Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
A Real-World Analysis of Treatment Patterns and Clinical Characteristics Among Patients with COPD Who Initiated Multiple-Inhaler Triple Therapy in New Zealand
Authors Xu X ![]() , Milea D, Navarro Rojas AA, Braganza A, Holbrook T, Marett B, Young R, Scott RJ, Gribben B
, Milea D, Navarro Rojas AA, Braganza A, Holbrook T, Marett B, Young R, Scott RJ, Gribben B
Received 3 December 2020
Accepted for publication 4 May 2021
Published 18 June 2021 Volume 2021:16 Pages 1835—1850
DOI https://doi.org/10.2147/COPD.S295183
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Richard Russell
Xiaomeng Xu,1 Dominique Milea,1 Aldo Amador Navarro Rojas,1 Anthony Braganza,1 Tim Holbrook,2 Brett Marett,3 Robert Young,4 Raewyn J Scott,4 Barry Gribben5
1Value Evidence and Outcomes, GlaxoSmithKline plc., 139234, Singapore; 2Real World Evidence, Adelphi Real World, Bollington, Macclesfield, Cheshire, UK; 3Medical Affairs, GlaxoSmithKline NZ Limited, Auckland, 1010, New Zealand; 4Faculty of Medical and Health Sciences, University of Auckland, Auckland, New Zealand; 5CBG Health Research Limited, Faculty of Medical and Health Sciences, Auckland, New Zealand
Correspondence: Xiaomeng Xu
Value Evidence and Outcomes, GlaxoSmithKline Plc., 23 Rochester Park, 139234, Singapore
Tel +65 81616659
Email [email protected]
Purpose: Real-world data on maintenance treatment and prescription patterns provide insights into healthcare management among patients with chronic obstructive pulmonary disease (COPD), which benefits our understanding of current COPD treatment patterns in New Zealand.
Methods: We retrospectively analyzed real-world data from the HealthStat general practice database to evaluate treatment patterns among patients with COPD in New Zealand who initiated multiple-inhaler triple therapy (MITT): inhaled corticosteroid (ICS) + long-acting muscarinic antagonist + long-acting β2-agonist (LABA). Our main objective described treatment patterns (class, duration, modification, persistence, and adherence) and characteristics of patients with COPD initiating MITT between 1 May 2016 and 30 April 2017, with 12-months’ follow-up. We also assessed the number of patients receiving MITT between 2015 and 2017, among a larger patient population receiving long-acting bronchodilator and ICS-containing therapies.
Results: Of 6249 eligible patients, 421 (mean age 67.3 years; mean number exacerbations at baseline 1.8) initiated MITT: 59.1% received combination ICS/LABA therapy prior to MITT initiation, and median treatment duration prior to MITT initiation was 350 days. Overall, 33.5% of patients remained on index treatment for 12 months. Of the remaining patients who modified treatment (on average at 144.4 days), those who had a direct switch (24.9%) or retreatment (13.5%) remained on MITT, 19.7% of patients stepped down to mono/dual therapy, and 8.3% discontinued treatment. Mean (standard deviation) persistence to any MITT over 12 months was 47.3 (50.0), and 53.4% of patients were considered adherent to MITT. Total proportions of patients receiving long-acting bronchodilator therapy and MITT increased between 2015 and 2017.
Conclusion: Most patients with COPD in New Zealand who initiated MITT had characteristics appropriate for triple therapy prescription, suggesting prescription behavior among general practitioners was largely consistent with treatment guidelines. Our findings may help optimize treatment decisions, with a focus on improving long-term triple therapy persistence and adherence.
Keywords: chronic obstructive pulmonary disease, inhaled corticosteroid, long-acting β-agonist, long-acting muscarinic antagonist, New Zealand, multiple-inhaler triple therapy
Plain Language Summary
Multiple-inhaler triple therapy (MITT: inhaled corticosteroid [ICS] + long-acting muscarinic antagonist + long-acting β2-agonist [LABA]) is key in the pharmacological management of chronic obstructive pulmonary disease (COPD). However, information on triple therapy treatment patterns and the characteristics of patients initiated on such regimens in New Zealand is unavailable.
Using data from the HealthStat general practice database, we analyzed treatment patterns and characteristics of 421 patients with COPD who initiated MITT between 1 May 2016 and 30 April 2017. All patients had no history of MITT use in the 2 years prior to MITT initiation. The overall numbers of patients receiving MITT from 2015 to 2017 were also evaluated.
Most patients who initiated MITT had characteristics appropriate for triple therapy prescription: approximately 60% had a COPD exacerbation history, and the mean number of exacerbations prior to MITT initiation was 1.8. Most patients stepped up to MITT from ICS/LABA; frequent ICS/LABA use was likely a result of widespread comorbid asthma and treatment availability at the time of study. Most patients (71.9%) remained on some form of MITT regimen (including approximately one third of patients who remained on their index treatment for 12 months) and overall adherence was approximately 50%, suggesting that MITT was an appropriate treatment choice for these patients. MITT use increased from 2015 to 2017, possibly due to an easing of restrictions on drug reimbursement costs during this period.
Our findings may help inform treatment choices and aid healthcare practitioners in optimizing care for patients with COPD in New Zealand.
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of mortality and morbidity worldwide.1 Some previous studies on the prevalence and severity of COPD in New Zealand have been conducted,2–4 and in 2006 it was estimated that the respiratory disorders COPD and asthma contributed to approximately 5.3% of New Zealand’s total disease burden.5 However, up-to-date information on the current prevalence and burden of COPD in New Zealand is unavailable.
International recommendations such as the Global Initiative for Chronic Obstructive Lung Disease (GOLD) strategy,1 and local recommendations such as the COPD-X in Australia and New Zealand,6 provide COPD treatment guidance for physicians. Originally, GOLD treatment recommendations based the assessment of COPD severity on spirometric grading of airflow limitation (GOLD grade I–IV). This assessment was later refined7–9 to include symptoms and exacerbation history, while also considering spirometric grading of airflow limitation (GOLD groups A–D), which better reflected disease complexity and helped facilitate more precise treatment recommendations for patients.7,9 The GOLD strategy recommends prescription of long-acting β2-agonist (LABA) and long-acting muscarinic antagonist (LAMA) monotherapies, alone or in combination, for patients with less severe disease, with the subsequent addition of an inhaled corticosteroid (ICS) or an escalation to ICS+LAMA+LABA triple therapy for patients with a history of exacerbations who remain symptomatic despite ongoing treatment.1
As of March 2016, various maintenance therapies indicated for COPD have been subsidized in New Zealand, including three LABA inhalers and three LAMA inhalers, plus three combination LAMA/LABA inhalers and three combination ICS/LABA inhalers.10 ICS/LAMA/LABA single-inhaler triple therapy (SITT) is currently not subsidized for the treatment of COPD in New Zealand.11 Prescribing of COPD medications in New Zealand is subject to reimbursement approval and any specific Pharmaceutical Management Agency (PHARMAC) and Special Authority criteria which, along with COPD treatment guidelines, may also influence prescription choice in routine practice.
