Back to Journals » International Journal of Women's Health » Volume 15
A Retrospective Cohort Study on the Prevalence, Risk Factors, and Improvement of Overactive Bladder Symptoms in Women with Pelvic Organ Prolapse
Authors Aimjirakul K, Ng JJ, Saraluck A ![]() , Wattanayingcharoenchai R, Mangmeesri P, Manonai J
, Wattanayingcharoenchai R, Mangmeesri P, Manonai J ![]()
Received 12 April 2023
Accepted for publication 29 June 2023
Published 13 July 2023 Volume 2023:15 Pages 1039—1046
DOI https://doi.org/10.2147/IJWH.S413670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Everett Magann
Komkrit Aimjirakul, Jun Jiet Ng, Apisith Saraluck, Rujira Wattanayingcharoenchai, Peeranuch Mangmeesri, Jittima Manonai
Department of Obstetrics & Gynaecology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Jun Jiet Ng; Jittima Manonai, Department of Obstetrics & Gynaecology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, 10400, Thailand, Tel +66-2-2012167, Fax +66-2-2011416, Email [email protected]; [email protected]
Background: Overactive bladder (OAB) symptoms are common in women with pelvic organ prolapse (POP), but the explanation is unclear. It is also uncertain whether OAB symptoms improve or persist after POP reduction. This study aimed to determine the prevalence and risk factors for OAB symptoms in women with POP, and to compare the improvement of OAB symptoms among women in three treatment groups: pelvic floor exercise, pessary, and surgery.
Methods: This retrospective cohort study included patients who visited our urogynecology clinic from January 2016 to December 2020. The Pelvic Floor Bother Questionnaire was used to evaluate selected pelvic floor symptoms (OAB and POP). Demographic characteristics and clinical findings, including Pelvic Organ Prolapse Quantification System and number of prolapsed compartments, were analyzed. Univariate and multivariate analyses were conducted to identify risk factors for OAB symptoms in women with POP. Subgroup analyses were performed in 533 patients to evaluate the improvement of OAB symptoms following POP treatment.
Results: A total of 754 patients were analyzed. The incidence of OAB symptoms was 70% (533/754) and two-thirds (65%) reported moderate to severe bother. The lowest points of the anterior wall (OR 0.60; 95% CI 0.41– 0.87; p = 0.01), longer perineal body (OR 0.78; 95% CI 0.21– 0.76; p = 0.02), and previous vaginal delivery (OR 2.10; 95% CI 1.14– 3.89; p = 0.02) were identified as significant risk factors. In the subgroup analyses, improvement in OAB symptoms was observed in 36.6% (195/533) of women who underwent POP treatment. Compared with pelvic floor exercise, pessary (OR 1.40; 95% CI 0.94– 2.07; p = 0.10) and surgery (OR 1.30; 95% CI 0.80– 2.12; p = 0.28) had higher odd ratios but the effects were not significant.
Conclusion: The prevalence of OAB symptoms in women with POP was high at 70%. Improvement in OAB symptoms was observed in one-third of women who underwent POP treatment. However, there were no significant differences between the treatment methods.
Keywords: pelvic organ prolapse, overactive bladder, pelvic floor bother questionnaire, prevalence, risk factors, pessary, surgery
Introduction
The female pelvic floor can be divided into three compartments: anterior, apical, and posterior.1 Pelvic floor disorders include pelvic organ prolapse (POP), urinary incontinence, voiding dysfunction, anal incontinence, defecatory dysfunction, pelvic pain syndrome, and sexual dysfunction.2 These conditions are usually related to one another and share common risk factors, such as aging, pregnancy, vaginal delivery, and heavy lifting.3 POP, referring to descent of the vaginal wall, uterus, or post-hysterectomy vaginal vault,4 is an extremely prevalent problem that occurs in approximately 50% of parous women.5 Overactive bladder (OAB) is a condition characterized by urinary urgency, typically with urinary frequency and nocturia, with or without urgency urinary incontinence (UUI).6 According to the Epidemiology Urinary Incontinence and Comorbidities (EPIC) study, OAB affects 13% of women regardless of age.7 However, the pathophysiology of OAB is not fully understood.
