Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
A Review of Research Progress on Glycemic Variability and Gestational Diabetes
Authors Yu W, Wu N ![]() , Li L, OuYang H, Qian M, Shen H
, Li L, OuYang H, Qian M, Shen H
Received 21 May 2020
Accepted for publication 11 July 2020
Published 4 August 2020 Volume 2020:13 Pages 2729—2741
DOI https://doi.org/10.2147/DMSO.S261486
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Wenshu Yu,1 Na Wu,1 Ling Li,1 Hong OuYang,1 Meichen Qian,1 Haitao Shen2
1Department of Endocrinology, Shengjing Hospital of China Medical University, Shenyang, People’ s Republic of China; 2Department of Emergency Medicine, Shengjing Hospital of China Medical University, Shenyang, People’s Republic of China
Correspondence: Na Wu
Department of Endocrinology, Shengjing Hospital of China Medical University, 36 Sanhao Road, Heping District, Shenyang, Liaoning Province 110004, People’ s Republic of China
Tel +86 18940258445
Email [email protected]
Abstract: Gestational diabetes mellitus (GDM) is associated with many adverse obstetric outcomes and neonatal outcomes, including preeclampsia, Cesarean section, and macrosomia. Active screening and early diabetes control can reduce the occurrence of adverse outcomes. Glycosylated hemoglobin (HbA1c) only reflects average blood glucose levels, but not glycemic variability (GV). Studies have shown that GV can cause a series of adverse reactions, and good control of GV can reduce the incidence of adverse pregnancy outcomes in patients with GDM. In order to provide clinicians with a better basis for diagnosis and treatment, this study reviewed the measurement, evaluation, and control of GV, the importance of GV for patients with GDM, and correlations between GV and maternal and neonatal outcomes.
Keywords: gestational diabetes mellitus, glycemic variability, outcomes, self-monitoring of blood glucose, continuous glucose monitoring
Introduction
The state of hyperglycemia during pregnancy is divided into gestational diabetes mellitus (GDM), overt diabetes mellitus (ODM) and pre-gestational diabetes mellitus (PGDM). Among these hyperglycemic variations, GDM refers to abnormal glucose metabolism in which blood glucose does not reach the level of overt diabetes during pregnancy, accounting for 80–90% of hyperglycemia during pregnancy.1 Due to the special clinical status of pregnant women, the demand for glucose increases during pregnancy, while insulin resistance increases and insulin secretion is insufficient, so some pregnant women develop GDM. At present, the diagnostic criteria for GDM varies between different guidelines (see Table 1 for details).2–8 Pregnant women with GDM may have persistent hyperglycemia after delivery, or blood glucose levels may rise again after being restored to normal. Studies have shown that about 70% of women with gestational diabetes will develop diabetes within 22–28 years after delivery,8 so patients diagnosed with GDM are advised to receive regular screening for type 2 diabetes after delivery.9
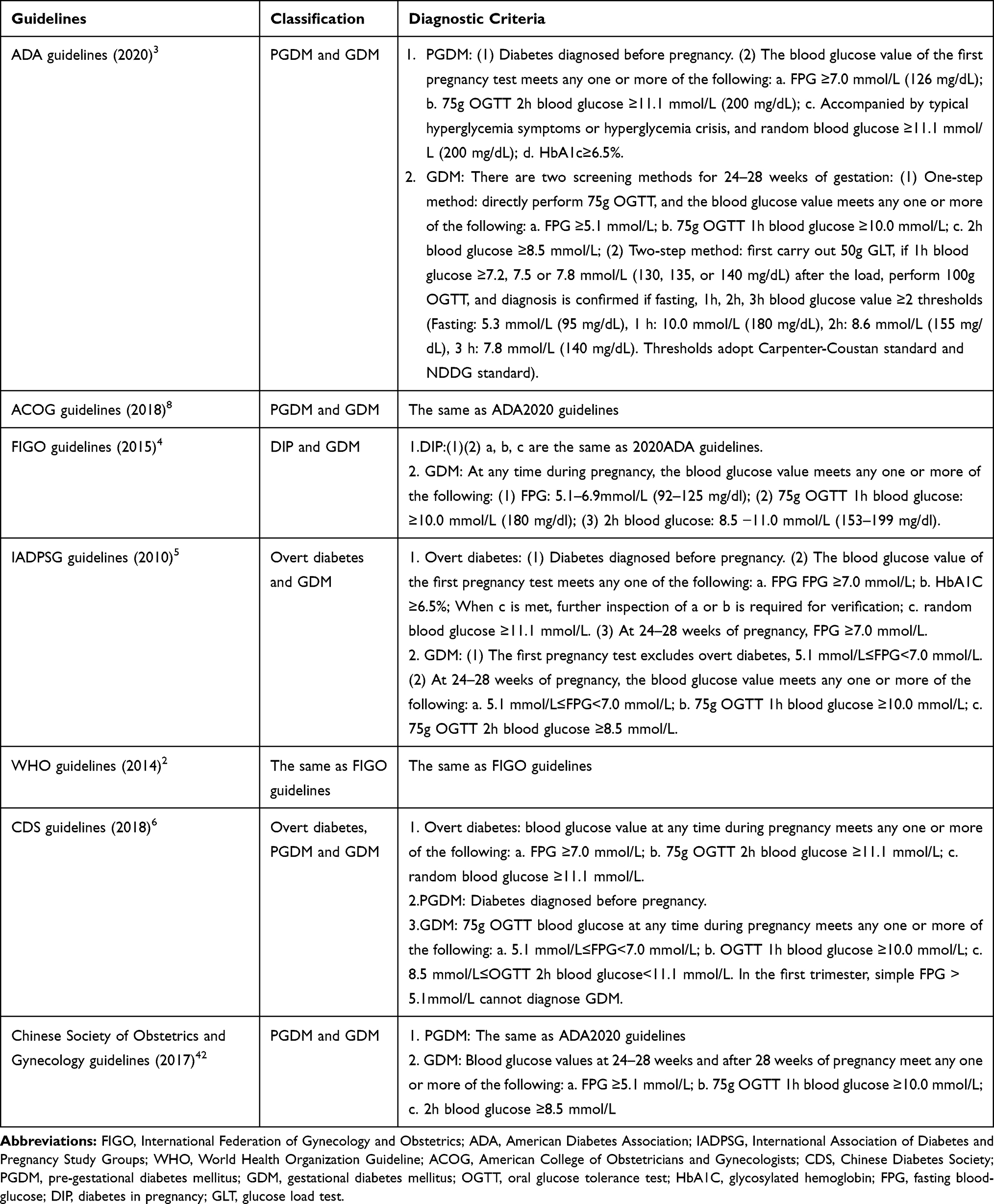 |
Table 1 Guidelines for the Classification and Diagnostic Criteria of Hyperglycemia During Pregnancy |
Because GDM is associated with many adverse obstetric and neonatal outcomes, including preeclampsia, Cesarean section, and macrosomia, active screening and early management can help to reduce the occurrence of adverse outcomes. Although glycosylated hemoglobin (HbA1c) reflects the average blood glucose level, it is not the most complete expression of blood glucose levels. For example, it does not reflect other characteristics of blood glucose control such as increasing or decreasing the risk of complications.10 It does not reflect the acute changes of blood glucose, the range of glucose changes during day and day, and it cannot reflect blood glucose variability (GV).10 Different ranges of blood glucose variability under the same HbA1c value can result in different risks of risk of diabetic microvascular complications, and the risk of adverse obstetric and neonatal outcomes is also different.11 In recent years, GV has attracted the attention of global researchers as a new concept for controlling blood glucose levels. Previous studies have reviewed the relationship between diabetes and GV, but no study has reviewed the relationship between GDM and GV.12–16 Opinions are not unified yet about whether or not the optimization of GV can reduce the occurrence of adverse obstetric and neonatal outcomes.17–21 In this regard, in order to optimize blood glucose control and avoid the occurrence of complications, we conducted a review to discuss the importance of GV in GDM and the current state of research progress on GV in GDM, and provide a basis by which clinicians can optimize blood glucose control and monitor blood glucose levels.
