")
Back to Journals » Patient Preference and Adherence » Volume 17
A Review on the Application of Hospice Care in Patients with Advanced Cancer
Authors Li X, Bai F, Liu X, Yang G
Received 8 August 2023
Accepted for publication 31 October 2023
Published 8 December 2023 Volume 2023:17 Pages 3219—3231
DOI https://doi.org/10.2147/PPA.S434509
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Qizhi (Cathy) Yao
Xiaoyu Li,1 Feng Bai,2 Xinmei Liu,1 Guangyu Yang1
1Department of Otorhinolaryngology Head and Neck Surgery, First Hospital of Jilin University, Changchun, People’s Republic of China; 2Department of Otorhinolaryngology Head and Neck Surgery, the Second Hospital of Jilin University, Changchun, People’s Republic of China
Correspondence: Guangyu Yang, Department of Otorhinolaryngology Head and Neck Surgery, First Hospital of Jilin University, No. 1 of Xinmin Street, Chaoyang District, Changchun, 130021, People’s Republic of China, Tel +86-43188785539, Fax +86-43188785505, Email [email protected]
Abstract: Hospice care is to improve the quality of life and help patients die comfortably, peacefully and dignified by controlling pain and discomfort symptoms and providing physical, psychological and spiritual care and humanistic care in the final stage of the patient’s life. Hospice care clients were primarily cancer patients at first and then slowly extended to other critically patients. Hospice care can alleviate the physical, psychosocial and mental problems of patients with advanced cancer, meet the diversified and multi-level health service needs of patients, improve the quality of life of patients and their families, and also save medical expenditure and improve the efficiency of medical resources. At present, there were few studies on hospice care for Chinese patients with advanced cancer. In this study, the needs of hospice care for patients with advanced cancer were reviewed from physical comfort and pain reduction, dignity maintenance, social support, and help calm death, and specific screening and evaluation tools for hospice care for patients with advanced cancer. And this study was summarized to review the influencing factors of hospice care in order to provide a reference for clinical hospice care practice for patients with advanced cancer in China.
Keywords: advanced cancer, hospice care, influencing factors, clinical practice, evaluation tools
Introduction
Advanced cancer refers to cancer in which treatment is no longer effective, and the disease is considered difficult to cure, and the patient’s condition is gradually deteriorating.1 Cancer is one of the major diseases that seriously threaten human health, and its incidence continues to increase.2 With the development of medical technology, the terminal stage of advanced cancer patient life may be prolonged, but it has not significantly succeeded in improving the cure rate of cancer.3 With the development of medical technology, the life of patients with advanced cancer is prolonged, but the physical function of patients is declining, the quality of life is decreasing, and the degree of dependence on the lives of caregivers is becoming stronger. At the same time, patient privacy is not protected, due to the lack of independent mobility, patients need to be cared for all the time, lack privacy space and time. This leads to a gradual loss of the patient “s self-worth, causing the patient” s self-esteem to decline and dignity to be compromised.4 According to statistics, in 2020, there were 19.29 million new cases of cancer and 10 million deaths each year worldwide.5–7 In China, there were 4.29 million new cancer cases and more than 2.8 million deaths among cancer patients in 2015.8 Cancer is the leading cause of death in China, with a mortality rate of 164.35/100,000 in urban residents and 154.98/100,000 in rural dwellers. In addition, the number of cancer deaths in China increased by 73.8% from 2000 to 2011, and the number of people requiring hospice care surged.8 In 2017, China issued the Guidelines for Practice of Hospice Care (Trial). Patients can obtain hospice care services if they meet the following conditions: (1) end-stage disease, symptoms. (2) refuse examination, diagnosis, and treatment of the primary disease. (3) The concept of receiving hospice care has the demand and willingness of hospice care. This study summarized the hospice care needs of patients with advanced cancer and the current situation of hospice care, and analyzed the influencing factors of hospice care needs in order to provide a reference for better clinical practice of hospice care.
Life Status of Patients with Advanced Cancer
In terms of health service utilization, it is very common for patients to receive aggressive treatment at the end stage of life. As death approaches, the proportion of patients using chemotherapy, emergency department, hospitalization, and ICU increases dramatically during the three months before patient death.9–11 Up to 91.97% of urban patients with advanced cancer were hospitalized in the last trimester of life, with 2.13 hospitalizations per capita and 41.13 hospitalizations per capita, and 72.19% of rural cancer patients were hospitalized, with 2.02 hospitalizations per capita and 27.22 hospitalizations per capita in China.12 Chemotherapy is a common method used for palliative care in patients with advanced cancer, which can reduce the patient’s pain and play a role in slowing the further progression of advanced cancer. The proportion receiving chemotherapy in the last month increased by 14% compared with the last two months of patient life,13 and in the last month of life, about 20% of patients received chemotherapy or radiotherapy, and about 10% used the ICU.11 In terms of medical costs, the average cost of treatment for cancer is as high as $ 14,000 – $ 52,000, far exceeding $ 7000 – $ 28,000 for general major diseases in China. With the development of the disease course, the cost of cancer treatment is distributed in a U-shaped pattern,14–16 and during cancer treatment, the second year after diagnosis and the last year of life are the periods of the most intensive resources and costs, and the cost rises dramatically as death approaches.17 Treatment costs occurring in the last trimester of life of cancer patients account for approximately 40% of overall health care expenditures, with hospital costs accounting for approximately 70% of overall end-of-life costs.12 There is still a dearth of research on hospice care and place of death in terms of place of death. Influenced by the development of modern medicine, the proportion of hospice deaths in Chinese hospitals increased from 19.84% in 2005 to 37.56% in 2008.18,19 However, there have not been any national reports in recent years regarding the location of population-based deaths. In terms of quality of life, the quality of life of patients with advanced cancer at the end of life is worrisome, there is a very low sense of well-being, often bearing symptoms such as pain, loss of appetite, fatigue, weakness and dyspnea, and psychological stress.20 Palliative services are underutilized, and palliative care has been received in a very low proportion of cancer patients in mainland China (2.68% - 12.31%).12 In summary, patients with advanced cancer have excessive medical treatment, high medical costs, poor quality of life, and palliative care services are not fully utilized during the end of life. The vast majority of patients with advanced cancer suffer from “economic poverty”, “physical poverty” and “mental poverty”, which together cause “end-of-life poverty” in patients with advanced cancer.21 It is urgent to improve the quality of hospice care for patients with advanced cancer and get them out of “poverty at the end of life”.
