Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
A Retrospective Study on the Clinical, Laboratory, and Nutritional Status of Pediatric Epidermolysis Bullosa in a Tertiary Referral Hospital in West Java, Indonesia
Authors Tsaqilah L ![]() , Diana IA, Gondokaryono SP
, Diana IA, Gondokaryono SP ![]() , Effendi RMRA
, Effendi RMRA ![]() , Suwarsa O
, Suwarsa O ![]() , Gunawan H
, Gunawan H ![]() , Hidayah RMN
, Hidayah RMN ![]() , Dwiyana RF
, Dwiyana RF ![]()
Received 11 April 2023
Accepted for publication 21 June 2023
Published 24 June 2023 Volume 2023:16 Pages 1615—1621
DOI https://doi.org/10.2147/CCID.S413093
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Laila Tsaqilah, Inne Arline Diana, Srie Prihianti Gondokaryono, Raden Mohamad Rendy Ariezal Effendi, Oki Suwarsa, Hendra Gunawan, Risa Milliawati Nurul Hidayah, Reiva Farah Dwiyana
Department of Dermatology and Venereology, Dr. Hasan Sadikin General Hospital, Faculty of Medicine Universitas Padjadjaran, Bandung, Indonesia
Correspondence: Laila Tsaqilah, Department of Dermatology and Venereology Faculty of Medicine, Universitas Padjadjaran – Dr. Hasan Sadikin General Hospital, Jl. Pasteur 38, Bandung, West Java, 40161, Indonesia, Tel +62 222032426 ext. 3449, Fax +62 222032426, Email [email protected]
Background: Epidermolysis bullosa (EB) is a genodermatosis disease with bullae and erosions of the skin and mucous membrane that can last for a lifetime and decrease quality of life. Oral and gastrointestinal disorders inhibit the patients’ ability to achieve optimal nutrition, making the patients prone to infection, leading to prolonged wound healing, and delayed growth and developmental process. However, there has been no research on the clinical, laboratory, and nutritional status of pediatric EB patients in Indonesia.
Purpose: This study aims to describe the clinical, laboratory, and nutritional characteristics of pediatric EB patients treated in Dr. Hasan Sadikin General Hospital Bandung, Indonesia.
Patients and Methods: This was a retrospective descriptive study of pediatric EB patient records in Dermatology and Venereology Outpatient of Dr. Hasan Sadikin General Hospital Bandung, Indonesia, from April 2018-March 2020.
Results: Study results showed 12 pediatric EB patients consisting of 7 dystrophic EB (DEB) (4 recessive dystrophic EB [RDEB] patients and 3 dominant dystrophic EB [DDEB]), 3 junctional EB (JEB), and 2 EB simplex (EBS). The most extensive EB wounds was found affecting 10– 20% of the body surface area with a < 10% infected wound area. Pain was found in all patients. The most frequent abnormalities in laboratory examination were anemia and low zinc levels. Severe malnutrition was found in almost half of the patients.
Conclusion: RDEB is the most commonly found type of pediatric EB. Wounds on the skin, tooth decay, hand deformity, pain when changing dressings, low zinc levels, and low hemoglobin levels are the clinical features and laboratory findings that contribute to the development of moderate and severe malnutrition in RDEB patients.