Importance of GV
GV manifests mainly in its unstable state between low and high blood glucose values, and is of greater risk than continuously high blood glucose status in the development of diabetic complications.22 Both postprandial hyperglycemia and fasting hyperglycemia will increase the overall blood glucose level, but in recent years, the types and efficacy of hypoglycemic drugs have increased, and it is easier to reduce hyperglycemia than before, and the probability of hypoglycemia is higher than before.14 Many studies have shown that the increase in GV will increase the risk of death. Hypoglycemia is most common among patients with elevated GV, and even if it is corrected in a timely manner in patients with severe hypoglycemia, the subsequent risk of death of patients with hypoglycemia is still twice that of patients without hypoglycemia.23 In addition, the variability of fasting blood glucose can lead to an increased risk of sudden cardiovascular disease events in diabetic patients,24 and it may also be an important risk factor for microvascular complications such as retinopathy.25 Studies suggest that sudden changes in blood glucose levels are related to oxidative stress, and oxidative stress is related to the induction of inflammatory cytokines.26 The corresponding products of oxidative stress are also relatively increased in those with large GV amplitude, and increasing evidence suggests that blood glucose variability can cause acute vascular complications.27 It is worth noting that the high concentration of blood glucose damages endothelial cells to a greater extent, and thereby increases adverse effects within the cardiovascular system.28,29 When the degree of blood glucose fluctuation exceeds a narrow range, it will increase functional impairment, especially for pregnant women with initial narrow blood glucose control ranges. Abnormal blood glucose variation during pregnancy may cause irreparable cell damage, which may affect both the mother and the developing fetus.30
Some studies have compared the blood glucose fluctuations of pregnant women with GDM and pregnant women without GDM (non-diabetic pregnancies, NDP). However, the conclusions of these studies are not consistent. Four studies have shown that the blood glucose fluctuations of pregnant women with GDM are greater than those of pregnant women with NDP.31–34 Mazze et al31 found that the GV of the GDM group was significantly higher than that of the NDP group. Similarly, Su et al32 showed that the GV of the GDM group was higher than those of the NDP group and the non-pregnant healthy control group. Dalfra et al33 found that the GV index of pregnant women with GDM was significantly higher than that of pregnant women with NDP. Nigam et al34 also showed that pregnant women with GDM had significantly higher GV index values than pregnant women with NDP. Contrary to the above-mentioned reports, Cypryk et al35 found no significant differences in blood glucose fluctuations between pregnant women with GDM and pregnant women with NDP. Those authors also found no significant differences in GV-related indicators between pregnant women with GDM and pregnant women with NDP.35 In addition to comparing the blood glucose fluctuations of women with GDM and women with NDP, Wang et al36 suggested that having GDM during one pregnancy is an influencing factor that will have an impact on blood glucose fluctuations in subsequent pregnancies. Those authors found that the GV indicators of women with NDP who had previously experienced GDM were higher than those of women with NDP who had not experienced GDM.36 This conclusion means that the impact of GDM is not limited to the current pregnancy, but will also have an impact on future pregnancies. Studies have explored the relationship between blood glucose fluctuations in pregnant women during normal pregnancies and adverse maternal and neonatal outcomes. Porter et al37 found that GV could not predict fetal birth weight, the blood glucose fluctuation was significant in women without polyhydramnios or macrosomia, and they believed that the obvious fluctuation in the blood glucose level over a relatively long period of time may have a protective effect on the mother. However, the sample size of Porter et al‘s study was small, which may be a factor contributing to the bias of the results.
Evaluation Indicators of Blood Glucose Fluctuations
Due to the widespread use of blood glucose monitoring systems, a large amount of blood glucose monitoring data requires systematic statistical analysis, and evidence shows a correlation between blood glucose fluctuations and diabetes complications. It is necessary to reduce blood glucose fluctuations to achieve blood glucose stability, which requires simple measurement and evaluation of blood glucose fluctuations. Here we summarize the discovery and development of indicators to evaluate blood glucose fluctuations (Table 2).
