Back to Journals » Neuropsychiatric Disease and Treatment » Volume 13
A review of the efficacy of atomoxetine in the treatment of attention-deficit hyperactivity disorder in children and adult patients with common comorbidities
Authors Clemow DB, Bushe C, Mancini M, Ossipov MH, Upadhyaya H
Received 24 June 2016
Accepted for publication 3 November 2016
Published 3 February 2017 Volume 2017:13 Pages 357—371
DOI https://doi.org/10.2147/NDT.S115707
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
David B Clemow,1 Chris Bushe,2 Michele Mancini,3 Michael H Ossipov,4 Himanshu Upadhyaya1
1Eli Lilly and Company, Indianapolis, IN, USA; 2Eli Lilly, Windlesham, UK; 3Eli Lilly Italia S.p.A., Sesto Fiorentino, Italy; 4inVentiv Health Clinical, LLC, Blue Bell, PA, USA
Abstract: Attention-deficit hyperactivity disorder (ADHD) is a common neuropsychiatric disorder that is often diagnosed during childhood, but has also increasingly been recognized to occur in adults. Importantly, up to 52% of children (including adolescents) and 87% of adults with ADHD also have a comorbid psychiatric disorder. The presence of a comorbid disorder has the potential to impact diagnosis and could affect treatment outcomes. Atomoxetine is a nonstimulant treatment for ADHD. Despite numerous published studies regarding efficacy of atomoxetine in the treatment of ADHD in patients with comorbid disorders, there is limited information about the impact of individual common comorbid disorders on the efficacy of atomoxetine for ADHD, especially with regard to adults. Moreover, a cumulative review and assessment of these studies has not been conducted. For this reason, we performed a literature review to find, identify, and cumulatively review clinical studies that examined the efficacy of atomoxetine in the treatment of patients with ADHD and comorbid psychiatric disorders. We found a total of 50 clinical studies (37 in children; 13 in adults) that examined the efficacy of atomoxetine in patients with ADHD and a comorbid disorder. The comorbidities that were studied in children or in adults included anxiety, depression, and substance use disorder. Overall, the presence of comorbidity did not adversely impact the efficacy of atomoxetine in treatment of ADHD symptoms in both patient populations. In the studies identified and assessed in this review, atomoxetine did not appear to exacerbate any of the comorbid conditions and could, therefore, be an important therapy choice for the treatment of ADHD in the presence of comorbid disorders.
Keywords: comorbid psychiatric disorders, ADHD in children or adolescents, adult attention-deficit hyperactivity disorder, ADHD
Introduction
Attention-deficit hyperactivity disorder (ADHD) is a common neuropsychiatric disorder in both children and adults.1 The global incidence of ADHD in children (ie, less than 18 years of age) ranges between 5.9% and 7.1%, and in adults, it ranges between 3% and 5%.1–3 A considerable proportion of individuals diagnosed with ADHD as children continue to need long-term therapy into adulthood4,5 and are at risk for continued difficulties with employment, social interactions, and education, and even have increased mortality risk.4,6,7
Complicating the clinical picture of patients with ADHD is the realization that a majority of these patients are likely to have coexisting psychiatric disorders.8–11 A recent study of 14,825 patients in Danish psychiatric inpatient or outpatient clinics who were between the ages of 4 and 17 years and diagnosed with ADHD for the first time between 1995 and 2010 found that 52% had at least 1 comorbid disorder and 26% had 2 or more comorbid disorders.8 The incidence of comorbidities in children with ADHD is summarized in Table 1.
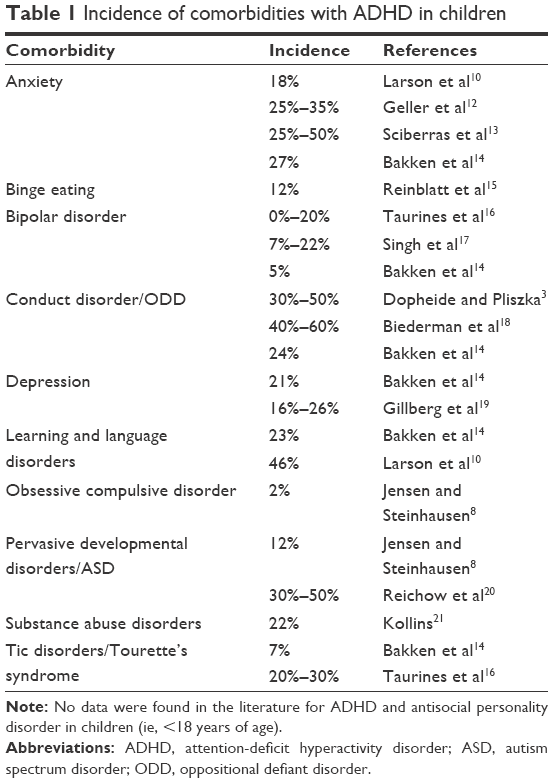 | Table 1 Incidence of comorbidities with ADHD in children |
It appears that adults with ADHD may have a higher incidence of comorbid disorders than do children. In a large family study, it was found that 87% of adults with ADHD had at least 1 comorbid psychiatric disorder, and 56% had at least 2 disorders.22 In this study, the most common comorbidities were anxiety, depression, mood disorders, and substance use disorder (SUD). Of note, adult ADHD is under-treated;23–25 consequently, treatment paradigms for adults, especially in the presence of a comorbid condition, are not as well established as for children, emphasizing the importance of establishing reliable treatment paradigms in this population. The incidence of comorbidities in adults with ADHD is summarized in Table 2. Tables 1 and 2 provide detailed insight into the incidence of each type of comorbidity, and list the comorbidities for which no studies were identified in the literature search.
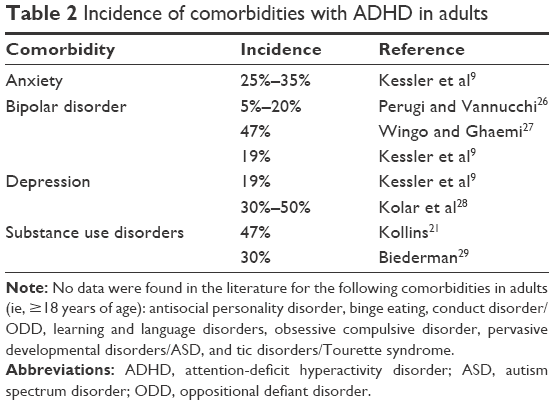 | Table 2 Incidence of comorbidities with ADHD in adults |
Although the stimulants, which include various formulations of methylphenidates and amphetamines, provide good efficacy in treating symptoms of ADHD, these drugs are often contraindicated in patients with comorbid disorders, including Tourette’s syndrome and bipolar disorder, as well as in patients at risk for substance abuse.30–32 Further, some investigators advise caution in prescribing these products to patients with comorbid disorders that are not explicitly contraindicated, such as tic disorders33 and anxiety.3,34 Suicidal ideation is a symptom that may be present in ADHD patients with comorbid psychiatric disorders, especially depression and bipolar disorder. The presence of suicidal ideation in ADHD patients is a contraindication for methylphenidate in the European Union (EU).32 The labeling of both the EU and the US has a warning regarding suicidal ideation in child ADHD patients taking atomoxetine.35–38
The selective noradrenergic reuptake inhibitor atomoxetine is approved for the treatment of ADHD in children and adults.6 Moreover, it has no abuse potential, and consequently, atomoxetine is considered a first-line therapy for patients at risk for substance abuse disorders.28,39,40 In addition, atomoxetine is often preferred over stimulants for patients with ADHD and comorbid tic disorders or anxiety.28,33,40–42 Data from recent longer-term studies that incorporate current ADHD trial design concepts also show that there is equivalent efficacy for atomoxetine and methylphenidate, both in adults and children,43,44 including data from the most recent updated network meta-analysis. Reported effect sizes for atomoxetine in children with ADHD are consistent with those for the stimulants and range from 0.6 to 1.3.45 Effect sizes for atomoxetine in adults were estimated to be 0.40 and 0.41, which are within the range reported for methylphenidate in adults as well.45
Because of the high incidence of psychiatric comorbidities in patients with ADHD, an alternative to stimulants that may be contraindicated due to comorbidities could be warranted in some cases. Therefore, understanding the effect of comorbidities on atomoxetine ADHD treatment is clinically relevant. Thus, the aim of this literature review was to provide insight into the effects of comorbid disorders on the efficacy of atomoxetine for the treatment of ADHD symptomology. To the best of our knowledge, there are no comprehensive reviews collectively covering the common ADHD comorbidities in relationship to ADHD treatment for children and adults. The current findings may aid physicians making treatment algorithm decisions that include atomoxetine for patients with ADHD and psychiatric comorbidities.
