Back to Journals » Clinical Interventions in Aging » Volume 15
A Scoping Review and Template Analysis of Manual-Based Complex Interventions in Dementia Care
Authors Anderson-Ingstrup J ![]() , Ridder HM
, Ridder HM ![]()
Received 9 November 2019
Accepted for publication 23 January 2020
Published 13 March 2020 Volume 2020:15 Pages 363—371
DOI https://doi.org/10.2147/CIA.S237924
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Video abstract of "Manual-based interventions in dementia care" [ID 237924]
Views: 292
Jens Anderson-Ingstrup, Hanne Mette Ridder
Department of Communication and Psychology, Doctoral Programme in Music Therapy, Aalborg University, Aalborg, Denmark
Correspondence: Jens Anderson-Ingstrup Musikkens Hus, Musikkens Plads 1, Aalborg 9000, Denmark
Tel +45 60 15 48 67
Email [email protected]
Purpose: In dementia care, the complexity of psychosocial needs and contextual variables often demands nonpharmacological interventions of a complex nature. The purpose of this scoping review was to investigate (1) how manuals published in refereed journals explaining procedures of complex interventions in dementia care are structured and their content disseminated and (2) to provide recommendations for future manuals.
Methods: A systematic search was conducted using four databases (Embase, PsychInfo, CINAHL and Scopus) following PRISMA-ScR and PICo method. The results were analysed using template analysis aiming to describe the possibility of tailoring the intervention, degree of flexibility of the manual and dissemination elements used in the manual.
Results: A total of 882 records were identified, and 86 full-text articles were assessed. Nine articles containing manuals met the inclusion criteria. All of the included manuals allowed the user to tailor actions in the intervention to specific situations. Two-thirds of the manuals showed a medium degree of flexibility. The types of dissemination elements varied. All used written text, and some used various graphical organisers such as headlines and lists. None used illustrations or audio/video material.
Conclusion: Currently, only few manuals for complex interventions in the field of dementia are published in refereed journals, all disseminated as written text. For future manuals, we suggest considering the inclusion of illustrations and/or audio/video material to describe actions, to allow for tailoring of the intervention, and to maintain a medium or low degree of flexibility by structuring the content hierarchically in phases while providing the user with detailed description of what to do, and how to decide what to.
Keywords: manual-based intervention, dementia, complex intervention, nonpharmacological intervention, ecopsychosocial intervention
Introduction
In national clinical guidelines for dementia, pharmacological interventions are recommended and described in detail both in Denmark and the UK. In contrast, other kinds of interventions, such as psychosocial interventions and approaches to care, are defined as nonpharmacological and as such by what they are not. In many countries, this leaves the clinical guidelines with two sections, one with pharmacological interventions, and one with the imprecise term nonpharmacological interventions. As an example, the NICE guidelines for dementia in the UK mention the following nonpharmacological interventions: aromatherapy, multisensory stimulation, therapeutic use of music and/or dancing, animal-assisted therapy, and massage. These approaches should be considered for non-cognitive symptoms and changed behaviours and should be tailored to the person’s preferences, skills and abilities.1 The guidelines describe evidence of clinical effectiveness of these nonpharmacological interventions, but also point out how more research into their cost-effectiveness is needed.1 The most recent NICE guidelines still highlight the need for further research in this field.2
Thus, there is a need for more research of specific types of nonpharmacological interventions in order to guide clinicians and decision makers in choosing the best methods.3 This, however, highlights the problem that nonpharmacological research in general is poorly described. In a systematic review of 137 nonpharmacological interventions within dementia care, a large proportion (61%) did not describe what the treatment consisted of in detail.4 In medical research such “ingredients” would be dose, frequency, monitoring, titration, mode of delivery, and duration of use of which all can influence efficacy and safety of the interventions.4 With no such details, a study cannot be replicated and results cannot be implemented in daily dementia care. Therefore, it is necessary to develop and strengthen the field of research currently termed nonpharmacological dementia care. This demands clear explications including methods, routines, habits, and tacit knowledge for other professionals to be informed about best practice and assure implementation where it is needed.
The “ingredients” of nonpharmacological interventions should not be compared with medication although the focus on personalized, stratified or precision medicine has brought new perspectives on the variations of responses to medication and ruled out a simple cause/effect-relationship to medical treatment.5 All interventions may thus be considered complex. However, for clarity, we define it as a continuum of interventions with simple interventions of single-component actions on the one end, and complex interventions on the other consisting of multicomponent psychosocial methods with several interacting components. Some psychosocial interventions may be described by a clear manual but for complex interventions of a person-centered, relational, psychotherapeutic and/or ecopsychosocial nature, it is highly challenging to narrow down actions and responses in a serial order of events and capture simple interconnections between them.6–8 The level of complexity increases further when interventions are not a planned session-based service, but an interaction intended to be implemented as required or PRN (pro re nata. From Latin, meaning in the circumstances or as the circumstance arises.) in daily care. While manuals informing caregivers to conduct defined activities or sessions with persons with dementia exist,9,10 there is a pressing need to also describe the details of complex interventions in manuals in order to strengthen research in the broad spectrum of ecopsychosocial interventions.
