Back to Journals » Research and Reports in Tropical Medicine » Volume 9
A review of the genus Rickettsia in Central America
Authors Bermúdez C SE ![]() , Troyo A
, Troyo A
Received 27 December 2017
Accepted for publication 1 May 2018
Published 29 June 2018 Volume 2018:9 Pages 103—112
DOI https://doi.org/10.2147/RRTM.S160951
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Thomas Unnasch
Sergio E Bermúdez C,1 Adriana Troyo2
1Department of Medical Entomology, Gorgas Memorial Institute for Health Research, Panamá; 2Vector Research Laboratory, Tropical Diseases Research Center, Faculty of Microbiology, University of Costa Rica, San Jose, Costa Rica
Abstract: In this paper, we present a historical review of rickettsiosis in Central America and also the most recent findings of Rickettsia in ectoparasites. All countries of Central America have records of rickettsiosis. Regarding the typhus group rickettsioses, there is clinical or serological evidence of Rickettsia prowazekii in Guatemala, Rickettsia typhi in Panama, Guatemala, and Costa Rica and unidentified species of the typhus group in El Salvador. Concerning spotted fever group rickettsiosis, there is serological evidence of infection by Rickettsia akari in Costa Rica and confirmed cases involving Rickettsia rickettsii in Panama and Costa Rica. There are also reports of spotted fever group rickettsiosis in acute patients from Guatemala, Honduras, and Nicaragua. Serological studies in Central America show reactivity of Rickettsia ambyommatis, Rickettsia bellii, Rickettsia felis, Rickettsia rhipicephali, and R. rickettsii in domestic and wild mammals. Eight species of Rickettsia have been detected in ectoparasites from Central America: R. africae (or very similar), R. amblyommatis, R. asembonensis, R. bellii, R. felis, R. parkeri, R. rhipicephali, and R. rickettsii, in addition to undescribed strains such as Atlantic Rainforest, Colombianensi, IbR/CRC, Barva, Aragaoi, and Candidatus “Rickettsia nicoyana;” the latter being the only one associated with Argasidae (Ornithodoros knoxjonesi). R. amblyommatis is the most common species in Central America, seeing as it has been reported in 10 species of ticks and one of fleas in five of the seven countries of the region. In this study, we demonstrate that the genus Rickettsia is widely distributed in Central America and that rickettsiosis could be an underestimated problem in the absence of greater diagnostic efforts in undetermined febrile cases.
Keywords: rickettsiosis, Rickettsia, Rocky Mountain spotted fever, vector, Central America
Introduction
Rickettsia is a genus composed of 27 species of obligate intracellular bacteria, and ~17 of them are considered pathogens of animals and humans.1 Pathogenic species are divided into the typhus group (TG), transmitted by insects, and the spotted fever group (SFG), which is mainly transmitted by mites and hard ticks.1,2 Regarding the differences between the two groups, TG rickettsiae lack the capacity to polymerize actin and produce infections only in the cytoplasm of host cells, whereas SFG rickettsiae can polymerize actin and infect nuclei; in addition, there are differences in optimal growth temperatures (35°C for TG and 32°C for SFG), G-C content (29% in TG and 32%–33% in SFG), and outer membrane proteins (type B in TG and types A and B in SFG).3
The TG includes two pathogens: Rickettsia prowazekii causes epidemic typhus and is transmitted mainly by contact with infected feces of the human body louse; Rickettsia typhi is responsible for endemic or murine typhus, and its transmission is associated with fleas.4,5 Both the rickettsiae seem to be cosmopolitan because of the wide geographical distribution of their vectors.1 General symptoms of infection with TG rickettsiae are non-specific: headache, fever (higher in epidemic typhus), muscle and joint pain; patients also present nausea and vomiting, cough, rash (moderate in murine typhus, but severe in epidemic typhus), chills, decrease in blood pressure, stupor, photosensitivity, delirium, and death in untreated cases of epidemic typhus.6 In fact, mortality in untreated cases of epidemic typhus is usually high (10%–60%), but decreases significantly if the adequate antibiotic treatment is administered within the first days of infection.6 In addition to these species, other pathogenic bacteria are recognized as etiological agents of “typhus,” although they belong to the SFG (eg, Queensland ticks typhus, Rickettsia australis) or to another genus (eg, scrub typhus by Orientia tsutsugamushi).
More than 25 species belong to the SFG, and they present geographical distributions in accordance with the range of their principal tick vectors, with the exception of the cosmopolitan Rickettsia felis, associated mainly with fleas.7 Of these, currently 15 pathogenic species are reported worldwide, in addition to several other species that are considered potential human pathogens, but for which clinical evidence has not been conclusive.1 The severity of SFG rickettsial infections vary greatly between species, and similar to TG rickettsial infections, there are usually no specific symptoms that can be used to clearly differentiate SFG rickettsioses from several other fevers caused by viruses (eg, dengue) or bacteria (eg, Leptospira sp.). In general, and depending on the Rickettsia species involved, patients may present mild or high fever, an eschar at the site of bacterial entry, inflammation of regional or satellite lymph nodes, and exanthema or erythematous maculopapular rash; also, damage to different organs may be involved due to vasculitis and, in extremes cases, death may occur.8 Rickettsia rickettsii is the most lethal agent within the genus and the most important tick-borne disease in America, as it presents high fatality rates in untreated cases.9,10 Infection by R. rickettsii causes the disease known as Rocky Mountain spotted fever (RMSF) in the USA, but it also has regional names like “fiebre maculosa Brasileira” (Brazil) or “fiebre de Tobia” (Colombia).10
In the last three decades, rickettsial diseases have awakened the interest of specialists in public health due to the increase of reported cases and the possibility that they will continue rising due to anthropogenic modifications and global climate change, in addition to the threat that these bacteria represent as a potential bioterrorism weapon.4 Therefore, efforts to improve the diagnosis of rickettsioses and the methods for detection of rickettsiae in arthropods have generated a large number of scientific literature around the world.11
In Central America, although rickettsial diseases are known, the low number of cases per year and the higher prevalence of other infectious diseases have prevented greater attention from professionals and institutions working in human health. In the present study, we present a historical review and the most recent findings pertaining species of Rickettsia and rickettsioses in Central America. For this, we searched for scientific publications in English and Spanish in databases and search engines such as PubMed, Scielo, LILACS, and Google Scholar, and by using keywords (Rickettsia, rickettsiosis, country names). An initial selection was made when the title and abstract suggested reports of rickettsiae or rickettsiosis in any country of Central America, and complete documents were read when in doubt about the content. Local libraries and retired rickettsiologists in Panama and Costa Rica were contacted to locate and obtain publications that were not readily available. All resulting articles were read in detail, as well as any additional publications that were cited in them but had not been identified previously.
