Back to Journals » Infection and Drug Resistance » Volume 19
A Retrospective, Descriptive Analysis of MRSA Infections in a Low-Endemicity Region, Focusing on Empiric Treatment Adequacy
Authors Haapia T ![]() , Vuopio J, Oksi R, Vahlberg T, Silvola J, Kanerva M
, Vuopio J, Oksi R, Vahlberg T, Silvola J, Kanerva M
Received 18 August 2025
Accepted for publication 23 January 2026
Published 3 March 2026 Volume 2026:19 556192
DOI https://doi.org/10.2147/IDR.S556192
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Tiina Haapia,1 Jaana Vuopio,2– 4 Rasmus Oksi,1 Tero Vahlberg,5 Jaakko Silvola,2,3 Mari Kanerva,1 On behalf of the MRSA Study Group
1Infection Control Unit, Turku University Hospital, The Wellbeing Services County of Southwest Finland, Turku, Finland; 2Institute of Biomedicine, University of Turku, Turku, Finland; 3Clinical Microbiology Laboratory, Turku University Hospital, The Wellbeing Services County of Southwest Finland, Turku, Finland; 4Department of Public Health, Finnish Institute for Health and Welfare, Helsinki, Finland; 5Department of Biostatistics, University of Turku and Turku University Hospital, Turku, Finland
Correspondence: Tiina Haapia, Email [email protected]
Background: Previously, MRSA transmission and infections were mostly recognized as healthcare-associated. Community-associated MRSA (CA-MRSA) cases have become increasingly common, also in low-endemicity countries. Hence, also doctors in outpatient care encounter these patients. Despite increased general awareness on risk factors of MRSA carriage, it does not always influence clinical practice. As the total number of MRSA cases had increased in our region, it provoked us to analyze how this may have reflected the recognition of these infections and their empiric treatment adequacy in Hospital District of Southwest Finland (HDSWF).
Methods: All new MRSA cases detected between 2007 and 2016 in Hospital District of Southwest Finland were retrospectively analyzed. This single-center study describes MRSA carriers, whose carriage was first detected from a clinical specimen. The cases were recognized from the hospital’s MRSA registry, and their background data, including the antibiotic treatments given, were collected manually from electronic patient records.
Results: A total of 280 MRSA cases having an active clinical infection were detected. Skin and soft tissue infections (SSTIs) were the most common infection type (76%; 213/280 cases). Information on antibiotic treatments were obtained in 46.8% (131/280) of the cases. In 81.7% (107/131) of the cases, the empiric treatment did not cover MRSA. After adjusting the treatment according to susceptibility results, MRSA was ultimately covered in 49.3% (68/138) of the cases.
Conclusion: In low-endemicity settings, skin infections typically caused by S. aureus may be missed to being caused by a resistant pathogen, resulting in suboptimal or ineffective treatment. More awareness is needed to recognize the risk, to evaluate and possibly adjust the treatment.
Plain Language Summary: Based on our study findings, the possibility of an MRSA infection may be missed, and therefore the initial treatment is not optimally chosen in low-endemicity settings. Specimens from infection sites may be taken, but the subsequent treatment may still be ineffective against MRSA.
Keywords: meticillin-resistant Staphylococcus aureus, MRSA, MRSA infection, MRSA treatment
Introduction
Methicillin-resistant Staphylococcus aureus (MRSA) may merely cause colonization of the skin and mucous membranes and cause no harm to its host, but it can also cause recurrent and possibly life-threatening infections. Before 1990s, MRSA was recognized as a hospital-acquired pathogen and affected patients who had other comorbidities. Since 1990s, however, increasing numbers of infections are found in healthy individuals with no risk factors for an MRSA infection.1,2
Traditionally, MRSA cases have been classified as health-care associated (HA-MRSA) or community-associated (CA-MRSA) based on different features between the groups (eg patient risk factors, different strains causing the infections, different antibiotic susceptibilities, infection type etc).3 The barrier between these classifications has become more vague as the strains intermingle in the community, and the patients may not have any predisposing risk factors for an MRSA infection.2,4
Globalization plays its part in changing the risk profile for a possible MRSA carriage, since both refugees, asylum seekers and also travelling must be taken into account when assessing the risk for an MRSA infection.4–6 The guidelines for screening for possible MRSA carriage have somewhat changed over the years, but at the moment (latest update in 2020) the Finnish guidelines advice screening samples to be taken in following situations: patient has been hospitalized abroad within one year, patient is transferred from any ward that has an ongoing epidemic or patient has been treated in such a ward within one year, patient is living in same household with a known MRSA carrier or patient comes from a refugee camp, reception centre or foreign orphanage.7 The latter patient group was only added in the local guidelines in HDSWF in 2015 and intravenous drug users (IVDU) in 2017. The time period regarding screening after hospital care abroad has previously varied between one and five years.
