Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
A Rare Case on Capecitabine Induced Acquired Palmoplantar Keratoderma
Authors Tsaqilah L ![]() , Mudia KAM, Usman HA
, Mudia KAM, Usman HA ![]() , Dharmadji HP, Hidayah RMN
, Dharmadji HP, Hidayah RMN ![]() , Avriyanti E
, Avriyanti E ![]()
Received 27 September 2023
Accepted for publication 17 December 2023
Published 23 December 2023 Volume 2023:16 Pages 3713—3718
DOI https://doi.org/10.2147/CCID.S442194
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Laila Tsaqilah,1 Keshia Amalia Mivina Mudia,1 Hermin Aminah Usman,2 Hartati Purbo Dharmadji,1 Risa Miliawati Nurul Hidayah,1 Erda Avriyanti1
1Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran–Dr. Hasan Sadikin General Hospital, Bandung, West Java, Indonesia; 2Department of Anatomical Pathology, Faculty of Medicine, Universitas Padjadjaran–Dr. Hasan Sadikin General Hospital, Bandung, West Java, Indonesia
Correspondence: Laila Tsaqilah, Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran–Dr. Hasan Sadikin General Hospital, Jl. Pasteur 38, Bandung, West Java, 40161, Indonesia, Tel +6282284474849, Email [email protected]
Abstract: Acquired palmoplantar keratoderma (PPK) is a non-hereditary hyperkeratosis of the palms and soles that is caused by various factors, including chemotherapeutic agents. The purpose of this case report is to present a rare case of acquired PPK caused by the chemotherapeutic agent capecitabine. A 54-year-old female complained of painful erythematous plaques on her palms and soles with history of consuming capecitabine. Physical examination revealed scaly erythematous plaques on the palmoplantar surface and knuckle pads on both hands. Histopathological features showed hyperkeratosis, acanthosis, vasodilatation, and perivascular lymphocytic infiltration. Therefore, the patient was diagnosed with acquired PPK due to capecitabine. The dose of capecitabine was reduced and the patient was administered topical corticosteroid and emollient. Improvement of skin lesions was strongly observed after discontinuation of capecitabine. The underlying cause of PPK should be identified to determine the appropriate treatment. Dose reduction or drug discontinuation is the mainstay therapy for patients with acquired PPK caused by chemotherapeutic agents.
Keywords: capecitabine, chemotherapy, palmoplantar keratoderma
Introduction
Acquired palmoplantar keratoderma (PPK) is a non-hereditary hyperkeratosis of the palms and soles covering ≥50% of the skin surface of involved acral area that can be caused by inflammatory disease, metabolic disease, or exposure to drugs,1,2 such as chemotherapeutic agents, including capecitabine, doxorubicin, hydroxyurea, and tegafur.2,3 The mechanism by which capecitabine causes PPK is still not clear.3 Clinical manifestations of PPK can affect the patient’s quality of life, therefore the underlying causes of PPK must be identified immediately to determine the appropriate management.4 This case report aim to report a rare case of acquired PPK caused by chemotherapeutic agent capecitabine.
Case
A 54 years old woman with erythematous skin and hyperkeratotic scales on her palms and soles was referred to our dermatology clinic. Four and a half months before consultation, she felt discomfort and slight pain in both palms and soles. Two weeks later, erythematous macules appeared with scales. Sometimes, vesicles appear, which then break into erosion that felt pain. After a couple of months, the skin had thickened into erythematous plaques with thickening scales. The patient was diagnosed with breast cancer six years prior, and a unilateral mastectomy had already been carried out. The patient had history of taking 500 mg capecitabine for five months, which was administered orally as four tablets in the morning and three tablets in the evening. No other medication was consumed by the patient other than capecitabine. No similar complaints were found in the families of the patients. A history of contact with or application of any topical agent before the lesions appeared was ruled out. Upon physical examination, knuckle pads were found in both hands. Dermatological examination revealed erythematous plaques and scales on both palms and soles (Figure 1). Microscopic examination of skin scrapings with 10% potassium hydroxide did not reveal any fungal elements. Thyroid-stimulating hormone examination results were within normal limits, and the antinuclear antibody was nonreactive. Histopathological examination revealed that the epidermis was covered with stratified squamous epithelium, with hyperkeratosis, orthokeratosis, and acanthosis. The dermis consists of stromal connective tissue covered with perivascular lymphocytic inflammatory cells, which corresponds to palmoplantar keratoderma (Figure 2). Based on the history, physical examination, and histopathological features, the patient was diagnosed with acquired PPK due to capecitabine. The patient was treated with vaseline album and 0.05% clobetasol propionate cream twice a day, also the dose of capecitabine was reduced to two tablets in the morning and one tablet in the evening. After the second month of observation, a clinical improvement was observed. The improvement in the skin lesions was more pronounced after capecitabine was discontinued by the hematology and oncology clinic (Figure 3).
