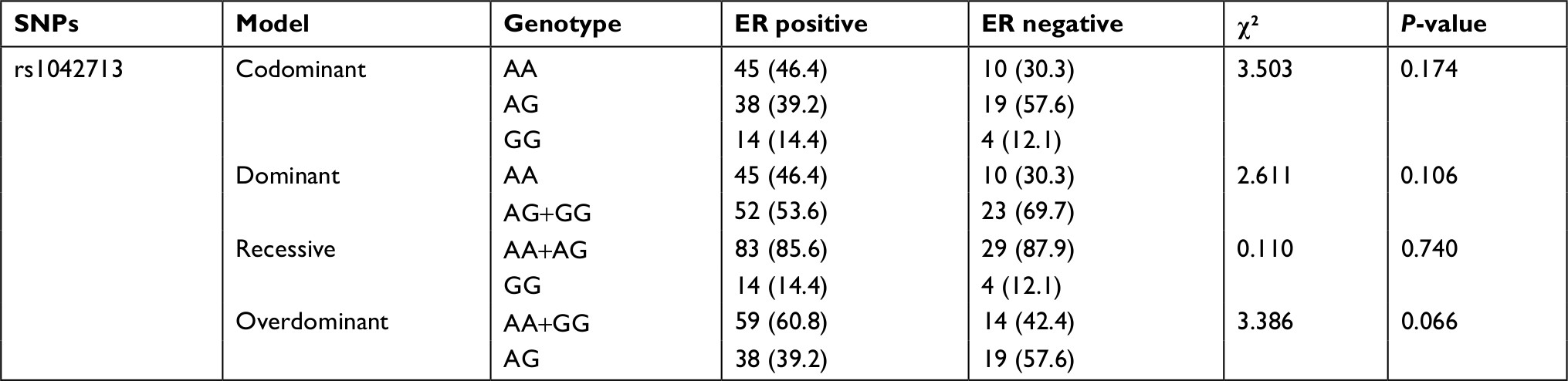 | Table 2 Associations between genotypes of rs1042713 and ER in patients with locally advanced breast cancer Abbreviations: ER, estrogen receptor; SNP, single-nucleotide polymorphism. |
Associations of genotype with response to neoadjuvant chemotherapy
Thirty-six out of 130 (27.7%) patients had pCR following neoadjuvant chemotherapy. The pCR rate was 18.2% in patients with the ADRB2 rs1042713 AA genotype, 38.6% and 38.9% in patients with the AG and GG genotypes, respectively, and 38.7% in patients with the AG+GG genotype. In the univariate analysis, significant differences were detected in the dominant model of rs1042713 between pCR and non-pCR patients (P=0.046). In the multivariate analysis, significant differences were detected in the dominant model of rs1042713 between these two groups (P=0.046). This finding suggests that the genotypes of this SNP are associated with response to neoadjuvant chemotherapy. Genotype distributions in the pCR and non-pCR patients are shown in Table 3. Women carrying the AG+GG (OR =2.91, 95% CI: 1.02–8.29, P=0.046) genotype of ADRB2 rs1042713 had a higher pCR rate than those carrying the AA genotype (Table 3). Further analysis showed that there were significant differences in rs1042713 between the pCR and non-pCR patients in luminal type (P=0.035) and HER2-positive breast cancers (P=0.045) (Figure 1).