Keywords: clinical, epidermolysis bullosa, laboratory, nutritional status
Introduction
Epidermolysis bullosa (EB) is a rare autosomal genodermatosis disease characterized by the formation of bullae and erosions of the skin and mucous membranes,1 indicating that the skin and mucosa are brittle2 and vulnerable to spontaneous mechanical trauma3 or friction.1 Mutations of the gene encoding the basement membrane zone (BMZ) protein are linked to its etiopathogenesis.3 According to the 2014 Consensus, there are four primary types of EB: simplex EB (EBS), junctional EB (JEB), dystrophic EB (DEB) (either recessive dystrophic EB [RDEB] and dominant dystrophic EB [DDEB]), and Kindler syndrome (KS).1,3,4 Bullae, erosions, and crusts exist in all kinds of EB.3 Additionally, milia, nail dystrophy, and anonychia may also develop in EB.5 Extracutaneous involvement occurs in numerous subtypes of EB, particularly in the generalized and severe subtypes. Oropharynx, trachea, esophagus, eyes, hair, and teeth are commonly affected.1,6
The main complications of the chronic erosive lesions of EB are secondary bacterial infection7 and squamous cell carcinoma.2 Chronic wounds in EB patients may lead to anemia, nutritional disorder, and limited physical activity, which will decrease the patient’s quality of life, resulting in failure to thrive, and death.8 To date, there has been no causative treatment for EB.2 Management of wound healing in addition to preventing new lesions and supportive therapy are priorities in the treatment of EB patients.9 Nutritional balance is required in chronic wounds, as it contributes to wound healing and the prevention of secondary bacterial infections.7 Optimal hemoglobin, ferritin, zinc, and albumin levels are factors for optimal wound healing.10–12
There have been no clinical, laboratory, or nutritional studies of pediatric epidermolysis bullosa patients in Indonesia. Therefore, the authors are interested in studying the clinical, laboratory, and nutritional characteristics of EB patients treated at Dr. Hasan Sadikin General Hospital Bandung. The findings of this study are expected to provide scientific information on the clinical outcomes, laboratory findings, and nutritional status of pediatric EB patients at Dr. Hasan Sadikin General Hospital Bandung. Furthermore, the findings of this study are expected to be used as a model for future research and management of pediatric EB patients.
Materials and Methods
This study was conducted at Dr. Hasan Sadikin Hospital Bandung, an Indonesian Tertiary Referral Hospital located in the West Java province, and has been approved by the Institutional Review Board of Health Research Ethics Committee at Dr. Hasan Sadikin Hospital. Parents/legal guardians of every study participant gave consent before study commencement. In this retrospective study, hospital patient records from April 2018 to March 2020 were analyzed. These registers were maintained in the outpatient department of the Pediatric Dermatology Clinic at Dr. Hasan Sadikin General Hospital Bandung and contained information regarding patients’ history, physical examination, body weight, height, and blood examination.
Ethical clearance was obtained from the ethical committee of the institute. Total sampling technique was used; thus, all medical records that fulfilled the inclusion criteria were included in the study. Inclusion criteria were medical records of newly-admitted pediatric EB patients as diagnosed by a dermatologist based on clinical findings from April 2018 – March 2020 that include the patients’ history, physical examination, body weight, height, and blood examination. Exclusion criteria were medical records that were damaged or indecipherable and medical records that were unavailable. Data were then entered into Microsoft Excel for statistical analysis.
Variables in this study were clinical features, laboratory results, and nutritional status. The clinical features studied were onset of illness, duration of illness, type of EB, and clinical factors affecting nutritional status. The latter refer to skin involvement (percentage of EB wound area and percentage of infected EB wound area based on body surface area [BSA], according to the EB Clinical Practice Guidelines); gastrointestinal involvement (oral blisters or sores, microstomia, ankyloglossia, tooth decay, dysphagia, odynophagia, heartburn, epigastric pain, constipation, painful defecation); extraintestinal involvement (hand deformity [pesudosyndactyly] and pain when changing dressings). Laboratory parameters affecting wound healing included hemoglobin, ferritin, albumin, and zinc levels. Nutritional status was assessed using a weight for height chart for children aged <5 years old and a body mass index for age chart for children >5 years old based on World Health Organization (WHO) Z-scores growth charts.
Results
A total of 12 medical records of EB patients were assessed, consisting of records of 6 girl and 6 boy patients. Based on the age group, there were 6 patients aged 1–5 years (the largest age group in this study), 4 patients aged <1 year, and 2 patients aged 11–15 years old. The youngest EB patient was 9 days old and the oldest was 15 years old with a mean of 3.8 ± 4.7 years old. In terms of patients’ recent education, the majority of patients did not go to school due to the fact that 10 patients were not yet of school age and 1 patient decided not to go to school. Only one patient went to school and graduated from elementary school.
The most common type of EB in this study was DEB with 7 patients (4 RDEB and 3 DDEB), followed by JEB (n = 3), and EBS (n = 2). The onset of illness in all patients occurred before 1 year old, as the first complaint was felt since birth or shortly after birth. The clinical features of 12 pediatric EB patients showed that erosion was the most frequent skin involvement as it was found in all patients. Other skin involvements, such as bullae was found in 10 patients, scars in 8 patients, vesicles in 7 patients, and milia in 5 patients. Nail abnormalities were more commonly found on toenails (11 patients) compared to fingernails (7 patients). Oral and throat mucosal abnormalities were seen in 5 patients.