 |
Figure 1 Clinical image of erythematous plaques with scales on the palms and soles accompanied with knuckle pads on the back of the hands before treatment. |
 |
Figure 2 Histopathological feature revealed (A) hyperkeratosis and acanthosis; (B) vasodilatation and perivascular lymphocytic infiltrates (red arrows). |
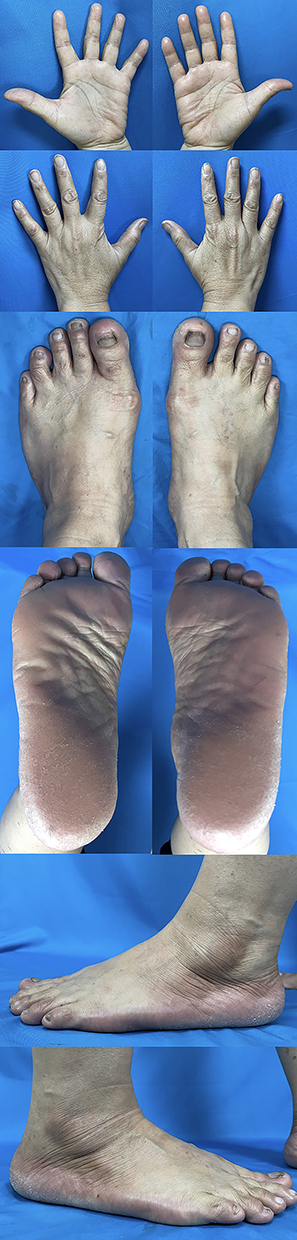 |
Figure 3 Improvement of skin lesions after capecitabine was discontinued. |
Discussion
Palmoplantar keratoderma has recently been observed as an uncommon cutaneous complication of some medications.3 Studies reporting acquired PPK are still very limited. PPK lesions can be classified based on their pattern of skin involvement into three categories: diffuse, focal, and punctate. Diffuse PPK involves the entire surface of palms and soles. Punctate PPK presents as multiple discrete keratotic papules on the palms and soles. PPK lesions can also accompanied by thickening of the skin on the back of the hands and feet, such as on the knuckles, called knuckle pads.2 This patient showed a diffuse pattern with knuckle pads on both hands.
Based on etiology, acquired PPK can be divided into (1) keratoderma climactericum; (2) drug related PPK; (3) malnutrition associated PPK; (4) chemically induced PPK; (5) PPK related to systemic disease; (6) PPK related to malignancy; (7) PPK due to other dermatoses; (8) PPK due to infection; and (9) idiopathic PPK.2 PPK has been identified as a rare adverse event for numerous medications, including glucan, lithium, venlafaxine, verapamil, antimalarial, and chemotherapeutic agents.2,3 One of study reported that the most often drugs related to PPK were B-Raf proto-oncogene (BRAF) inhibitors (73.7%), combination of BRAF inhibitors and mitogen-activated protein kinase (15.4%), tyrosine kinase inhibitors (3.2%), as well as chemotherapeutic agents (2.4%).3 Six chemotherapeutic agents reported in that study were capecitabine in two patients, doxorubicin in two patients, hydroxyurea in one patient, and tegafur in one patient. The patient in this case report had been taking capecitabine for five months before being consulted and started experiencing symptoms one month after taking capecitabine.