POP and OAB symptoms often coexist. In a recent population-based study, 82% of women with POP reported at least one OAB symptom of any degree and 40% had at least one bothersome OAB symptom.8 However, evidence for correlations between specific anatomical defects and symptom severity is conflicting. Among many theories related to OAB, one theory that can explain the correlation of OAB symptoms with POP is the Integral Theory proposed by Petros and Ulstem.9 The Integral Theory views OAB pathogenesis as anatomical, resulting from defects and damage to the pelvic floor musculo-ligamentous system. Moreover, laxity of the suspensory ligaments inactivates the vector forces that contract against them.9 Observed improvement of OAB symptoms after repair of loose cardinal and uterosacral ligaments proved that the origins of OAB symptoms are not only within the bladder.8 Stretching of the bladder wall is likely to occur in vaginal prolapse, and this may trigger stretch receptors and result in detrusor contractions.10 Other theories such as bladder outflow obstruction causing bladder distention and release of detrusor stimulants, traction and kinking of the urethra, denervation of the bladder wall, detrusor muscle changes, and changes of the spinal micturition reflex have also been postulated.11 However, data for the relationships between stages of prolapse and OAB symptoms are sparse and conflicting. Bladder outlet obstruction from advanced anterior wall prolapse might be the most possible pathophysiology of OAB symptoms,11 though urgency and UUI were more frequently observed in women with less advanced prolapse overall.12,13
Treatment of POP can be divided into pelvic floor exercise, pessary, and surgery. Few studies have compared the improvement of OAB symptoms in women with POP after different modalities of treatment. Several studies attempted to predict the effects of POP treatment on OAB symptoms, but the results were inconsistent. While the majority of the studies indicated improvement in bothersome OAB symptoms after POP treatment,7,13–15 Johnson et al found that 40% of patients had persistent OAB symptoms and 6% of patients had de novo OAB symptoms after POP treatment.16 Thus, it remains unclear which patients will experience resolution or persistence of OAB symptoms after treatment to correct POP, and this may cause frustration and disappointment for patients. In this study, the prevalence and correlation between OAB symptoms and POP were reviewed and risk factors for OAB symptoms in women with POP were identified. The efficacies of the different treatment modalities for the improvement of OAB symptoms in women with POP were also compared.
Materials and Methods
Study Setting and Population
This retrospective cohort study was conducted in Ramathibodi Hospital, Bangkok, Thailand. The inclusion criteria were consecutive female patients who visited the urogynecology clinic with POP symptoms from January 2016 to December 2020. The exclusion criteria were OAB treatment, pelvic reconstructive or anti-incontinence surgery, urinary tract infection, or neurological diseases. Patients with missing data, which were variables studied and 6-month follow-up, in their medical records were also excluded.
Data Collection
The electronic medical records of the eligible patients were reviewed. The Pelvic Floor Bother Questionnaire (PFBQ) was used to identify POP and OAB symptoms in the patients at their first visit. Data for demographic characteristics, including age, body mass index (BMI), menopausal status, parity, history of vaginal delivery, previous hysterectomy, and previous pelvic floor surgery, were collected for all patients. Physical examination findings, including Pelvic Organ Prolapse Quantification (POP-Q) and pelvic floor muscle strength (Brink score), were recorded and analyzed. The PFBQ is a nine-item self-administered questionnaire developed by The Cleveland Clinic that has been validated as a tool to evaluate symptoms and bother related to prolapse, bladder, and bowel symptoms.17 Symptom severity was assessed using a Likert scale bother score. The PFBQ has been translated, validated, and used in our center because of its clarity, simplicity, and ease of self-filling.18 Women with POP were identified through a positive response to Question 6 of the PFBQ (Do you experience the feeling of a bulge in the vagina?). Different stages of POP in the different compartments (anterior, apical, and posterior) were classified according to the IUGA and ICS terminology and grouped into four categories (Stages I, II, III, and IV). The study had two groups: women with OAB symptoms and women without OAB symptoms. Presence of OAB symptoms was determined using the PFBQ and defined as a positive response to Question 3 (Do you experience an abnormal strong feeling of urgency to urinate?) or Question 4 (Do you experience urine leakage associated with the feeling of urgency?). A urine analysis was conducted in all patients to rule out urinary tract infection. The POP treatments provided were pelvic floor exercise, pessary, and surgery. Data at 3 and 6 months post-treatment visits were evaluated for the improvement of OAB symptoms. Improvement was defined as either complete resolution of urgency and/or frequency and/or urgency incontinence, or a decrease in the degree of symptom bother.