Rickettsioses in Central America
TG rickettsioses
Both epidemic and endemic (murine) typhus have been documented in Central America (Table 1). Epidemic typhus is one of the most ancient human diseases known, and outbreaks have occurred along the history of humanity, with numerous deaths.4 Although epidemics of this disease decreased considerably after the control of lice populations and the use of antibiotic treatment, cases still occur in poor villages in cold regions of North America, Eastern Europe, Asia, and mountainous towns in Central and Eastern Africa, as well as South and Central America.6 According to Hume, epidemic typhus may have entered Central America during the European conquest.12 Since then, this disease has remained as isolated outbreaks in mountainous areas of Central America, in particular in villages and town of Guatemala with elevations between 2,500 and 3,500 m above sea level.13 A high mortality was reported in Guatemala during outbreaks in 1932–1934, with ~180 fatal cases per year.13
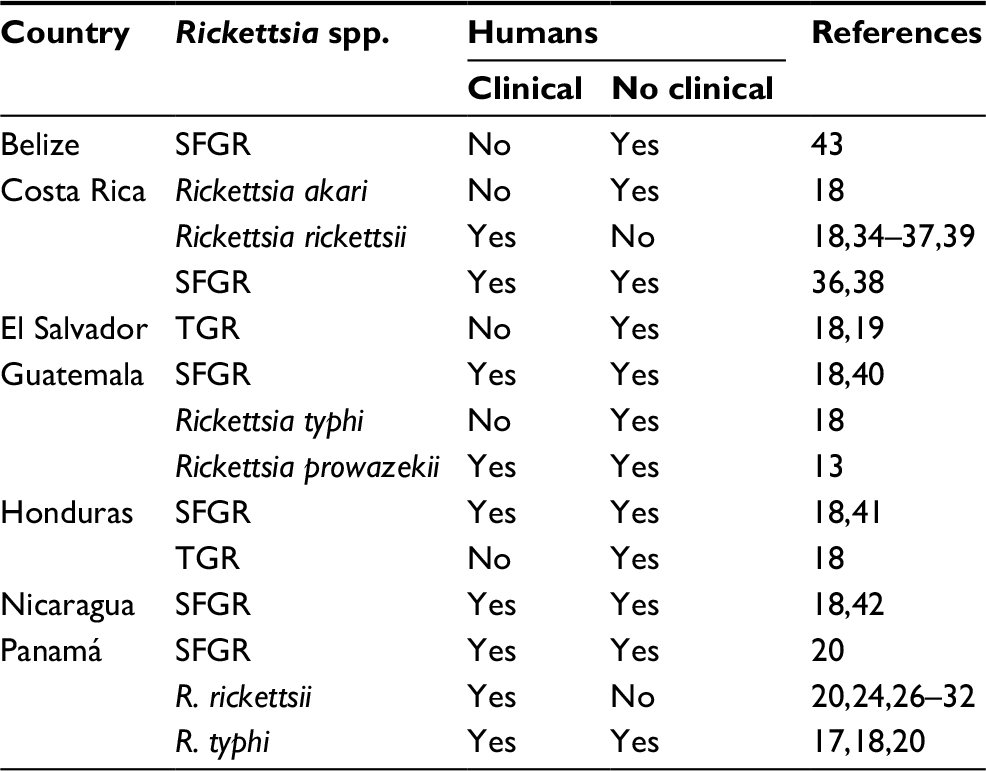 | Table 1 Rickettsial infections in humans reported in Central America Abbreviations: SFGR, spotted fever group rickettsiosis; TGR, typhus group rickettsiosis. |
Regarding murine typhus, it is present worldwide but predominantly in areas of tropical and subtropical regions that have poor sanitation, where humans inhabit close to rodents.14,15 Currently, murine typhus is present in the Mediterranean basin, some countries of Africa, Asia, and America.16 In Central America, the first mention of murine typhus was in the descriptions of clinical symptoms of cases diagnosed in Panama.17 In this country, more than 50 cases were confirmed during 1932–1947, with the last outbreak (13 patients) in the City of Panama that affected mostly people working or visiting a storeroom where dead rats had been reported.17
A serological survey in Central America showed antibody titers against TG Rickettsia in humans in Guatemala, Honduras, El Salvador, Nicaragua, and Panama, with a high positivity to endemic typhus in the highlands of Guatemala.18 Later, in a global surveillance study developed by WHO in 1993, eight volunteers (n=40) from El Salvador had a positive reaction to TG rickettsiae, using an end titer of 64 as cutoff for reactivity in immunofluorescence assays (IFAs).19 More recently, IgG antibodies against TG rickettsiae have been found in humans from a rural town of Panama.20 To the authors’ knowledge, no more recent references of TG rickettsioses in Central America are available in the scientific literature.
SFG rickettsioses
Currently, RMSF or other SFG rickettsioses have been confirmed in the seven countries of Central America (Table 1).
Spotted fever rickettsiosis, and specifically RMSF, was originally described in the early 20th century as “piroplasmosis hominis” from cases in Bitterroot Valley Montana (USA); Dermacentor ticks were associated with transmission.21 Later, cases were diagnosed in México (1918), Brazil (1929), and Colombia (1938).10,22,23 In Central America, the first records of RMSF were registered in Panama in the early 1950s.24 During the investigation of these cases, R. rickettsii was isolated from the tick Amblyomma mixtum (cited as Amblyomma cajennense), and Rhipicephalus sanguineus s.l. was implicated as a potential vector in an urban case.25,26 After these cases, no more spotted fevers were reported in Panama for several decades; however, a serosurvey showed a relatively high prevalence (5.4%–15.2%) of antibodies to SFG rickettsiae in 1,400 volunteers, but without determining the possible Rickettsia species.27
Indeed, almost 60 years passed until new cases of RMSF were confirmed in Panama: one case in 2004, three in 2007, one in 2008, one in 2012, one in 2015, and three in 2017 (only two of them were reported in the scientific literature).28–32 Nine of the patients died, with a 90% fatality. Recently, R. rickettsii was detected in intradomiciliary R. sanguineus s.l. as part of an investigation of an urban case in the City of Panama. This may represent a new scenario as to the ecology of RMSF transmission, where dogs and their ticks may play an important role in urban areas.32 In addition to these confirmed cases, a serological study revealed a relatively high seroprevalence of SFG infections (29%–31%) in people from rural areas.20,33
In Costa Rica, SFG infections were reported for the first time in 1952 from serological studies.34,35 Regardless, no febrile cases were documented until 1974, when patients presented symptoms compatible with SFG rickettsiosis.36 In 1975, the first confirmations of RMSF cases in Costa Rica were given, including a fatal case.37 Additional serological studies in humans and animals followed.38 In contrast to Panama, several cases of RMSF have been confirmed in Costa Rica since these reports in the late 1970s, and children seemed to be the most affected.34,35,39
A serological survey carried out in the late 1960s showed antibodies to SFG Rickettsia in sera from Costa Rica (13 positives of 507 samples), Honduras (3/348), Nicaragua (1/312), and Panama (4/336).18 In that study, antibodies against Rickettsia akari were detected in Costa Rica. With the exception of this report, no other information is available about R. akari in the region.