Kundel et al5 reported that the most common side effect of capecitabine was nausea (38%), followed by weakness (24%), diarrhea (24%), mucositis (10%), and hand-foot syndrome (HFS) (7%). HFS is the most common cutaneous side effect of capecitabine, with characteristic symptoms preceded by dysesthesia or discomfort, followed by symmetrical erythema and edema on the palms and soles. Skin manifestations can also be accompanied by blisters and erosions. The pathogenesis of HFS remains unknown; however, it is thought to be related to the dose and duration of chemotherapy. Several theories have been proposed for the pathogenesis of HFS. First, high levels of thymidine phosphorylase in keratinocytes, especially on the palms and soles, result in increased accumulation of capecitabine metabolites. Second, capecitabine can be eliminated via the eccrine glands, which are abundant in palms and soles, resulting in the accumulation of capecitabine metabolites that affect acrosyringium differentiation and hyperkeratosis. Another supporting theory is that microtrauma to the capillaries due to mechanical stress can cause chemotherapy agents to escape from the blood vessels and cause cytotoxic effects on the surrounding tissues.6 Capecitabine has also been reported to cause a variety of dermatologic reaction, such as lichenoid drug eruption,7 leukocytoclastic vasculitis,8 skin hyperpigmentation,9 oral stomatitis,10 although less frequently reported than HFS. HFS skin lesions can develop into PPK if chemotherapy agents are not stopped,2 although rarely reported. The initial complaint in this case report corresponded to the symptoms of HFS manifesting as discomfort on both the palms and soles, followed by diffuse erythematous skin with scales on both palms and soles that sometimes develop blisters that break into erosions. Symptoms of PPK with thickening of the skin on the palms and soles were felt two months after HFS symptoms appeared or three months after consuming capecitabine.
The diagnosis of PPK is established based on history taking, physical examination, and supported by histopathological feature.11 First, acquired PPK must be differentiated from inherited PPK. Acquired PPK generally occurs at an advanced age, whereas inherited PPK is characterized by a relatively early age of onset with familial occurrence. Physical examination of acquired PPK shows thickening of the skin limited to the palms and soles,12 inherited PPK is often accompanied by extracutaneous features.13 The main histopathological feature of PPK is hyperkeratosis. Other features such as acanthosis, parakeratosis, hyperplasia of the stratum spinosum and granulosum, and perivascular inflammatory cell infiltrate can also be found.12 While in contrast, the histopathological features of HFS is epidermal changes range from scattered necrotic keratinocytes with basal layer vacuolar degeneration to full-thickness necrosis that resemble patterns seen in cytotoxic reactions.14 The patient in this case report was diagnosed with acquired PPK based on the history that the onset of the complaint was at a later age, 54 years old, with a negative family history. Physical examination did not show any extracutaneous features, and histopathological examination in accordance with PPK.
The management of acquired PPK due to chemotherapeutic agents includes patient education, symptomatic therapy, and reducing the dose or stopping chemotherapy.15 Various therapeutic options aim to improve symptoms by improving the skin barrier, reducing the thickening of the skin,12 and improving inflammation.15 Potent topical corticosteroid administration can reduce inflammation and show better results when combined with moisturizers, such as vaseline album.6 The patient in the case report was given topical therapy with vaseline album and 0.05% clobetasol propionate cream, which was applied twice daily to the palms and soles. The dose of capecitabine was also reduced by 50% from the initial dose and showed improvement in the skin lesions. Skin thickening, scales, and erythema improved. Improvements in skin lesions were more pronounced after discontinuation of capecitabine.
PPK is a nonlife-threatening condition. Study conducted by Mirali et al3 showed that complete resolution of PPK occurred in the range of two weeks to six months with an average of 2.4 months after chemotherapy discontinuation. The main treatment for acquired PPK is to eliminate the underlying condition.2 Capecitabine, as the suspected etiology of acquired PPK in this case report, had been discontinued for three weeks at the time of the last observation, and the skin lesions were notably improved.
Conclusion
Acquired PPK can be caused by chemotherapeutic agents such as capecitabine. Before starting the medication, patients receiving capecitabine should thoroughly informed and undergo regular follow-up to detect possible side effects. We report a case of PPK that developed after the preceding cutaneous reaction of HFS shortly after capecitabine chemotherapy. Dermatologists and other healthcare providers should be aware that PPK can develop as a sequential event of HFS during capecitabine chemotherapy. Reducing the dose or stopping the drug is the main management strategy for patients with acquired PPK caused by chemotherapeutic agents, as occurred in our patient that showed pronounced clinical improvement after capecitabine was discontinued.