Statistical Analysis
Data entry and statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) version 24. The chi-square test was used to compare risk factors between women with and without OAB symptoms. Student’s t-test and the Mann–Whitney U-test were used to assess the differences in continuous variables. A multivariate logistic regression analysis was conducted to estimate the associations between other variables. The adjusted odds ratio (OR) and 95% confidence interval (CI) were estimated for each correlation. Values of p <0.05 were considered to indicate statistical significance. Data were presented as mean ± standard deviation, median (minimum, maximum), or percentage depending on the variable.
The required sample size was calculated using a sample size formula with the following assumptions: confidence interval of 95%, precision of 5% and power of 80%. These assumptions were based on the reported prevalence of 37% for OAB symptoms among women with POP,19 and gave a sample size of 754 women.
Results
Patient Characteristics
The medical records of 840 patients were evaluated. After exclusion of 86 patients with missing data and loss to follow-up, the final study population contained 754 patients with a mean age of 65.77±9.45 years. No differences were found between the included and the excluded groups in terms of age and OAB symptoms. The sociodemographic characteristics and physical examination findings were analyzed. Among the total 754 patients, 95% were postmenopausal, the mean BMI was 25.23±3.47 kg/m2, 94% of women had a history of vaginal delivery, and 5.8% were nulliparous. Regarding pelvic compartments, 27.7% had a single prolapsed compartment, 27.7% had two prolapsed compartments, and 38.2% had three prolapsed compartments. The POP-Q examination findings revealed a mean perineal body of 2.5±0.72 cm and a mean genital hiatus of 4.11±0.99 cm. The prevalence of OAB symptoms in women with POP was 70.4% (533/754). According to the PFBQ, approximately two-thirds of the patients (65%) were moderately and severely bothered by their OAB symptoms, such as the need for sanitary pad wearing, toilet mapping, and reduced participation in social activities.
Risk Factors for OAB Symptoms