Current Status of Hospice Care
The concept of end-of-life care first originated in England. The world ‘s first modern hospice facility was built in England in 1967 and is staffed by British senior nurse Cicily Sanders.22 In the 1970s and 1980s, the concept of end-of-life care spread from the United Kingdom to other countries, while new thinking, change suggestions, and various debates on active treatment, end-of-life, location of death, and quality of death formed a rather influential Good Death Movement. In the 1990s, the World Health Organization placed hospice care on the agenda of work as one of four priorities.23 The advent of hospice care marks the ultimate formation of a modern health care system.24 At present, patient-centered palliative care and hospice care have become very popular in most developed countries such as the United Kingdom, Australia, the United States, Canada, and other countries, for example, the United Kingdom Health Department established the National Hospice Care Program in 2004, and subsequently issued a series of national strategy documents to incorporate hospice care into the health insurance system (NHS) and social welfare system.25 There are more than 5800 hospice hospitals and facilities in the United States, 56% of which provide home hospice care services. In 2015, 1381,182 Medicare beneficiaries had received hospice care services: about 46% of hospices had received at least one day of hospice care before death and died at hospice hospitals.26 In a report by the National Commission on Hospice Care, Near Death: Improving Hospice Care, it is recommended that all physicians throughout the vast healthcare system in the United States should be educated about death.27 At present, hospice care in China is still in its infancy. In the 1990s, China firstly established a hospice care institution in Tianjin, marking the beginning of hospice care in China. In 2017, China issued the Guidelines for the Practice of Hospice Care (Trial) and the Basic Standards and Management Specifications for Hospice Care Centers (Trial), which put forward guidelines for the number of beds, department setting, staffing, building requirements, equipment configuration and other hardware facilities in Hospice Care Centers, and developed specifications for software services such as symptom control, comfort care, psycho-psychiatric and social support in Hospice Care Centers. The promulgation of these documents has standardized hospice care in China.
Assessing the needs of patients with advanced cancer is one of the key issues in palliative care and is the basis for providing personalized care. Need assessment can identify areas that patients believe are important and where they need help and support and provide precise intervention, thereby improving their physical and mental health and care satisfaction, and further improving the quality of care for cancer patients, and failure to fully meet the needs of patients can seriously affect the quality of life of end-of-life patients.28–30 The needs of patients vary according to their disease diagnosis and different stages of disease development. If some studies have pointed out that for patients with end-stage chronic diseases, social needs are particularly important, while for patients with end-stage cancer, physical symptoms, opportunities to share emotions and religious needs are more important. Nurses should prepare to talk about death, existence and mental problems with patients when providing care for patients with end-stage cancer.31
Advanced cancer care needs vary according to age, sex, cancer type, personal expectations, and existing palliative services. Continuous, systematic, personalized needs assessment is the core of hospice care, and can accurately assess the needs of patients through effective communication with patients, caregivers, nursing staff, and health professionals to reduce symptom distress, improve daily function, and quality of life. Vivian et al32 investigated the quality of life, disease-related and treatment-related symptoms, and unmet needs of 102 patients with advanced ovarian cancer who survived at least 6 months using the Cancer Patient Need at the End⁃of-life Screening Tool (NEST), and the results showed that the most common disease-related symptoms of patients with advanced cancer were fatigue (92%), anxiety (89%), and sleep difficulties (76%), and the most common unmet needs were symptom dimensions. Buzgova et al33 evaluated palliative care needs in 349 in patients with advanced disease using the Patient Needs Assessment in Palliative Care (PNAP) and showed that patients had the lowest satisfaction with physical symptoms, and other unmet needs included continuing normal activities (44%), having the opportunity to participate in religious or other ceremonies (36%), fatigue (32%), fear of relying on help from others (26%), and sharing feelings about death and dying (16%). A systematic review conducted in 2016 by Moghaddam et al34 included 23 studies and showed that unmet needs were identified in many areas, with information (30% to 55%), psychology (18% to 42%), physical (17% to 48%), and function (17% to 37%) being prevalent. Because there is considerable heterogeneity in the evaluation methods and reporting methods of hospice care needs of patients with advanced cancer, it is difficult to carry out homogenization analysis. At the same time, the differences in the performance between studies also explain the importance of personalized evaluation of hospice care needs.
Needs Assessment Tools for Hospice Care
Problems and Needs in Palliative Care
Problems and Needs in Palliative Care (PNPC) was developed by Osse et al35 in 2004 and consists of two parts: the problem part and the care needs. It contains activities of daily living, physical symptoms, role activities, economic/administrative problems, social problems, psychological problems, spiritual problems, autonomy, nine dimensions of information needs, 138 items, each item determines whether it is a patient ‘s need through two questions: ① whether this is a problem for you; ② whether you need professional help for this problem. A higher score indicates a greater need for end-of-life care. Cronbach′s α coefficient of the scale ranged from 0.65 to 0.70. In 2007, Osse et al36 developed a simple scale PNPC-sv, which was reduced to 33 items. The scale was more concise and could more quickly and effectively identify the problems affecting the quality of life and nursing needs of patients, with good universality and reliability. In 2019, Wang et al37 conducted a Chinese version of this scale and verified the applicability of the Chinese version of PNPC-sv in the assessment of hospice care needs in patients with advanced cancer, with a Cronbach′s α coefficient of 0.88 and an average completion time of 11 min. The PNP-sv operation method is simple and easy to understand. This scale is not only helpful to evaluate the needs of cancer patients for hospice care, but also helps to clarify the degree of needs of patients for help, and can help medical staff determine the needs of cancer patients, so that the diagnosis, treatment and nursing measures are better closely related to the needs.
Palliative Care Needs Assessment Tool
Palliative Care Needs Assessment Tool (PC-NAT) was developed in 2008 by Australian scholar Waller et al38 to assess the care needs of patients with advanced cancer and caregivers, and consists of five parts, the first part is a review of professional palliative care services, including three items, that is, whether there is a lack of caregivers, whether patients or caregivers request referral to professional palliative care services, and whether health professionals have needs in providing professional care. Part 2 consists of 7 items assessing the patient’s physical condition, including physical condition, functional status change, psychological, informational, spiritual/existential, health beliefs/cultural/social, economic/legal aspects. Part 3 is to assess the ability of the caregiver/family primary caregiver and consists of five items, namely physical condition, functional status change, psychological, information, family, and relationship aspects. Part 4 assesses the health status of the caregiver and includes 2 items, namely physical, psychological problems and grief at bereavement. Part 5 consists of an item assessing whether the patient needs further intervention by a special palliative care service. The response options for Parts 1 and 5 were “Yes” or “No”; items in Parts 2 through 4 were assessed with “None”, “Sometimes”, “Very” based on the level of concern they aroused. Waller et al39 validated the validity, reliability, and clinical feasibility of PC-NAT in the needs assessment tool for patients with advanced cancer in 2010. PC-NAT does not have a specific scoring system, given the differences in the ability of the professionals involved to provide the patient with the care required. PC-NAT can help health professionals identify unmet needs of patients and thus implement service interventions that are more closely linked to needs.
Hospice Care Needs Questionnaire for Cancer Patients
Hospice care needs questionnaire for cancer patients was developed by Wu Honghan et al40 in 2020 to evaluate the care needs of hospice care patients and consists of a total of 28 items, which are divided into six dimensions: physical, psychological, environmental, social support, disease-related knowledge and information needs. A total of 198 patients with advanced cancer were investigated by questionnaire. The results showed that the Cronbach′s α coefficient of the questionnaire was 0.934, and the Cronbach′s α coefficient of each factor was 0.789 ~ 0.900. The results showed that the internal consistency of the questionnaire was good, the test-retest reliability of the questionnaire was 0.907, and the test-retest reliability of each factor was 0.737 ~ 0.896, indicating that the questionnaire had good stability and could be used as an evaluation tool for the safety care needs of cancer patients. At present, the questionnaire has only been validated in 198 patients with advanced cancer, and larger sample studies are needed to verify the generality of the questionnaire in the future.
