Back to Journals » Infection and Drug Resistance » Volume 17
A Rare Case of Infective Endocarditis with Recurrent Fever Caused by Elizabethkingia anophelis
Authors Tang X, Liu Z, Li D, Xiong Y, Liao K, Chen Y ![]()
Received 14 August 2024
Accepted for publication 18 October 2024
Published 23 October 2024 Volume 2024:17 Pages 4625—4632
DOI https://doi.org/10.2147/IDR.S483796
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Xiuxin Tang,1,* Zhiyun Liu,2,* Danni Li,3 Yan Xiong,3 Kang Liao,1 Yili Chen1
1Department of Laboratory Medicine, The First Affiliated Hospital of Sun Yat-Sen University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Clinical Laboratory, Huizhou Central People ‘s Hospital, Huizhou, Guangdong, 516001, People’s Republic of China; 3Department of Emergency Medicine, The First Affiliated Hospital of Sun Yat-Sen University, Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yili Chen, Department of Laboratory Medicine, The First Affiliated Hospital of Sun Yat-sen University, No. 58 Zhongshan Er Road Guangzhou, Guangzhou, Guangdong Province, 510080, People’s Republic of China, Tel +8620-87330808-8461, Fax +8620-87330808, Email [email protected]
Background: Elizabethkingia anophelis, an opportunistic pathogen that can cause infections in multiple parts of the human body, has multiple drug resistance and a high mortality rate. However, there have been few reports of infective endocarditis (IE) caused by Elizabethkingia anophelis, which means that diagnosis and treatment face challenges that cannot be ignored. Rapid and accurate identification and drug sensitivity results are needed to make timely treatment adjustments.
Case Presentation: An 81-year-old man presented with recurrent fever and increased infection index for more than a month. Based on his clinical symptoms, infection index, reduplicative blood cultures, and results of transesophageal echocardiography, he was ultimately diagnosed with infective endocarditis caused by Elizabethkingia anophelis. The patient had a favorable outcome with a 6-week course of intravenous antibiotic therapy.
Conclusion: This is a rare and successfully cured case of IE caused by the pathogen of Elizabethkingia anophelis, which is difficult not only in diagnosis but also in treatment. This case provides a certain referential significance to the treatment of Elizabethkingia anophelis-caused IE in clinical practice.
Keywords: Elizabethkingia anophelis, infective endocarditis, drug resistance, treatment
Introduction
Elizabethkingia anophelis, belonging to the genus Elizabethkingia, is a strain of Gram-negative, aerobic, oxidase-positive, oxidase-positive, indole-positive, non-fermenting, and non-motile bacillus.1 It exists widely in natural environments such as soil and water and meanwhile can be also isolated from dry and moist clinical environmental and equipment surfaces and intravenous lipid solutions in the hospital.2,3 It is worth noting that Elizabethkingia anophelis is an emerging pathogen and has increasingly caused severe infections in human beings. The first case of neonatal meningitis infected by Elizabethkingia anophelis was reported in the Central Africa Republic in 2011.4 In recent years, there have been shocking outbreaks of Elizabethkingia anophelis-caused infections in Singapore, Hong Kong, Taiwan, the USA, and South Korea.5–10 It has been reported that the infection of Elizabethkingia anophelis had two prominent features: multiple drug resistance and high mortality,11,12 both of which seriously threaten human’s life and health. The predisposition factors of Elizabethkingia anophelis infection include long-term use of antibiotics, immunosuppression, catheter retention, and prior invasive surgery. Moreover, Elizabethkingia anophelis can cause bacteraemia, eye infections, pneumonia, neonatal meningitis and so on.13–15 Unfortunately, people have limited understanding of Elizabethkingia anophelis, which poses an obstacle to the management of their infection. It is particularly noteworthy that E. anophelis has not been reported to cause IE, so there is a large gap in the management of E. anophelis-associated IE.
