Back to Journals » Orthopedic Research and Reviews » Volume 17
A Rare Case of Multiple Carpometacarpal Joint Fracture-Dislocations with Fractures of the Hamate and Capitate
Authors Ghanem W ![]() , Saber A
, Saber A ![]() , Najjar J, Ezzeddine H
, Najjar J, Ezzeddine H ![]() , Badra M, Moucharafieh R
, Badra M, Moucharafieh R
Received 11 July 2025
Accepted for publication 12 October 2025
Published 27 October 2025 Volume 2025:17 Pages 497—502
DOI https://doi.org/10.2147/ORR.S552996
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Wendy Ghanem,1 Antoine Saber,1 Joseph Najjar,1 Hady Ezzeddine,1 Mohamad Badra,1,2 Ramzi Moucharafieh1,2
1Department of Orthopedics and Traumatology, Faculty of Medicine, University of Balamand, Beirut, Lebanon; 2Department of Orthopedics and Traumatology, Clemenceau Medical Center, Beirut, Lebanon
Correspondence: Wendy Ghanem, Department of Orthopedics and Traumatology, Faculty of Medicine, University of Balamand, Beirut, Lebanon, Email [email protected]
Introduction: Carpometacarpal (CMC) joint dislocations and fracture-dislocations are infrequent and often challenging to diagnose. Among these, dorsal fracture-dislocations involving the capitate and third metacarpal, as well as the hamate with the fourth and fifth metacarpals, represent an exceptionally rare subset. These injuries are typically the result of high-energy mechanisms, such as axial loading transmitted through a clenched fist striking a solid surface. Their subtle clinical signs and often inconspicuous radiographic findings, particularly in the context of polytrauma, contribute to a high rate of missed or delayed diagnoses. This paper aims to highlight the diagnostic challenges and management considerations of these rare dorsal CMC fracture-dislocations, emphasizing the importance of clinical suspicion and appropriate imaging in ensuring timely and effective treatment.
Case Presentation: We report a rare case of dorsal fracture-dislocation involving the capitate–third metacarpal and hamate–fourth/ fifth metacarpal joints. The patient sustained the injury following blunt force trauma consistent with a clenched-fist mechanism. Definitive diagnosis was made following advanced imaging, which guided successful surgical management using open reduction and internal fixation of the hamate, capitate as well as the third and fourth CMC joints with excellent post-operative result and range of motion.
Conclusion: Dorsal fracture-dislocations of the capitate–third and hamate–fourth/fifth metacarpal joints are rare but potentially debilitating. Early recognition through careful clinical evaluation and targeted imaging is critical to prevent chronic pain, stiffness, and impaired hand function.
Keywords: carpometacarpal, hamate, capitate, fracture, dislocation
Introduction
Carpometacarpal (CMC) joint dislocations and fracture-dislocations are rare injuries, accounting for less than 1.5% of all hand trauma cases.1 Among these, dorsal fracture-dislocations involving the capitate with the third metacarpal and the hamate with the fourth and fifth metacarpals are exceptionally uncommon.2 These injuries frequently result from high-energy trauma, with one of the most recognized mechanisms being the axial loading of a clenched fist against a solid object.3 Despite their potential to cause significant functional impairment, such injuries are often overlooked due to their subtle clinical and radiological presentations, particularly in polytrauma patients.
In this case report, we present a rare dorsal fracture-dislocation involving the capitate with the third metacarpal and the hamate with the fourth metacarpal. We discuss the challenges in diagnosis, the importance of recognizing the characteristic mechanism of injury, and the implications of delayed treatment. By increasing awareness of these rare injuries, we aim to highlight the need for meticulous clinical evaluation and appropriate imaging to prevent long-term morbidity in affected patients.
Case Presentation
A 42-year-old male patient, previously healthy, presented to our emergency room after suffering from trauma to his right hand and wrist. The injury occurred during a basketball game, where the patient reports the dorsal aspect of his hand was forced into a hyperflexion moment. Upon presentation he was in severe pain with presence of significant swelling of the ulnar side of his right hand and wrist. Physical exam showed loss of range of motion of the fourth and fifth fingers that was limited to only a few degrees. Sensory function was preserved at the wrist, and the patient had a normal vascular exam.