Methods
The strategy for the literature search was a thorough review conducted in PubMed. Searches were conducted for (atomoxetine [Title OR Abstract] AND [search term (Title OR Abstract)]). The search was repeated for every item on the list of search terms (Table 3). The searches were limited to articles in English and covering human clinical data (animal data were not included). Each output item was examined for document type (ie, original article, review, case report), and any article that discussed the efficacy of atomoxetine in the treatment of ADHD in patients who also had 1 of the comorbidities was included in this review. Review articles that were discovered by the search were examined and included in the present review if they contained original research results that were not otherwise captured by the literature search. Moreover, only studies that employed validated ADHD rating scales, such as the Attention-Deficit/Hyperactivity Disorder Rating Scale or the Adult ADHD Self-Report Scale-v1.1, were included. Clinical reports representing results found with a single patient were not included in this review. The searches were not limited by time period. The search terms were selected to cover the common comorbidities, and associated search terms were employed to broaden the search. Further, the general term “anxiety” would return specific disorders such as “social anxiety”. Tables 1 and 2 indicate the comorbidities that were found to be common based on the literature search and practical clinical experience. Tables 1 and 2 also provide published estimates of the incidence of these comorbidities in children and adults with ADHD, respectively. It should be noted that, throughout this review, the terms “child” or “children” are used to describe all patients aged less than 18 years. Although some studies might refer to “adolescents”, the age ranges tended to vary, and data were not stratified to select age groups other than those aged less than 18 years and 18 years or more. Unless otherwise indicated, the terms “significant” or “significantly” refer to statistical significance.
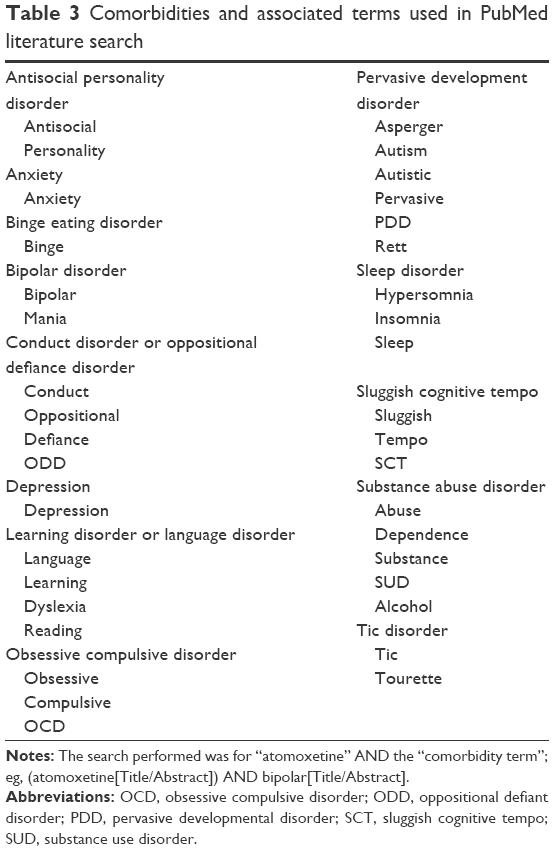 | Table 3 Comorbidities and associated terms used in PubMed literature search |
Results
The search yielded a total of 50 studies that included ADHD and atomoxetine and at least 1 comorbid disorder. Of these, 37 were in reference to children, whereas 13 were studies performed with adults.
Of the studies performed with children, 23 were double-blind, placebo-controlled randomized clinical trials (RCTs). Among these 23, there were 3 meta-analyses of RCTs and 4 post hoc subgroup analyses of RCTs. One of the RCTs was preceded by an open-label phase, and another contained an open-label extension. In addition, there were 10 open-label studies, including 4 prospective open-label studies. We also found 2 retrospective chart reviews, 1 retrospective review of medical records, and 1 consecutive case series in this search. No results were returned for atomoxetine in ADHD and antisocial personality disorder, binge eating disorders, or obsessive compulsive disorder in children. The studies on atomoxetine use in children with ADHD and at least 1 comorbid disorder identified in our literature search are summarized in Table 4.
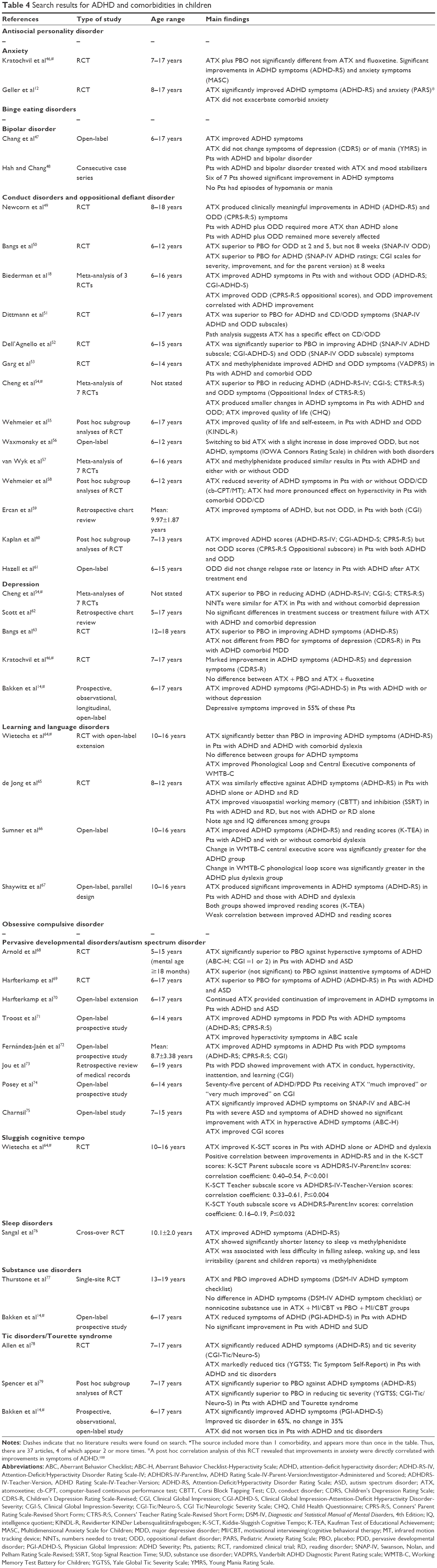 | Table 4 Search results for ADHD and comorbidities in children |
Of the 13 studies that were found with regard to adult patients with ADHD and a comorbidity, 9 were RCTs, including 2 post hoc subgroup analyses. The remaining 4 studies included 3 open-label investigations and a within-subject retrospective design with naturalistic follow-up. No results were found for atomoxetine-treated adults with ADHD and either antisocial personality disorder, binge eating disorders, bipolar disorder, conduct disorders (CDs), oppositional defiant disorder (ODD), learning and language disorders, obsessive compulsive disorder, pervasive developmental disorders/autism spectrum disorder (ASD), sluggish cognitive tempo (SCT), or sleep disorders. The studies on atomoxetine use in adults with ADHD and at least 1 comorbid disorder identified in our literature search are summarized in Table 5.