Here, we report the first case of IE caused by Elizabethkingia anophelis, with difficulties in the diagnosis and treatment because of concealed symptoms and drug resistance. In this case, IE was finally diagnosed through a variety of examinations. Elizabethkingia anophelis developed induced resistance to multiple drugs in just one week, which brought great challenges to anti-infection therapy. Therefore, clinical attention should be paid to the early diagnosis of IE, new drug resistance phenotypes of bacteria and timely adjustments should be made.
Case Presentation
An 81-year-old male, with a history of hypertension and cerebral infarction, was admitted to hospital (The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, China), due to recurrent fever for more than one month. On examination, he had a body temperature of 37.7°C, blood pressure of 118/60 mmHg, pulse rate of 97/min and respiratory rate of 28/min. Laboratory evaluation revealed increased white blood cell of 15.84*10^9/L, C-reactive protein 56.17mg/L and procalcitonin 2.77ng/mL. On the next day after admission, his both hands venous and central venous catheter (CVC) blood culture were reported positive after 16.1 hours. Blood culture smear showed gram-negative bacteria(G−b) (Figure 1). After blood culture inoculation on Columbia blood agar, there were white, raised and moist colonies growing after 24h incubation (Figure 2). It was identified as Elizabethkingia anophelis by matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS) (bioMérieux, Marcy l’Etoile, France) (Figure 3). Bronchoalveolar lavage fluid (BALF) and next-generation sequencing (NGS) result revealed 17956 total reads corresponding to Elizabethkingia anophelis, with 30.7% coverage and 89% relative abundance in bacteria (Table 1). The antibiotic sensitivity profile of Elizabethkingia anophelis showed resistance to aztreonam and colistin (Table 2). Targeted antibiotic therapy with intravenous drip of meropenem 1.0 g every 8 h, vancomycin 0.5 g twice-daily (Q12H) and minocycline 100 mg once daily (QD) was started. His body temperature and inflammation indexes began to decrease on Day 4.
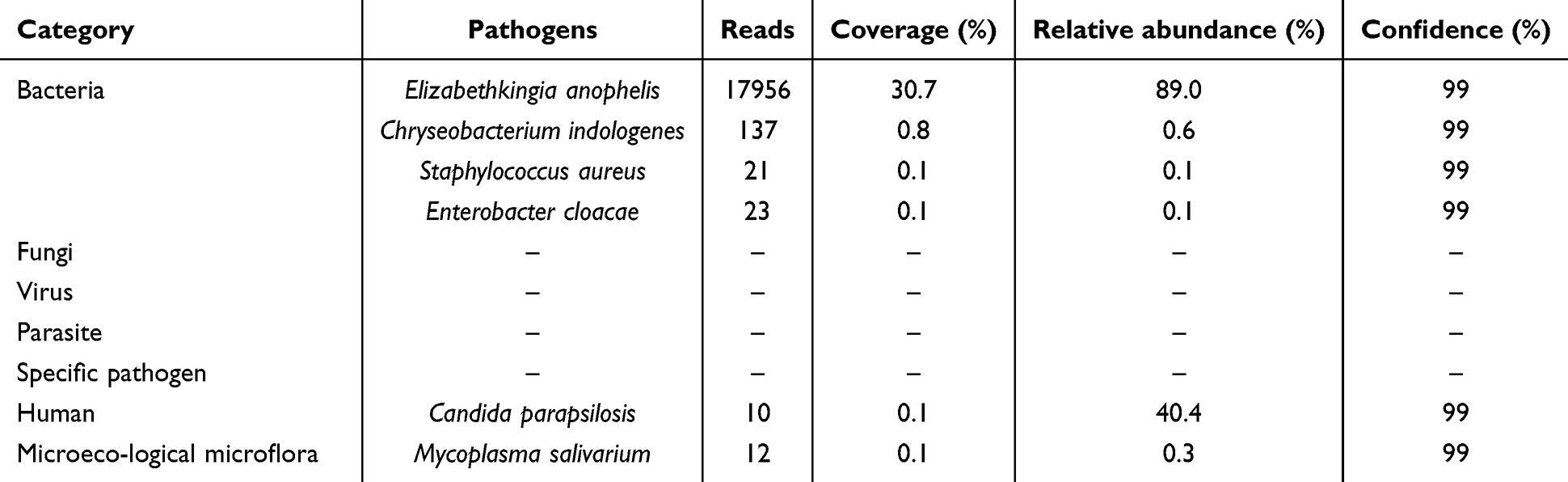 |
Table 1 The Micro-Organisms Were Detected by BALF NGS on Day 3 |
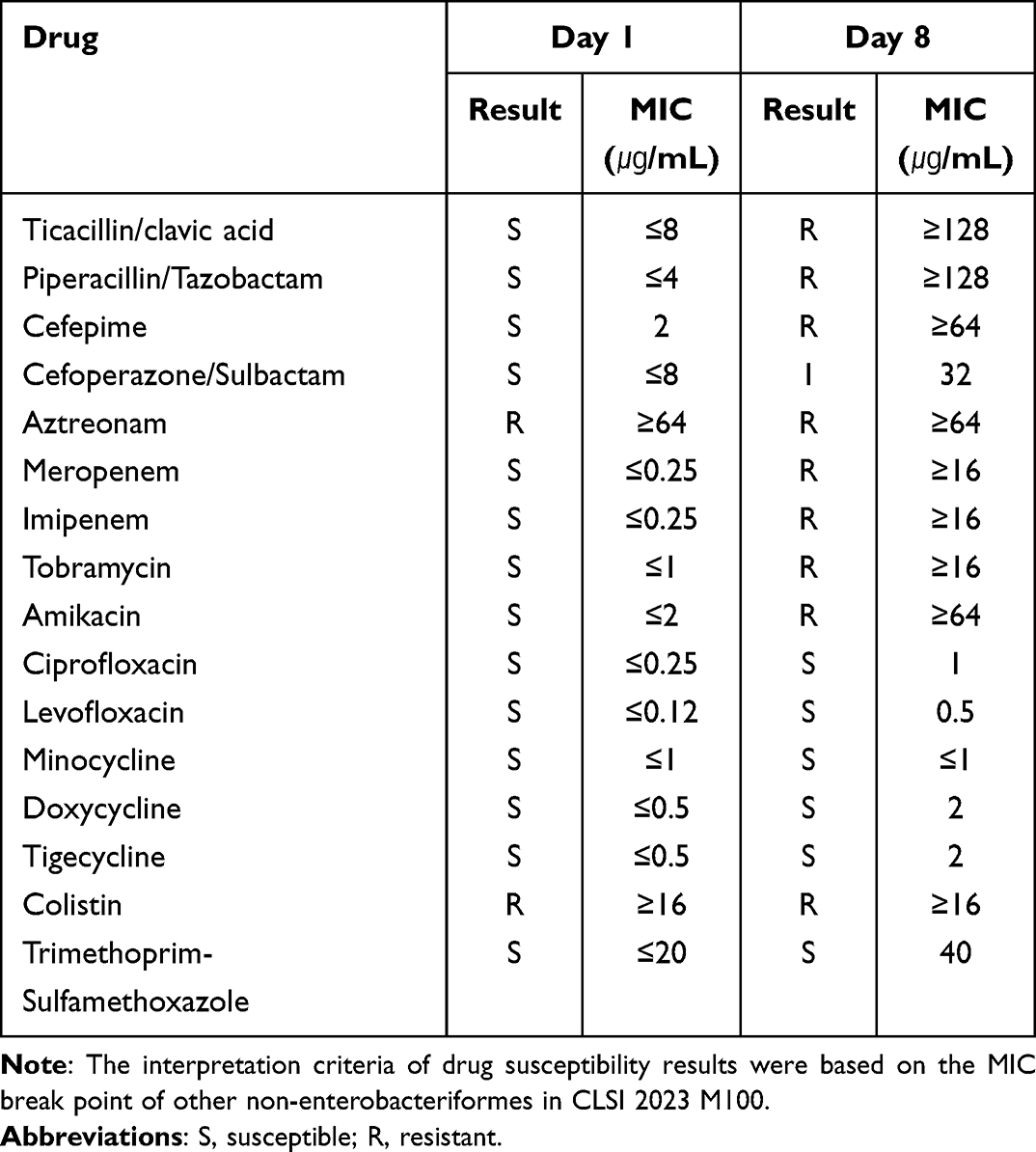 |
Table 2 The Antibiotic Sensitivity Profile of Elizabethkingia Anophelis from Blood Culture |
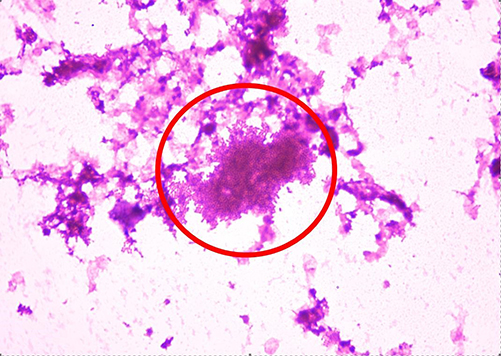 |
