Back to Journals » Vascular Health and Risk Management » Volume 19
A Scoping Review of Predictors Associated with Self-Efficacy Among Patients with Coronary Heart Disease
Authors Sugiharto F ![]() , Nuraeni A
, Nuraeni A ![]() , Trisyani Y
, Trisyani Y ![]() , Putri AM
, Putri AM ![]() , Armansyah NA, Zamroni AH
, Armansyah NA, Zamroni AH ![]()
Received 13 August 2023
Accepted for publication 4 November 2023
Published 9 November 2023 Volume 2023:19 Pages 719—731
DOI https://doi.org/10.2147/VHRM.S435288
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Harry Struijker-Boudier
Firman Sugiharto,1 Aan Nuraeni,2 Yanny Trisyani,2 Azalia Melati Putri,3 Nuraulia Aghnia Armansyah,3 Asroful Hulam Zamroni4
1Master Study Program Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 3Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 4Regional General Hospital Dr. Soetomo, Surabaya, East Java, Indonesia
Correspondence: Firman Sugiharto, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Ir. Soekarno KM. 21, Hegarmanah Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +6282218235600, Fax +6202287793411, Email [email protected]
Abstract: Self-efficacy (SE) is the main predictor of self-care behaviour in patients with coronary heart disease (CHD). Several studies identified factors that influence SE in CHD patients. However, review studies have yet to synthesize these results systematically. This review aims to identify SE and the factors influencing SE in CHD patients. This scoping review is reported based on the PRISMA Extension for Scoping Reviews (PRISMA-ScR). We searched using relevant keywords using five databases: CINAHL Plus with Full Text and Academic Search Complete, PubMed, ScienceDirect, Scopus, Taylor and Francis, and one search engine: Google Scholar, which was accessed on June 23, 2023. Articles with an observational design were included without date restrictions. The quality of evidence was assessed using the Joanna Briggs Institute critical appraisal checklist, and data synthesis used thematic analysis. We found 11 articles discussing SE and the factors influencing SE in CHD patients. In this review, most studies reported that the SE level of CHD patients tends to be low to moderate. Factors associated with SE in this population are classified into three categories (low, moderate, and high). Cardiac knowledge and patient activation are the most influential predictors of SE in CHD patients. Public health interventions such as raising awareness about heart disease, modifying health behaviours, early screening, diagnosis, and appropriate treatment are critical to improving SE and cardiac care outcomes.
Keywords: coronary heart disease, self-care, self-efficacy
Introduction
Coronary Heart Disease (CHD) is a health problem with high morbidity and mortality rates in various countries.1 In 2020, American Heart Association data shows that 244.1 million people worldwide suffer from CHD.2 In addition, from 2012 to 2022, 1.522.669 deaths related to heart disease, including CHD, occurred in the United States.2 Meanwhile, CHD cases in Indonesia have increased from 0.5% in 2013 to 1.5% in 2018.3 This death rate is expected to continue to increase to 24.2 million people in 2030.1
CHD is a non-communicable disease caused by coronary atherosclerosis, which results in stenosis and occlusion of the coronary artery lumen, resulting in insufficient blood supply to the heart.1 If this process lasts a long time, it can cause cardiac ischemia, myocardial infarction, and the risk of death.4 This situation requires revascularization as soon as possible to restore blood flow and myocardial reperfusion.5
The increase in CHD mortality and morbidity goes hand in hand with poor quality of life (QoL) and self-efficacy (SE).6 Patients with CHD experience a decline in their physical and psychological health status, so they need a high SE to support the management and control of self-care behaviour until the end of their lives.7–9 SE is an individual’s belief about a person’s ability to organize and carry out certain activities.10
SE has an essential role in managing CHD and reducing risk factors.11–13 SE is essential in initiating and maintaining healthy behaviours, leading to reduced recurrence of cardiac events.14 CHD patients with high SE rates will have good disease management, increased psychological well-being and quality of life, and they will be more compliant in participating in cardiac rehabilitation.10,15,16 Meanwhile, if CHD patients have a low SE level, they will have poor self-care, especially in exercise.17 Poor self-care can disrupt emotional balance and reduce a person’s ability to deal with stress and affect their physical and psychological health.18 In addition, low SE in CHD sufferers is also associated with a lack of self-acceptance, poor health status, and the onset of depressive symptoms.11 Therefore, paying more attention to the factors that influence SE in this population is necessary.19
Previous studies conducted in Nepal said that the strongest predictor of SE in CHD patients was knowledge related to heart disease.20 CHD patients with good health knowledge and behaviour will undoubtedly have a high SE.20 In addition, SE in CHD patients is also influenced by several factors such as age, gender, place of residence, social status, education, occupation, income, BMI, smoking history, length of suffering from CHD, and medical history.14,20,21
Several studies have found various predictors affecting SE in patients with CHD.11,14,20,22–27 However, based on our literature search, no studies have been systematically reviewed to explore synthesizing SE and its predictors. Previous reviews reported that SE is a significant predictor of self-care behaviour in hypertensive patients and a prognostic indicator in patients with chronic disease.28–30 In addition, previous cohort studies also reported that SE could predict hospitalization in heart failure patients and all causes of death.31 Therefore, it is essential to systematically explore predictors of SE so that it can facilitate health workers to develop interventions and strategies to improve SE among this population.
Self-care behaviour in patients with CHD has different characteristics from several other diseases, as in the results of the studies previously mentioned, so there may be some specific things related to different SE predictors. It shows the importance of exploration in this regard. Based on these considerations, we need to explore the factors that influence SE in CHD patients through scoping reviews so that they can provide input to anticipate a decrease in SE in this population.
Materials and Methods
Design
This study uses a scoping review design. This design has flexible methodological techniques to identify and explore the latest rapidly developing topics.32 Besides, a scoping review has a more comprehensive conceptual range to explain relevant study results. The framework for writing a scoping review consists of several stages, including identifying research questions, relevant study results, selecting studies, mapping data, compiling, summarizing and reporting the results of a literature search.32 The study protocol was not published or registered.
Eligibility Criteria
The articles were selected for this review by six reviewers based on the PRISMA Extension for Scoping Reviews (PRISMA-ScR) (see Figure 1).33 Research questions and eligibility criteria for research articles use the PCC (Population, Concept, and Context) approach. The research question in this review is: what factors are associated with self-efficacy in CHD patients?