For manuals in the area of activities, therapy or daily care, the aim is to provide a consistent and effective treatment compared to relying on idiographic knowledge, subjective feelings, and tacit or non-defined intentions of different therapists and caregivers.11 When it comes to interventions for so-called non-cognitive symptoms and changed behaviour, the NICE guidelines recommend interventions to be tailored to the person’s preferences, skills and abilities, as some may respond better to one treatment than another.1,12 Also, the manual needs to maintain a certain degree of flexibility. Flexibility can be applied by providing frameworks or directions rather than step-by-step instructions or a combination of both while maintaining a contained setting or time and place for the intervention such as a session.13
While reviews have been conducted to assess the availability and effectiveness of evidence-based training manuals and to inform the development of interventions,14–16 the purpose of this scoping review is to learn from research studies which have taken on the challenge to construct manuals for complex interventions carried out by caregivers and tailored to the preferences, skills, and abilities of the person with dementia. With this review, we aim to stress the importance of availability of manuals through refereed journals in order to inform future research in dementia care and improve clinical interventions and care. This is synthesized in the following research question:
How are manuals describing complex interventions in dementia care structured and disseminated in refereed journals, and what is important to consider for future manuals?
Method
The search followed the PRISMA extension for scoping reviews and the PRISMA-ScR checklist.17 Relevant search terms were identified, and searches conducted according to the PICo model (Population, Intervention, Context).18,19 A process of identifying search terms included brainstorming, pre-existing knowledge and the use of the thesaurus in each database. Using thesauruses allowed us to find and use controlled terms in order to ensure accuracy and a higher degree of consensus about terms within each database. Furthermore, it enabled us to control the process by narrowing or broadening the search. If no controlled terms existed or were not accurate enough, we used free-text searching either as a stand-alone strategy or together with controlled terms. To ensure a higher chance of detecting relevant results and when possible, we chose to use broader terms such as using the parent term “cognitive impairment”.