Figure 1 Blood culture smear showed gram-negative bacteria (as indicated by the red circle). |
 |
Figure 2 White, raised, moist colonies appeared on the blood-agar plate 24 h after incubation. |
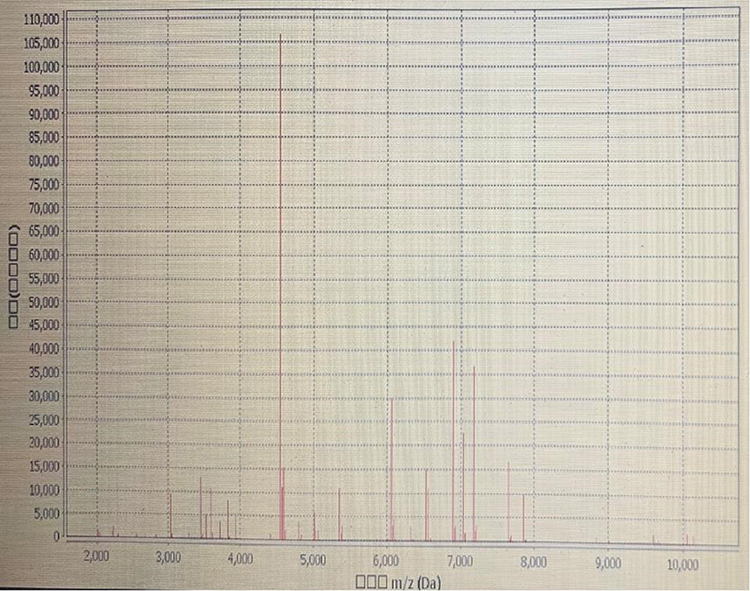 |
Figure 3 It was identified as Elizabethkingia anophelis by matrix-assisted laser desorption ionization time-of-flight mass spectrometry. |
However, the patient began to experience recurrent fever from Day 7 onwards. Elizabethkingia anophelis strains were still repeatedly isolated from blood culture and sputum culture, and the results of metagenomic next-generation sequencing (mNGS) were consistent (Figure 4). The Elizabethkingia anophelis isolated on Day 8 developed resistance to β-lactam drugs (Table 2), so that the treatment was switched to omacycline 100 mg intravenously (i.v). QD and polymyxin 750000 IU i.v. Q12H. Then, omacycline was first switched to tigecycline 75mg i.v. Q12H and then to cefoperazone-sulbactam 3 g iv. drip Q6H because of repeatedly positive blood cultures. In addition, levofloxacin 0.5g i.v. QD and trimethoprim-sulfamethoxazole 0.96 g nasal feeding every 6 h were added according to the antibiotic sensitivity profile of Elizabethkingia anophelis.