At the beginning of the 21st century and in accordance with the re-emergence of fatal cases of RMSF in Panama, new evidence of rickettsial diseases in other countries of Central America was confirmed. In 2007, an investigation of febrile illness in a rural area of Guatemala caused at least 17 cases of SFG rickettsiosis, including two fatalities.40 During the epidemiological investigation, DNA closely related to Rickettsia africae and Rickettsia sibirica was detected in A. cajennense s.l. Subsequently, in 2009, a case of SFG rickettsiosis was reported from a US traveler who returned from Honduras.41 In Nicaragua, the first evidence of SFG rickettsiosis was reported in 2016 from patients in the acute phase of infection, which also included diagnosis of Q fever.42 In this study, the sample included 825 patients and about 1% was considered positive for SFG rickettsiosis, but specifically RMSF was not confirmed. In Belize, there is only one report that supports SFG rickettsial infection in humans; the study found a seroprevalence of 54% (IFA using R. rickettsii antigen) in a group of healthy pregnant women.43
It is important to note that R. rickettsii has been isolated and molecularly identified from symptomatic human cases only in Panama and Costa Rica, but not in the cases from Guatemala, Honduras, and Nicaragua (Table 1). In addition, only Panama and Costa Rica have serological studies in domestic and wild mammals (Table 2).
 | Table 2 Serological evidence of rickettsial infection in domestic and wild mammals of Central America Notes: aCited as Rickettsia amblyommi or Candidatus “Rickettsia amblyommii.” bThis coyote showed symptoms similar to those described for R. rickettsii infections in dogs. Abbreviation: SFGR, spotted fever group rickettsiosis. |
Rickettsia species in ectoparasites in Central America
For many decades, R. rickettsii, R. akari, R. typhi (=Rickettsia mooseri), and R. prowazekii were the only known species of Rickettsia in the region, and they were mainly characterized from patients with acute phase infections or isolated from ticks in eco-epidemiological studies.23 After several decades, and with the use of molecular tools, the detection of rickettsiae was extended to ecological studies, especially in more species of ticks. In recent years, research in the region has involved many species of ticks and fleas, which has resulted in the detection of pathogenic rickettsiae including R. rickettsii, R. felis, Rickettsia parkeri, and R. africae (or very similar), as well as strains of undescribed or Candidatus species (Table 3).
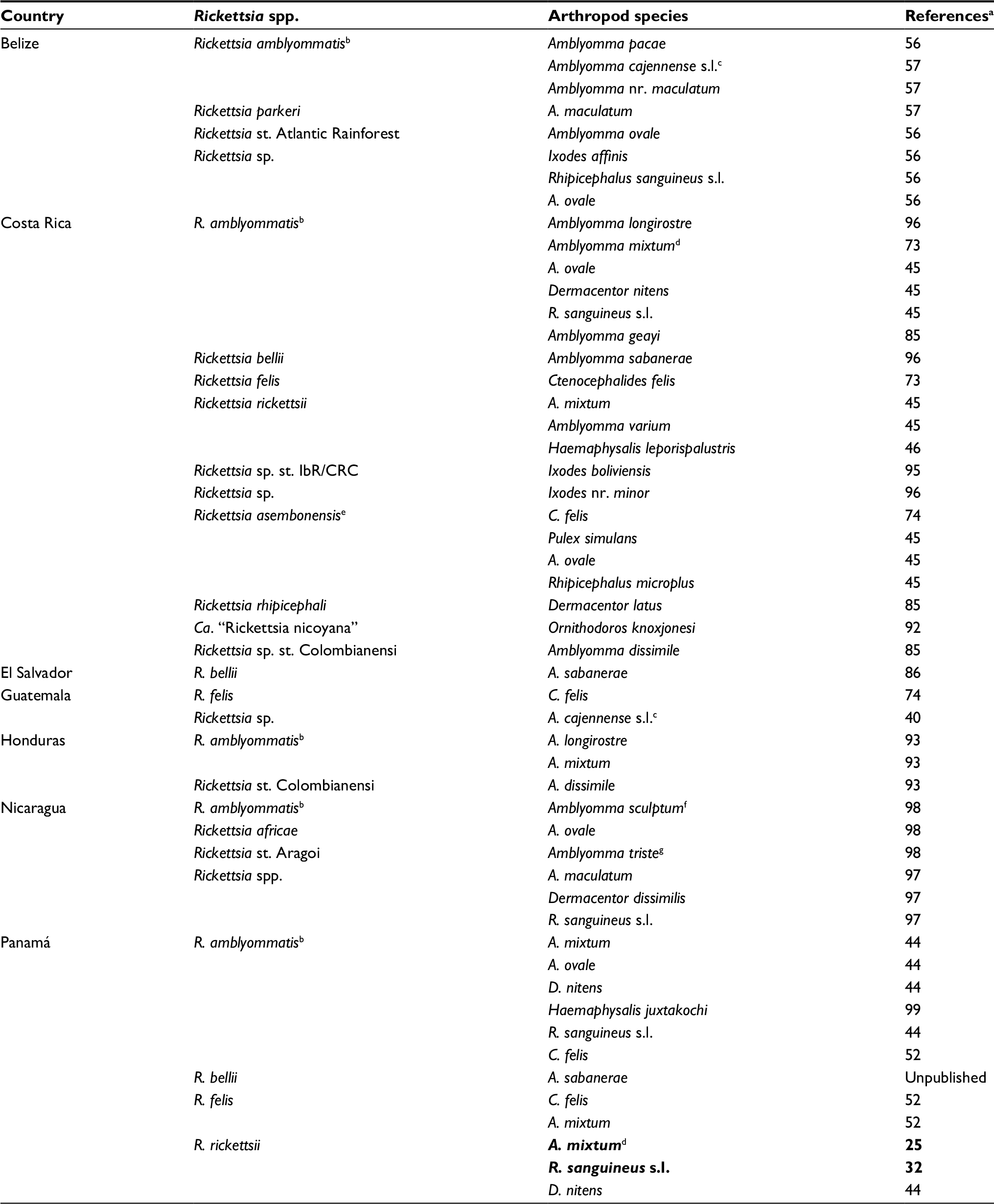 | Table 3 Checklist of Rickettsia species detected in arthropods from Central America Notes: Ticks associated with human cases of RMSF are represented in bold format. aOnly the first mention in the scientific literature is presented. bCited as Rickettsia amblyommii or Candidatus “Rickettsia amblyommii.” cA. cajennense s.l. probably corresponds to A. mixtum. dCited as A. cajennense. eCited also as R. felis genotype RF2125. fA. sculptum probably corresponds to A. mixtum. gA. triste probably corresponds to A. maculatum. Abbreviation: RMSF, Rocky Mountain spotted fever. |
R. rickettsii has been detected in R. sanguineus s.l. and Dermacentor nitens from Panama,32,44 A. mixtum from Panama and Costa Rica,24,31,45 and Amblyomma varium and Haemaphysalis leporispalustris from Costa Rica.45,46 Contrary to A. mixtum and R. sanguineus s.l., the findings of R. rickettsii in D. nitens, H. leporispalustris, and A. varium were not associated with febrile cases, but may have implications in public health because these are ticks that present different behavior. For example, D. nitens is a one-host tick that mainly parasitizes horses in paddocks and stubble, and parasitism in humans is rare.47 D. nitens commonly shares environments and hosts (equines) with A. mixtum, although this last species is considered an eclectic parasite, and the reports parasitizing humans are frequent.47 In contrast, adults of A. varium parasite almost exclusively sloths and immature have been found parasitizing birds, but very few studies mention humans as hosts.45,48,49 Similarly, H. leporispalustris is an almost exclusive parasite of wild rabbits (Sylvilagus), and parasitism of humans is rare.47 Thus, it is possible that the relevance of these ticks in RMSF transmission is associated with enzootic cycles.