In New Zealand, COPD diagnosis and management occur mainly in the primary care setting, and it was estimated that between 95–98% of New Zealanders were registered with a general practice to receive primary care in 2020.12,13 Real-world data on patients registered with general practices in New Zealand can be found in the HealthStat general practice database.13 Many other healthcare databases exist worldwide – for example, the Clinical Practice Research Datalink14 in the United Kingdom, Hospital Episode Statistics15 and American Hospital Directory16 in the United States, and MedicineInsight17 in Australia. Although the level of information collected by healthcare databases varies greatly between countries and institutions, these data nevertheless remain important in assessing disease epidemiology and overall healthcare quality for specific diseases or within specific healthcare delivery systems, and in helping to improve critical care for patients.18 Analysis of real-world healthcare data can provide useful insights for healthcare practitioners into, for example, overall patient adherence to given treatment guidelines,19 and how prescription patterns in a given setting align with local/national treatment guidelines.20,21 Awareness of such factors could subsequently be used to advise targeted interventions and to optimize patient care in COPD; however, there is no current information from everyday clinical practice that describes treatment patterns of triple therapy in COPD, or the characteristics of patients initiated on such regimens, in New Zealand.
Our study used real-world data to provide an overview of patients with COPD in New Zealand who were receiving triple ICS+LAMA+LABA therapy (specifically multiple-inhaler triple therapy [MITT]). The main objective was to describe patients with COPD who were initiated on MITT between 1 May 2016 and 30 April 2017, and we also assessed the number of patients who were receiving MITT in the years 2015, 2016, and 2017 among a larger patient population who were receiving any long-acting bronchodilator (LABD)- or ICS-containing treatment. We investigated how the prescribing of triple therapy compared with current COPD treatment guidelines, and the subsequent implications this had for healthcare practitioners in terms of informing treatment choices and optimizing patient care in New Zealand.
Methods
Study Design
Using real-world data from the HealthStat general practice database collected between 1 January 2014 and 30 April 2018, our retrospective, descriptive analysis evaluated the treatment patterns of patients with COPD in New Zealand who initiated MITT between 1 May 2016 and 30 April 2017 (the index period). These patients had no MITT prescription for 24 months prior to MITT initiation (baseline period), and duration of previous treatment in the 12 months prior to MITT initiation was recorded. For MITT initiators, the first MITT prescription within the index period was described as the index date. Patients were required to have 24 months of baseline data prior to the index period and 12 months of follow-up data after their index date. For patients with >24 months of data prior to the index period, only data in the 24-month baseline period were analyzed. Data were collected up until 30 April 2018 to facilitate a 12-month follow-up period for patients who had an index date in April 2017 (Figure 1). Our study also included an additional analysis to evaluate temporal MITT use from 2015 to 2017 in a larger population of patients who were receiving LABD- or ICS-containing treatments.
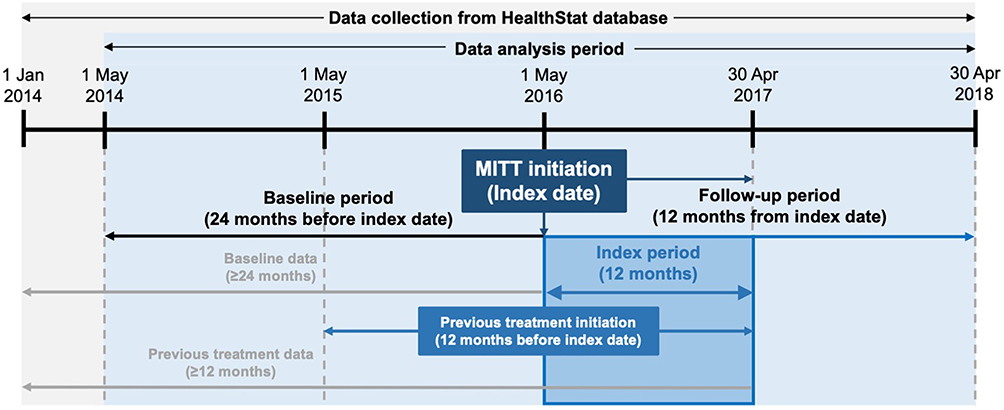 |
Figure 1 Study design. Abbreviation: MITT, multiple-inhaler triple therapy. |
MITT was defined as the concurrent prescription of ICS, LAMA, and LABA as follows: a fixed combination ICS/LABA or LAMA/LABA that overlapped by ≥1 day with a LAMA or ICS, respectively; or an open combination of three separate ICS, LAMA, and LABA inhalers, all of which overlapped with each other by ≥1 day (Table 1).
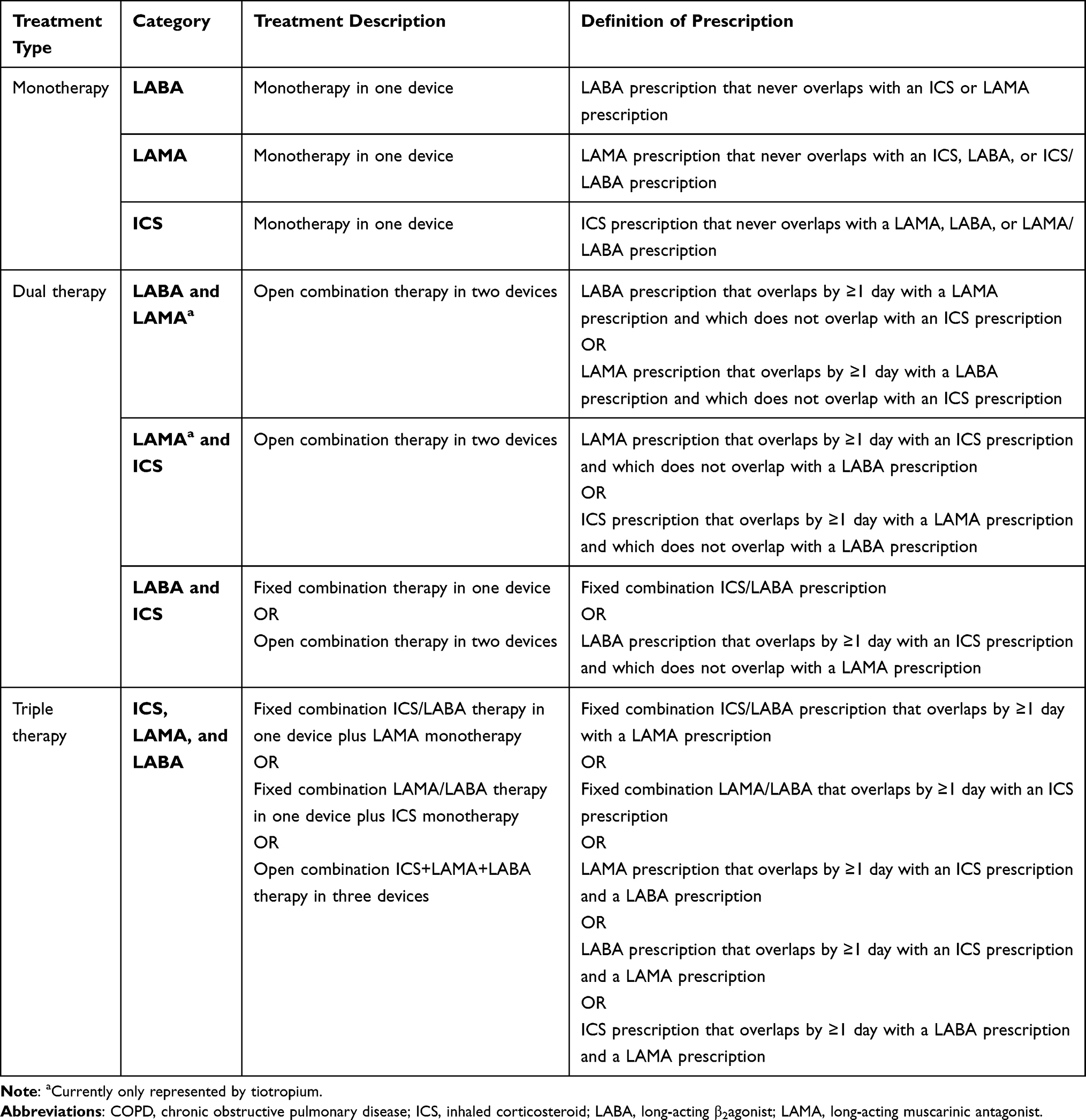 |
Table 1 Definitions of Treatments for COPD That Were Recorded Across the Study Period (1 January 2014 to 30 April 2018) |
This study was conducted in accordance with the Declaration of Helsinki, Good Clinical Practice guidelines, and ethical review requirements of participating institutions, and received formal ethical approval from the New Zealand Health and Disability Ethics Committee (ref: 13/CEN/139/AM06). No direct patient contact or primary collection of individual human patient data occurred.
