Back to Journals » Journal of Inflammation Research » Volume 18
A Retrospective Observational Analysis of Factors Determining the Formation of Pressure Ulcers in ICU Patients Treated for COVID-19
Authors Woźniak A ![]() , Janc J
, Janc J ![]() , Leśnik P, Słabisz N, Uchmanowicz I
, Leśnik P, Słabisz N, Uchmanowicz I ![]()
Received 22 February 2025
Accepted for publication 19 July 2025
Published 29 August 2025 Volume 2025:18 Pages 11883—11894
DOI https://doi.org/10.2147/JIR.S524364
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Anna Woźniak,1 Jarosław Janc,2 Patrycja Leśnik,3 Natalia Słabisz,4 Izabella Uchmanowicz1
1Department of Nursing and Midwifery, Wroclaw Medical University, Wroclaw, Poland; 2Department of Anaesthesiology and Intensive Therapy, Hospital of the Ministry of the Interior and Administration, Wroclaw, Poland; 3Department of Microbiology, Wroclaw Medical University, Wroclaw, Poland; 4Department of Laboratory Diagnostics, 4th Military Clinical Hospital, Wroclaw, Poland
Correspondence: Anna Woźniak, Department of Nursing and Midwifery, Wroclaw Medical University, Bartla 5 Street, Wroclaw, 51-618, Poland, Email [email protected]
Background: Critically ill COVID-19 patients are at heightened risk for pressure ulcers (PUs), with the pandemic altering both the frequency and location of PU development and challenging hospital preparedness. The study aimed to investigate clinical and demographic factors associated with PUs in critically ill COVID-19 patients, compared outcomes between those who did and did not develop PUs, and assessed the impact of septic shock, prone positioning, and other interventions on PU formation, prolonged hospitalization, and mortality.
Materials and Methods: A retrospective analysis was conducted on 160 adults with lab-confirmed COVID-19 treated in the intensive care unit (ICU) of the 4th Military Clinical Hospital in Wroclaw (Poland) between September 2020 and September 2022. The criterion for inclusion in the study was confirmed COVID-19 disease and need for invasive ventilation. Demographic data, incidence of septic shock, use of the Extracorporeal Membrane Oxygenation (ECMO), prone positioning, colonization, survival rates, SAPS (Simplified Acute Physiology Score) II scores, and vasopressor (argipressin) requirements were recorded. Univariate and multivariate logistic regression identified significant predictors of PUs development.
Results: PUs occurred in 48.12% (n=77) of patients. Septic shock was more prevalent among those with PUs (30.12% vs 16.88%, p=0.049). PUs group had higher mean SAPS II scores (56.40) and greater argipressin use (0.50 units, p=0.015). Length of stay was significantly longer for patients with PUs (mean=14.08 days, p< 0.001). Multivariate analysis showed that higher SAPS II scores, argipressin use, and extended hospitalization were independent risk factors, while 28-day survival was protective against PUs formation.
Conclusion: PUs development in critically ill COVID-19 patients is strongly linked to disease severity, vasopressor requirements, and prolonged hospitalization. Targeted preventive measures focusing on these risk factors could help mitigate PUs incidence and improve patient outcomes.
Keywords: pressure ulcers, COVID-19, SAPS II, prone positioning, septic shock, argipressin
Introduction
Pressure ulcers (PUs) are one of the serious complications in critically ill patients hospitalized in intensive care units. Circulatory and respiratory disorders, malnutrition, limited mobility, significantly increase the risk of skin damage, which is pointed out by expert groups dealing with the problem of PUs. This ailment is observed in most health care systems around the world.1 High costs of treatment prompt the analysis of the phenomenon and the search for new structured solutions aimed at reducing their occurrence.2
According to the World Health Organization (WHO), PUs affect 5 to 10% of patients hospitalized in intensive care units, with a significantly higher risk in critically ill people due to their general condition and concomitant conditions (WHO 2021). A study by Smith and colleagues indicates that as many as 40% of ICU patients develop PUs within the first 14 days of hospitalization.3
The time of treatment of patients for COVID-19 slightly changed the image of the PU phenomenon, in the number and place of their formation, approach to the problem, which forced additional solutions for which hospitals were not prepared at that time. All strength was devoted to the treatment of the underlying disease, which resulted in the fact that a small group of patients received appropriate PUs prophylaxis. Patients placed in the prone position were exposed to pressure in the particularly sensitive area of the face and knee, covered with a small amount of subcutaneous tissue. In addition, anatomical conditions, disturbed circulation, distribution of load in these areas intensified the problem. A well-thought-out action aimed at reducing the pressure on this particular area should be one of many elements of management in patients with confirmed self-care dysfunction.
The biological mechanisms linking clinical factors to PUs risk are complex and result from interactions between mechanical, physiological and molecular factors. The authors of many publications draw attention to the multifactorial pathogenesis of skin damage at the end of life, classifying and define wounds as “unavoidable”.4 It should be noted that the study group did not only concern elderly patients, nor were they people with multimorbidity.
In the case of patients with COVID-19, the worsening critical condition progressed at a very rapid pace: respiratory disorders, hypoxia, circulatory disorders, including perfusion. In addition to standard procedures, it required the implementation of forced positioning of patients in a forced position on the stomach without the possibility of repositioning, which was a significant risk factor.5 The prone position has become a key element in the fight for survival of patients during respiratory therapy, often taking the lead or accompanying pharmacological treatment. However, the effectiveness of the prone position is linearly dependent on the length of its application. According to the guidelines of the WHO, NIH, EDCD, PTChP, SCCM it is from 12 to 24 hours in cycles for 3 to 7 days.6
A higher degree of disease severity measured by available scales (APACHE II, SAPS II, SOFA, GCS), laboratory biomarkers, doses of vasoactive drugs and prolonged hospitalization time have a significant impact on the formation of PU.
It is widely believed that more than 80% of incidents can be avoided by early detection of threat.7 Prevention of in-hospital acquired PUs reduces patient harm and healthcare costs. Domestic and foreign initiatives help healthcare professionals focus on key activities and have ready-made solutions in relation to reducing the occurrence of PU. All patients admitted to hospital should have a risk assessment using an appropriate scale within six hours of admission and every day thereafter, and those at risk should be given an adjusted regimen. ICU patients undergoing sedation treatment do not report symptoms of deep tissue injury, which significantly hinders prevention in the prevention of PUs.7
Early identification of people at risk of PUs and the implementation of preventive programs are recommended by national and global experts dealing with the prevention and treatment of wounds. Actions such as: relieving, repositioning, maintaining proper circulation, breathing, nutrition, and eliminating infections are key defensive measures.8 These activities are also the basis for keeping the patient in a stable and safe state at every stage of the underlying disease.