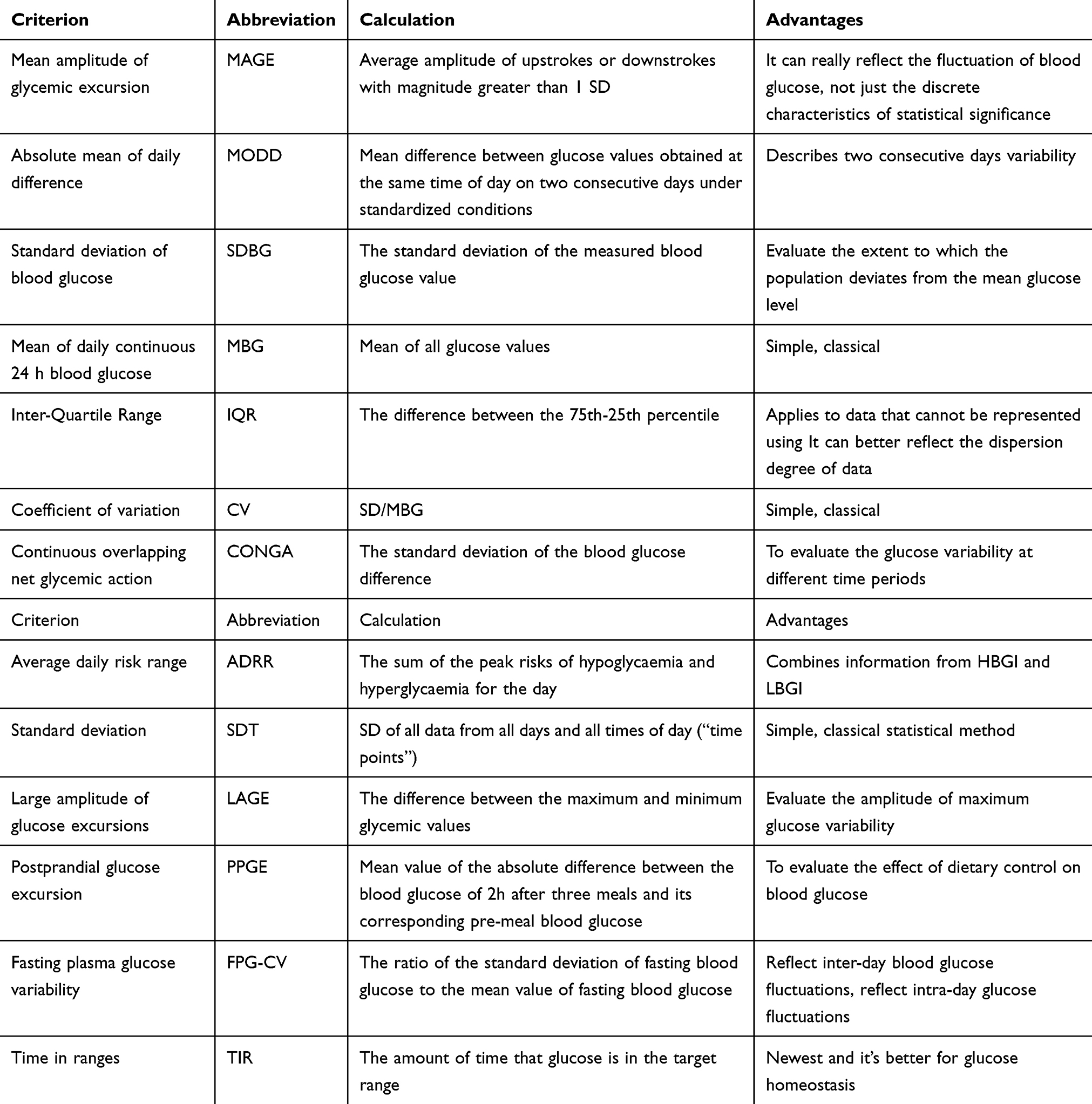 |
Table 2 Measures of Glucose Variability |
Initially, Service et al38 conducted research on mean amplitude of glycemic excursion (MAGE) and absolute mean of daily difference (MODD). Subsequent studies have proposed standard deviation of blood glucose (SDBG) values, mean of daily continuous 24-hour blood glucose (MBG) and its derivative indicators such as inter-quartile range (IQR) and coefficient of variation (CV). These indicators are simple and convenient, but data processing cannot be performed on non-Gaussian, skewed asymmetric distribution or outliers.39 McDonnell et al40 proposed the use of continuous overlapping net glycemic action (CONGA) as a new method for evaluating intraday blood glucose variability. A high CONGA value indicates unstable blood glucose control, while a low CONGA value reflects stable blood glucose control. Since most measurement methods such as SDBG, average blood glucose value, etc. depend mainly on free high blood glucose, they are not very sensitive to low blood glucose. In 2006, Kovatchev et al10 proposed using average daily risk range (ADRR) as a new indicator for GV evaluation, which is equally sensitive to hypoglycemia and hyperglycemia, and can be easily detected by self-monitoring of blood glucose (SMBG). The value of ADRR is the glycemic data converted into the corresponding risk value for the occurrence of hyperglycemia and hypoglycemia. Low risk means that the occurrences of hyperglycemia and hypoglycemia were less. The ADRR is scored based on risk categories: low risk, 0–19; moderate risk, 20–40; and high risk, 40 and above. Rodbard41 suggested that when the degree of blood glucose variation is great, blood glucose changes will occur within a short period of time, between days and days or between daily averages, which requires the use of “overall” SDBG to measure, namely, SDT. The parameters are flexible and changeable. When new treatment methods or other interventions are introduced, these parameters can be changed; that is, some parameters increase, while others decrease. With the increasing number of blood glucose fluctuation parameters, the 2017 Chinese diabetes blood glucose fluctuation management expert consensus42 divided the commonly used blood glucose fluctuation indicators of the Chinese population into intra-day blood glucose fluctuation indicators and inter-day glucose fluctuation indicators. The indicators that reflect intra-day glucose fluctuations are MAGE, maximum amplitude of glucose excursions (LAGE), SDBG, and postprandial glucose excursion (PPGE). The indicators that reflect inter-day blood glucose fluctuations include fasting plasma glucose variability (FPG-CV) and MODD. Study on the indicators of blood glucose fluctuations will continue. In 2020, Foreman et al43 used the Maastricht Study to conduct continuous glucose monitoring (CGM) testing, suggesting that GV is highly correlated with 1 hour-oral glucose tolerance test (OGTT), incremental glucose peak (IGP) and the glucose peak; the author recommended these indicators as the preferred OGTT derivative indicators for evaluating GV. The 2020 ADA guidelines proposed a new indicator——Time in ranges (TIR), which referred to the time or percentage of blood glucose within the target range within 24 hours.3 The core of TIR control is to ensure the patient’s “glucose homeostasis”, and to control the patient’s blood glucose by simulating the ability of healthy people to regulate blood glucose.44 For patients with type 1 and type 2 diabetes without special risk factors, the TIR target should be greater than 70%.45 Similarly, when TIR falls short of its target, it reflects fluctuations in blood sugar in terms of time. For patients with gestational diabetes, there is no special indicator to assess their blood glucose fluctuations. We reviewed the English literature related to GDM and GV, and summarized the evaluation indicators of GV. The results are shown in Table 3. MAGE, SD, CONGA, IQR, CV and MBG are used commonly in the available studies. The use of these indicators shows that they are able to better manage the blood glucose metabolism of pregnant women with GDM. In clinical practice, SMBG is widely used, and patients are not monitored on a daily basis as required. We believe that SD, CV, MBG and other traditional indicators are more suitable for GDM pregnant women. However, with the development of the times and the popularization of CGM system, indicators such as MAGE and MODD will be more suitable for GDM pregnant women.
