Back to Journals » Psychology Research and Behavior Management » Volume 16
A Real-World Data Study on the Impact of the ReadRx Cognitive Training and Reading Intervention on Cognition, Basic Reading Ability, and Psychosocial Skills for 3527 Children
Authors Moore AL ![]() , Miller TM, Moore JJ, Ledbetter C
, Miller TM, Moore JJ, Ledbetter C
Received 29 November 2022
Accepted for publication 11 April 2023
Published 17 April 2023 Volume 2023:16 Pages 1195—1220
DOI https://doi.org/10.2147/PRBM.S397665
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Amy Lawson Moore,1 Terissa M Miller,1 Jeffrey J Moore,1 Christina Ledbetter1,2
1Department of Psychology, Gibson Institute of Cognitive Research, Colorado Springs, CO, USA; 2Department of Neurosurgery, Louisiana State University Health, Shreveport, LA, USA
Correspondence: Amy Lawson Moore, Gibson Institute of Cognitive Research, 5085 List Drive, Suite 200-A, Colorado Springs, CO, 80919, USA, Tel +1 719-219-0940, Email [email protected]
Background: The state of reading proficiency among children in the United States continues to be a subject of concern among psychologists, teachers, parents, policy makers, and the education community at large. Despite the widespread use of curricular methods that teach basic reading skills, there remains a large percentage of children that struggle to read. Therefore, novel approaches to reading remediation should be explored.
Purpose: The aims of this study were to examine 1) the effect of a multicomponent cognitive and reading intervention on cognitive and reading skills; 2) the role of ADHD, age, sex, IQ score, and individual cognitive skills on the effectiveness of the ReadRx intervention; and 3) parent-reported behavioral outcomes following the ReadRx intervention.
Methods: The current study analyzed a large real-world dataset to examine cognitive, reading, and behavioral outcomes for struggling readers (n = 3527) who had completed 24 weeks (120 hours) of intense cognitive training integrated with a structured literacy intervention using ReadRx in a one-on-one clinic setting.
Results: Analyses of pretest and post-test scores showed statistically significant changes on all cognitive and reading measures including attention, visual processing, processing speed, long-term memory, working memory, reasoning, phonological awareness, Work Attack, phonetic coding, spelling, comprehension, and overall IQ score with medium to very large effect sizes. The results included an average 4.1-year gain in reading skills including a 6-year gain in phonological awareness. No differences were found based on age, sex, or ADHD status, and minimal differences were found based on pre-intervention IQ score and cognitive test scores. The study also included a qualitative thematic analysis of parent-reported behavioral outcomes revealing themes of improved cognition, academic performance, and psychosocial skills including confidence and perseverance.
Conclusion: Our findings were consistent with previous controlled studies on this intervention and offer an encouraging alternative instructional approach to reading remediation that aligns with the Science of Reading and includes intensive remediation of underlying cognitive skills.
Keywords: cognitive training, brain training, LearningRx, reading, dyslexia, phonemic awareness, literacy, reading disorder
Introduction
According to the Report on the Condition of Education 2021 by the National Center for Education Statistics, only 35% of 4th grade children and 34% of 8th grade children can read proficiently.1 The ability to read and understand text is highly correlated with phonological awareness, or the ability to analyze and manipulate spoken parts of syllables, words, and sentences.2–4 That also includes the most advanced phonological awareness skill of phonemic awareness, or the ability to understand the individual sounds, called phonemes, that make up words. Children with reading struggles may have difficulty discriminating, evaluating, and separating individual phonemes within words. Further, children do not necessarily acquire the ability to segment words into sounds through simple exposure to instruction in reading.2 In fact, reading is not inherently natural. It must be systematically taught for children to correlate spoken sounds with the written codes representing each sound.5,6 This ability is dependent upon an understanding of the alphabetic principle, or the concept that letter and letter clusters represent the sounds in spoken language. When a child learns the predictable and reversible relationships between sounds and letters, they can begin to apply these correspondences to both familiar and unfamiliar words. Learning the alphabetic principle is critical for acquisition of reading and writing because it is necessary for phonological decoding—or the process of converting the written word to the spoken word.7 Once children have received systematic and explicit instruction in phonological awareness and decoding, they can begin to develop fluency and reading comprehension skills.6
Science of Reading
A comprehensive body of reading research across multiple fields of study—collectively known as the Science of Reading—has led to a consensus that skilled reading is the coordination of word recognition skills including decoding, phonological awareness, and sight recognition along with language comprehension skills including verbal reasoning along with knowledge of the structures of language, facts, vocabulary, and print concepts.6 This consensus is grounded in the Simple View of Reading proposed in 1986 by Gough and Tumner7 which states that reading comprehension is the product of word recognition and language comprehension. It was later expounded upon by Scarborough8 in his seminal “Reading Rope” which illustrates how the word recognition skills intertwine with the language comprehension skills to create skilled reading ability. The Science of Reading points to an instructional approach that includes systematic, sequential, and cumulative instruction in phonological awareness, phonics, spelling, fluency, comprehension, and vocabulary delivered with multisensory methods. The importance of beginning with systematic phonics instruction was highlighted by Ehri’s review9 of both research and theory which emphasizes sequential instruction in grapheme–phoneme knowledge, phoneme segmenting and blending, decoding, spelling, contextual word-reading practice, and morpheme-syllable knowledge. Indeed, the Science of Reading serves as the theoretical lens through which reading intervention is now discussed.
Further, as the most widely accepted model of cognition, we should also discuss reading acquisition through the lens of the Cattell–Horn–Carroll theory of cognition10 which identifies reading skills (decoding, fluency, and reading comprehension) as acquired cognitive abilities intricately—and statistically—related to the primary cognitive skills of attention, visual processing, auditory processing, processing speed, long-term memory, working memory, and reasoning. Although there is widespread instruction in basic reading skills, there continues to be a significant problem with reading proficiency as evidenced by the ongoing national assessments of children in the United States. This problem may be because reading struggles are complex and multifaceted rather than simply a deficit in phonological awareness and decoding skills.11,12 In fact, a growing body of research recognizes the complexity of reading skill development and the contribution of multiple cognitive skills to reading ability, particularly working memory13,14 and processing speed,15 but also visuo-spatial ability,16,17 verbal working memory and response inhibition,18 perceptual processing,19,20 sustained attention,21 and executive function.22,23 Not only do cognitive skills influence reading skills acquisition, they also predict response to reading interventions. For example, executive function skills significantly predicted response to the computer-assisted reading intervention, GraphoGame Rime,24 and attention skills differentiated inadequate responders from adequate responders to small group reading intervention.25 Yet, the role of cognitive skills development in school-based reading curricula remains elusive. Considering that CHC theory in relation to reading also aligns with the increasingly popular multiple deficits model in reading—the theory that suggests reading disabilities and their comorbidities result from various deficits in cognitive and linguistic skills,26 it is intriguing that we are not seeing a proliferation of research on multi-construct and individualized reading remediation interventions.
Existing Research on Non-School Reading Interventions
A body of research describing targeted non-school remedial interventions for some of these cognitive skills has emerged but with varying results. For example, Christodoulou27 observed improvements for 6- o 9-year-old children in oral reading fluency and symbol imagery following summer instruction with the Lindamood Bell Seeing Stars program that focuses on visual processing skills like visual symbol recognition. However, the significant interactions between the treatment and control groups on untimed and timed pseudoword reading were due primarily to a decline from pretest to post-test in the control group rather than from improvements in the treatment group. In another study of a non-school-based intervention, Maehler14 examined the effects of the AGENT 8-1-0 working memory training program on three aspects of working memory, finding no significant improvements in working memory among children with dyslexia nor any transfer to academic performance. A recent meta-analysis of programs based on the Orton–Gillingham approach28 revealed a lack of significant improvement in foundational reading skills. However, Lipowska29 studied the Warnke Method of improving reading by training central auditory and visual processing skills in children with dyslexia, finding improvements in short-term phonological memory and phonological awareness. So, some interventions with cognitive components are moving the needle on at least a couple of reading skills.
Existing Research on Predictors of Reading Intervention Outcomes
Unfortunately, there is little published science on multi-component cognitive training interventions delivered one-on-one to remediate struggles with reading and the associated cognitive deficits or research on the characteristics of children that may influence response to such interventions. According to the Cumulative Risk and Resilience Model of dyslexia,30 there is a complex interplay between multiple risk factors (genetics, early language difficulties, environment, low-quality literacy instruction) and multiple protective factors (high-quality literacy instruction, growth mindset, supportive relationships) that determine the likelihood of developing dyslexia. Given that many variables may be associated with reading intervention outcomes, it is important to examine these relationships.
One key area of reading disability research has focused on comorbid attention deficits. Children with attention deficits frequently struggle with reading, as evidenced by studies including one with a sample size of more than 4000 children with ADHD who were found to be at significantly greater risk of difficulty spelling and reading compared to children without ADHD.31 The multiple deficits model has been used as a framework for research examining this comorbidity which has shown that deficits in processing speed32 and executive functions33 partially explain this association between dyslexia and ADHD.34 A large meta-analysis revealed processing speed, verbal working memory, and response variability as the shared cognitive connection between ADHD and reading disabilities.35 This line of research reveals considerable overlap in deficits among children with dyslexia and ADHD. However, to our knowledge, the only meta-analysis to date of reading interventions for children with ADHD in special education settings revealed positive effects but found no use of evidence-based practices and was limited to a total of 65 participants across 16 studies.36 Considering the comorbidity of word reading disabilities and attention deficits is estimated to be between 25% and 50% of children with reading difficulties,37,38 it is important to look at attention struggles as a predictor of response to reading intervention.
There is also evidence that executive function39 and IQ score40 are associated with reading ability, but research on how response to intervention is influenced by IQ score is mixed.41,42 For example, despite research that refutes the idea that low IQ score contributes to reduced response to reading intervention,43 other researchers have found that IQ does have at least a minimal influence on intervention response,42,44 especially with more complex tasks.45 Therefore, it is important to look at IQ score as a predictor of reading intervention response in a large sample.
Sex differences in reading are also important to evaluate. In an analysis of three decades of reading achievement data taken from the National Assessment of Educational Progress,46 researchers found small differences in reading achievement by sex in Grade 4 but increased by Grade 8 and even further by Grade 12 with girls achieving higher scores on reading measures than boys at all three time points. Therefore, it is also essential to assess differences in response to a reading intervention based on sex. Finally, there is intriguing research that indicates reading struggles persist with age. For example, in a study of children with dyslexia, phonological awareness deficits were greater at age 17 than at age 8.47 As the latest report from the National Center for Education Statistics indicated, a smaller percentage of 8th grade children were proficient in reading than 4th grade children.1 Although the Matthew Effect—a phenomenon where there is a tendency for strong readers to become even stronger while weak readers fall further behind over time—may account for much of this trend,48 it is still important to examine the influence of age on response to a reading intervention.
Current Study
The current study addresses this gap by examining a large dataset from children who have completed ReadRx,49 a structured reading intervention integrated with a multicomponent, one-on-one cognitive training intervention called ThinkRx.50 The effectiveness of ThinkRx and ReadRx has been examined in prior research. For example, in four controlled studies, children who completed ThinkRx had statistically significant changes across multiple cognitive skills including visual processing, auditory processing, processing speed, long-term memory, working memory, reasoning, and IQ score.51–55 In one study of ReadRx52 with children ages 5–18, researchers found statistically significant differences between treatment and controls in Word Attack and phonetic coding skills. Jedlicka53 examined parent-reported improvements in academic skills and oppositional behavior following ReadRx training for children and discovered statistically significant differences compared to controls. The current study of ReadRx will be the first to measure seven cognitive skills plus five reading skills and to analyze qualitative outcomes which are critical for identifying the transfer effects of the intervention.
The aims of the current study were to examine 1) the effect of a multicomponent cognitive and reading intervention on cognitive and reading skills; 2) the role of ADHD, age, sex, IQ score, and individual cognitive skills on the effectiveness of the ReadRx intervention; and 3) parent-reported behavioral outcomes following the ReadRx intervention. For Aim 1, our goal was to examine outcome variables that had not yet been explored in research on ReadRx. Because prior research on the intervention documented significant improvements in Word Attack and phonetic coding (sound blending) skills,52 we expected to find similar improvements in phonological awareness, spelling, and comprehension skills. For Aim 2, we were interested in examining predictors of ReadRx outcomes. Because the existing research is equivocal on variables that predict response to reading interventions, we were intrigued by the possibility of finding significant predictors such as age, sex, IQ score, and ADHD status. Further, the role of individual cognitive skills such as attention and processing speed have previously influenced response to reading intervention while memory56 has not. Therefore, we expected to find an influence of some of these variables but potentially not others on the current study’s outcomes. Our dataset is large and lent itself to identifying these trends well. Finally, for Aim 3, we wanted to identify trends in parent-reported behavioral outcomes following ReadRx and were interested to see if there were differences based on age (younger versus older children) or by the presence of an ADHD diagnosis. Although previous research on ReadRx documented quantitative survey-based behavioral changes,53 no ReadRx study had examined open-ended responses from parents on exit surveys. Because prior research on the ThinkRx cognitive training part of the ReadRx intervention had documented parent-reported improvements in self-confidence, self-esteem, cognition, behavior, and academic performance,55 we expected to find similar themes in the qualitative analysis of the parent-reported outcomes in the current study. We did not expect to find large differences based on age group but did expect to see some differences based on ADHD status.