The primary objective of this study was to investigate the clinical and demographic factors associated with the development of PUs in critically ill patients. Specifically, the study aimed to compare the clinical outcomes, severity of illness, and interventions between patients who developed PUs and those who did not. Additionally, the study sought to assess the impact of septic shock, prone positioning, and other clinical interventions on the development of PUs, as well as their association with prolonged hospitalization and mortality.
Materials and Methods
Participants and Settings
Adult patients with clinical symptoms and lab-confirmed COVID-19 infection (irrespective of gender) who were treated in the ICU of the 4th Military Clinical Hospital in Wroclaw (Poland) during the period from September 2020 to September 2022 were enrolled in the present study. The study group consisted of 160 individuals, with a predominance of male patients (65%, n = 104), while females represented 35% (n = 56).
The criterion for inclusion in the study was confirmed COVID-19 disease and need for invasive ventilation; the severity of the disease was analyzed on the basis of laboratory tests, drugs used, treatment methods, scales used. We monitored PUs using their medical records: Pressure Ulcer Monitoring Cards, Waterlow Pressure Ulcer Risk Assessment tools, current medical history, and medical history. The data collected and analyzed on an ongoing basis by the authors of the article.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethics Committee at The Military Medical Chamber in Warsaw, Poland (approval no.: KB–3/21, approval date: 21.05.2021). Informed and written consent was obtained from all patients. The standards for Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) were followed.
Measured Outcomes
The following clinical and demographic variables were analyzed: age, height, weight, BMI; clinical severity scores (APACHE II, SAPS II, SOFA, GCS); inflammatory and organ function biomarkers (CRP, procalcitonin, leukocytes, albumin, lactate, bilirubin, creatinine, urea); metabolic control variables (maximum and minimum blood glucose levels); indicators of renal function (daily urine output); vasoactive drug dosages (norepinephrine, argipressin, adrenaline); other therapeutic interventions (loop diuretics dosage, prone positioning, ECMO use); clinical conditions (sepsis, septic shock); infection and colonization status; lactate category; 28-day and overall survival rates; and duration of ICU hospitalization.
Also, the analysis included clinical conditions (sepsis, septic shock); 28-day survival and overall survival; use of ECMO and prone positioning; infection and complications; lactate – septic shock category (<2mmol/l vs ≥2mmol/l). In our study, we used prone position for 16 hours a day for 3 to 5 days.
Statistical Analysis
Sample size. Prior to data collection, a sample size estimation was conducted based on the primary objective of identifying factors associated with the development of PUs in critically ill patients hospitalized in the ICU. Assuming an expected incidence of PUs of approximately 30% among ICU patients, a confidence level of 95%, and a statistical power of 80%, it was determined that a minimum of 140 participants would be required to detect significant associations with relevant clinical predictors. Accordingly, the final sample of 160 patients included in this study was deemed sufficient to achieve the study objectives and support robust multivariate logistic regression analysis.
Statistical analysis. Descriptive statistics were used to summarize the characteristics of the study population. Continuous variables are presented as means and standard deviations (SD) for normally distributed data, and as medians with interquartile ranges (Q1, Q3) for non-normally distributed data. The normality of the distribution was assessed using the Shapiro–Wilk test. Categorical variables are presented as counts and percentages. The dataset was examined for missing values. Variables with substantial missingness (>10%) were excluded from the analysis. For the purposes of multivariate analysis, single imputation was applied for variables with less than 10% missing data (using the median for continuous variables and the mode for categorical variables). However, in descriptive and univariate analyses, no imputation was performed; hence, sample sizes may vary slightly across variables. To compare categorical variables between groups (eg, gender, sepsis, septic shock, survival), the chi-square test (Pearson chi-square) was employed. For continuous variables (eg, age, BMI, clinical scores, laboratory biomarkers), comparisons between the two groups (patients with and without PUs) were performed using the Mann–Whitney U-test, as the majority of variables did not meet the assumptions of normal distribution. A p-value of less than 0.05 was considered statistically significant. All statistical analyses and visualizations were conducted using Python (version 3.11.2), ensuring reproducibility and transparency in the analysis.
Data visualizations were created using both matplotlib and seaborn for static plots, and plotly for interactive visualizations. Matplotlib and seaborn were used for generating histograms, box plots, and scatterplots to illustrate the distribution and relationships of the continuous variables, while plotly was employed for interactive graphs to enhance data presentation.
The analysis conducted a multivariate logistic regression aimed at estimating the effect of selected variables on the risk of PUs. The Maximum Likelihood Estimation (MLE) method was used to estimate the model parameters. The model included variables selected based on univariate regression analysis, where variables with a p-value < 0.3 were included in the multivariate model.
Results
The incidence of septic shock occurred in 23.75% (n = 38) of the patients, while 76.25% (n = 122) did not experience this condition. The survival rate after 28 days was 27.5% (n = 44), with 72.5% (n = 116) of patients not surviving. Overall survival during the study period was recorded at 26.25% (n = 42), while 73.75% (n = 118) of patients did not survive. ECMO (Extracorporeal Membrane Oxygenation) was implemented in 6.37% of cases (n = 10), whereas 93.63% (n = 147) did not require ECMO. Prone positioning was applied to 45.22% (n = 71) of patients, while 54.78% (n = 86) did not undergo this intervention. Colonization was observed in 15.62% of patients (n = 25), with the remaining 84.38% (n = 135) not showing colonization. PUs were present in 48.12% of patients (n = 77), and 51.88% (n = 83) were free of PUs (Table 1).