P (Population) : Adults and Patients with Coronary Heart Disease
C (Concept) : Cardiac self-efficacy OR Self-efficacy
C (Context) : Predictors of self-efficacy
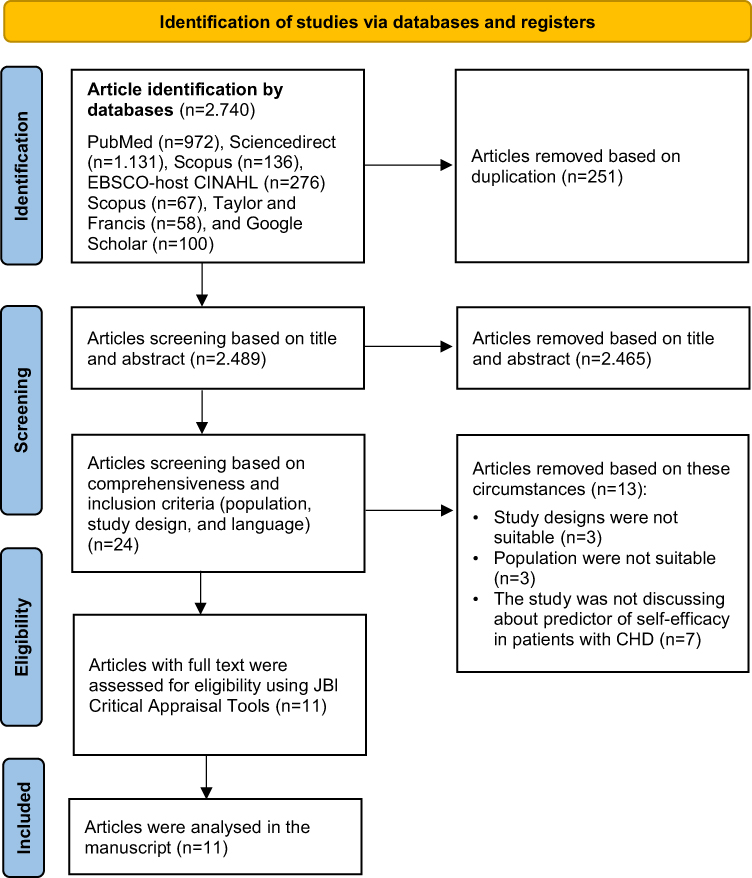 |
Figure 1 PRISMA Flow Diagram. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372: n71. Creative Commons.33 |
The inclusion criteria in this review were full-text articles in English, with cross-sectional and cohort designs discussing predictors of SE in CHD patients. Then, this review excluded studies using non-English languages, inaccessible full-text publications, and secondary research.
Data Collection and Analysis
Search Strategy
The literature search process was carried out systematically using five databases: CINAHL Plus with Full Text and Academic Search Complete, PubMed, ScienceDirect, Scopus, Taylor and Francis, and one search engine: Google Scholar, which was accessed on June 23, 2023. The search results are expanded using the snowballing technique based on relevant topics. The keywords used were
coronary heart disease OR coronary artery disease OR myocardial infarction OR cardiovascular disease OR Heart Disease AND Predictors OR Factors AND Self-efficacy OR Cardiac Self-efficacy OR General Self-efficacy.
Study Selection and Quality Appraisal
Four independent authors selected studies that were relevant and met the eligibility criteria. The authors checked for duplication in the initial article selection process using Mendeley’s reference manager. Then, the writer checked the title, abstract and read the article in full according to the relevance of the selected research topic based on the inclusion and exclusion criteria set by the author. The final process at the selection study stage is for the authors to assess each article that meets the inclusion criteria using the Joanna Briggs Institute (JBI) critical assessment checklist for cross-sectional studies.34
This guideline consists of eight assessment criteria consisting of research sample inclusion criteria, explanation of the study subject and research setting, exposure measurement, use of objective and standard criteria in measurement, identification of confounding factors, explanation of strategies for overcoming confounding factors, valid and reliable outcome measurement, and the accuracy of the use of statistics.35 The assessment consists of “yes”, “no”, “unclear”, and “not applicable”, with a score of 1 for each “yes” answer and a score of 0 for other answers. The total number of these scores will determine how worthy the article is to be included in the review. It allows the researcher to ascertain the extent to which the level of trust and relevance of the study results are included in further discussion. After the JBI assessment, we eliminated all studies that had a JBI score of <70% with final approval from the first, second, and third authors so that the final decision resulted in a unanimous opinion regarding the feasibility of the study, which will analyze in depth in this scoping review.
Data Extraction and Analysis
In the data extraction and analysis stages, this review uses extraction tables to describe all research results that are related and relevant to the research topic. The extraction table contains information related to the studies’ characteristics, including authors, study design, country, sample (sample size and mean age), research findings (Level of SE, category of SE, and predictors of SE), and final results of the JBI. All studies analyzed were primary studies with cross-sectional and cohort designs. Therefore, data analysis was done thematically and qualitatively with an exploratory, descriptive approach. The process of data analysis begins with the identification and presentation of the data obtained in tabular form based on the articles reviewed. After obtaining the data, all authors analyzed and explained the results of each study that focused on predictors of cardiac SE among patients with CHD.
The authors divide the predictor category into three classifications based on the odds ratio (OR) value. It was categorized as low if the OR value was <0.5, medium if the OR value was ≥0.5 to 1, and high if the OR value was more than 1. In addition, in studies that did not display an OR value, we categorized SE predictors based on the r correlation value where the predictor category was high. It has a correlation value of r > 0.60, the medium category is in the range of 0.41 to 0.60, and the low category is less than 0.41. If the research does not include OR and r correlation values, then it is considered that it cannot be categorized.
Results
Study Selection
The results of the selection of studies in the early stages of this review obtained 2.740 articles. Furthermore, the authors selected the articles based on the title, abstract, and predetermined inclusion criteria so that the remaining 24 studies were then analyzed based on full-text article analysis. As a result, 11 studies were appraised with the JBI tool. Figure 1 shows the process of selecting study flow to obtain 11 studies which are further analyzed in this scoping review using the PRISMA flowchart.