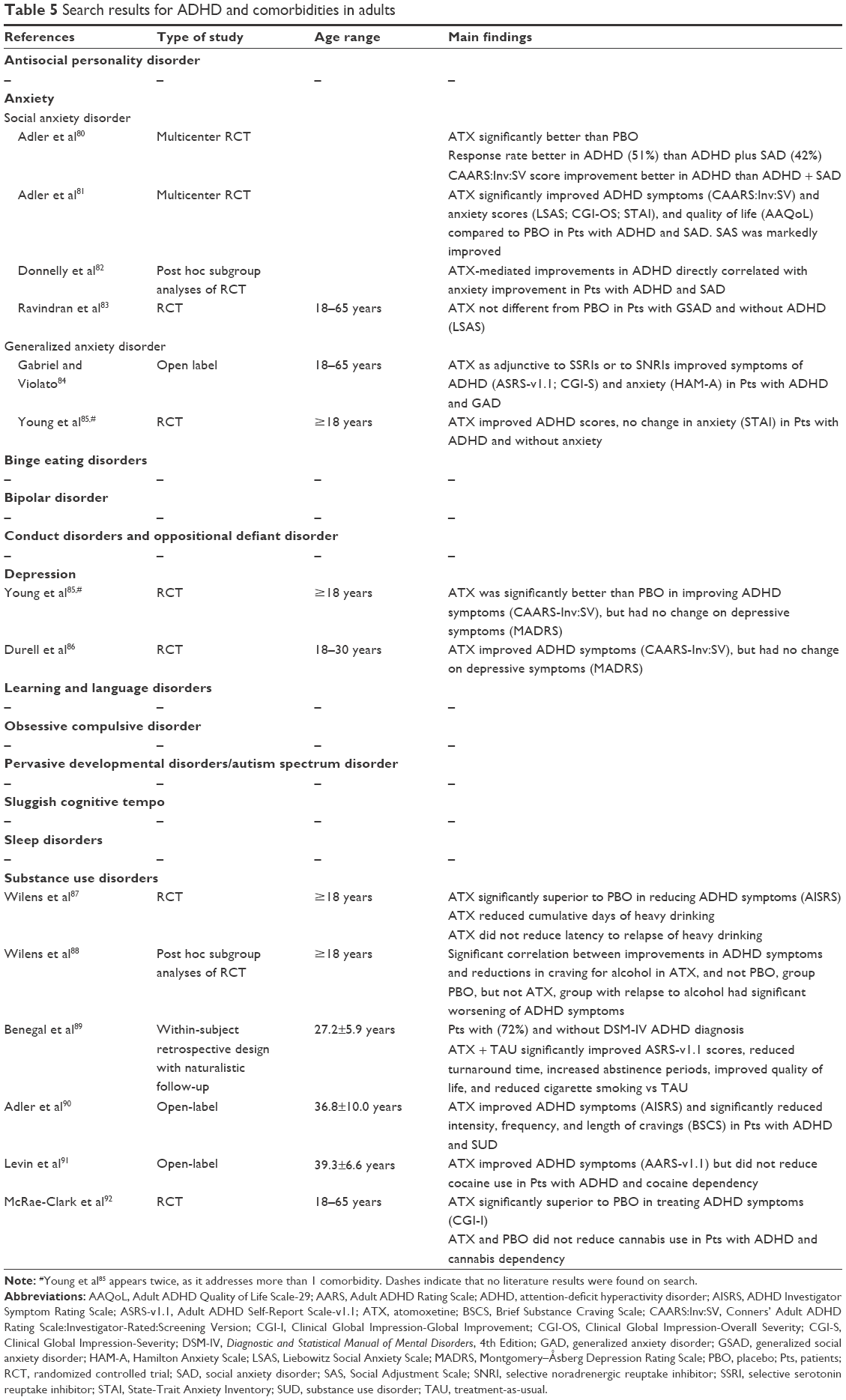 | Table 5 Search results for ADHD and comorbidities in adults |
Effects of atomoxetine in children with ADHD and comorbidity
Anxiety
Anxiety is one of the common comorbidities found in children with ADHD and affects approximately 18% of children with ADHD, which is substantially greater than the 2% incidence reported in children without ADHD.10,93 Other studies have estimated the comorbidity of anxiety occurs in 25%–50% of children with ADHD.12,13 In spite of the rather large incidence of this comorbidity, only 2 studies were found that addressed the use of atomoxetine in young patients with ADHD and anxiety.12,46 In those studies, atomoxetine improved symptoms of ADHD and did not exacerbate anxiety in these patients. Moreover, there was some evidence that symptoms of anxiety were reduced in these patients.12,46
Bipolar disorder
Comorbid bipolar disorder is also a clinical concern, affecting up to 22% of children with ADHD.16 Only 1 open-label study and 1 consecutive case series were found addressing atomoxetine use for ADHD in patients with comorbid bipolar disorder.47,48 These studies indicated that atomoxetine improved ADHD symptoms, but not bipolar symptoms, in children with these disorders. Atomoxetine use was not associated with any episodes of mania in these studies.47,48
Oppositional defiant disorder
Both ODD and CD rank among the more common of the comorbidities that present with ADHD, which is a significant concern since they are often associated with worsened ADHD symptoms.50,94 A total of 14 studies were found addressing the use of atomoxetine in this patient population (Table 4). Overall, atomoxetine produced significant improvements in symptoms of both ADHD and CD/ODD. In addition, a path analysis suggests that atomoxetine may have a specific effect on CD/ODD.51 Interestingly, atomoxetine appeared to have a more pronounced effect on hyperactivity in patients with comorbid ODD/CD, and it was suggested that the presence of this disorder may enhance the efficacy of atomoxetine against symptoms of ADHD.58 Atomoxetine also protected against relapse in pediatric ADHD patients with concurrent ODD.61
Depression
Overall, the studies found in this search indicated that atomoxetine was equally effective in reducing symptoms of ADHD in patients with or without comorbid depressive symptoms (Table 4). In 1 RCT with patients who had ADHD with comorbid major depressive disorder, atomoxetine improved ADHD symptoms but did not improve those of major depressive disorder.63 A second RCT showed that atomoxetine given alone or with fluoxetine improved both ADHD and depressive symptoms, but no placebo group was included.46 In an open-label study, atomoxetine improved ADHD symptoms, and symptoms of depression were improved in 55% of the patients.14 Depressive symptoms were unchanged in 34% and worsened in 11% of patients who had comorbid depression, but significance was not reported.14
Learning and language disorders
Dyslexia frequently occurs with ADHD, possibly due to common genetic influences and neuropsychological traits.64 The search revealed 2 RCTs and 2 open-label studies that examined the effect of atomoxetine in children with ADHD and a language disorder (Table 4). Overall, atomoxetine was comparable in efficacy against ADHD symptoms in patients with ADHD with or without a learning or language disorder. Importantly, correlation analyses indicated that improvement in ADHD symptoms alone did not explain the improvement in reading scores.67
Pervasive developmental disorders/ASD
The co-occurrence of pervasive developmental disorders, which include ASDs, with ADHD is estimated to range between 12% and 50%,8,20 and some studies have estimated that as many as 80% of patients with ADHD have some symptoms of pervasive developmental disorders.19 Our search returned 2 blinded, placebo-controlled RCTs, 5 open-label studies, and 1 retrospective examination of patient records addressing atomoxetine and children with ADHD and pervasive developmental disorders or ASD (Table 4). In general, atomoxetine was significantly superior to placebo in treating symptoms of ADHD in this patient population (Table 4). It should be noted that the magnitude of the effect of atomoxetine was reduced compared to studies with children with ADHD without ASD.69 However, extending the time-course of atomoxetine administration resulted in continued improvement in ADHD symptoms, suggesting that more time is needed for the full effects of atomoxetine to become established in patients with ADHD and ASD.70
Sluggish cognitive tempo
SCT is an experimental construct rather than a clinical diagnosis that is characterized by drowsiness, daydreaming, lethargy, mental confusion, and slowed thinking/behavior, and it is unclear whether SCT is the inattentive subtype of ADHD or a distinct disorder.95 A single double-blind RCT examined the effects of atomoxetine on children with ADHD, dyslexia, or both disorders with regard to SCT symptoms.64 Atomoxetine significantly improved SCT symptoms for patients with ADHD alone or ADHD and dyslexia, and also significantly improved the scores of the Parent and Teacher subscales of the Kiddie-Sluggish Cognitive Tempo (K-SCT) for those with dyslexia alone.64 While there was a positive correlation (correlation coefficient of 0.40–0.54, P<0.001, for K-SCT Parent subscale score with changes in Attention-Deficit/Hyperactivity Disorder Rating Scale-IV-Parent-Version:Investigator-Administered and Scored [ADHDRS-IV-Parent:Inv] scores; correlation coefficient of 0.33–0.61, P≤0.004, for K-SCT Teacher subscale score with changes in Attention-Deficit/Hyperactivity Disorder Rating Scale-IV-Teacher-Version scores; correlation coefficient of 0.16–0.19, P≤0.032, for K-SCT Youth subscale score with changes in ADHDRS-IV-Parent:Inv scores) between improvements in ADHD rating scale and in the K-SCT scores, it appears that changes in ADHD symptoms did not fully drive improvements in SCT.64
Sleep disorders
Children with ADHD have shorter sleep time, longer interrupted sleep time, greater difficulty waking up, and more daytime sleepiness than healthy children.96 One RCT (Table 4) showed that atomoxetine slightly shortened latency to sleep onset and children had less difficulty in falling asleep or waking up and were less irritable.76
Substance use disorders
Although SUD comorbid with ADHD is a clinical concern even in youths, our search returned only 1 RCT77 and 1 open-label prospective study14 regarding atomoxetine in this patient population (Table 4). Atomoxetine, in combination with motivational interviewing/cognitive behavioral therapy (MI/CBT), was not different from placebo and MI/CBT in improving ADHD symptoms or substance use in patients with ADHD and SUD.77 The lack of significant difference between the groups was attributed to a large effect from placebo and/or MI/CBT. In the open-label prospective study, only those patients with ADHD and SUD failed to show significant improvement of ADHD symptoms.14