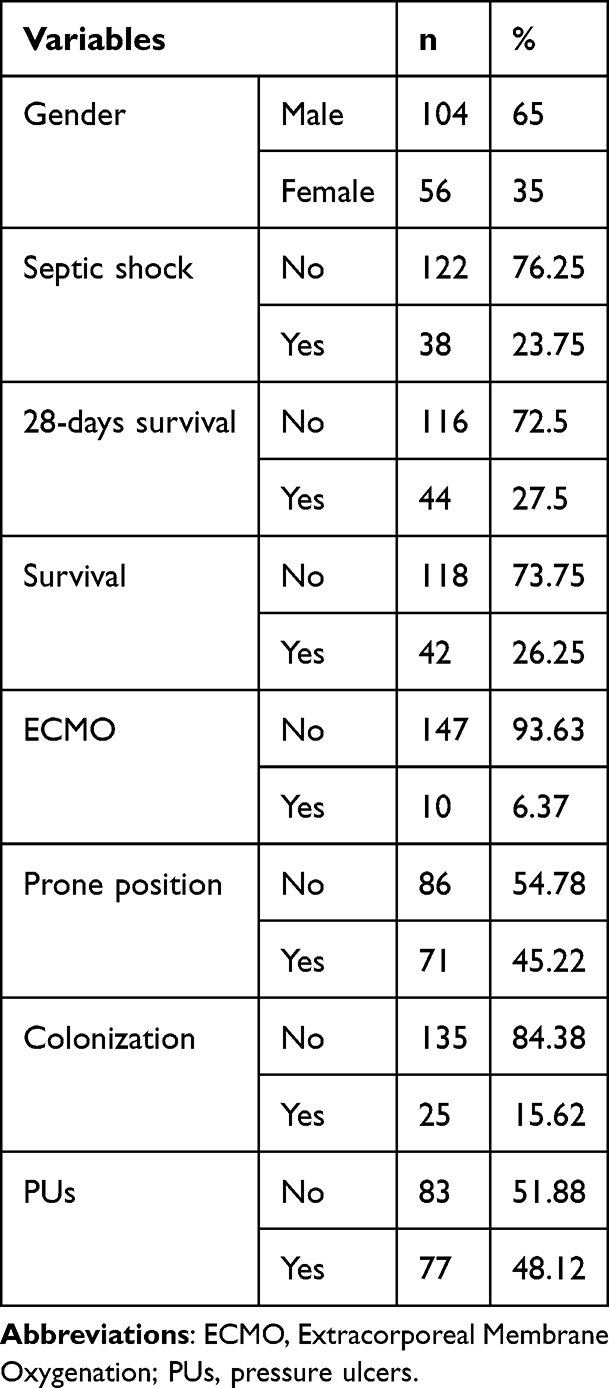 |
Table 1 Characteristics of the Study Group |
Table 2 includes a set of quantitative variables measured within the study group. The summary statistics provided for each variable include the mean, standard deviation (SD), minimum (Min), first quartile (Q1), median (Me), third quartile (Q3), and maximum (Max) values, giving a comprehensive overview of the distribution and range for each measured parameter across the study population (Table 2).
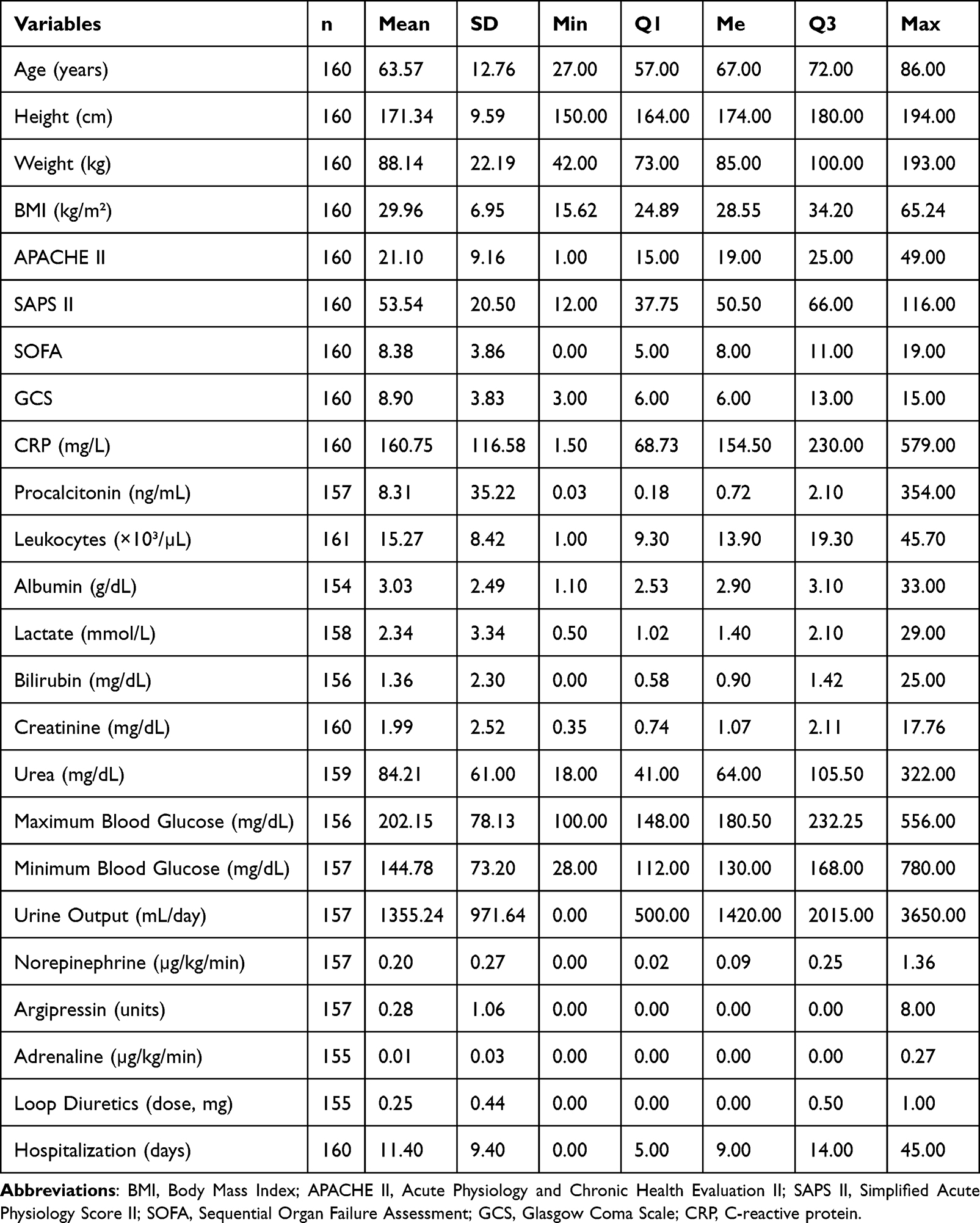 |
Table 2 Descriptive Statistics of Quantitative Variables in the Study Group |
Table 3 compares the distribution of several key clinical and demographic variables between two groups of patients: those who did not develop PUs (Group without PUs) and those who did (Group with PUs). The analysis includes gender, septic shock, 28-day survival, overall survival, use of ECMO, prone position, colonization, septic shock lactate category. The statistical significance of the differences between the two groups is evaluated using the Pearson chi-square test (p-value).