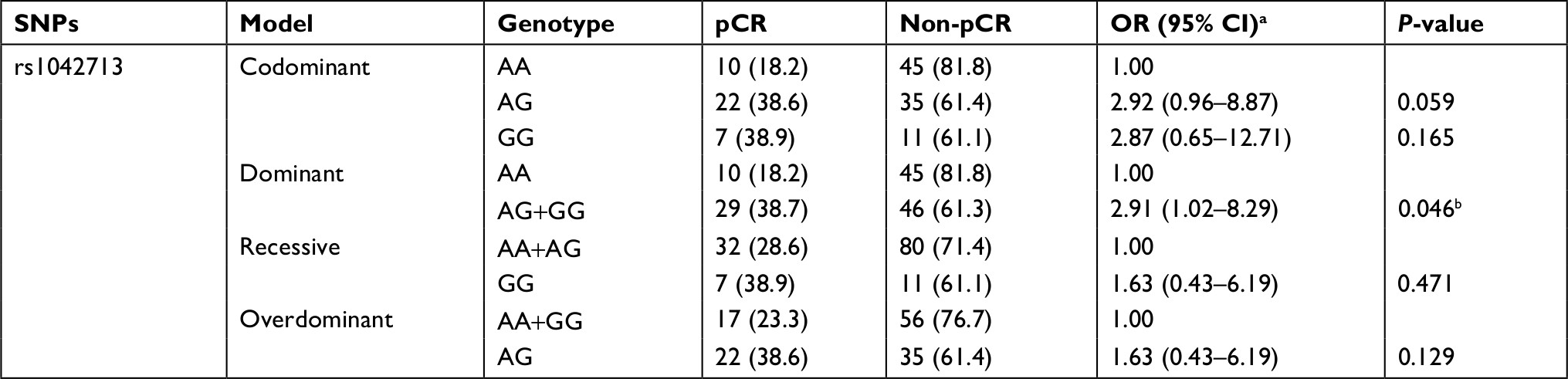 | Table 3 Associations between genotypes of rs1042713 and pCR after neoadjuvant chemotherapy in patients with locally advanced breast cancer Notes: aOR and 95% CI was analyzed by logistic regression and adjusted by age, menses status, ER, PR, and HER2 status. Common genotype was taken as reference. bP<0.05. Abbreviations: pCR, pathological complete response; SNP, single-nucleotide polymorphism. |
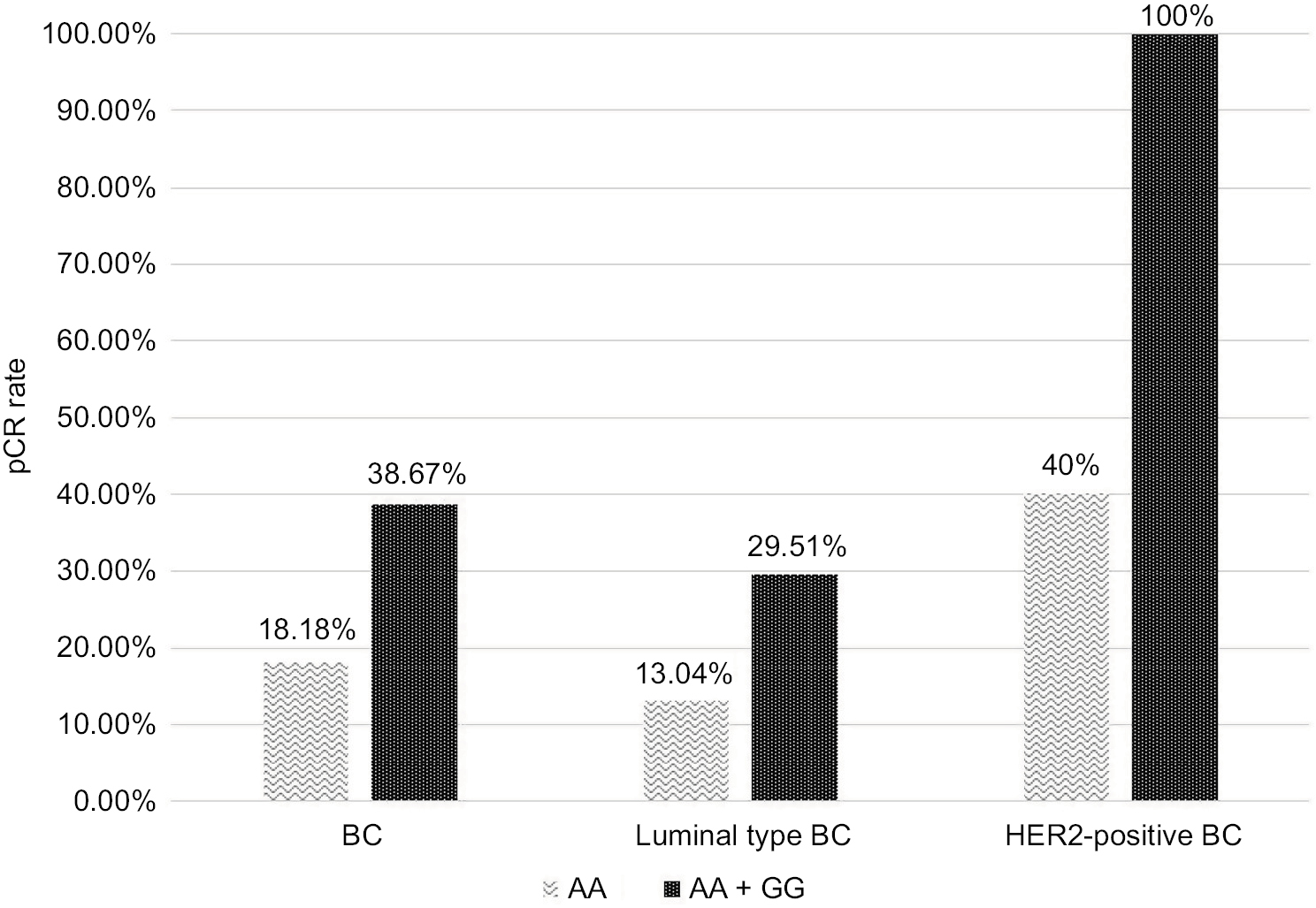 | Figure 1 The relationship between genotypes of rs1042713 and pCR in patients with BC, luminal type BC and HER2-positive BC. Abbreviations: BC, breast cancer; pCR, pathological complete response. |
Discussion
In this translational study, we report for the first time that ADRB2 rs1042713 could predict pCR to taxane- and platinum-based neoadjuvant chemotherapy in LABC, especially in luminal type and HER2-positive breast cancers. In the neoadjuvant setting, it is important to identify nonresponders to avoid ineffective treatments and provide alternative therapies such as surgery or switching to a noncross resistant chemotherapy regimen.
In this study, we showed that the ADRB2 rs1042713 genotypes were associated with ER status. Recent studies have found that similarities and interactions exist between the signaling pathways of ERs (ERα, ERβ, GPR30) and β adrenoceptors (β1, β2 and β3 adrenoceptors).21 GPR30, a recently discovered receptor, shares structural features with the β adrenoceptors. GPR30 has sites for protein kinase A phosphorylation, PDZ binding motifs, and interacts with A-kinase anchoring protein 5 (AKAP5), all of which enable its interaction with the β adrenoceptors pathways.21 Our previous study investigated the association between β2 adrenoceptor (encoded by the ADRB2 gene) and clinical outcomes in BC; we found that in hormone receptor-positive BC patients, strong β2 adrenoceptor expression was correlated with better disease-free survival than weak β2 adrenoceptor expression.22 These findings were consistent, indicating that there are interactions between ERs and β adrenoceptors that help coordinate one another.