MRSA can cause many types of infections from SSTIs, maxillary sinus infections and pneumonias to surgical site infections and bloodstream infections in hospital settings.3 Although MRSA cases, especially community-associated ones, have increased both world-wide2 and in Finland, including our hospital district (HD),8 the infections caused by MRSA have not been a major concern in patient care in Finland.
In this study, we aimed to characterize the spectrum of MRSA infections and their treatment in our HD. We also determined the spa types of MRSA isolates causing the infections. We retrospectively analyzed all new MRSA cases in HDSWF during 2007–2016.
Materials and Methods
Study Setting
This registry-based, retrospective study took place in HDSWF, which covers a population of 475543 residents (year 2016),9 representing 8.6% of the total population in Finland (5.5 million).10
MRSA Detection and Registries
The cases in our study were detected either by active screening and contact tracing based on Finnish MRSA tracing policies or from clinical specimens.
The Turku University Hospital clinical microbiology laboratory performed MRSA diagnostics for HDSWF.11 Finnish clinical microbiology laboratories notified all new MRSA findings by law12 to the National Infectious Disease Register (NIDR) maintained by the Finnish Institute for Health and Welfare (THL). The MRSA isolates were sent to the culture collection of NIDR. THL performed spa typing13 for them and reported the result back to the HD. The spa types from 2007 and 2008 were analyzed locally at the University of Turku.
All new MRSA cases (both screening and clinical samples) detected in HDSWF from January 2007 through December 2016 were recorded in the hospital MRSA registry; Register of Hospital Infections and Carriers of Resistant Bacteria (SAI register, SAI®, Neotide Oy, Vaasa, Finland). The information included data on specimen type, hospital or community association, contact tracing, spa type and the degree of colonization, if available. Data on the clinical details at the time of MRSA detection was collected manually by reading through the patient records (by the investigators, T. H. and R.O). The case was classified as a clinical infection, if MRSA was isolated from a clinical culture (instead of MRSA screening) and/or the patient records revealed a clinical infection by the time of sampling. Only the cases classified as a clinical infection were included in this study. Only the first MRSA infection of an individual was included. Data on possible recurrent or subsequent infections was not collected.
Patient Data
Background information (eg family cluster and CA-/HA-association)8 were collected from SAI register, and medical history of patients were collected from electronic patient records in Turku University Hospital and Turku primary health care. MRSA cases in healthcare workers (HCWs), infants under 28 days of age, and patients who were hospitalized or who had stayed in a nursing home within the previous 2 years in Finland, or 2 years14 abroad, were defined as healthcare-associated MRSA (HA-MRSA), and cases without such link were considered as being CA-MRSA cases if MRSA was isolated at outpatient care or within the first 2 days of hospital care.8 Many of the patients had been treated in private sector, from where we could not obtain any patient history. Medical conditions were classified using Charlson Comorbidity Index (CCI).15 The antibiotic therapy (both empiric and adjusted) was considered appropriate, if the prescribed antibiotic agent matched the susceptibility pattern of the MRSA isolate in question. The decision on whether antibiotic treatment was needed, and which antibiotic regimens were used, was made by the treating clinician, and the rationale was inconclusively stated in the patient record. Healing time was collected, if it was a mentioned in the patient record.