Anxin Card
Anxin Card is a poker card designed by Chen Minghui, head of Chinese American Coalition for Compassionate Care (CACCC) in 2014 to meet Chinese cultural characteristics based on end-stage patient care needs. Anxin card contains 54 cards, each describing a desire for end-of-life. Among them, spades, red hearts, plum blossom, and squares represent physical needs, spiritual needs, interpersonal needs, and financial needs, respectively, and additionally contain two special desire cards.41 The content on the peace card can guide patients to think about their important life issues and provide a reference for the development of advance care plans. Litzelmn et al42 carried out a feasibility study of Anxin Card in 33 patients to identify the care needs and goals of end-of-life patients and showed that Anxin Card could promote the importance of patients considering common care problems at the end of life in an impedance free environment compared with traditional methods, and could efficiently and accurately determine the end-of-life care goals of patients, laying the foundation for the development of advance care plans. Delgado Guay et al43 used a randomized controlled trial to compare the effectiveness of different tools in assessing patients’ end-of-life wishes between the two groups, and the results showed that there was no significant difference in desire selection between the Anxin Card group and the conventional group, and Anxin Card as a tool for “death education” did not increase patients’ death anxiety. At present, the application of Anxin Card Activity in critically ill patients in some areas of China and American Chinese is more popular.44 Cheng Fang et al45 carried out peace of mind tea activities in 33 patients with lung cancer and shared their experiences. The results showed that peace of mind tea house activities could assist in opening the door of patient death education and have a significant effect in understanding the wishes of lung cancer patients at the end of life.
Need at the End⁃of-Life Screening Tool
Need at the End-of-life Screening Tool (NEST) was developed by Emanuel et al46 in 2001 for brief screening of hospice clinical needs. The instrument consists of 13 items, and four themes corresponding to each letter of the NEST were assigned for ease of memory, namely social demands, concerns present, symptoms, and therapeutic interactions. Screening usually consists of 2 levels, the first level is screening through these 13 items, each question assesses the degree to which different needs are met from the patient ‘s perspective, and the subject scores each item in the range of 0 to 10, with higher scores indicating higher severity of needs. Level 2 evaluation refers to further evaluation of 48 questions that are extended by these 13 questions. Studies have shown that the tool has a sensitive and reliable bedside problem and can quickly screen and evaluate the overall care requirements of patients at the end of life. The use of this screening tool can improve the patient care needs record, improve the nursing process according to the patient ‘s needs, and improve the nursing results and nursing quality.
Patient Needs Assessment in Palliative Care
Patient Needs Assessment in Palliative Care (PNAP) is a scale developed by Buzgova et al33 by assessing the importance and satisfaction of the needs of patients receiving hospice care services and consists of 40 items and 7 dimensions, including physical symptoms, social domains, respect and support by health professionals, meaning of life, autonomy, opportunities to share emotions, and religious needs. Each item is asked to answer questions on both importance and satisfaction, with the question “In the past week, the importance of this item for you”, which is assessed using the Likert 5-level scoring method, ranging from “not at all important” to “very important” in 1 to 5 points; the question on satisfaction is “have you met this”, and the option is assessed using the Likert 5-level scoring method, ranging from “not met at all” in 1 to 5 points.47 PNAP has good acceptability, internal consistency and effectiveness, can accurately evaluate the needs of hospice care and demand satisfaction of patients, and helps medical staff to provide targeted diagnosis, treatment and nursing measures for patients. However, its long filling time may increase the burden on patients to answer questions. Currently, there is no translated or revised version of this scale, and subsequent large-sample, multicenter validation is lacking, and its clinical applicability needs further validation.
Resident Assess Instrument for Palliative Care
Resident Assess Instrument for Palliative Care (RAI-PC) is a standardized assessment tool developed by RAI-PC in 2003 to appropriately assess the needs of hospice patients and has been tested in Canada, Sweden, Spain, and the United States.48 The evaluation included basic information, medical history and health status, skin condition, oral cavity and nutritional status, communication, cognitive ability, mental health, functional status, mood, drugs, self-control, treatment and measures, responsibility/advance order, social support, evaluation information, and discharge.49 A systematic review by Kirsten et al50 in 2014 showed that the RAI-PC Hospice Assessment Scale met the requirements for multidimensional, fully humanized assessment of patients receiving hospice care.
Sheffield Assessment and Referral Care Scale
Sheffield Assessment and Referral Care Scale (SPARC) is a multidimensional screening tool to assess supportive care and end-of-life care needs for patients with advanced cancer, which contains 45 items: communication and information, physical symptoms psychological problems, religious and spiritual problems, independence and mobility, family and social problems, treatment, and personal problems.51 It provides a global assessment of cancer patients, facilitates patient understanding and follow-up tracking, and is suitable for patients of all ages and in inpatient, outpatient, and residential communities, with Cronbach′s α coefficients ranging from 0.65 to 0.86.52 Burton et al53 showed that the tool was also suitable for patients with acute stroke and interstitial lung disease.
There are few reports on the use of the above multiple assessment scales (Table 1) in China, and in order to promote the practice of hospice care in Chinese patients with advanced cancer, it is necessary to select the appropriate assessment scale according to different needs of patients. At the same time, an assessment scale suitable for Chinese patients should be developed according to the Chinese health care system as well as culture.