Some studies have demonstrated that germline polymorphisms have an effect on patient response to therapy for malignant diseases.23–25 However, the association between polymorphisms in the ADRB2 gene and response to neoadjuvant chemotherapy in BC has not yet been reported. Our data showed that ADRB2 rs1042713 can predict pCR to taxane- and platinum-based neoadjuvant chemotherapy in BC. Wu et al used modified miRNA probes to detect let-7a via in situ hybridization in formalin-fixed and paraffin-embedded sections from BC patients who received epirubicin-based neoadjuvant chemotherapy; they found that lower let-7a expression was associated with epirubicin resistance in BC tumors.26 They also showed that let-7a upregulation in an epirubicin-resistant SK-3rd sphere cell line sensitized this cell line to epirubicin and upregulated let-7a expression, increasing the apoptotic cell population in the SK-3rd sphere cells compared to the negative control groups.26 Additionally, Wang et al found that the ADRB2 gene was a target of let-7f.17 Under static conditions, let-7f actively repressed translation and established basal levels of β2 adrenoceptor expression. During agonist activation of β2 adrenoceptor, let-7f levels decreased, resulting in depressed ADRB2 gene silencing and a subsequent attenuation of agonist-promoted downregulation of β2 adrenoceptor.17 As a downstream molecule of let-7, ADRB2 may be involved in the regulation of miRNAs in let-7-related gene networks. Finally, changes in the function of ADRB2 itself may also influence the regulation of the let-7 response to chemotherapy. The correlation between response to chemotherapy and miRNA in let-7-related gene networks will be further investigated in our future work.