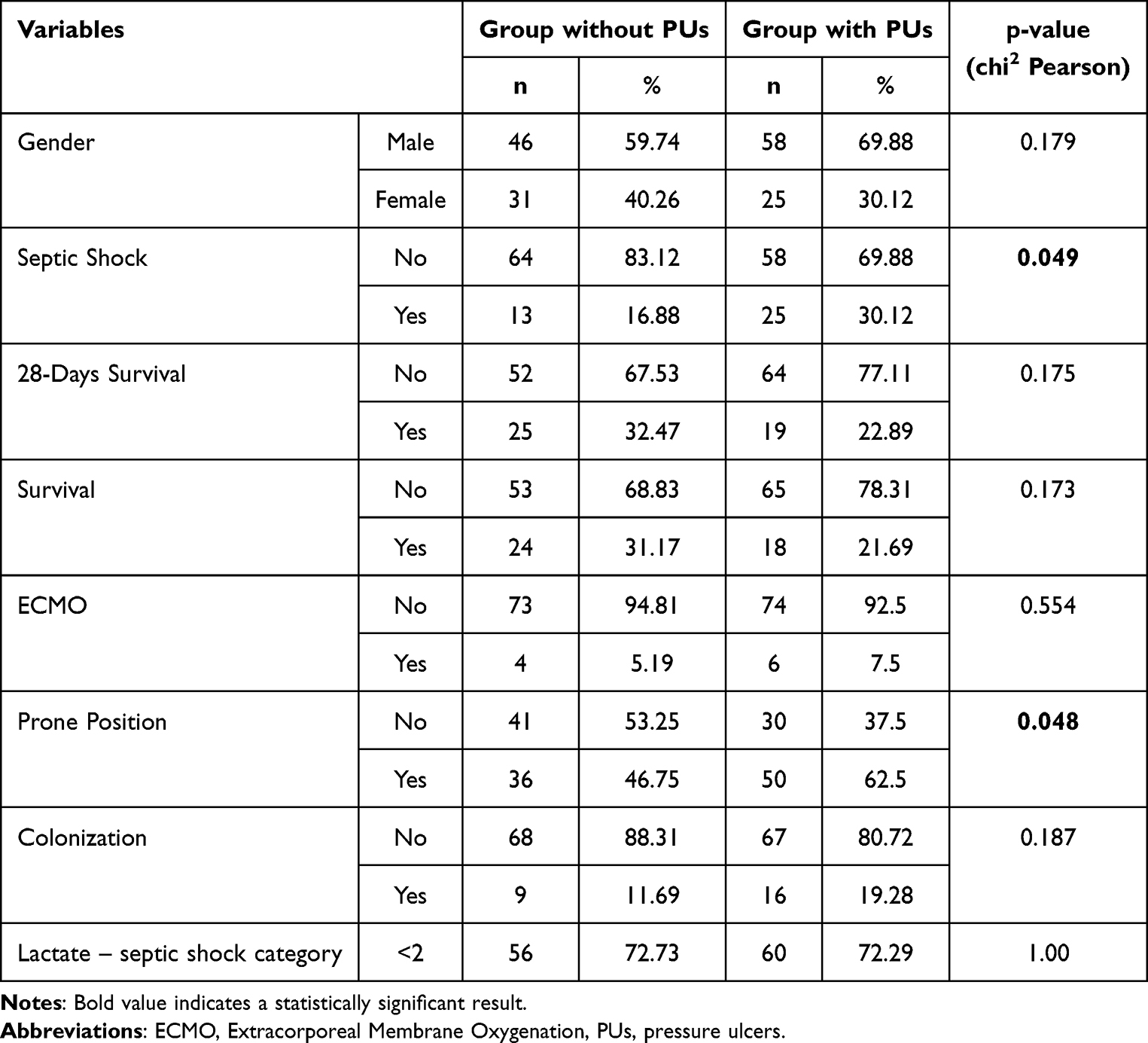 |
Table 3 Comparison of Group Characteristics Between Patients with and without PUs |
Statistically significant results are: (1) Septic Shock: The proportion of patients with septic shock was significantly higher in the group with PUs (30.12%) compared to the group without PUs (16.88%) (p = 0.049), indicating that septic shock may be more common in patients who develop PUs. (2) Prone Positioning: A significantly higher proportion of patients in the PU group (62.5%) underwent prone positioning compared to the group without PUs (46.75%) (p = 0.048). This suggests a potential relationship between prone positioning and the development of PUs.
The other variables, including gender, sepsis, 28-day survival, overall survival, ECMO use, colonization and lactate level, did not show statistically significant differences between the two groups.
Table 4 presents the comparison of quantitative variables between two groups of patients: those without PUs and those with PUs. Statistically significant results are: (1) SAPS II Score: patients with PUs had a significantly higher SAPS II score (mean = 56.40) compared to those without PUs (mean = 50.45), indicating a greater severity of illness in the PUs group (p = 0.034); (2) argipressin: the use of argipressin was significantly higher in the PUs group (mean = 0.50 units) compared to the group without PUs (mean = 0.05 units) (p = 0.015), suggesting a more frequent need for vasopressors in patients with PUs; (3) hospitalization duration: patients with PUs had significantly longer hospital stays (mean = 14.08 days) compared to those without PUs (mean = 8.51 days) (p < 0.001), highlighting the association between PUs and prolonged hospitalization; (4) other variables, such as age, height, weight, BMI, CRP, procalcitonin, leukocytes, urine output, and glucose levels, did not show statistically significant differences between the two groups.