 |
Figure 4 Treatment timeline including changes of Indicators of infection and etiology detection timepoints. |
After re-adjusting the medication regimen, the patient still experienced recurrent fever for over 3 weeks, and Elizabethkingia anophelis strains were still isolated from blood culture for multiple times. During the process of actively searching for the primary infection site, combining chest X ray which indicated pneumonia (Figure 5) and transthoracic cardiac color ultrasound which found a vegetation found on the aortic valve (Figure 6), the diagnosis was considered as infectious endocarditis (IE). Taking into account the tissue concentration of sensitive drugs, the final antibiotherapy was adjusted to cefoperazone sodium/ sulbactam sodium 3g i.v. every 6 hours (Q6H) and levofloxacin 0.75g i.v. QD. After one week of treatment, the patient’s body temperature and inflammatory indicators gradually decreased to normal, and blood culture specimen also achieved microbial clearance. Due to the older age of the patient, surgical surgery was not recommended in clinical practice. The patient’s condition improved and was discharged on Day 61.
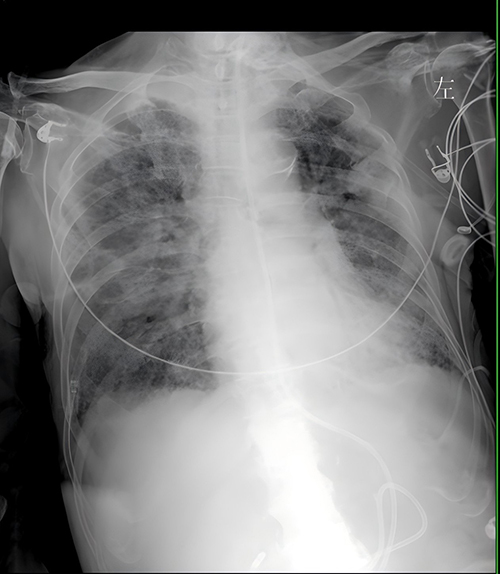 |
Figure 5 The chest X ray indicated pneumonia. |
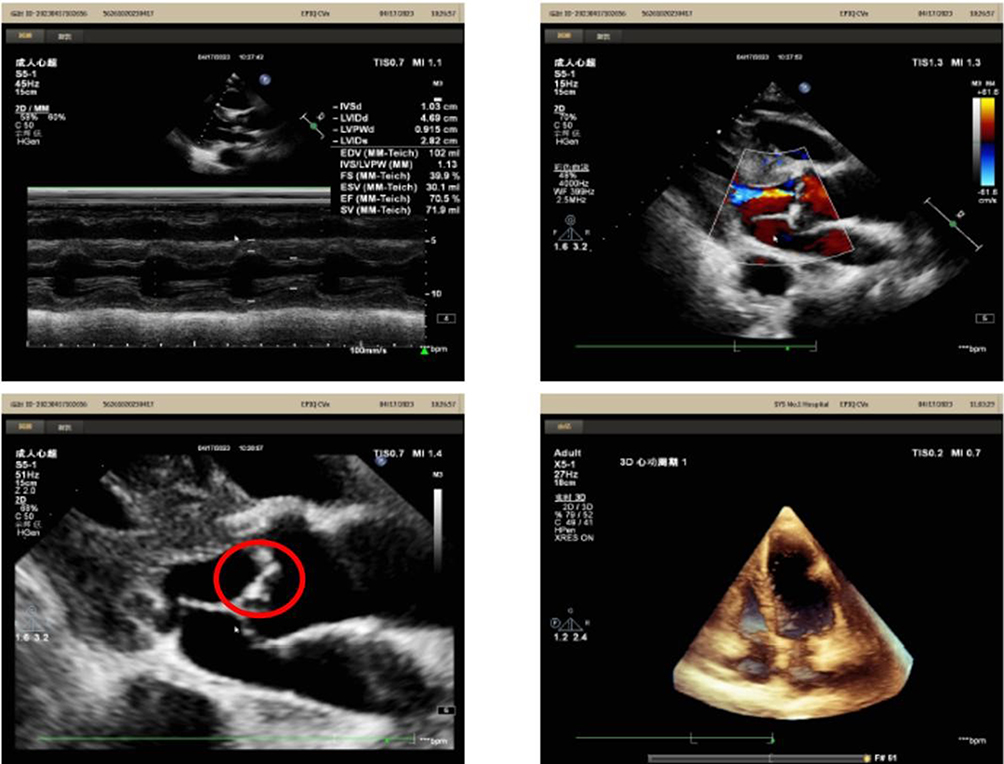 |
Figure 6 The echocardiograph images indicated existence of vegetation (as indicated by the red circle). |
Discussion
Currently, people’s knowledge about Elizabethkingia anophelis is still limited. It is worth noting that there have been several outbreaks of Elizabethkingia anophelis-associated infections worldwide in recent years. A hospital in South Korea reported that the infection rate of Elizabethobacteria among inpatients increased from 0.02‰ in 2009 to 0.88‰ in 2017.8 The first outbreak of Elizabethkingia anophelis infection occurred in Singapore in 2012, resulting in 60% of deaths from sepsis.7 Moreover, Elizabethkingia anophelis infection occurred in Wisconsin, Illinois, and Michigan in the United States, which led to a mortality rate of 30.8%–70% during 2014 to 2016.5,6,9,10 It is proved that Elizabethkingia anophelis possesses a series of pathogenic factors, including capsule, lipopolysaccharide, endopeptidase, lipid biosynthesis and metabolites, magnesium transporters, heat shock protein, catalase, peroxidase, superoxide dismutase, etc.16,17 In particular, it is found that the species identification of Elizabethkingia anophelis is often misidentified as E. meningoseptica by VITEK 2 GN, API 20E and API 20NE systems,18 while it can be accurately identified by MALDI-TOF MS and 16S rRNA.3