Family Clusters
In situations, where the MRSA carrier suffered from recurrent infections and/or was considered for eradication treatment, the whole family of the patient was tested for MRSA carriage. Majority of the family members were asymptomatic carriers. When more than one member of a family was MRSA positive, the family was considered a family cluster (FC).8
Statistical Analysis
The statistical analysis was made using IBM SPSS Statistics [version 29.0.2.0 (142)]. The antibiotic usage and healing time between groups were compared using chi-squared test or Fisher’s exact test. P-values less than 0.05 were considered statistically significant.
Results
In total, there were 983 new MRSA cases in HDSWF during the study period of 2007–2016. Of these, 280 were clinical infections. More than half of the patients (55.7%; 156/280) were adults in working age (18–64 years), the median age being 46 years (IQR 47). Children (<18 years) accounted for 14.3% (40/280) of the cases. Of the patients with clinical infections, 53.6% (150/280) were male. Table 1
 |
Table 1 Background Information |
We obtained information on medical conditions in 81.8% (229/280) of the patients with clinical infections. The details of empiric antibiotic treatment were available in 46.8% (131/280) and of adjusted treatment in 49.3% (138/280) of the cases, respectively. The information on clinical outcome was obtained in 23.2% (65/280) of the cases.
Of the 280 clinical infections in our study population, 22.1% (62/280) patients belonged to an FC. There were 56 different FCs in this study material. The largest FCs consisted of five MRSA positive family members. Only one or two persons of each FC had a clinical infection during the study period.
The most common spa type in our material was spa t172 (52 cases, 18.6%), followed by spa t032 (23 cases, 8.2%) and spa t008 (19 cases, 6.8%). Altogether 76 different spa types were detected, most (49/76; 64.5%) of them sporadic. Table 1
SSTIs were dominant in our study population, 213 (76.1%) cases. The median age of these patients was 46 years (0–96 years, IQR 41), and 115 of them (54%) were male. There were 64 different spa types causing SSTIs (Table 1). The four most common spa types caused 40.8% (87/213) of all SSTIs. There were 39 different FCs in the SSTI group, most of them having one family member with an infection. In four FCs there were two family members suffering from an infection during the study period.
Of SSTIs, 76 (76/213; 35.7%) were abscesses. The median age of the patients was 33 years (0–89 years, IQR 26). Majority of them were healthy (CCI 0) or had some comorbidities (CCI 1–4), 40 (40/76; 52.6%) and 17 (17/76; 22.4%), respectively. Of these patients, 13 (13/76; 17.1%) were born abroad, 11 (11/76; 14.5%) had been in hospital care 2 years prior to MRSA detection and 7 (7/76; 9.2%) were HCWs and three (3/76; 3.9%) were IVDUs. Of the abscess patients, 11 (11/76; 14.5%) were hospitalized due to the infection. Table 1
Surgical site infections accounted for 23.9% (51/213) of the SSTIs. Majority of the patients were healthy (CCI 0) or had some comorbidities (CCI 1–4), 13 (13/51; 25.5%) and 22 (22/51; 43.1%) cases, respectively. Six patients (6/51; 11.8%) were born abroad, four (4/51; 7.8%) had been in hospital care abroad within 2 years, three patients (3/51; 5.9%) were HCWs, and one patient (1/51; 2.0%) was an IVDU. Table 1
Of all the SSTI patients, 19 (19/51; 37.3%) were hospitalized due to the infection.
There were only six bacteremias in the study population, four of them being healthcare-associated (the information missing in one case). All six had a different spa type. Their CCI ranged from 0 (two cases) to 8 (one case), and none of them were HCWs nor had other known risk factors that could have indicated an MRSA infection (Table 1). Since there was no mention about metastatic foci in the patient records in all but one case, the clinical cure rate was not possible to be unambiguously calculated.
Only one patient suffering from an SSTI of a chronic wound died during the study period. They had a prior surgical procedure and had multiple comorbidities (CCI 5).