Search Strategy and Criteria
We conducted a systematic search on December 2nd 2016 which was repeated on April 8th 2019 using four databases; Embase, PsychInfo, CINAHL and Scopus and documented all searches and hits. These are available on request from the main author. The databases cover research in medicine, psychology, nursing and interdisciplinary research. The search terms were defined by the research question and the thesauruses in the databases and consisted of a range of controlled and open terms. For the final search terms, see Table 1. The search followed an un-published protocol available on request from the main author.
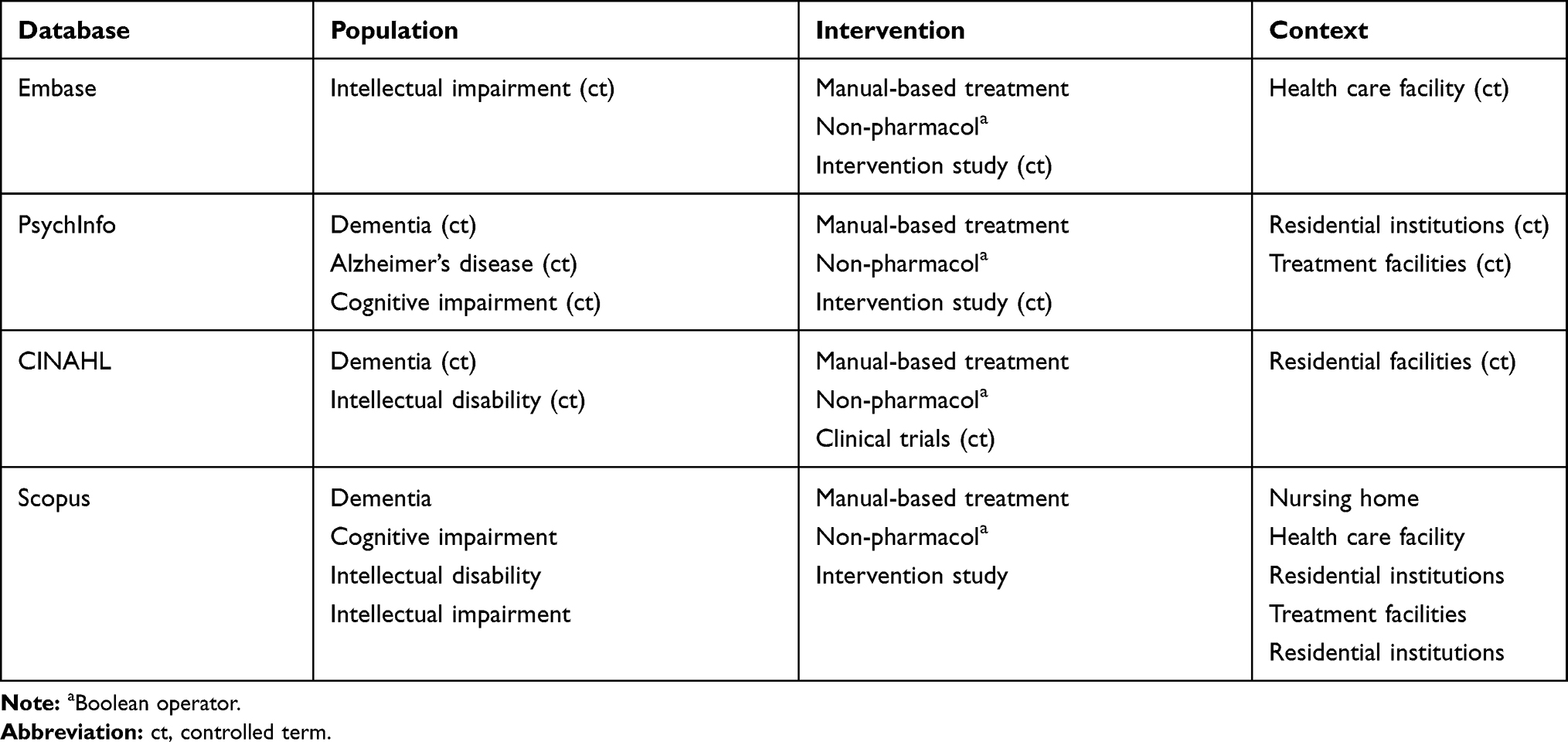 |
Table 1 Complete List of Final Search Terms |
The results were screened according to the inclusion and exclusion criteria presented in Table 2. The criteria allowed a broad search while maintaining a precise scope. We did not apply years of publication to limit the results. In order to maintain the chain of evidence, we kept track of the rationale for excluding papers by listing these in a spreadsheet.
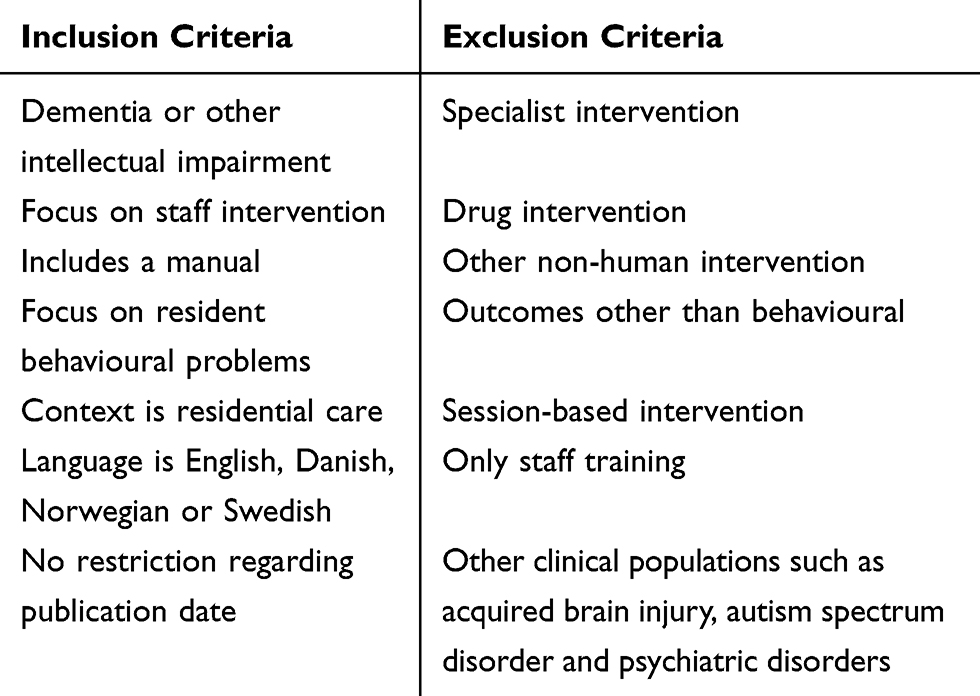 |
Table 2 List of Inclusion and Exclusion Criteria |
Analysis
The collected research studies and manuals were analysed using a phenomenological template analysis (TA). The focus of the analysis was not to explore the content of the manuals or their effectiveness, but to explore how researchers overcome complexity and tailor manuals for scientific purposes. Therefore, we applied a qualitative methodology. TA is the use of structured codes to analyse qualitative material, such as text. It differs from other phenomenological thematic analyses by defining the themes prior to the analysis. Where other methods require themes to develop “uniquely” and inductively during the analysis, TA establishes themes prior to or on the basis of a small part of the dataset. Next, subsequent pieces of data are then analysed according to these themes. TA is especially useful for studies with a clear focus and emphasis on similarities across the included material.20
In this study, the TA was conducted according to the following 5-step procedure:
- Familiarization with selected pieces of data,
- Establishing template of themes,
- Applying the template to the full dataset,
- Selecting most relevant themes,
- Dividing each main theme into subthemes.