Data Source
HealthStat is a general practice database in New Zealand. It is a representative sample comprising data from approximately 10% of all New Zealand general clinical practices. The database includes 15 years of data for over one million patients from 102 randomly selected general practices, each of which captures and uploads healthcare data (related to consultations, prescriptions, laboratory results, clinical measurements, and diagnostic coding for each patient) on a weekly basis. All prescriptions captured by our data analysis were limited to those issued by a general practitioner; other prescriptions issued by, for example, a specialist physician were not captured, and so the reason for prescription (for example, general practitioner or specialist physician assessment) were not known. Data from the National Minimum Dataset, including emergency department and hospital outpatient visits, and hospital admissions, may be linked to the primary care data in HealthStat using unique patient identifiers (National Health Index codes), which can thus be used to describe utilization of emergency departments, outpatient hospital visits, and inpatient hospital admissions.
Study Population
Patients with ≥1 prescription for MITT during the index period who were ≥40 years of age at their first COPD diagnosis and who had ≥1 COPD diagnostic read code at any point in their medical history were included. All diagnostic read codes for COPD are detailed in Supplementary Table 1. Patients who had a MITT prescription in the baseline period, who were <40 years of age at the index date, and those with a diagnostic code for a medical condition incompatible with COPD diagnosis at any time in their medical history were excluded. Incompatible diagnostic read codes are detailed in Supplementary Table 2.
Outcome Definitions
Baseline Demographics and Clinical Characteristics
Baseline characteristics included age at index date, sex, ethnicity, body mass index (BMI), and smoking status. Clinical characteristics of interest were number of previous exacerbations at baseline, severity of exacerbation (moderate or severe), and the presence of comorbidities ever recorded (specifically those included within the Charlson Index, and asthma). Moderate exacerbations were defined as those requiring a prescription for an oral corticosteroid and/or an antibiotic on the same date for ≥5 days, and severe exacerbations required an emergency department attendance or a hospital admission. Both moderate and severe exacerbations had a COPD exacerbation code in the diagnosis (see Supplementary Table 1). The exacerbation was counted as a new exacerbation if the code was not included within 14 days of an oral corticosteroid/antibiotic prescription, hospitalization, or emergency department visit. Comorbidities could occur at any time during the study period, and were defined by diagnosis codes for common comorbidities as listed in the Charlson Comorbidity Index.22
Treatment Prior to MITT Initiation
Non-triple therapy was identified in the 12 months preceding the index date. This included ICS, LAMA, and LABA monotherapies; plus combination ICS and LABA (together or in open combination), and LAMA+LABA (Table 1). The duration of treatment immediately preceding initiation of triple therapy was from the index date back to initiation of the first previous treatment: for patients who initiated previous treatment before the 12-month period analyzed, prior treatment duration was marked as 365 days.
Treatment Patterns, Modifications, and Duration
The supply of each component of triple therapy started on the date it was prescribed, and ended after a period comprising an assumed 90 days’ supply of medication. When assumed supplies of ICS, LAMA, and LABA all overlapped with each other by ≥1 day, this denoted MITT use. The start and end dates of overlap of individual supplies were identified as the first and last day of continuous overlap between treatment components. It was possible for patients to have multiple overlaps in treatment supply during the follow-up period. The start date of MITT was the start date of the first overlap of all three treatment components, and the end date was the theoretical end date of the last overlap.
The duration of break periods between treatment supplies, and the treatment patterns within these break periods, demonstrated whether a patient showed continuous use of their index MITT treatment, or whether they underwent a treatment modification. Patients who did not have a break of >60 days between two supplies of index treatment, from the index date until the end of the follow-up period, were considered to have exhibited continuous use. Patients who had a break between two supplies of index treatment were categorized into one of the following four index treatment modifications: (1) patients with a direct switch started a different MITT regimen after a break of <60 days between treatments; (2) patients who were retreated with MITT either restarted their index treatment or started a different MITT regimen after a break of >60 days between treatments; (3) patients who stepped down from MITT instead started a monotherapy or dual-combination therapy after a break of <60 days between treatments; and (4) patients who discontinued treatment stopped using their index treatment and were not issued with a new prescription for any treatment, after a 60-day break and until the end of the 12-month follow-up period (Supplementary Figure 1).
MITT Persistence and Adherence
Persistence with MITT (index treatment or any treatment) was defined by continuous medication use without a gap in an assumed 90-day supply for any component of triple therapy. The proportion of patients persistent to triple therapy was calculated at 3, 6, and 12 months after the index date.
Patient adherence to MITT was determined by calculating the medication possession ratio (MPR) and proportion of days covered (PDC).
MPR was calculated as the average number of days’ supply of each triple therapy component, divided by the total duration of MITT. The average days’ supply was calculated as the sum of the number of days’ supply for all prescriptions of any ICS, LAMA, or LABA during continuous use of index treatment, divided by the total number of inhalers used (two or three) (Figure 2). Patients were required to have two prescriptions for each individual component, in line with the International Society of Pharmacoeconomics and Outcomes Research criteria.23 Patients were considered adherent over the duration of triple therapy if their MPR ratio was ≥80%.
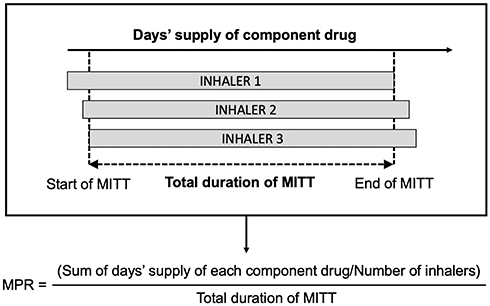 |
Figure 2 Diagram showing the calculation of MPR. Abbreviations: MITT, multiple-inhaler triple therapy; MPR, Medical Possession Ratio. |
PDC was calculated as the number of days with medication in possession during the follow-up period, divided by the total number of days in the follow-up period (3, 6, or 12 months). The number of days in possession of medication was calculated as the sum of days of supply of all prescriptions of the medication. Two measures of PDC were used in this study: PDC of triple therapy in which the number of days with medication included only the days with overlap of the three prescribed components (Figure 3A); and PDC for the individual components of the triple therapy regimen (using the average number of days covered for each inhaler of triple therapy) (Figure 3B). Patients were considered adherent if they had a PDC ≥80% for the days with overlap of all three prescribed components, or for each triple therapy component.
 |
Figure 3 PDC definition when considering overlap of all three triple therapy components (A); and when considering each triple therapy component separately (B). Abbreviations: ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; MITT, multiple-inhaler triple therapy; PDC, proportion of days covered. |
Data Analysis
All patients within the HealthStat database satisfying the eligibility criteria were included in the analyses: no sample size was specified a priori. All data were analyzed using descriptive statistics. Data on continuous variables were summarized as mean and standard deviation (SD) and/or median and interquartile range (IQR), with categorical data summarized as frequencies and percentages. Analyses were conducted by HealthStat using SAS software, Version 9.4 (SAS Institute, Cary, NC). Aggregated results were shared with the study sponsor.