Radiographs of the right wrist and hand revealed displaced fractures of the capitate and hamate bones associated with posterior displacement of bony fragments measuring up to 11x9mm with suspicion of a dislocation of the third, fourth and fifth carpometacarpal joints (Figure 1).
 |
Figure 1 AP, oblique and lateral views of the right hand and wrist showing displaced fractures of the capitate and hamate with suspicion of dislocation third, fourth and fifth carpometacarpal joints. |
Given the above findings, computed tomography (CT) was then ordered resulting in the following findings (Figure 2): an acute fracture of the capitate involving the distal articular surface at the base of the third metacarpal with posterior and proximal displacement of the dorsal osseous fragment estimated at 7mm. Impaction of the base of the third metacarpal was also noted on the articular surface of the dorsal osseous fragment of the capitate. An acute fracture of the hamate involving its distal articular surface with posterior and proximal displacement of the dorsal osseous fragment estimated to be 6mm. The base of the fourth metacarpal was aligned with the posteriorly displaced osseous fragment. The base of the fifth metacarpal encroached on the posterior wall of the collar osseous garment with the hamate, at the fracture site.
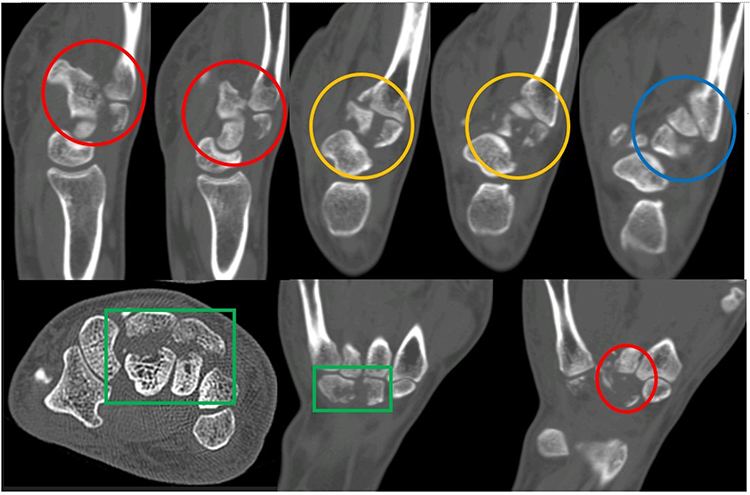 |
Figure 2 Axial, sagittal and coronal cuts of the CT scan of the right hand showing displaced fractures of the capitate and hamate (green rectangle) with dislocation of the third (red circle), fourth (yellow circle) and fifth (blue circle) carpometacarpal joints. |
Based on the findings provided in the CT scan, and after a failed attempt of closed reduction under general anesthesia, the patient was prepared for open reduction internal fixation.
A dorsal approach to the above described fracture dislocations was performed over the right hamate and fourth metacarpal bone. Using a single longitudinal incision, dissection was carried in layers through the fourth dorsal compartment with identification, preservation and careful retraction of all dorsal cutaneous branches. The extensor tendon sheath was incised and retracted. The hamate, capitate fractures and dislocation of the third, fourth and fifth carpometacarpal joints were identified. The capitate and hamate fractures were each reduced and transfixed using 2 cannulated screws under fluoroscopic guidance. The third (third metacarpal and capitate) and fourth (fourth metacarpal and hamate) carpometacarpal joints were then reduced and each fixed using a plate and 5 screws. The fifth carpometacarpal joint was automatically reduced and found to be stable on fluoroscopic control, and no procedure was performed on the carpal ligaments.
A volar splint was applied with the wrist in 30 degrees of extension and the metacarpophalangeal joints in 40 degrees of flexion. The patient’s splint was then removed at 3 weeks post op and early protected active, assisted active and gentle passive range of motion was started.
A full active range of motion was achieved at 6–8 weeks post operatively without any rotational deformity. Contact sports were prohibited for 3 months. Follow up Xrays at 6 months post op showed good reduction and alignment (Figure 3).
 |
Figure 3 AP, oblique and lateral views at 6 months post op showing good bone alignment and reduction. |
Although the third, fourth, and fifth CMC joints are inherently mobile, the across-joint fixation did not result in any limitation of motion or signs of excessive stress on the bridging plates. There was no evidence of mechanical failure or patient discomfort. Consequently, the decision was made to retain the hardware without removal at this stage.
Discussion
Carpometacarpal (CMC) joint dislocations and fracture-dislocations are rare, occurring in less than 2% of all carpal fractures.1 Among these, dorsal fracture-dislocations involving the capitate with the third metacarpal and the hamate with the fourth metacarpal are exceptionally uncommon. A landmark study by Dobyns et al highlighted the rarity of CMC dislocations and fracture-dislocations. In their review of 1621 fractures and dislocations of the hand and wrist over a three-year period at a military hospital, only 3 cases (0.2%) involved these types of injuries.2 This underscores the importance of maintaining a high index of suspicion when evaluating patients with hand trauma, as failure to recognize and promptly treat these injuries can result in chronic instability, persistent pain, reduced grip strength, and post-traumatic arthritis.