Materials and Methods
Procedures
After obtaining approval from the Institutional Review Board (IRB) at Gibson Institute of Cognitive Research to conduct the study, anonymized data were collected from a centralized database used by LearningRx centers around the United States. Similar to an electronic medical records system, the database houses demographics and assessment results for all children who participate in an intervention at any LearningRx center. The dataset was transferred to the research team on an EXCEL spreadsheet with the following information: age, birthdate, sex, ethnicity, diagnosis, pre-test and post-test dates, pre-test and post-test standard scores, percentiles, W scores, and age-equivalent scores from the Woodcock Johnson III Tests of Cognitive Abilities57 and Tests of Achievement58 and exit survey parent comments. All information on the EXCEL spreadsheet except for the parent comments was uploaded into SPSS for statistical analysis by the quantitative members of the research team. The parent comments were given to the qualitative members of the research team for thematic coding and analysis. No identifying information was included in the datasets used for analysis, and the intake forms completed by parents at LearningRx centers include permission to use de-identified child data for research purposes.
Sample
The sample for the current study includes 3527 children from 93 learning centers around the United States called LearningRx. LearningRx is a worldwide network of learning centers that specializes in cognitive training along with reading and math remediation programs. The dataset is comprised of records from children ages 6–18 (M = 11.4, SD = 2.8) identified as struggling readers who completed the ReadRx structured literacy intervention integrated with ThinkRx cognitive training through LearningRx. Struggling readers were defined as those with low pre-intervention achievement scores in reading <25th percentile on at least one of the following tests from the Woodcock Johnson III Tests of Cognitive Abilities or Tests of Achievement: Word Attack, Sound Blending, Sound Awareness, or Spelling Sounds. Forty percent reported a prior formal diagnosis of specific learning disability in reading (n = 437) or dyslexia (n = 973). In addition, 33% (n = 1174) had comorbid attention problems, identified by prior diagnosis of attention deficit hyperactivity disorder (ADHD) as reported by parents on the intake survey. The sample included 60.4% male (n = 2130) and 39.6% female (n = 1397). The racial makeup of the group was 61.7% Caucasian, 5.5% Black, 4.9% Hispanic, 3.0% Asian, 3.0% mixed race, 0.4% Native American, and 21.6% unreported.
Intervention
ReadRx49 is a multi-sensory, sound-to-code structured literacy intervention for ages six and above available at LearningRx centers. ReadRx is a 360-page curriculum delivered one-on-one by a certified cognitive trainer who has a minimum of a bachelor’s degree and 40 hours of training in the delivery of the program. ReadRx includes 120 hours of instruction in 90-minute sessions 3 or 4 days per week for approximately 24 weeks. It is delivered through a cognitive training approach that is integrated with 60 hours of the foundational cognitive training program at LearningRx, called ThinkRx, and 60 hours of ReadRx reading instruction. The ThinkRx portion of the training focuses on remediation of attention, visual processing, processing speed, long-term memory, working memory, and reasoning while the ReadRx portion focuses on building word recognition skills like phonemic and phonological awareness, decoding, and spelling as well as language and reading comprehension skills like vocabulary, structure, syntax, semantics, and reasoning. The ThinkRx portion of the training can be administered as a standalone program, but the ReadRx program is never administered without ThinkRx. The remediation of cognitive skills through the delivery of the ThinkRx part of the program is a key component of the ReadRx intervention and is, therefore, fully integrated into the curriculum.
In addition to providing children with explicit instruction and systematic introduction of skills that follow a planned scope and sequence, trainers provide responsive and immediate feedback throughout a cumulative cycle of repetition and practice. The lessons and drills are multi-sensory by combining speaking, listening, writing, reading, gesturing, and manipulating objects. All children experience the same intervention but at an individualized pace through the training tasks. Children starting with higher skill levels will master the early tasks rapidly, while children with lower skill levels spend more time on the early tasks to achieve mastery before moving on through the curriculum. Children will also vary in the time spent mastering the individual skills with some children needing more practice time than others on each skill. Therefore, the program focuses on where each child is currently performing on each cognitive and reading skill and builds from that point.
Cognitive Skills Training
The first half of the intervention focuses 50% of the time remediating the multiple cognitive skills that underlie reading skill development using the training tasks from the ThinkRx curriculum which has been fully described in our prior research.51,52,54 In brief, the ThinkRx portion of the training includes 23 basic cognitive training tasks each with 10 to 12 variations, providing more than 1000 training activities. A cognitive trainer utilizes a variety of hands-on materials to deliver the intervention face to face across a table. Examples of materials include a metronome, stopwatch, cards with shapes and numbers, Tangram pieces, timed worksheets, and a foot bag. A metronome is a critical aspect of the methodology and paces almost all of the training tasks. This pacing increases intensity, helps to develop sustained attention, incrementally increases processing speed, and serves to minimize mental breaks. A brief description of the basic cognitive training tasks, the skills they target, and how many variations of each task is presented in Figure 1.
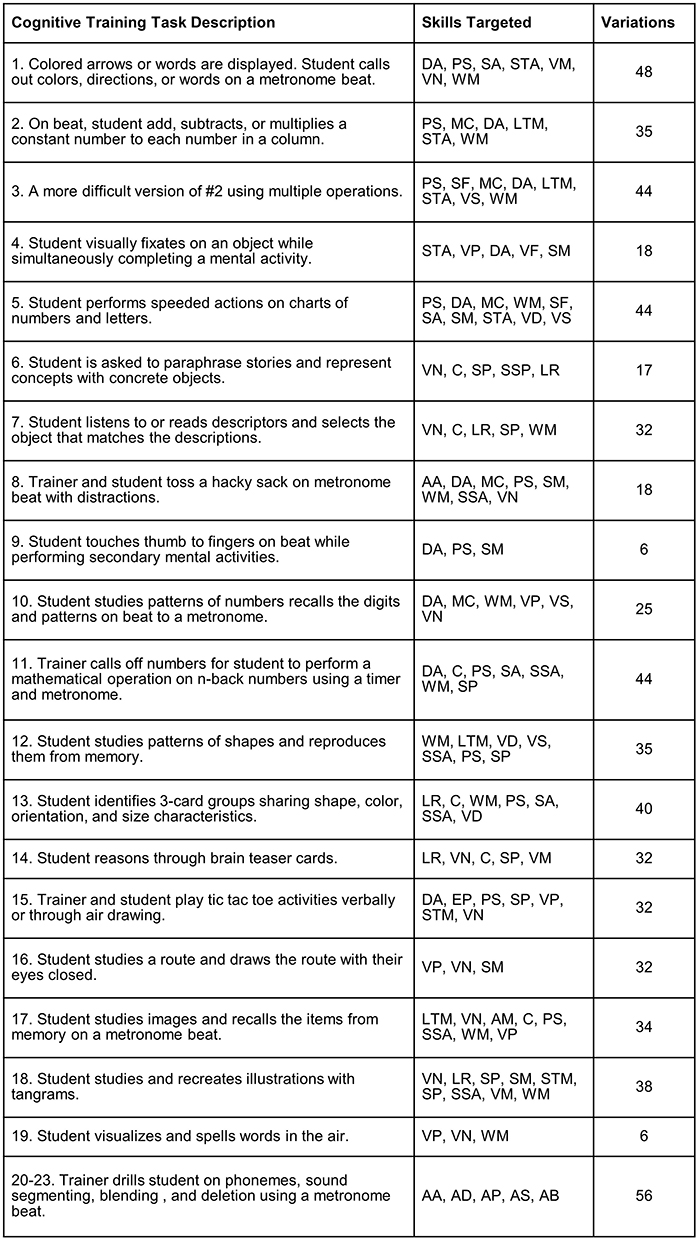 |
Figure 1 Brief descriptions of cognitive training tasks. Abbreviations: AA, auditory analysis; AB, auditory blending; AD, auditory discrimination; AP, auditory processing; AS, auditory segmenting; AM, associative memory; C, comprehension; DA, divided attention; EP, executive processing; LR, logic and reasoning; MC, math computation; PS, processing speed; SF, saccadic fixation; SA, selective attention; SM, sensory‐motor integration; SP, sequential processing; STM, short-term memory; SSP, simultaneous processing; STA, sustained attention; VP, visual processing; VD, visual discrimination; VF, visual fixation; VM, visual manipulation; VN, visualization; VS, visual span; WM, working memory. Notes: Adapted from Carpenter D, Ledbetter C and Moore AL. LearningRx cognitive training effects in children ages 8–14: a randomized controlled study. Applied Cognitive Psychology, 2016:30 (5);815–826. Copyright © 2016 The Authors Applied Cognitive Psychology Published by John Wiley & Sons Ltd. This is an open access article under the terms of the Creative Commons Attribution License.51 |
An example of one memory task is illustrated in Figure 2. In this task, the trainer arranges colorful cards in a pattern on a grid. The child is given just a few seconds to study the arrangement before the trainer covers their grid. Then, the child must create an identical pattern on their own grid from memory while concurrently counting on every other metronome beat. This is 1 of 34 variations on this task which all include the metronome and cards placed on up to nine spaces on each grid. This task also illustrates the multi-sensory nature of the training program. The manipulation of cards engages both visual and motor skills, the metronome requires listening, and verbal responses are also required.
 |
Figure 2 Example of a memory training task. Notes: Reproduced with permission from Gibson K, Carpenter DM, Moore AL, Mitchell T. Training the brain to learn: beyond vision therapy. Vision Dev Rehabil. 2015;1(2):120–129. Copyright 2015 College of Optometrists in Vision Development.52 |
The importance of training cognitive skills along with basic reading skills is based on the Cattell–Horn–Carroll theory of intelligence10 that recognizes the complex, multicomponent view of cognition. Further, multiple cognitive skills are employed while reading and writing, so deficits in individual cognitive skills such as memory,59 processing speed,60 attention,61 and visual processing62 can impact reading skill development and efficiency. For example, despite systematic and sequential reading instruction, a child with deficits in auditory processing or one who struggles with focus and concentration, performs lessons slowly, has trouble remembering, or fails to form mental images may complete schoolwork and tasks inefficiently or exhibit poor retention of information. Therefore, this element of the program–which aligns with the multiple deficit model of dyslexia previously mentioned—is essential for remediating potential cognitive deficits to optimize acquisition of reading skills.
Reading Skills Training
The second 60 hours of the ReadRx portion of the intervention spends 75% of the time on teaching and remediation of reading and spelling skills while reducing the ThinkRx portion to 25%. However, the spelling and reading tasks are delivered using the same cognitive training approach including metronome pacing. ReadRx includes 25 lessons with guided practice beginning with phonemic awareness tasks including sound segmenting, sound blending, and sound deletion using nonsense words, so children do not simply recall memorized words. Trainers also provide direct instruction on how each sound is formed by the lips, teeth, jaw, tongue, and vocal chords.
First, trainers teach 12 consonant sounds with just one primary spelling such as /d/ as in “dig” or “bid”. Next, the trainers teach the other 12 consonant sounds with the most probable spelling such as /ch/ as in “chant” or “such”. Then, trainers teach 18 vowel sounds in order from simple leading to complex. Sounds represented by the letters “a”, “e”, “i”, “o”, and “u” are taught first. Next, the sounds controlled by final “e” and the various sounds represented by the letter “o” are taught. Then, the vowel sounds controlled by the letter “r” are taught.
Once the child has mastered the most likely spelling for every sound, the trainer introduces the less likely alternative spellings. As an example, the /n/ sound might be represented by the letter “n” as in “not”, by “kn” as in “knob”, or by “gn” as in “gnaw”. Repeated drilling of these patterns of letters increases encoding and storage in long-term memory which should reduce guessing in spelling and reading. In addition, visual pictures are added to aid visual memory of these sounds in patterns of commonality tying the visual/auditory connections together aiding effectiveness of memory recall on demand.
Trainers also teach how codes overlap when a letter or a combination of letters represent more than just one sound. As an example, the letter “u” can represent four sounds in different ways such as in “but”, “flute”, “ruin”, or “full”. Instead of memorizing rules and sight words, the child is drilled with multiple exercises to learn how these codes overlap. The drills include decoding, encoding, and writing exercises to teach how the codes are reversible. The active and repeated nature of the drills are designed to increase the automatic recall of codes and code overlaps. This is in contrast to teaching passive lessons which may fall short in generating the automaticity needed for fluent reading and spelling.