Due to its ability to form biofilms, produce β- lactamases or encode efflux pumps genes, Elizabethkingia anophelis is resistant to many antibiotics commonly used clinical, such as β-lactam drugs and tetracycline.19–21 Whole-genome sequencing (WGS) revealed that Elizabethkingia anophelis carries serine beta-lactamase A (CME) gene and two metal-β-lactamases B (GOB and BLAB) genes on its chromosome. It is found that minocycline combined with levofloxacin is the most effective treatment against Elizabethkingia anophelis, when comparing to the regimen of minocycline or tigecycline combined with either ciprofloxacin in vitro and in vivo studies.22 YASMIN M et al23 reported that the combination of ceftazidime-avibactam and aztreonam was ineffective against Elizabethkingia anophelis bacteremia and pneumonia in a patient with relapsed acute myelogenous leukemia, while cefiderocol contributed to the microbiologic clearance. In the present case, Elizabethkingia anophelis showed induced resistance to multiple drugs in just one week, which brought great challenges to treatment. Therefore, it is necessary to closely monitor the emergence of new drug-resistant phenotypes.
To our knowledge, this is the first case report on IE caused by Elizabethkingia anophelis. IE is a rare and life-threatening disease.24 However, the diagnosis of IE usually requires a combination of clinical microbiological and echocardiography result. The pathogens commonly cause IE includes Staphylococcus aureus, Streptococci viridans and so on, but they have changed significantly due to the extensive use of broad-spectrum antibiotics, indicating that almost all known pathogenic microorganisms can cause IE.25 According to the updated diagnostic criteria,26 the patient’s diagnosis meets one primary criterion (IE indicated by cardiac ultrasound) and three secondary criteria (host susceptibility factors, fever symptoms, and pathogenic evidence). It was believed that in this patient, Elizabethkingia anophelis first caused respiratory infection, then spread into the blood to proliferate, reside and invade the originally normal aortic valve, eventually causing IE.
Conclusion
Elizabethkingia anophelis is a pathogen with high rate of drug resistance and increasing infection cases, which needs urgent attention. Further studies are required to enhance the awareness and develop effective therapies for Elizabethkingia anophelis-caused IE patients. Laboratories should improve the ability to identify the bacteria and monitor its drug resistance closely. Multidisciplinary communication is important so as to better reach the accurate diagnosis and treatment of infectious diseases.