Besides focusing on characteristics of the studies, we analysed the possibility of tailoring the intervention,12 flexibility of the manual13 and dissemination elements used in the manual including illustrations and graphical organisers.21
Results
The sorting of the results is visualised in the flowchart in Figure 1.
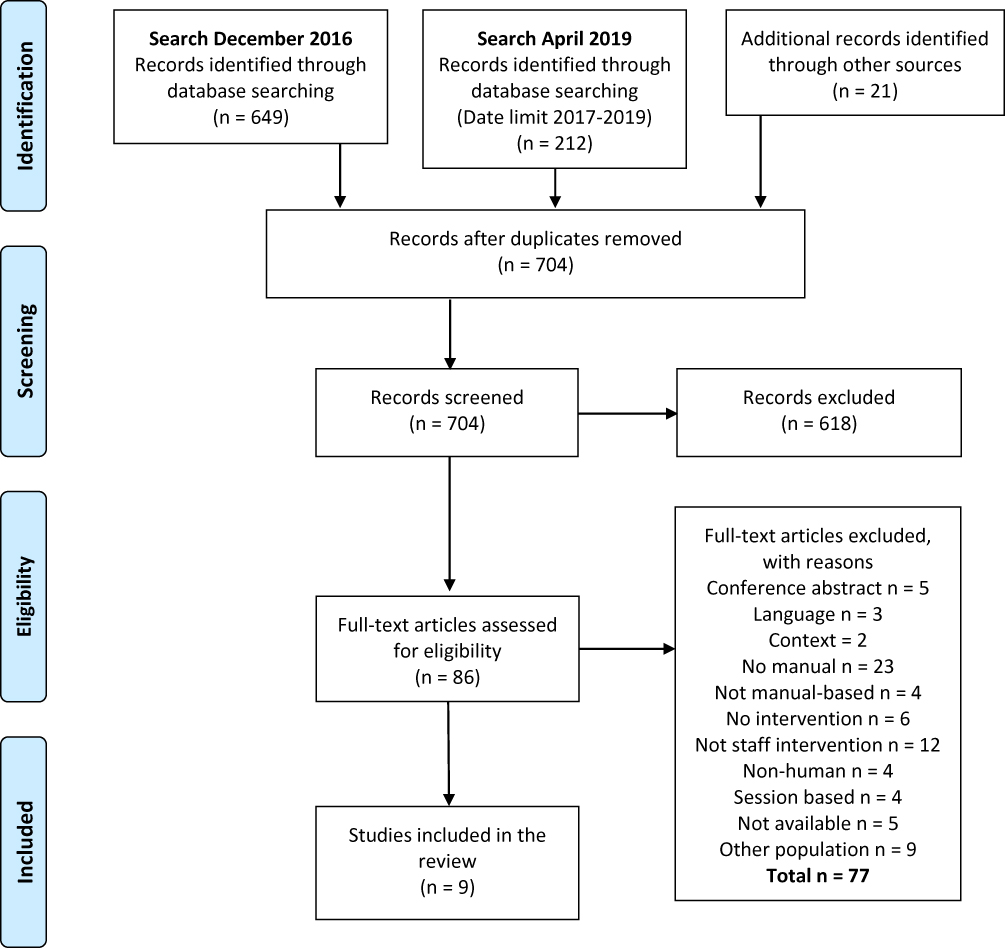 |
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) diagram. A full list of reasons for excluding records can be obtained from the main author.Notes: Adapted from Moher D, Liberati A, Tetzlaff J, Altman DG, et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009;6(7): e1000097. Creative Commons license and disclaimer available from: http://prisma-statement.org/PRISMAStatement/CitingAndUsingPRISMA.aspx.22 |
The search on the 2nd of December 2016 yielded 649 hits. The updated search conducted on the 8th of April 2019 was limited to include publications in the period 2016–2019 and yielded 212 hits. After including 21 additional potentially relevant records, we had a total of 882 hits. After removing 178 duplicates, we screened the titles and abstracts of 704 records adhering to the inclusion and exclusion criteria and excluded 618 records, the three most occurring reasons being focus on drug treatment, no focus on an intervention and focusing on issues other than behavioural. This led to a total number of 86 papers that were collected for full-text screening. We found that 77 of these papers did not meet the inclusion criteria, which left nine papers to be included in the template analysis.