A. mixtum and R. sanguineus s.l. have been previously implicated as vectors of R. rickettsii; in fact, several species of the A. cajennense and R. sanguineus species complexes are among its main vectors in many countries.50 Both are common in or around anthropogenic environments, but differ in preferences: A. mixtum is an eclectic parasite that inhabits paddocks, stubble, and riparian vegetation, while R. sanguineus s.l. feeds mainly from dogs and is a nidicolous species that may thrive inside houses, including highly urbanized areas.31,51 Therefore, their presence could be considered as a first caveat in the transmission of RMSF.31 Even so, many aspects of the ecology of RMSF transmission remain unknown in Central America, especially the role of domestic and wild vertebrates as reservoirs, because few studies in the region have focused on them. Research has resulted in serologic evidence of SFG exposure in dogs and horses from Panama,51 domestic dogs and cats from Costa Rica,53,54 and wild opossums (Didephis marsupialis) and coyotes from Panama.55 These results are a first clue of rickettsial infection in vertebrates that deserves further investigation.
Another closely related pathogenic species, R. parkeri, was recently reported in Central America, infesting Amblyomma maculatum and Amblyomma ovale (specifically the strain Atlantic rainforest) from Belize.56,57 Although A. maculatum and A. ovale frequently parasitize humans,47,58 until now there are no reports of human infection by these species in the region. Although R. parkeri was isolated in 1939, its involvement as a pathogen for humans was not confirmed until 2004.59,60 Clinical evidence shows that R. parkeri infections are usually not lethal and have been confirmed in several states of the USA, Argentina, and Uruguay.61–63 Vectors of R. parkeri include A. maculatum in the USA, as well as Amblyomma triste and Amblyomma tigrinum in South America.60,63
The strain Atlantic rainforest was first detected in Brazil as Rickettsia sp., but recent studies suggest that it belongs to the species R. parkeri.64–66 This strain has been associated with human cases of spotted fever in Brazil, and A. ovale seems to be the main vector.65 In addition to Brazil and Belize, R. parkeri strain Atlantic rainforest has been detected in Argentina (in Amblyomma dubitatum) and Colombia (in A. ovale).67,68
Of the species recognized as human pathogens in Central America, R. felis is the only one that has been detected in fleas, although no human cases have been confirmed in the region. This Rickettsia was first observed in Ctenocephalides felis in 1990; it was officially described in 1996 and the descriptions were emended in 2002.69,70 It is distributed worldwide, as is its main invertebrate host, C. felis. Disease in humans, known as flea-borne spotted fever, was first reported in the USA, Mexico, and Brazil, although it has now been reported from countries around the world; when they occur, symptoms are usually mild and unspecific, but severe cases have been described.71,72 The first findings of R. felis in Central America were documented in Panama and Costa Rica in 2011, from C. felis.52,73 The report from Costa Rica recorded the first isolation of this Rickettsia in a cell line (C6/36) in the region. R. felis has also been detected in C. felis in Guatemala and in dogs from Nicaragua, which suggests that it is also present in fleas in that country.74,75 The absence of reports from the other countries of Central America is probably due to a lack of investigation of rickettsiae in fleas.
It is possible that Rickettsia amblyommatis (referred to as Rickettsia amblyommii and “Candidatus Rickettsia amblyommii”) is the most common Rickettsia detected in Central America. It has been reported in 10 species of ticks and one of fleas in five of the seven countries of Central America (Tables 2 and 3). This Rickettsia was isolated from Amblyomma americanum from the USA and has since been reported along the continent.23,76 The effects of R. amblyommatis infection on vertebrates is not clearly defined. Some authors have pointed out that repeated exposure can induce very high serological titers in dogs.77 In Central America, there is serological evidence of exposure in dogs, horses, and opossums (D. marsupialis) from Panama and dogs from Costa Rica.52,54,55 In this country, the strain 9-CC-3-1 of R. amblyommatis was able to generate pathology and an immune response in guinea pigs, and it was protective against a subsequent infection with a lethal R. rickettsii strain. Therefore, the presence of R. amblyommatis in the region may modulate the epidemiology and severity of RMSF in areas where both the species circulate.78 In humans, despite its frequent presence in several species of ticks, there are no confirmed cases of human rickettsiosis caused by R. amblyommatis, although some authors suggest that humans develop an immune response and that it may cause clinical manifestations.79–82
Rickettsia rhipicephali is a species that has been reported only once in ticks from Central America. It was first isolated and described in 1975 from R. sanguineus in the USA, but it is known to be present also in South America.83,84 This species was detected by PCR in Dermacentor latus from Costa Rica, although currently very few information is available about this finding.85 Moreover, there is also serologic evidence of possible exposure of dogs to this or a very similar Rickettsia sp. from that same country, which supports its possible presence in the region.54 The pathogenic potential of R. rhipicephali in humans is unknown, although the disease has been confirmed in meadow voles after experimental infections.83
In Central America, Rickettsia bellii has been detected in Amblyomma sabanerae from El Salvador, Costa Rica, and Panama (S Bermúdez, unpublished data).85,86 This tick is a parasite of reptiles, in particular turtles and tortoises.47,51 This Rickettsia belongs to ancestral group different from the TG and SFG.3 Although no studies demonstrate its pathogenicity in humans, there is experimental evidence showing rickettsial ability to elicit an immune responses in capybaras.87 In Central America, there is serologic evidence of R. bellii exposure in horses from Panama.52 Thus, the role of R. bellii as a potential human pathogen deserves further investigation.