Study Characteristics
All studies analyzed in this review were cross-sectional (n = 11). Based on the results, most studies reporting SE in CHD patients have an average low to moderate level of SE (see Table 1). Most of the studies (n=6) were conducted in developing countries. All samples analyzed were patients with CHD (n = 2.164) with a mean age of 54 to 68 years. The largest sample is 451 respondents27 and the smallest 85 respondents.22 The results of the JBI analysis show that all studies analyzed using the cross-sectional method have good quality (>70%). Most of the studies examined had weaknesses in identifying confounding factors and did not include strategies to address these factors.
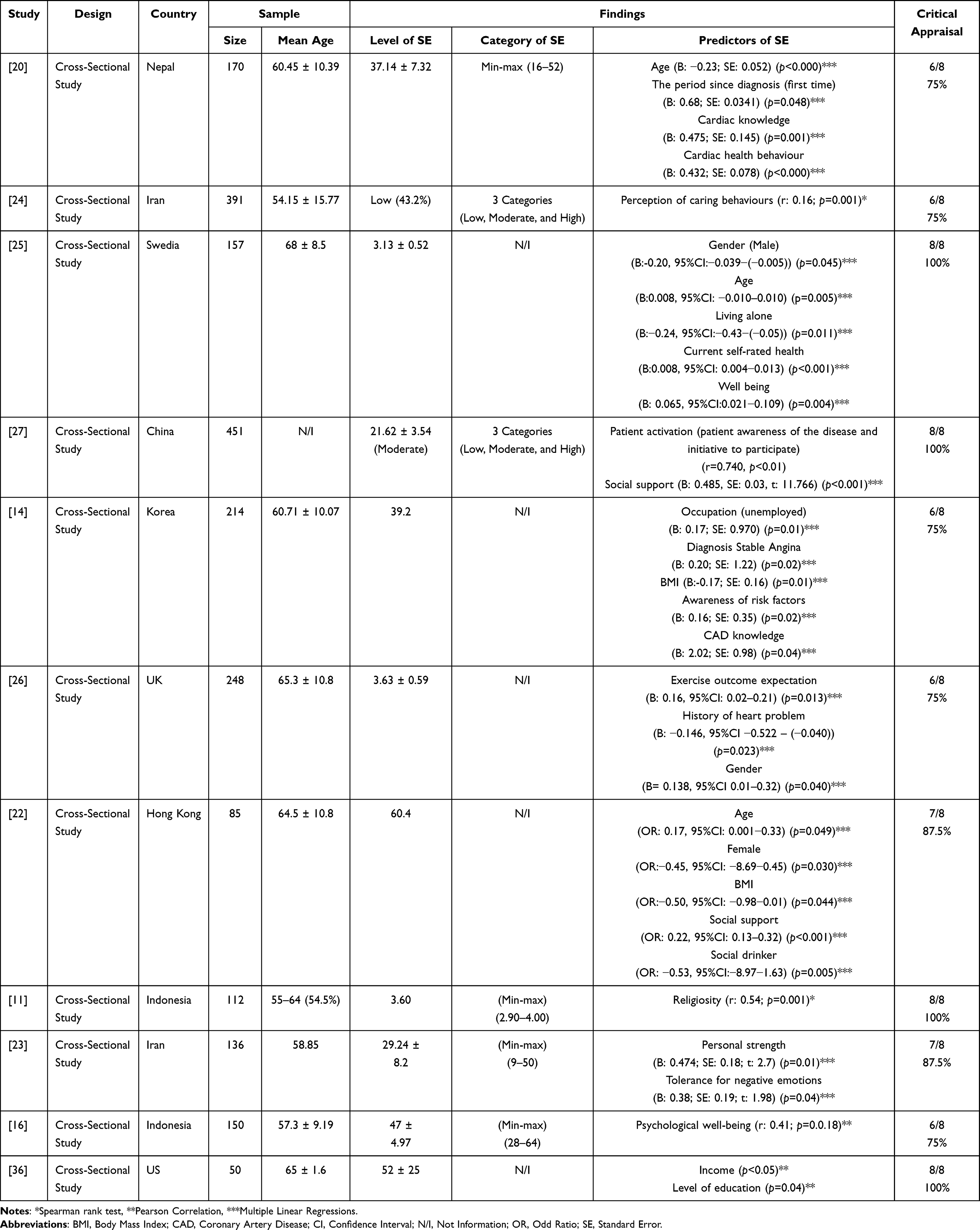 |
Table 1 Characteristics of Study |
Level and Category of Self-Efficacy
The analysis results in this review show that the SE level has heterogeneous results, some of which are analyzed using categorization24,27 and there is also analysis with numerical data.11,14,16,20,22,23,25,26,36 Two studies classified SE into three categories (low, moderate, and high).24,27 While, four studies were classified numerically and displayed minimum and maximum values,11,16,20,23 and five studies do not display minimum and maximum values.14,22,25,26,36 Based on research results, most studies report that SE in CHD patients tends to have a low to moderate average SE level (see Table 1).
Factors Associated with Self-Efficacy
This review identifies factors significantly associated with SE in patients with CHD. Based on the analysis results, demographic characteristics, health perception, knowledge and awareness of the illness, environmental factors, health behaviour, medical history, and psychological factors have a significant relationship with the level of SE in patients with CHD. Furthermore, these factors are then classified into three categories.
These factors were divided into three categories based on the OR and r correlation values, namely low (OR<0.5 or r<0.41), moderate (OR ≥0.5 to 1 or r=0.41 to 0.60), and high (OR >1 or r >0.60) (see Table 2). The higher the OR or r correlation value, the variable becomes the most influential predictor of SE in CHD patients. In this review, the predictors included in the high category are health perception, knowledge, and awareness of the illness (patient activation and cardiac knowledge). In addition, the moderate predictors included demographic characteristics (BMI), environmental factors (social drinkers), medical history (period since diagnosis), and psychological factors (religiosity). Then, predictors included in the low category are demographic characteristics (age, gender, occupation, and living alone), health perception, knowledge, and awareness of the illness (perception of caring behaviours, perception of current self-rated health, and exercise outcome), environmental factors (social support), health behaviour (cardiac health behaviour), medical history (diagnosis of stable angina), and psychological factors (psychological well-being, personal strength, and tolerance for negative emotions). Finally, the uncategorized factors are income and level of education. In this review, cardiac knowledge (B: 2.02; SE: 0.98; p=0.04) and patient activation (patient awareness) (r=0.74) was the most influential predictor of SE in patients with CHD (see Table 2).