Results
Baseline Demographics and Clinical Characteristics
Between 1 January 2014 and 30 April 2018, a total of 481,207 individuals were registered in the HealthStat database; 7829 (1.6%) had a recorded diagnosis of COPD, and of these individuals, 6249 (79.8%) were ≥40 years of age at the index date. Of these 6249 patients, 421 (6.7%) initiated MITT between 1 May 2016 and 30 April 2017; the remaining 5828 patients did not meet all eligibility criteria and so were excluded from further analysis (Figure 4).
 |
Figure 4 Flow chart of patient disposition. Abbreviations: COPD, chronic obstructive pulmonary disease; MITT, multiple-inhaler triple therapy. |
The 421 patients who initiated MITT had a mean (SD) age of 67.3 (11.0) years; 45.1% were male; and most fell into either the “obese” (39.2%) or “overweight” (26.6%) BMI categories. Most patients were of European (68.4%) or Māori (26.1%) ethnicity. In total, 179 (42.5%) patients also had a comorbid diagnosis of asthma; other comorbidities included mental conditions (34.4%), diabetes (20.2%), and ischemic heart disease (20%). The mean (SD) number of exacerbations at baseline was 1.8 (2.0), with 42.3% of patients having ≥2 exacerbations during the baseline period. The mean numbers of moderate and severe exacerbations per patient were 1.7 and 0.2, respectively (Table 2).
 |  | 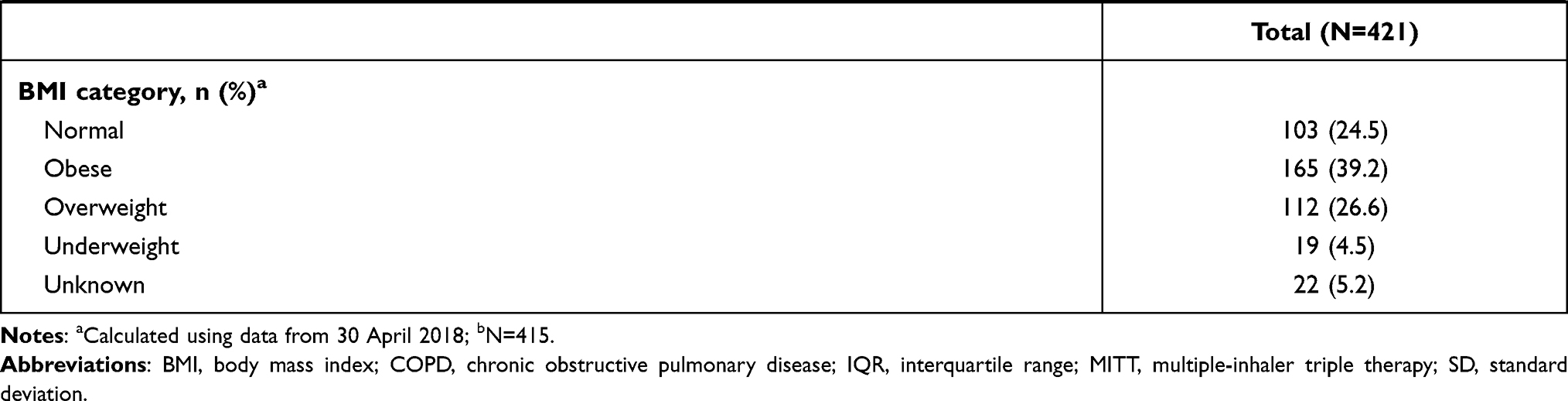 |
Table 2 Baseline Demographics and Clinical Characteristics of Patients with COPD Who Initiated MITT Between 1 May 2016 and 30 April 2017 |
Treatment Prior to MITT Initiation
In the 12 months prior to MITT initiation, most patients were receiving either ICS/LABA (59.1%) or no treatment (23.3%), and the fewest patients were receiving LABA monotherapy (0.7%). Overall, the median treatment duration prior to MITT initiation was 350 days. This was longer for patients who were receiving ICS+LAMA or no treatment (365 days), but was shorter in all other treatment groups, ranging from 92 days (LABA monotherapy and LAMA+LABA) to 323 days (ICS/LABA) (Table 3).
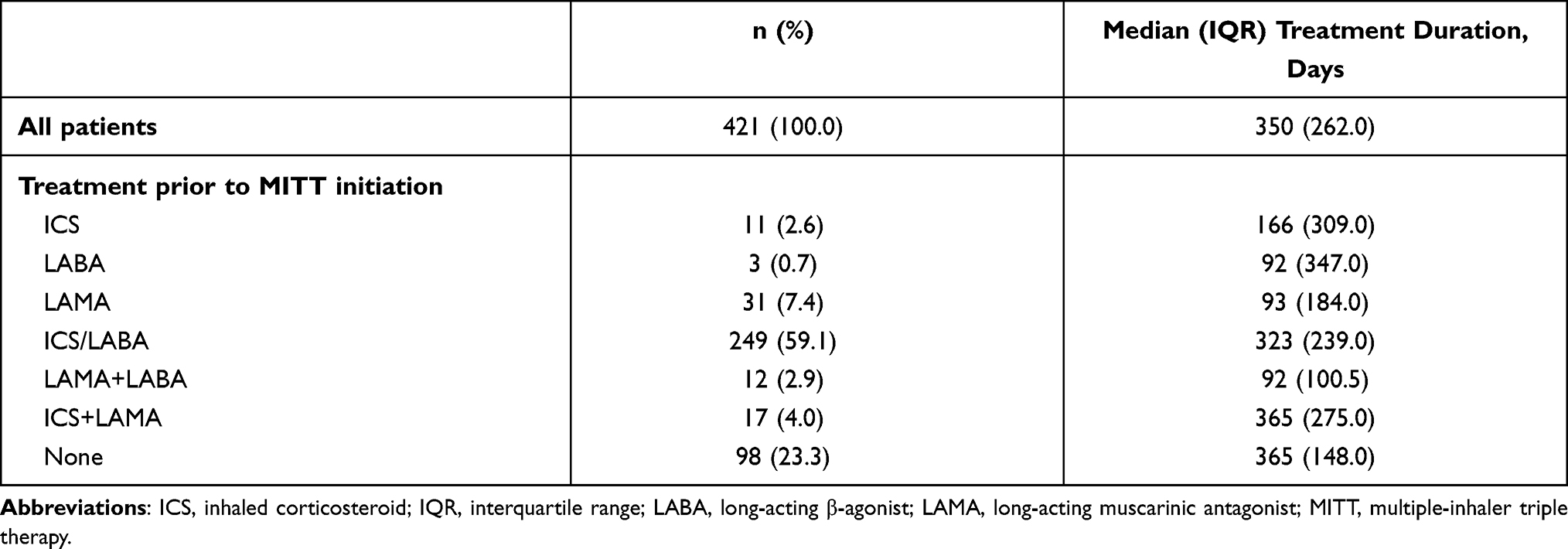 |
Table 3 Treatment Class and Median Treatment Duration in 12 Months Prior to MITT Initiation |
Treatment Patterns, Modifications, and Duration
The vast majority of patients (N=394, 93.6%) initiated MITT with ICS/LABA+LAMA, and the remaining patients (N=27, 6.4%) initiated MITT on either ICS+LAMA/LABA or ICS+LAMA+LABA. Overall, 33.5% of patients who initiated MITT showed continuous use of their index treatment during the 12-month follow-up period. The remaining 66.5% underwent a modification to their index treatment, classed as either a direct switch to another MITT (24.9%); retreatment with MITT (13.5%) after a minimum break of 60 days; step down (19.7%); or discontinuation (8.3%). Patients mostly stepped down from MITT to ICS and LABA (7.8%) or LAMA monotherapy (6.4%). On average, patients continued their index treatment for 144.4 days before undergoing a treatment modification. Median (IQR) time to first treatment modification was 150.0 (108.0) days (Table 4). Overall, 2.3% of patients had an index treatment modification within 30 days, and 12.0% of patients had an index treatment modification within 60 days.