Skin, gastrointestinal, and extraintestinal involvement as clinical factors influencing nutritional status were studied and are shown in Table 1. Most patients had wound areas in the range of 10–20% BSA, mostly found in JEB and DEB patients, and infected wound areas were <10% BSA, commonly found in DEB patients. Twenty gastrointestinal symptoms were recorded as each patient showed more than 1 gastrointestinal involvement. These symptoms were mostly found in DEB patients. Extraintestinal involvement was mostly in the form of pain, especially when changing wound dressings. This was found in all types of pediatric EB patients.
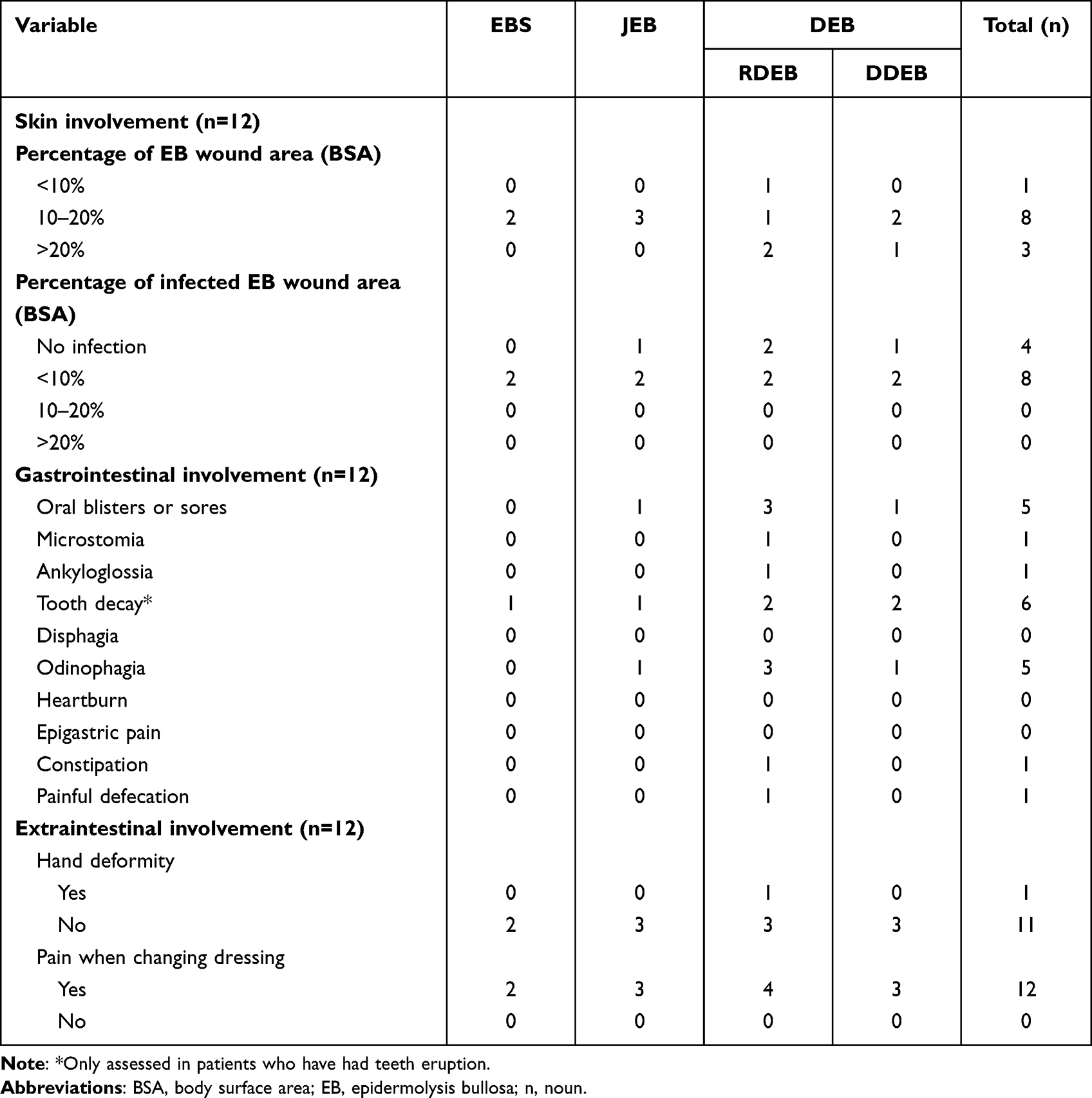 |
Table 1 Clinical Factors Affecting Nutritional Status |
Table 2 shows the laboratory examination and nutritional status of pediatric EB patients. Hemoglobin level was measured in all patients as part of routine blood work-up. The number of patients with low hemoglobin levels was proportional to those with normal hemoglobin levels. Most patients who had their ferritin level and albumin level measured had normal levels for both parameters. In contrast, low zinc level was mostly found in patients who had their zinc level measured. In terms of nutritional status, only 1 patient was observed to have normal nutritional status while the