Finally, trainers deliver tasks that promote development of vocabulary and language comprehension, including multisyllabic word patterns and multiple meaning words as a critical piece of overall reading skill. In addition, trainers using the ReadRx curriculum implement the following training techniques:
An example of a ReadRx task is illustrated in Figure 3. This is a “Reading Pictures” task that teaches complex code. An early or struggling reader is trained to use pictures or illustrations to help remember alternative spellings for the same sounds. In this example, the sound /o/ uses the code “o” as in the word “octopus” and “a” as in the word “watch”. Whichever picture is larger—in this case the octopus—represents the more common spelling of the sound.
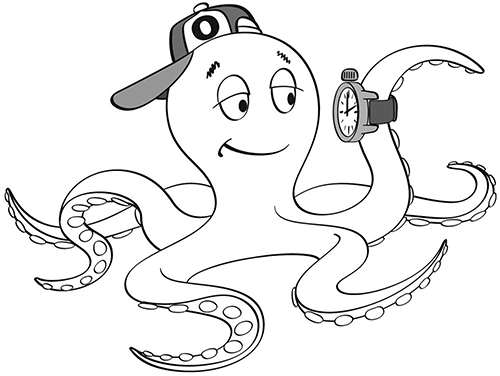 |
Figure 3 Example of a complex code training task. Notes: Reproduced with permission from Gibson K, Carpenter DM, Moore AL, Mitchell T. Training the brain to learn: beyond vision therapy. Vision Dev Rehabil. 2015;1(2):120–129. Copyright 2015 College of Optometrists in Vision Development. 52 |
A key component of the ReadRx program is one-on-one delivery. Each child is paired with a trainer individually for their session. The one-on-one delivery enables individualized goal setting, customized instruction, undivided attention, consistent building of schema and development of a strong therapeutic alliance. This practice is based on the theory of structural cognitive modifiability proposed by Feuerstein63 and on Bandura’s social cognitive theory.64 Feuerstein suggests that providing a mediator between learner and stimulus—called a mediated learning experience—focuses the learner’s attention, helps the learner understand and create meaning for the experience, and assists the learner with applying the new skill outside of immediate experience. The practice is also grounded in Bandura’s work on self-efficacy, or the belief in one’s ability to accomplish a task. Because the program is delivered by a human, the development of self-efficacy can be harnessed. First, a human trainer models the training tasks. The participant can vicariously experience tasks prior to attempt. Second, the human trainer gives the participant verbal persuasion and encouragement in attempting and completing each task. This dynamic feedback is a key element of self-efficacy development. Third, the human trainer assists the participant in responding to the stress of a challenging exercise. The trainer can scaffold or adapt tasks if the participant becomes frustrated or increase difficulty of tasks if the participant appears unchallenged. Finally, the human trainer provides frequent opportunities for mastery of training tasks.
Outcome Measures
Quantitative Assessments
Baseline and post-intervention assessments were conducted using subtests from the Woodcock Johnson III (WJ III) Tests of Cognitive Abilities57 and Tests of Achievement.58 The Woodcock Johnson batteries are widely used in both practice and research and are valid and reliable instruments for use with this population. Tests were administered or supervised by master’s-level clinicians with training in test administration and interpretation and are not administered by the same person who delivers the training to the child. The Woodcock Johnson test battery is a nationally normed test. To calculate the standard scores and age-equivalent scores, the raw scores from each subtest were entered by the test administrator or supervisor into software provided by the test publisher called Compuscore. The age-based standardized scores were then automatically calculated by the software, and a file was generated for download. Then, each score file was uploaded into the LearningRx centralized database following each administration. Below are descriptions of each subtest administered.
Cognitive Assessments
Long-Term Memory
Long-term and associative memory were evaluated with the Visual-Auditory Learning test from the WJ III Tests of Cognitive Abilities. The test requires the child to learn and recall pictographic representations of words presented in sentences. For example, the word “big” is represented by a large diamond shape. Every time the child sees the large diamond shape, they say the word “big”. There are 7 total stories with picture-word associations that children must retell. The median reliability is 0.86 for the ages of children in the current study.
Working Memory
Working memory and attentional capacity were evaluated with the Numbers Reversed test from the WJ III Tests of Cognitive Abilities. The child is presented with multiple series of numbers which increase in complexity and then is prompted to repeat them in reverse order. For example, the examiner will say the numbers “7, 5, 8, 2” and the child will need to repeat them in reverse order as “2, 8, 5, 7”. There are 30 series of numbers on this test. The median reliability is 0.86 for the ages of children in the current study.
Visual Processing
Visual-spatial thinking was measured by the Spatial Relations test from the WJ III Tests of Cognitive Abilities. This test requires the child to identify pieces of a puzzle that form a complete shape. For example, the target stimulus might be a rectangle adjacent to two squares that all combine to form a larger square. The child must identify from an array of choices, which three shapes are exact matches to the three shapes in the target. There are 33 target stimuli to which children must match the individual shapes. The median reliability is 0.81 for the ages of children in the current study.
Fluid Reasoning
Fluid reasoning and inductive logic were measured by the Concept Formation test from the WJ III Tests of Cognitive Abilities. For each item on the test, the child is asked to determine a rule governing a set of shapes and designs. For example, the target stimulus is two large yellow squares and two small yellow squares inside a larger shape. The child needs to determine the rule that governs the two sets of shapes. In this example, the rule would be “two and yellow”. There are 40 stimulus sets for which the child must identify the rule. The median reliability is 0.94 for the ages of children in the current study.
Processing Speed
Processing and perceptual speed were measured by the Visual Matching test from the WJ III Tests of Cognitive Abilities. The child must locate and identify two matching numbers or sets of numbers in each row of 6. For example, the target stimulus is a row of numbers including 27, 12, 49, 27 and 63. The child must identify the two numbers in that row that are the same. In this example, it would be 27. So, the child would mark a line through 27 and 27 to indicate a match. The child has 3 minutes to identify as many matches as possible from a total of 60 stimulus sets. The median reliability is 0.89 for the ages of children in the current study.
Attention
Sustained attention and executive processing were measured using the Pair Cancellation test from the WJ III Tests of Cognitive Abilities. In a 3-minute limit, the child must find and place a mark through a repeated pattern in each row. For example, the target stimulus is a page of dogs, soccer balls, and coffee cups in various combinations of pairs. The child must find all the pairs on the page that match the target stimulus pair. There are 69 possible pairs to identify correctly. The median reliability is 0.86 for the ages of children in the current study.
IQ Score
IQ score, or general intellectual ability, is a weighted composite of Tests 1 through 7 of the WJ III Tests of Cognitive Abilities Standard Battery including Comprehension Knowledge, Visual-Auditory Learning, Spatial Relations, Sound Blending, Concept Formation Visual Matching, and Numbers Reversed. The median reliability is 0.98 for the ages of children in the current study.
Reading Assessments
Phonological Awareness
Phonological awareness was assessed using the Sound Awareness test from the WJ III Tests of Achievement. This 4-part test includes rhyming, deletion, substitution, and reversal tasks. The rhyming task requires the child to identify the word that rhymes with the stimulus word and in later items produce a word that rhymes with the stimulus words. For example, the examiner would ask for a word that rhymes with “goat”. The deletion task requires the child to remove part of the stimulus word to make a new word. For example, the examiner prompts the examinee to say the word “cat” without the /k/ sound. The substitution task requires the child to substitute part of the stimulus word to make a new word. For example, the examiner prompts the examinee to change the /s/ in “sack” to /b/. The reversal task requires the child to swap parts of the stimulus word to make a new word. For example, the examiner prompts the examinee to say the sounds in the word “tire” backward. The median reliability is 0.81 for the ages of children in the current study.
Word Attack
The Word Attack test from the WJ III Tests of Achievement measures ability to read words or letter combinations by applying knowledge of decoding and word structure. The test requires the child to read nonsense or low-frequency words presented in a list on a flip chart. For example, the child must read words like “flib” and “bungic” to demonstrate knowledge of English language patterns. The median reliability is 0.87 for the ages of children in the current study.
Spelling
Spelling, phonological coding, and orthographic coding were measured using the Spelling Sounds subtest from the WJ III Tests of Achievement. This written test requires the child to listen to sound combinations and nonsense words and then spell them correctly. Examples include nonsense words like “smuff” and “barches”. The median reliability is 0.74 for the ages of children in the current study.
Phonetic Coding
The auditory processing skill of phonetic coding was measured using the Sound Blending test in the WJ III Tests of Cognitive Abilities Standard Battery. The task requires children to listen to a sequence of phonemes and then orally blend those sounds to make a word. For example, the child hears the sounds /c/-/a/-/t/ and must say the word “cat”. The median reliability is 0.86 for the ages of children in the current study.
Comprehension
Reading comprehension was assessed with the Passage Comprehension test from the WJII Tests of Achievement. The test requires to first match pictures with corresponding words, then to identify a picture as described by a phrase, and finally to silently read increasingly more complex passages and identify the missing word in each one. For example, an early passage is, “Martha had her wet swimsuit in the closet. She was hoping that her parents would not find out that she had gone _________”. From a list of words, the child choose the word that best fits in the blank. There are 47 passages and the median reliability is 0.83 for the ages of children in the current study.
Qualitative Exit Surveys
After each child completed the ReadRx® program at a LearningRx center, parents were asked to complete an exit survey. The survey link was emailed to the parent of each child upon completion of the program. When the parent visits the link, they are asked a set of questions about their experience at the learning center. For example, they are asked to rate their experience with their child’s cognitive trainer and the director. They are also asked how likely they would be to recommend the program to a friend. At the end of the survey, there is an open-ended question requesting them to answer the following: “Please share with us the changes you have seen in your child as a result of the LearningRx training”. These open-ended responses were collected by researchers for thematic analysis.
Data Analyses
Quantitative Data Analyses
All quantitative data analyses were conducted using IBM SPSS Statistics 28. To test for significant differences between pretest and post-test scores within each group of struggling readers, we performed paired samples t-tests on the standard scores. Effect sizes indicate the practical significance of score gains and are reported in Cohen’s d which can be interpreted as small = 0.2, medium = 0.5, and large = 0.8. Effect sizes over 0.9 are considered “very large”.65 A Bonferroni-corrected alpha of p < 0.004 was used to control for 12 comparisons. In addition to significance testing on standard scores, we also performed paired samples t-tests on age-equivalent scores for each reading measure as a simpler metric by which the current reading intervention might be compared to other structured reading program gains.
To assess predictors of reading outcomes, we conducted multiple regression analyses using post-intervention scores in phonological awareness, Word Attack, spelling, phonetic coding, and comprehension scores as our outcome variables and pretest reading scores, presence or absence of ADHD, age, sex, pre-intervention IQ score, and pre-intervention scores on the individual cognitive skills of attention, working memory, long-term memory, visual processing, processing speed, and fluid reasoning as our predictor variables.
Analyses of outcomes on all cognitive measures and four of the reading measures (phonological awareness, Word Attack, spelling, and phonetic coding) were performed on the entire sample of n = 3527. The sample size for the comprehension measure is smaller (n = 296) because the subtest is not required to be administered to ReadRx clients at the learning centers in our study. The comprehension measure is typically only administered to clients participating in a separate advanced reading comprehension intervention at LearningRx (called ComprehendRx). However, several test administrators within the system prefer to administer the complete battery of Woodcock Johnson subtests to all clients regardless of the program in which they are enrolled. Therefore, we included the comprehension measure as exploratory since it was interesting to examine the available data.
Qualitative Data Analyses
The dataset for our qualitative analysis was composed of parent-reported outcomes following the ReadRx intervention. The use of parent-reported outcomes in real-world data studies and qualitative or mixed-methods research on perceived child outcomes is common66–68 because knowledge of parent reported outcomes can help improve program delivery, help researchers understand the participant experience, and communicate the day-to-day impact of interventions beyond what can be seen on standardized tests. The qualitative data were collected from a web-based exit survey using responses to the following question: “Please share with us the changes you have seen in your child as a result of LearningRx training”. The qualitative researchers were blind to the characteristics of the participants. Responses were analyzed using inductive thematic analysis. Two researchers independently coded data at the phrase level and met to discuss and determine themes which were then analyzed by age group (older and younger) and by ADHD status.
Results
Effects on Cognitive and Reading Skills
Our first objective was to examine if struggling readers improved significantly on tests of basic reading skills and cognitive skills after 24 weeks of ReadRx, an intensive structured literacy intervention with integrated cognitive training. Using paired samples t-tests on pretest and post-test scores, analysis indicated statistically significant changes from pretest to post-test on all five reading measures and all seven cognitive measures. Table 1 illustrates the pretest scores, post-test scores, standard deviations, significance testing results, and effect sizes for each variable. Effect sizes range from medium to very large with smallest effects found for spelling (0.56) and processing speed (0.68). The largest effects can be seen in overall IQ score (1.68) and phonological awareness (1.37) followed closely by long-term memory (1.10), fluid reasoning (1.08), broad attention (1.08), Word Attack (1.05), and phonetic coding (0.99)—all of which show very large effect sizes.