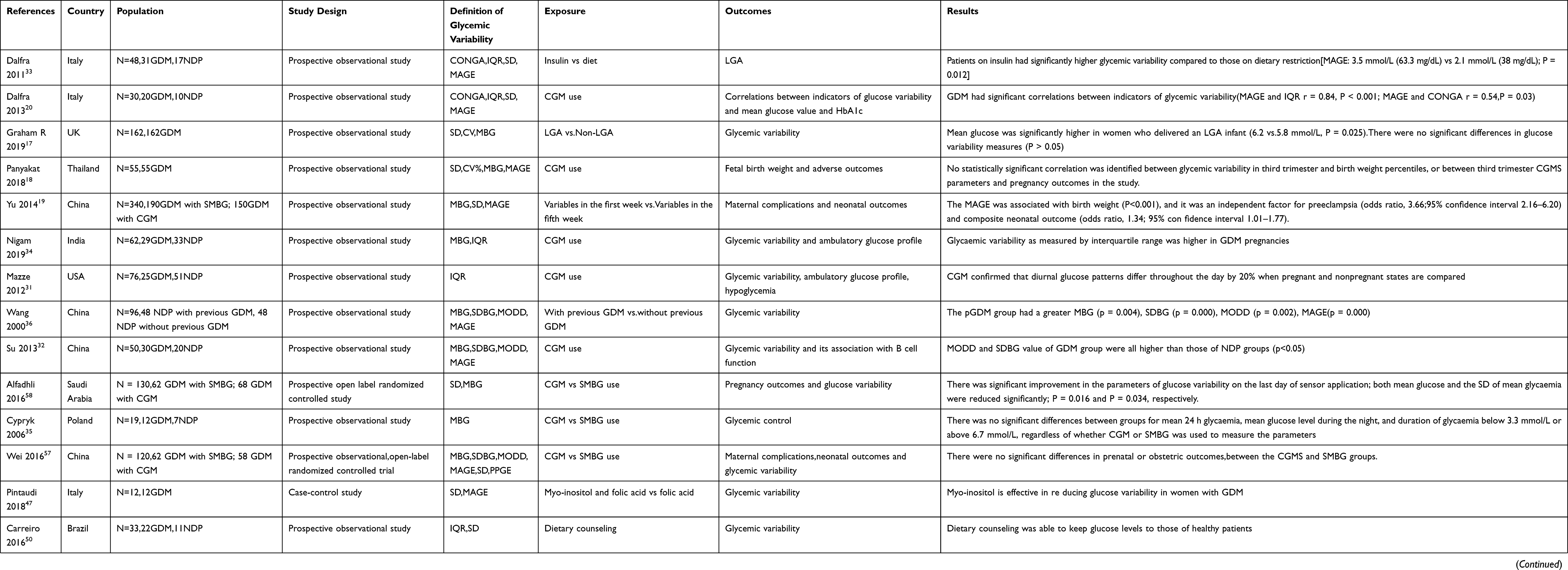 |
Table 3 Indicators Evaluating GV in GDM Researches |
Adverse Maternal and Neonatal Outcomes of Gestational Diabetes and Blood Glucose Fluctuations
GDM can lead to many adverse maternal and neonatal outcomes. Women with GDM are at risk of postpartum complications, including diabetes after the end of pregnancy and GDM in subsequent pregnancies. The unborn child has a higher risk of complications, inluding premature delivery, miscarriage, macrosomia and intrauterine growth retardation.46 The adverse intrauterine environment caused by GDM may result in epigenetic changes, making future generations more prone to metabolic diseases in later life. That is, children born to women with GDM have a higher risk of developing type 2 diabetes, obesity, cardiovascular disease, and metabolic syndrome in late childhood and adulthood.47
Although studies have evaluated the blood glucose fluctuations of pregnant women with GDM and the occurrence of adverse maternal and neonatal outcomes, the conclusions are inconsistent. Two studies have shown that blood glucose fluctuations have no correlation with the occurrence of adverse maternal and neonatal outcome.17,18 Law et al17 showed that the average blood glucose level of women giving birth to fetuses that are large for gestational age (LGA) was relatively high, especially at night, accounting for more than 25% of fluctuations. However, no significant differences were found in blood glucose levels during the day, and no significant differences were found in the measurement of blood glucose fluctuations between pregnant women who delivered LGA and those who did not. Panyakat et al18 found no statistically significant differences in birth weight percentiles, perinatal outcomes and average blood glucose levels, percentage coefficient of variation (% CV), and no correlation between blood glucose changes in late pregnancy and birth weight percentile or adverse pregnancy outcomes. However, the Panyakat study included relatively few pregnant women and only studied women in late pregnancy. Contrary to the above conclusions, three studies have shown that greater blood glucose fluctuations are more likely to cause adverse maternal and infant outcomes.19–21 Yu et al19 found that MAGE in the first week was an independent risk factor for adverse neonatal outcomes such as LGA, small for gestational age (SGA), and neonatal RDS; and in the fifth week, a strong correlation was shown between MAGE and birth weight, and birth weight percentile. Moreover, MAGE also predicted poor prognoses such as preeclampsia and neonatal hypoglycemia. Dalfra et al20 suggested that although the GV index and average blood glucose level of patients with GDM are only slightly higher than those of the non-GDM control group, the slight increase will also affect the growth of the fetus. A large-scale multicenter study of hyperglycemia and adverse pregnancy outcomes (HAPO study)21 showed that the risk of LGA may increase along with the increase of every standard deviation of maternal blood glucose concentration. Conversely, the risk of SGA will increase according to every decrease of maternal blood glucose concentration by one standard deviation. In addition, the maternal blood glucose level is related to adverse outcomes such as premature delivery, shoulder dystocia or birth injury, neonatal intensive care, neonatal hyperbilirubinemia and preeclampsia more or less.
According to the results of the above studies, consistent opinions are lacking about the impact of GV on the occurrence of adverse maternal and neonatal outcomes in women with GDM. The discrepancies between results of these studies may be due to the small number of samples in some studies, or certain differences in the effect of GV on the maternal and neonatal outcomes in pregnant women in the second and third trimesters. From an ethical point of view, we suggest that clinicians often use the CGM system and the SNBG system to perform blinded experiments to obtain a large number of blood glucose values for pregnant women, and when the proportion of blood glucose values is too large in the ranges of hyperglycemia and hypoglycemia, glycemic control must be achieved instead of letting the experimental results develop, which may be a biasing factor for invalid results. We have included all studies on the correlations between blood glucose fluctuations and adverse outcomes in gestational diabetes, but the number of such studies is still too small. Therefore, more relevant studies are needed in the future, and future studies also should have a larger sample size, longer follow-up time, and a standardized research design to detect the actual impact of GV on maternal and neonatal outcomes. In addition, because birth weight reflects the intrauterine environment provided by maternal nutrition, hormones, and metabolic environment, it is often used as an indicator of fetal growth, and many studies on the adverse maternal and neonatal outcomes study mainly LGA and SGA. We hope that future studies will address more aspects of GV in pregnant women.