Ethical Statement
Publications of images were included in the patient’s consent to publish the case. The case report has been approved by the Research Ethics Committee of Dr. Hasan Sadikin General Hospital, Bandung, Indonesia (Ethical Clearance No.: LB.02.01/X.6.5/484/2023.
Consent Statement
The authors certify that they have obtained all appropriate patient consent forms. The patient signed a consent form for the publication of case details and images.
Acknowledgments
The authors would like to thank the staff of the Dermatology and Venereology Department and the Anatomical Pathology Department, Faculty of Medicine, Universitas Padjadjaran, Dr. Hasan Sadikin General Hospital, Bandung, West Java, Indonesia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Samuelov L, Sprecher E. Inhereted palmoplantar keratoderma. In: Kang S, Amagai M, Bruckner AL, Enk AH, Margolis DJ, McMichael AJ, editors. Fitzpatrick’s Dermatology.
2. Patel S, Zirwas M, English JC. Acquired palmoplantar keratoderma. Am J Clin Dermatol. 2007;8(1):1–11. doi:10.2165/00128071-200708010-00001
3. Mirali S, Abduelmula A, Mufti A, Sachdeva M, Yeung J. Drugs associated with the development of palmoplantar keratoderma: a systematic review. J Cutan Med Surg. 2021;25(5):553–554. doi:10.1177/12034754211004560
4. Narayana B. Assessment of clinical manifestations related to palmoplantar keratoderma and its impact on quality of life of cases. Indian J Clin Exp Dermatol. 2018;4(4):274–277. doi:10.18231/2581-4729.2018.0057
5. Kundel Y, Nasser NJ, Purim O, et al. Phase II study of concurrent capecitabine and external beam radiotherapy for pain control of bone metastases of breast cancer origin. PLoS One. 2013;8(7):1–6. doi:10.1371/journal.pone.0068327
6. Bianti M, Marina A, Indriatmi W, Widaty S. Hand-foot syndrome due to capecitabine: report of two cases.
7. Gehlhausen JR, Strausburg MB, Aouthmany M, Katona TM, Turner MJ. Capecitabine-induced lichenoid drug eruption: a case report. Dermatol Online J. 2017;23(2):1–4.
8. Al-Shamsi HO, Kee BK, Tetzlaff MT, Wolff RA. Capecitabine-induced leukocytoclastic vasculitis under neoadjuvant chemotherapy for locally advanced colorectal cancer. J Gastrointest Oncol. 2015;6(3):40–43.
9. Adelman M, Veenstra J, Wollner I, McGoey J. Why is my skin turning black? A rare side effect of capecitabine. SKIN J Cutaneous Med. 2020;4(3):275–278. doi:10.25251/skin.4.3.12
10. Mignogna MD, Fortuna G, Falleti J, Leuci S. Capecitabine-induced stomatitis: a likely pathogenetic mechanism of oral lichenoid mucositis. Eur J Clin Pharmacol. 2009;65(10):1057–1059. doi:10.1007/s00228-009-0674-z
11. Mathon S, Singh M. A review on hereditary palmoplantar keratoderma. Sch J Appl Med Sci. 2020;08(03):821–826. doi:10.36347/sjams.2020.v08i03.011
12. Schiller S, Seebode C, Hennies HC, Giehl K, Emmert S. Palmoplantar keratoderma: acquired and genetic causes of a not so rare disease. J Dtsch Dermatol Ges. 2014;12(9):781–788. doi:10.1111/ddg.12418
13. Has C, Technau-Hafsi K. Palmoplantar keratodermas: clinical and genetic aspects. J Dtsch Dermatol Ges. 2016;14(2):123–139. doi:10.1111/ddg.12930
14. Miller KK, Gorcey L, McLellan BN. Chemotherapy-induced hand-foot syndrome and nail changes: a review of clinical presentation, etiology, pathogenesis, and management. J Am Acad Dermatol. 2014;71(4):787–794. doi:10.1016/j.jaad.2014.03.019
15. Kwakman JJM, Elshot YS, Punt CJA, Koopman M. Management of cytotoxic chemotherapy-induced hand-foot syndrome. Oncol Rev. 2020;14(1):442. doi:10.4081/oncol.2020.442
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.