The univariate analyses of associations between OAB symptoms and variables of interest are shown in Table 1. Age (p = 0.89), parity (p = 0.08), BMI (p = 0.08), menopausal status (p = 0.22), previous hysterectomy (p = 0.09), and previous pelvic floor surgery (p = 0.52) were not risk factors for OAB symptoms in women with POP. In contrast, history of vaginal delivery, point Ba beyond the hymen, and perineal body were associated with OAB symptoms. On physical examination, the apical compartment; point C (p = 0.37), the posterior compartment; point Bp (p = 0.19), GH (p = 0.71), TVL (p = 0.06), number of prolapsed compartments (p = 0.14), and Brink score (p = 0.7) were not related to OAB symptoms.
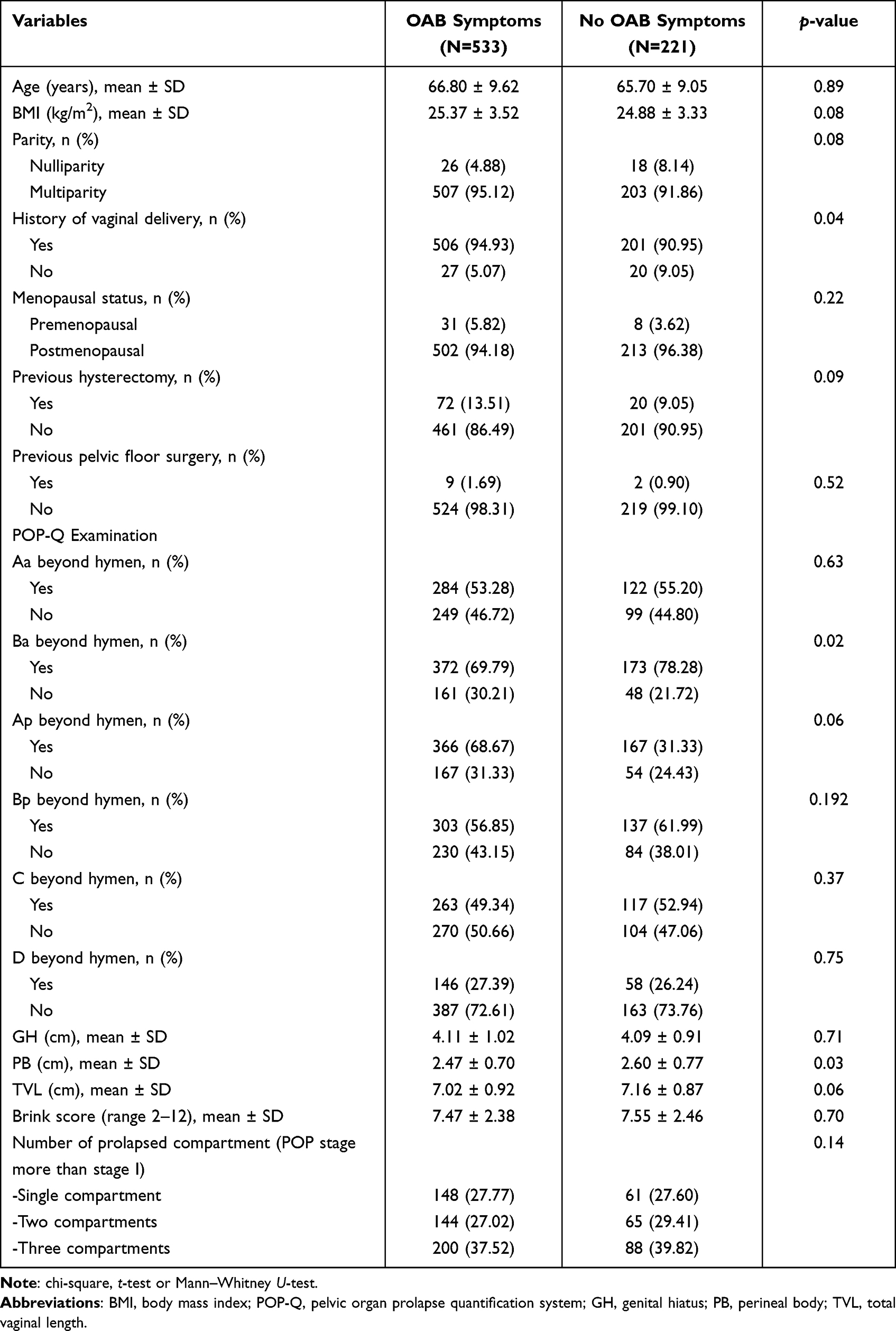 |
Table 1 Women with POP with or Without Overactive Bladder (OAB) Symptoms (N = 754) |
The results for the stepwise multivariate regression analysis are shown in Table 2. The analysis revealed that less advanced anterior vaginal wall prolapse with point Ba above the hymen (OR 0.60; 95% CI 0.41–0.87; p = 0.01) and longer perineal body (OR 0.78; 95% CI 0.21–0.76; p = 0.02) were protective factors against OAB symptoms in women with POP. Meanwhile, history of vaginal delivery (OR 2.10; 95% CI 1.14–3.89; p = 0.02) significantly increased the risk of OAB symptoms in women with POP.
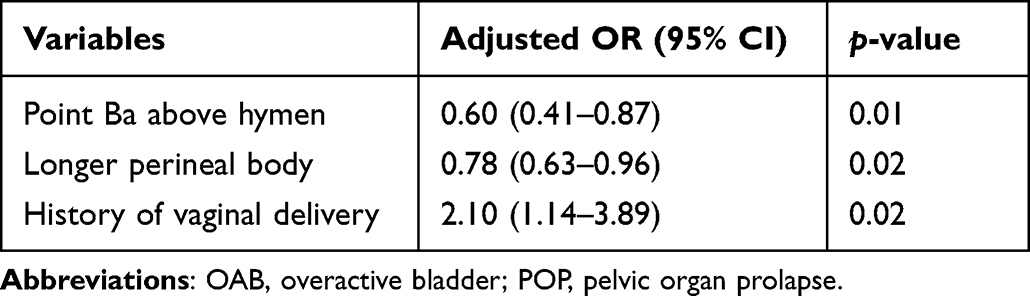 |
Table 2 Multivariate Associations Between Risk Factors and OAB Symptoms in Women with POP |
Improvement of OAB Symptoms After POP Treatment
Regarding POP treatment, the most common type of pessary used was ring with support (88.32%) and the three most common surgical procedures were apical with anterior compartment repair (32.69%), apical with anterior with posterior compartment repair (29.81%), and colpocleisis (22.11%). Table 3 shows the results for the three POP treatment groups: pelvic floor exercise, pessary, and surgery. Overall improvement in OAB symptoms after 6 months of treatment was seen in 36.6% (195/533) of women who underwent treatment for POP, comprising 40.9% (88/215) for pelvic floor exercise, 33.1% (71/214) for pessary, and 36% (36/104) for surgery (Figure 1). Compared with pelvic floor exercise, pessary (OR 1.40; 95% CI 0.94–2.07; p = 0.10) and surgery (OR 1.30; 95% CI 0.80–2.12; p = 0.28) had higher odd ratios, but the effects were not significant.