Tic disorders/Tourette’s syndrome
A total of 2 RCTs and 1 prospective, observational open-label study were found to address the activity of atomoxetine on child patients with ADHD and tic disorders, including Tourette syndrome (Table 4). One RCT showed that atomoxetine was associated with a significant improvement in ADHD symptoms, and some evidence suggests a reduction in tic severity.78 A subgroup analysis of patients with comorbid Tourette syndrome from this study showed similar results.79 In the open-label study, atomoxetine use was associated with reported improvement in the tic disorder in 65% of the patients, and no change in the remainder (ie, no patients reported a worsening of tic disorder).14
Effects of atomoxetine in adults with ADHD and anxiety
Anxiety
We found 4 RCTs, an open-label study, and a post hoc correlation analysis of an RCT when searching for atomoxetine with ADHD and anxiety in adults (Table 5). Of these 6 reports, 3 RCTs addressed social anxiety disorder (SAD),80–82 1 RCT addressed generalized social anxiety disorder (GSAD),83 and 2 addressed generalized anxiety disorder (GAD).84 In these reports, atomoxetine improved symptoms of ADHD in individuals with the disorder with or without either of the comorbid anxiety disorders. In addition, atomoxetine reduced symptoms of anxiety in patients with ADHD and with SAD, GSAD, or GAD (Table 5). Response rates or changes in severity of ADHD symptoms were also significantly greater in patients with ADHD compared to those with ADHD and SAD,80 which is consistent with reports that anxiety in general is often associated with a greater severity of ADHD symptoms.97 Importantly, atomoxetine produced improvements or no change in anxiety scores of patients with ADHD but with no diagnosis of anxiety disorders.85
Depression
Although depression with ADHD is a common occurrence,9,28 we found only 2 RCTs on atomoxetine in adults with ADHD and depression (Table 5). In both studies, atomoxetine significantly improved ADHD symptoms, but did not produce changes in assessments of depression.85,86
Substance use disorders
The presence of SUD in patients with ADHD is an important clinical concern, occurring up to 4 times the incidence observed in individuals without ADHD.98 This search yielded 2 RCTs, a post hoc subgroup analysis of 1 of the RCTs, 2 open-label studies, and a retrospective study with a naturalistic follow-up (Table 5). Atomoxetine significantly improved ADHD symptoms in individuals with ADHD in each of these studies. However, results with substance abuse were mixed. Atomoxetine significantly reduced cumulative days of heavy drinking, but did not reduce the latency to relapse of heavy drinking.87 A subgroup analysis from this study found a significant correlation between improvements in ADHD symptoms and reductions in cravings for alcohol in atomoxetine-treated patients and not in the placebo group, and those that relapsed showed worsening of ADHD symptoms.88 In contrast, both atomoxetine and placebo did not change cannabis use in an RCT of patients with ADHD who were also using cannabis.92
An open-label study of adult patients with ADHD and cocaine use showed that atomoxetine significantly improved ADHD symptoms, but did not change cocaine use.91 A later open-label study with adult patients with ADHD and poly-substance use (cocaine, cannabis, alcohol, and opioids were the primary abused substances) reported that atomoxetine treatment decreased intensity, frequency, and length of cravings based on the Brief. Substance Craving Scale, each of these dimensions of craving was scored from 0 to 4.90
However, atomoxetine did not reduce the number of times that participants thought that they had a craving within the past 24 hours.90 A retrospective study of patients with SUD, with (72%) or without (28%) ADHD, receiving atomoxetine plus treatment-as-usual (TAU) reported a significant reduction in measures of nicotine use when compared to the TAU-alone group.89 However, results were presented for the entire group, and not separated by presence or absence of ADHD.89
Discussion
The 50 studies included in this review suggest that atomoxetine is as effective in treating ADHD symptoms in both child and adult patients with ADHD with comorbid psychiatric conditions as those with ADHD without comorbidities. Although ADHD in children has been described for over a century, the same condition in adults has not received serious attention until the 1990s.9 It is therefore not surprising that we found 37 studies referencing young patients compared to 13 for adult patients for this review.
Anxiety, depression, mania, and tics have been reported as adverse events in patients taking atomoxetine.37,38 However, the atomoxetine product label also states that clinical trials have reported that atomoxetine improves symptoms of ADHD in patients with comorbid anxiety and tic disorders, without worsening these comorbid symptoms.37,38 In the studies reviewed, atomoxetine improved various ADHD symptoms in cohorts with and without comorbidities. This observation is supported by a recent systematic review of 24 studies (RCTs and within-subject designs) that concluded that the presence of a comorbidity did not lessen the efficacy of atomoxetine in treating ADHD symptoms.99 Importantly, this systematic review did not make clear that in both adults and children, the efficacy of atomoxetine is similar to stimulants and hence atomoxetine has an important role in ADHD treatment for many patients with and without comorbid disorders.43,44
In the studies reviewed, there is no evidence of worsening of any of the comorbidities examined, and in some cases, there is significant improvement. It is important however to differentiate usage of atomoxetine when a comorbidity is present from usage in that comorbid condition alone. Atomoxetine does not improve symptoms of anxiety in patients with anxiety disorders but without ADHD. For example, a placebo-controlled RCT showed that atomoxetine was no different from placebo in improving anxiety scores in patients with GSAD.83 A post hoc correlation analysis of an RCT of ADHD patients with SAD who were treated with atomoxetine revealed that improvements in anxiety were directly correlated with improvements in symptoms of ADHD.100 Moreover, atomoxetine did not exacerbate comorbid anxiety.100 It is therefore likely that when improvements in anxiety symptoms are seen, it is probably related to improvement of ADHD symptoms.