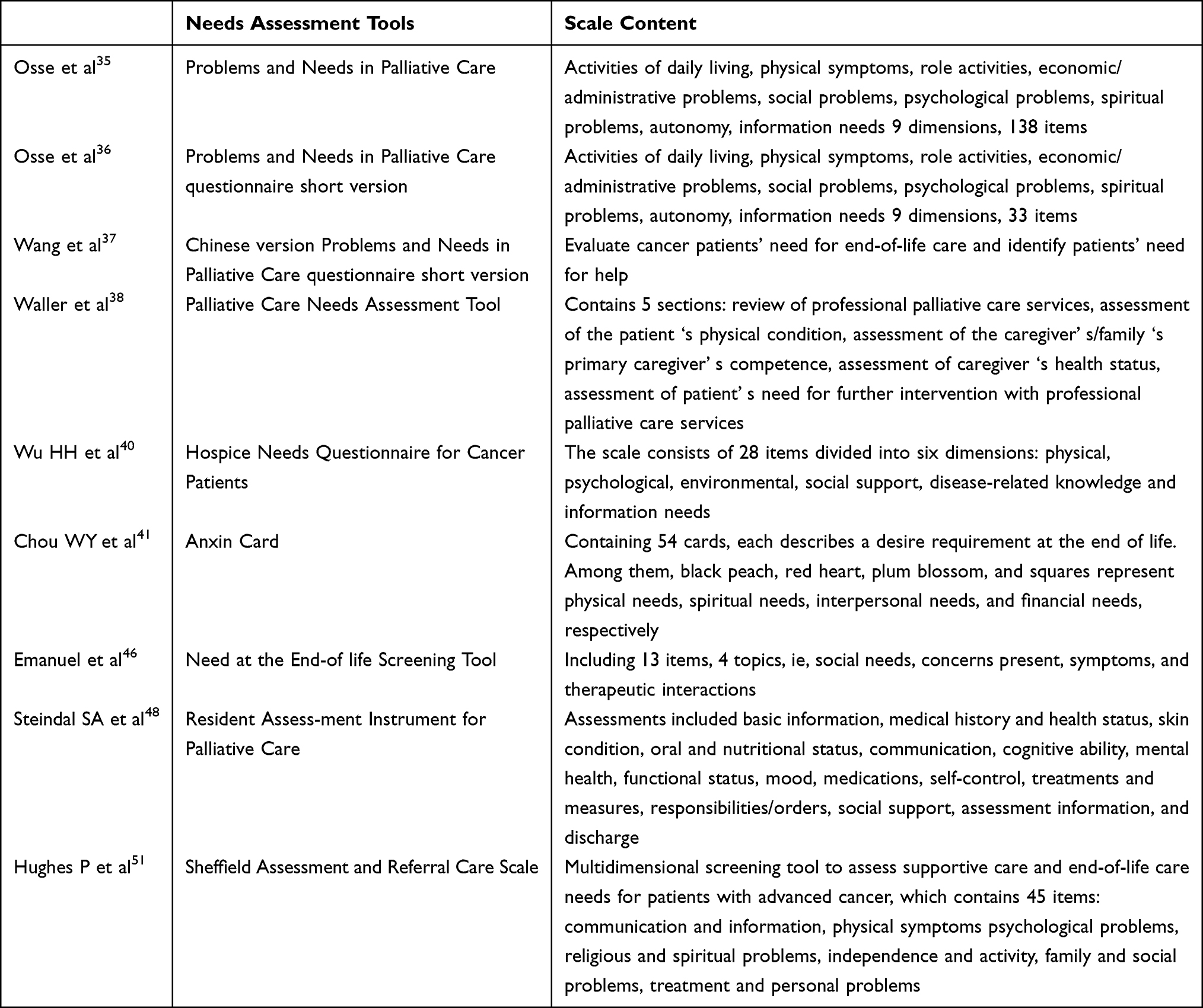 |
Table 1 Needs Assessment Tools for Hospice Care |
Implementation Effect of Hospice Care
Physical Comfort and Less Pain
The focus of care for patients with end-stage cancer in the final stages of life is no longer to treat the disease, but to make the patient painless and peacefully accept death. Zhuang Juping et al54 investigated the nursing needs of 128 patients with advanced cancer, and the results showed that patients with advanced cancer had a higher demand for hospice care, and the contents with a higher score in terms of physiological needs included ensuring sleep quality, effectively controlling pain, and keeping the skin and mouth clean and intact. Long-term disease distress and multi-cycle treatment bring great pain to patients, seriously affecting the daily life of patients, patients cannot walk for a long time, do housework, do leisure and recreational activities, and even lose their self-care ability, patients have to rely on others, will make patients feel helpless.55 In the process of implementing basic care, the needs, experiences and feelings of patients should be respected, and the main caregivers of families should be encouraged and instructed to participate in the comfort care of end-of-life patients, enhance companionship and emotional communication, and achieve the purpose of maintaining cleanliness and comfort, maintaining dignity, and ensuring safety. Masel et al56 learned through in-depth interviews with advanced cancer patients and palliative care teams that the placement of green plants in a convalescent environment can positively stimulate patients, arouse good memories of patients, and distract patients. In addition, family members can be added to the ward setting to visit the companionship place to avoid the patient died without relatives companionship regret. In the choice of place of death, some patients prefer to die alone, hoping that the heart is calm and the environment is quiet, while some patients hope to spend the last time at home in places they like and are safe, and some are willing to choose to spend the last time at home, with loved people accompanied around them.57 It is suggested that the physical environment of hospice ward and hospice convalescent institution should be designed with the concept of humanistic care and fully meet the physical, psychological and social needs of patients.
Maintaining Dignity
Seeking meaning of life is the main impetus of human life, and different stages of life have different pursuits. The process of finding meaning of life is to find the value of self-existence again, so as to produce a sense of identity with their own life. Geller et al58 showed that active search for life significance can achieve harmony and stability in all aspects of the patient ‘s body, psychology and spirit, and face death with dignity and achieve a good end. Patients hope that they will not become a burden on their families,59 and patients hope to maintain clear thinking during daily activities. We hope to be able to play their own value for the family to do their own responsibility, for the family to make future life arrangements. Emily et al60 found through multiple in-depth interviews with patients with advanced lung cancer that life significance is an important content affecting the quality of life of patients, and finding life significance can help patients find the reasons, hope and sense of accomplishment of life, and achieve self-transcendence. With the increasing awareness of public rights protection, the call to protect the right to know the patient is increasing, and the patient urgently hopes to understand the condition of the disease, medical measures and medical risks. Only after full informed consent, the patient may make choices conducive to himself/herself and in line with his/her wishes. Konstantinidis et al31 conducted an in-depth interview with 95 patients with advanced solid tumors and pointed out that 73.7% of patients wanted to understand their disease information, 56.8% wanted to understand their treatment information, 51.6% wanted to understand their examination information, and 50.5% wanted to understand their diagnostic information, especially patients living in cities or regions farther away from the hospital had a higher demand for information. A systematic review published in 2019 reviewed end-stage patient expectations and needs for death, in which the patient ‘s dignity needs mentioned that many patients crave attention to their right to know and that patients felt entitled to decide when they chose to stop treatment.61 There are also many patients who want to understand their disease diagnosis results, which is conducive to them to well arrange their uncompleted matters, see the person who wants to see, make arrangements for their own aftermath, and make full preparations for dealing with family internal problems, financial problems, and death.
Calm Death
Some religions believe that the end of life is only a process of life, not the end of life. Terminal patients in China often have fear and anxiety due to the unknown after death, which will cause great restlessness of patients and seriously affect the quality of death. Yang Qing et al62 conducted an in-depth interview on the care needs of 9 patients with advanced cancer and found that some patients had religious belief needs and hoped that the hospital could set up a Buddhist hall, read the Diamond Meridian and Great Sadness Charm in the ward, and could talk about Jesus with other patients, hoping to help them and relieve or alleviate psychological pain. Fifty percent of hospice patients in Diane et al63 identified prayer as a common need. The most frequently mentioned unmet need was for religious service. Religious beliefs can empower people, and patients adhere to the concept of “being with God, obeying God ‘s arrangement, and living in peace with God” and feel religious support, thereby enhancing the courage to fight cancer. It is suggested that medical staff should pay more attention to spiritual beliefs in the process of providing nursing care for patients at the end of their lives. Fear of death refers to the emotional reactions such as fear, worry and reluctance of the patient when faced with the approaching of death, which originate from the patient ‘s uncontrollable perception of the unknown world of death. Tang et al64 interviewed 14 white women with metastatic breast cancer and conducted an audio-recorded interview over the phone for 30 to 90 min using open-ended questions to encourage patients to talk about their feelings, and the results showed that 71% of patients had fear of dying. Payne et al65 used semi-structured interviews to understand the understanding of “good death” in 18 patients, and the results showed that patients believed that “good death” was characterized by “dying in sleep, dying quietly, without pain, and suddenly dying”, that is, avoiding the fear of death and leaving peacefully. Liao Jing et al66 investigated the death view and its influencing factors of patients with advanced cancer in a tertiary care hospital, and the results showed that women had a higher degree of anxiety about death. McDonald et al67 proposed that advanced cancer patients who had discussed hospice care were better able to participate in advance care plans and were able to face death with a calm attitude.