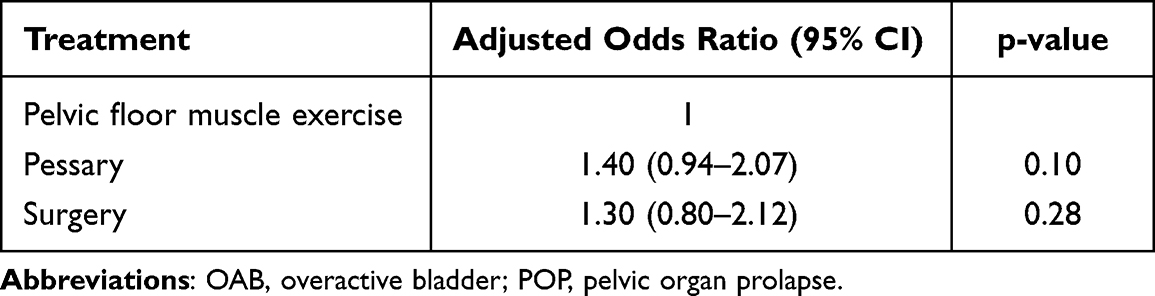 |
Table 3 Comparison of Different Treatments Groups in Improvement of OAB Symptoms in Women with POP |
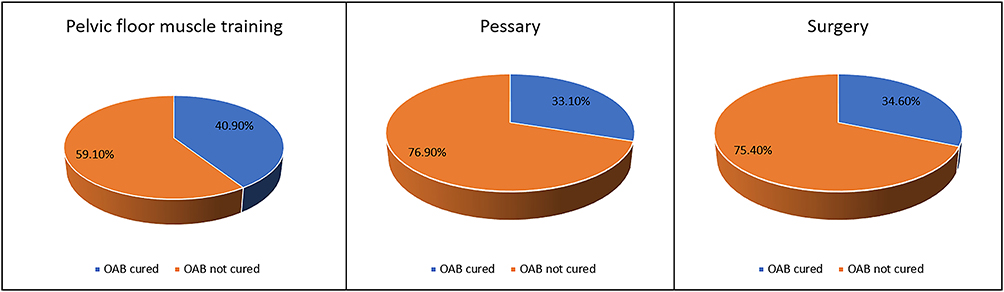 |
Figure 1 Improvement of overactive bladder (OAB) symptoms in women with organ prolapse (POP) symptoms after 6 months of treatment. |
Discussion
OAB symptoms and POP are two different pelvic floor disorders, but commonly coexist in patients. The findings of the present study confirmed the high correlation between OAB symptoms and POP. Moreover, the anatomical and structural factors for POP, namely advanced anterior wall prolapse and shorter perineal body, were clearly associated with OAB symptoms. Therefore, understanding the relationship between POP and OAB symptoms is important in clinical practice. Women who report prolapse symptoms should be asked about their OAB symptoms to achieve appropriate management of their symptoms. In addition to symptoms assessment and evaluation of their impact on quality of life, a focused physical examination is also needed, with special attention paid to the genitourinary examination and prolapse severity. In doing so, a complete clinical decision plan, reliable preoperative counseling, and appropriate goals of treatment would be developed. OAB symptoms should be examined in women with POP and the degree of bother caused by these symptoms should be quantified using validated patient-reported outcome measures such as the PFBQ.