Depression is an important clinical concern in patients with ADHD, as it occurs at a 5-fold greater incidence in these patients than in the population at large.101 A link between depression and ADHD is suggested by imaging studies that show that these 2 disorders share common brain regions and neural pathways.102 In comorbid patients treated with atomoxetine, it is likely that reported improvements in depressive symptoms result from an improvement in ADHD, and not from a direct antidepressant effect of atomoxetine. This interpretation is consistent with the RCTs that showed that atomoxetine does not act as an antidepressant.103–106 The studies in which depression was comorbid with ADHD showed that the presence of depressive symptoms did not adversely impact the efficacy of atomoxetine against ADHD.
Although tics are listed as a possible adverse event with atomoxetine, several treatment guidelines indicate that atomoxetine is preferred over the stimulants for patients with ADHD and comorbid tic disorders. The European ADHD Guidelines Group concluded that the stimulants could worsen comorbid tics, whereas atomoxetine significantly improves them.107 The National Institute for Health and Care Excellence (NICE) suggests atomoxetine or methylphenidate when tic disorders or Tourette syndrome is present.108
Both child and adult patients with ADHD are at a higher risk of SUD.29,109,110 There is an approximately 4-fold greater incidence of SUD in adult ADHD patients compared to individuals without ADHD.98 Despite variable evidence for the role of stimulants in the management of SUD among patients with ADHD, there exists a clinical concern regarding the use of the psychostimulants in patients with SUD, since these drugs show some abuse liability.98,110 In contrast, atomoxetine has no abuse liability,111 and thus often will be a first-choice treatment in patients with concern for SUD.111 Treatment guidelines suggest the use of atomoxetine or of extended-release formulations of methylphenidate in this population to reduce abuse liability.107,112,113
Although atomoxetine may be preferable over other treatments for ADHD in the presence of certain psychiatric comorbidities described, there remains reluctance among some clinicians to administer atomoxetine first because of perceptions that it may be less effective. However, a recent systematic review and a network meta-analysis have shown similar efficacy for responders.43,44 Many RCTs specifically exclude patients with specific comorbid disorders such as major depressive disorder and anxiety. Our search found clinical studies addressing only 3 comorbid disorders in adults: anxiety, depression, and SUD. There are more studies performed with children, but no data were found with regard to antisocial personality disorder, binge eating disorders, or obsessive compulsive disorder. While it is known that adults with ADHD have irregular sleep–wake cycles and disrupted sleep patterns, we found no studies addressing the effect of atomoxetine on sleep in adults with ADHD, and only 1 study on children with ADHD. Overall, although there is an association of binge eating disorder with ADHD,114 there is currently a dearth of evidence as to its incidence, and little guidance on appropriate therapy. There is an appreciable level of comorbidity of bipolar disorder with ADHD. Estimates of comorbid bipolar disorder range up to 22% of children with ADHD,16 and as high as 47% in adults.27 In spite of these estimates, there are few studies on the treatment of individuals with ADHD and bipolar disorder.115 Care should be taken in treating ADHD patients with comorbid bipolar disorder because of concern for possible induction of a mixed/manic episode.37 This cumulative review and analysis of studies of atomoxetine in patients with common comorbidities should help improve current treatment guidelines for ADHD.
Limitations
An important limitation of this review is that the activity of atomoxetine in ADHD with some comorbid disorders is not well examined. Whereas some of these conditions are subjected to rigorous placebo-controlled, double-blind RCTs, some, such as ODD, are lacking in such studies because individuals with these comorbidities are often excluded from ADHD clinical trials. Also, there are only a few head-to-head comparisons of atomoxetine vs methylphenidate or the other psychostimulants in ADHD patients with common comorbidities. A limitation of this analysis is that it is not a systematic review.
Summary and conclusion
Overall, atomoxetine shows good efficacy in improving symptoms of ADHD in children and adults. Based on the studies reported in the present review, the presence of comorbid psychiatric disorders does not appear to alter the efficacy of atomoxetine in treating ADHD. Moreover, atomoxetine may be preferable to psychostimulants in the treatment of ADHD in the presence of psychiatric disorders contraindicated for stimulants, while providing similar levels of efficacy and tolerability.
Acknowledgments
Angela Lorio and Meghana Kuntla of inVentiv Health Clinical, LLC, provided editorial assistance. Eli Lilly and Company contracted inVentiv Health Clinical, LLC, for writing and editorial services.
Disclosure
This work was sponsored and funded by Eli Lilly and Company, Indianapolis, IN, USA, and/or any of its subsidiaries. David Clemow and Himanshu Upadhyaya are employed by Eli Lilly and Company, Michele Mancini is employed by Eli Lilly Italia S.p.A, Chris Bushe is employed by Eli Lilly, UK, and Michael Ossipov is employed by inVentiv Health Clinical, LLC.
References
Moffitt TE, Houts R, Asherson P, et al. Is adult ADHD a childhood-onset neurodevelopmental disorder? Evidence from a four-decade longitudinal cohort study. Am J Psychiatry. 2015;172(10):967–977. | ||
Willcutt EG. The prevalence of DSM-IV attention-deficit/hyperactivity disorder: a meta-analytic review. Neurotherapeutics. 2012;9(3):490–499. | ||
Dopheide JA, Pliszka SR. Attention-deficit-hyperactivity disorder: an update. Pharmacotherapy. 2009;29(6):656–679. | ||
Brod M, Pohlman B, Lasser R, Hodgkins P. Comparison of the burden of illness for adults with ADHD across seven countries: a qualitative study. Health Qual Life Outcomes. 2012;10:47. | ||
Faraone SV, Biederman J, Mick E. The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol Med. 2006;36(2):159–165. | ||
Adler LA, Spencer T, Brown TE, et al. Once-daily atomoxetine for adult attention-deficit/hyperactivity disorder: a 6-month, double-blind trial. J Clin Psychopharmacol. 2009;29(1):44–50. | ||
Upadhyaya H, Adler LA, Casas M, et al. Baseline characteristics of European and non-European adult patients with attention deficit hyperactivity disorder participating in a placebo-controlled, randomized treatment study with atomoxetine. Child Adolesc Psychiatry Ment Health. 2013;7(1):14. | ||
Jensen CM, Steinhausen HC. Comorbid mental disorders in children and adolescents with attention-deficit/hyperactivity disorder in a large nationwide study. Atten Defic Hyperact Disord. 2015;7(1):27–38. | ||
Kessler RC, Adler L, Barkley R, et al. The prevalence and correlates of adult ADHD in the United States: results from the National Comorbidity Survey Replication. Am J Psychiatry. 2006;163(4):716–723. | ||
Larson K, Russ SA, Kahn RS, Halfon N. Patterns of comorbidity, functioning, and service use for US children with ADHD, 2007. Pediatrics. 2011;127(3):462–470. | ||