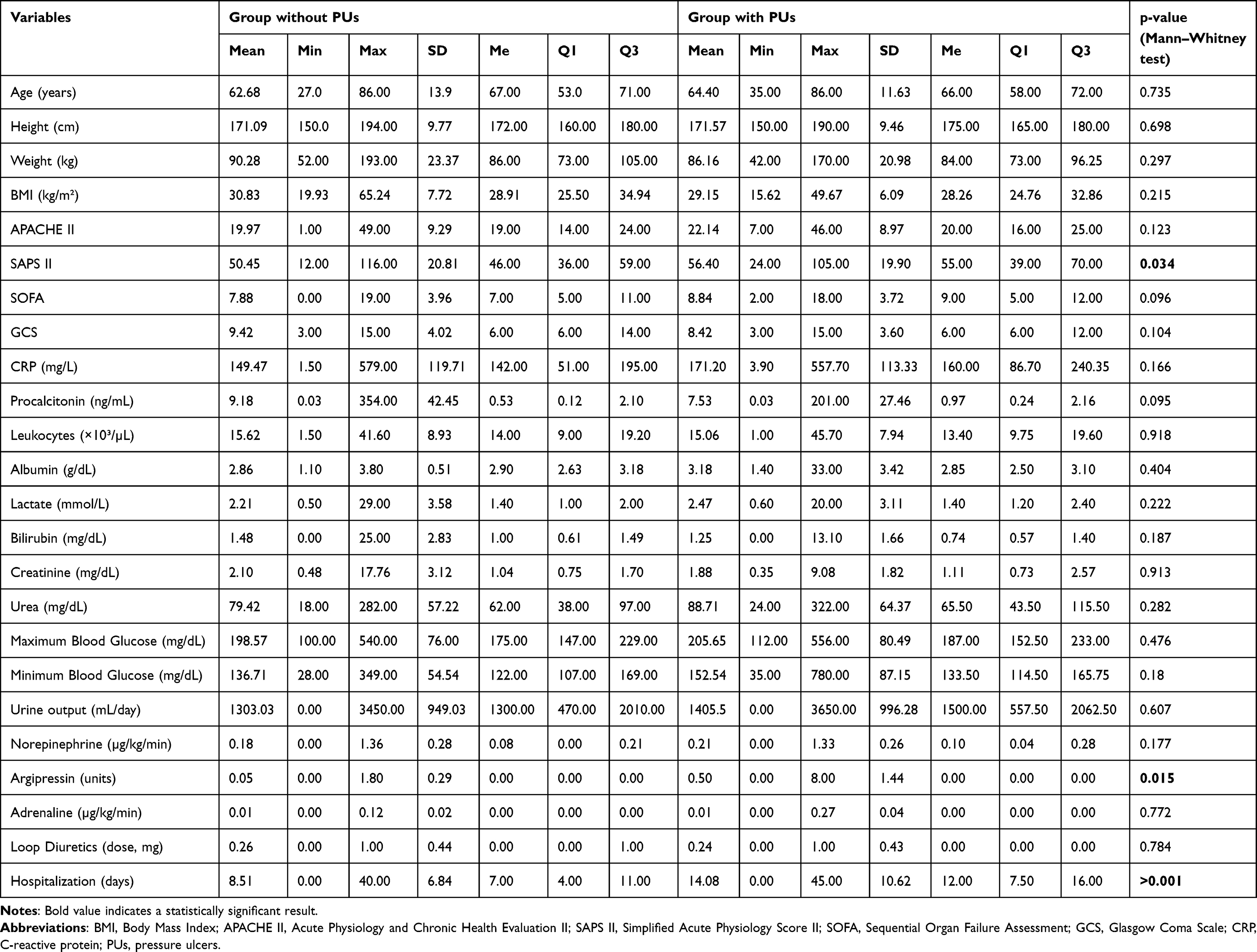 |
Table 4 Comparison of Quantitative Variables Between Patients with and without PUs |
In a univariate logistic regression analysis to assess risk factors for PUs, several variables were identified with p-values indicating potential statistical significance (p < 0.05) or close to statistical significance (Table 5). The analysis identified two statistically significant risk factors for PUs development: use of argipressin and length of hospitalization. Argipressin significantly increased the risk of developing PUs (OR = 2.22; 95% CI: 1.05–4.69; p = 0.036). Additionally, each extra day of hospitalization significantly raised the likelihood of PUs (OR = 1.09; 95% CI: 1.04–1.14; p = 0.001).
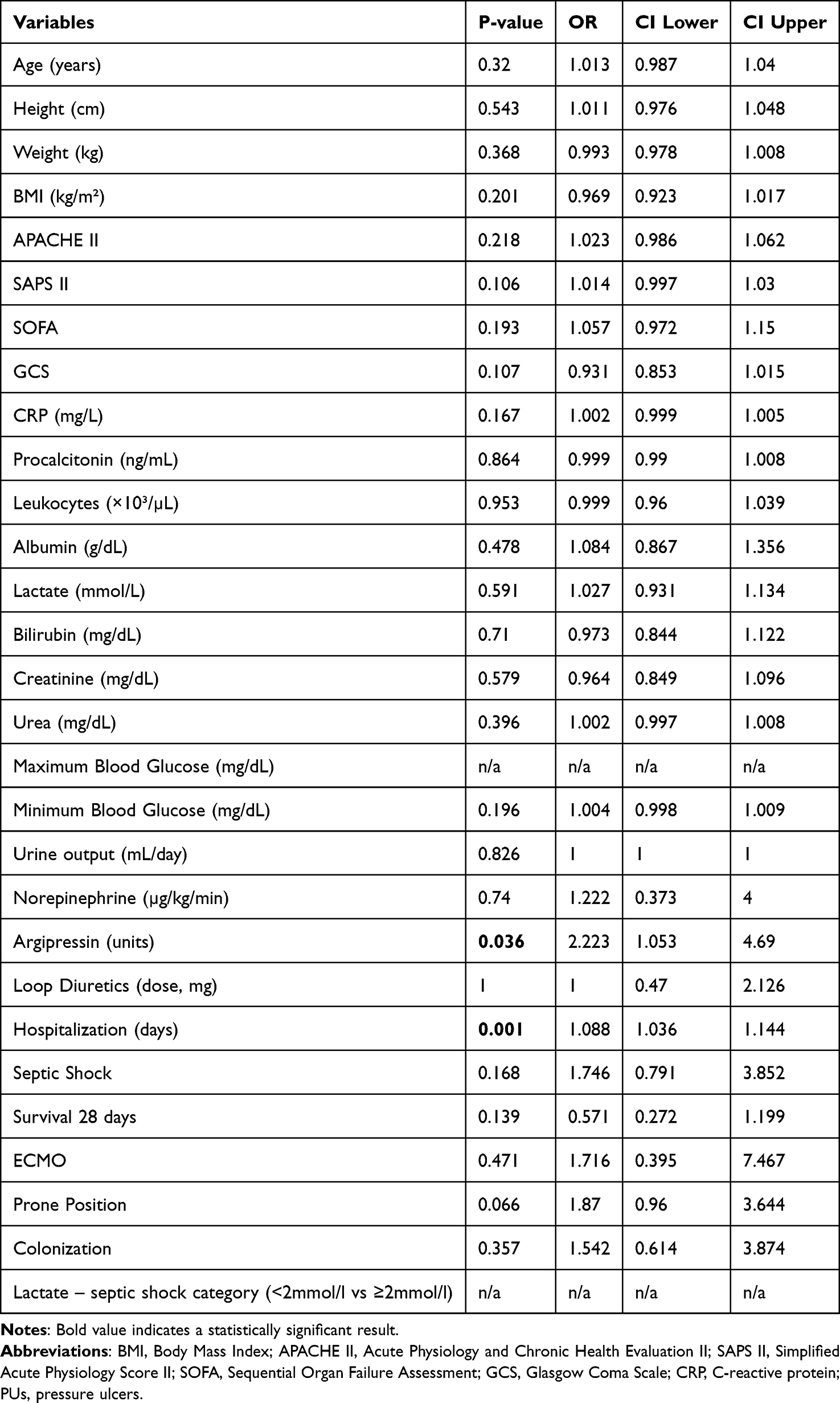 |
Table 5 Univariate Logistic Regression Analysis to Assess Risk Factors for PUs |
The following variables approached, but did not reach statistical significance: prone positioning, SAPS II score, and GCS. Patients placed in prone position showed a nearly doubled risk of PUs (OR = 1.87; 95% CI: 0.96–3.64; p = 0.066), indicating a potentially important clinical relationship worthy of further study. Additionally, higher SAPS II scores were slightly associated with increased PU risk (OR = 1.01; 95% CI: 1.00–1.03; p = 0.106). Lower GCS scores also showed a trend toward higher risk of developing PUs (OR = 0.93; 95% CI: 0.85–1.02; p = 0.107). While these findings were not statistically significant, their proximity to significance thresholds suggests that further investigation in larger studies may be warranted.