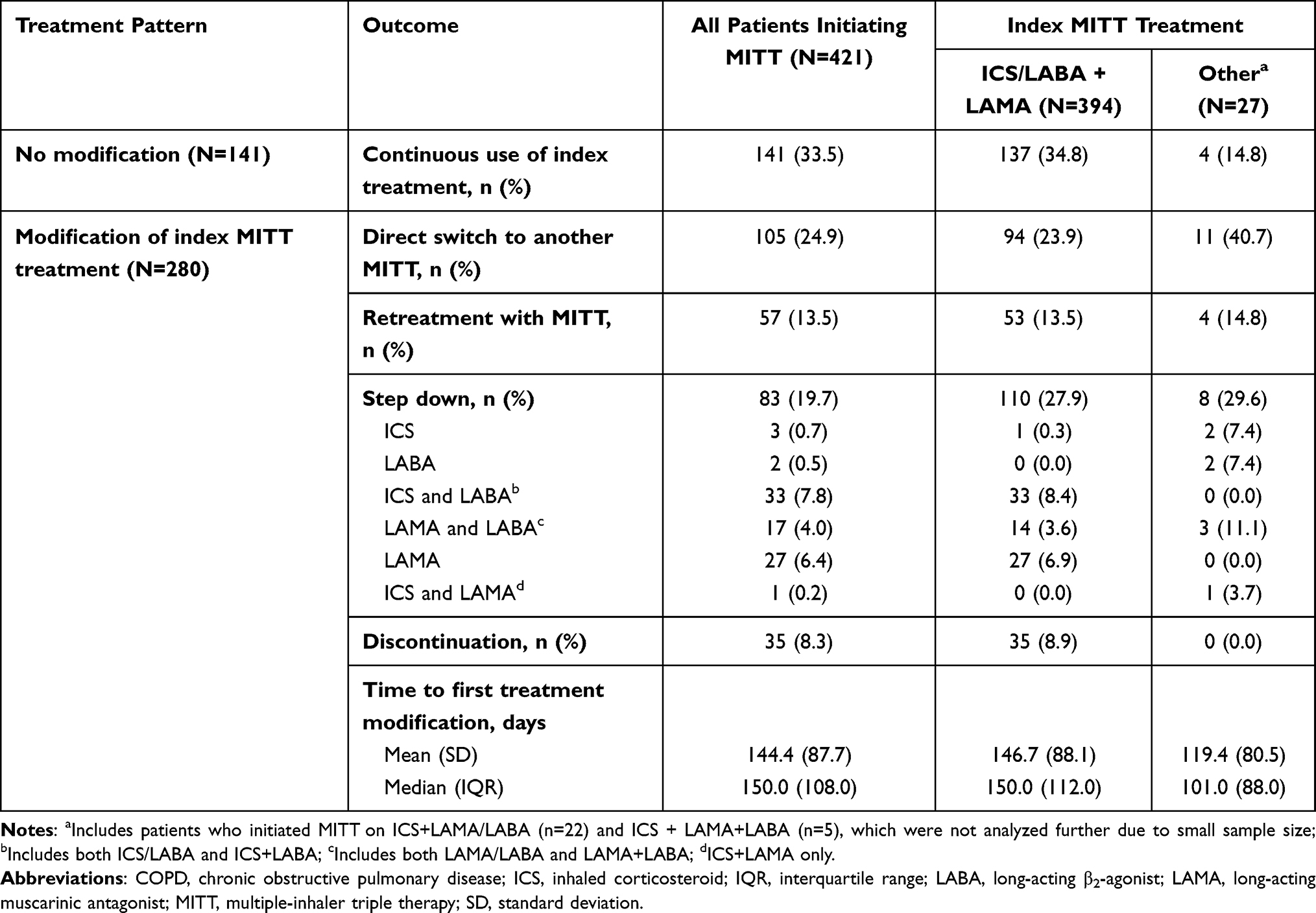 |
Table 4 Treatment Patterns Among Patients with COPD Who Initiated MITT Between 1 May 2016 and 30 April 2017 |
MITT Persistence and Adherence
Overall persistence with MITT decreased in the months following initiation. Mean (SD) persistence was 91.4 (28.0) at 3-months follow-up, 63.2 (48.3) at 6-months follow-up, and 47.3 (50.0) at 12-months follow-up.
Of patients persistent with MITT, mean (SD) MPR was 75.9 (22.7). Overall, 53.4% of patients were considered adherent using the MPR calculation (MPR ≥80%).
Mean (SD) PDC for overlap of all three triple therapy components was 97.0 (11.8), 89.6 (18.5), and 77.9 (28.3) at 3-, 6-, and 12-months follow-up, respectively. Per this PDC definition, the proportion of patients considered adherent to treatment (PDC ≥80%) decreased from 94.3% (3-months follow-up) to 86.5% (6-months follow-up) to 62.9% (12-months follow-up). All patients were considered adherent to individual components of MITT at 3-months follow-up, and this had declined to 76.2% at 12-months follow-up. Although adherence to individual components of MITT was lowest at 6-months follow-up (47.5%), this result was not unexpected due to the nature of the analysis (Table 5). PDC offered a more conservative measure of triple therapy use among sampled patients than MPR because it did not double-count the days of medication coverage, but only counted days on which all component drugs were available.
 |
Table 5 Persistence and Adherence for Patients with COPD Who Initiated MITT Between 1 May 2016 and 30 April 2017 |
Temporal LABD/ICS and MITT Use
In 2015, data from the HealthStat database identified a total of 2271 patients with COPD who were prescribed LABD- or ICS-containing treatment. This increased to 2492 patients in 2016 and again to 2582 patients in 2017. Amongst these patients, prescription of MITT also increased from 33% (n=749) in 2015, 39.5% (n=984) in 2016, and 42.8% (n=1105) in 2017.
Discussion
Our retrospective analysis of patterns of MITT use in the primary care setting in New Zealand found that, between 2015 and 2016, approximately two thirds of patients who initiated MITT were stepped up from ICS/LABA dual combination therapy. According to GOLD treatment guidelines for COPD,1 escalation to MITT from a dual therapy would be expected in a patient population who demonstrated persistent and/or severe exacerbations despite ongoing treatment with an existing LABD. These recommendations are consistent with our findings: around two fifths of patients had experienced ≥2 exacerbations, had experienced an average of 1.8 exacerbations each at baseline, and the vast majority of exacerbations were of moderate severity. Previous literature surrounding patients with COPD (for example, literature reviews by Hoogendoorn et al24 and Seemungal et al,25 and a retrospective study by Hurst et al26) have found wide variation in annual exacerbation rate, ranging from 0.5 to 3.5 per year and affected by overall COPD severity. This would perhaps suggest that the overall rate of exacerbations in our study population was fairly low, particularly when considering that around a quarter of the patients sampled were Māori. Compared to other ethnicities in New Zealand, Māori have been shown to have a greater burden of disease and higher risks of hospitalization and death from COPD.27 Nevertheless, our findings remain consistent with a patient population who were suitable candidates for MITT prescription.