Newcorn JH, Weiss M, Stein MA. The complexity of ADHD: diagnosis and treatment of the adult patient with comorbidities. CNS Spectr. 2007;12(8 Suppl 12):1–14. | ||
Geller D, Donnelly C, Lopez F, et al. Atomoxetine treatment for pediatric patients with attention-deficit/hyperactivity disorder with comorbid anxiety disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(9): 1119–1127. | ||
Sciberras E, Lycett K, Efron D, Mensah F, Gerner B, Hiscock H. Anxiety in children with attention-deficit/hyperactivity disorder. Pediatrics. 2014;133(5):801–808. | ||
Bakken RJ, Paczkowski M, Kramer HP, et al. Effects of atomoxetine on attention-deficit/hyperactivity disorder in clinical pediatric treatment settings: a naturalistic study. Curr Med Res Opin. 2008;24(2):449–460. | ||
Reinblatt SP, Leoutsakos JM, Mahone EM, Forrester S, Wilcox HC, Riddle MA. Association between binge eating and attention-deficit/hyperactivity disorder in two pediatric community mental health clinics. Int J Eat Disord. 2015;48(5):505–511. | ||
Taurines R, Schmitt J, Renner T, Conner AC, Warnke A, Romanos M. Developmental comorbidity in attention-deficit/hyperactivity disorder. Atten Defic Hyperact Disord. 2010;2(4):267–289. | ||
Singh MK, DelBello MP, Kowatch RA, Strakowski SM. Co-occurrence of bipolar and attention-deficit hyperactivity disorders in children. Bipolar Disord. 2006;8(6):710–720. | ||
Biederman J, Spencer TJ, Newcorn JH, et al. Effect of comorbid symptoms of oppositional defiant disorder on responses to atomoxetine in children with ADHD: a meta-analysis of controlled clinical trial data. Psychopharmacology (Berl). 2007;190(1):31–41. | ||
Gillberg C, Gillberg IC, Rasmussen P, et al. Co-existing disorders in ADHD – implications for diagnosis and intervention. Eur Child Adolesc Psychiatry. 2004;13 Suppl 1:I80–I92. | ||
Reichow B, Volkmar FR, Bloch MH. Systematic review and meta-analysis of pharmacological treatment of the symptoms of attention-deficit/hyperactivity disorder in children with pervasive developmental disorders. J Autism Dev Disord. 2013;43(10):2435–2441. | ||
Kollins SH. ADHD, substance use disorders, and psychostimulant treatment: current literature and treatment guidelines. J Atten Disord. 2008;12(2):115–125. | ||
McGough JJ, Smalley SL, McCracken JT, et al. Psychiatric comorbidity in adult attention deficit hyperactivity disorder: findings from multiplex families. Am J Psychiatry. 2005;162(9):1621–1627. | ||
Biederman J. Attention-deficit/hyperactivity disorder: a life-span perspective. J Clin Psychiatry. 1998;59 Suppl 7:4–16. | ||
Ramos-Quiroga JA, Nasillo V, Fernández-Aranda F, Casas M. Addressing the lack of studies in attention-deficit/hyperactivity disorder in adults. Expert Rev Neurother. 2014;14(5):553–567. | ||
Wilens TE, Morrison NR, Prince J. An update on the pharmacotherapy of attention-deficit/hyperactivity disorder in adults. Expert Rev Neurother. 2011;11(10):1443–1465. | ||
Perugi G, Vannucchi G. The use of stimulants and atomoxetine in adults with comorbid ADHD and bipolar disorder. Expert Opin Pharmacother. 2015;16(14):2193–2204. | ||
Wingo AP, Ghaemi SN. A systematic review of rates and diagnostic validity of comorbid adult attention-deficit/hyperactivity disorder and bipolar disorder. J Clin Psychiatry. 2007;68(11):1776–1784. | ||
Kolar D, Keller A, Golfinopoulos M, Cumyn L, Syer C, Hechtman L. Treatment of adults with attention-deficit/hyperactivity disorder. Neuropsychiatr Dis Treat. 2008;4(2):389–403. | ||
Biederman J. Attention-deficit/hyperactivity disorder: a selective overview. Biol Psychiatry. 2005;57(11):1215–1220. | ||
Adderall® (dextroamphetamine saccharate, amphetamine aspartate, dextroamphetamine sulfate and amphetamine sulfate tablets) [prescribing information]. Horsham, PA: Teva Pharmaceuticals USA; 2015. | ||
Ritalin® (methylphenidate hydrochloride tablets) [prescribing information]. Gainesville, GA: Novartis Pharmaceuticals Corporation; 2007. | ||
Ritalin® (methylphenidate hydrochloride tablets) [summary of product characteristics]. Surrey: Novartis Pharmaceuticals UK Ltd; 2015. | ||
Felt BT, Biermann B, Christner JG, Kochhar P, Harrison RV. Diagnosis and management of ADHD in children. Am Fam Physician. 2014;90(7):456–464. | ||
Coughlin CG, Cohen SC, Mulqueen JM, Ferracioli-Oda E, Stuckelman ZD, Bloch MH. Meta-analysis: reduced risk of anxiety with psychostimulant treatment in children with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. 2015;25(8):611–617. | ||
Bangs ME, Tauscher-Wisniewski S, Polzer J, et al. Meta-analysis of suicide-related behavior events in patients treated with atomoxetine. J Am Acad Child Adolesc Psychiatry. 2008;47(2):209–218. | ||
Garnock-Jones KP, Keating GM. Atomoxetine: a review of its use in attention-deficit hyperactivity disorder in children and adolescents. Paediatr Drugs. 2009;11(3):203–226. | ||
Strattera® (atomoxetine capsules) [strattera prescribing information]. Indianapolis, IN: Eli Lilly and Company; 2009. | ||
Strattera® (atomoxetine capsules) [strattera summary of product characteristics]. Hampshire: Eli Lilly and Company Ltd.; 2015. | ||
Wilens TE. Impact of ADHD and its treatment on substance abuse in adults. J Clin Psychiatry. 2004;65 Suppl 3:38–45. | ||
Bolea-Alamañac B, Nutt DJ, Adamou M, et al; British Association for Psychopharmacology. Evidence-based guidelines for the pharmacological management of attention deficit hyperactivity disorder: update on recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2014;28(3):179–203. | ||
Canadian Attention Deficit Hyperactivity Disorder Resource Alliance (CADDRA). Pharmacological treatment of ADHD. In: Canadian ADHD Practice Guidelines. 3rd ed. Toronto, ON: CADDRA; 2014. | ||
Weiss MD, Weiss JR. A guide to the treatment of adults with ADHD. J Clin Psychiatry. 2004;65 Suppl 3:27–37. | ||
Bushe C, Day K, Reed V, et al. A network meta-analysis of atomoxetine and osmotic release oral system methylphenidate in the treatment of attention-deficit/hyperactivity disorder in adult patients. J Psychopharmacol. 2016;30(5):444–458. | ||
Bushe CJ, Savill NC. Systematic review of atomoxetine data in childhood and adolescent attention-deficit hyperactivity disorder 2009–2011: focus on clinical efficacy and safety. J Psychopharmacol. 2014;28(3):204–211. | ||
Clemow DB, Bushe CJ. Atomoxetine in patients with ADHD: a clinical and pharmacological review of the onset, trajectory, duration of response and implications for patients. J Psychopharmacol. 2015;29(12):1221–1230. | ||
Kratochvil CJ, Newcorn JH, Arnold LE, et al. Atomoxetine alone or combined with fluoxetine for treating ADHD with comorbid depressive or anxiety symptoms. J Am Acad Child Adolesc Psychiatry. 2005;44(9):915–924. | ||
Chang K, Nayar D, Howe M, Rana M. Atomoxetine as an adjunct therapy in the treatment of co-morbid attention-deficit/hyperactivity disorder in children and adolescents with bipolar I or II disorder. J Child Adolesc Psychopharmacol. 2009;19(5):547–551. | ||
Hah M, Chang K. Atomoxetine for the treatment of attention-deficit/hyperactivity disorder in children and adolescents with bipolar disorders. J Child Adolesc Psychopharmacol. 2005;15(6):996–1004. | ||
Newcorn JH, Spencer TJ, Biederman J, Milton DR, Michelson D. Atomoxetine treatment in children and adolescents with attention-deficit/hyperactivity disorder and comorbid oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry. 2005;44(3):240–248. | ||