Of all the infections, we obtained details of the use of systemic empiric antibiotics in 46.8% (131/280) cases and for the usage of antibiotics after culture results in 49.3% (138/280) cases. Of these, 81.7% (107/131) received empiric treatment that did not cover MRSA. After the culture results, the treatment was modified in 34.1% (47/138) cases, resulting in appropriate antibiotic treatment in 49.3% (68/138) of the cases (Figure 1). Most often the antibiotic treatment was modified in surgical site infections and infections of chronic wounds, 7.8% vs 35.3% and 5.9% vs 29.4%, respectively. There was no statistically significant difference in the outcome of the infections between these two groups (p=0.433).
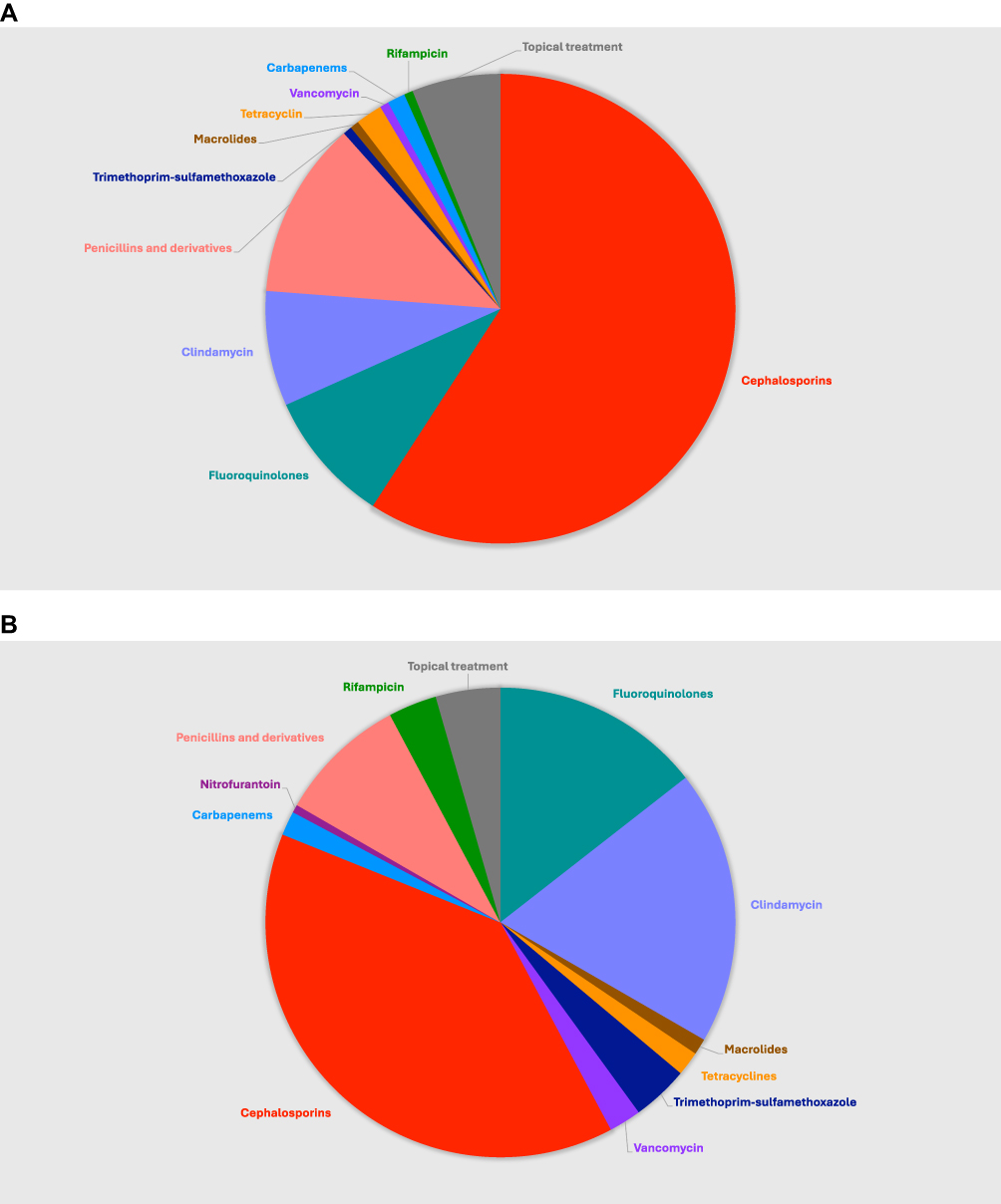 |
Figure 1 (A) Empiric antibiotic treatments, one or multiple agents simultaneously (B) Treatment after culture results, one or multiple agents simultaneously. |
Within the patients (107/131) receiving inappropriate empiric treatment, 13.1% (14/107) were born abroad (Table 1 esupplement), 10.3% (11/107) had been in hospital care abroad within 2 years, 1.9% (2/107) were IVDUs, and 34.6% (37/107) had had some surgical procedure (eg prosthetic joint replacement, abdominal surgery, tympanostomy tube insertion etc.) done within 2 years prior to diagnosis.