The biomechanical forces leading to CMC dislocations and fracture-dislocations have been widely discussed. The predominant mechanism involves a forceful impact delivered through a clenched fist, which transmits axial and rotational forces through the metacarpals to the CMC joints.3 Studies by Cain et al and Prokuski et al support this hypothesis, reporting that over 50% of CMC dislocations occur due to punching or striking a solid object.4,5 Other reported mechanisms include falls onto an outstretched hand and motor vehicle accidents, both of which can generate sufficient force to disrupt the complex stabilizing structures of the CMC joints.
Diagnosing CMC dislocations and fracture-dislocations remains challenging due to their subtle radiographic findings. Standard anteroposterior and lateral views may not adequately reveal the injury, necessitating oblique or stress views, and in some cases, advanced imaging such as CT scans for definitive diagnosis. A missed diagnosis or delayed intervention can lead to long-term functional impairment, emphasizing the need for early recognition and appropriate management. Due to subtle clinical presentations and radiographic findings, these injuries are frequently overlooked, leading to chronic instability, grip weakness, and post-traumatic arthritis.3
The stability of the CMC joints is maintained by a combination of bony congruency, interosseous ligaments, joint capsule integrity, and surrounding musculotendinous attachments. The capitate and hamate bones serve as keystones in the central and ulnar columns of the wrist, respectively, and their disruption can severely compromise hand function.6,7 A fracture-dislocation involving these structures, as seen in our case, is particularly concerning because it disrupts the natural biomechanics of the wrist, affecting grip strength and dexterity.
CMC joint fracture dislocations can be treated non operatively via closed reduction and casting or operatively by closed reduction and internal fixation or open reduction and internal fixation (ORIF). A retrospective study was done by Pundkare et. al reporting 6 cases of CMC joint fracture dislocation treated with ORIF using Kirschner wires. Immobilization was applied for 6 weeks, after which the Kirschner wires were removed and physiotherapy was initiated at 6 weeks post op. Patients had Average Quick DASH score that improved from 75.76 to 1.9 from 6 weeks to 18 months. However, one of the complications encountered post operatively was loss of fracture reduction for which a revision surgery had to be performed.8 Other case reports also described multiple CMC joint fracture dislocations along with fractures of carpal bones that were treated with ORIF using carpal bone plates and Kirschner wire for CMC joint fixation. Physiotherapy was initiated after Kirschner wire removal at 4 to 6 weeks.9,10 On another note, Lai et al reported a CMC joint dislocation concomitant to a capitate fracture that was treated with a dorsal plate. Active range of motion was allowed at 2 weeks post op and the 6-year follow up of the patient showed decrease in pain score and amelioration in functional scores.11
The treatment of CMC fracture dislocations remains controversial; however, the preferred treatment method is ORIF. Compared to ORIF, closed reduction had a higher risk of displacement and redislocation.12,13 On the other hand, ORIF provides a reduction under vision while taking great care to the tendons and surrounding tissue, and most importantly, it allows a stable enough construct to begin early range of motion thus preventing stiffness and chronic pain.
We reported a case of a young man presenting for pain and swelling on the ulnar aspect of the hand after sustaining a trauma. He was found to have fractures of the capitate and hamate with dislocations of the third, fourth and fifth carpometacarpal joints. The third and fourth CMC joints were found to be unstable after closed reduction and percutaneous pinning using Kirschner wires, therefore we opted for ORIF using plates and screws with excellent reduction. ORIF was also preferred in this case due to the patient’s age and the desire to achieve rigid fixation and earlier range of motion. For the fifth CMC joint, it was initially planned to have it fixed using one Kirschner wire, however its stability was tested intraoperatively and was found to be stable on anteroposterior and lateral radiographs, therefore the decision of conservative treatment was then taken. In our review of the literature, there were very few cases of CMC joint fracture dislocations associated with several carpal bones fracture, which makes this a rare case report. Additionally, most of fractures dislocations reported were treated with ORIF using Kirschner wires with good post-operative outcomes, range of motion and functional scores.8,9,14 In fact, the same outcomes and post-operative pain scores and range of motion were also reported with ORIF using locking plates and screws,10,11 which would prompt the need for more comparative case studies and randomized controlled trials regarding the better method of treatment of such fractures dislocations.
Conclusion
This case report presents a dorsal fracture-dislocations involving the capitate with the third metacarpal and the hamate with the fourth and fifth metacarpals which are exceptionally uncommon. Both fractures dislocations were treated surgically with locking plates and screws with excellent post-operative outcomes. Rigid fixation with plate and screws allowed for early rom and achieved full active rom at 6 weeks post operatively. The findings highlight the critical importance of early recognition, the use of appropriate imaging modalities, and timely intervention to minimize the risk of long-term functional impairment. Due to the complex anatomy of the hand and wrist, the management of such cases requires significant clinical experience, detailed anatomical knowledge, and careful surgical planning to ensure optimal outcomes.