Bangs ME, Hazell P, Danckaerts M, et al; Atomoxetine ADHD/ODD Study Group. Atomoxetine for the treatment of attention-deficit/hyperactivity disorder and oppositional defiant disorder. Pediatrics. 2008;121(2):e314–e320. | ||
Dittmann RW, Schacht A, Helsberg K, et al. Atomoxetine versus placebo in children and adolescents with attention-deficit/hyperactivity disorder and comorbid oppositional defiant disorder: a double-blind, randomized, multicenter trial in Germany. J Child Adolesc Psychopharmacol. 2011;21(2):97–110. | ||
Dell’Agnello G, Maschietto D, Bravaccio C, et al; LYCY Study Group. Atomoxetine hydrochloride in the treatment of children and adolescents with attention-deficit/hyperactivity disorder and comorbid oppositional defiant disorder: a placebo-controlled Italian study. Eur Neuropsychopharmacol. 2009;19(11):822–834. | ||
Garg J, Arun P, Chavan BS. Comparative efficacy of methylphenidate and atomoxetine in oppositional defiant disorder comorbid with attention deficit hyperactivity disorder. Int J Appl Basic Med Res. 2015;5(2):114–118. | ||
Cheng JY, Chen RY, Ko JS, Ng EM. Efficacy and safety of atomoxetine for attention-deficit/hyperactivity disorder in children and adolescents-meta-analysis and meta-regression analysis. Psychopharmacology (Berl). 2007;194(2):197–209. | ||
Wehmeier PM, Schacht A, Dittmann RW, et al. Effect of atomoxetine on quality of life and family burden: results from a randomized, placebo-controlled, double-blind study in children and adolescents with ADHD and comorbid oppositional defiant or conduct disorder. Qual Life Res. 2011;20(5):691–702. | ||
Waxmonsky JG, Waschbusch DA, Akinnusi O, Pelham WE. A comparison of atomoxetine administered as once versus twice daily dosing on the school and home functioning of children with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. 2011;21(1):21–32. | ||
van Wyk GW, Hazell PL, Kohn MR, Granger RE, Walton RJ. How oppositionality, inattention, and hyperactivity affect response to atomoxetine versus methylphenidate: a pooled meta-analysis. J Atten Disord. 2012;16(4):314–324. | ||
Wehmeier PM, Kipp L, Banaschewski T, Dittmann RW, Schacht A. Does comorbid disruptive behavior modify the effects of atomoxetine on ADHD symptoms as measured by a continuous performance test and a motion tracking device? J Atten Disord. 2015;19(7):591–602. | ||
Ercan ES, Akyol Ardic U, Kabukcu Basay B, Ercan E, Basay O. Atomoxetine response in the inattentive and combined subtypes of attention deficit hyperactivity disorder: a retrospective chart review. Atten Defic Hyperact Disord. 2013;5(4):377–385. | ||
Kaplan S, Heiligenstein J, West S, et al. Efficacy and safety of atomoxetine in childhood attention-deficit/hyperactivity disorder with comorbid oppositional defiant disorder. J Atten Disord. 2004;8(2):45–52. | ||
Hazell P, Zhang S, Wolanczyk T, et al. Comorbid oppositional defiant disorder and the risk of relapse during 9 months of atomoxetine treatment for attention-deficit/hyperactivity disorder. Eur Child Adolesc Psychiatry. 2006;15(2):105–110. | ||
Scott NG, Ripperger-Suhler J, Rajab MH, Kjar D. Factors associated with atomoxetine efficacy for treatment of attention-deficit/hyperactivity disorder in children and adolescents. J Child Adolesc Psychopharmacol. 2010;20(3):197–203. | ||
Bangs ME, Emslie GJ, Spencer TJ, et al; Atomoxetine ADHD and Comorbid MDD Study Group. Efficacy and safety of atomoxetine in adolescents with attention-deficit/hyperactivity disorder and major depression. J Child Adolesc Psychopharmacol. 2007;17(4):407–420. | ||
Wietecha L, Williams D, Shaywitz S, et al. Atomoxetine improved attention in children and adolescents with attention-deficit/hyperactivity disorder and dyslexia in a 16 week, acute, randomized, double-blind trial. J Child Adolesc Psychopharmacol. 2013;23(9):605–613. | ||
de Jong CG, Van De Voorde S, Roeyers H, et al. Differential effects of atomoxetine on executive functioning and lexical decision in attention-deficit/hyperactivity disorder and reading disorder. J Child Adolesc Psychopharmacol. 2009;19(6):699–707. | ||
Sumner CR, Gathercole S, Greenbaum M, et al. Atomoxetine for the treatment of attention-deficit/hyperactivity disorder (ADHD) in children with ADHD and dyslexia. Child Adolesc Psychiatry Ment Health. 2009;3:40. | ||
Shaywitz BA, Williams DW, Fox BK, Wietecha LA. Reading outcomes of children and adolescents with attention-deficit/hyperactivity disorder and dyslexia following atomoxetine treatment. J Child Adolesc Psychopharmacol. 2014;24(8):419–425. | ||
Arnold LE, Aman MG, Cook AM, et al. Atomoxetine for hyperactivity in autism spectrum disorders: placebo-controlled crossover pilot trial. J Am Acad Child Adolesc Psychiatry. 2006;45(10):1196–1205. | ||
Harfterkamp M, van de Loo-Neus G, Minderaa RB, et al. A randomized double-blind study of atomoxetine versus placebo for attention-deficit/hyperactivity disorder symptoms in children with autism spectrum disorder. J Am Acad Child Adolesc Psychiatry. 2012;51(7):733–741. | ||
Harfterkamp M, Buitelaar JK, Minderaa RB, van de Loo-Neus G, van der Gaag RJ, Hoekstra PJ. Long-term treatment with atomoxetine for attention-deficit/hyperactivity disorder symptoms in children and adolescents with autism spectrum disorder: an open-label extension study. J Child Adolesc Psychopharmacol. 2013;23(3):194–199. | ||
Troost PW, Steenhuis MP, Tuynman-Qua HG, et al. Atomoxetine for attention-deficit/hyperactivity disorder symptoms in children with pervasive developmental disorders: a pilot study. J Child Adolesc Psychopharmacol. 2006;16(5):611–619. | ||
Fernández-Jaén A, Fernández-Mayoralas DM, Calleja-Pérez B, Muñoz-Jareño N, Campos Díaz MR, López-Arribas S. Efficacy of atomoxetine for the treatment of ADHD symptoms in patients with pervasive developmental disorders: a prospective, open-label study. J Atten Disord. 2013;17(6):497–505. | ||
Jou RJ, Handen BL, Hardan AY. Retrospective assessment of atomoxetine in children and adolescents with pervasive developmental disorders. J Child Adolesc Psychopharmacol. 2005;15(2):325–330. | ||
Posey DJ, Wiegand RE, Wilkerson J, Maynard M, Stigler KA, McDougle CJ. Open-label atomoxetine for attention-deficit/hyperactivity disorder symptoms associated with high-functioning pervasive developmental disorders. J Child Adolesc Psychopharmacol. 2006;16(5):599–610. | ||
Charnsil C. Efficacy of atomoxetine in children with severe autistic disorders and symptoms of ADHD: an open-label study. J Atten Disord. 2011;15(8):684–689. | ||
Sangal RB, Owens J, Allen AJ, Sutton V, Schuh K, Kelsey D. Effects of atomoxetine and methylphenidate on sleep in children with ADHD. Sleep. 2006;29(12):1573–1585. | ||
Thurstone C, Riggs PD, Salomonsen-Sautel S, Mikulich-Gilbertson SK. Randomized, controlled trial of atomoxetine for attention-deficit/hyperactivity disorder in adolescents with substance use disorder. J Am Acad Child Adolesc Psychiatry. 2010;49(6):573–582. | ||
Allen AJ, Kurlan RM, Gilbert DL, et al. Atomoxetine treatment in children and adolescents with ADHD and comorbid tic disorders. Neurology. 2005;65(12):1941–1949. | ||
Spencer TJ, Sallee FR, Gilbert DL, et al. Atomoxetine treatment of ADHD in children with comorbid Tourette syndrome. J Atten Disord. 2008;11(4):470–481. | ||
Adler LA, Rubin R, Qiao M, Heinloth AN, Durell TM. Patient characteristics and treatment response to atomoxetine in adults with ADHD versus ADHD comorbid with social anxiety disorder. J ADHD Relat Disord. 2010;1(3):5–15. | ||