Knowledge of the risk factors for OAB symptoms in women with POP can assist in the prevention and treatment of OAB symptoms in women with POP. The identification of history of vaginal delivery as a risk factor for OAB symptoms in women with POP can be explained by damage to the musculoligamentous system during passage of the fetus through the birth canal, leading to loss of bladder support, more distal position of point Ba, and shorter perineal body, which were significant findings in the present study. A more distal position of point Ba indicated a more significant anterior vaginal wall prolapse, which predisposed women with POP to OAB symptoms. Advanced anterior wall prolapse, which causes stretching of the bladder wall and prolonged outlet obstruction, could have an influence through an increased bladder sensation and enhancement of the spinal micturition reflex.10,11 Effective POP treatment can help relief of bladder outlet obstruction and bladder wall overstretching. Consequently, the reduction of urinary urgency, frequency, and UUI has been shown after treatment in our study and other studies.13–16
For women with POP, the various treatment options should be explained and appropriate preoperative counseling should be provided to avoid disappointment. The risk of de novo OAB symptoms and persistance or even worsening of OAB symptoms should be highlighted to patients prior to POP surgery.20 Also prior to surgery, all patients should be offered a pessary trial for POP reduction to gauge the dynamics of their OAB symptoms, because a pessary has the benefits of being minimally invasive, inexpensive, and associated with a low complication rate.21 The present findings demonstrated that pelvic floor exercise, pessary, and surgery were equally effective for treatment of OAB symptoms in women with POP, with an overall treatment efficacy of 36.6%. These findings are consistent with those in a study by Zacharakis et al,14 in which women with coexisting POP and OAB symptoms experienced a significant improvement in urgency and frequency symptoms after successful pessary fitting. Urgency, UUI, and Overactive Bladder Symptom Score were also significantly improved in patients with POP and OAB symptoms at 3 and 6 months after pelvic reconstruction surgery in previous studies.16,20 These phenomena may be explained by anatomical correction of the lower urinary tract obstruction by pessary use or surgery that provides effective relief of OAB symptoms in women with POP. However, the predictors for OAB symptom relief in women with POP remain unclear. Based on previous studies, predictors of persistent OAB symptoms following surgery for advanced POP include overweight status, preoperative UUI and detrusor overactivity, lower preoperative maximal flow rate, and postoperative complications.22–25 Preoperative counseling should include a discussion about persistent OAB symptoms following prolapse repair. Our study did not demonstrate the difference between treatment in alleviating OAB symptoms. This could be explained by a low sample size with low statistical power to detect a true effect of treatment, which was considered as the secondary outcome. Addition of other treatment modalities, such as antimuscarinic drugs, beta-3 agonists, and neuromodulation, may be helpful for women with persistent OAB symptoms despite correction of POP.
In medicine, prevention is better than cure. Because history of vaginal delivery was identified as a risk factor for OAB symptoms in women with POP, it is important to prevent maternal birth trauma. Counseling for vaginal delivery has always focused on obstetric anal sphincter injury, but the risk of OAB symptoms after vaginal delivery should also be included. Other variables such as fetal birth weight, instrumental delivery, and episiotomy should be investigated. Levator avulsion should be evaluated using digital palpation and ultrasound.26 Further examination for these variables will provide more information on the risk factors for OAB symptoms in women with POP.
The strength of the present study was that its conduction in Asian women to reflect our local condition, given that much of the existing literature was extrapolated from studies conducted in Caucasian populations. The study was carried out in a urogynecology clinic where women were asked about and were comfortable with disclosing their pelvic floor symptoms. This was reflected in the high prevalence of OAB symptoms among women with POP. The study also had several limitations that should be considered. First, it had a retrospective design. Second, data on OAB symptoms were collected by a self-reporting questionnaire without confirmation by urodynamic examinations or bladder diaries. Third, a specific scale for OAB or urgency severity scale were not used, thus, we could not quantify the impact and bother of the urgency symptoms in detail. Further prospective studies in which OAB symptoms are verified and quantified using an OAB-specific scale should be considered. Comparative studies on other treatment modalities for OAB symptoms in women with POP, such as antimuscarinic drugs, beta-3 agonists, and neuromodulation, should also be taken into consideration.
Conclusions
In the present study, the prevalence of OAB symptoms in women with POP was high at 70%, and approximately two-thirds of the patients reported moderate to severe symptoms that affected their quality of life. Advanced anterior wall prolapse, shorter perineal body, and previous vaginal delivery were identified as significant risk factors for OAB symptoms in women with POP. There was a one-third chance of OAB symptom improvement in women who received POP treatment with pelvic floor exercise, pessary, or surgery. This information can be useful for patient counseling and to guide patient expectations. Other treatment modalities should be considered in women whose OAB symptoms persist despite POP correction.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding authors upon reasonable request.