Regarding empiric and adjusted treatment, details about the treatment outcome were available in 43.5% (57/131) and 42.8% (59/138) cases, respectively. Healing times did not differ upon appropriateness of the antibiotics used (data not shown).
Discussion
Based on our findings, surprisingly many patients (81.7%) whose infection was later found to be caused by MRSA were treated with empiric treatment that did not cover the pathogen. In at least fourth (25/107) of these cases, the patient history could have revealed a risk of MRSA carriage and infection. Although the local guideline describing risk factors had recently been updated, some risk factors were seemingly not implemented in clinical practice.
Several studies16–19 have shown, that inappropriate empiric antibiotic therapy is common, 15% – more than 50% of patients having received inadequate antibiotic treatment for an MRSA infection. Also, Berla-Kerzhner et al19 have reported that the treating physicians do not refer to the culture results, which leads to mistreatment. We do not know whether the low percentage of adequate treatment in our study population may have been due to ignoring the culture results, just overlooking the resistance pattern, or due to the fact that the infection had healed in spite of the treatment.
Within the available information in our study, we found no indication that the lack of appropriate antimicrobial treatment would have resulted in a worse clinical outcome. There might be several reasons for this. Only fifth of the patients were hospitalized during the MRSA infection, indicating that the infections were generally mild, and therefore could possibly have been cured even without antibiotics, merely with incision and drainage. The patients in our study population were generally healthy, suggesting that they had a good immune system to fight the infection.
The infections could also have been polymicrobial, as was the case in a study of Clayes et al.20 In such case, the given antibiotics might still have had some effect, albeit not against MRSA. It should also be considered whether the MRSA strain cultured was the actual pathogen causing the infection. Pulido-Cejudo et al18 raised the question about patients with chronic skin and skin structure infections often being colonized with bacteria that do not cause the acute infection requiring prompt empiric antibiotic therapy. It is important to distinguish the cases that need timely, adequate treatment with effective antibiotics from the non-life-threatening ones.
By far, the most common empiric antibiotics used in our material were cephalosporins, followed by penicillins, fluoroquinolones and clindamycin. Trimethoprim-sulfamethoxazole was rarely used either for empiric or final treatment in our study population, even though our laboratories in general do test the susceptibilities for this antibiotic. Agostino21 had noted that 98.5% of the MRSA infections in their study could have been treated with trimethoprim-sulfamethoxazole. At the moment Finland still is a country of low MRSA incidence, thus trimethoprim-sulfamethoxazole should not be considered as an empiric treatment option for every patient. When antibiotic treatment is needed, these are still appropriate first-line choices for most patients, as long as the MRSA risk assessment has taken place prior to prescribing antibiotics. For the treatment of SSTIs, our guidelines advocate benzylpenicillin, (flu)cloxacillin or I–II generation cephalosporins as first-line treatment options. As is previously shown in many studies,22–24 infectious diseases (ID) consultation improves quality of care, the use of appropriate antibiotics, and also reduces mortality. It would be beneficial that an ID specialist is consulted more often during the treatment of an infection caused by a resistant pathogen.
As is universally noted,18,25,26 SSTIs were the most common infection type also in our study population. The most common spa types (spa t002, t008, t019, t044 and t437) causing abscesses in our study population were spa types that have previously been associated with PVL positivity in the literature.27–31 We were not able to consistently assess for PVL positivity in our study. Even though some spa types were more common, the spa type variation was wide, and many of the strains were sporadic.