Controlling GV
GV has a certain impact on both non-pregnant and pregnant women with GDM. The means by which to reduce GV and regulate blood glucose levels is the focus of many clinicians, which is also aimed at ways to reduce the adverse outcomes of GDM. Measures to reduce GV are reflected in blood glucose monitoring equipment, drug application, and diet. Previous studies have shown that CGM is useful as an educational and motivational tool for poorly controlled type 1 and type 2 diabetes. Recent studies have shown that for pregnant women with GDM, the CGM system is more capable of reducing GV than SMBG.19,48 The CGM system helps pregnant women to understand the effects of food, exercise, and insulin on their blood glucose levels, which helps to change patients’ diet and exercise habits.
Several studies have shown that myo-inositol (Myo-Ins) supplementation can improve blood glucose fluctuations.49 Pintaudi et al49 suggested that the blood glucose peak of human beings can reduce GV. In that study, SD, MAGE and CV values in the group of patients taking inositol were significantly improved compared to those in the group of patients taking folic acid alone.49 This is because inositol can effectively reduce insulin resistance and stabilize glucose levels.50,51 Three studies have shown specifically that dietary control can reduce blood glucose fluctuations in pregnant women with GDM.52–54 Studies also have shown that reducing postprandial hyperglycemia can effectively reduce postprandial hyperglycemia peak. Carreiro et al52 found that receiving dietary consultation can improve the GV of pregnant women with GDM. A study by Rasmussen et al53 showed that the GV of pregnant women with GDM in the group eating a high-carbon breakfast was significantly higher than that of pregnant women with GDM in the group eating a low-carbon breakfast. Similarly, a small sample study54 showed that the low-glycemic-load diet significantly reduced the GV index of pregnant women with GDM compared with the high-glycemic-load diet. Dalfra et al33 found that diet therapy alone can improve GV in pregnant women with GDM. The 2020 ADA guidelines55 specify that a good lifestyle (diet control and proper exercise) is an important part of GDM management. About 70%-85% of women diagnosed with GDM can control postprandial hyperglycemia and reduce GV by simply changing lifestyles, which can meet the treatment needs of many women. Reasonable insulin treatment can help make the blood glucose of patients with gestational diabetes stable to reach the standard.55 However, unreasonable insulin application may increase the risk of hypoglycemia, including not properly adjusting insulin doses, not monitoring and adjusting the insulin dose in a timely manner, and not receiving sufficient health education. Therefore, in clinical practice, it is necessary to carry out health education for patients and guide patients to monitor blood glucose on a timely basis and adjust insulin dosage to avoid blood glucose fluctuations caused by hypoglycemia.
Application of Blood Glucose Monitoring in GDM
Providing more convenient and accurate blood glucose measuring equipment for patients with diabetics is essential. In recent years, different types of blood glucose monitoring methods have emerged one after another, and SMBG and CGM are used most commonly. According to the SMBG standard, patients are required to perform finger-puncture 7 times a day to determine blood glucose levels. This method is convenient, inexpensive, and easily popularized. However, in real life, few diabetic individuals measure blood glucose 7 times a day. Most patients only measure fasting and postprandial blood glucose levels, and a few people may only measure the fasting blood glucose level, so that patients cannot know their actual blood glucose status, which eventually leads to greater blood glucose fluctuations and increased complications. CGM uses subcutaneous sensors to measure glucose levels in interstitial fluid, and no missed measurements will occur. This method can not only monitor blood glucose continuously, but also can display blood glucose fluctuations. Nevertheless, CGM is more expensive and is therefore more difficult to be popularized. CGM systems commonly used today are divided into two categories, real-time continuous glucose monitoring (rtCGM) and intermittently viewed CGM (iCGM).56 The iCGM can provide the current glucose value and trace the glucose data after the reader comes into contact with the glucose sensor in the patient’s upper arm.57 rtCGM can view real-time digital and graphic information of current glucose level, glucose trend and glucose change direction at any time.58 CGM is licensed by The US Food and Drug Administration (FDA), although no studies have shown that the product has adverse effects on patients or children.56,59 However, the CGM system is an invasive method of diagnosis and treatment, so the patient’s authorization must be obtained when using it. In the ten years after CGM was introduced into clinical application, more and more studies compared it with SMBG, confirming that CGM not only had the same accuracy as SMBG,60 but also obtains better results in patients with type 2 diabetes.61 It can also improve glycated hemoglobin and reduce GV in patients with type 1 diabetes.62 Studies have compared the frequency and severity of hyperglycemia and hypoglycemia in GDM patient population using CGM and SMBG, and the results show that the CGM system can better monitor the occurrence of hyperglycemia and hypoglycemia.63 Due to the specificity of the GDM patient population, more and more patients have started to pay attention to the relationship between the use of SMBG and CGM and the incidence of adverse maternal and neonatal outcomes.
Some studies have compared the occurrence of adverse maternal and neonatal outcomes of pregnant women with GDM after using CGM and SMBG, but the conclusions of these authors are inconsistent. Three studies showed no significant differences in the occurrence of adverse maternal and neonatal outcomes between pregnant women with GDM who used CGM and those who used SMBG.64–66 Wei et al64 found no significant differences in women receiving Cesarean section and fluctuations of glycated hemoglobin between patients with GDM who used CGM and those who used SMBG for blood glucose monitoring, and there were also no significant differences in fetal adverse outcomes. Similarly, Alfadhli et al65 found no significant differences between two blood glucose monitoring methods in Cesarean section-related fetal adverse outcomes and GV parameters of pregnant women with GDM. McLachlan et al66 found that the use of CGM and SMBG for blood glucose monitoring showed no significant differences in the rates of pre-eclampsia, hypertension during pregnancy, maternal laceration, Cesarean section and adverse fetal outcomes in pregnant women with GDM.