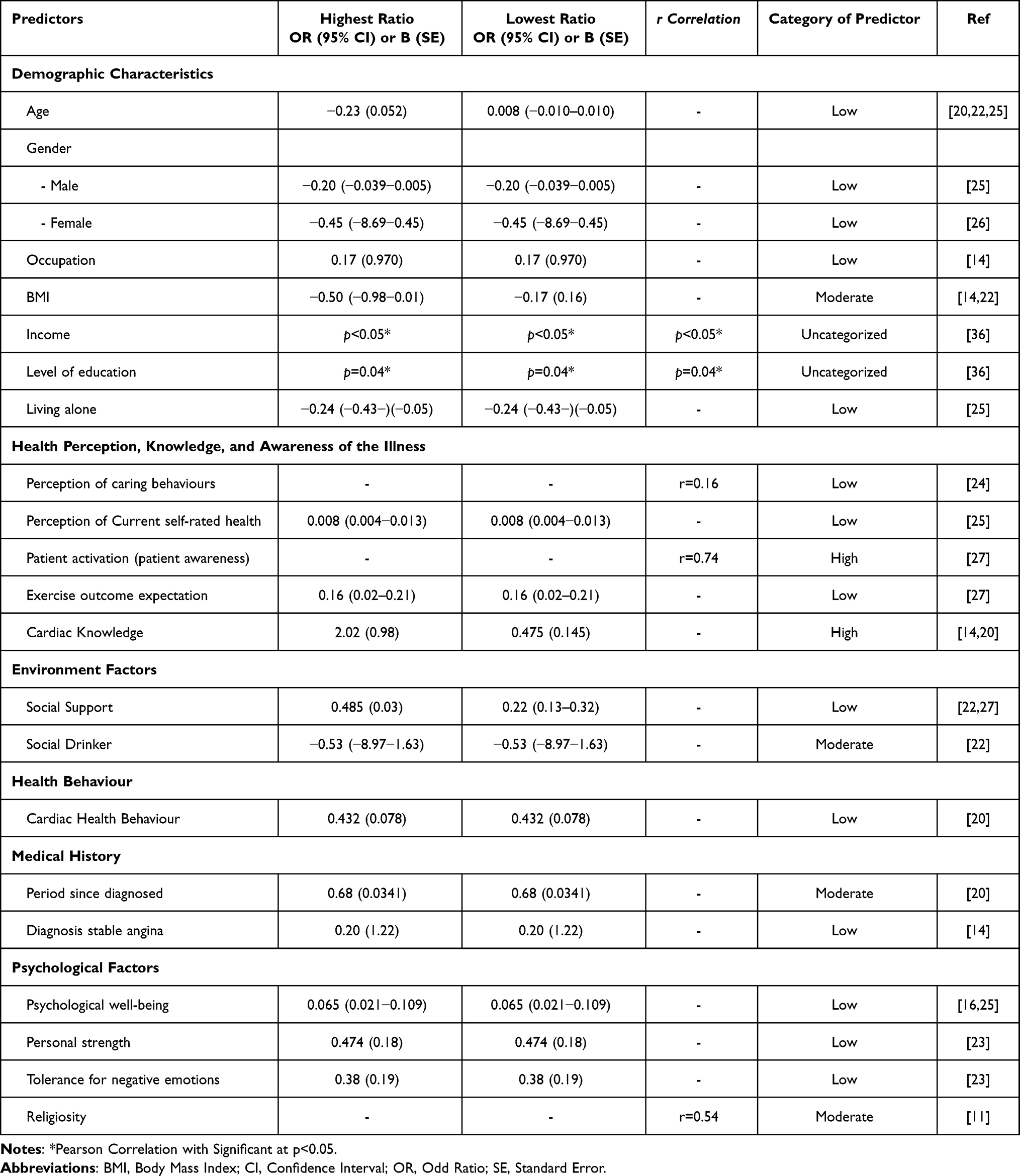 |
Table 2 Predictors of Cardiac Self-Efficacy |
Discussion
This scoping review identifies SE and factors that may influence SE in patients with CHD. In general, the results of this review show that most of the studies analyzed reported that patients with CHD tended to have low to moderate SE rates. There are six predictors that can influence the level of SE, including demographic characteristics, health perception, knowledge and awareness of the illness, environment, health behaviour, medical history, and psychological factors. Then, we classified these predictors into three categories, namely low, moderate, and high.