Ethical Considerations
This study was approved by the Medical and Research Ethics Committee of Ramathibodi Hospital Number MURA2022/773 (Expedited). Since this project was a retrospective chart review in which the data already exist, the informed consent was not required. However, the patient data were maintained with confidentiality and compliance with the Declaration of Helsinki.
Acknowledgments
The authors would like to thank Ms. Sasiporn Sitthisorn for assistance with the statistical analyses. The authors also thank Alison Sherwin, PhD, from Edanz (https://www.edanz.com/ac) for editing a draft of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest.
References
1. Delancey JOL. Anatomy. In: Cardozo L, Staskin D, editors. Textbook of Female Urology and Urogynecology.
2. Bump RC, Norton PA. Epidemiology and natural history of pelvic floor dysfunction. Obstet Gynecol Clin North Am. 1998;25(4):723–746. doi:10.1016/s0889-8545(05)70039-5
3. National Institute for Health and Care Excellence (NICE), London. Pelvic floor dysfunction: prevention and non-surgical management. NICE Guideline, No. 210; 2021.
4. Haylen BT, Maher CF, Barber MD, et al. An International Urogynecological Association (IUGA) / International Continence Society (ICS) joint report on the terminology for female pelvic organ prolapse (POP). Neurourol Urodynam. 2016;35(2):137–168. doi:10.1002/nau.22922
5. Digesu GA, Chaliha C, Salvatore S, Hutchings A, Khullar V. The relationship of vaginal prolapse severity to symptoms and quality of life. BJOG. 2005;112(7):971–976. doi:10.1111/j.1471-0528.2005.00568.x
6. Haylen BT, de Ridder D, Freeman RM, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn. 2010;29(1):4–20. doi:10.1002/nau.20798
7. Irwin DE, Milsom I, Hunskaar S, et al. Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol. 2006;50(6):1306–1315. doi:10.1016/j.eururo.2006.09.019
8. Karjalainen PK, Tolppanen AM, Mattsson NK, et al. Pelvic organ prolapse surgery and overactive bladder symptoms—a population-based cohort (FINPOP). Int Urogynecol J. 2022;33(1):95–105. doi:10.1007/s00192-021-04920-w
9. Petros PE, Ulmsten UI. An integral theory of female urinary incontinence. Experimental and clinical considerations. Acta Obstet Gynecol Scand Suppl. 1990;153(Suppl):7–31. doi:10.1111/j.1600-0412.1990.tb08027.x
10. Petros PEP. The Integral Theory System. A simplified clinical approach with illustrative case histories. Pelviperineology. 2010;29(1):37–51.
11. Boer T, Salvatore S, Cardozo L, et al. Pelvic organ prolapse and overactive bladder. Neurourol Urodyn. 2010;29(1):30–39. doi:10.1002/nau.20858
12. Burrows LJ, Meyn LA, Walters MD, et al. Pelvic symptoms in women with pelvic organ prolapse. Obstet Gynecol. 2004;104(5):982–988. doi:10.1097/01.AOG.0000142708.61298.be
13. Dietz HP, Clarke B. Is the irritable bladder associated with anterior compartment relaxation? A critical look at the ‘integral theory of pelvic floor dysfunction’. Aust N Z J Obstet Gynaecol. 2001;41(3):317–319. doi:10.1111/j.1479-828x.2001.tb01236.x
14. Zacharakis D, Grigoriadis T, Pitsouni E, Kypriotis K, Vogiatzis N, Athanasiou S. Assessment of overactive bladder symptoms among women with successful pessary placement. Int Urogynecol J. 2018;29(4):571–577. doi:10.1007/s00192-017-3461-x
15. Coolen AWM, Troost S, Mol BWJ, et al. Primary treatment of pelvic organ prolapse: pessary use versus prolapse surgery. Int Urogynecol J. 2018;29(1):99–107. doi:10.1007/s00192-017-3372-x
16. Johnson JR, High RA, Dziadek O, et al. Overactive bladder symptoms after pelvic organ prolapse repair. Female Pelvic Med Reconstr Surg. 2020;26(12):742–745. doi:10.1097/SPV.0000000000000700
17. Peterson TV, Karp DR, Aguilar VC, et al. Validation of a global pelvic floor symptom bother questionnaire. Int Urogynecol J. 2010;21(9):1129–1135. doi:10.1007/s00192-010-1148-7
18. Manonai J, Wattanayingcharoenchai R. Relationship between pelvic floor symptoms and POP-Q measurements. Neurourol Urodyn. 2016;35(6):724–727. doi:10.1002/nau.22786
19. Kinno K, Sekido N, Takeuchi Y, Sawada Y, Watanabe S, Yoshimura Y. Association between overactive bladder and pelvic organ mobility as evaluated by dynamic magnetic resonance imaging. Sci Rep. 2021;11(1):1–11. doi:10.1038/s41598-021-93143-6
20. Miranne JM, Lopes V, Carberry CL, Sung VW. The effect of pelvic organ prolapse severity on improvement in overactive bladder symptoms after pelvic reconstructive surgery. Int Urogynecol J. 2013;24(8):1303–1308. doi:10.1007/s00192-012-2000-z
21. Yaranun S, Chiengthong K, Ruanphoo P, Bunyavejchevin S. Overactive bladder symptom score changes after pessary insertion in women with pelvic organ prolapse and overactive bladder. Thai J Obstet Gynaecol. 2022;28:1–7.