Abbreviations
IE, infective endocarditis; CVC, central venous catheter; G−b, gram-negative bacteria; MALDI-TOF MS, matrix-assisted laser desorption ionization-time-of-flight mass spectrometry; BALF, Bronchoalveolar lavage fluid; NGS, Next-generation sequencing; QD, Quaque die; mNGS, metagenomic next-generation sequencing; WGS, Whole-genome sequencing.
Ethics Approval and Consent to Participate
The study publication of the case details was approved by the Research Ethics Committee of The First Affiliated Hospital of Sun Yat-sen University approved the study ([2023]758). Consent for publication: Written informed consent was obtained from the patient for publication of this Case Report and any accompanying images.
Acknowledgments
We express our sincere gratitude for the unwavering trust bestowed upon our medical team by the patient throughout the entire treatment process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hu S, Xu H, Meng X, et al. Population genomics of emerging Elizabethkingia anophelis pathogens reveals potential outbreak and rapid global dissemination[J]. Emerg Microbes Infect. 2022;11(1):2590–2599. doi:10.1080/22221751.2022.2132880
2. S JS, Lee WS, L CF, et al. Elizabethkingia meningoseptica: an important emerging pathogen causing healthcare-associated infections[J]. J Hosp Infect. 2014;86(4):244–249. doi:10.1016/j.jhin.2014.01.009
3. K KK, Kim MK, H LJ, et al. Transfer of Chryseobacterium meningosepticum and Chryseobacterium miricola to Elizabethkingia gen. nov. as Elizabethkingia meningoseptica comb. nov. and Elizabethkingia miricola comb. nov[J]. Int J Syst Evol Microbiol. 2005;55(3):1287–1293. doi:10.1099/ijs.0.63541-0
4. Frank T, C GJ, B NL, et al. First case of Elizabethkingia anophelis meningitis in the Central African Republic[J]. Lancet. 2013;381(9880):1876. doi:10.1016/S0140-6736(13)60318-9
5. N LJ, H LC, Yang CH, et al. Clinical manifestations, molecular characteristics, antimicrobial susceptibility patterns and contributions of target gene mutation to fluoroquinolone resistance in Elizabethkingia anophelis[J]. J Antimicrob Chemother. 2018;73(9):2497–2502. doi:10.1093/jac/dky197
6. Perrin A, Larsonneur E, C NA, et al. Evolutionary dynamics and genomic features of the Elizabethkingia anophelis 2015 to 2016 Wisconsin outbreak strain[J]. Nat Commun. 2017:15483. doi:10.1038/ncomms15483
7. Teo J, Y TS, Tay M, et al. First case of E anophelis outbreak in an intensive-care unit[J]. Lancet. 2013;382(9895):855–856. doi:10.1016/S0140-6736(13)61858-9
8. Janda JM, Lopez DL. Mini review: new pathogen profiles: elizabethkingia anophelis[J]. Diagn Microbiol Infect Dis. 2017;88(2):201–205. doi:10.1016/j.diagmicrobio.2017.03.007
9. Navon L, J CW, Morgan J, et al. Notes from the Field: investigation of Elizabethkingia anophelis Cluster- Illinois, 2014-2016[J]. MMWR Morb Mortal Wkly Rep. 2016;65(48):1380–1381. doi:10.15585/mmwr.mm6548a6
10. H CM, Kim M, J JS, et al. Risk Factors for Elizabethkingia Acquisition and Clinical Characteristics of Patients, South Korea[J]. Emerg Infect Dis. 2019;25(1):42–51. doi:10.3201/eid2501.171985
11. N LJ, H LC, Yang CH, et al. Elizabethkingia Infections in Humans: from Genomics to Clinics[J]. Microorganisms. 2019;7(9). doi:10.3390/microorganisms7090295
12. K LS, N CW, H FC, et al. Elizabethkingia anophelis bacteremia is associated with clinically significant infections and high mortality[J]. Sci Rep. 2016:26045. doi:10.1038/srep26045