The factors that most influence SE in this review are included in the high category (see Table 2). Cardiac knowledge is the most influential factor on SE in patients with CHD14,20 SE, and internal locus of control has direct and indirect effects on health where knowledge of risk factors is treated as a potential mediator affecting SE.37 Previous studies reported that patient knowledge of risk factors for CHD was associated with low rates of disease recurrence and SE in sufferers.37 Moreover, patients who are knowledgeable about CHD and accurately understand their risk factors may realize that they have more control over their symptoms and maintain functional activity, so it is not surprising that they have high SE rates.14
Another predictor included in the high category is patient activation.27 In this review, patient activation refers to the patient’s awareness of the disease and the initiative to participate in disease management which is closely related to the level of knowledge.14,20,27 Previous studies reported that patients with CHD almost do not feel their CHD risk factors, such as gender, hyperlipidemia, hypertension, obesity, and so on.38 Knowledge of CHD risk factors will inform individuals to adopt a healthy diet, weight management, and physical activity.39 Moreover, patient activation is a major driver of effective self-management among patients with chronic disease.40 Patients who have a high level of activation, most of them have a high SE, so they are considered to easy to face various difficulties or problems in disease rehabilitation, promote their behaviour change, actively cooperate with medical staff and participate in management.27 Higher patient activation rates are also associated with better self-management, lower medical costs, and improved health outcomes in different groups of patients with chronic diseases.27,40,41
Predictors in the moderate category that influence SE in this review are BMI, social drinkers, the period since diagnosis, and religiosity.11,14,20,22 Previous studies reported that BMI was a significant predictor of low exercise SE in CHD patients.14,22 In addition, social drinkers have an impact on someone having an excess BMI.22 Individuals with an overweight BMI category are one of the barriers for someone to do activities or sports.14 The same thing was reported by the research of Rachmah et al, which informed that the level of physical activity is related to BMI and sedentary activity.42 Individuals who engage in moderate to vigorous levels of activity have a higher SE and are, therefore, more able to overcome obstacles than their counterparts who are included in the light physical activity category.42
The period since diagnosis and religiosity also have an influence on the SE of CHD patients in the moderate category. Patients diagnosed with CHD for a long time have more knowledge and experience, so they will apply good health care and behaviour in their daily lives.20 In addition, religion is also a predictor in the moderate category because it provides reinforcement and a person’s belief through prayer to improve the patient’s health and recovery.11 Patients with CHD perform prayer services to gain strength, comfort and hope for the meaning of support in improving their quality of life and can improve coping in overcoming obstacles while managing the disease.43 Previous studies reported that patients with CHD with a high religious level are better able to manage lifestyles such as quitting smoking, reducing alcohol consumption, and increasing exercise so that they have fewer cardiovascular risk factors at the onset of the disease.11 Therefore, the relationship between religiosity and SE can have a substantial value and have a positive effect on better self-care levels in CHD patients, so this can also prevent prolonged hospital stays and participation in cardiac rehabilitation.44–46
In this review, predictors in the low category that affect SE based on demographic characteristics are age, gender, occupation, and living alone.14,20,22,25,26 Increasing age is often associated with a decrease in the SE of patients with heart disease.20,22,25 With increasing age, SE will tend to decrease due to ageing and decreased muscle strength, so it has an impact on tolerance in carrying out daily physical activities.20 However, these results differ from a study conducted in Nepal which reported that people with heart disease at a younger age had a lower SE compared to elderly patients.20 This can happen because it is related to lifestyle, such as excessive alcohol consumption by these patients.22
Gender can also affect SE in the low category.25,26 The study results show that women are identified as having significantly more symptoms of heart disease, which are more likely to reduce SE compared to men.26 The group that has a job shows a much higher cardiac SE than the unemployed group.14 Also, previous studies suggest that older adults have more hours of productive activity.44 Thus, involvement in productive activities such as working at the end of life can maintain or even increase SE. Furthermore, living alone is also included in the low predictor that affects SE.25 Patients who live alone are often unable to develop independent coping mechanisms due to a lack of adequate social support.47 This impacts the lack of adherence to recommended therapy guidelines, fewer visits to doctors or cardiac rehabilitation, and also seeking medical help when needed.47
Factors such as perception of caring behaviours, perception of current self-rated health (SRH), and exercise outcome expectation are included in the low category based on health perception, knowledge, and awareness of the illness, which can affect SE. Perception of caring behaviour is described by the patient’s perception of the nurse’s caring behaviour in physical touch and being empathetic with patients.24 Meanwhile, the perception of SRH is used to evaluate the state of health based on biological, mental, functional, and spiritual dimensions that can assist in making decisions for each individual in critical situations. Thus, someone who has a good perception of SRH will affect the increase in SE in CHD patients.25 Exercise outcome expectations also play an essential role in high or low SE.27 Someone who has high outcome expectations in curing their illness will be more motivated to perform the correct health behaviour to get the desired outcome.48
Other predictors in the low category that affect SE in CHD patients are the type of patient diagnosis, psychological factors, and social support. Diagnosis is a significant predictor that can affect cardiac SE.14 The study results show that patients diagnosed with stable angina tend to have a higher level of cardiac SE than patients diagnosed with unstable angina.14 This difference can be explained through the characteristic symptoms of each patient with the two diagnoses. As mentioned in previous studies, increased symptom burden, physical impairment, and lower health status are associated with poor cardiac SE.13 Although chest pain is a common symptom of angina, in unstable angina or myocardial infarction (MI), the chest pain will not wholly subside with rest or nitroglycerin.13
Differences in diagnostic conditions do not only have an impact on the patient’s physical condition, but also affect the physical and psychological burden of the patient so that it has an impact on the SE level, which in turn affects the patient’s well-being and ability to adapt to the conditions of the disease he is suffering.13,16,25 This is in line with the findings in this review, where psychological well-being is a predictor in the low category, which affects SE in patients with CHD.16,25 Even though it is included in the low category, improving the well-being of CHD patients indirectly has the potential to increase cardiac SE in CHD patients.49
Other psychological factors contributing to CHD sufferers’ SE are personal strength and tolerance for negative emotions.23 Personal strength and tolerance for negative emotions are aspects or parts of one’s resilience. As is well known, CHD patients experience physical and cognitive and emotional processing disorders.50 In this context, an increase in SE in CHD patients can be supported by increasing the patient’s resilience in dealing with dynamic changes in physical and psychological aspects.51 Even though a person can change and adapt to the difficulties experienced, family and community support is still needed to increase resilience.52
In this review, social support is one of the low-category predictors of SE, which also has an essential role for CHD patients.27 This is because good social support can reduce psychological stress, increase patient confidence in overcoming the disease, and encourage patient participation in disease management.53 This strengthens the results of previous studies, which state that social support is associated with SE.22,27 Patients with good cardiac SE tend to have the motivation to adopt positive behaviours related to their health problems.54 These results align with previous studies, which state that increased cardiac SE is associated with improved cardiac health behaviour.20 This behaviour can be related to physical activity, smoking, dietary intake, and BMI.55 Considering that the management of CHD patients is a continuous chronic process, patients with good SE who are active in the disease management process are more likely to get better long-term health outcomes.56
The predictors included in the uncategorized category in this review are income and level of education.36 Although these predictors are uncategorized, patients with CHD with high incomes and education levels tend to have high SE values. A better SE level in this group will make them more confident and have more time and resources that can support and maintain healthy behaviour.14,36 The same thing was also reported in research conducted in China, which explained that someone with a low income also tends to have a low SE level.57 Low income is reported to cause difficulties in accessing health literacy so that patients receive less information regarding self-management and disease knowledge.57
In this review, the predictors of SE in CHD patients are multifactorial. However, the most important finding in this review is that knowledge and patient activation are predictors in the high category affecting CHD patients’ SE rate. Therefore, health education is the primary strategy to improve SE in CHD patients. Previous studies in Indonesia reported that health education using workbooks significantly improved SE in CHD patients.58 The same thing was reported in previous studies, which ascertained that increased knowledge about self-care of patients with heart disease was associated with increased cardiac SE.59,60 In addition, the digital cardiac rehabilitation program also positively affects knowledge and SE in CHD patients.61 Therefore, some of these strategies are expected to increase SE in CHD patients so that the increase in SE will align with the increase in QoL in patients with CHD.