other 11 patients had abnormalities, including 4 patients (2 JEB and 2 DEB patients) with severe malnutrition, 3 patients (2 EBS and 1 DEB patient) with moderate malnutrition, 3 DEB patients at risk of obesity, and 1 DEB patient was overweight.
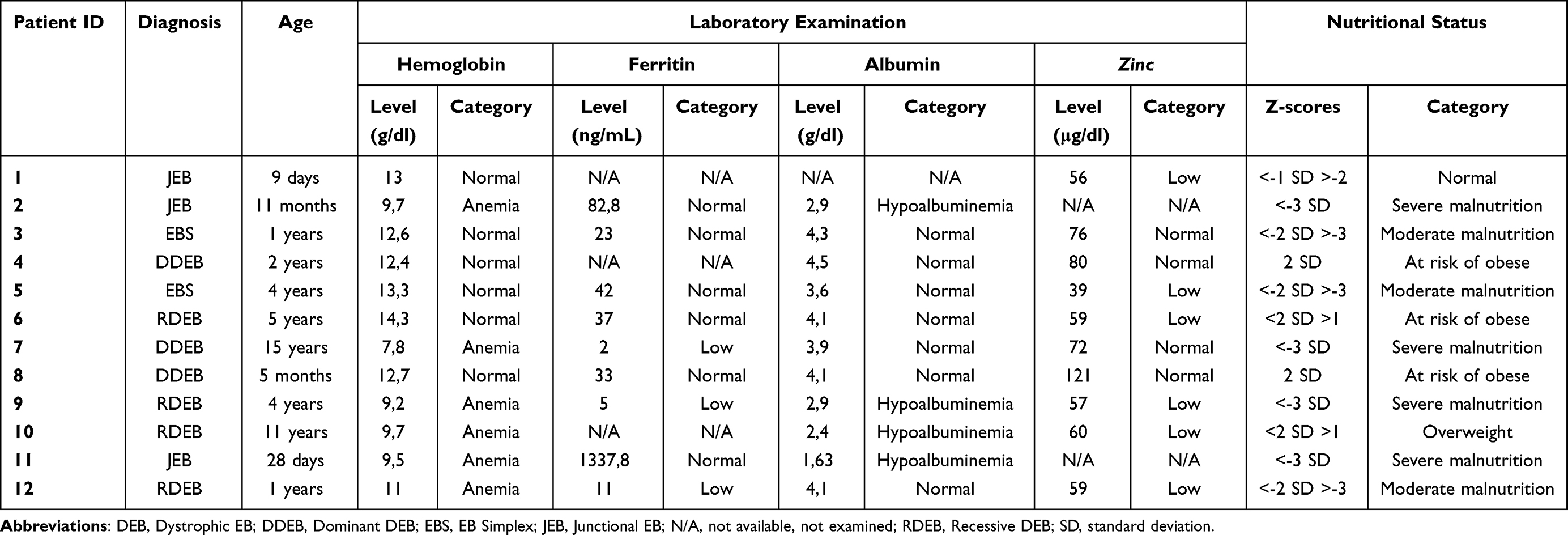 |
Table 2 Laboratory and Nutritional Status in Pediatric EB Patients |
Discussion
According to the literature, the most common type of EB is EBS.1 This study found that the most common type of EB in a Tertiary Referral Hospital in West Java, Indonesia, was RDEB, followed by DDEB, JEB, and EBS. Morales-Olvera et al13 found that RDEB followed by DDEB was the common type of EB at The National Institute of Pediatrics, Mexico. Danescu et al4 also found that the most common type of EB was DEB which occurred in as many as 58 of 89 subjects. DEB was found to be the most common type of EB in previous studies due to the fact that other EB patients were not diagnosed by dermatologists due to limitations in the data registry.4 The result shown in this study is presumably because DEB patients who seek treatment were already in severe condition. In addition, low socioeconomic status, low awareness of medical care, and low education of EB in Indonesia might lead to undiagnosed EB, and therefore accurate data cannot be obtained.