There are some limitations in our study. It is a relatively small, retrospective, register-based, single-center study in a low-endemicity region. We did not have access to patient record data from the private sector, nor were the antibiotic treatments given always stated in the records. Patients might also have moved to a different HD, resulting in no further patient record data in HDSWF. All these factors lead to partly incomplete and inadequate data. Due to small numbers of cases in different clinical subgroups, broader inferential analyses were not possible to perform. A strength of our study is the comprehensive Finnish MRSA surveillance system allowing identification of the cases.
Conclusion
In low-endemicity settings, risk factors for MRSA carriage and infection may not always be recognized in clinical settings. If cultures are not obtained or if empiric treatment is not adjusted upon culture results and resistance patterns, adequate treatment may be delayed or missed.
Health-care personnel’s awareness of the possibility of an MRSA infection is important in order for them to recognize these infections, to assess the outcome of empirical treatment, and to re-evaluate the treatment options upon culture results.
Data Sharing Statement
The datasets generated during the current study are not publicly available as they contain health-related data, but limited datasets (without any identifiable, person-related data) are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Hospital District of Southwest Finland (T162/2016; J28/21), the City of Turku (12143-2017; 4660-2022) and the Finnish Institute for Health and Welfare (THL336/6.02.00/2016; THL/319/5.05.00/2020). The study was exempted from ethics approval; according to the Finnish Medical Research Act (488/1999), the Act of the Medical Use of Human Organs, Tissues and Cells (101/2001) and the Biobank Act (688/2012), as amended, and as confirmed by the Hospital District of Southwest Finland Research Ethics Committee (since 2023 named as Research Ethics Committee of The Wellbeing Services County of Southwest Finland), no ethical committee approvals or informed consent were needed for this retrospective, register-based study. The data accessed complied with relevant data protection and privacy regulations.
The material is original and has not been published elsewhere. Parts of this study have been presented as a poster in The Federation of Infection Societies conference (FIS/HIS International 2024) in Liverpool, UK, in November 20–22, 2024.
Acknowledgments
Authors kindly thank Associate Professor Esa Rintala for his important work in designing and executing the study. Infection control nurse Tiina Kurvinen is thanked for assistance in data collection and the use of the patient records. Research professor Outi Lyytikäinen and Mr. Jukka Ollgren are thanked for valuable advice and discussions during planning of the study. MRSA Study Group is thanked for their valuable input.
Collaborators
MRSA Study Group: Harri Marttila (Infection Control Unit, Turku University Hospital, The Wellbeing Services County of Southwest Finland, Turku, Finland), Kirsi Gröndahl–Yli–Hannuksela (Institute of Biomedicine, University of Turku, Turku, Finland), Anu Harttio-Nohteri (Infection Control Unit, Turku University Hospital, The Wellbeing Services County of Southwest Finland, Turku, Finland), Jenna Junnila (Institute of Biomedicine, University of Turku, Turku, Finland), Laura Lindholm (Finnish Institute for Health and Welfare, Helsinki, Finland), Kaisu Rantakokko-Jalava (Institute of Biomedicine, University of Turku, Turku, Finland and Clinical Microbiology Laboratory, Turku University Hospital, The Wellbeing Services County of Southwest Finland, Turku, Finland).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Open access funding provided by the University of Turku (UTU) including the Turku University Central Hospital. Dr. Sakari Alhopuro, M.D., Ph.D., is kindly thanked for financial support for this project. The work has also been supported by the Competitive State Research Financing of the Expert Responsibility area of the Turku University Hospital (M3016) for J.V. and by a grant from the Infectious Diseases Specialists’ Society, the Turku University Hospital and the Turunmaa Duodecim Society for T.H.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. European Centre for Disease Prevention and Control. Antimicrobial resistance in the EU/EEA (EARS-Net) - Annual Epidemiological Report for 2019. Available from: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2019.