The association between CRP levels and PUs risk was not statistically significant (OR = 1.002; 95% CI: 0.999–1.005; p = 0.167). However, the direction of the association suggests that higher CRP levels might slightly increase the risk of developing PUs, warranting further exploration in future research with larger cohorts.
A univariate logistic regression analysis identified argipressin and hospitalization time as significant risk factors for PUs. In addition, variables such as prone position, SAPS II, GCS, and CRP showed p-values close to the significance threshold, which may suggest their role in the risk of PUs, but requires further verification in multivariate analyses.
In the logistic regression analysis, several factors significantly influenced PUs risk. Higher SAPS II scores significantly predicted increased PU risk (OR = 1.05; 95% CI: 1.01–1.09; p = 0.014), meaning each additional SAPS II point raised PU risk by approximately 5.3%. Argipressin use was also strongly associated with PU development, more than tripling the risk (OR = 3.37; 95% CI: 1.38–8.21; p = 0.008). Longer hospitalization was significantly related to higher PU risk, with each additional day increasing the risk by about 19% (OR = 1.19; 95% CI: 1.11–1.28; p < 0.001). Finally, patients surviving beyond 28 days showed a significantly reduced risk of developing PUs, indicating that improved clinical condition was protective (OR = 0.22; 95% CI: 0.06–0.79; p = 0.021).
The logistic regression analysis identified several variables approaching statistical significance. Higher BMI showed a trend toward slightly lower risk of PUs (OR = 0.94; 95% CI: 0.88–1.01; p = 0.116). Elevated CRP levels demonstrated a slight, though not statistically significant, increase in PUs risk (OR = 1.003; 95% CI: 0.999–1.007; p = 0.107). Additionally, prone positioning was associated with more than double the risk of PUs (OR = 2.14; 95% CI: 0.77–5.96; p = 0.132), suggesting clinical relevance that merits further investigation.
A multivariate logistic regression model showed that the most important factors associated with an increased risk of PUs were a higher SAPS II score, the use of argipressin and a longer duration of hospitalization. In addition, survival after 28 days was found to be a protective factor against PUs. Some variables, such as BMI, CRP or prone position, have shown trends close to significance and may require further analysis in larger research samples (Table 6).
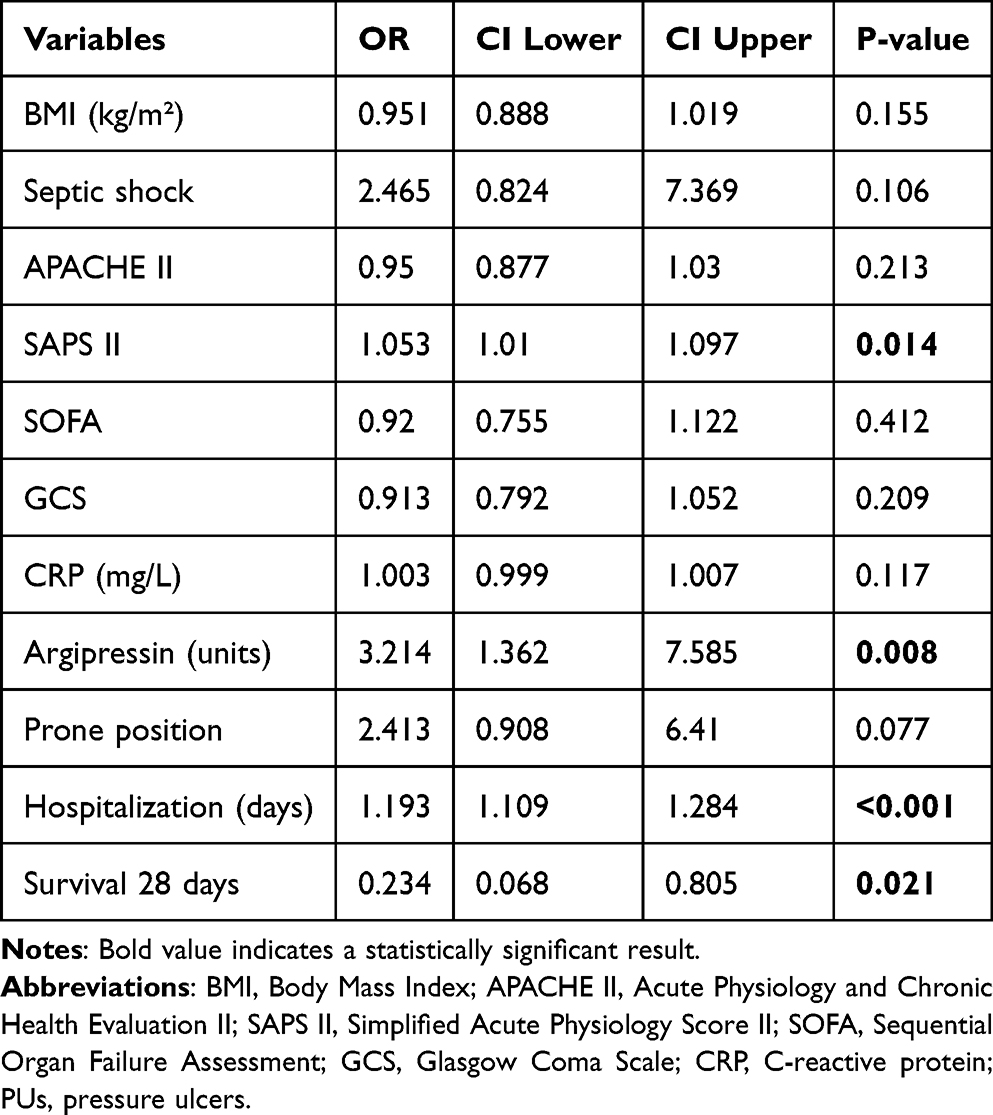 |
Table 6 Multivariate Logistic Regression Analysis to Assess Risk Factors for PUs |
Discussion
PUs represent a significant healthcare challenge, particularly in intensive care units (ICUs), where critically ill patients face multiple risk factors for their development. These wounds not only impact patient outcomes and quality of life but also substantially increase healthcare costs and resource utilization. Recent studies indicate that ICU-acquired PUs can increase hospital length of stay by an average of 4.3 days and add significant additional costs to patient care.9 Extended stay in the intensive care unit is additionally associated with an increased risk of hospital infection, including multidrug-resistant strains.10 This leads to an increased risk of death, the need for prolonged hospitalization, and the risk of complications.