Characteristics of the Included Papers
Table 3 summarizes the characteristics of the included papers. The papers served different purposes. Three papers focused on improving caregivers’ communicational, interactional and relational skills.23–25 The remaining six papers aimed at preventing or treating BPSD, arousal imbalance and the use of restraint.26–31 The users addressed by the papers were mainly professional caregivers. Four of the included papers reported results from RCTs, three were theoretical papers and the remaining two were a literature review and a quantitative, post-test only study. Seven of the included papers recommended training as part of using the content of the manual.
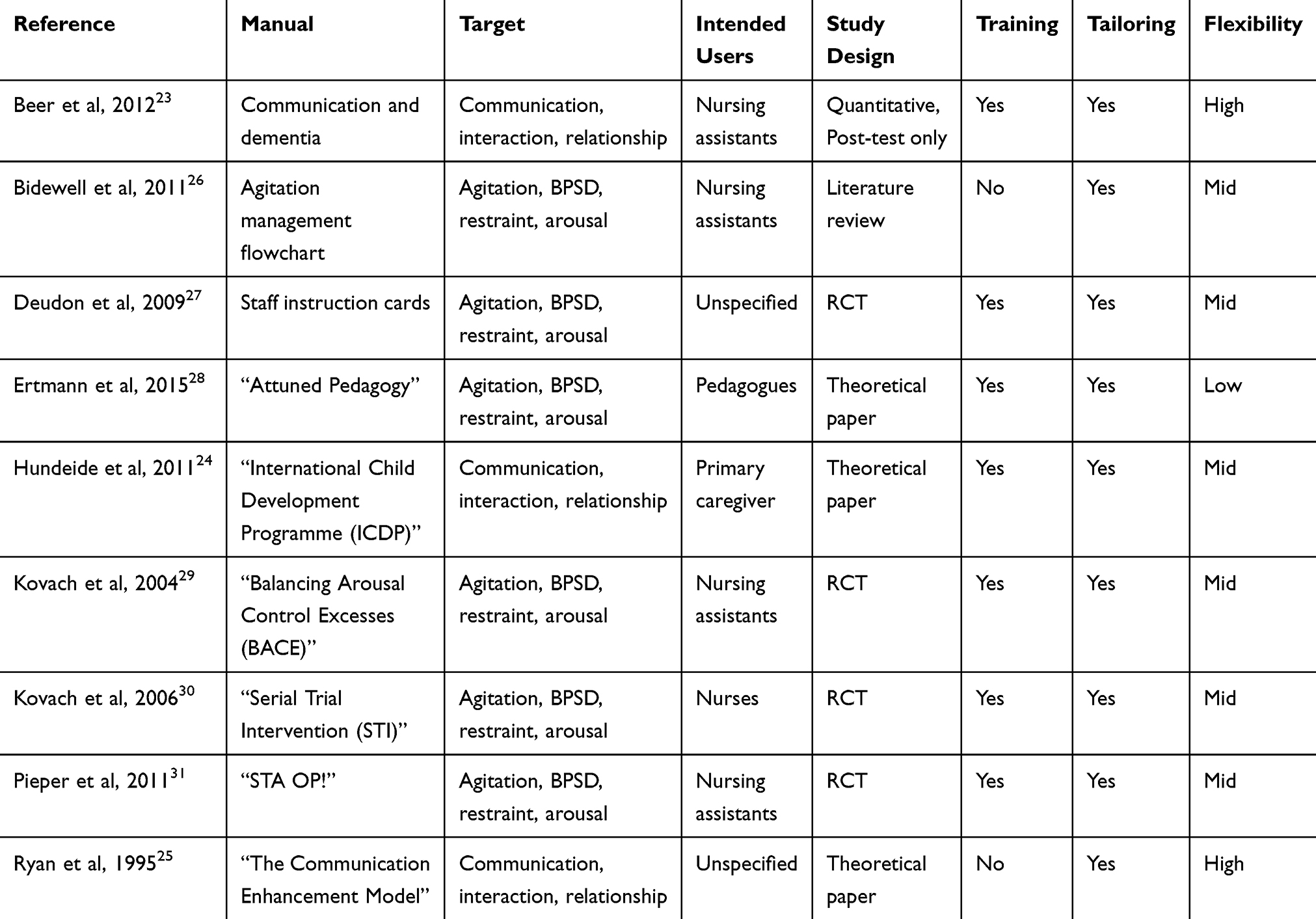 |
Table 3 Characteristics of Included Papers |
Tailoring and Flexibility
All of the manuals allowed or required the user to tailor actions in the intervention to the specific person with dementia. The degree of flexibility depends on the extent to which the manuals specify precise instructions about the content and may be described as either low, medium or high. A manual with a high degree of flexibility is not very directive and allows for many different actions, where a manual with a low degree of flexibility resembles a step-by-step protocol with clearly described actions that the user cannot and should not affect. A true step-by-step protocol could be described as having no flexibility.