2. Ippolito G, Leone S, Lauria FN, Nicastri E, Wenzel RP. Methicillin-resistant Staphylococcus aureus: the superbug. Int J Infect Dis. 2010;14(SUPPL. 4). doi:10.1016/j.ijid.2010.05.003
3. David MZ, Daum RS. Community-associated methicillin-resistant Staphylococcus aureus: epidemiology and clinical consequences of an emerging epidemic. Clin Microbiol Rev. 2010;23(3):616–9. doi:10.1128/CMR.00081-09
4. Aro T, Kantele A. High rates of meticillin-resistant Staphylococcus aureus among asylum seekers and refugees admitted to Helsinki university hospital, 2010 to 2017. Eurosurveillance. 2018;23(45). doi:10.2807/1560-7917.ES.2018.23.45.1700797
5. Zhou YP, Wilder-Smith A, Hsu LY. The role of international travel in the spread of methicillin-resistant Staphylococcus aureus. J Travel Med. 2014;21(4):272–281. doi:10.1111/jtm.12133
6. Schwartz KL, Morris SK. Travel and the spread of drug-resistant bacteria. Curr Infect Dis Rep.Current Medicine Group LLC 1. 2018;20(9). doi:10.1007/s11908-018-0634-9
7. Kolho E, Lyytikäinen O, Jalava J. Available from: Ohjaus 2/2020 ohje moniresistenttien mikrobien tartunnantorjunnasta. http://urn.fi/URN:ISBN:978-952-343-463-9.
8. Junnila J, Hirvioja T, Rintala E, et al. Changing epidemiology of methicillin-resistant Staphylococcus aureus in a low endemicity area—new challenges for MRSA control. Eur J Clin Microbiol Infect Dis. 2020;39:2299–307. doi:10.1007/s10096-020-03824-9
9. Lounaistieto. Available from: https://pxdata.stat.fi/PxWeb/pxweb/fi/Kuntien_avainluvut/Kuntien_avainluvut__2019/kuntien_avainluvut_2019_aikasarja.px/table/tableViewLayout1/.
10. Tilastokeskus. Tilastokeskus. Available from: https://www.stat.fi.
11. Petersen A, Larssen KW, Gran FW, et al. Increasing incidences and clonal diversity of methicillin-resistant Staphylococcus aureus in the nordic countries - results from the nordic MRSA surveillance. Front Microbiol. 2021;12(April). doi:10.3389/fmicb.2021.668900
12. Communicable Diseases Act. Available from: https://www.finlex.fi/eli?uri=http://data.finlex.fi/eli/sd/2016/1227/ajantasa/2025-06-27/fin.
13. Harmsen D, Claus H, Witte W, et al. Typing of methicillin-resistant Staphylococcus aureus in a university hospital setting by using novel software for spa repeat determination and database management. J Clin Microbiol. 2003;41(12):5442–5448. doi:10.1128/JCM.41.12.5442-5448.2003
14. Silvola J, Gröndahl-Yli-Hannuksela K, Hirvioja T, et al. Whole genome sequencing reveals new links between spa t172/CC59 methicillin-resistant Staphylococcus aureus cases in low-endemicity region of Southwest Finland, 2007‒2016. Sci Rep. 2022;12(1). doi:10.1038/s41598-022-25556-w
15. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. PMID: 3558716. doi:10.1016/0021-9681(87)90171-8
16. Nurjadi D, Friedrich-Jänicke B, Schäfer J, et al. Skin and soft tissue infections in intercontinental travellers and the import of multi-resistant Staphylococcus aureus to Europe. ClinMicrobiol Infect. 2015;21(6):567.e1–567.e10. doi:10.1016/j.cmi.2015.01.016
17. Cosgrove SE, Sakoulas G, Perencevich EN, Schwaber MJ, Karchmer AW, Carmeli Y. Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: a meta-analysis. Clin Infect Dis. 2003;36(1): 53–59. PMID: 12491202. doi:10.1086/345476
18. Pulido-Cejudo A, Guzmán-Gutierrez M, Jalife-Montaño A, et al. Management of acute bacterial skin and skin structure infections with a focus on patients at high risk of treatment failure. Ther Adv Infect Dis. 2017;4(5):143–161. PMID: 28959445; PMCID: PMC5593224. doi:10.1177/2049936117723228