Hospice Care in Patients with Advanced Cancer
Advanced cancer poses difficult and complex situations for patients, while family caregivers face high levels of distress. In this complex situation, end-of-life care becomes increasingly important and demand increases. Hospice care aims not only to improve the quality of life of patients, but also to improve the quality of life of their families and their caregivers. Patients with advanced brain malignancies frequently present with progressive focal neurological deficits with a wide range of symptoms: cognitive deficits, paralysis, seizures, fatigue, dysphagia, headache, somnolence, loss of consciousness, incontinence, and psychosocial burden.68–70 Patients with advanced brain malignancies therefore have an increasing need for end-of-life care. Xiao et al71 found through systematic analysis that there are multiple needs for end-of-life care for patients with advanced glioma, including physical, psychological, social and spiritual needs, and glioma patients should meet their personalized treatment needs, improve the quality of life of patients at the end of their lives, and reduce the family burden of patients. Koekkoek et al69 reported that hospice care can reduce the pain of patients in the later stage of high-grade glioma patients, while improving the quality of life of patients in the later stage of life, and reducing the family burden of patients and their families.
Patients with advanced lung cancer also usually suffer from the pain caused by cancer. The emotional, social, spiritual and cultural phenomena of patients are factors that can also affect the pain.72 Hospice care can effectively improve the emotional, social and spiritual levels of patients at the end of life, thereby relieving the pain caused by cancer. Hou et al73 found by analyzing the data of 69,414 patients with non-small cell lung cancer that the proportion of patients with metastatic non-small cell lung cancer receiving palliative care showed an increasing trend year by year, and receiving palliative care and hospice care at the end of their lives could reduce the pain of patients while reducing the medical costs of patients with end-stage lung cancer. Hwang et al74 came to the same conclusion by analyzing data on palliative care for patients with advanced lung cancer in the United States, the use of hospice care in patients with advanced lung cancer increased year by year, and palliative care services were associated with reduced hospital costs. In contrast, however, life-sustaining treatment is associated with increased hospitalization costs. Triplett et al75 investigated the impact of palliative care on patients in a sample of 6580 patients with advanced cancer and found that hospice care significantly reduced health care use among Medicare beneficiaries with advanced cancer, emphasizing the importance of early integration of palliative care with standard oncology care. Vincent Mor et al76 concluded that hospice care is necessary for patients with advanced cancer by studying the clinical data of 13,085 patients with lung cancer, while hospice care can improve the life treatment of patients’ lives, preserve the patient “life dignity, and reduce the patient” family burden, which is associated with lower medical costs.
Breast cancer is the most common tumor in women, and the survival rate of advanced breast cancer is only about three years.77 Multiple organ metastasis often occurs in patients with advanced breast cancer, which exacerbates the patient ‘s physical pain and seriously affects the quality of life of patients and their families.78 A retrospective analysis by Bergqvist et al79 found that hospice care for advanced breast cancer patients was influenced by multiple factors, whereas emergency room visits, hospitalizations, and in-hospital deaths were registered less frequently for advanced breast cancer patients receiving hospice care. Wan et al80 analyzed 5481 patients with advanced breast cancer receiving palliative care and found that the effect of hospice care became more obvious with increasing patient age, and hospice care specifically significantly improved patients with advanced breast cancer. Joseph A. Greer et al81 showed that personalized hospice care needs to be developed for patients with advanced breast cancer, while increasing the length of hospice care is necessary. At present, in various types of advanced cancer, the increasing demand for hospice care can effectively improve the quality of life of patients in the later stages of life, reduce the pain of patients, and reduce the burden of life of patients and families.
Influencing Factors of Hospice Care
Sociodemographic Factors
It has been shown that younger age, living in rural areas, and female patients may have more unmet needs.82 In terms of age, some scholars have found that young patients need more support, mainly to seek the significance of life and reconcile with the disease, elderly patients believe that religious needs are important, with the highest satisfaction of life significance and reconciliation needs, while physical symptom needs are less important; in terms of gender, women express more needs compared with men, report more troublesome symptoms, and require more effective care.83 In terms of education level, education level showed a negative correlation with spiritual needs, patients with higher education level had reduced disease burden, lower anxiety and depression levels, and relatively lower spiritual needs. In terms of religious beliefs, it has been shown that patients without religious beliefs have higher needs in the social sphere, respect and support of health professionals, meaning of life, reconciliation, and opportunities to share emotions.47 Hospice needs assessment should be centered on the patient and his family, taking into account the patient ‘s cultural customs, living habits and other personalized characteristics.
In China, the traditional concept of life and death is also one of the barriers to the development of hospice care in China. Limited by the lack of traditional life and death outlook and life education, the Chinese people have a low recognition of hospice care services and become an important factor affecting the development of hospice care services in China. On the one hand, influenced by traditional ideas, Chinese people have negative attitude towards death and often fear avoiding it. Filial piety, on the other hand, further hinders children from choosing peaceful care at the end of their parents’ lives. Because the choice of hospice care can easily be questioned as not filial piety, the public is under double pressure from the outside world and the ontology, often difficult to recognize and accept hospice care, hindering the intervention of professional institutions. Therefore, it is necessary to increase the publicity of life education, promote the further development of hospice care in China, and contribute to the calm death of patients at the end stage of life.
Disease-Related Factors
In terms of time to diagnosis, some researchers believe that patients with longer cancer diagnosis have higher spiritual needs, possibly because they are exposed to greater threats to life and will have more thinking in exploring the significance and purpose of life. In terms of disease type, Konstantinidis et al31 showed that more than half of patients with advanced breast and lung cancer reported more than 8 needs, especially the unmet need for supportive care when assessing patients with advanced lung cancer was significantly increased, and the main care needs included better symptom control, diet, dressing assistance, and better attention by nurses and others, and the analysis may be related to shorter life expectancy and many serious complications associated with lung cancer. In terms of accompanying symptoms, studies have shown that the accompanying symptoms of patients are related to spiritual needs, and persistent painful symptom distress will change the patient ‘s mentality, lose the pursuit of life significance, and doubt the existing value, thus causing confusion and desire for death on life significance.
Degree of Anxiety and Depression
Patients with end-stage cancer often experience anxiety, pessimism, hopelessness, depression and other adverse emotional and psychological problems due to protracted disease and decreased physical self-care ability. Patients with anxiety and depression have more unmet needs, and these patients have low needs in physical symptoms, social domains, and meaning of life, but are more eager to share emotions. Hocker et al84 explored the factors associated with spiritual needs, and the results showed that anxiety was a significant predictor of spiritual needs, and the degree of anxiety was significantly correlated with the patient ‘s existing needs, inner calm and positive giving, and patients with lower levels of depression had higher spiritual needs for positive giving. Nursing staff should fully evaluate the psychological status of patients, identify patients with depression as soon as possible, ensure adequate psychological care, and timely meet their needs.
Social Support
End-stage cancer patients are under great physical and mental pressure, facing the fear of death and physical and mental pain often hope that someone can accompany around. Isaksen et al85 found that spiritual needs of patients with advanced cancer are closely related to social support. Boyes et al86 also confirmed that both lower social support and emotional support can greatly affect the unmet needs of patients, and patients with lower social emotional support will have higher unmet health information. Therefore, caregivers should take the initiative to create a harmonious and loving family atmosphere, with an equal, respectful, and receptive attitude, stand in the patient’s position to consider the problem, care in life, spiritual comfort, and timely counseling and dissolving the patient’s bad emotions.