13. Hu S, Jiang T, Zhang X, et al. Elizabethkingia anophelis Isolated from Patients with Multiple Organ Dysfunction Syndrome and Lower Respiratory Tract Infection: report of Two Cases and Literature Review[J]. Front Microbiol. 2017;8:382. doi:10.3389/fmicb.2017.00382
14. P BE, Manivannan B, Mahalingam N, et al. Comparative genomic analysis of a naturally competent Elizabethkingia anophelis isolated from an eye infection[J]. Sci Rep. 2018;8(1):8447. doi:10.1038/s41598-018-26874-8
15. Reed T, Watson G, Kheng C, et al. Elizabethkingia anophelis Infection in Infants, Cambodia, 2012-2018[J]. Emerg Infect Dis. 2020;26(2):320–322. doi:10.3201/eid2602.190345
16. Li Y, Liu Y, C CS, et al. Complete Genome Sequence and Transcriptomic Analysis of the Novel Pathogen Elizabethkingia anophelis in Response to Oxidative Stress[J]. Genome Biol Evol. 2015;7(6):1676–1685. doi:10.1093/gbe/evv101
17. Chen S, Bagdasarian M, Walker ED. Elizabethkingia anophelis: molecular manipulation and interactions with mosquito hosts[J]. Appl Environ Microbiol. 2015;81(6):2233–2243. doi:10.1128/AEM.03733-14
18. L CK, Cheng B, Lin R, et al. Elizabethkingia anophelis Is the Dominant Elizabethkingia Species Found in Blood Cultures in Singapore[J]. J Clin Microbiol. 2018;56(3). doi:10.1128/JCM.01445-17
19. Breurec S, Criscuolo A, Diancourt L, et al. Genomic epidemiology and global diversity of the emerging bacterial pathogen Elizabethkingia anophelis[J]. Sci Rep. 2016;6:30379. doi:10.1038/srep30379
20. H CY, L PC, J JM, et al. Multicentre study evaluating matrix-assisted laser desorption ionization-time of flight mass spectrometry for identification of clinically isolated Elizabethkingia species and analysis of antimicrobial susceptibility[J]. Clin Microbiol Infect. 2019;25(3):340–345. doi:10.1016/j.cmi.2018.04.015
21. S HM, Kim H, Lee Y, et al. Relative Prevalence and Antimicrobial Susceptibility of Clinical Isolates of Elizabethkingia Species Based on 16S rRNA Gene Sequencing[J]. J Clin Microbiol. 2017;55(1):274–280. doi:10.1128/JCM.01637-16
22. N LJ, H LC, Huang YH, et al. Antimicrobial Effects of Minocycline, Tigecycline, Ciprofloxacin, and Levofloxacin against Elizabethkingia anophelis Using In Vitro Time-Kill Assays and In Vivo Zebrafish Animal Models[J]. Antibiotics. 2021;10(3). doi:10.3390/antibiotics10030285
23. Yasmin M, J RL, H MS, et al. Characterization of a Novel Pathogen in Immunocompromised Patients: elizabethkingia anophelis-Exploring the Scope of Resistance to Contemporary Antimicrobial Agents andβ-lactamase Inhibitors[J]. Open Forum Infect Dis. 2023;10(2):d14. doi:10.1093/ofid/ofad014
24. Cimmino G, Bottino R, Formisano T, et al. Current Views on Infective Endocarditis: changing Epidemiology, Improving Diagnostic Tools and Centering the Patient for Up-to-Date Management[J]. Life. 2023;13(2). doi:10.3390/life13020377
25. G FV, T DD, Selton-Suty C, et al. The 2023 Duke-ISCVID Criteria for Infective Endocarditis: updating the Modified Duke Criteria[J]. Clin Infect Dis. 2023 doi:10.1093/cid
26. G FV, T DD, Selton-Suty C, et al. The 2023 Duke-International Society for Cardiovascular Infectious Diseases Criteria for Infective Endocarditis: updating the Modified Duke Criteria[J]. Clin Infect Dis. 2023;77(4):518–526. doi:10.1093/cid/ciad271
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.