The COVID-19 pandemic has introduced new challenges in PU prevention and management, particularly in critical care settings. The unique characteristics of COVID-19 patient care, including prolonged mechanical ventilation, prone positioning requirements, and complex hemodynamic support, have potentially altered the traditional risk profile for PUs development.11 Notably, the implementation of prone positioning as a crucial intervention for severe COVID-19 has introduced new anatomical areas at risk for pressure injury, particularly the face, anterior chest, and knees.12
Current literature suggests that ICU patients are particularly vulnerable to PUs development, with reported prevalence rates ranging from 6% to 18% in general ICU populations.13 However, these rates may be significantly higher in COVID-19 patients due to their complex care requirements. Multiple risk factors contribute to this increased vulnerability, including impaired tissue perfusion, prolonged immobility, altered consciousness, and the use of vasoactive medications.14
In our study a logistic regressions analysis identified argipressin use, high SAPS II score and hospitalization time as significant risk factors for PUs which is similar result to other studies.7,9,11,13,14
The pathophysiology of PU development in critically ill patients is multifaceted, involving both extrinsic and intrinsic factors. While mechanical forces such as pressure, shear, and friction play crucial roles, systemic factors including inflammation, hypoxemia, and altered tissue perfusion significantly contribute to tissue vulnerability.15 The COVID-19 disease process, characterized by severe inflammatory responses and endothelial dysfunction, may further exacerbate these pathophysiological mechanisms.
Prevention strategies have traditionally focused on regular repositioning, pressure redistribution surfaces, and skin assessment protocols. However, the implementation of these preventive measures has become more challenging in COVID-19 patients due to prone positioning requirements, staffing constraints, and the need for personal protective equipment.16 The European Pressure Ulcer Advisory Panel (EPUAP) guidelines emphasize the importance of risk assessment and preventive interventions, yet their application in COVID-19 patients often requires modification to accommodate specific care requirements. In our analysis, despite the fact that no statistical significance was found in the development of PU in the group of patients with prone positioning in the multivariate analysis, a higher risk of their development was shown in a simple demographic analysis and almost twice as high risk of their development in the univariate analysis. Due to the risk of PU in locations in the front part of the body (head, face, knees), it seems important to pay attention to this aspect of the care of patients with COVID-19. In the available literature, the use of the prone position technique increases the risk of PUs, mainly on the anterior parts of the body.6,17,18 In 2020, Moore et al12 pointed to the need for close observation, skin care and use of special dressings to reduce the risk of PU formation in this group of patients ie in the study of Yoshimura et al,19 the positive effect of the use of soft silicone, multilayered foam dressings and their effect on the reduction of PU in patients in prone position after neurosurgery was demonstrated.
Recent studies have highlighted the economic impact of hospital-acquired PUs, with estimated costs ranging from $20,900 to $151,700 per PU.20 In COVID-19 patients, these costs may be even higher due to extended hospital stays and additional care requirements. Understanding the specific risk factors and patterns of PU development in COVID-19 patients is crucial for developing targeted prevention strategies and optimizing resource allocation (22).
Despite existing research on PUs in critical care, there remains a significant knowledge gap regarding the specific risk factors and patterns of PU development in COVID-19 patients. The unique characteristics of COVID-19 patient care, including prolonged prone positioning and complex hemodynamic support, necessitate a detailed examination of PU risk factors in this population. This understanding is crucial for developing targeted prevention strategies and improving patient outcomes.
This study provides valuable insights into PU risk factors specific to COVID-19 ICU patients, contributing to the evolving body of knowledge in critical care medicine. These findings can inform evidence-based prevention strategies and resource allocation in critical care settings, potentially improving patient outcomes during current and future health crises.
Study Limitations
The main limitation of the study was the relatively small and single-center size of the study group. Future research directions should focus on prospective validation of these risk factors in larger, multicenter populations and the development of targeted preventive strategies. Additionally, investigation into the mechanistic relationships between identified risk factors and PU formation could enhance our understanding of tissue injury in critical illness.
Continuation of the study using the effective pronation position during the COVID-19 pandemic is quite difficult due to the rarity of the method. The study would require multicenter study in patients with severe respiratory failure covering a longer period of time.
Clinical Implications
These findings have substantial implications for clinical practice, suggesting the need for enhanced preventive strategies in patients with identified risk factors. The results support the implementation of comprehensive risk assessment protocols that specifically consider disease severity scores, vasopressor requirements, and anticipated length of stay. Furthermore, our findings indicate the importance of tailored preventive measures for patients requiring prone positioning or extended critical care support.
Conclusion
This study demonstrates that PU development in COVID-19 patients treated in intensive care units is influenced by multiple interrelated factors. Our findings reveal a notably high prevalence of PUs in this population, substantially exceeding typical rates reported in general intensive care settings. Through multivariate analysis, we identified several independent risk factors that significantly impact PU formation, notably higher SAPS II scores, argipressin administration, and extended hospitalization duration.
The strong association between disease severity, as measured by SAPS II scores, and PU development underscores the complex relationship between systemic illness and tissue vulnerability. The marked impact of argipressin use on PU formation suggests that hemodynamic support measures, while essential for patient survival, may compromise tissue perfusion and increase susceptibility to pressure injury. Furthermore, the correlation between extended hospitalization and PU development emphasizes the cumulative nature of tissue damage risk during critical illness.