Our analysis also showed that almost a quarter of patients initiated MITT with no prior treatment for COPD. This is not consistent with GOLD treatment guidelines for COPD, but similar trends have been observed in other retrospective studies of triple therapy treatment patterns in patients with COPD. For example, a similar study in various European countries and Australia by Quint et al28 found that most patients were either receiving ICS+LABA (28.3%) or no previous therapy (22.7%) prior to triple therapy initiation, and another study in the United Kingdom by Quint et al29 found that most patients were receiving either ICS+LABA (27.9%), LAMA (13.1%), or no previous therapy (12.1%) prior to triple therapy initiation. The study of patients initiating triple therapy in the United Kingdom also captured possible factors influencing pathways to triple therapy: female patients with severe COPD and comorbid asthma were more likely to have received previous therapy than no previous therapy prior to triple therapy initiation (compared with male patients and those without comorbid asthma and less severe COPD).29 Although our analysis did not capture the reasons for MITT initiation, there are several possible explanations for why so many patients initiated MITT after receiving no previous therapy. Patients may have previously been prescribed treatment for COPD but discontinued its use as a result of no perceivable therapeutic benefits, or adverse side effects.30 There may have been a poor understanding of the early signs of COPD,31 or a lack of diagnostic access,32 which could have delayed diagnosis until a late stage, and misdiagnosis may have occurred where patients with COPD presented symptoms similar to another disease such as asthma.33 Additionally, if patients were being monitored or receiving treatment outside of their general practice by, for instance, an independent respiratory specialist, this information would not be coded in the HealthStat database because, per the study methodology, all prescriptions recorded in our dataset were limited to those issued by a general practitioner. Lack of initial treatment or lack of therapeutic benefits of any treatment prior to MITT initiation could also have impacted upon the number of exacerbations seen at baseline, although the reasons for exacerbations were not specified/captured by our analysis.
Overall, most patients (71.9%) continued some form of triple therapy despite a change in components or breaks between prescriptions: approximately one third of patients (33.5%) continued their index treatment until the end of the 12-month follow-up period, and the remainder of patients underwent a treatment modification after an average of 144.4 days on index treatment; treatment modifications to triple therapy included a direct switch to another MITT regimen (24.9%) or retreatment with index/another MITT regimen (13.5%). Fewer patients overall (19.7%) stepped down to either a monotherapy or a dual therapy when they modified their treatment, and the fewest patients (8.3%) discontinued treatment altogether. Given that this study is unique among studies of COPD in New Zealand, and that there is variation between similar studies of triple therapy treatment patterns in other countries, it cannot be said whether our findings reflect expected treatment patterns of patients initiating MITT. For example, the study in Europe and Australia by Quint et al28 found that, overall, patients had longer median times to treatment modification than in our study (ranging from 2.7–18.2 months), but that the proportions of patients stepping down from or discontinuing MITT were much higher (ranging from 59.1%–84.9%). Another study in the United States by Bogart et al34 found that, when allowing for 30 days after the last day of treatment, patients had a median time to treatment discontinuation of 1.8 months and 86% of MITT users discontinued their treatment in 12 months’ follow-up. Although not directly comparable to these studies, the low step-down and discontinuation rates in our study nevertheless suggest that triple therapy was an appropriate treatment choice for the majority of patients who initiated MITT after previously being naïve to triple therapy. This has subsequent implications for healthcare practitioners in New Zealand in terms of optimizing treatment choices and care among patients with COPD. The high proportion of patients remaining on MITT at 12 months may have partly been due to improvements in clinical outcomes, but this was not evaluated in our study. Although the reasons for treatment modification or discontinuation were not captured in this study, future studies of MITT use that consider such factors over a longer follow-up period would be valuable for understanding why currently available triple therapies may not be optimal for all patients.
Most patients (93.6%) from our dataset were prescribed triple therapy in two inhalers, but a small proportion (6.4%) were receiving triple therapy via three inhalers. This is potentially explained by the increased risk of handling errors and suboptimal drug delivery to the lungs with the use of multiple inhalers, and so use of as few inhalers as possible may allow for a simplified medication regimen that ultimately helps improve patient adherence.34,35 Around half (53.4%) of patients were considered adherent to MITT at 12 months. A systematic literature review conducted by Usmani et al36 found that increasing age, education status, previous inhaler instruction, comorbidities, and socioeconomic status were associated with a greater frequency of handling errors among patients with COPD. Our population had a mean age of 67.3 years and around 13% of patients were ≥80 years of age; this could have led to issues with adherence and persistence that would have been less frequent in, for instance, a younger population, particularly those with fewer comorbid conditions, although as we did not stratify our dataset by age this cannot be confirmed. Adherence may also be influenced by patient perceptions of the effectiveness of a given treatment;37 lack of adherence to treatment prior to MITT initiation may also have impacted upon the number of exacerbations seen at baseline, but this was not evaluated in our study. Additionally, inhaler type was not specified in our analysis, but this too has potential implications for adherence among patients if one inhaler type was considered easier to use than the other.38 The LAMA and LABA treatments subsidized without Special Authority/PHARMAC restrictions in New Zealand include dry-powder inhalers and metered-dose inhalers,10 so it is likely that both dry-powder inhalers and metered-dose inhalers were prescribed. Comorbidities may affect patient response to/suitability for receipt of a particular drug,39 and could subsequently affect ICS, LABA, and/or LAMA prescription patterns. Indeed, our study population contained over 40% of patients with a diagnosis of asthma, the recommended treatment for which is an ICS-containing regimen,40 which could have explained why the majority of patients in our study population were receiving ICS/LABA treatment prior to MITT initiation. Further analysis of prescription patterns in patients with COPD, asthma, and comorbid COPD/asthma would be of interest in exploring this trend further. Additionally, in our study population, around two fifths of patients experienced ≥2 COPD exacerbations in the year prior to MITT initiation. Patients with COPD who experience persistent exacerbations may have elevated blood eosinophil levels compared to those who have fewer exacerbations, and ICS-containing regimens (including triple therapy) have demonstrably improved lung function in such patients.35,41 Although biomarkers were not analyzed, and their influence on prescription patterns was not evaluated in our study, this could nevertheless be an area of interest in future real-world data analyses for informing optimal patient treatment and management.
There has been a limited number of prescription pattern analyses among patients in New Zealand with respiratory disorders. Dummer et al42 conducted a retrospective case note review of healthcare utilization in 2015. Data were obtained from 340 patients with severe COPD from the Southern Region of New Zealand. The authors reported that triple therapy was the most common regimen at hospital admission, and they also reported deficits in care provision among patients studied. This study restricted its focus to a small number of patients with severe COPD in the Southern region of New Zealand, and so the results are not directly comparable to our findings; nevertheless, it perhaps indicates that prescription restrictions could affect treatment patterns in different regions, which may be of interest in future real-world studies in New Zealand. A retrospective, New Zealand-wide study of LABD use among 83,435 patients with asthma by Parkin et al,43 conducted between February 2006 and December 2013, showed complex patterns of ICS, LAMA, and LABA use and a progressive increase in ICS use over the study period, and indicated that ICS use was inconsistent with treatment guidelines. In this case, the use of ICS may have been influenced by patients with asthma and COPD overlap, which would differ from treatment guidelines for asthma or COPD when considered as individual conditions and subsequently highlights the potential need for an updated study of prescription patterns in patients with asthma and/or COPD. Although our study did include patients with comorbid asthma and COPD, we did not stratify our results by disease diagnosis and this could be of interest in future studies.