Conclusion
Promoting hospice care for patients with advanced cancer is both a humanistic care and a favorable policy for a country. At present, cancer patients worldwide are increasing, hospice care demand is very large, there is a certain social basis, the promotion of hospice care has great practical significance. The need for end-of-life care varies among patients and is influenced by cultural background, family perceptions, personal roles, and experiences. Different assessment methods and tools have been used in studies on hospice care needs of patients with advanced cancer, including descriptive studies and different assessment tools, which reflect the limitations of hospice care needs assessment for patients with advanced cancer. Further exploration of needs assessment tools for patients with advanced cancer and interventions to address unmet needs is needed to promote the further development of hospice care and improve the quality of life of patients with advanced cancer. At present, the evaluation methods and tools for the use of hospice care in China remain to be further explored, and the existing evaluation methods and tools are optimized or new hospice care evaluation tools suitable for the use of advanced cancer in China are developed. At the same time, China should develop hospice care standards and measures suitable for its own national conditions according to the actual situation of its own medical institutions, strengthen the publicity and education of hospice care, and improve the EOL treatment of Chinese patients with advanced cancer.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
An ethics statement is not applicable because this study is based exclusively on published literature.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
All of the authors had no any personal, financial, commercial, or academic conflicts of interest separately.
References
1. Tegenborg S, Fransson P, Martinsson L. Physicians’ and nurses’ experience of using the Abbey Pain Scale (APS) in people with advanced cancer: a qualitative content analysis. BMC Nursing. 2023;22(1):95. doi:10.1186/s12912-023-01227-7
2. Schmidt DR, Patel R, Kirsch DG, et al. Metabolomics in cancer research and emerging applications in clinical oncology. CA Cancer J Clin. 2021;71(4):333–358. doi:10.3322/caac.21670
3. Qureshi S, Boily G, Boulanger J, et al. Inequalities in survival and care across social determinants of health in a cohort of advanced lung cancer patients in Quebec (Canada): a high-resolution population-level analysis. Cancer Med. 2023;12(11):12683–12704. doi:10.1002/cam4.5897
4. Robbins-Welty GA, Webb JA, Shalev D, et al. Advancing Palliative Care Integration in Hematology: building Upon Existing Evidence. Curr Treat Options Oncol. 2023;24(5):542–564. doi:10.1007/s11864-023-01084-1
5. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
6. Cortes J, Perez‐García JM, Llombart‐Cussac A, et al. Enhancing global access to cancer medicines. CA Cancer J Clin. 2020;70(2):105–124. doi:10.3322/caac.21597
7. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
8. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.21338
9. Zhang Z, Gu X-L, Chen M-L, et al. Use of Palliative Chemo- and Radiotherapy at the End of Life in Patients With Cancer: a Retrospective Cohort Study. Am J Hosp Palliat Care. 2017;34(9):801–805. doi:10.1177/1049909116653733
10. Tang ST, Wu S-C, Hung Y-N, et al. Trends in quality of end-of-life care for Taiwanese cancer patients who died in 2000–2006. Ann Oncol. 2009;20(2):343–348. doi:10.1093/annonc/mdn602
11. Wu SC, Chen JS, Wang HM, et al. Determinants of ICU care in the last month of life for Taiwanese cancer decedents, 2001 to 2006. Chest. 2010;138(5):1071–1077. doi:10.1378/chest.09-2662
12. Leng A, Jing J, Nicholas S, et al. Geographical disparities in treatment and health care costs for end-of-life cancer patients in China: a retrospective study. BMC Cancer. 2019;19(1):39. doi:10.1186/s12885-018-5237-1
13. Zhu Y, Tang K, Zhao F, et al. End-of-life chemotherapy is associated with poor survival and aggressive care in patients with small cell lung cancer. J Cancer Res Clin Oncol. 2018;144(8):1591–1599. doi:10.1007/s00432-018-2673-x
14. Laudicella M, Walsh B, Burns E, et al. Cost of care for cancer patients in England: evidence from population-based patient-level data. Br J Cancer. 2016;114(11):1286–1292. doi:10.1038/bjc.2016.77
15. Yabroff KR, Lamont EB, Mariotto A, et al. Cost of care for elderly cancer patients in the United States. J Natl Cancer Inst. 2008;100(9):630–641. doi:10.1093/jnci/djn103
16. Langton JM, Srasuebkul P, Reeve R, et al. Resource use, costs and quality of end-of-life care: observations in a cohort of elderly Australian cancer decedents. Implement Sci. 2015;10:25. doi:10.1186/s13012-014-0148-2
17. Bateman RM, Sharpe MD, Jagger JE, et al. 36th International Symposium on Intensive Care and Emergency Medicine. Crit Care. 2016;20(Suppl 2):94. doi:10.1186/s13054-016-1208-6
18. Chen Z. Third National Review and Sample Survey Report on Cause of Death [D]. Beijing: China union medical university press; 2008.
19. China center for disease control and prevention. National Cause of Death Surveillance Report in 2008. China Center for Disease Control and Prevention; 2009.
20. Cui J, Fang F, Shen F, et al. Quality of life in patients with advanced cancer at the end of life as measured by the McGill quality of life questionnaire: a survey in China. J Pain Symptom Manage. 2014;48(5):893–902. doi:10.1016/j.jpainsymman.2014.02.016
21. Chang HT, Lin MH, Chen CK, et al. Medical care utilization and costs on end-of-life cancer patients: the role of hospice care. Medicine. 2016;95(44):e5216. doi:10.1097/MD.0000000000005216
22. Yoong SQ, Wang W, Seah ACW, et al. Nursing students’ experiences with patient death and palliative and end-of-life care: a systematic review and meta-synthesis. Nurse Educ Pract. 2023;69:103625. doi:10.1016/j.nepr.2023.103625
23. Pinto S, Lopes S, Bruno de Sousa A, et al. Preferences about place of end-of-life care and death of patients with life-threatening illnesses and their families: a protocol for an umbrella review. BMJ Open. 2023;13(3):e066374. doi:10.1136/bmjopen-2022-066374
24. Rabitti E, Cavuto S, Díaz Crescitelli ME, et al. Hospice Patients’ End-of-Life Dreams and Visions: a Systematic Review of Qualitative Studies. Am J Hosp Palliat Care. 2023:10499091231163571. doi:10.1177/10499091231163571
25. Söderman A, Werkander Harstäde C, Hälleberg Nyman M, et al. Valuing the individual - evaluating the Dignity Care Intervention. Nurs Ethics. 2023;30(1):86–105. doi:10.1177/09697330221122902
26. Bhatnagar M, Lagnese KR. Hospice Care. Treasure Island (FL): StatPearls Publishing; 2023.
27. Pierce JG, Ricon R, Rukmangadhan S, et al. Adherence to the TQIP Palliative Care Guidelines Among Patients With Serious Illness at a Level I Trauma Center in the US. JAMA Surg. 2022;157(12):1125–1132. doi:10.1001/jamasurg.2022.4718
28. Skedsmo K, Nes AAG, Stenseth HV, et al. Simulation-based learning in palliative care in postgraduate nursing education: a scoping review. BMC Palliat Care. 2023;22(1):30. doi:10.1186/s12904-023-01149-w
29. Iocolano M, Langi A, Dharmarajan KV, et al. Palliative Care Delivery Systems and Integration With Palliative Care Teams. Semin Radiat Oncol. 2023;33(2):211–217. doi:10.1016/j.semradonc.2022.11.003
30. Pun J, Chow JCH, Fok L, et al. Role of patients’ family members in end-of-life communication: an integrative review. BMJ Open. 2023;13(2):e067304. doi:10.1136/bmjopen-2022-067304
31. Konstantinidis T, Linardakis M, Samonis G, et al. Quality of life of patients with advanced cancer treated in a regional hospital in Greece. Hippokratia. 2016;20(2):139–146.