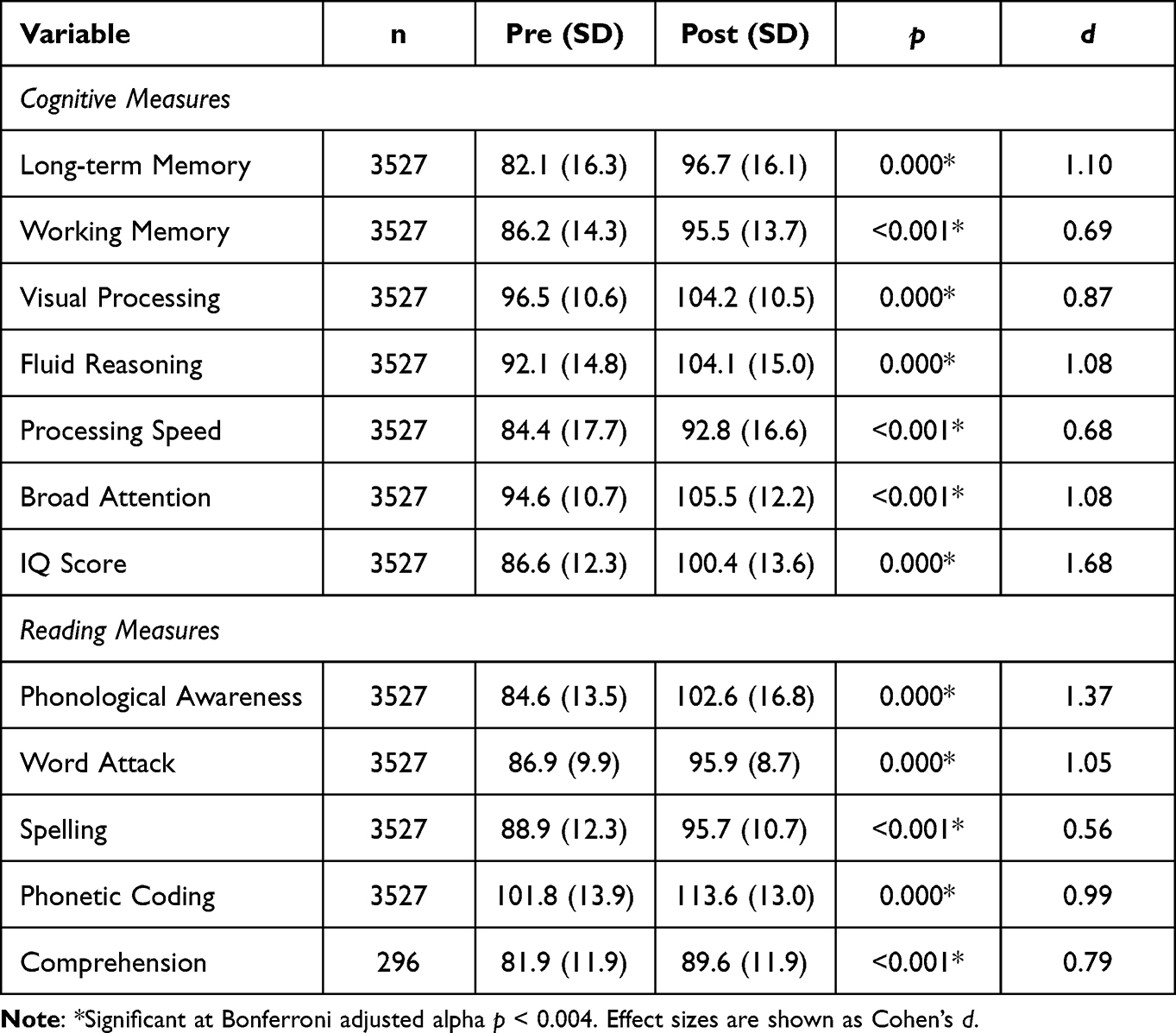 |
Table 1 Paired Samples t-tests for Cognitive and Reading Outcome Measures in Standard Scores |
To report a metric that will make comparisons with other reading programs easier, we also examined changes in age-equivalent scores for the reading measures. Paired samples t-tests revealed statistically significant changes in age-equivalent scores on all five reading measures with medium to very large effect sizes (0.59 to 1.0). Table 2 illustrates the mean change in age-equivalent scores on the five reading measures. The average change was 4.07 years. The largest age-equivalent gain was in phonological awareness (5.8 years) and the smallest gain was in spelling (2.2 years).
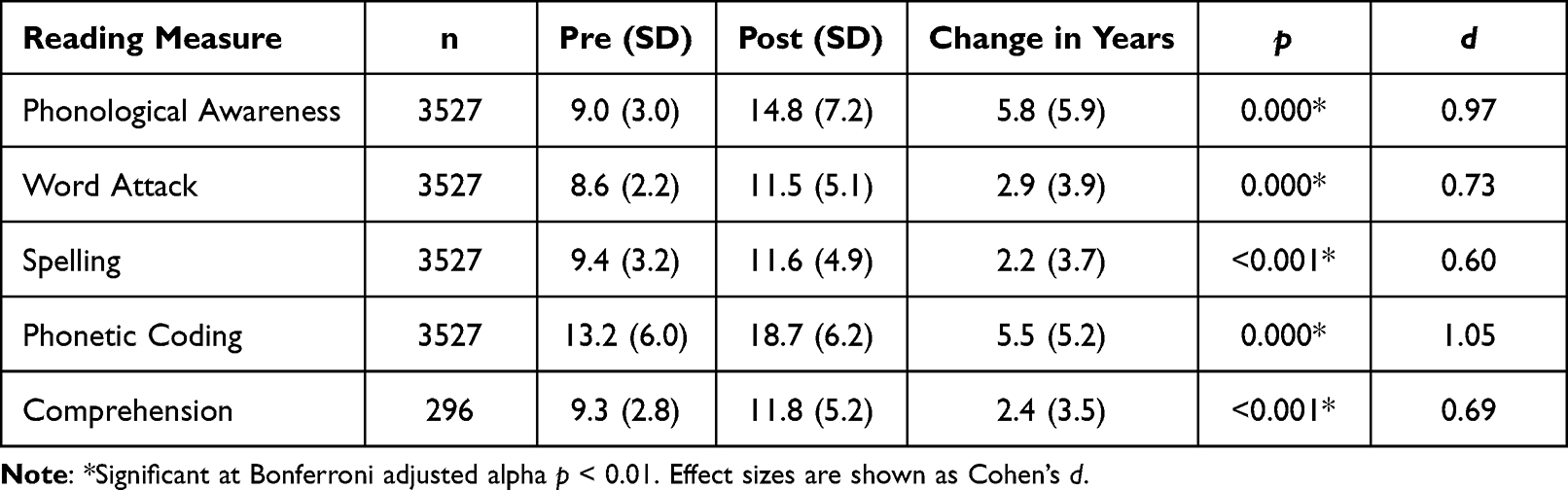 |
Table 2 Age-Equivalent Change in Reading Skills |
Predictors of Change in Reading Scores
Our second objective was to examine if the presence or absence of ADHD, age, sex, or pre-intervention IQ score predicted basic reading skill response to the ReadRx intervention for struggling readers. We also examined if pre-intervention scores of the individual cognitive skills of attention, working memory, long-term memory, processing speed, visual processing, or fluid reasoning predicted response to the intervention as well. We ran multiple regression analyses using post-intervention scores on phonological awareness, Word Attack, spelling, phonetic coding, and comprehension scores as our outcome variables and presence or absence of ADHD, age, sex, pre-intervention IQ score, and pre-intervention scores on tests of attention, working memory, long-term memory, processing speed, visual processing, or fluid reasoning as our predictor variables. In each regression model, we also included the associated pretest score for each reading outcome to control for any differences at pretest. The significance threshold was set at p<0.004 after Bonferroni correction for the 11 comparisons in each model. The results are shown in Tables 3 through 7.
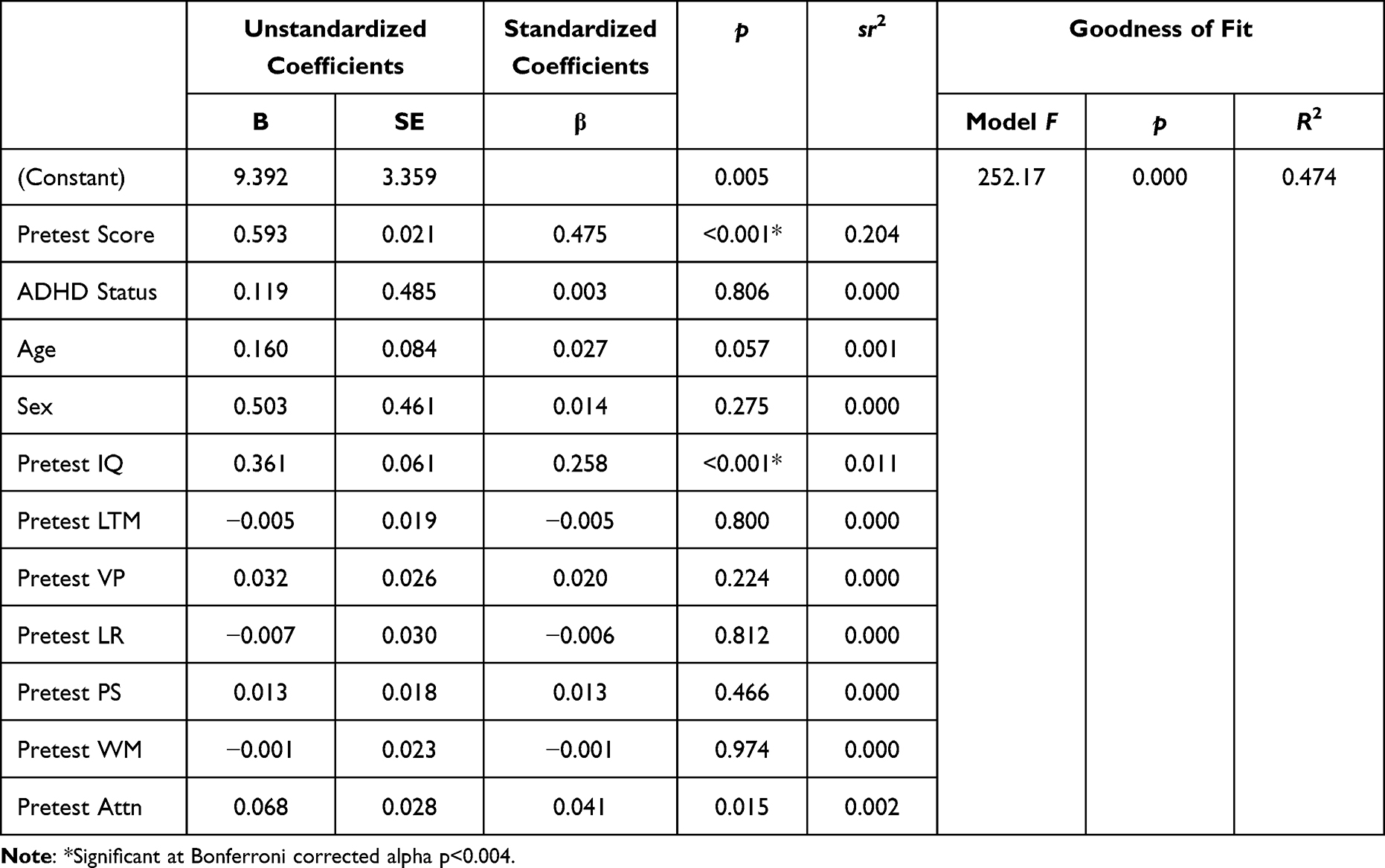 |
Table 3 Predictors of Change in Phonological Awareness Scores |
Predictors of Phonological Awareness Outcomes
For predictors of phonological awareness outcomes, the overall regression model was significant. A look at the contribution of the individual predictors (Table 3) revealed that IQ Score was a significant predictor of change in phonological awareness scores but only about 1% of the variance in the post-intervention phonological awareness scores can be explained by IQ score, and none of the variance was explained by ADHD, age, sex, or the individual cognitive skill levels at pretest after controlling for pretest phonological awareness scores which accounted for about 20% of the variance.
Predictors of Word Attack Outcomes
For predictors of Word Attack outcomes, the overall regression model was significant. A look at the contribution of the individual predictors (Table 4) revealed that pre-intervention scores on tests of processing speed and working memory were significant predictors of change in Word Attack scores. However, each skill explained less than 1% of the variance in the post-intervention Word Attack scores, and none of the variance was explained by IQ, ADHD, age, sex, or the individual pretest scores on tests of attention, visual processing, long-term memory, or fluid reasoning after controlling for pretest Word Attack scores which accounted for 31% of the variance.