Consent and Ethical Considerations
Institutional approval was not required as written informed consent for publication was obtained from the patient. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Acknowledgments
We extend our gratitude to the patient for his cooperation and willingness to participate in this case report. We also thank the healthcare team involved in his care and our colleagues who provided valuable feedback in preparing this report.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The authors have no relevant financial or non-financial interests to disclose for this work.
References
1. Siddiqui YS, Zahid M, Sabir AB, et al. Multiple carpometacarpal fracture dislocation of the hand: an uncommon pattern of injury which is often missed: a case report with review of literature. J Clin Diagn Res. 2011;5:618–620.
2. Dobyns JH, Linscheid RL, Cooney WP. Fractures and dislocations of the wrist and hand, then and now. J Hand Surg Am. 1983;8(5 Pt 2):687–690. doi:10.1016/S0363-5023(83)80247-0
3. Yoshida R, Shah MA, Patterson RM, Buford WL, Knighten J, Viegas SF. Anatomy and pathomechanics of ring and small finger carpometacarpal joint injuries. J Hand Surg Am. 2003;28(6):1035–1043. doi:10.1016/s0363-5023(03)00373-3
4. Prokuski LJ, Eglseder WA. Concurrent dorsal dislocations and fracture-dislocations of the index, long, ring, and small carpometacarpal joints. J Orthop Trauma. 2001;15(8):549–554. doi:10.1097/00005131-200111000-00003
5. Cain JE, Shepler TR, Wilson MR. Hamatometacarpal fracture-dislocation: classification and treatment. J Hand Surg Am. 1987;12(5):762–767. doi:10.1016/S0363-5023(87)80064-3
6. Hartwig RH, Louis DS. Multiple carpometacarpal dislocations. A review of four cases. J Bone Joint Surg Am. 1979;61(6A):906–908. PMID: 479239. doi:10.2106/00004623-197961060-00018
7. El-Shennawy M, Nakamura K, Patterson RM, Viegas SF. Three-dimensional kinematic analysis of the second through fifth carpometacarpal joints. J Hand Surg Am. 2001;26(6):1030–1035. PMID: 11721246. doi:10.1053/jhsu.2001.28761
8. Pundkare GT, Patil AM. Carpometacarpal joint fracture dislocation of second to fifth finger. Clin Orthop Surg. 2015;7(4):430–435. PMID: 26640624; PMCID: PMC4667109. doi:10.4055/cios.2015.7.4.430
9. Al-Battat MY, Al Hassan MA, Al Qahtani SM. Carpometacarpal dislocation second to fifth with associated hamate fracture: a case report of rare injury. Int J Surg Case Rep. 2023;108:108417. PMID: 37348202; PMCID: PMC10382768. doi:10.1016/j.ijscr.2023.108417
10. Iwata N, Komura S, Hirakawa A, et al. Dorsal buttress plate fixation for the treatment of fracture-dislocation of the fifth carpometacarpal joint with avulsion fracture of the hamate: a case report. Arch Orthop Trauma Surg. 2019;139(1):135–139. PMID: 30413942. doi:10.1007/s00402-018-3072-0
11. Lai CC, Fang HW, Chang CH, et al. Unusual capitate fracture with dorsal shearing pattern and concomitant carpometacarpal dislocation with a 6-year follow-up: a case report. World J Clin Cases. 2023;11(9):2060–2066. PMID: 36998955; PMCID: PMC10044964. doi:10.12998/wjcc.v11.i9.2060
12. Sharma AK, John JT. Unusual case of carpometacarpal dislocation of all the four fingers of ulnar side of hand. Med J Armed Forces India. 2005;61(2):188–189. PMID: 27407748; PMCID: PMC4922986. doi:10.1016/S0377-1237(05)80024-3
13. Jilani LZ, Abbas M, Goel S, Akhtar MN. Multiple volar dislocations of the carpometacarpal joints with an associated fracture of the first metacarpal base. Chin J Traumatol. 2014;17(1):38–40. PMID: 24506922.
14. Suwannaphisit S, Suwanno P, Fongsri W, Wongsiri S. Multiple carpometacarpal joint fracture-dislocation from the second to fifth: a case report. Ann Med Surg. 2022;76:103596. PMID: 35495402; PMCID: PMC9052289. doi:10.1016/j.amsu.2022.103596
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.