We acknowledge that the present study has some limitations. The sample size of the patient cohort was small. Our findings indicate that the SNP ADRB2 rs1042713 was associated with response to neoadjuvant chemotherapy and may have a potential role as a predictive marker in clinical settings. However, we acknowledge that we did not investigate other SNPs located in the ADRB2 gene or miRNAs in the let-7-related gene networks.
Conclusion
The results of the present study showed that ADRB2 rs1042713 can predict pCR to taxane- and platinum-based neoadjuvant chemotherapy in LABC. A significant association was detected between the rs1042713 genotypes and ER status. Further work is needed to clarify the molecular mechanisms underlying this relationship.
Acknowledgments
This research is supported by grants from the National Natural Science Foundation of China (grant numbers 81172505 and 81302302), the Doctoral Programs Foundation of the Ministry of Education of China (grant number 20120071120105), the Shanghai Natural Science Foundation (grant number 13ZR1452800), the Shanghai Municipal Commission of Health and Family Planning (grant numbers 20144Y0218, 201640006), the Science and Technology Commission of Shanghai Municipality (grant number 14411950202), the Clinical Research Plan of SHDC (grant number SHDC 12016231), the Nurturing Fund of Renji Hospital 2016 (grant number PYMDT-002) and the Nurturing Fund of Renji Hospital 2015 (grant number RJZZ15-023). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Kaufmann M, von Minckwitz G, Mamounas EP, et al. Recommendations from an international consensus conference on the current status and future of neoadjuvant systemic therapy in primary breast cancer. Ann Surg Oncol. 2012;19(5):1508–1516. | ||
van der Hage JA, van de Velde CJ, Julien JP, Tubiana-Hulin M, Vandervelden C, Duchateau L. Preoperative chemotherapy in primary operable breast cancer: results from the European Organization for Research and Treatment of Cancer trial 10902. J Clin Oncol. 2001;19(22):4224–4237. | ||
de Groot S, Charehbili A, van Laarhoven HW, et al. Insulin-like growth factor 1 receptor expression and IGF1R 3129G > T polymorphism are associated with response to neoadjuvant chemotherapy in breast cancer patients: results from the NEOZOTAC trial (BOOG 2010-01. Breast Cancer Res. 2016;18(1):3. | ||
Liedtke C, Mazouni C, Hess KR, et al. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J Clin Oncol. 2008;26(8):1275–1281. | ||
Rastogi P, Anderson SJ, Bear HD, et al. Preoperative chemotherapy: updates of National Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27. J Clin Oncol. 2008;26(5):778–785. | ||
Guarneri V, Broglio K, Kau SW, et al. Prognostic value of pathologic complete response after primary chemotherapy in relation to hormone receptor status and other factors. J Clin Oncol. 2006;24(7):1037–1044. | ||
Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164–172. | ||
Vymetalkova V, Pardini B, Rosa F, et al. Polymorphisms in microRNA binding sites of mucin genes as predictors of clinical outcome in colorectal cancer patients. Carcinogenesis. 2017;38(1):28–39. | ||
Li MM, Shao YB, Liu H, Xu B, He BX. [Effect of single nucleotide polymorphisms of RS1799937 located in WT1 gene on the pathlogical complete response to neoadjuvant chemotherapy in breast cancer patients]. Zhonghua Yi Xue Za Zhi. 2016;96(44):3559–3562. Chinese. | ||