Adler LA, Liebowitz M, Kronenberger W, et al. Atomoxetine treatment in adults with attention-deficit/hyperactivity disorder and comorbid social anxiety disorder. Depress Anxiety. 2009;26(3):212–221. | ||
Donnelly CL, Adler LA, Qiao M, Durell TM. Anxiety response to atomoxetine in patients with attention-deficit/hyperactivity disorder and comorbid anxiety. Poster presented at: 23rd Annual U.S. Psychiatric and Mental Health Congress (USPMHC); November 18, 2010; Orlando, FL. | ||
Ravindran LN, Kim DS, Letamendi AM, Stein MB. A randomized controlled trial of atomoxetine in generalized social anxiety disorder. J Clin Psychopharmacol. 2009;29(6):561–564. | ||
Gabriel A, Violato C. Adjunctive atomoxetine to SSRIs or SNRIs in the treatment of adult ADHD patients with comorbid partially responsive generalized anxiety (GA): an open-label study. Atten Defic Hyperact Disord. 2011;3(4):319–326. | ||
Young JL, Sarkis E, Qiao M, Wietecha L. Once-daily treatment with atomoxetine in adults with attention-deficit/hyperactivity disorder: a 24-week, randomized, double-blind, placebo-controlled trial. Clin Neuropharmacol. 2011;34(2):51–60. | ||
Durell TM, Adler LA, Williams DW, et al. Atomoxetine treatment of attention-deficit/hyperactivity disorder in young adults with assessment of functional outcomes: a randomized, double-blind, placebo-controlled clinical trial. J Clin Psychopharmacol. 2013;33(1):45–54. | ||
Wilens TE, Adler LA, Weiss MD, et al; Atomoxetine ADHD/SUD Study Group. Atomoxetine treatment of adults with ADHD and comorbid alcohol use disorders. Drug Alcohol Depend. 2008;96(1–2):145–154. | ||
Wilens TE, Adler LA, Tanaka Y, et al. Correlates of alcohol use in adults with ADHD and comorbid alcohol use disorders: exploratory analysis of a placebo-controlled trial of atomoxetine. Curr Med Res Opin. 2011;27(12):2309–2320. | ||
Benegal V, Viswanath B, Narayanaswamy JC, et al. The efficacy of atomoxetine as adjunctive treatment for co-morbid substance use disorders and externalizing symptoms. Asian J Psychiatry. 2013;6(6):544–547. | ||
Adler LA, Guida F, Irons S, Shaw DM. Open label pilot study of atomoxetine in adults with ADHD and substance use disorder. J Dual Diagn. 2010;6(3–4):196–207. | ||
Levin FR, Mariani JJ, Secora A, et al. Atomoxetine treatment for cocaine abuse and adult attention-deficit hyperactivity disorder (ADHD): a preliminary open trial. J Dual Diagn. 2009;5(1):41–56. | ||
McRae-Clark AL, Carter RE, Killeen TK, Carpenter MJ, White KG, Brady KT. A placebo-controlled trial of atomoxetine in marijuana-dependent individuals with attention deficit hyperactivity disorder. Am J Addict. 2010;19(6):481–489. | ||
Liu X, Kubilis P, Xu D, Bussing R, Winterstein AG. Psychotropic drug utilization in children with concurrent attention-deficit/hyperactivity disorder and anxiety. J Anxiety Disord. 2014;28(6):530–536. | ||
Kuhne M, Schachar R, Tannock R. Impact of comorbid oppositional or conduct problems on attention-deficit hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 1997;36(12):1715–1725. | ||
Becker SP, Marshall SA, McBurnett K. Sluggish cognitive tempo in abnormal child psychology: an historical overview and introduction to the special section. J Abnorm Child Psychol. 2014;42(1):1–6. | ||
Owens J, Sangal RB, Sutton VK, Bakken R, Allen AJ, Kelsey D. Subjective and objective measures of sleep in children with attention-deficit/hyperactivity disorder. Sleep Med. 2009;10(4):446–456. | ||
Tsang TW, Kohn MR, Efron D, et al. Anxiety in young people with ADHD: clinical and self-report outcomes. J Atten Disord. 2015;19(1):18–26. | ||
Clemow DB, Walker DJ. The potential for misuse and abuse of medications in ADHD: a review. Postgrad Med. 2014;126(5):64–81. | ||
Hutchison SL, Ghuman JK, Ghuman HS, Karpov I, Schuster JM. Efficacy of atomoxetine in the treatment of attention-deficit hyperactivity disorder in patients with common comorbidities in children, adolescents and adults: a review. Ther Adv Psychopharmacol. 2016;6(5):317–334. | ||
Walker DJ, Mason O, Clemow DB, Day KA. Atomoxetine treatment in adults with attention-deficit/hyperactivity disorder. Postgrad Med. 2015;127(7):686–701. | ||
Jerrell JM, McIntyre RS, Park YM. Risk factors for incident major depressive disorder in children and adolescents with attention-deficit/hyperactivity disorder. Eur Child Adolesc Psychiatry. 2015;24(1):65–73. | ||
McIntyre RS, Kennedy SH, Soczynska JK, et al. Attention-deficit/hyperactivity disorder in adults with bipolar disorder or major depressive disorder: results from the international mood disorders collaborative project. Prim Care Companion J Clin Psychiatry. 2010;12(3):e1–e7. | ||
Dell’Osso B, Palazzo MC, Oldani L, Altamura AC. The noradrenergic action in antidepressant treatments: pharmacological and clinical aspects. CNS Neurosci Ther. 2011;17(6):723–732. | ||
Chouinard G, Annable L, Bradwejn J. An early phase II clinical trial of tomoxetine (LY139603) in the treatment of newly admitted depressed patients. Psychopharmacology (Berl). 1984;83(1):126–128. | ||
Blier P. Psychopharmacology for the Clinician Psychopharmacologie pratique. J Psychiatry Neurosci. 2006;31(4):288. | ||
Michelson D, Adler LA, Amsterdam JD, et al. Addition of atomoxetine for depression incompletely responsive to sertraline: a randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2007;68(4):582–587. | ||
Cortese S, Holtmann M, Banaschewski T, et al; European ADHD Guidelines Group. Practitioner review: current best practice in the management of adverse events during treatment with ADHD medications in children and adolescents. J Child Psychol Psychiatry. 2013;54(3):227–246. | ||
National Institute for Health and Care Excellence. Clinical guideline 72: attention deficit hyperactivity disorder: diagnosis and management of ADHD in children, young people and adults. 2013. | ||
Katusic SK, Barbaresi WJ, Colligan RC, Weaver AL, Leibson CL, Jacobsen SJ. Psychostimulant treatment and risk for substance abuse among young adults with a history of attention-deficit/hyperactivity disorder: a population-based, birth cohort study. J Child Adolesc Psychopharmacol. 2005;15(5):764–776. | ||
Kollins SH. A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders. Curr Med Res Opin. 2008;24(5):1345–1357. | ||
Upadhyaya HP, Desaiah D, Schuh KJ, et al. A review of the abuse potential assessment of atomoxetine: a nonstimulant medication for attention-deficit/hyperactivity disorder. Psychopharmacology (Berl). 2013;226(2):189–200. | ||
Wolraich M, Brown L, Brown RT, et al; Subcommittee on Attention-Deficit/Hyperactivity Disorder; Steering Committee on Quality Improvement and Management. ADHD: clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics. 2011;128(5):1007–1022. | ||
Pliszka S; AACAP Work Group on Quality Issues. Practice parameter for the assessment and treatment of children and adolescents with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(7):894–921. | ||
Brewerton TD, Duncan AE. Associations between attention deficit hyperactivity disorder and eating disorders by gender: results from the national comorbidity survey replication. Eur Eat Disord Rev. 2016;24(6):536–540. | ||
Asherson P, Young AH, Eich-Höchli D, Moran P, Porsdal V, Deberdt W. Differential diagnosis, comorbidity, and treatment of attention-deficit/hyperactivity disorder in relation to bipolar disorder or borderline personality disorder in adults. Curr Med Res Opin. 2014;30(8):1657–1672. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.