Our analysis revealed an inverse relationship between 28-day survival and PU development, suggesting potential interactions between overall patient outcomes and tissue integrity. While prone positioning demonstrated a trend toward increased PU risk, this finding, though not achieving statistical significance in multivariate analysis, warrants careful consideration in clinical practice.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author.
Ethical Statement
The study was approved by the Bioethics Committee at The Military Medical Chamber in Warsaw, Poland (approval no.: KB–3/21, approval date: 21.05.2021).
Acknowledgments
There were no other contributors to the article than the authors as well as there was no writing assistance regarding our paper.
Funding
This study was not supported by the external fundings. The APC is funded from subvention for maintaining the research potential of the Faculty of Nursing and Midwifery, Wroclaw Medical University (Poland).
Disclosure
The authors declare no conflict of interest.
References
1. Vanderwee K, Clark M, Dealey C, Gunningberg L, Defloor T. Pressure ulcer prevalence in Europe: a pilot study. J Eval Clin Pract. 2007;13(2):227–235. doi:10.1111/j.1365-2753.2006.00684.x
2. Jacobson TM, Thompson SL, Halvorson AM, Zeitler K. Enhancing documentation of pressure ulcer prevention interventions: a quality improvement strategy to reduce pressure ulcers. J Nurs Care Qual. 2016;31(3):207–214. doi:10.1097/NCQ.0000000000000175
3. Smith G. Improved clinical outcomes in pressure ulcer prevention using the SEM scanner. J Wound Care. 2019;28(5):278–282. doi:10.12968/jowc.2019.28.5.278
4. VanGilder CA, Cox J, Edsberg LE, Koloms K. Pressure injury prevalence in acute care hospitals with unit-specific analysis: results from the international pressure ulcer prevalence (IPUP) survey database. J Wound Ostomy Continence Nurs. 2021;48(6):492–503. doi:10.1097/WON.0000000000000817
5. Venus K, Munshi L, Fralick M. Prone positioning for patients with hypoxic respiratory failure related to COVID-19. CMAJ. 2020;192(47):E1532–E1537. doi:10.1503/cmaj.201201
6. Priya V, Sen J, Ninave S. A comprehensive review of prone ventilation in the intensive care unit: challenges and solutions. Cureus. 2024;16(3):e57247. doi:10.7759/cureus.57247
7. Saindon K, Nguyen TD, Berlowitz DR. The 2021 update on pressure injuries: a review of the literature. Adv Skin Wound Care. 2022;35(8):422–428. doi:10.1097/01.ASW.0000834588.32255.0d
8. Langer G, Wan CS, Fink A, Schwingshackl L, Schoberer D. Nutritional interventions for preventing and treating pressure ulcers. Cochrane Database Syst Rev. 2024;2(2):CD003216. doi:10.1002/14651858.CD003216.pub3
9. Labeau SO, Afonso E, Benbenishty J, et al. Prevalence, associated factors and outcomes of pressure injuries in adult intensive care unit patients: the DecubICUs study. Intensive Care Med. 2021;47(2):160–169. doi:10.1007/s00134-020-06234-9
10. Woźniak A, Janc J, Łysenko L, et al. How to defeat multidrug-resistant bacteria in intensive care units. A lesson from the COVID-19 pandemic. prevention, reservoirs, and implications for clinical practice. Int J Med Sci. 2024;21(3):530–539. doi:10.7150/ijms.88519
11. Team V, Team L, Jones A, Teede H, Weller CD. Pressure injury prevention in COVID-19 patients with acute respiratory distress syndrome. Front Med Lausanne. 2021;7:558696. doi:10.3389/fmed.2020.558696
12. Moore Z, Patton D, Avsar P, et al. Prevention of pressure ulcers among individuals cared for in the prone position: lessons for the COVID-19 emergency. J Wound Care. 2020;29(6):312–320. doi:10.12968/jowc.2020.29.6.312
13. Cox J, Roche S. Vasopressors and development of pressure ulcers in adult critical care patients. Am J Crit Care. 2015;24(6):501–510. doi:10.4037/ajcc2015123
14. Lima Serrano M, González Méndez MI, Carrasco Cebollero FM, Lima Rodríguez JS. Risk factors for pressure ulcer development in intensive care units: a systematic review. Med Intensiva. 2017;41(6):339–346. doi:10.1016/j.medin.2016.09.003
15. Gefen A, Alves P, Ciprandi G, et al. Device-related pressure ulcers: SECURE prevention. J Wound Care. 2020;29(Sup2a):S1–S52. doi:10.12968/jowc.2020.29.Sup2a.S1
16. Wu J, Wang B, Zhu L, Jia X. Nurses’ knowledge on pressure ulcer prevention: an updated systematic review and meta-analysis based on the pressure ulcer knowledge assessment tool. Front Public Health. 2022;10:964680. doi:10.3389/fpubh.2022.964680
17. Ibarra G, Rivera A, Fernandez-Ibarburu B, Lorca-García C, Garcia-Ruano A. Prone position pressure sores in the COVID-19 pandemic: the madrid experience. J Plast Reconstr Aesthet Surg. 2021;74(9):2141–2148. doi:10.1016/j.bjps.2020.12.057
18. Girard R, Baboi L, Ayzac L, Richard JC, Guérin C. Proseva trial group. The impact of patient positioning on pressure ulcers in patients with severe ARDS: results from a multicentre randomised controlled trial on prone positioning. Intensive Care Med. 2014;40(3):397–403. doi:10.1007/s00134-013-3188-1
19. Yoshimura M, Ohura N, Santamaria N, Watanabe Y, Akizuki T, Gefen A. High body mass index is a strong predictor of intraoperative acquired pressure injury in spinal surgery patients when prophylactic film dressings are applied: a retrospective analysis prior to the BOSS Trial. Int Wound J. 2020;17(3):660–669. doi:10.1111/iwj.13287
20. Padula WV, Delarmente BA. The national cost of hospital‐acquired pressure injuries in the United States. Int Wound J. 2019;16(3):634–640. doi:10.1111/iwj.13071
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cold Plasmamed Beam as a Supporting Treatment of Soft Tissue Injuries in Severe Covid-19 Patients: A Preliminary Report
Nguyen TX, Nguyen DH, Ho-Man TP, Bui VDA, Phan PN
Medical Devices: Evidence and Research 2022, 15:277-283
Published Date: 18 August 2022