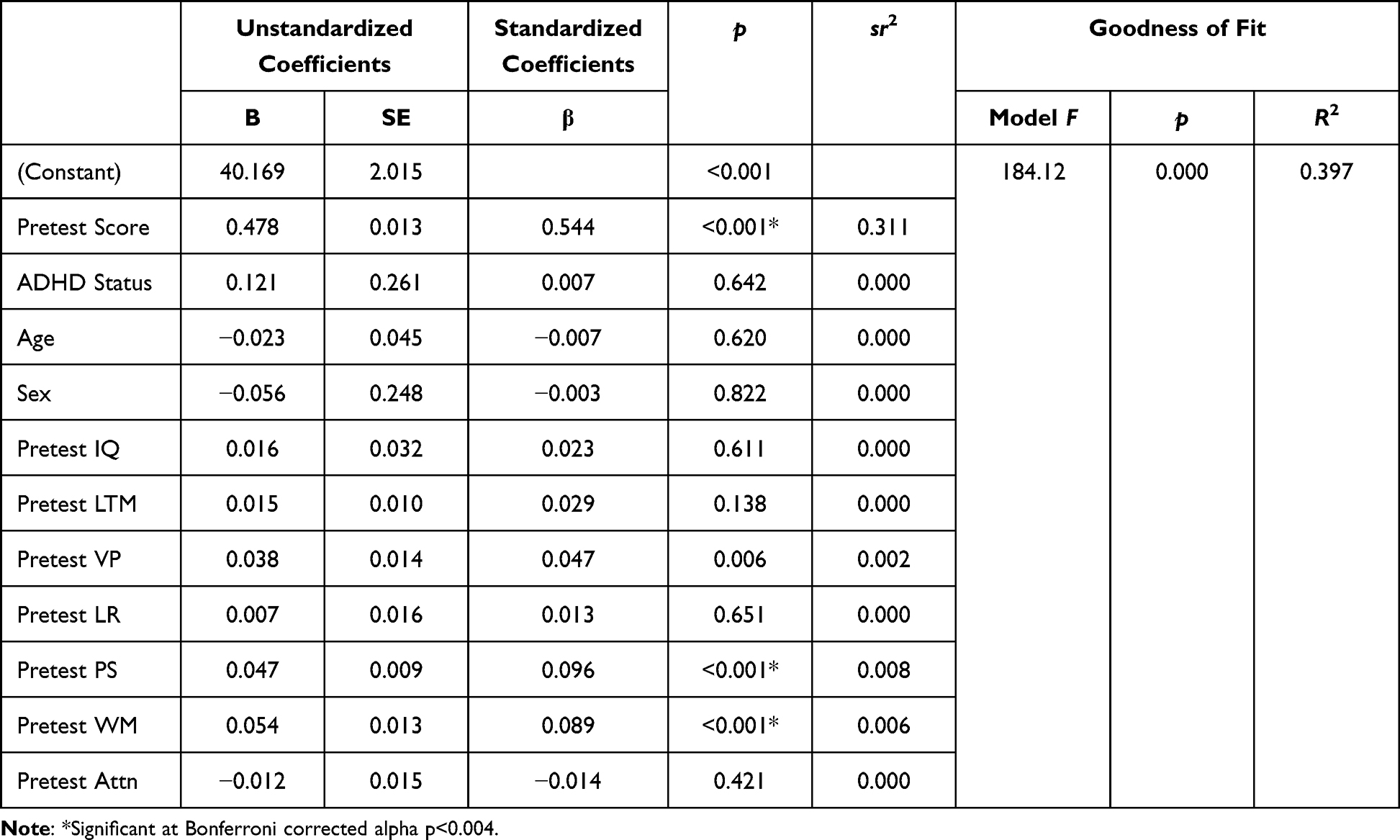 |
Table 4 Predictors of Change in Word Attack Scores |
Predictors of Spelling Outcomes
For predictors of spelling outcomes, the overall regression model was significant. A look at the contribution of the individual predictors (Table 5) revealed that only IQ score was a significant predictor of change in spelling scores. However, just 0.6% of the variance in post-intervention spelling scores can be explained by IQ score, and none of the variance was explained by ADHD, age, sex, or the individual cognitive skill levels at pretest after controlling for pretest spelling scores which accounted for about 18% of the variance.
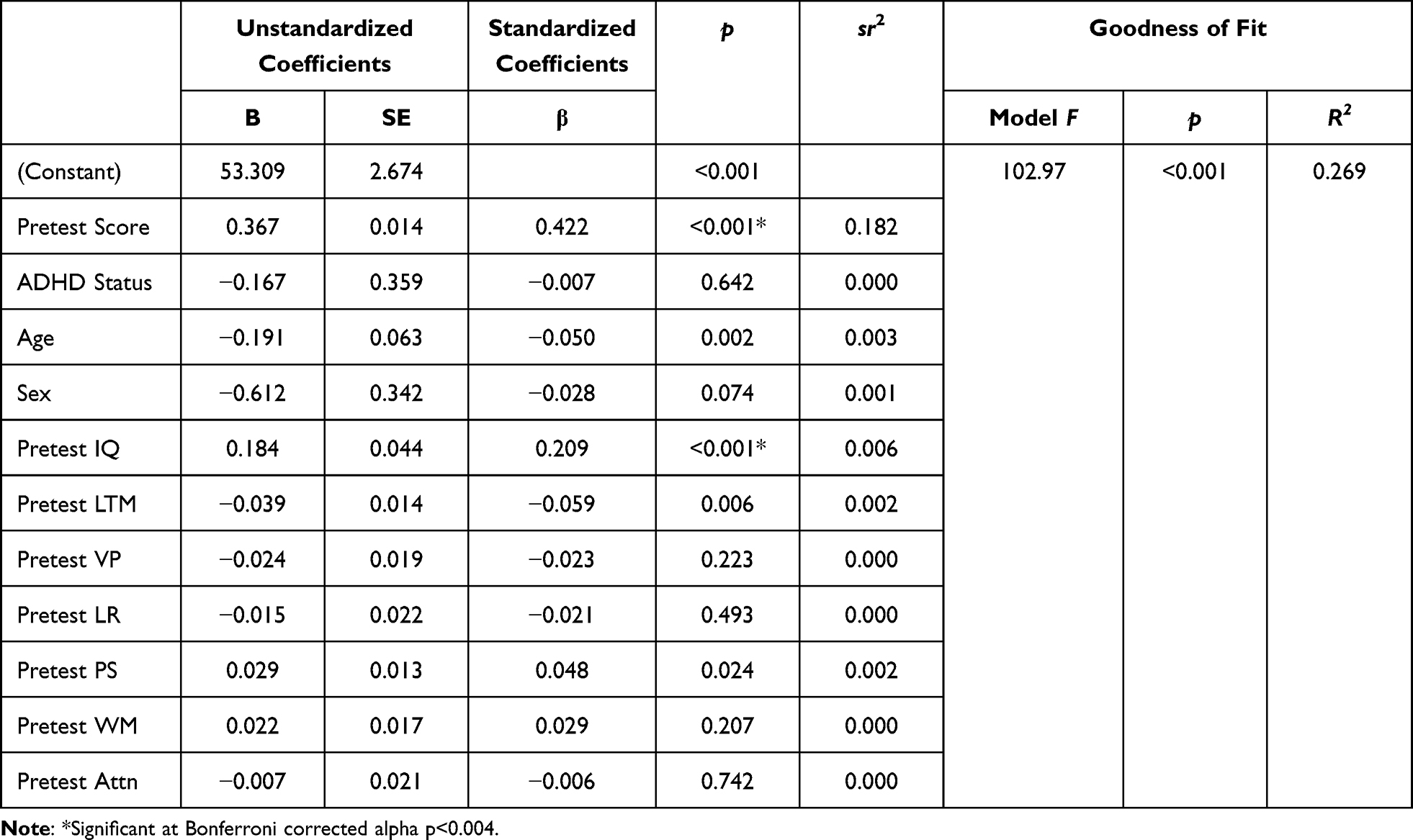 |
Table 5 Predictors of Change in Spelling Scores |
Predictors of Phonetic Coding Outcomes
For predictors of phonetic coding outcomes, the overall regression model was significant. A look at the contribution of the individual predictors (Table 6) revealed that only IQ score was a significant predictor of change in phonetic coding scores. Just 0.4% of the variance in the post-intervention phonetic coding scores can be explained by IQ score, and none of the variance was explained by ADHD, age, sex, or the individual cognitive skill levels at pretest after controlling for pretest phonetic coding scores which accounted for about 19% of the variance.
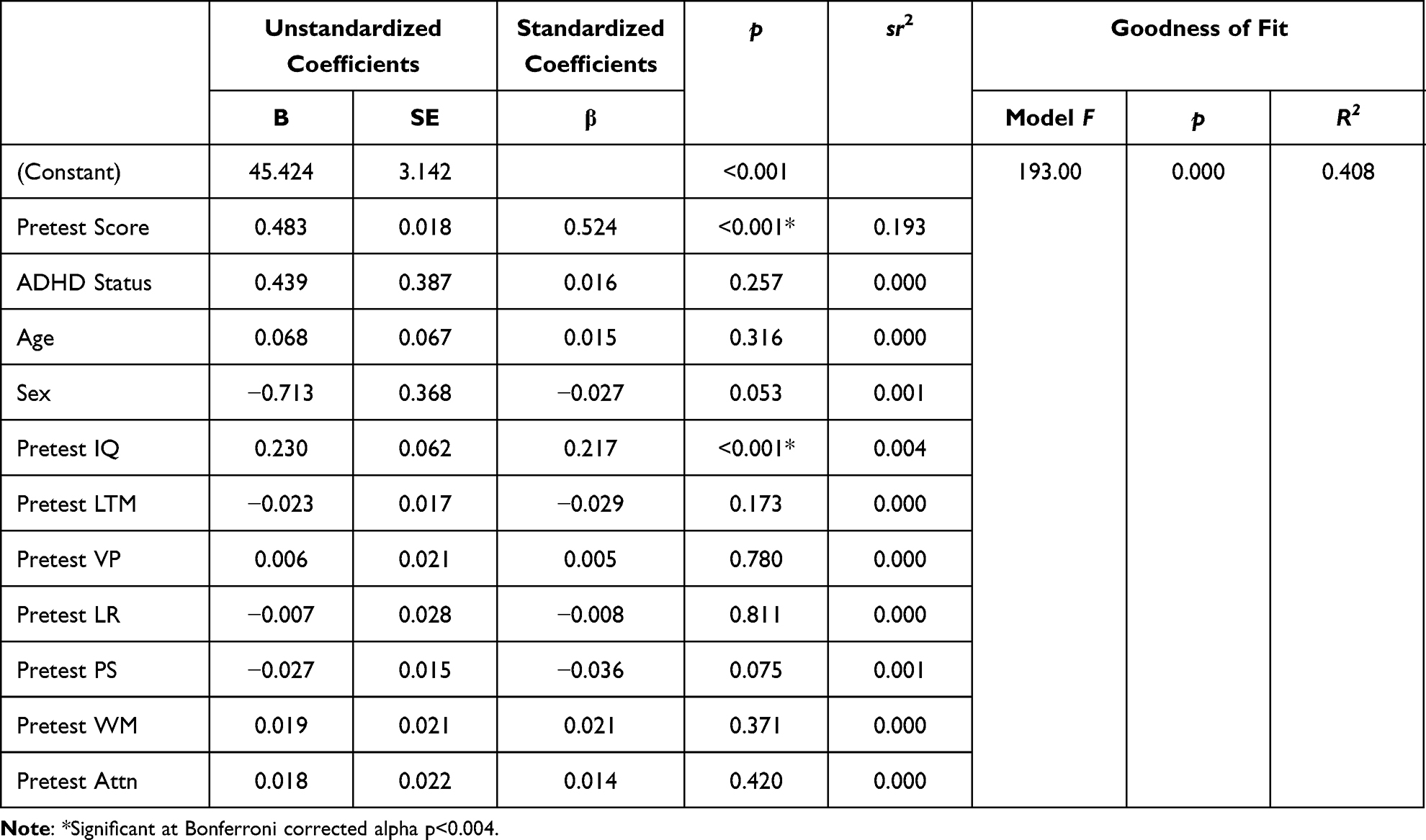 |
Table 6 Predictors of Change in Phonetic Coding Scores |
Predictors of Comprehension Outcomes
For predictors of comprehension outcomes, the overall regression model was significant. A look at the contribution of the individual predictors (Table 7), however, revealed no significant predictors in post-intervention comprehension scores after controlling for pretest comprehension scores which accounted for 30% of the variance.
 |
Table 7 Predictors of Change in Comprehension Scores |
Qualitative Analysis of Parent-Reported Outcomes
Themes and Subthemes of Parent-Reported Outcomes
Our third goal of the current study was to examine parent-reported outcomes, or changes parents saw in their children at the end of the intervention period. Of 3527 records comprising this sample, 85% (n = 3009) completed an exit survey following completion of the intervention. Of the surveys completed, 57% (n = 1723) of them included comments. Those comments were used for our thematic analysis of qualitative outcomes. The analysis revealed 75% (n = 1299) of parents reported psychosocial changes, 66% (n = 1140) of parents reported improved school performance, and 36% (n = 612) of parents reported improvements in cognition. Table 8 breaks down the percentage of comments coded in each theme and subtheme, and we share representative comments in the section below.