Strengths and Limitations
The limitation of this scoping review is that the authors found it difficult to classify the levels and predictors of SE. The SE categorization and predictors in the analyzed articles are quite heterogeneous, so it is not easy to generalize them. In overcoming this limitation, the author decided not to categorize the level of SE because it could cause bias and only mentioned it descriptively in the results section. Then, in determining the predictor categories, the author carried out an in-depth analysis regarding the meaning of each predictor so that each predictor with the same meaning can be combined. In addition, the SE predictor categories in this review are based on OR and r correlation values, where these values are quite variable, and most of them tend to be small. When new research (cohort studies) is added, this category will change depending on how large the OR or r correlation value is obtained from the analyzed studies. Therefore, to clarify SE categories based on OR/B values, it is necessary to identify predictors of SE in CHD patients in the future using a cohort design. When compared cross-sectionally, research results from cohort studies will be much better and more comprehensive if the research objective is to identify predictors or risk factors.
Although this study has several limitations, this study is the first review regarding predictors of SE in CHD patients. Apart from that, the studies analyzed in this review are of good quality and have carried out critical appraisal using the JBI tool. This review may provide a better understanding of the factors influencing SE of CHD patients. Thus, it can assist health professionals in developing more effective and evidence-based health interventions to improve the SE of CHD patients.
Conclusions
Cardiac knowledge and patient activation are the most influential predictors of the low SE of CHD patients. The predictors of SE are multifactorial, so health workers, especially nurses, can correctly identify these factors and design a strategy to optimize or increase the level of SE. Policymakers can encourage implementing public health education programs that focus on improving SE in CHD patients. In addition, health professionals can also participate in facilitating patients by providing health education and encouraging patients to adopt a healthy lifestyle. Health education can be specifically designed to increase the SE of this population so that an increase in SE will go hand in hand with the fast healing process and good disease management. Identification of appropriate educational methods for improving SE in CHD patients is also essential so that future researchers can consider this in the process of developing future educational strategies.
Acknowledgments
All authors thank Universitas Padjadjaran and the Education Fund Management Institution or Lembaga Pengelola Dana Pendidikan (LPDP), who has facilitated the database and supported funding for this review.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization (WHO). Cardiovascular diseases (CVDs) [Internet]; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-cvds.
2. American Heart Association. 2023 Heart Disease and Stroke Statistics Update Fact Sheet [Internet]; 2023. Available from: https://professional.heart.org/en/science-news/heart-disease-and-stroke-statistics-2023-update.
3. Ministry of Health Republic of Indonesia. Hasil Riset Kesehatan Dasar Tahun 2018 (Results of Basic Health Research 2018). Health Dev Res Agcy. 2018;53:
4. Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart disease and stroke statistics-2017 Update: a Report From the American Heart Association. Circulation. 2017;135(10):e146–603. doi:10.1161/CIR.0000000000000485
5. Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: a Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79(2):e21–129.
6. Du S, Feng Z, Wang W, Tian L, Wang Y. A structural equation model linking health literacy, self efficacy and quality of life in adults with coronary heart disease. BMC Cardiovasc Disord. 2022;22(1):285. doi:10.1186/s12872-022-02720-8
7. Sol BGM, van der Graaf Y, van Petersen R, Visseren FLJ. The effect of self-efficacy on cardiovascular lifestyle. Eur J Cardiovasc Nurs. 2011;10(3):180–186. doi:10.1016/j.ejcnurse.2010.06.005
8. Salari A, Rouhi Balasi L, Moaddab F, Zaersabet F, Nouri Saeed A, Habib Nejad S. Patients’ cardiac self-efficacy after coronary artery angioplasty. Jundishapur J Chronic Dis Care. 2016;1–5. doi:10.17795/jjcdc-37251
9. Ahn S, Song R, Choi SW. Effects of self-care health behaviors on quality of life mediated by cardiovascular risk factors among individuals with coronary artery disease: a structural equation modeling approach. Asian Nurs Res (Korean Soc Nurs Sci). 2016;10(2):158–163. doi:10.1016/j.anr.2016.03.004
10. Almeida JAB, Florêncio RB, Lemos DA, Leite JC, Monteiro KS, Peroni Gualdi L. Self-efficacy instruments for individuals with coronary artery disease: a systematic review protocol. BMJ Open. 2022;12(7):1–4. doi:10.1136/bmjopen-2022-062794
11. Wantiyah RFRP, Hakam M, Hakam M. The correlation between religiosity and self-efficacy in patients with coronary artery disease. Belitung Nurs J. 2020;6(5):172–176. doi:10.33546/bnj.1134
12. Brink E, Alsén P, Herlitz J, Kjellgren K, Cliffordson C. General self-efficacy and health-related quality of life after myocardial infarction. Psychol Health Med. 2012;17(3):346–355. doi:10.1080/13548506.2011.608807
13. Sarkar U, Ali S, Whooley MA. Self-efficacy and health status in patients with coronary heart disease: findings from the heart and soul study. Psychosom Med. 2007;69(4):306–312. doi:10.1097/PSY.0b013e3180514d57
14. Kang Y, Yang I. Cardiac self-efficacy and its predictors in patients with coronary artery diseases. J Clin Nurs. 2013;22(17–18):2465–2473. doi:10.1111/jocn.12142
15. Al-Sutari M, Ahmad M. Predictors of adherence to self-care behaviors among patients with coronary heart disease. Nurs Pract Today. 2022;9(2):145–157.
16. Fahmi I, Suryaman A, Ganefianty A. The relationship of psychological well-being with a cardiac diet self efficacy in acute coronary syndrome patients. J Pendidik Keperawatan Indones. 2022;8(2):119–126.