In our study, most patients were of European ethnicity and approximately a quarter were Māori, which may have been a result of practice location (ie, Māori are historically more prevalent in northern New Zealand than in southern regions44). Compared to other ethnic groups in New Zealand, a greater burden of disease is apparent among patients with COPD of Māori ethnicity;4,27,45–47 although our study did not stratify triple therapy data by ethnicity, this too could be a point of interest for future studies.
Drug availability in New Zealand is determined by national policy settings and, generally, there is very good access to primary care throughout the country. Some regional guidelines and restrictions may affect prescription options for patients with COPD or other respiratory conditions; for instance, sparsely populated areas may have reduced general practitioner coverage and more barriers to accessible treatment compared to more densely populated areas.48 The greater proportions of patients being prescribed MITT from 2015 to 2017 may have been influenced by changes to subsidies for treatments indicated in COPD. For example, in 2016, one combination ICS/LABA treatment (fluticasone furoate/vilanterol) became available without restriction through PHARMAC/Special Authority; additionally, three combination LAMA/LABA treatments (tiotropium/olodaterol, umeclidinium/vilanterol, and glycopyrronium/indacaterol) were fully subsidized on the condition that a patient remained fully adherent to their therapy and received greater therapeutic benefits than with LAMA monotherapy.10 We have acknowledged that the prevalence of comorbid asthma in our study population could have accounted for widespread ICS/LABA prescription, but it is also possible that this was influenced by the lack of PHARMAC/Special Authority reimbursement restriction on the prescription of ICS/LABA compared to LAMA/LABA. While PHARMAC/Special Authority criteria apply specifically to New Zealand, a similar study of prescription patterns in Australia following 2018 changes in national reimbursement criteria found that more new users of SITT had previously been prescribed MITT (42%) rather than ICS/LABA (17%), LAMA/LABA (16%), or LAMA monotherapy (9%), despite widespread comorbid asthma in 46% of patients.49 This is consistent with drug availability influencing prescription patterns rather than comorbidities.
Our study used a comprehensive real-world data set representative of general practices in New Zealand, which had both potential strengths and limitations. Although our dataset was slightly outdated (2015–2017), we did include a time period that captured changes to PHARMAC/Special Authority reimbursement restrictions, and given that our results indicated an increased prescription of triple therapy during this time, this does have important implications for present day treatment and management of COPD. General practices routinely monitor patients and all HealthStat data is linked to hospital data, which reliably indicates whether or not a patient has visited a hospital; however, some of the codes used may not be reliable for the diagnosis. It is possible that some prescriptions may be missed if a patient is hospitalized or referred to a specialist for further treatment, and this could also account for the gaps between prescriptions that were observed when assessing treatment patterns. Additionally, it is worth noting that although the date of a prescription being issued is recorded, there is no guarantee that a patient then took this prescription to a pharmacist and proceeded to take all doses of medication as prescribed. Thus, the exposure of a patient to a particular medication may have been under- or over-estimated depending on individual circumstances. Patients who were symptomatic for COPD but who had not yet received a formal diagnosis could potentially have been excluded from the analysis if an incorrect diagnosis code was used. Spirometry data was not captured due to a lack of consistency in recording methods across general practices, which subsequently presented challenges with standardizing and analyzing available data. At the time of the study, only 10% of practices captured in our analysis had recorded spirometry data in a structured manner, while other practices had recorded this in a “free notes” section of the database (if applicable). Although additional fields for recording spirometry data are now available within the HealthStat database, these data cannot be included for historical records such as those presented in our manuscript. Additionally, no data on COPD severity or smoking pack years was recorded, which could have impacted upon a COPD diagnosis being correctly recorded and upon optimal treatment decisions being made. The HealthStat database represents patients of different ages, genders, and ethnicities, but there may be some misrepresentation between regions if areas containing particularly high or low concentrations of different ethnic groups, such as people of Māori ethnicity, are over- or under-sampled.
Conclusion
In this retrospective, descriptive analysis of triple therapy for COPD in New Zealand, most patients who initiated MITT had characteristics appropriate for triple therapy prescription. This suggests that prescription behavior among New Zealand general practitioners is mostly consistent with treatment guidelines. Overall persistence and adherence after MITT initiation were high. Although almost 72% of patients overall remained on MITT at 12 months, around half of these patients modified their index treatment within one year and approximately 28% of patients overall stepped-down from or discontinued MITT. This could be due to the baseline disease status of the patients included. Our findings may serve as a starting point to aid healthcare practitioners in developing strategies to optimize treatment decisions and patient care for patients with COPD in New Zealand, with a focus on strategies to improve adherence and long-term persistence to triple therapy.
Data Sharing Statement
Anonymized individual participant data and study documents can be requested for further research from www.clinicalstudydatarequest.com.
Acknowledgments
The authors would like to thank Janine Beale (affiliated with GlaxoSmithKline plc., New Zealand at the time of the study) for her contributions to study setup until December 2019. Medical writing support for the development of this manuscript, under the direction of the authors, was provided by Joanna Wilson, PhD, of Ashfield MedComms (Glasgow, UK), an Ashfield Health company, and was funded by GlaxoSmithKline plc.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was funded by GlaxoSmithKline plc. (study 209016).
Disclosure
XX received funding from GlaxoSmithKline plc. (through GMP Technologies PTE Ltd.) to conduct this study. DM, AANR, AB, and BM are employees of, and shareholders in, GlaxoSmithKline plc. TH is an employee of Adelphi Real World, who received funding from GlaxoSmithKline plc. to conduct this study. RY and RJS have received honorarium from GlaxoSmithKline plc. for educational talks and participation in advisory groups. BG is an employee of, shareholder in, and receives funding for project management and analysis from CBG Health Research Ltd, and is also a shareholder in HealthStat who received funding for data collection from GlaxoSmithKline plc. to conduct this study. Trademarks are owned by or licensed to their respective owners. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2021 report). 2021 Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
2. Shirtcliffe P, Weatherall M, Marsh S, et al. COPD prevalence in a random population survey: a matter of definition. Eur Respir J. 2007;30(2):232–239.
3. Telfar Barnard L, Zhang J. The impact of respiratory disease in New Zealand: 2018 update. Asthma and Respiratory Foundation New Zealand. 2018. Available from: https://s3-ap-southeast-2.amazonaws.com/assets.asthmafoundation.org.nz/images/NZ-Impact-Report-2018_FINAL.pdf.
4. Milne RJ, Beasley R. Hospital admissions for chronic obstructive pulmonary disease in New Zealand. N Z Med J. 2015;128(1408):23–35.
5. Ministry of Health. Health loss in New Zealand: a report from the New Zealand burden of diseases, injuries and risk factors study, 2006–2016. 2013. Available from: https://www.moh.govt.nz/notebook/nbbooks.nsf/0/F85C39E4495B9684CC257BD3006F6299/$file/health-loss-in-new-zealand-final.pdf.
6. Yang IA, Brown JL, George J, et al. The COPD-X Plan: Australian and New Zealand guidelines for the management of chronic obstructive pulmonary disease. 2020. Available from: https://copdx.org.au/copd-x-plan/.
7. Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365.
8. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2017 report). 2017. Available from: https://goldcopd.org/wp-content/uploads/2017/02/wms-GOLD-2017-FINAL.pdf.
9. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582.