Contrary to the above conclusions, two studies have shown that the use of CGM in pregnant women with GDM reduces the incidence of adverse maternal and neonatal outcomes more effectively compared with SMBG.19,48 Voormolen et al48 showed that the incidence of preeclampsia in the CGM group was much lower than that in the SMBG group, while adverse fetal outcomes incidence was consistent with that reported in the previous three studies. Similarly, Yu et al19 also confirmed that, compared with the CGM group, the SMBG group had a lower incidence of preeclampsia and better fetal outcomes, namely, relatively low incidences of macrosomia, neonatal hypoglycemia, neonatal hyperbilirubinemia, and neonatal respiratory distress syndrome. The above review verifies that CGM can effectively obtain blood glucose profiles during pregnancy, which allows clinicians to gain a better grasp of the onset of hyperglycemia and hypoglycemia, so as to make appropriate adjustments in medication and diet, thereby improving the therapeutic effect of pregnant women with GDM. CGM detects more blood glucose abnormalities than SMBG, and can detect higher GV in pregnant women with GDM than in normal pregnancies. However, controversy still exists over whether the CGM system can improve maternal and neonatal outcomes or not. In terms of financial aspect, SMBG is cheaper on both test strips and devices than the CGM, making it more affordable for a patient who needs a lifetime of home glucose monitoring.67,68 And CGM as a new monitoring technique, high prices, at least now cannot be popular, but it’s for blood glucose fluctuations and diabetes complications early warning effect is obvious to all,69 so we suggest that there is high blood sugar and the risk of hypoglycemia in type 1 and type 2 diabetes patients with short-term use, thereby reducing the occurrence of diabetes complications. For patients with gestational diabetes, the duration of gestational diabetes is limited, and the fluctuation of blood glucose has a great impact on mothers and infants. Considering the advantages and disadvantages, we recommend that patients with gestational diabetes with economic conditions use the CGM system.
Conclusion
As a new concept of glycemic control, GV has many unique evaluation indicators such as MAGE, SD, IQR, etc. The importance of GV for pregnant women with GDM cannot be ignored. The GV of pregnant women with GDM is significantly higher than that of pregnant women with NDP. Many studies have shown certain correlations between GV and adverse outcomes of pregnant women with GDM. Therefore, clinicians need to pay more attention to how to control GV. GV can be controlled by adjusting insulin levels and improving lifestyles. In addition, the application of the CGM system can control GV better than SMBG, obtain the dynamic blood glucose curve of patients with GDM, and monitor more blood glucose abnormalities. Because control of GV has a definite impact on improving outcomes of GDM pregnancies, it is necessary to carry out further, rigorous and complete studies to obtain more clinical data and help clinicians address this challenge in clinical practice.
Statement of Ethics
This article does not contain any studies with human or animals performed by any of the authors.
Acknowledgments
We gratefully acknowledge Yueyang Zhao for providing intellectual support and technical assistance.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Correa A, Bardenheier B, Elixhauser A, Geiss LS, Gregg E. Trends in prevalence of diabetes among delivery hospitalizations, United States, 1993–2009. Matern Child Health J. 2015;19(3):635–642. doi:10.1007/s10995-014-1553-5
2. Mukesh M.Agarwal, Michel Boulvain, Edward Coetzee, et al. Diagnostic criteria and classification of hyperglycaemia first detected in pregnancy: a World Health Organization guideline. Diabetes Res Clin Pract. 2014;103(3):341–363. doi:10.1016/j.diabres.2013.10.012
3. American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes–2020. Diabetes Care. 2020;43(Suppl1):S14–s31. doi:10.2337/dc20-S002
4. Hod M, Kapur A, Sacks DA, et al. The International Federation of Gynecology and Obstetrics (FIGO) initiative on gestational diabetes mellitus: a pragmatic guide for diagnosis, management, and care. Int J Gynaecol Obstet. 2015;131(Suppl 3):S173–s211. doi:10.1016/S0020-7292(15)30033-3
5. Metzger BE, Gabbe SG, Persson B, et al. International Association of Diabetes and Pregnancy Study Groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33(3):676–682. doi:10.2337/dc10-0719
6. Society. CD. Guidelines for the prevention and control of type 2 diabetes in China (2017 Edition). Chin J Pract Intern Med. 2018;38(4):292–344.
7. gynecology Csooa. Guidelines for the diagnosis and treatment of gestational diabetes mellitus. Diabetes World. 2014;8(11):489–498.
8. Gestational Diabetes Mellitus. ACOG Practice Bulletin No. 190. Obstet Gynecol. 2018;131(2):e49–e64. doi:10.1097/AOG.0000000000002501
9. Noctor E, Crowe C, Carmody LA, et al. Abnormal glucose tolerance post-gestational diabetes mellitus as defined by the International Association of Diabetes and Pregnancy Study Groups criteria. Eur J Endocrinol. 2016;175(4):287–297. doi:10.1530/EJE-15-1260
10. Kovatchev BP, Otto E, Cox D, Gonder-Frederick L, Clarke W. Evaluation of a new measure of blood glucose variability in diabetes. Diabetes Care. 2006;29(11):2433–2438. doi:10.2337/dc06-1085
11. Hirsch IB, Brownlee M. Should minimal blood glucose variability become the gold standard of glycemic control? J Diabetes Complications. 2005;19(3):178–181. doi:10.1016/j.jdiacomp.2004.10.001
12. Rodbard D. Glucose variability: a review of clinical applications and research developments. Diabetes Technol Ther. 2018;20(S2):S25–s215. doi:10.1089/dia.2018.0092
13. Škrha J, Šoupal J, Škrha J, Prázný M. Glucose variability, HbA1c and microvascular complications. Rev Endocr Metab Disord. 2016;17(1):103–110. doi:10.1007/s11154-016-9347-2
14. Smith-Palmer J, Brändle M, Trevisan R, Orsini Federici M, Liabat S, Valentine W. Assessment of the association between glycemic variability and diabetes-related complications in type 1 and type 2 diabetes. Diabetes Res Clin Pract. 2014;105(3):273–284. doi:10.1016/j.diabres.2014.06.007
15. Gorst C, Kwok CS, Aslam S, et al. Long-term glycemic variability and risk of adverse outcomes: a systematic review and meta-analysis. Diabetes Care. 2015;38(12):2354–2369. doi:10.2337/dc15-1188
16. Chehregosha H, Khamseh ME, Malek M, Hosseinpanah F, Ismail-Beigi F. A view beyond HbA1c: role of continuous glucose monitoring. Diabetes Ther. 2019;10(3):853–863. doi:10.1007/s13300-019-0619-1
17. Law GR, Alnaji A, Alrefaii L, et al. Suboptimal nocturnal glucose control is associated with large for gestational age in treated gestational diabetes mellitus. Diabetes Care. 2019;42(5):810–815. doi:10.2337/dc18-2212
18. Panyakat WS, Phatihattakorn C, Sriwijitkamol A, Sunsaneevithayakul P, Phaophan A, Phichitkanka A. Correlation between third trimester glycemic variability in non-insulin-dependent gestational diabetes mellitus and adverse pregnancy and Fetal outcomes. J Diabetes Sci Technol. 2018;12(3):622–629. doi:10.1177/1932296817752374
19. Yu F, Lv L, Liang Z, et al. Continuous glucose monitoring effects on maternal glycemic control and pregnancy outcomes in patients with gestational diabetes mellitus: a prospective cohort study. J Clin Endocrinol Metab. 2014;99(12):4674–4682. doi:10.1210/jc.2013-4332
20. Dalfrà MG, Chilelli NC, Di Cianni G, et al. Glucose fluctuations during gestation: an additional tool for monitoring pregnancy complicated by diabetes. Int J Endocrinol. 2013;2013:279021. doi:10.1155/2013/279021
21. Boyd E.Metzger, Lynn P. Lowe, Alan R. Dyer, et al. Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study: associations with neonatal anthropometrics. Diabetes. 2009;58(2):453–459. doi:10.2337/db08-1112
22. Picconi F, Di Flaviani A, Malandrucco I, Giordani I, Frontoni S. Impact of glycemic variability on cardiovascular outcomes beyond glycated hemoglobin. Evidence and clinical perspectives. Nutr Metab Cardiovasc Dis. 2012;22(9):691–696. doi:10.1016/j.numecd.2012.03.006
23. Cryer PE, Davis SN, Shamoon H. Hypoglycemia in diabetes. Diabetes Care. 2003;26(6):1902–1912. doi:10.2337/diacare.26.6.1902
24. Meigs JB, Nathan DM, D’Agostino RB, Wilson PW. Fasting and postchallenge glycemia and cardiovascular disease risk: the Framingham Offspring Study. Diabetes Care. 2002;25(10):1845–1850. doi:10.2337/diacare.25.10.1845
25. Shichiri M, Kishikawa H, Ohkubo Y, Wake N. Long-term results of the Kumamoto Study on optimal diabetes control in type 2 diabetic patients. Diabetes Care. 2000;23(Suppl 2):B21–29.