Two manuals fit the “high” degree of flexibility category because they do not propose any hierarchy or order of how and what to do. One of them proposes a circular relationship emphasizing the scope of the manual without suggesting any actions or order of actions.25 The other manual within the category presents a range of suggested actions in various levels of detail23 without presenting any order to employ these in.
Six manuals are in the “medium” category. Five of these present a hierarchy of steps or phases with a specific order to follow.24,26,29-31 The manuals also include broad suggestions of actions on a meta-level, where the actions are not described in a highly detailed manner but are described broadly and vaguely. The last manual in this category does not include a clear-cut hierarchy but does include more detailed descriptions of the suggested actions.27
One manual is placed in the “low” category28 and includes descriptions of phases providing the user with suggested actions in various levels of detail. Furthermore, it includes a description of how the users should document and plan goals and interventions for the person in focus which enables tailoring while still maintaining rigor. However, this manual does not provide clear hierarchically ordered phases with all actions described in high detail.
Dissemination Elements
We analysed the dissemination elements in the manuals according to the following six themes; Media, Physical format, Graphical organisers, Illustrations, Hierarchical structure and Directing content (see Table 4).
 |
Table 4 Dissemination Elements in the Included Papers |
All nine manuals use written text as their media. The physical format of the manual is only described in one article, that being pocket-sized cards. One manual did not use graphical organisers. Different graphical organisers are used in the eight remaining manuals. These include lists (7 manuals), Headlines (6 manuals), Flowcharts (3 manuals), Boxes (1 manual), Tables (2 manuals) and Graphs (1 manual). However, none of the manuals make use of illustrations. Seven of the manuals organise their content in a hierarchical manner, where there is an ordered progression in the actions described in the manual. The remaining two manuals do not do this. Overall, the manuals direct the user by providing Directions (6 manuals), Suggestions (5 manuals), Do-nots (3 manuals), Questions (1 manual) and Examples (1 manual).
Discussion
With this article, our aim was to explore the structure of manual-based complex interventions within dementia care published in refereed journals, how they disseminate their content, and further discuss important factors to keep in mind when designing future manuals. The scoping review revealed nine publications adhering to the inclusion criteria and findings from the template analysis include characteristics of the studies as well as information about training, tailoring, degree of flexibility and dissemination elements. All manuals recommended users to tailor interventions to specific situations and most had a medium level of flexibility. All manuals used written text as the primary element of dissemination. While there was no use of audio/visual material or illustrations, a number of the manuals used graphical organisers such as lists and headlines and a few also used flowcharts, boxes, graphs and tables. A majority of included manuals organised their content in a hierarchical manner and provided users with directions and suggestions of what to do.
Users, Training and Tailoring
The intended users of the manuals included informal caregivers, “basic” caregivers, nurses and pedagogues suggesting that use of manuals is applicable across groups. Seven of the manual-based interventions also required or suggested training in relation to the content of the manual. All of the manuals allowed or suggested tailoring the content thus enabling users to adapt interventions to specific needs and the situation of the person with dementia. When considering persons with dementia as unique individuals with different challenges and resources, it seems vital that manuals are flexible enough to allow tailoring while also providing fixed steps or stages offering users a hierarchy or structure of the intervention. Combining tailoring and structure is done in seven of the included articles. To discuss the importance of this combination thoroughly, it seems relevant to analyse differences between manuals regarding applicability and user-friendliness. However, available data in the publications do not allow such an analysis.
Flexibility
The concept of flexibility in this study refers to how flexible the content of the included manuals is. Six of the included manuals can be labelled as having a medium level of flexibility, while two could be labelled as having a high level of flexibility and one as having a low level of flexibility. However, the manual that fit into the “low” category was not constructed as a strict protocol with tailoring not being allowed. In that sense, flexibility could have been even lower. Keeping in mind the idiographic nature of persons with dementia, it probably would not be sensible to construct such manuals considering nonpharmacological interventions. Interventions and users of the manual need to be able to adapt and respond to the actions and reactions of the person with dementia. A high degree of flexibility may, however, affect factors such as replicability and consistency, which can lead to an undesirable amount of heterogeneity when implementing interventions.
While deciding on an optimal flexibility level would require further research, we suggest that the optimal level achievable in this field could be to structure the intervention in hierarchical phases, providing users with suggestion of specific actions, detailed descriptions of them and a method of choosing the “appropriate” action for the given situation. Such a manual would ensure a certain amount of homogeneity whilst remaining flexible enough to allow for the needed adaptions in the interaction with individual persons with dementia.