10. Booker C, Harris H, Leitch S, et al. Best practice: newly subsidised medicines for COPD. Best Pract J. 2016;(74):7–13.
11. PHARMAC. Online pharmaceutical schedule - April 2021: community schedule, respiratory system and allergies. 2021. Available from: https://schedule.pharmac.govt.nz/ScheduleOnline.php?code=A28&edition=2021-04.
12. Tikkanen R, Osborn R, Mossialos E, et al. International health care system profile. New Zealand. 2020. Available from: https://www.commonwealthfund.org/international-health-policy-center/countries/new-zealand.
13. HealthStat Primary Health Care Intelligence. HealthStat general practice database. Available from: http://www.healthstat.co.nz/Login.aspx?ReturnUrl=%2fdefault.aspx.
14. Clinical Practice Research Datalink. 2021. Available from: https://www.cprd.com/.
15. NHS Digital. Hospital Episode Statistics (HES). 2020. Available from: https://digital.nhs.uk/data-and-information/data-tools-and-services/data-services/hospital-episode-statistics.
16. American Hospital Directory. 2021. Available from: https://www.ahd.com/.
17. MedicineInsight. 2021. Available from: https://www.nps.org.au/medicine-insight.
18. Martin GS. The essential nature of healthcare databases in critical care medicine. Crit Care. 2008;12(5):176.
19. Asche CV, Leader L, Plauschinat P, et al. Adherence to current guidelines for chronic obstructive pulmonary disease (COPD) among patients treated with combination of long-acting bronchodilators or inhaled corticosteroids. Int J Chron Obstruct Pulmon Dis. 2012;7:201–209.
20. Make B, Dutro MP, Paulose-Ram R, et al. Undertreatment of COPD: a retrospective analysis of US managed care and Medicare patients. Int J Chron Obstruct Pulmon Dis. 2012;7:1–9.
21. Diette GB, Orr P, McCormack MC, et al. Is pharmacologic care of chronic obstructive pulmonary disease consistent with the guidelines? Popul Health Manag. 2010;13(1):21–26.
22. Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383.
23. Cramer JA, Roy A, Burrell A, et al. Medication compliance and persistence: terminology and definitions. Value Health. 2008;11(1):44–47.
24. Hoogendoorn M, Feenstra TL, Hoogenveen RT, et al. Association between lung function and exacerbation frequency in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2010;5:435–444.
25. Seemungal TA, Hurst JR, Wedzicha JA. Exacerbation rate, health status and mortality in COPD – a review of potential interventions. Int J Chron Obstruct Pulmon Dis. 2009;4:203–223.
26. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138.
27. Best Practice Advocacy Centre New Zealand (BPACnz). Diagnosis and management of COPD in Māori and Pacific peoples. Best Pract J. 2012;43:14–25.
28. Quint JK, O’Leary C, Venerus A, et al. Prescribing pathways to triple therapy: a multi-country, retrospective observational study of adult patients with chronic obstructive pulmonary disease. Pulm Ther. 2020;6(2):333–350.
29. Quint JK, Venerus A, O’Leary C, et al. Prescribing pathways to triple therapy: a retrospective observational study of adults with chronic obstructive pulmonary disease in the UK. Int J Chron Obstruct Pulmon Dis. 2020;15:3261–3271.
30. Bourbeau J, Bartlett SJ. Patient adherence in COPD. Thorax. 2008;63(9):831–838.
31. Street RL
32. Jones RC, Price D, Ryan D, et al. Opportunities to diagnose chronic obstructive pulmonary disease in routine care in the UK: a retrospective study of a clinical cohort. Lancet Respir Med. 2014;2(4):267–276.
33. Tinkelman DG, Price DB, Nordyke RJ, et al. Misdiagnosis of COPD and asthma in primary care patients 40 years of age and over. J Asthma. 2006;43(1):75–80.
34. Bogart M, Stanford RH, Laliberte F, et al. Medication adherence and persistence in chronic obstructive pulmonary disease patients receiving triple therapy in a USA commercially insured population. Int J Chron Obstruct Pulmon Dis. 2019;14:343–352.
35. Ferguson GT, Brown N, Compton C, et al. Once-daily single-inhaler versus twice-daily multiple-inhaler triple therapy in patients with COPD: lung function and health status results from two replicate randomized controlled trials. Respir Res. 2020;21(1):131.
36. Usmani OS, Lavorini F, Marshall J, et al. Critical inhaler errors in asthma and COPD: a systematic review of impact on health outcomes. Respir Res. 2018;19(1):10.
37. Khdour MR, Hawwa AF, Kidney JC, et al. Potential risk factors for medication non-adherence in patients with chronic obstructive pulmonary disease (COPD). Eur J Clin Pharmacol. 2012;68(10):1365–1373.
38. Kerwin EM, Spangenthal S, Zvarich M, et al. ELLIPTA versus DISKUS plus HandiHaler in COPD: a randomized, open-label, crossover study in a clinical trial setting. Chronic Obstr Pulm Dis. 2020;7(2):118–129.
39. Negewo NA, Gibson PG, Wark PA, et al. Treatment burden, clinical outcomes, and comorbidities in COPD: an examination of the utility of medication regimen complexity index in COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:2929–2942.
40. Global Initiative for Asthma. Global strategy for asthma management and prevention. 2020. Available from: https://ginasthma.org/wp-content/uploads/2020/06/GINA-2020-report_20_06_04-1-wms.pdf.
41. Hanania NA, Papi A, Anzueto A, et al. Efficacy and safety of two doses of budesonide/formoterol fumarate metered dose inhaler in COPD. ERJ Open Res. 2020;6:2.
42. Dummer J, Tumilty E, Hannah D, et al. Health care utilisation and health needs of people with severe COPD in the southern region of New Zealand: a retrospective case note review. COPD. 2020;17(2):136–142.
43. Parkin L, Barson D, Zeng J, et al. Patterns of use of long-acting bronchodilators in patients with COPD: a nationwide follow-up study of new users in New Zealand. Respirology. 2017;23:583–592.
44. Nolan F. Census snapshot: Māori (key statistics - article, April 2002, p9). 2002. Available from: http://infoshare.stats.govt.nz/browse_for_stats/people_and_communities/maori/census-snapshot-maori.aspx#gsc.tab=0.
45. Telfar Barnard L, Zhang J. The impact of respiratory disease in New Zealand: 2018 update. Asthma Respir Foundation NZ. 2019. Available from: https://www.asthmafoundation.org.nz/assets/images/NZ-Impact-Report-2018_FINAL.pdf. Accessed April 20, 2021.
46. Shirtcliffe P, Weatherall M, Marsh S, et al. COPD prevalence in a random population survey: a matter of definition. Eur Respir J. 2007;30(2):232–239.
47. Hopkins RJ, Kendall C, Gamble GD, et al. Are New Zealand Māori more susceptible to smoking related lung cancer? A comparative case-case study. EC Pulmonol Respir Med. 2019;8.1:72–91.
48. Stokes T, Tumilty E, Latu ATF, et al. Improving access to health care for people with severe chronic obstructive pulmonary disease (COPD) in Southern New Zealand: qualitative study of the views of health professional stakeholders and patients. BMJ Open. 2019;9(11):e033524.
49. NPS Medicinewise. Characterization of patients with chronic obstructive pulmonary disease (COPD) treated with single-inhaler triple therapy (SITT) or multiple-inhaler triple therapy (MITT) in Australia, using MedicineInsight and Pharmaceutical Benefits Scheme (PBS) data. 2021. Available from: https://www.nps.org.au/assets/NPS/pdf/Summary-of-GSK-COPD-project.pdf.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.