26. Ceriello A, Ihnat MA. ‘Glycaemic variability’: a new therapeutic challenge in diabetes and the critical care setting. Diabet Med. 2010;27(8):862–867. doi:10.1111/j.1464-5491.2010.02967.x
27. Ceriello A, Esposito K, Piconi L, et al. Oscillating glucose is more deleterious to endothelial function and oxidative stress than mean glucose in normal and type 2 diabetic patients. Diabetes. 2008;57(5):1349–1354. doi:10.2337/db08-0063
28. Reece EA, Homko CJ. Prepregnancy care and the prevention of fetal malformations in the pregnancy complicated by diabetes. Clin Obstet Gynecol. 2007;50(4):990–997. doi:10.1097/GRF.0b013e31815a634b
29. Desouza CV, Bolli GB, Fonseca V. Hypoglycemia, diabetes, and cardiovascular events. Diabetes Care. 2010;33(6):1389–1394. doi:10.2337/dc09-2082
30. Herranz L, Pallardo LF, Hillman N, Martin-Vaquero P, Villarroel A, Fernandez A. Maternal third trimester hyperglycaemic excursions predict large-for-gestational-age infants in type 1 diabetic pregnancy. Diabetes Res Clin Pract. 2007;75(1):42–46. doi:10.1016/j.diabres.2006.05.019
31. Mazze R, Yogev Y, Langer O. Measuring glucose exposure and variability using continuous glucose monitoring in normal and abnormal glucose metabolism in pregnancy. J Matern Fetal Neonatal Med. 2012;25(7):1171–1175. doi:10.3109/14767058.2012.670413
32. Su JB, Wang XQ, Chen JF, et al. Glycemic variability in gestational diabetes mellitus and its association with β cell function. Endocrine. 2013;43(2):370–375. doi:10.1007/s12020-012-9753-5
33. Dalfrà MG, Sartore G, Di Cianni G, et al. Glucose variability in diabetic pregnancy. Diabetes Technol Ther. 2011;13(8):853–859. doi:10.1089/dia.2010.0145
34. Nigam A, Sharma S, Varun N, Munjal YP, Prakash A. Comparative analysis of 2-week glycaemic profile of healthy versus mild gestational diabetic pregnant women using flash glucose monitoring system: an observational study. Bjog. 2019;126(Suppl 4):27–33. doi:10.1111/1471-0528.15849
35. Cypryk K, Pertyńska-Marczewska M, Szymczak W, Wilcyński J, Lewiński A. Evaluation of metabolic control in women with gestational diabetes mellitus by the continuous glucose monitoring system: a pilot study. Endocr Pract. 2006;12(3):245–250. doi:10.4158/EP.12.3.245
36. Wang Y, Storlien LH, Jenkins AB, et al. Dietary variables and glucose tolerance in pregnancy. Diabetes Care. 2000;23(4):460–464. doi:10.2337/diacare.23.4.460
37. Porter H, Lookinland S, Belfort MA. Evaluation of a new real-time blood continuous glucose monitoring system in pregnant women without gestational diabetes. A pilot study. J Perinat Neonatal Nurs. 2004;18(2):93–102. doi:10.1097/00005237-200404000-00004
38. Service FJ, Molnar GD, Rosevear JW, Ackerman E, Gatewood LC, Taylor WF. Mean amplitude of glycemic excursions, a measure of diabetic instability. Diabetes. 1970;19(9):644–655. doi:10.2337/diab.19.9.644
39. Rodbard D. Interpretation of continuous glucose monitoring data: glycemic variability and quality of glycemic control. Diabetes Technol Ther. 2009;11(Suppl 1):S55–67. doi:10.1089/dia.2008.0132
40. McDonnell CM, Donath SM, Vidmar SI, Werther GA, Cameron FJ. A novel approach to continuous glucose analysis utilizing glycemic variation. Diabetes Technol Ther. 2005;7(2):253–263. doi:10.1089/dia.2005.7.253
41. Rodbard D. Optimizing display, analysis, interpretation and utility of self-monitoring of blood glucose (SMBG) data for management of patients with diabetes. J Diabetes Sci Technol. 2007;1(1):62–71. doi:10.1177/193229680700100111
42. endocrinology Cso. Experts consensus on management of glycemic variability of diabetes mellitus. Drug Evaluation. 2017;014(17):5–8,14.