Clinical factors influencing nutritional status were skin,9 gastrointestinal, and extraintestinal involvement.2 Wound assessment of EB can be done based on the body surface area or affected BSA.9 The largest EB wound lesion area was 10–20%, found in 8 patients. The largest percentage of infected EB wound lesions was <10%, found in 8 patients. This is in accordance with the study by Zidorio et al14 who reported in their study that the largest EB wound lesion area was <10% in 8 patients. Skin involvement and infected skin in pediatric EB patients were spontaneous or caused by friction or trauma.3 Persistent friction and trauma might lead to secondary infections.1
The most frequent gastrointestinal manifestations found in this study were tooth decay, odynophagia, and oral blisters. Tooth decay was observed in 6 patients with RDEB and JEB. This condition may cause difficulty in chewing, resulting in decreased nutritional intake and calories, as well as decreased nutritional status in EB patients.2 Oral blisters and odynophagia were found in 5 patients. The buccal mucosa, tongue, palate, and pharynx are the most frequently affected mucosa in RDEB.15 The presence of bullae and erosions in the oral cavity may cause pain when eating and drinking,16 while complaints of acute dysphagia16 were not found in patients with bullae and erosions on the oral mucosa. These may cause inadequate intake and further affect nutritional status in EB patients.2
Hand deformity was found in 1 patient as an extraintestinal involvement in this study. The deformity is caused by repeated hand injuries leaving progressive scarring tissue which can become quite extensive. Pseudosyndactyly is a hand deformity in EB patients that results from a closure of the digits in a “mitten” of skin. EB patients who have progressive scarring of the hand may develop flexion contracture14 which disturbs eating, resulting in decreased food intake.2 This study found that all EB patients felt pain, especially when changing dressings. Poor nutritional status in EB patients can affect the severity of pain.2
The most common laboratory abnormalities in this study were anemia and low zinc levels. In this study, half of the pediatric EB patients were anemic. The incidence of anemia in this study is consistent with a previous study,17 which reported that anemia was more common in JEB and RDEB. The cause of anemia in pediatric EB patients is thought to be due to the chronicity of the disease17 that appears in 2 of 6 EB patients with anemia who have had EB for 11–15 years. In addition, anemia in this study may be caused by extensive skin lesions that may cause chronic bleeding. Decreased intake of high-iron foods, such as meat, liver, and green vegetables (spinach, kale, and broccoli) might also be contributory.2 Six out of 10 pediatric EB patients were found to have low zinc levels (1 EBS patient, 1 JEB patient, and 4 RDEB patients). The presence of zinc deficiency may lead to impaired wound healing due to decreased activation of nuclear factor (NF)-κβ, proinflammatory cytokines such as IL1β, tumor necrosis factor (TNF)-α, and neutrophil infiltration during the early wound healing process.18 The cause of the decreased zinc levels in pediatric EB patients in this study is thought to be due to a decrease in the intake of foods high in zinc, such as breast milk in patients who were still breastfeeding, as well as meat, fish, and shellfish in patients who had received solid food.19 These might be caused by a disturbance in eating due to mouth blisters and odynophagia.