22. Wu LY, Huang KH, Yang TH, et al. The surgical effect on overactive bladder symptoms in women with pelvic organ prolapse. Sci Rep. 2021;11(1):20193. doi:10.1038/s41598-021-99537-w
23. Padoa A, Levy E, Fligelman T, Tomashev-Dinkovich R, Tsviban A, Serati M. Predictors of persistent overactive bladder following surgery for advanced pelvic organ prolapse. Int Urogynecol J. 2023;34(3):759–767. doi:10.1007/s00192-022-05313-3
24. Liang CC, Hsieh WC, Lin YH, Tseng LH. Predictors of persistent detrusor overactivity in women with pelvic organ prolapse following transvaginal mesh repair. J Obstet Gynaecol Res. 2016;42(4):427–433. doi:10.1111/jog.12927
25. Frigerio M, Manodoro S, Cola A, Palmieri S, Spelzini F, Milani R. Risk factors for persistent, de novo and overall overactive bladder syndrome after surgical prolapse repair. Eur J Obstet Gynecol Reprod Biol. 2019;233:141–145. doi:10.1016/j.ejogrb.2018.12.024
26. Dietz HP, Moegni F, Shek KL. Diagnosis of levator avulsion injury: a comparison of three methods. Ultrasound Obstet Gynecol. 2012;40(6):693–698. doi:10.1002/uog.11190
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Psychological Impact of Quarantine During the COVID-19 Pandemic on Quarantined Non-Healthcare Workers, Quarantined Healthcare Workers, and Medical Staff at the Quarantine Facility in Saudi Arabia
Alfaifi A, Darraj A, El-Setouhy M
Psychology Research and Behavior Management 2022, 15:1259-1270
Published Date: 17 May 2022
Anaemia, Morphological Classification and Its Associated Risk Factors Among Lactating Mothers at Mbarara City Council Health Centre IV, Southwestern Uganda
Clinton O, Micheal K, Namyalo Angella K, Mary M, Mike M, Muwanguzi E, Okongo B, Wagubi R
Journal of Blood Medicine 2022, 13:473-481
Published Date: 2 September 2022
Dry Season Eimeria Infection in Dairy Cattle and Sheep in and Around Adama and Bishoftu Towns, Oromia, Ethiopia
Ayana D, Temesgen K, Kumsa B, Alkadir G
Veterinary Medicine: Research and Reports 2022, 13:235-245
Published Date: 9 September 2022
Chronic Obstructive Pulmonary Disease Prevalence and Associated Risk Factors in Adults Aged 40 Years and Older in Southeast China: A Cross-Sectional Study During 2019–2020
Chen J, Yin Y, Zhang Y, Lin X, Chen T, Yang Z, Wang D, Zhong W
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2317-2328
Published Date: 17 September 2022
Prevalence, Management, and Risk Factors of Asthma Among School-Age Children in Yogyakarta, Indonesia
Triasih R, Setyowireni D, Nurani N, Setyati A
Journal of Asthma and Allergy 2023, 16:23-32
Published Date: 5 January 2023