Rickettsia asembonensis, which is closely related to R. felis, is also present in Central America. This is a recently described species, which was isolated from C. felis from Kenya,88 although it seems to be the same Rickettsia sp. genotype RF2125 that had been reported much earlier in the same flea species in the Thailand–Myanmar border.89–91 R. asembonensis was first documented in C. felis from the Caribbean slope of Costa Rica as the genotype RF2125.74 It was later reported from C. felis in the metropolitan area of that same country (Cartago province), as well as from other species of ectoparasites including Pulex simulans, Rhipicephalus microplus, and A. ovale.45,54 It is unknown if this species is able to infect humans or generates disease.
In addition to the described species of rickettsiae, several rickettsiae that have not been formally described have been reported in Central America. “Candidatus R. nicoyana” was first isolated from Ornithodoros knoxjonesi ticks collected from bats in Costa Rica.92 Two isolates of this Rickettsia were obtained in Vero E6 cell lines, and a partial molecular characterization placed it in the SFG, close to “Candidatus Rickettsia wissemanii” and Rickettsia peacockii. In addition, Rickettsia sp. strain Colombianensi has been detected in Amblyomma dissimile from both Honduras and Costa Rica.85,93 This strain was first reported in A. dissimile and R. sanguineus from Colombia, and it groups phylogenetically with Rickettsia tamurae and R. monacensis within the SFG.94 In Guatemala, a Rickettsia sp. genetically similar to R. africae and Rickettsia sibrica was detected in A. cajennense s.l. (probably A. mixtum).40
Recently, Rickettsia spp. were reported in Dermacentor dissimilis, A. maculatum and R. sanguineus s.l. from Nicaragua, as part of a microbiome study.97 These data require further investigation in order to identify the species present and determine whether they represent a health threat for humans or animals. In addition, another study in Nicaragua reported R. africae in A. ovale and a Rickettsia sp. (matching strain Aragaoi) in an A. triste.98 Considering that rickettsiae related to R. africae have been detected in ticks from both Guatemala and Nicaragua,40,98 further studies will be needed to determine their taxonomic status and related ecology.
Lastly, several Rickettsia strains have been detected in the species of Ixodes from Central America, including I. boliviensis (Rickettsia sp. strain IbR/CRC) and I. minor (Rickettsia sp. strain Barva) from Costa Rica, and Ixodes affinis from Belize.56,95,96 These rickettsiae seem to be closely related to each other and group closely related to R. monacensis, as well as endosymbionts of Ixodes from North America. For all of these “unofficial” species, the potential pathogenicity for humans is yet to be determined.
Conclusion
In Central America, the development of research related to the ecology of ectoparasites and their role as vectors of Rickettsia has generated a considerable amount of information in the last 10 years, both in anthropogenic environments and in wild areas.99 However, there is still a need to improve the awareness and diagnosis of cases, as well as to expand on eco-epidemiological studies especially in countries where information is still lacking. The data available from ticks and fleas suggest that these bacteria are widely distributed in the region; thus, rickettsioses could be an underestimated problem in the absence of greater diagnostic efforts in undetermined febrile cases.
Acknowledgments
The authors thank Dr Nicole Gottdenker (University of Georgia) for the helpful comments, grammatical editing, and revision of English language. A Troyo’s contributions were supported in part by University of Costa Rica project ED-548.
Disclosure
The authors report no conflicts of interest in this work.
References
Fang R, Blanton LS, Walker DH. Rickettsiae as emerging infectious agents. Clin Lab Med. 2017;37(2):383–400. | ||
Fenollar F, Fournier P, Raoult D. Diagnostic strategy of rickettsioses and ehrlichioses. In: Raoult D, Parola P, editors. Rickettsial Diseases. New York: Informa Healthcare; 2007:315–330. | ||
Fournier P, Raoult D. Bacteriology, taxonomy, and phylogeny of Rickettsia. In: Raoult D, Parola P, editors. Rickettsial Diseases. New York: Informa Healthcare; 2007:1–14. | ||
Houmhandi L, Raoult D. Louse-borne epidemic typhus. In: Raoult D, Parola P, editors. Rickettsial Diseases. New York: Informa Healthcare; 2007:51–61. | ||
Tselentis Y, Gikas A. Murine typhus. In: Raoult D, Parola P, editors. Rickettsial Diseases. New York: Informa Healthcare; 2007:38–49. | ||
The Center for Food Security and Public Health. Rickettsia prowazekii infections. Iowa State University [updated 2017]. Available from: http://www.cfsph.iastate.edu/Factsheets/pdfs/typhus_fever.pdf. Accessed March 7, 2018. | ||
Parola P. Rickettsia felis: from a rare disease in the USA to a common cause of fever in sub-Saharan Africa. Clin Microbiol Infect. 2011;17(7):996–1000. | ||
Valbuena G. Patogénesis de las rickettsiosis en las Américas [Pathogenesis of infections caused by rickettsiae in the Americas]. Rev MVZ. 2010;15(1):2004–2006. Spanish. | ||
Minniear TD, Buckingham SC. Managing Rocky Mountain spotted fever. Expert Rev Anti Infect Ther. 2009;7(9):1131–1137. | ||
Oteo JA, Nava S, de Sousa R, et al. Guías latinoamericanas de la RIICER para el diagnóstico de las rickettsiosis transmitidas por garrapatas [Latinamerican guidelines of RIICER for diagnosis of tick-borne rickettsioses]. Rev Chilena Infectol. 2014;31(1):54–65. Spanish. | ||