The WHO recommends using the Z-scores threshold system that can be found on growth charts to assess nutritional status.20 In this study, severe malnutrition was found in 4 patients (2 JEB, 1 RDEB patient, and 1 DDEB patient) while moderate malnutrition was observed in 3 patients (2 EBS and 1 DEB patient). This is in line with a study conducted by Morales-Olvera et al13 who reported that the frequency of malnutrition was high in EB patients (82.3%). Their study found that RDEB and JEB patients frequently had chronic malnutrition, wasting, and stunting. A study by Birge21 also found that 27 out of 35 DEB patients (77%), 4 of 7 JEB patients (57%), and 4 out of 18 EBS patients (22%) had a risk of malnutrition. Nutritional balance in EB patients is one of the components of comprehensive management in pediatric EB patients.22 Assessment of nutritional status and early nutritional interventions affect nutritional intake in pediatric EB patients.23 In addition, optimal nutrition can improve nutritional status,21 reduce morbidity and mortality,23 increase growth and development,24 improve clinical manifestations,25 promote healing, decrease susceptibility to infection, and improve the quality of life of pediatric EB patients.23
This study was not without its limitations. One limitation lies in the fact that the medical records of pediatric EB patients were not completed thoroughly and in detail, resulting in missing or unavailable data. Medical records of EB patients should be completed, so data can be obtained accurately. This is particularly important since EB is a rare condition.
Conclusion
Based on the results of this study, it can be concluded that the clinical features and laboratory findings of RDEB, as the most commonly found type of EB in our pediatric cohorts, contribute to their nutritional status–in this case, moderate and severe malnutrition. Clinical features of RDEB that contribute to nutritional status include wounds on the skin, tooth decay, hand deformity, and pain when changing dressings. Laboratory findings that contribute to the nutritional status of pediatric EB patients include anemia and low zinc levels. The findings of this study are expected to be useful as baseline data for further studies, including prospective evaluations of nutritional status to the clinical symptoms and nutrition, as well as the quality of life of pediatric EB patients.
Ethics Approval
This study was conducted in compliance with the Declaration of Helsinki, Good Clinical Practices, and local regulatory requirements, and was approved by the Medical Ethics Committee of Hasan Sadikin General Hospital Bandung (approval number: LB.02.01/X.2.2.1/15095/2020).
Acknowledgments
The author would like to thank all of the Dermatology and Venereology Department staff, Faculty of Medicine, Universitas Padjadjaran – Dr. Hasan Sadikin General Hospital.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Paller AS, Mancini AJ. Bullous disorders of childhood. In: Paller AS, Mancini AJ, editors. Hurwitz Clinical Pediatric Dermatology.
2. Salera S, Tadini G, Rossetti D, et al. A nutrition-based approach to epidermolysis bullosa: causes, assessments, requirements, and management. Clin Nutr. 2020;39(2):343–352. doi:10.1016/J.CLNU.2019.02.023
3. Fine JD, Melleria JE. Epidermolysis bullosa. In: Bolognia JL, Schaffer JV, Cerroni L, editors. Dermatology.
4. Danescu S, Has C, Senila S, Ungureanu L, Cosgarea R. Epidemiology of inherited epidermolysis bullosa in Romania and genotype-phenotype correlations in patients with dystrophic epidermolysis bullosa. J Eur Acad Dermatol Venereol. 2015;29(5):899–903. doi:10.1111/JDV.12709
5. McGrath JA. Genetic blistering diseases. In: Griffiths CEM, Barker J, Bleiker T, Chalmers R, Creamer D, editors. Rook’s Textbook of Dermatology.
6. Fine JD. Epidemiology of inherited epidermolysis bullosa based on Incidence and prevalence estimates from the national epidermolysis bullosa registry. JAMA Dermatol. 2016;152(11):1231–1238. doi:10.1001/JAMADERMATOL.2016.2473
7. Ingen-Housz-Oro S, Blanchet-Bardon C, Vrillat M, Dubertret L. Vitamin and trace metal levels in recessive dystrophic epidermolysis bullosa. J Eur Acad Dermatol Venereol. 2004;18(6):649–653. doi:10.1111/J.1468-3083.2004.01067.X
8. Denyer J, Pillay E. Best practice guidelines for skin and wound care in epidermolysis bullosa. An international consensus. Wound International; 2017. Available from: https://af13d689-15eb-4199-8733-e91a7bb8ae3f.usrfiles.com/ugd/af13d6_01ed147ab87e49c584c20a917c47f19f.pdf.