32. von Gruenigen VE, Huang HQ, Cella D, et al. Quality of life, symptoms and care needs in patients with persistent or recurrent platinum-resistant ovarian cancer: an NRG Oncology/Gynecologic Oncology Group study. Gynecol Oncol. 2018;150(1):119–126. doi:10.1016/j.ygyno.2018.05.017
33. Buzgova R, Kozakova R, Sikorova L, et al. Development and psychometric evaluation of patient needs assessment in palliative care (PNAP) instrument. Palliat Support Care. 2016;14(2):129–137. doi:10.1017/S1478951515000061
34. Moghaddam N, Coxon H, Nabarro S, et al. Unmet care needs in people living with advanced cancer: a systematic review. Support Care Cancer. 2016;24(8):3609–3622. doi:10.1007/s00520-016-3221-3
35. Osse BH, Vernooij MJ, Schadé E, et al. Towards a new clinical tool for needs assessment in the palliative care of cancer patients: the PNPC instrument. J Pain Symptom Manage. 2004;28(4):329–341. doi:10.1016/j.jpainsymman.2004.01.010
36. Osse BH, Vernooij-Dassen MJ, Schadé E, et al. A practical instrument to explore patients’ needs in palliative care: the Problems and Needs in Palliative Care questionnaire short version. Palliat Med. 2007;21(5):391–399. doi:10.1177/0269216307078300
37. Wang T, Molassiotis A, Chung BPM, et al. Psychometric assessment of the Chinese version of the Problems and Needs in Palliative Care questionnaire-short version in advanced cancer patients. BMC Palliat Care. 2019;18(1):68. doi:10.1186/s12904-019-0450-5
38. Waller A, Girgis A, Currow D, et al. Development of the palliative care needs assessment tool (PC-NAT) for use by multi-disciplinary health professionals. Palliat Med. 2008;22(8):956–964. doi:10.1177/0269216308098797
39. Waller A, Girgis A, Lecathelinais C, et al. Validity, reliability and clinical feasibility of a Needs Assessment Tool for people with progressive cancer. Psychooncology. 2010;19(7):726–733. doi:10.1002/pon.1624
40. Wu HH, Chen XY, Yin XL. Development and validation of cancer patients’ palliative care needs questionnaire. J Nurs Sci. 2020;35(7):5–8. doi:10.3870/j.issn.1001-4152.2020.07.005
41. Chou WY, Stokes SC, Citko J, et al. Improving end-of-life care through community-based grassroots collaboration: development of the Chinese-American Coalition for Compassionate Care. J Palliat Care. 2008;24(1):31–40.
42. Litzelman DK, Inui TS, Schmitt-Wendholt KM, et al. Clarifying Values and Preferences for Care Near the End of Life: the Role of a New Lay Workforce. J Community Health. 2017;42(5):926–934. doi:10.1007/s10900-017-0336-5
43. Delgado-Guay MO, Rodriguez-Nunez A, De la Cruz V, et al. Advanced cancer patients’ reported wishes at the end of life: a randomized controlled trial. Support Care Cancer. 2016;24(10):4273–4281. doi:10.1007/s00520-016-3260-9
44. Menkin ES. Go Wish: a tool for end-of-life care conversations. J Palliat Med. 2007;10(2):297–303. doi:10.1089/jpm.2006.9983
45. Cheng F, Wen Q, Cheng XL. Effect of heart to heart® café on lung cancer patients’ end-of-life concerns. J Nursing. 2018;25(21):73–76. doi:10.16460/j.issn1008-9969.2018.21.073
46. Emanuel LL, Alpert HR, Emanuel EE. Concise screening questions for clinical assessments of terminal care: the needs near the end-of-life care screening tool. J Palliat Med. 2001;4(4):465–474. doi:10.1089/109662101753381601
47. Buzgova R, Sikorova L, Jarosova D. Assessing Patients’ Palliative Care Needs in the Final Stages of Illness During Hospitalization. Am J Hosp Palliat Care. 2016;33(2):184–193. doi:10.1177/1049909114556528
48. Steindal SA, Bredal IS, Ranhoff AH, et al. The last three days of life: a comparison of pain management in the young old and the oldest old hospitalised patients using the Resident Assessment Instrument for Palliative Care. Int J Older People Nurs. 2015;10(4):263–272. doi:10.1111/opn.12076
49. Steindal SA, Ranhoff AH, Bredal IS, et al. Last three days of life in the hospital: a comparison of symptoms, signs and treatments in the young old and the oldest old patients using the Resident assessment instrument for palliative care. Int J Older People Nurs. 2013;8(3):199–206. doi:10.1111/j.1748-3743.2012.00313.x
50. Hermans K, De Almeida Mello J, Spruytte N, et al. A comparative analysis of comprehensive geriatric assessments for nursing home residents receiving palliative care: a systematic review. J Am Med Dir Assoc. 2014;15(7):467–476. doi:10.1016/j.jamda.2014.01.002
51. Hughes P, Ahmed N, Winslow M, et al. Consumer views on a new holistic screening tool for supportive and palliative-care needs: Sheffield Profile for Assessment and Referral for Care (SPARC): a survey of self-help support groups in health care. Health Expect. 2015;18(4):562–577. doi:10.1111/hex.12058
52. Leppert W, Majkowicz M, Ahmedzai SH. The adaptation of the Sheffield Profile for Assessment and Referral for Care (SPARC) to the Polish clinical setting for needs assessment of advanced cancer patients. J Pain Symptom Manage. 2012;44(6):916–922. doi:10.1016/j.jpainsymman.2011.12.286
53. Burton CR, Payne S, Addington-Hall J, et al. The palliative care needs of acute stroke patients: a prospective study of hospital admissions. Age Ageing. 2010;39(5):554–559. doi:10.1093/ageing/afq077
54. Zhuang JP. The status of hospice demand for advanced cancer patients and its influence on patients’ quality of life. Chin General Practice Nursing. 2018;16(19):2411–2413. doi:10.12104/j.issn.1674-4748.2018.19.044
55. Li N, Wang Y. Qualitative research on quality of life of woman with advanced breast cancer. Tianjin J Nursing. 2010;18(4):190–192. doi:10.3969/j.issn.1006-9143.2010.04.003
56. Masel EK, Trinczek H, Adamidis F, et al. Vitamin “G”arden: a qualitative study exploring perception/s of horticultural therapy on a palliative care ward. Support Care Cancer. 2018;26(6):1799–1805. doi:10.1007/s00520-017-3978-z
57. Rainsford S, Phillips CB, Glasgow NJ, et al. The ‘safe death’: an ethnographic study exploring the perspectives of rural palliative care patients and family caregivers. Palliat Med. 2018;32(10):1575–1583. doi:10.1177/0269216318800613