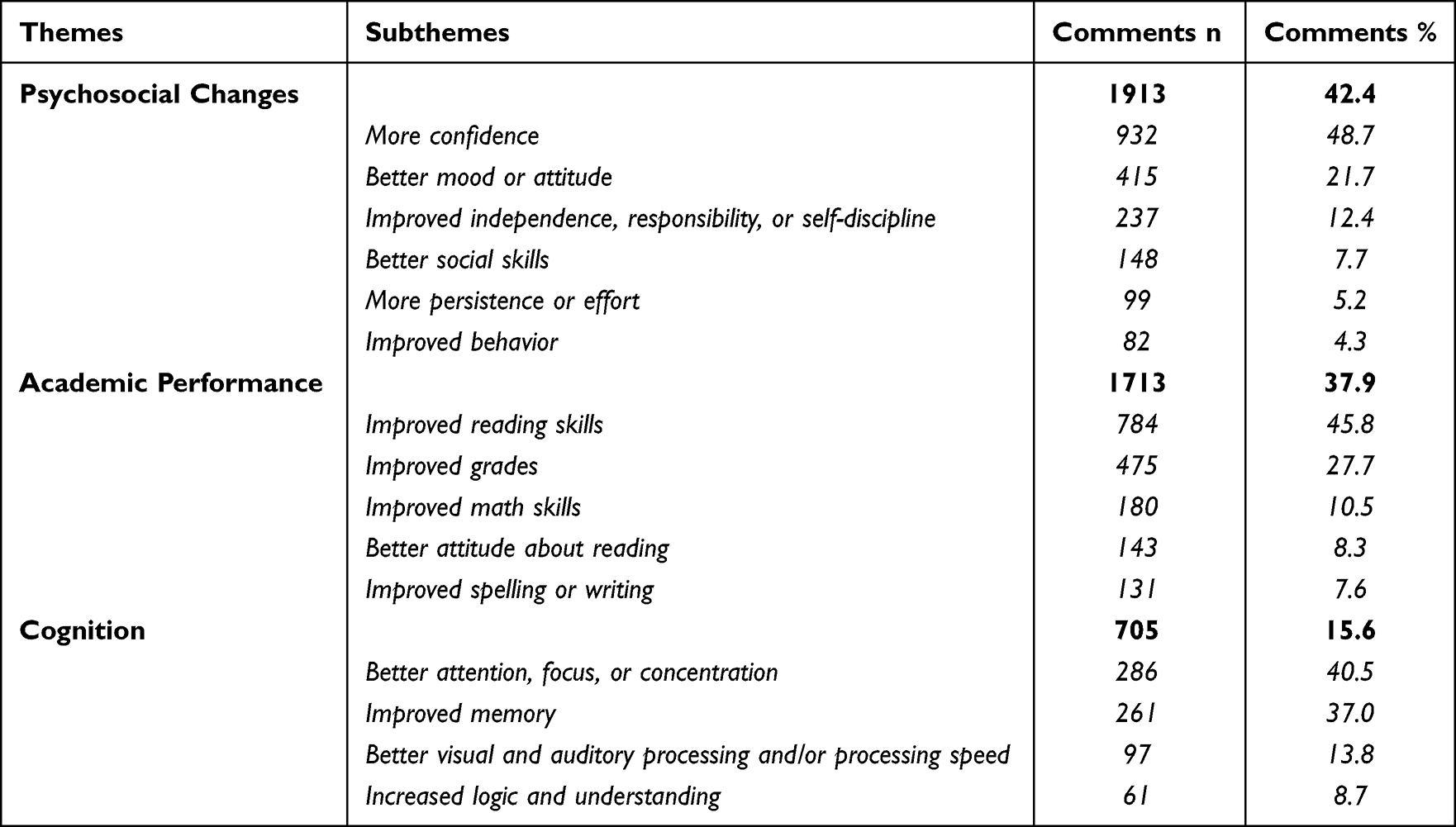 |
Table 8 Qualitative Themes and Subthemes |
Psychosocial Changes
Thematic analysis revealed the greatest number of exit survey comments regarding psychosocial changes. Examples included behavioral improvements at home and increased persistence and effort, such as “she has become more determined and persistent”. Comments from parents reporting improved social skills mentioned “new friends”, “improved socialization”, “less shy”, “more talkative”, and “engages more with classmates”. Other psychosocial comments referred to greater responsibility, independence, and/or self-discipline. Some of the parents stated, “she does her homework without prompting from me”, “more organized and responsible at school and home”, and “now has the self-discipline to complete his work on time”. There were additional psychosocial remarks about children having a better mood or attitude, such as, “not as frustrated”, “hopeful now and looking forward to college”, and “finally, happy child”!
By far the most prevalent response was regarding confidence. Forty-nine percent (n = 932) of the psychosocial comments were about increased self-esteem and confidence, such as “so much more confident”, “her self-esteem has sky-rocketed”, “increased confidence in school, sports, friendships, and at home”, and “he now has the fortitude and confidence to tackle obstacles and succeed in life”!
School Performance
Parents reported improved reading skills and comprehension, including remarks about a better attitude toward reading stating, “our child reads with ease now”, “finally reading confidently at grade level”, and “he is reading chapter books, and wants to check out books from the library!” Parents also reported spelling and/or writing improvements citing “better spelling grades”, and “her writing has improved so much”. School performance comments included general improvements in grades or academic achievement, with responses like “ACT scores improved…accepted into college”, and “she went up two grade levels, now on track!”
Cognition
In addition to specific grade-related comments, parents reported general changes in cognition. Parents who commented about improved cognition said things like, “she is remembering things better at home and at school”, “better reasoning and thinking through problems”, “my son has found new techniques for learning – the visualization processing technique has been priceless”, “he displays a longer attention span”, and “concentrates better in school”.
Additional Comments
Several comments did not fit into the themes identified. For example, 2.6% of the comments were negative. Parents wrote things such as, “the cost is more than most people can afford” or “the time commitment was hard”. Another suggested “better communication from the trainer” and one indicated “we had hoped for better results”. About 1% of the comments referenced improvements in sports, music, or other extracurricular activities, such as “doing better in piano”, “soccer coach noticed more focus on the plays”, and “increased attention in choir”.
Comparison of Parent-Reported Outcomes by ADHD Status
We also analyzed differences in the percentage of parent-reported outcomes in each theme based on ADHD status of the student and noted minimal variation between struggling readers with attention problems and struggling readers without attention problems as shown in Figure 4.
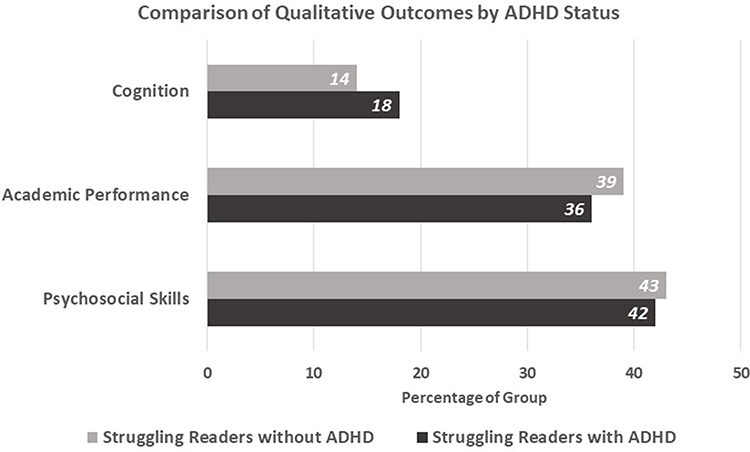 |
Figure 4 Percentage of students with and without ADHD reporting improvements in each qualitative theme. |
Comparison of Parent-Reported Outcomes by Age
Next, we explored the difference in parent-reported outcomes by age. A comparison of qualitative themes between younger and older children in the sample indicated a difference between age groups in the percentage of reporting changes in school performance but showed little variation between age groups on reporting psychosocial changes and improvements in cognition (Figure 5).
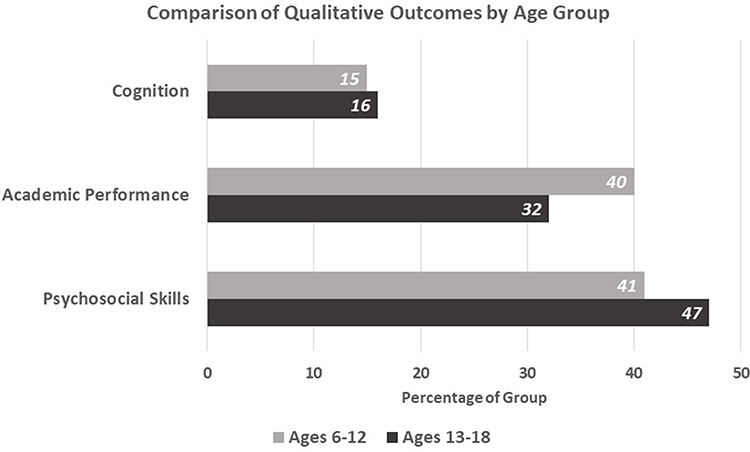 |
Figure 5 Percentage of each age group reporting improvements in each qualitative theme. |
Discussion
The objectives of the current study were to examine 1) the effect of a multicomponent cognitive and reading intervention on cognitive and reading skills; 2) the role of age, sex, ADHD, IQ score, and individual cognitive skills (attention, working memory, long-term memory, visual processing, processing speed, fluid reasoning) on the effectiveness of the ReadRx intervention; and 3) parent-reported outcomes following the ReadRx intervention. The sample for the current study included 3527 children including 1174 with a prior diagnosis of ADHD. Baseline and post-intervention assessments were conducted using subtests from the Woodcock Johnson III (WJ III) Tests of Cognitive Abilities and Tests of Achievement, including the cognitive measures of working memory, long-term memory, processing speed, visual processing, fluid reasoning, and attention; and the reading measures of phonological processing, Word Attack, phonetic coding, and spelling. A subset of the sample (n = 296) was also administered a WJ III reading comprehension measure.