Eremeeva M, Dasch G. Challenges posed by tick-borne rickettsiae: eco-epidemiology and public health implications. Front Public Health. 2015;3:55. | ||
Hume E. Spanish colonial medicine. Bull Johns Hopkins Hosp. 1934;2(4):215–230. | ||
Romero A, Zeissig O, España D, Rizzo L. Tifus exantemático en Guatemala [Exanthematic typhus in Guatemala]. Bol Oficina Santit Panam. 1977;83(3):223–236. Spanish. | ||
Raoult D, Woodward T, Dumler JS. The history of epidemic typhus. Infect Dis Clin North Am. 2004;18(1):127–140. | ||
Martínez-Ortíz D, Torres-Castro M, Koyoc-Cardeña E, et al. Detección molecular de Rickettsia typhi en perros de una comunidad rural de Yucatán, México [Molecular evidence of Rickettsia typhi infection in dogs from a rural community in Yucatán, México]. Biomédica. 2016;36(Suppl 1):45–50. Spanish. | ||
Walter G, Botelho-Nevers E, Scolovschi C, Raoult D, Parola P. Murine typhus in returned travelers: a report of thirty-two cases. Am J Trop Med Hyg. 2012;86(6):1049–1053. | ||
Calero C. Outbreak of typhus of the murine type. First report from the Isthmus of Panama. Am J Trop Med Hyg. 1948;28(2):313–321. | ||
Peacock M, Ormsbee R, Johnson K. Rickettsioses of Central America. Am J Trop Med Hyg.1971;20(6):941–949. | ||
WHO. Global surveillance of rickettsial diseases: Memorandum from a WHO meeting. Bull World Health Organ. 1993;71(3/4):293–296. | ||
Bermúdez S, Lyons C, García G, Zaldívar Y, Gabster A, Arteaga G. Serologic evidence of human Rickettsia infection found in three locations in Panama. Biomédica. 2013;33(Suppl 1):31–37. | ||
Wilson LB, Chowning WM. Studies in piroplasmosis hominis. (“spotted fever” or “tick fever” of the Rocky Mountains). J Infect Dis. 1904;1:31–57. | ||
Walker DH. Ricketts creates Rickettsiology, the study of vector-borne, obligately intracellular bacteria. J Infect Dis. 2004;189(5):938–955. | ||
Labruna M, Mattar S, Nava S, et al. Rickettsioses in Latin America, Caribbean, Spain and Portugal. Revista MVZ. 2011;16(2):2435–2457. | ||
de Rodaniche EC, Rodaniche A. Spotted fever in Panama; isolation of the etiologic agent from a fatal case. Am J Trop Med Hyg. 1950;30(4):511–517. | ||
de Rodaniche EC. Natural infection of the tick, Amblyomma cajennense, with Rickettsia rickettsii in Panama. Am J Trop Med Hyg. 1953;2(4):696–699. | ||
Calero C, Nuñez JM, Silva-Goytía R. Rocky Mountain spotted fever in Panama; report of two cases. Am J Trop Med Hyg. 1952;1(4):631–636. | ||
Silva-Goytia R, Calero C. Estudio sobre fiebre manchada, fiebre Q y tifus exantemático en el istmo de Panamá [Studies on spotted fever, Q fever and exanthematous typhus in the Isthmus of Panama]. Arch Med Panam. 1956;5:99–106. Spanish. | ||
Estripeaut D, Aramburú MG, Sáez-Llorens X, et al. Rocky Mountain spotted fever, Panama. Emerg Infec Dis. 2007;13(11):1763–1765. | ||
Tribaldos M, Zaldivar Y, Bermudez S, et al. Rocky Mountain spotted fever in Panama: a cluster description. J Infec Dev Ctries. 2011;5:737–741. | ||
De Lucas J, García E, García G, et al. Nuevo caso de rickettsiosis humana en Panamá, a partir de evidencia serológica y clínica [New case of human rickettsiosis in Panama, from serologic and clinical evidences]. Rev Méd Pan. 2013;34:40–43. Spanish. | ||
Bermúdez SE, Castro AM, Trejos D, et al. Distribution of spotted fever group rickettsiae in hard ticks (Ixodida: Ixodidae) from Panamanian urban and rural environments (2007–2013). EcoHealth. 2016;13(2):274–284. | ||
Martínez-Caballero, Moreno B, González C, et al. Descriptions of two new cases of Rocky Mountain spotted fever in Panama, and coincident infection with Rickettsia rickettsii in Rhipicephalus sanguineus s.l. in an urban locality of Panama City, Panama. Epi Infec. In press 2018. | ||
Bermudez SE, Lyons CR, García GG, et al. Detection of Rickettsia rickettsii on Rhipicephalus sanguineus s.l., a new scenario in the transmission of spotted fever in Panamá. Rev Colomb Cienc Pecu. 2017;30(Supl):304–305. | ||
Hun L. Las fiebres manchadas y su importancia en Costa Rica [Spotted fevers and their importance in Costa Rica]. Acta Med Costarric. 2008;50(2):77–86. Spanish. | ||
Hun L. Rickettsiosis en Costa Rica [Rickettsiosis in Costa Rica]. Acta Med Costarric. 2013;55(Suppl 1):25–28. Spanish. | ||
Campbell CC, Hobbs JH, Marranghello L, Vargas M, Shepard C, Feldman RA. An apparent outbreak of rickettsial illness in Costa Rica, 1974. Bull Panam Health Organ. 1978;12(2):104–111. | ||
Fuentes LG. Primer caso de fiebre de las Montañas Rocosas en Costa Rica, América Central [First case of Rocky Mountain Spotted Fever in Costa Rica, Central America]. Rev Latinoam Microbiol. 1979;21:167–172. Spanish. | ||
Fuentes LG. Ecological study of Rocky Mountain spotted fever in Costa Rica. Am J Trop Med Hyg. 1986;35(1):192–196. | ||
Argüello AP, Hun L, Rivera P, Taylor L. Case report: a fatal urban case of Rocky Mountain spotted fever presenting an eschar in San José, Costa Rica. Am J Trop Med Hyg. 2012;87(2):345–348. | ||
Eremeeva ME, Berganza E, Suarez G, et al. Investigation of an outbreak of rickettsial febrile illness in Guatemala, 2007. Int J Infect Dis. 2013;17(5):304–311. | ||
Chen LH, Wilson ME. Tick-borne rickettsiosis in traveler returning from Honduras. Emerg Infect Dis. 2009;15(8):1321–1323. | ||
Reller M, Chikeka I, Miles J, et al. First identification and description of rickettsioses and Q fever as causes of acute febrile illness in Nicaragua, 2016. PLoS Negl Trop Dis. 2016;10(12):e0005185. | ||
Wood H, Drebot MA, Dewailly E, et al. Seroprevalence of seven zoonotic pathogens in pregnant women from the Caribbean. Am J Trop Med Hyg. 2014;91(3):642–644. | ||