58. Geller G, Warren LR. Toward an optimal healing environment in pediatric rehabilitation. J Altern Complement Med. 2004;10 Suppl 1:S179-S192. doi:10.1089/1075553042245999
59. Perera MC, Ramadasa GU, Chandrasiri GMLW, et al. A good death in Ratnapura: a qualitative study. Ceylon J Otolaryngol. 2015;4(1):20. doi:10.4038/cjo.v4i1.5225
60. Harrop E, Noble S, Edwards M, et al. Managing, making sense of and finding meaning in advanced illness: a qualitative exploration of the coping and wellbeing experiences of patients with lung cancer. Sociol Health Illn. 2017;39(8):1448–1464. doi:10.1111/1467-9566.12601
61. Zhang JX, Jin YH, Cao YJ, et al. Expectation and needs of a good death in patients with end-stage chronic diseases: a systematic review. Chin J Nurs. 2019;54(12):1788–1794. doi:10.3761/j.issn.0254-1769.2019.12.005
62. Yang Q, Yu Y, Li XF. Care needs of terminal cancer patients: a qualitative study. J Nurs Sci. 2015;30(14):30–33. doi:10.3870/hlxzz.2015.14.030
63. Hampton DM, Hollis DE, Lloyd DA, et al. Spiritual needs of persons with advanced cancer. Am J Hosp Palliat Care. 2007;24(1):42–48. doi:10.1177/1049909106295773
64. Tang PL, Chiou CP, Lin HS, et al. Correlates of death anxiety among Taiwanese cancer patients. Cancer Nurs. 2011;34(4):286–292. doi:10.1097/NCC.0b013e31820254c6
65. Payne SA, Langley-Evans A, Hillier R. Perceptions of a ‘good’ death: a comparative study of the views of hospice staff and patients. Palliat Med. 1996;10(4):307–312. doi:10.1177/026921639601000406
66. Liao J, Ni P, Chen FJ, et al. The Concept of Death of Patients with Advanced Cancer in Grade A Hospital and its Influencing Factors. J Qilu Nursing. 2019;25(5):18–21. doi:10.3969/j.issn.1006-7256.2019.05.006
67. McDonald JC, du Manoir JM, Kevork N, et al. Advance directives in patients with advanced cancer receiving active treatment: attitudes, prevalence, and barriers. Support Care Cancer. 2017;25(2):523–531. doi:10.1007/s00520-016-3433-6
68. Sizoo EM, Braam L, Postma TJ, et al. Symptoms and problems in the end-of-life phase of high-grade glioma patients. Neuro Oncol. 2010;12(11):1162–1166. doi:10.1093/neuonc/nop045
69. Koekkoek JA, Dirven L, Sizoo EM, et al. Symptoms and medication management in the end of life phase of high-grade glioma patients. J Neurooncol. 2014;120(3):589–595. doi:10.1007/s11060-014-1591-2
70. Walbert T, Khan M. End-of-life symptoms and care in patients with primary malignant brain tumors: a systematic literature review. J Neurooncol. 2014;117(2):217–224. doi:10.1007/s11060-014-1393-6
71. Xiao Z, Chen W, Zhao H, et al. Palliative care for patients with glioma: a recent scientometric analysis of the Web of Science in 2022. Front Oncol. 2022;12:995639. doi:10.3389/fonc.2022.995639
72. World Health Organization. Global Atlas of Palliative Care at the End of Life; Worldwide Palliative Care Alliance. London, UK; 2014.
73. Huo J, Hong YR, Turner K, et al. Utilization pattern and service settings of palliative care for patients with metastatic non-small cell lung cancer. Cancer. 2019;125(24):4481–4489. doi:10.1002/cncr.32478
74. Hwang J, Shen J, Kim SJ, et al. Ten-Year Trends of Utilization of Palliative Care Services and Life-Sustaining Treatments and Hospital Costs Associated With Patients With Terminally Ill Lung Cancer in the United States From 2005 to 2014. Am J Hosp Palliat Care. 2019;36(12):1105–1113. doi:10.1177/1049909119852082
75. Triplett DP, LeBrett WG, Bryant AK, et al. Effect of Palliative Care on Aggressiveness of End-of-Life Care Among Patients With Advanced Cancer. J Oncol Pract. 2017;13(9):e760–e769. doi:10.1200/JOP.2017.020883
76. Mor V, Wagner TH, Levy C, et al. Association of Expanded VA Hospice Care With Aggressive Care and Cost for Veterans With Advanced Lung Cancer. JAMA Oncol. 2019;5(6):810–816. doi:10.1001/jamaoncol.2019.0081
77. Cardoso F, Senkus E, Costa A, et al. 4th ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 4)†. Ann Oncol. 2018;29(8):1634–1657. doi:10.1093/annonc/mdy192
78. Caplette-Gingras A, Savard J. Depression in women with metastatic breast cancer: a review of the literature. Palliat Support Care. 2008;6(4):377–387. doi:10.1017/S1478951508000606
79. Bergqvist J, Hedman C, Schultz T, et al. Equal receipt of specialized palliative care in breast and prostate cancer: a register study. Support Care Cancer. 2022;30(9):7721–7730. doi:10.1007/s00520-022-07150-y
80. Wan S, Lorenz KA, Fischer SM, et al. Local Area Hospice Capacity and Rural Disparities in Hospice Use among Older Adults with Metastatic Breast Cancer. J Palliat Med. 2023;26(2):182–190. doi:10.1089/jpm.2022.0227
81. Greer JA, Moy B, El-Jawahri A, et al. Randomized Trial of a Palliative Care Intervention to Improve End-of-Life Care Discussions in Patients With Metastatic Breast Cancer. J Natl Compr Canc Netw. 2022;20(2):136–143. doi:10.6004/jnccn.2021.7040
82. Barg FK, Cronholm PF, Straton JB, et al. Unmet psychosocial needs of Pennsylvanians with cancer: 1986-2005. Cancer. 2007;110(3):631–639. doi:10.1002/cncr.22820
83. Wijk H, Grimby A. Needs of elderly patients in palliative care. Am J Hosp Palliat Care. 2008;25(2):106–111. doi:10.1177/1049909107305646
84. Höcker A, Krüll A, Koch U, et al. Exploring spiritual needs and their associated factors in an urban sample of early and advanced cancer patients. Eur J Cancer Care. 2014;23(6):786–794. doi:10.1111/ecc.12200
85. Johansson AK, Sundh V, Wijk H, et al. Anticipatory grief among close relatives of persons with dementia in comparison with close relatives of patients with cancer. Am J Hosp Palliat Care. 2013;30(1):29–34. doi:10.1177/1049909112439744
86. Boyes AW, Girgis A, D’Este C, et al. Prevalence and correlates of cancer survivors’ supportive care needs 6 months after diagnosis: a population-based cross-sectional study. BMC Cancer. 2012;12:150. doi:10.1186/1471-2407-12-150
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.