Le Morvan V, Litière S, Laroche-Clary A, et al. Identification of SNPs associated with response of breast cancer patients to neoadjuvant chemotherapy in the EORTC-10994 randomized phase III trial. Pharmacogenomics J. 2015;15(1):63–68. | ||
Marmé F, Werft W, Walter A, et al. CD24 Ala57Val polymorphism predicts pathologic complete response to sequential anthracycline- and taxane-based neoadjuvant chemotherapy for primary breast cancer. Breast Cancer Res Treat. 2012;132(3):819–831. | ||
Gu W, Liu J, Wang Z, Liu Y, Wen S. ADRB2 polymorphisms and dyslipidemia risk in Chinese hypertensive patients. Clin Exp Hypertens. 2017;39(2):139–144. | ||
Jean-Alphonse FG, Wehbi VL, Chen J, et al. β2-adrenergic receptor control of endosomal PTH receptor signaling via Gβγ. Nat Chem Biol. 2017;13(3):259–261. | ||
Kilpeläinen TO, Lakka TA, Laaksonen DE, et al. Interaction of single nucleotide polymorphisms in ADRB2, ADRB3, TNF, IL6, IGF1R, LIPC, LEPR, and GHRL with physical activity on the risk of type 2 diabetes mellitus and changes in characteristics of the metabolic syndrome: The Finnish Diabetes Prevention Study. Metabolism. 2008;57(3):428–436. | ||
Szendrei B, González-Lamuño D, Amigo T, et al. Influence of ADRB2 Gln27Glu and ADRB3 Trp64Arg polymorphisms on body weight and body composition changes after a controlled weight-loss intervention. Appl Physiol Nutr Metab. 2016;41(3):307–314. | ||
Huang XE, Hamajima N, Saito T, et al. Possible association of beta2- and beta3-adrenergic receptor gene polymorphisms with susceptibility to breast cancer. Breast Cancer Res. 2001;3(4):264–269. | ||
Wang WC, Juan AH, Panebra A, Liggett SB. MicroRNA let-7 establishes expression of beta2-adrenergic receptors and dynamically down-regulates agonist-promoted down-regulation. Proc Natl Acad Sci USA. 2011;108(15):6246–6251. | ||
Geretto M, Pulliero A, Rosano C, Zhabayeva D, Bersimbaev R, Izzotti A. Resistance to cancer chemotherapeutic drugs is determined by pivotal microRNA regulators. Am J Cancer Res. 2017;7(6):1350–1371. | ||
Zhou L, Xu S, Yin W, et al. Weekly paclitaxel and cisplatin as neoadjuvant chemotherapy with locally advanced breast cancer: a prospective, single arm, phase II study. Oncotarget. 2017;8(45):79305–79314. | ||
International HapMap Consortium. The International HapMap Project. Nature. 2003;426(6968):789–796. | ||
Machuki JO, Zhang HY, Harding SE, Sun H. Molecular pathways of oestrogen receptors and β-adrenergic receptors in cardiac cells: Recognition of their similarities, interactions and therapeutic value. Acta Physiol. 2018;222(2):e12978. | ||
du Y, Zhou L, Wang Y, et al. Association of alpha2a and beta2 adrenoceptor expression with clinical outcome in breast cancer. Curr Med Res Opin. 2014;30(7):1337–1344. | ||
Xu Y, Yao L, Ouyang T, et al. p53 Codon 72 polymorphism predicts the pathologic response to neoadjuvant chemotherapy in patients with breast cancer. Clin Cancer Res. 2005;11(20):7328–7333. | ||
Marmé F, Werft W, Benner A, et al. FGFR4 Arg388 genotype is associated with pathological complete response to neoadjuvant chemotherapy for primary breast cancer. Ann Oncol. 2010;21(8):1636–1642. | ||
Gréen H, Söderkvist P, Rosenberg P, Horvath G, Peterson C. mdr-1 single nucleotide polymorphisms in ovarian cancer tissue: G2677T/A correlates with response to paclitaxel chemotherapy. Clin Cancer Res. 2006;12(3 Pt 1):854–859. | ||
Wu J, Li S, Jia W, et al. Reduced Let-7a Is Associated with Chemoresistance in Primary Breast Cancer. PLoS One. 2015;10(7):e0133643. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.