Bermúdez SE, Eremeeva ME, Karpathy SE, et al. Detection and identification of rickettsial agents in ticks from domestic mammals in Eastern Panama. J Med Entomol. 2009;46(4):856–861. | ||
Troyo A, Moreira-Soto RD, Calderon-Arguedas O, et al. Detection of rickettsiae in fleas and ticks from areas of Costa Rica with history of spotted fever group rickettsioses. Ticks Tick Borne Dis. 2016;7(6):1128–1134. | ||
Fuentes L, Calderón A, Hun L. Isolation and identification of Rickettsia rickettsii from the rabbit tick Haemaphysalis leporispalustris in the Atlantic zone of Costa Rica. Am J Trop Med Hyg. 1985;34(3):564–567. | ||
Guglielmone RA, Robbins RG, Apanaskevich DA, et al. The Hard Ticks of the World. Dordrecht: Springer; 2014. | ||
Ogrzewalska M, Pinter A. Ticks (Acari: Ixodidae) as ectoparasites of Brazilian wild birds and their association with rickettsial diseases. Braz J Vet Res Anim Sci. 2016;53(1):1–31. | ||
Serra-Freire NM. Occurrence of ticks (Acari: Ixodidae) on human hosts, in three municipalities in the State of Pará, Brazil. Rev Bras Parasitol Vet. 2010;19(3):141–147. | ||
Dantas-Torres F. Rocky Mountain spotted fever. Lancet Infec Dis. 2007;7(11):724–732. | ||
Fairchild G, Kohls G, Tipton J. The ticks of Panama (Acarina: Ixodoidea). In: Wenzel RL, Tipton VJ, editors. Ectoparasites of Panama. Chicago: Field Museum of Natural History; 1966:167–207. | ||
Bermúdez SE, Zaldívar AY, Spolidorio MG, et al. Rickettsial infection in domestic mammals and their ectoparasites in El Valle de Antón, Coclé, Panamá. Vet Parasitol. 2011;177(1–2):134–138. | ||
Fonseca-Salazar L, Gutiérrez-Fernández R, Moreira-Soto RD, et al. Exposición de gatos a Rickettsia felis y otras rickettsias del grupo fiebres manchadas en Costa Rica [Exhibition of cats to Rickettsia felis and other rickettsiae from the group of spotted fevers in Costa Rica]. Biomédica. 2016;26(Suppl 1):143–144. Spanish. | ||
Moreira-Soto A, Carranza MV, Taylor L, Calderon-Arguedas O, Hun L, Troyo A. Exposure of dogs to spotted fever group rickettsiae in urban sites associated with human rickettsioses in Costa Rica. Ticks Tick Borne Dis. 2016;7(5):748–753. | ||
Bermúdez SE, Gottdenker N, Krishnavajhala A, et al. Synanthropic mammals as potential hosts of tick-borne pathogens in Panama. PLoS One. 2017;12(1):e0169047. | ||
Lopes MG, May Junior J, Foster RJ, et al. Ticks and rickettsiae from wildlife in Belize, Central America. Parasit Vectors. 2016;9:62. | ||
Polsomboon S, Hoel DF, Murphy JR. Molecular detection and identification of Rickettsia species in ticks (Acari: Ixodidae) collected from Belize, Central America. J Med Entomol. 2017;54(6):1718–1726. | ||
Murgas IL, Castro AM, Bermúdez SE. Current status of Amblyomma ovale (Acari: Ixodidae) in Panama. Ticks Tick Borne Dis. 2013;4(1–2):164–166. | ||
Parker RR, Kohls GM, Cox GW, Davis GE. Observations on an infectious agent from Amblyomma maculatum. Public Health Rep. 1939;54:1482–1484. | ||
Paddock CD, Sumner JW, Comer JA, et al. Rickettsia parkeri: a newly recognized cause of spotted fever rickettsiosis in the United States. Clin Infect Dis. 2004;38(6):805–811. | ||
Pacheco RC, Horta MC, Moraes-Filho J, Ataliba AC, Pinter A, Labruna MB. Rickettsial infection in capybaras (Hydrochaeris hydrochoerus) from São Paulo, Brazil: serological evidence for infection by Rickettsia bellii and Rickettsia parkeri. Biomédica. 2007;27(3):364–371. | ||
Silveira I, Pacheco RC, Szabó MPJ, Ramos HGC, Labruna MB. Rickettsia parkeri in Brazil. Emerg Infect Dis. 2007;13(7):1111–1113. | ||
Venzal JM, Nava S. El género Rickettsia como agente de zoonosis en el cono sur de Suramérica [Rickettsia as zoonotic agent in the Southern Cone of America]. Rev Med Urug. 2011;27(2):98–106. Spanish. | ||
Spolidorio MG, Labruna MB, Mantovani E, Brandão PE, Richtzenhain LJ, Yoshinari NH. Novel spotted fever group rickettsiosis, Brazil. Emerg Infect Dis. 2010;16(3):521–523. | ||
Allerdice MEJ, Beati L, Yaglom H, et al. Rickettsia parkeri (Rickettsiales: Rickettsiaceae) detected in ticks of the Amblyomma maculatum (Acari: Ixodidae) group collected from multiple locations in southern Arizona. J Med Entomol. 2017;54(6):1743–1749. | ||
Silveira I, Martins TF, Olegário MM, et al. Rickettsial infection in animals, humans and ticks in Paulicéia, Brazil. Zoonoses Public Health. 2015;62(7):525–533. | ||
Monje LD, Nava S, Eberhardt AT, Correa AI, Guglielmone AA, Beldomenico PM. Molecular detection of the human pathogenic Rickettsia sp. strain Atlantic rainforest in Amblyomma dubitatum ticks from Argentina. Vector Borne Zoonotic Dis. 2015;15(2):167–169. | ||
Londoño AF, Díaz FJ, Valbuena G. et al. Infection of Amblyomma ovale by Rickettsia sp. strain Atlantic rainforest, Colombia. Ticks Tick Borne Dis. 2014;5(6):672–675. | ||
Higgins JA, Radulovic S, Schriefer ME, Azad AF. Rickettsia felis: a new species of pathogenic rickettsia isolated from cat fleas. J Clin Microbiol. 1996;34(3):671–674. | ||
La Scola B, Meconi S, Fenollar F, Rolain JM, Roux V, Raoult D. Emended description of Rickettsia felis (Bouyer et al. 2001), a temperature-dependent cultured bacterium. Int J Syst Evol Microbiol. 2002;52(Pt 6):2035–2041. | ||
Hun L, Troyo A. An update on the detection and treatment of Rickettsia felis. Res Rep Trop Med. 2012;3:47–55. | ||
Parola P, Paddock CD, Socolovschi C, et al. Update on tick-borne rickettsioses around the world: a geographic approach. Clin Microbiol Rev. 2013;26(4):657–702. | ||
Hun L, Troyo A, Taylor L, Barbieri AM, Labruna MB. First report of the isolation and molecular characterization of Rickettsia amblyommii and Rickettsia felis in Central America. Vector Borne Zoonotic Dis. 2011;11(10):1395–1397. | ||