Effects of ReadRx on Cognitive and Reading Scores
Our analysis of this large real-world dataset revealed statistically significant changes in all reading and cognitive skills measured with medium to very large effect sizes indicating practical significance of these findings. The cognitive results are consistent with prior research on the ThinkRx cognitive training portion of this intervention.51–55 For example, in a randomized controlled trial, Carpenter et al examined the impact of 60 hours of ThinkRx cognitive training on cognitive skills for children ages 8–14 and found significant differences between treatment and controls in fluid reasoning, processing speed, working and long-term memory, visual processing, phonetic coding (sound blending), and overall IQ score with large effect sizes (d = 0.89 to 2.9).51 In a randomized controlled trial, Moore et al compared two methods of delivering the ThinkRx program to children ages 8–14 and found significant changes across all cognitive skills measured for both treatment groups with no significant differences between them except on long-term memory.54 In another study, Moore et al examined the effects of 112 hours of ThinkRx cognitive training for children and adults during the pandemic and found significant changes on attention, fluid reasoning, processing speed, working and long-term memory, visual processing, auditory processing, and overall IQ score with large effect sizes (d = 0.60 to 1.2) for both in-person and remote treatment groups.55
An interesting finding in the current study is the magnitude of age-equivalent change in reading skills. Averaging 4.1 years of growth following a 24-week intervention is unique in the field of reading remediation. Further, noting a gain of 6 years in phonological awareness after just 24 weeks (120 hours) is indeed noteworthy. Perhaps, the mechanism that drove this additional growth beyond developmental expectations (ie a year’s growth in a year’s time) is the integration of the cognitive skills training aspect of the ReadRx program. Because reading development requires the engagement of core cognitive skills including memory, processing speed, attention, reasoning, and visual processing, we hypothesize that strengthening those skills is critical to optimizing reading outcomes. We support this hypothesis with results from prior controlled studies on ReadRx.52,53 For example, in a propensity-matched controlled study, Gibson et al examined the effects of 120 hours of ReadRx combined with ThinkRx for children ages 6–18 and found statistically significant gains on tests of working memory, long-term memory, processing speed, fluid reasoning, Word Attack, and phonological awareness with medium-to-large effect sizes (R2 = 0.21 to 0.45).52 Jedlicka compared outcomes from 60 hours of ThinkRx alone and 120 hours of ReadRx integrated with ThinkRx compared to a control group and found significantly reduced difficulty ratings on academic tasks, cognitive tasks, and oppositional behaviors as reported by parents of children ages 6–18 in both treatment groups.53
We also consider the results of prior ThinkRx cognitive training studies that included measures of reading in considering this hypothesis that strengthening cognitive skills is a critical component to enhancing reading outcomes. For example, in a randomized controlled trial on ThinkRx alone, Carpenter et al demonstrated statistically significant gains in phonetic coding (sound blending) following 60 hours of LearningRx cognitive training.51 Moore et al encountered similar significant results in the second phase of that RCT studying ThinkRx.54 Jedlicka compared outcomes for ThinkRx alone and ReadRx integrated with ThinkRx and found statistically significant gains in phonetic coding (sound blending) for both ThinkRx and ReadRx® groups.53 Although other reading skills were not measured in those three studies, the impact of cognitive skills training on one reading measure along with existing research on the neuroscience of reading and the research grounded in the multiple deficit model of reading does give us a reason to dig more deeply into this hypothesis that strengthening cognitive skills along with reading skills may lead to greater reading outcomes. We also suspect that the elements of the intervention unique to the ThinkRx/ReadRx methodology also contribute to these findings. For example, the one-on-one delivery method with coaching and dynamic feedback provides all four sources of self-efficacy development identified by Bandura: modeling, mastery experiences, verbal persuasion, and management of physiological responses to stress. The literature connecting self-efficacy to learning is robust and would indeed help explain the positive results. However, the research identifying deficits in processing speed, attention, and executive function skills as contributors to reading disabilities also supports the hypothesis that strengthening those skills would provide a more solid foundation for the acquisition of stronger reading skills. Finally, the Science of Reading points to the importance of structured literacy instruction using a multi-sensory approach which are both key components of the ReadRx methodology. Combined, these factors certainly help explain the positive findings in the current study. Importantly, the current study extended the prior research on both ReadRx and ThinkRx by examining additional reading variables and parent-reported outcomes with a very large sample and documenting results that were consistent with prior research on these programs.
Predictors of Change in Reading Scores
Our analysis to examine predictors of change in reading skills following ReadRx training indicated that age, sex, ADHD, IQ score, and pretest scores on tests of individual cognitive skills did not account for much of the variance in post-intervention outcomes. Sex and age were not significant predictors of any of the reading outcome measures, indicating no difference between outcomes based on sex or age. The presence of an ADHD diagnoses at pretest was not a significant predictor of reading outcomes, indicating no differences in outcomes between children with and without ADHD. Although there were several regression models (phonological awareness, spelling, phonetic coding) that achieved significance for IQ score, less than 1% of the variance in post-test scores could be explained by either pretest IQ score. Therefore, we conclude IQ score had no practical significance in predicting outcomes on any of the variables of interest. Our findings were consistent with prior research on the influence of IQ score on reading intervention response which had also revealed minimal effect42,44,45 to no effect43 of IQ score on reading outcomes.
We also examined individual cognitive predictors of reading outcomes and found similar results. None of the individual cognitive skills were significant predictors of reading outcomes except for Word Attack skills. Pretest working memory and processing speed scores were significant predictors of post-test Word Attack scores. However, less than 1% of the variance was explained by working memory or processing speed. Given the very small effect, we conclude there was no practical significance to this finding. We did expect to see processing speed, attention, and working memory factor more significantly in our models given the deficits we see in these skills among children with reading disabilities and comorbid ADHD. What our finding does suggest, then, is that the intervention is not as sensitive to those pretest deficits in overall IQ score or individual cognitive skills as we expected, and was effective for children in the current study regardless of pretest cognitive functioning. Further, we surmise that because a key component of the intervention targets cognitive skill deficits, there was little to no predictive association between pretest cognitive functioning and post-test reading outcomes since the cognitive deficits were remediated along with the reading skills.
Parent-Reported Outcomes of ReadRx Effects
The qualitative thematic analysis of parent comments on the exit survey revealed that increased confidence and self-esteem were overwhelmingly the most reported change after children completed ReadRx. This finding, along with reported improvements in school performance and overall cognition, is consistent with our prior research on qualitative outcomes following completion of a LearningRx program.54,55,69 For example, Moore et al documented three similar themes of parent-reported outcomes including behavioral changes, academic changes, and cognitive changes following training with learning programs.55 In a study of LearningRx outcomes for children with ADHD,69 the themes of parent-reported outcomes were confidence, self-discipline and cooperative behaviors with 83% of parents of participants in the treatment group reporting changes in their child’s confidence and self-esteem. In another study, all participants who completed a LearningRx training program reported improvements in academic skills and nearly all participants reported improvements in self-esteem.54
While parent outcomes were not measured through standardized tools in the current study, the large number of records did enable us to identify robust trends in the improvements parents noted. Indeed, these trends and themes aligned strongly with our prior controlled studies on smaller samples of children. Due to the nature of the therapeutic alliance created by the one-on-one training model and targeted goal-setting engaged in by children and their trainers, the impact of the training on the themes identified by analysis of the parent reported outcomes is plausible. In addition, there is a strong motivational aspect to the trainer–child interactions and intentional conversations about how to apply new skills to other environments. The existing research that supports a relationship between reading achievement and self-esteem70,71 is certainly consistent with the improvements in self-esteem and confidence that parents reported in the current study. Further, we speculate that one-on-one delivery of ReadRx contributes greatly to these training effects of psychosocial changes, academic improvements, and everyday cognition.
Strengths, Limitations, and Future Directions
There are some strengths and limitations to the current research study that should be noted. One strength of this study is the large sample size. With data from more than 3500 children, it is easy to examine patterns that support the statistical results. Another strength is the inherent generalizability of findings from studying real-world data. The ecological validity of the results is strong and demonstrated effectiveness for this very large sample in a non-school learning center environment in which the intervention is actually being delivered day to day. That is, real-world data from clinics represent routine practices in a more realistic way than data collected from a controlled research environment. Further, the data are consistent with prior controlled studies on the ReadRx and ThinkRx programs.51–54,69
A limitation to using real-world data in research is the inability to control for confounding factors which can threaten the internal validity of the study. Randomization of participants in controlled trials accounts for these factors making it the gold-standard for intervention research. Future research on ReadRx should include randomization or propensity matching of participants in order to draw causal comparisons between ReadRx and another intervention on a greater number of reading outcomes. However, the magnitude of age-equivalent change on the reading measures mitigates the threat of time for normal development as a counterfactual in the current study. That is, we would not expect to see a 6-year gain in phonological awareness skills in 24 weeks through natural aging and in the absence of an intervention.
Finally, future research should include evaluation of reading comprehension outcomes in a larger sample. In future research, it would also be important to examine the role of socioeconomic status as a predictor of outcomes. Given that families with greater financial resources may expose their children to multiple interventions, it would be good to tease apart any potential priming effects.
Conclusion
The current study documented statistically significant changes in cognitive skills (attention, visual processing, processing speed, long-term memory, working memory, reasoning) and basic reading skills (phonological awareness, Word Attack, spelling, and phonetic coding) with robust effect sizes following completion of ReadRx for struggling readers (n = 3527). We also found significant gains in reading comprehension for a subset of the sample to which a comprehension test was administered (n = 296). Further, the current study reported three major themes of parent-reported behavioral outcomes including psychosocial changes, improved academic skills, and improved cognition. There were no differences by sex or age, and only minimal differences based on pre-intervention IQ and cognitive test scores. These results were consistent with prior research on smaller samples who completed the ReadRx intervention. The current study adds to the literature in several ways. First, given recent meta-analytical research results revealing a lack of significant improvement in foundational reading skills for the branded programs aligned with the widely used Orton–Gillingham reading approach (ie, Wilson Reading, Spalding Method, Barton Reading),28 it was important to bring awareness to the results of a large set of real-world data from a novel structured reading program. In order to positively impact the current state of poor reading proficiency for children in the United States or around the world, alternative methods like ReadRx needed to be examined and considered. The current study also fills a gap in the literature by examining a multicomponent structured reading intervention delivered through a cognitive training approach which addresses remediation of cognitive skills in addition to deficits in phonological and decoding skills. It also adds to the literature by examining characteristics of children which may impact response to a structured literacy intervention delivered through a cognitive training approach and finding that participant variables did not meaningfully influence the outcomes. This suggests that the intervention could have applicability across age groups for children with and without ADHD, for boys and girls equally, and without regard to IQ score or pre-intervention cognitive functioning.
Although future research should include a large randomized controlled trial of ReadRx in order to strengthen causal conclusions about the efficacy of the intervention, the current study offers robust real-world evidence of the impact of ReadRx on reading skills and cognition in addition to parent-reported improvements in confidence, self-esteem, school performance, and cognition for a large sample of struggling readers with and without attention problems.
Ethics Statement
The current study was reviewed for ethical compliance and approved by the Gibson Institute of Cognitive Research Institutional Review Board (IRB). Data collection procedures complied with all data protection and privacy regulations and laws. Permission to use the dataset was obtained from the dataset owner, LearningRx, for the purpose of our research. The dataset was anonymized, and no identifying information was associated with the test scores or survey results used in the study.
Disclosure
ALM and TMM are employees of LearningRx, the organization that created the intervention assessed in the current study. Neither have a financial interest in the organization, the intervention, or the research outcomes. ALM is also a volunteer board member of the 501c3 non-profit research institute founded by intervention’s creator. CL is a volunteer scientific advisory board member of the organization that created the intervention assessed in the current study and on the board of directors of the 501c3 non-profit research institute founded by intervention’s creator. CL receives zero financial compensation for those volunteer roles. JM is also a volunteer scientific advisory board member of the organization that created the intervention assessed in the current study. JM receives zero financial compensation for that volunteer role.
References
1. Irwin V, Zhang J, Wang X, et al. Report on the condition of education 2021 (NCES 2021-144). U.S. Department of Education. Washington, DC: National Center for Education Statistics; 2021. Available from https://nces.ed.gov/pubsearch/pubsinfo.asp?pubid=2021144.
2. Blau V, Reithler J, van Atteveldt N, et al. Deviant processing of letters and speech sounds as proximate cause of reading failure: a functional magnetic resonance imaging study of dyslexic children. Brain. 2010;133(3):868–879. doi:10.1093/brain/awp308
3. Castles A, Rastle K, Nation K. Ending the reading wars: reading acquisition from novice to expert. Psychol Sci Public Interest. 2018;19(1):5–51. doi:10.1177/1529100618772271
4. Snowling MJ, Hulme C, Nationa K. The Science of Reading: A Handbook.
5. Buckingham J, Wheldall R, Wheldall K. Systematic and explicit phonics instruction: a scientific, evidence-based approach to teaching the alphabetic principle. In: Cox R, Feez S, Beveridge L, editors. The Alphabetic Principle and Beyond. Primary English Teaching Association Australia; 2019:49–67.
6. The Reading League. Science of reading: defining guide; 2022. Available from: https://www.thereadingleague.org/what-is-The-science-of-reading/.
7. Gough PB, Tunmer WE. Decoding, reading, and reading disability. Remedial Special Educ. 1986;7:6–10. doi:10.1177/074193258600700104
8. Scarborough HS. Connecting early language and literacy to later reading (dis)abilities: evidence, theory, and practice. In: Neuman S, Dickinson D, editors. Handbook for Research in Early Literacy. Guilford Press; 2001:97–110.
9. Ehri LC. The science of learning to read words: a case for systematic phonics instruction. Read Res Q. 2020;55(S1):S45–S60 . doi:10.1002/rrq.334
10. Schneider WJ, McGrew KS. The Cattell-Horn-Carroll theory of cognitive abilities. In: Flanagan DP, McDonough EM, editors. Contemporary Intellectual Assessment: Theories, Tests, and Issues.