9. Haynes L. Clinical practice guidelines for nutrition support in infants and children with epidermolysis bullosa (EB). Including THINC (Tool to Help Identify Nutritional Compromise in EB). Great Ormond street hospital. International Consensus. DEBRA; 2007. Available from: https://www.debra.org.uk/downloads/community-support/eb-clinical-practice-guidelines-nutrition-in-children-100613.pdf.
10. Lin PH, Sermersheim M, Li H, Lee PHU, Steinberg SM, Ma J. Zinc in wound healing modulation. Nutrients. 2017;10(1):16. doi:10.3390/NU10010016
11. Wright JA, Richards T, Srai SKS. The role of iron in the skin and cutaneous wound healing. Front Pharmacol. 2014;5:156. doi:10.3389/FPHAR.2014.00156
12. Sindgikar V, Narasanagi B, Ragate A, Ahmed Patel F. Effect of serum albumin in wound healing and its related complications in surgical patients. Al Ameen J Med Sci. 2017;10(2):132–135.
13. Morales-Olvera D, Gris-Calvo JI, Garcia-Romero MT. Nutritional status of pediatric patients with epidermolysis bullosa. A cross-sectional study. Nutr Clin Diet Hosp. 2022;42(1):146–151. doi:10.12873/421garcia-romero
14. Zidorio APC, Dutra ES, Leão DOD, Costa IMC. Nutritional aspects of children and adolescents with epidermolysis bullosa: a literature review. An Bras Dermatol. 2015;90(2):217–223. doi:10.1590/ABD1806-4841.20153206
15. Marinkovich M. Inherited Epidermolysis. In: Kang S, Amagai M, Bruckner A, editors. Fitzpatrick’s Dermatology.
16. Houghton LA, Parnell WR, Thomson CD, Green TJ, Gibson RS. Serum zinc is a major predictor of anemia and mediates the effect of selenium on hemoglobin in school-aged children in a nationally representative survey in New Zealand. J Nutr. 2016;146(9):1670–1676. doi:10.3945/JN.116.235127
17. Hwang SJE, Daniel BS, Fergie B, Davey J, Murrell DF. Prevalence of anemia in patients with epidermolysis bullosa registered in Australia. Int J Womens Dermatol. 2015;1(1):37–40. doi:10.1016/J.IJWD.2014.12.001
18. Lim Y, Levy M, Bray TM. Dietary zinc alters early inflammatory responses during cutaneous wound healing in weanling CD-1 mice. J Nutr. 2004;134(4):811–816. doi:10.1093/JN/134.4.811
19. Yan A. Cutaneous changes in nutritional disease. In Kang S, Amagai M, Bruckner A, editors. Fitzpatrick’s Dermatology.
20. Seetharaman N, Chacko T, Shankar S, Mathew A. Measuring malnutrition - the role of Z scores and the composite index of anthropometric failure (CIAF). Indian J Com Med. 2007;32(1):35–39. doi:10.4103/0970-0218.53392
21. Birge K. Nutrition management of patients with epidermolysis bullosa. J Am Diet Assoc. 1995;95(5):575–579. doi:10.1016/S0002-8223(95)00157-3
22. Cohn HI, Teng JMC. Advancement in management of epidermolysis bullosa. Curr Opin Pediatr. 2016;28(4):507–516. doi:10.1097/MOP.0000000000000380
23. Lechner‐Gruskay D, Honig PJ, Pereira G, McKinney S. Nutritional and metabolic profile of children with epidermolysis bullosa. Pediatr Dermatol. 1988;5(1):22–27. doi:10.1111/J.1525-1470.1988.TB00879.X
24. Allman S, Haynes L, MacKinnon P, Atherton DJ. Nutrition in dystrophic epidermolysis bullosa. Pediatr Dermatol. 1992;9(3):231–238. doi:10.1111/J.1525-1470.1992.TB00337.X
25. Kim KY, Namgung R, Lee SM, et al. Nutritional outcomes in children with epidermolysis bullosa: the experiences of two centers in Korea. Yonsei Med J. 2014;55(1):264–269. doi:10.3349/YMJ.2014.55.1.264
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.