Dissemination Elements
The primary means of disseminating manual content is through written text. There seems to be a lack of audio/visual material, which could potentially have been informative for the user. Body language, tone of voice and other non-verbal forms of communication potentially influencing the quality of interactions, could be disseminated more clearly through audio/visual material. The lack of audio/visual material might be due to formal requirements when publishing in academic journals, where artefacts such as pictures or videos might not be an option. However, electronic publications now make it possible to either include links to online video resources, references to “real-life” videos or pictures included as an appendix.
Some graphical organisers are present in different forms in several of the publications with a main purpose of structuring word messages for users, eg, by grouping related terms, illustrating processes described with words and highlighting key messages. Including actual illustrations in future publications could have an impact both on user’s ability to remember the content21 and providing a clear message of what the user is supposed to do.
Limitations
An obvious limitation to this review is the fact that it only includes material available through academic databases. Manuals published outside of this area were not included which could have increased the amount of information in this review. However, this limitation also highlights the potential issue of not being able to publish manuals or reduced editions in refereed journals, thereby reducing the accessibility to fellow researchers.
Conclusion
We conducted this scoping review for the purpose of investigating how manual-based complex interventions in dementia care are structured and disseminated in refereed journals including what to consider for future manuals. Even though complex interventions in dementia care require the caregiver to execute different and complex actions where non-verbal elements are important, the primary language of dissemination is currently through written text. When developing future manuals, we suggest considering using illustrations or audio/video material to allow for a more detailed dissemination and provide users with directions of what to do while maintaining flexibility and allowing users to tailor interventions to the specific situation.
While it can be desirable to obtain a high degree of homogeneity in manuals when wanting to ensure reliability and consistent treatment, manuals need to have a certain degree of flexibility to allow tailoring and adaption in order to address the idiographic and changing needs of different people with dementia. Based on this review, we recommend that manuals describing complex interventions maintain a medium to low degree of flexibility and map and structure interventions in a hierarchical order with suggestions of actions relevant for each step, allowing users to tailor the intervention. Actions should be described in high detail and audio/video material as well as illustration and graphical organizers could be useful to ensure better understanding of some actions. Finally, the manual should include information on how to choose between different actions. Based on the results of this review, we also suggest that training should be provided in conjunction with manuals. Future reviews could use the themes (Tailoring, Flexibility and Dissemination Elements) generated from this review to analyse manual-based complex interventions in the field of dementia published outside of academically journals possibly leading to a greater understanding of the field and providing researchers and clinicians guidelines concerning the construction of a clinical manual.
Acknowledgments
This work was supported by the Velux Foundations under Grant number 10346.
Disclosure
Mr Jens Anderson-Ingstrup report grants from Velux Foundations, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. NICE. Dementia: supporting people with dementia and their carers in health and social care. Clinical guideline [CG42]; 2016. Available from: https://www.nice.org.uk/guidance/cg42.
2. NICE. Dementia: assessment, management and support for people living with dementia and their carers [NG97]; 2018. Available from: https://www.nice.org.uk/guidance/ng97/evidence/appendix-l-research-recommendations-pdf-174697045527.
3. Vasse E, Vernooij-Dassen M, Cantegreil I, et al. Guidelines for psychosocial interventions in dementia care: a European survey and comparison. Int J Geriatr Psychiatry. 2012;27(1):40–48. doi:10.1002/gps.2687
4. Hoffmann TC, Erueti C, Glasziou PP. Poor description of non-pharmacological interventions: analysis of consecutive sample of randomised trials. BMJ. 2013;347(7924):1–10. doi:10.1136/bmj.f3755
5. PMC. The Personalized Medicine Coalition. The personalized medicine report. Opportunity, challenges, and the future; 2017. Available from: http://www.personalizedmedicinecoalition.org/Userfiles/PMC-Corporate/file/The_PM_Report.pdf. Accesed June 23, 2018.
6. Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new medical research council guidance. BMJ Clin Res Ed. 2008;337:a1655. doi:10.1136/bmj.a1655
7. Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new medical research council guidance. Int J Nurs Stud. 2013;50(5):587–592. doi:10.1016/j.ijnurstu.2012.09.010
8. Zeisel J, Reisberg B, Whitehouse P, Woods R, Verheul A. Ecopsychosocial interventions in cognitive decline and dementia: a new terminology and a new paradigm. Am J Alzheimers Dis Other Demen. 2016;31(6):502–507. doi:10.1177/1533317516650806
9. Spector A, Thogrimsen L, Woods B, Orrel M. Making a Difference: An Evidence-Based Group Programme to Offer Cognitive Stimulation Therapy (CST) to People with Dementia. Wandsworth, UK: Hawker Publications Ltd.; 2006.