17. Woodgate J, Brawley LR. Self-efficacy for exercise in cardiac rehabilitation: review and recommendations. J Health Psychol. 2008;13(3):366–387. doi:10.1177/1359105307088141
18. Cilli E, Ranieri J, Guerra F, Ferri C, Di Giacomo D. Cardiovascular disease, self-care and emotional regulation processes in adult patients: balancing unmet needs and quality of life. Biopsychosoc Med. 2022;16(1):20. doi:10.1186/s13030-022-00249-y
19. Nuraeni A, Sugiharto F, Anna A, et al. Self-efficacy in self-care and its related factors among patients with coronary heart disease in Indonesia : a Rasch analysis self-efficacy in self-care and its related factors among patients with coronary heart disease. Vasc Health Risk Manag. 2023;Volume 19:583–593. doi:10.2147/VHRM.S427488
20. Shrestha R, Rawal L, Bajracharya R, Ghimire A. Predictors of cardiac self-efficacy among patients diagnosed with coronary artery disease in tertiary hospitals in Nepal. J Public Health Res. 2020;9(4):1787. doi:10.4081/jphr.2020.1787
21. Barham A, Ibraheem R, Zyoud SH. Cardiac self-efficacy and quality of life in patients with coronary heart disease: a cross-sectional study from Palestine. BMC Cardiovasc Disord. 2019;19(1):1–12. doi:10.1186/s12872-019-01281-7.
22. Chair SY, Wong KB, Tang JYM, Wang Q, Cheng HY. Social support as a predictor of diet and exercise self-efficacy in patients with coronary artery disease. Contemp Nurse. 2015;51(2–3):188–199. doi:10.1080/10376178.2016.1171726
23. Ghaedrahamt M, Zohari Anboohi S, Borhani F, Gholami Chaboki B. The relationship between spiritual intelligence and self-efficacy in patients with acute coronary syndrome admitted to cardiac care unit. J Adv Pharm Educ Res. 2021;10(1):120–127.
24. Kargar L, Khademian Z, Rambod M. Association between perception of caring behaviors and self-efficacy in patients with cardiovascular disease at coronary care units: a cross-sectional study. Acute Crit Care. 2021;36(2):118–125. doi:10.4266/acc.2020.00752
25. Kärner Köhler A, Tingström P, Jaarsma T, Nilsson S. Patient empowerment and general self-efficacy in patients with coronary heart disease: a cross-sectional study. BMC Fam Pract. 2018;19(1):76. doi:10.1186/s12875-018-0749-y
26. Lau-Walker M. Relationship between illness representation and self-efficacy. J Adv Nurs. 2004;48(3):216–225. doi:10.1111/j.1365-2648.2004.03190.x
27. Zhu Y, Song Y, Wang Y, et al. Relationships among social support, self-efficacy, and patient activation in community-dwelling older adults living with coronary heart disease: a cross-sectional study. Geriatr Nurs (Minneap). 2022;48:135–140. doi:10.1016/j.gerinurse.2022.09.008
28. Martinez-Calderon J, Zamora-Campos C, Navarro-Ledesma S, Luque-Suarez A. The role of self-efficacy on the prognosis of chronic musculoskeletal pain: a systematic review. J Pain. 2018;19(1):10–34. doi:10.1016/j.jpain.2017.08.008.
29. Tan FCJH, Oka P, Dambha-Miller H, Tan NC. The association between self-efficacy and self-care in essential hypertension: a systematic review. BMC Fam Pract. 2021;22(1):1–12. doi:10.1186/s12875-021-01391-2
30. Benyon K, Hill S, Zadurian N, Mallen C. Coping strategies and self-efficacy as predictors of outcome in osteoarthritis: a systematic review. Musculoskelet Care. 2010;8(4):224–236. doi:10.1002/msc.187
31. Sarkar U, Ali S, Whooley MA. Self-efficacy as a marker of cardiac function and predictor of heart failure hospitalization and mortality in patients with stable coronary heart disease: findings from the heart and soul study. Health Psycool. 2009;28(2):166–173. doi:10.1037/a0013146
32. Peterson J, Pearce PF, Ferguson LA, Langford CA. Understanding scoping reviews: definition, purpose, and process. J Am Assoc Nurse Pract. 2017;29(1):12–16. doi:10.1002/2327-6924.12380
33. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:1–11.
34. Joanna Briggs Institute (JBI). JBI’s critical appraisal tools [Internet]. Joanna Briggs Institute; 2022 [cited January 1, 2023]. Available from: https://jbi.global/critical-appraisal-tools.
35. Joanna Briggs Institute. JBI Checklist for Analytical Cross Sectional Studies [Internet]. Joanna Briggs Institute Reviewer’s Manual; 2017. Available from: https://synthesismanual.jbi.global/.
36. LaPier TK, Cleary K, Kidd J. Exercise self-efficacy, habitual physical activity, and fear of falling in patients with coronary heart disease. Cardiopulm Phys Ther J. 2009;20(4):5–11. doi:10.1097/01823246-200920040-00002
37. Moore SM, Prior KN, Bond MJ, et al. The contributions of psychological disposition and risk factor status to health following treatment for coronary artery disease. Eur J Cardiovasc Nurs. 2007;6(2):137–145. doi:10.1016/j.ejcnurse.2006.06.004
38. Yang IS, Choi D, Kang Y. The Awareness of Cardiovascular Risk Factors and Its Correlates in Patients with Coronary Artery Diseases. J Korean Acad Adult Nurs. 2010;22(5):499–508.
39. Abdul M, Alotaibi NA, Rashikh MA, et al. Awareness and prevalence of coronary artery disease risk factors among Saudi adults in Dawadmi, Riyadh province: a cross‑sectional study. J Fam Med Prim Care. 2017;6(2):169–170.
40. Shnaigat M, Downie S, Hosseinzadeh H. Effectiveness of patient activation interventions on chronic obstructive pulmonary disease self-management outcomes: a systematic review. Aust J Rural Health. 2022;30(1):8–21. doi:10.1111/ajr.12828
41. Blakemore A, Hann M, Howells K, et al. Patient activation in older people with long-term conditions and multimorbidity: correlates and change in a cohort study in the United Kingdom. BMC Health Serv Res. 2016;16(1):582. doi:10.1186/s12913-016-1843-2
42. Rachmah Q, Setyaningtyas SW, Rifqi MA, et al. Self-efficacy to engage in physical activity and overcome barriers, sedentary behavior, and their relation to body mass index among elderly Indonesians with diabetes. J Prev Med Public Heal. 2019;52(4):242–249. doi:10.3961/jpmph.19.003
43. Abu HO, Ulbricht C, Ding E, et al. Association of religiosity and spirituality with quality of life in patients with cardiovascular disease: a systematic review. Qual Life Res An Int J Qual Life Asp Treat Care Rehabil. 2018;27(11):2777–2797.