19. Berla-Kerzhner E, Biber A, Parizade M, et al. Clinical outcomes and treatment approach for community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA) infections in Israel. European Journal of Clinical Microbiology and Infectious Diseases. 2017;36(1):153–162. doi:10.1007/s10096-016-2789-3
20. Claeys KC, Zasowski EJ, Lagnf AM, Levine DP, Davis SL, Rybak MJ. Novel application of published risk factors for methicillin-resistant S. aureus in acute bacterial skin and skin structure infections. Int J Antimicrob Agents. 2018;51(1):43–46. doi:10.1016/j.ijantimicag.2017.05.015
21. Agostino JW, Ferguson JK, Eastwood K, Kirk MD. The increasing importance of community-acquired methicillin-resistant Staphylococcus aureus infections. Medical Journal of Australia. 2017;207(9):388–393. doi:10.5694/mja17.00089
22. Hollingshead CM, Khazan AE, Franco JH, et al. A needs assessment for infectious diseases consultation in community hospitals. Infect Dis Ther. 2023;12(6):1725–1737. doi:10.1007/s40121-023-00810-4
23. Burnham JP, Olsen MA, Stwalley D, Kwon JH, Babcock HM, Kollef MH. Infectious diseases consultation reduces 30-day and 1-year all-cause mortality for multidrug-resistant organism infections. Open Forum Infect Dis. 2018;5(3). doi:10.1093/ofid/ofy026
24. Bai AD, Showler A, Burry L, et al. Impact of infectious disease consultation on quality of care, mortality, and length of stay in Staphylococcus aureus bacteremia: results from a large multicenter cohort study. Clinical Infectious Diseases. 2015;60(10):1451–1461. doi:10.1093/cid/civ120
25. Calfee DP. Trends in community versus health care-acquired methicillin-resistant Staphylococcus aureus infections. Curr Infect Dis Rep. 2017;19(12):1–7. doi:10.1007/s11908-017-0605-6
26. Andreassen AES, Jacobsen CM, de Blasio BF, White R, Kristiansen IS, Elstrøm P. The impact of methicillin-resistant S. aureus on length of stay, readmissions and costs: a register based case-control study of patients hospitalized in Norway. Antimicrob Resist Infect Control. 2017;6(1). doi:10.1186/s13756-017-0232-x
27. European Food Safety Authority, European Centre for Disease Prevention and Control. The European Union summary report on antimicrobial resistance in zoonotic and indicator bacteria from humans, animals and food in 2018/2019. EFSA J. 2021;19(4). doi:10.2903/j.efsa.2021.6490
28. Kawaguchiya M, Urushibara N, Yamamoto D, et al. Characterization of PVL/ACME-positive methicillin-resistant Staphylococcus aureus (Genotypes ST8-MRSA-IV and ST5-MRSA-II) isolated from a university hospital in Japan. Microbial Drug Resistance. 2013;19(1):48–56. doi:10.1089/mdr.2012.0089
29. Rahmani Z, Hosseini SS, Bagheri P, Dadashi M, Haghighi M, Goudarzi M. Phenotypic and genotypic characterization of Staphylococcus aureus strains isolated from otitis externa: emergence of CC30-spa t019-SCCmec IV carrying PVL as major genotype. Heliyon. 2024;10(11). doi:10.1016/j.heliyon.2024.e32002
30. Klein S, Hannesen J, Zanger P, Heeg K, Boutin S, Nurjadi D. Entry of Panton–Valentine leukocidin-positive methicillin-resistant Staphylococcus aureus into the hospital: prevalence and population structure in Heidelberg, Germany 2015–2018. Sci Rep. 2020;10(1). doi:10.1038/s41598-020-70112-z
31. Stańkowska M, Garbacz K, Piechowicz L, Bronk M. Dissemination of t437-SCCmeciv and coagulase-negative t037-sccmeciii types among borderline oxacillin-resistant Staphylococcus aureus isolated from skin infections and diabetic foot ulcers. Infect Drug Resist. 2019;12:3197–3203. doi:10.2147/IDR.S219557
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.