11. Fostick L, Revah H. Dyslexia as a multi-deficit disorder: working memory and auditory temporal processing. Acta Psychologica. 2018;183:19–28. doi:10.1016/j.actpsy.2017.12.010
12. Rappolt-Schlichtmann G, Boucher AR, Evans M, et al. From deficit remediation to capacity building: learning to enable rather than disable children with dyslexia. Lang Speech Hear Serv Sch. 2018;49(4):864–874. doi:10.1044/2018_LSHSS-DYSLC-18-0031
13. Gray S, Fox AB, Green S, et al. Working memory profiles of children with dyslexia, developmental language disorder, or both. J Speech Lang Hear Res. 2019;62(6):1839–1858. doi:10.1044/2019_JSLHR-L-18-0148
14. Maehler C, Joerns C, Schuchardt K. Training working memory of children with and without dyslexia. Children. 2019;6(3):47. doi:10.3390/children6030047
15. Park H, Lombardino LJ. Relationships among cognitive deficits and component skills of reading in younger and older children with developmental dyslexia. Res Dev Disabil. 2013;34(9):2946–2958. doi:10.1016/j.ridd.2013.06.002
16. Chamberlain R, Brunswick N, Siev J, McManus IC. Meta-analytic findings reveal lower means but higher variances in visuospatial ability in dyslexia. Br J Psychol. 2018;109(4):897–916. doi:10.1111/bjop.12321
17. Chong A, Normah CD, Ibrahim N, Ahmad M, Pheh KS, Razak RA. A review on phonological awareness and visual-spatial ability among children with dyslexia. Malay J Health Sci. 2018;20:145–154. doi:10.17576/JSKM-2018-20
18. Booth JN, Boyle JME, Kelly SW. The relationship between inhibition and working memory in predicting children’s reading difficulties. J Res Read. 2014;37(1):84–101. doi:10.1111/1467-9817.12011
19. Gabay Y, Karni A, Banai K. The perceptual learning of time-compressed speech: a comparison of training protocols with different levels of difficulty. PLoS One. 2017;12(5):e0176488. doi:10.1371/journal.pone.0176488
20. Stenneken P, Egetemeir J, Schulte-Korne G, Muller H, Schneider WX, Finke K. Slow perceptual processing speed at the core of developmental dyslexia: a parameter-based assessment of visual attention. Neuropsychologia. 2011;49(12):3454–3465. doi:10.1016/j.neuropsychologia.2011.08.021
21. Barnes MA, Clemens NH, Fall A-M, et al. Cognitive predictors of difficulties in math and reading in pre-kindergarten children at high risk for learning disabilities. J Educ Psychol. 2020;112(4):685–700. doi:10.1037/edu0000404
22. Morgan PL, Farkas G, Hillemeier MM, Pun WH, Maczuga S. Kindergarten children’s executive functions predict their second-grade academic achievement and behavior. Child Dev. 2019;90(5):1802–1816. doi:10.1111/cdev.13095
23. Varvara P, Varuzza C, Sorrentino A, Vicari S, Menghini D. Executive functions in developmental dyslexia. Front Hum Neurosci. 2014;8(120):1–8. doi:10.3389/fnhum.2014.00120
24. Wilson AM, Ahmed H, Mead N, et al. Neurocognitive predictors of response to intervention with GraphoGame Rime. Front Educ. 2021;6:639294. doi:10.3389/feduc.2021.639294
25. Cho E, Roberts GJ, Capin P, Roberts G, Miciak J, Vaughn S. Cognitive attributes, attention, and self-efficacy of adequate and inadequate responders in a fourth grade reading intervention. Learn Disabil Res Pract. 2015;30(4):159–170. doi:10.1111/ldrp.12088
26. Pennington BF. From single to multiple deficit models of developmental disorders. Cognition. 2006;101(2):385–413. doi:10.1016/j.cognition.2006.04.008
27. Christodoulou JA, Cyr A, Murtagh J, et al. Impact of intensive summer reading intervention for children with reading disabilities and difficulties in early elementary school. J Learn Disabil. 2017;50(2):115–127. doi:10.1177/0022219415617163
28. Stevens E, Austin C, Moore C, Scammacca N, Boucher A, Vaughn S. Current state of the evidence: examining the effects of Orton-Gillingham reading interventions for children with or at-risk for word-level reading disabilities. Except Child. 2021;87(4):397–417. doi:10.1177/0014402921993406
29. Lipowska M, Łada AB, Pawlicka P, Jurek P. The use of the Warnke Method in dyslexia therapy for children. J Appl Dev Psychol. 2019;64:1–11. doi:10.1016/j.appdev.2019.101060
30. Catts HW, Petscher Y. A cumulative risk and resilience model of dyslexia. J Learn Disabil. 2022;55(3):171–184. doi:10.1177/00222194211037062
31. Czamara D, Tiesler C, Kohlböck G, et al. Children with ADHD symptoms have a higher risk for reading, spelling and math difficulties in the GINIplus and LISAplus cohort studies. PLoS One. 2013;8(5):e63859. doi:10.1371/journal.pone.0063859
32. Peterson RL, Boada R, McGrath LM, Willcutt EG, Olson RK, Pennington BF. Cognitive prediction of reading, math, and attention: shared and unique influences. J Learn Disabil. 2017;50(4):408–421. doi:10.1177/0022219415618500
33. Willcutt EG, Betjemann RS, McGrath LM, et al. Etiology and neuropsychology of comorbidity between RD and ADHD: the case for multiple-deficit models. Cortex. 2010;46(10):1345–1361. doi:10.1016/j.cortex.2010.06.009
34. Doyle AE, Vuijk PJ, Doty ND, et al. Cross-disorder cognitive impairments in youth referred for neuropsychiatric evaluation. J Int Neuropsychol Soc. 2017;24:91–103. doi:10.1017/s1355617717000601
35. Willcutt EG, Sonuga-Barke EJS, Nigg JT, Sergeant JA. Recent developments in neuropsychological models of childhood disorders. Adv Biol Psychiatry. 2008;24:195–226.
36. Stewart AA, Austin CR. Reading interventions for children with or at risk of attention-deficit/hyperactivity disorder: a systematic review. Remedial Special Educ. 2020;41(6):352–367. doi:10.1177/0741932519849660
37. Luoni C, Balottin U, Zaccagnino M, Brembilla L, Livetti G, Termine C. Reading difficulties and attention-deficit/hyperactivity behaviours: evidence of an early association in a nonclinical sample. J Res Read. 2015;38(1):73–90. doi:10.1111/j.1467-9817.2013.01555.x
38. Pennington BF. Diagnosing Learning Disorders: A Neuropsychological Framework.
39. Church JA, Cirino PT, Miciak J, Juranek J, Vaughn S, Fletcher JM. Cognitive, intervention, and neuroimaging perspectives on executive function in children with reading disabilities. N Direct Child Adolesc Dev. 2019;165:25–54. doi:10.1002/cad.20292
40. Mayes SD, Calhoun SL, Bixler EO, Zimmerman DN. IQ and neuropsychological predictors of academic achievement. Learn Individ Differ. 2009;19(2):238–241. doi:10.1016/j.lindif.2008.09.001
41. Morris RD, Lovett MW, Wolf M, et al. Multiple-component remediation for developmental reading disabilities: IQ, socioeconomic status, and race as factors in remedial outcome. J Learn Disabil. 2012;45(2):99–127. doi:10.1177/0022219409355472
42. Stuebing KK, Barth AE, Molfese PJ, Weiss B, Fletcher JM. IQ is not strongly related to response to reading instruction: a meta-analytic interpretation. Except Child. 2009;76(1):31–51. doi:10.1177/001440290907600102
43. Shaywitz SE, Morris R, Shaywitz B. The education of dyslexic children from childhood to young adulthood. Ann Rev Psychol. 2008;59:451–475. doi:10.1146/annurev.psych.59.103006.093633
44. Stage SA, Abbott RD, Jenkins JR, Berninger VW. Predicting response to early reading intervention from verbal IQ, reading-related language abilities, attention ratings, and verbal IQ-word reading discrepancy: failure to validate discrepancy method. J Learn Disabil. 2003;36(1):24–33. doi:10.1177/00222194030360010401
45. Fuchs D, Young CL. On the irrelevance of intelligence in predicting responsiveness to reading instruction. Except Child. 2006;73(1):8–30. doi:10.1177/001440290607300101
46. Reilly D, Neumann DL, Andrews G. Gender differences in reading and writing achievement: evidence from the National Assessment of Educational Progress (NAEP). Am Psychol. 2019;74(4):445–458. doi:10.1037/amp0000356
47. Wilson AM, Lesaux NK. Persistence of phonological processing deficits in college students with dyslexia who have age-appropriate reading skills. J Learn Disabil. 2001;34(5):394–400. doi:10.1177/002221940103400501
48. Pfost M, Hattie J, Dörfler T, Artelt C. Individual differences in reading development: a review of 25 years of empirical research on Matthew effects in reading. Rev Educ Res. 2014;84(2):203–244. doi:10.3102/0034654313509492
49. Gibson K, Mitchell T, Tenpas D. ReadRx Sound-to-Code Reading and Spelling Program. Colorado Springs, CO: LearningRx; 2003.
50. Gibson K. ThinkRx: Cognitive Training Procedures Workbook. Colorado Springs, CO: LearningRx; 2003.
51. Carpenter D, Ledbetter C, Moore AL. LearningRx cognitive training effects in children ages 8–14: a randomized controlled study. Appl Cogn Psychol. 2016;30(5):815–826. doi:10.1002/acp.3257
52. Gibson K, Carpenter DM, Moore AL, Mitchell T. Training the brain to learn: beyond vision therapy. Vision Dev Rehabil. 2015;1(2):120–129.
53. Jedlicka E. LearningRx cognitive training for children and adolescents ages 5–18: effects on academic skills, behavior, and cognition. Front Educ. 2017;2(62). doi:10.3389/feduc.2017.00062
54. Moore AL, Carpenter DM, Miller TM, Ledbetter C. Comparing two methods of delivering ThinkRx cognitive training to children ages 8–14: a randomized controlled trial of equivalency. J Cognitive Enhancement. 2019;3(3):261–270. doi:10.1007/s41465-018-0094-z
55. Moore AL, Miller TM, Ledbetter C. Remote vs. in-person delivery of LearningRx one-on-one cognitive training during the COVID-19 pandemic: a non-inferiority study. Front Psychol. 2021;12:749898. doi:10.3389/fpsyg.2021.749898
56. Lam EA, McMaster KL. Predictors of responsiveness to early literacy intervention: a 10-year update. Learn Disabil Quart. 2014;37(3):134–147. doi:10.1177/0731948714529772
57. Woodcock RW, McGrew KS, Mather N. Woodcock-Johnson III Tests of Cognitive Abilities. Itasca, IL: Riverside Publishing; 2001.
58. Woodcock RW, McGrew KS, Mather N. Woodcock-Johnson III Tests of Achievement. Itasca, IL: Riverside Publishing; 2001.
59. Nouwens S, Groen MA, Verhoeven L. How working memory relates to “children’s reading comprehension: the importance of domain-specificity in storage and processing. Read Writ. 2017;30(1):105–120. doi:10.1007/s11145-016-9665-5
60. Memisevic H, Dedic A, Malec D. Differentiating between good readers and poor readers: the role of linguistic and cognitive factors. Eur J Educ Pedag. 2022;3(1):31–36. doi:10.24018/ejedu
61. Gavril L, Roșan A, Szamosközi S. The role of visual-spatial attention in reading development: a meta-analysis. Cogn Neuropsychol. 2021;38(6):387–407. doi:10.1080/02643294.2022.2043839
62. Lobier M, Dubois M, Valdois S. The role of visual processing speed in reading speed development. PLoS One. 2013;8(4):e58097. doi:10.1371/journal.pone.0058097
63. Feuerstein R. The theory of structural modifiability. In: Presseisen B, editor. Learning and Thinking Styles: Classroom Interaction. National Education Association; 1990.
64. Bandura A. Self-efficacy. In: Ramachaudran VS, editor. Encyclopedia of Human Behavior. Vol. 4. Academic Press; 1994:71–81.
65. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
66. Baumas V, Zebdi R, Julien-Sweerts S, et al. Patients and parent’s experience of multi-family therapy for anorexia nervosa: a pilot study. Front Psychol. 2021;12:584565. doi:10.3389/fpsyg.2021.584565
67. Rodríguez-Naveiras E, Cadenas M, Borges Á, Valadez D. Educational responses to students with high abilities from the parental perspective. Front Psychol. 2019;10:1187. doi:10.3389/fpsyg.2019.01187
68. Biederman J, Faraone SV, Monuteaux MC, et al. How informative are parent reports of attention-deficit/hyperactivity disorder symptoms for assessing outcome in clinical trials of long-acting treatments? A pooled analysis of parents’ and teachers’ reports. Pediatrics. 2004;113:1667–1671. doi:10.1542/peds.113.6.1667
69. Moore AL, Carpenter DM, Ledbetter C, Miller TM. Clinician-delivered cognitive training for children with attention problems: transfer effects on cognitive and behavior from the ThinkRx randomized controlled trial. Neuropsychiatr Dis Treat. 2018;14:1671–1683. doi:10.2147/NDT.S165418
70. McArthur GM, Filardi N, Francis DA, Boyes ME, Badcock NS. Self-concept in poor readers: a systematic review and meta-analysis. PeerJ. 2020;8:e8772. doi:10.7717/peerj.8772
71. Merisuo-Storm T, Soininen M. The interdependence between young children’ reading attitudes, reading skills, and self-esteem. J Educ Soc Res. 2014;4(2). doi:10.5901/jesr.2014.v4n2p122
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.