43. Foreman YD, Brouwers M, van der Kallen CJH, et al. Glucose variability assessed with continuous glucose monitoring: reliability, reference values, and correlations with established glycemic indices – the Maastricht study. Diabetes Technol Ther. 2020;22:395–403. doi:10.1089/dia.2019.0385
44. Li C, Liu C, Nissim I, et al. Regulation of glucagon secretion in normal and diabetic human islets by γ-hydroxybutyrate and glycine. J Biol Chem. 2013;288(6):3938–3951. doi:10.1074/jbc.M112.385682
45. Beck RW, Bergenstal RM, Riddlesworth TD, Kollman C. The association of biochemical hypoglycemia with the subsequent risk of a severe hypoglycemic event: analysis of the DCCT data set. Diabetes Technol Ther. 2019;21(1):1–5. doi:10.1089/dia.2018.0362
46. Jolly MC, Sebire NJ, Harris JP, Regan L, Robinson S. Risk factors for macrosomia and its clinical consequences: a study of 350,311 pregnancies. Eur J Obstet Gynecol Reprod Biol. 2003;111(1):9–14. doi:10.1016/S0301-2115(03)00154-4
47. Murtaugh MA, Jacobs DR, Moran A, Steinberger J, Sinaiko AR. Relation of birth weight to fasting insulin, insulin resistance, and body size in adolescence. Diabetes Care. 2003;26(1):187–192. doi:10.2337/diacare.26.1.187
48. Voormolen DN, DeVries JH, Sanson RME, et al. Continuous glucose monitoring during diabetic pregnancy (GlucoMOMS): a multicentre randomized controlled trial. Diabetes Obes Metab. 2018;20(8):1894–1902. doi:10.1111/dom.13310
49. Pintaudi B, Di Vieste G, Corrado F, et al. Effects of myo-inositol on glucose variability in women with gestational diabetes. Eur Rev Med Pharmacol Sci. 2018;22(19):6567–6572. doi:10.26355/eurrev_201810_16073
50. Corrado F, D’Anna R, Di Vieste G, et al. The effect of myoinositol supplementation on insulin resistance in patients with gestational diabetes. Diabet Med. 2011;28(8):972–975. doi:10.1111/j.1464-5491.2011.03284.x
51. Costabile L, Unfer V. Treatment of gestational diabetes mellitus with myo-inositol: analyzing the cutting edge starting from a peculiar case. Eur Rev Med Pharmacol Sci. 2017;21(2 Suppl):73–76.
52. Carreiro MP, Lauria MW, Naves GN, et al. Seventy two-hour glucose monitoring profiles in mild gestational diabetes mellitus: differences from healthy pregnancies and influence of diet counseling. Eur J Endocrinol. 2016;175(3):201–209. doi:10.1530/EJE-16-0015
53. Rasmussen L, Christensen ML, Poulsen CW, et al. Effect of high versus low carbohydrate intake in the morning on glycemic variability and glycemic control measured by continuous blood glucose monitoring in women with gestational diabetes mellitus – a randomized crossover study. Nutrients. 2020;12(2):475. doi:10.3390/nu12020475
54. Kizirian NV, Goletzke J, Brodie S, et al. Lower glycemic load meals reduce diurnal glycemic oscillations in women with risk factors for gestational diabetes. BMJ Open Diabetes Res Care. 2017;5(1):e000351. doi:10.1136/bmjdrc-2016-000351
55. American Diabetes Association. 14. Management of diabetes in pregnancy: standards of medical care in diabetes-2020. Diabetes Care. 2020;43(Suppl1):S183–s192. doi:10.2337/dc20-S014
56. Danne T, Nimri R, Battelino T, et al. International consensus on use of continuous glucose monitoring. Diabetes Care. 2017;40(12):1631–1640. doi:10.2337/dc17-1600
57. Bolinder J, Antuna R, Geelhoed-Duijvestijn P, Kröger J, Weitgasser R. Novel glucose-sensing technology and hypoglycaemia in type 1 diabetes: a multicentre, non-masked, randomised controlled trial. Lancet. 2016;388(10057):2254–2263. doi:10.1016/S0140-6736(16)31535-5
58. Kropff J, Choudhary P, Neupane S, et al. Accuracy and longevity of an implantable continuous glucose sensor in the PRECISE study: a 180-day, prospective, multicenter, pivotal tRial. Diabetes Care. 2017;40(1):63–68. doi:10.2337/dc16-1525
59. Administration UFaD. FDA authorizes first fully interoperable continuous glucose monitoring system, streamlines review pathway for similar devices. Fda News Release. 2018.
60. Chitayat L, Zisser H, Jovanovic L. Continuous glucose monitoring during pregnancy. Diabetes Technol Ther. 2009;11(Suppl 1):S105–111. doi:10.1089/dia.2008.0136
61. Cypryk K, Bartyzel L, Zurawska-Klis M, et al. Continuous glucose monitoring in type 1 diabetes pregnancy shows that fetal heart rate correlates with maternal glycemia. Diabetes Technol Ther. 2015;17(9):619–624. doi:10.1089/dia.2014.0255
62. Slattery D, Choudhary P. Clinical use of continuous glucose monitoring in adults with type 1 diabetes. Diabetes Technol Ther. 2017;19(S2):S55–s61. doi:10.1089/dia.2017.0051
63. Afandi B, Hassanein M, Roubi S, Nagelkerke N. The value of continuous glucose monitoring and self-monitoring of blood glucose in patients with gestational diabetes mellitus during Ramadan fasting. Diabetes Res Clin Pract. 2019;151:260–264. doi:10.1016/j.diabres.2019.01.036
64. Wei Q, Sun Z, Yang Y, Yu H, Ding H, Wang S. Effect of a CGMS and SMBG on maternal and neonatal outcomes in gestational diabetes mellitus: a randomized controlled trial. Sci Rep. 2016;6:19920. doi:10.1038/srep19920
65. Alfadhli E, Osman E, Basri T. Use of a real time continuous glucose monitoring system as an educational tool for patients with gestational diabetes. Diabetol Metab Syndr. 2016;8:48. doi:10.1186/s13098-016-0161-5
66. McLachlan K, Jenkins A, O’Neal D. The role of continuous glucose monitoring in clinical decision-making in diabetes in pregnancy. Aust N Z J Obstet Gynaecol. 2007;47(3):186–190. doi:10.1111/j.1479-828X.2007.00716.x
67. Xie Y, Agiro A, Bowman K, DeVries A. Lowering cost share may improve rates of home glucose monitoring among patients with diabetes using insulin. J Manag Care Spec Pharm. 2017;23(8):884–891. doi:10.18553/jmcp.2017.23.8.884
68. Yeaw J, Lee WC, Aagren M, Christensen T. Cost of self-monitoring of blood glucose in the United States among patients on an insulin regimen for diabetes. J Manag Care Pharm. 2012;18(1):21–32. doi:10.18553/jmcp.2012.18.1.21
69. Rodbard D. Continuous glucose monitoring: a review of successes, challenges, and opportunities. Diabetes Technol Ther. 2016;18(Suppl2):S3–s13. doi:10.1089/dia.2015.0417
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.