10. Barrick AL, Rader J, Hoeffer B, Sloane PD, Biddle S. Bathing Without a Battle.
11. Wilson GT. Manual-based treatments: the clinical application of research findings. Behav Res Ther. 1996;34(4):295–314. doi:10.1016/0005-7967(95)00084-4
12. Tonga JB, Karlsoeen BB, Arnevik EA, Werheid K, Korsnes MS, Ulstein ID. Challenges with manual-based multimodal psychotherapy for people with Alzheimer’s disease: a case study. Am J Alzheimers Dis Other Demen. 2016;31(4):311–317. doi:10.1177/1533317515603958
13. Heimberg RG. Manual-based treatment: an essential ingredient of clinical practice in the 21st century. Clin Psychol Pract. 1998;5:387–390. doi:10.1111/j.1468-2850.1998.tb00159.x
14. Fossey J, Masson S, Stafford J, Lawrence V, Corbett A, Ballard C. The disconnect between evidence and practice: A systematic review of person-centred interventions and training manuals for care home staff working with people with dementia. Int J Geriatr Psychiatry. 2014;29(8):797–807. doi:10.1002/gps.4072
15. Jennings AA, Foley T, Walsh KA, Coffey A, Browne JP, Bradley CP. General practitioners’ knowledge, attitudes, and experiences of managing behavioural and psychological symptoms of dementia: a mixed-methods systematic review. Int J Geriatr Psychiatry. 2018;33(9):1163–1176. doi:10.1002/gps.4918
16. Tang WK, Chan CYJ. Effects of psychosocial interventions on self-efficacy of dementia caregivers: A literature review. Int J Geriatr Psychiatry. 2016;31(5):475–493. doi:10.1002/gps.4352
17. Tricco AC, Lillie E, Zarin W, et al. Preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews (PRISMA-ScR) checklist. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
18. Danish Ministry of Health. Model for Development of National Clinical Guidelines; 2014.
19. Joanna Briggs Institute. Joanna Briggs Institute Reviewers’ Manual: 2014 Edition; 2014.
20. Brooks J, McCluskey S, Turley E, King N. The utility of template analysis in qualitative psychology research. Qual Res Psychol. 2015;12(2):202–222. doi:10.1080/14780887.2014.955224
21. Levie WH, Lentz R. Effects of text illustrations: a review of research. ECTJ. 1982;30(4):195–232.
22. Moher D, Liberati A, Tetzlaff J, et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009;6(7): e1000097. doi: 10.1371/journal.pmed1000097.dd
23. Beer EL, Hutchinson RS, Skala-Cordes KK. Communicating with patients who have advanced dementia: training nurse aide students. Gerontol Geriatr Educ. 2012;33(4):402–420. doi:10.1080/02701960.2012.702165
24. Hundeide K, Armstrong N. ICDP approach to awareness-raising about children’s rights and preventing violence, child abuse, and neglect. Child Abuse Negl. 2011;35(12):1053–1062. doi:10.1016/j.chiabu.2011.09.008
25. Ryan EB, Meredith SD, Maclean MJ, Orange JB. Changing the way we talk with elders: promoting health using the communication enhancement model. Int J Aging Hum Dev. 1995;41(2):89–107. doi:10.2190/FP05-FM8V-0Y9F-53FX
26. Bidewell JW, Chang E. Managing dementia agitation in residential aged care. Dement Int J Soc Res Pract. 2011;10(3):299–315. doi:10.1177/1471301211407789
27. Deudon A, Maubourget N, Gervais X, et al. Non-pharmacological management of behavioural symptoms in nursing homes. Int J Geriatr Psychiatry. 2009;24(12):1386–1395. doi:10.1002/gps.2275
28. Ertmann B, Woetmann CZ, Pejstrup S-E, Fischer E. Afstemt Pædagogik - Metodebeskrivelse Del II: Praktisk Gennemgang. 2015.
29. Kovach CR, Taneli Y, Dohearty P, Schlidt AM, Cashin S, Silva-Smith AL. Effect of the BACE intervention on agitation of people with dementia. Gerontologist. 2004;44(6):797–806. doi:10.1093/geront/44.6.797
30. Kovach CR, Cashin JR, Sauer L. Deconstruction of a complex tailored intervention to assess and treat discomfort of people with advanced dementia. J Adv Nurs. 2006;55(6):678–688. doi:10.1111/jan.2006.55.issue-6
31. Pieper MJ, Achterberg WP, Francke AL, van der Steen JT, Scherder EJ, Kovach CR. The implementation of the serial trial intervention for pain and challenging behaviour in advanced dementia patients (STA OP!): a clustered randomized controlled trial. BMC Geriatr. 2011;11:12. doi:10.1186/1471-2318-11-12
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.