44. Baker LA, Cahalin LP, Gerst K, Burr JA. Productive activities and subjective well-being among older adults: the influence of number of activities and time commitment. Soc Indic Res. 2005;73(3):431–458. doi:10.1007/s11205-005-0805-6
45. Sugiharto F, Nuraeni A, Trisyani Y, Melati Putri A, Aghnia Armansyah N. Barriers to participation in cardiac rehabilitation among patients with coronary heart disease after reperfusion therapy: a scoping review. Vasc Health Risk Manag. 2023;19:557–570. doi:10.2147/VHRM.S425505
46. Sugiharto F, Trisyani Y, Nuraeni A, Mirwanti R, Melati Putri A, Aghnia Armansyah N. Factors associated with increased length of stay in post primary percutaneous coronary intervention patients: a scoping review. Vasc Health Risk Manag. 2023;19:329–340. doi:10.2147/VHRM.S413899
47. Gandhi S, Goodman SG, Greenlaw N, et al. Living alone and cardiovascular disease outcomes. Heart. 2019;105(14):1087–1095. doi:10.1136/heartjnl-2018-313844
48. Rismayanthi C, Alim A, Apriyanto KD, Mulyawan R, Miftachurochmah Y. Relationship between self-efficacy and outcome expectation on body mass index in the elderly population. Univers J Public Heal. 2022;10(6):581–589. doi:10.13189/ujph.2022.100605
49. Levine GN, Cohen BE, Commodore-Mensah Y, et al. Psychological health, well-being, and the mind-heart-body connection: a scientific statement from the American Heart Association. Circulation. 2021;143(10):e763–83. doi:10.1161/CIR.0000000000000947
50. Krok D, Zarzycka B. Self-efficacy and psychological well-being in cardiac patients: moderated mediation by affect and meaning-making. J Psychol. 2020;154(6):411–425. doi:10.1080/00223980.2020.1772702
51. Ghaedrahamt M, Anboohi SZ, Borhani F, Chaboki BG. Relationship between resiliency and self-efficacy in patients with acute Coronary Syndrome admitted to intensive care units. J Adv Pharm Educ Res. 2019;9(S2):147–151.
52. Southwick SM, Bonanno GA, Masten AS, Panter-Brick C, Yehuda R. Resilience definitions, theory, and challenges: interdisciplinary perspectives. Eur J Psychotraumatol. 2014;5(1):25338. doi:10.3402/ejpt.v5.25338
53. Rodriguez LA, Thomas TW, Finertie H, Turner CD, Heisler M, Schmittdiel JA. Psychosocial and diabetes risk factors among racially/ethnically diverse adults with prediabetes. Prev Med Rep. 2022;27:101821. doi:10.1016/j.pmedr.2022.101821
54. O’Neil A, Berk M, Davis J, Stafford L. Cardiac-self efficacy predicts adverse outcomes in coronary artery disease (CAD) patients. Health (Irvine Calif). 2013;5(7A3):6–14.
55. Shay CM, Gooding HS, Murillo R, Foraker R. Understanding and improving cardiovascular health: an update on the American Heart Association’s concept of cardiovascular health. Prog Cardiovasc Dis. 2015;58(1):41–49. doi:10.1016/j.pcad.2015.05.003
56. Tsay SL, Chao YFC. Effects of perceived self-efficacy and functional status on depression in patients with chronic heart failure. J Nurs Res. 2002;10(4):271–278. doi:10.1097/01.JNR.0000347608.76047.7a
57. Zhang Q, Huang F, Zhang L, Li S, Zhang J. The effect of high blood pressure-health literacy, self-management behavior, self-efficacy and social support on the health-related quality of life of Kazakh hypertension patients in a low-income rural area of China: a structural equation model. BMC Public Health. 2021;21(1):1114. doi:10.1186/s12889-021-11129-5
58. Nuraeni A, Mirwanti R, Anna A. Effect of a workbook in health education on self-efficacy and quality of life of patients with coronary heart disease. Belitung Nurs J. 2019;5(6):218–224. doi:10.33546/bnj.801
59. Polsook R, Aungsuroch Y. A cross-sectional study of factors predicting readmission in Thais with coronary artery disease. J Res Nurs. 2021;26(4):293–304. doi:10.1177/1744987120946792
60. Yehle KS, Plake KS. Self-efficacy and educational interventions in heart failure: a review of the literature. J Cardiovasc Nurs. 2010;25(3):175–188. doi:10.1097/JCN.0b013e3181c71e8e
61. Salah Eldin Saad N, El Ashery Ashery Asker R. Effect of digital cardiac rehabilitation program on self efficacy of patients with coronary artery diseases. Egypt J Heal Care. 2020;11(1):400–416. doi:10.21608/ejhc.2020.177145
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Self-Efficacy in Self-Care and Its Related Factors Among Patients with Coronary Heart Disease in Indonesia: A Rasch Analysis
Nuraeni A, Sugiharto F, Anna A, Sari E, Mirwanti R, Trisyani Y, Emaliyawati E
Vascular Health and Risk Management 2023, 19:583-593
Published Date: 5 September 2023
Health Educational Methods for Improving Self-Efficacy Among Patients with Coronary Heart Disease: A Scoping Review
Sugiharto F, Haroen H, Alya FP, Jamlaay R, Mai F, Abdillah H, Yusanti I, Assidiqy B, Nuraeni A
Journal of Multidisciplinary Healthcare 2024, 17:779-792
Published Date: 22 February 2024
Predictors of Self-Care Self-Efficacy in Adults Familiar with Palliative Care: The Role of Patient-Centered Communication, Health, and Well-Being
Ramos-Vera C, Basauri-Delgado M, Krikorian A, Calizaya-Milla YE, Saintila J
Patient Preference and Adherence 2025, 19:3025-3035
Published Date: 26 September 2025
Social Support and Hospital Discharge Readiness in CHD Patients: Mediating Roles of Self-Efficacy and Adherence
Wang D, Yang N, Wei C, Wang J, Yuan L, Sun R
Patient Preference and Adherence 2026, 20:601646
Published Date: 4 June 2026