Troyo A, Álvarez D, Taylor L, et al. Rickettsia felis in Ctenocephalides felis from Guatemala and Costa Rica. Am J Trop Med Hyg. 2012;86(6):1054–1056. | ||
Wei L, Kelly P, Ackerson K, et al. First report of Babesia gibsoni in Central America and survey for vector-borne infections in dogs from Nicaragua. Parasit Vectors. 2014;7:126. | ||
Karpathy SE, Slater KS, Goldsmith CS, Nicholson WL, Paddock CD. Rickettsia amblyommatis sp. nov., a spotted fever group Rickettsia associated with multiple species of Amblyomma ticks in North, Central and South America. Int J Syst Evol Microbiol. 2016;66(12):5236–5243. | ||
Barret A, Little SE, Shaw E. “Rickettsia amblyommii” and R. montanensis infection in dogs following natural exposure to ticks. Vector Borne Zoonotic Dis. 2014;14(1):20–25. | ||
Rivas JJ, Moreira-Soto A, Alvarado G, et al. Pathogenic potential of a Costa Rican strain of “Candidatus Rickettsia amblyommii” in guinea pigs (Cavia porcellus) and protective immunity against Rickettsia rickettsii. Ticks Tick Borne Dis. 2015;6(6):805–811. | ||
Dasch GA, Kelly DJ, Richards AL, Sanchez JL, Rives CC. Western blotting analysis of sera from military personnel exhibiting serological reactivity to spotted fever group rickettsiae. Am J Trop Med Hyg. 1993;49(Suppl 1):220. | ||
Billeter SA, Blanton HL, Little SE, Levy MG, Breitschwerdt EB. Detection of Rickettsia amblyommii in association with a tick bite rash. Vector Borne Zoonotic Dis. 2007;7(4):607–610. | ||
Apperson CS, Engber B, Nicholson WL, et al. Tick-borne diseases in North Carolina: is “Rickettsia amblyommii” a possible cause of rickettsiosis reported as Rocky Mountain spotted fever? Vector Borne Zoonotic Dis. 2008;8(5):597–606. | ||
Jiang J, Yarina T, Miller MK, Stromdahl EY, Richards AL. Molecular detection of Rickettsia amblyommii in Amblyomma americanum parasitizing humans. Vector Borne Zoonotic Dis. 2010;10(4):329–340. | ||
Parola P, Padock CD, Socolovschi C, et al. Update on tick-borne rickettsioses around the world: a geographic approach. Clin Microbiol Rev. 2013;26(4):657–702. | ||
Labruna MB, Pacheco RC, Richtzenhain LJ, Szabó MP. Isolation of Rickettsia rhipicephali and Rickettsia bellii from Haemaphysalis juxtakochi ticks in the state of São Paulo, Brazil. Appl Environ Microbiol. 2007;73(3):869–873. | ||
Moreira-Soto RD, Moreira-Soto A, Calderón-Arguedas O, Jiménez M, Corrales-Aguilar E, Troyo A. Rickettsias en ectoparásitos de fauna silvestre de Costa Rica [Rickettsiae in ectoparasites of wildlife in Costa Rica]. Biomédica. 2015;26(Suppl 1):45–46. Spanish. | ||
Barbieri AR, Romero L, Labruna MB. Rickettsia bellii infecting Amblyomma sabanerae ticks in El Salvador. Pathog Glob Health. 2012;106(3):188–189. | ||
Pacheco RC, Horta MC, Moraes-Filho J, Ataliba AC, Pinter A, Labruna MB. Rickettsial infection in capybaras (Hydrochoerus hydrochaeris) from São Paulo, Brazil: serological evidence for infection by Rickettsia bellii and Rickettsia parkeri. Biomédica. 2007;27(3):364–371. | ||
Maina AN, Luce-Fedrow A, Omulo S, et al. Isolation and characterization of a novel Rickettsia species (Rickettsia asembonensis sp. nov.) obtained from cat fleas (Ctenocephalides felis). Int J Syst Evol Microbiol. 2016;66(11):4512–4517. | ||
Parola P, Sanogo OY, Lerdthusnee K, et al. Identification of Rickettsia spp. and Bartonella spp. in from the Thai-Myanmar border. Ann N Y Acad Sci. 2003;990:173–181. | ||
Jiang J, Maina AN, Knobel DL, et al. Molecular detection of Rickettsia felis and Candidatus Rickettsia asemboensis in fleas from human habitats, Asembo, Kenya. Vector Borne Zoonotic Dis. 2013;13(8):550–558. | ||
Oteo JA, Portillo A, Portero F, Zavala-Castro J, Venzal JM, Labruna MB. “Candidatus Rickettsia asemboensis” and Wolbachia spp. in Ctenocephalides felis and Pulex irritans fleas removed from dogs in Ecuador. Parasit Vectors. 2014;7:455. | ||
Moreira-Soto RD, Moreira-Soto A, Corrales-Aguilar E, Calderón-Arguedas Ó, Troyo A. “Candidatus Rickettsia nicoyana”: a novel Rickettsia species isolated from Ornithodoros knoxjonesi in Costa Rica. Ticks Tick Borne Dis. 2017;8(4):532–536. | ||
Novakova M, Literak I, Chevez L, Martins TF, Ogrzewalska M, Labruna MB. Rickettsial infections in ticks from reptiles, birds and humans in Honduras. Ticks Tick Borne Dis. 2015;6(6):737–742. | ||
Miranda J, Portillo A, Oteo JA, Mattar S. Rickettsia sp. strain colombianensi (Rickettsiales: Rickettsiaceae): a new proposed Rickettsia detected in Amblyomma dissimile (Acari: Ixodidae) from iguanas and free-living larvae ticks from vegetation. J Med Entomol. 2012;49(4):960–965. | ||
Troyo A, Moreira-Soto A, Carranza M, Calderón-Arguedas O, Hun L, Taylor L. Detection of an undescribed Rickettsia sp. in Ixodes boliviensis from Costa Rica. Ticks Tick Borne Dis. 2014;5(6):883–886. | ||
Ogrzewalska M, Literák I, Capek M, et al. Bacteria of the genus Rickettsia in ticks (Acari: Ixodidae) collected from birds in Costa Rica. Ticks Tick Borne Dis. 2015;6(4):478–482. | ||
Tauer A, Fiorello C, Düttmann C. The tick microbiome at the interface of domestic animals and wildlife in Nicaragua. Poster presented at: Wildlife Diseases Association; July 2017; Chiapas, Mexico. | ||
Vogel H, Foley J, Fiorello CV. Rickettsia africae and novel rickettsial strain in Amblyomma spp. ticks, Nicaragua, 2013. Emerg Infect Dis. 2018;24(2):385–387. | ||
Castro AM, García GG, Dzul-Rosado K, et al. Questing Amblyomma mixtum and Haemaphysalis juxtakochi (Acari: Ixodidae) infected with Candidatus “Rickettsia amblyommii” from the natural environment in Panama Canal Basin, Panama. Trop Med Health. 2015;43(4):217–222. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.