Back to Archived Journals » Open Access Surgery » Volume 15
A Quasi-Experimental Study Compared the Learning Experiences of Inexperienced Trainees Using Laparoscopic Surgery with 2-Dimensional and 3-Dimensional Imaging Systems
Authors Paleekupt J, Sukhvibul P, Tansawet A, Kasetsermwiriya W, Laopeamthong I, Techapongsatorn S ![]()
Received 8 January 2022
Accepted for publication 15 March 2022
Published 25 March 2022 Volume 2022:15 Pages 25—29
DOI https://doi.org/10.2147/OAS.S357311
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Luigi Bonavina
Jiroot Paleekupt,1 Pakkapol Sukhvibul,2 Amarit Tansawet,2 Wisit Kasetsermwiriya,2 Issaree Laopeamthong,2 Suphakarn Techapongsatorn2
1Department of Surgery, Surin Hospital, Surin, Thailand; 2Department of Surgery, Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand
Correspondence: Suphakarn Techapongsatorn, Department of Surgery, Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand, Email [email protected]
Objective: This study aimed to compare surgical residency training learning curves using 2-dimensional (2D) and 3-dimensional (3D) laparoscopic views.
Materials and Methods: Twenty surgical residents were divided into two groups according to their laparoscopic view: 2D and 3D. The seven tasks (peg transfer, pattern cutting, threading, rubber banding, ball transfer, specimen retrieval, and suturing) of the essential laparoscopic training box were performed. The time taken to complete each task was recorded and analyzed. After performing all the tasks, the participants were asked to complete a questionnaire of their experience with the equipment.
Results: The time taken for the 3D group was significantly faster than that of the 2D group for peg transferring (3.44 vs 2.69, p < 0.0001), threading (3.02 vs 2.63, p = 0.0027), ball transferring (4.45 vs 3.40, p = 0.0001), specimen retrieval (3.78 vs 2.99, p < 0.0001), and suturing (13.62 vs 11.13, p < 0.0001). The 3D group was also faster in pattern cutting (2.81 vs 2.63, p = 0.17) and rubber banding (2.8 vs 2.78, p = 0.83), but the difference was not significant. After the training, 60% of the participants in the 3D group reported eye strain on the questionnaire.
Conclusion: The 3D laparoscopic view improves surgical performance and learning for surgical residents over that of the 2D laparoscopic view.
Keywords: learning curve, 2-dimensional, 3-dimensional laparoscopic view
Introduction
Recent advances in laparoscopic surgery have evolved many procedures and changed the surgical paradigm. Laparoscopic surgery has become an alternative surgical technique in patient care.1 The standard treatment for some diseases, like cholecystitis, is now laparoscopic surgery. This is because it reduces patients’ pain after surgery, speeds their recovery, and shortens their stay in the hospital.2–4 However, successful laparoscopy requires a high level of surgical skill such as hand-eye coordination and laparoscopic instrument control due to the lack of fine touch sensation and on-screen visualization, where images may differ from real images in terms of depth. Thus, to achieve surgical success and minimize complications, skillful training on laparoscopy is required for inexperience trainee. Several methods of learning experience, such as lectures, videos, live demonstrations, or hands-on workshops in laparoscopic surgery, are now part of the training program for both medical students and surgical residents.
One factor affecting laparoscopic surgery or skill training is on-screen image visualization. The recent of a camera system that provides on-screen image visualization of the operative field includes 2-dimensional (2D), 3-dimensional (3D), and 4K resolution ultra-high-definition display technique (4098 x 2160 pixels).
The purpose of this study was to evaluate and compare the effects of the 2D and 3D laparoscopic views on the learning period of essential laparoscopic training skills in surgical residents.
Materials and Methods
A quasi-experimental study was conducted using an essential laparoscopic training workshop that was arranged for new surgical residents every academic year from 2016–2019. First-year surgical residents and sixth-year medical student were recruited for this study by voluntarily inviting them to participate in it. Those willing to participate in this study will sign an informed consent form. All the surgical residents were given a detailed explanation of the study’s objective and divided into two groups according to their laparoscopic view (2D and 3D groups). The recorded times of the following seven essential laparoscopic box training tasks (peg transfer, pattern cutting, threading, rubber banding, ball transfer, specimen retrieval, and suturing) were used to evaluate training skill (Figure 1). The main outcome of this study was learning experience by taking their time with each task. The second outcome was how they felt after using the instruments.
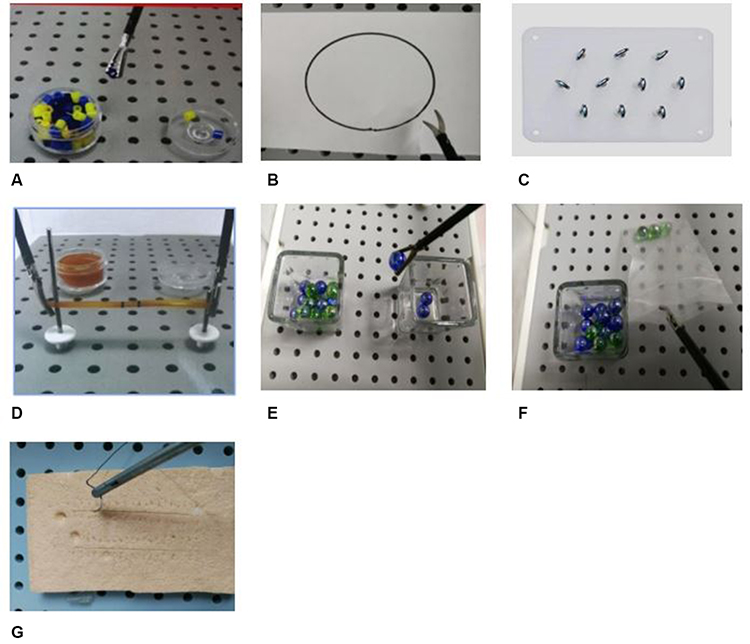 |
Figure 1 The seven essential laparoscopic training tasks, (A) peg transferring, (B) pattern cutting, (C) threading, (D) rubber banding, (E) ball transfer, (F) specimen retrieval, (G) suturing. |
The data of this study were analyzed by the STATA version 15 program. Comparison of continuous variables was performed using the Mann–Whitney U-test as the data had a non-normal distribution. P-values of <0.05 were considered statistically significant. Descriptive data are presented as numbers and percentages.
Results
From 2016 to 2019, this study recruited 40 first-year surgery residents and sixth-year medical student for evaluation (Figure 2). Table 1 demonstrated baseline characteristics of participant. Table 2 shows the recorded times of each task for both groups. The time taken for the 3D group was significantly faster than that of the 2D group in peg transferring (3.44 vs 2.69, p < 0.0001), threading (3.02 vs 2.63, p = 0.0027), ball transferring (4.45 vs 3.40, p = 0.0001), specimen retrieval (3.78 vs 2.99, p < 0.0001), and suturing (13.62 vs 11.13, p < 0.0001). The 3D group was also faster than the 2D group in pattern cutting (2.81 vs 2.63, p = 0.17) and rubber banding (2.8 vs 2.78, p = 0.83), but the difference was not significant. However, about 60% of the participants in the 3D group experienced eye-strain after using the 3D instruments.
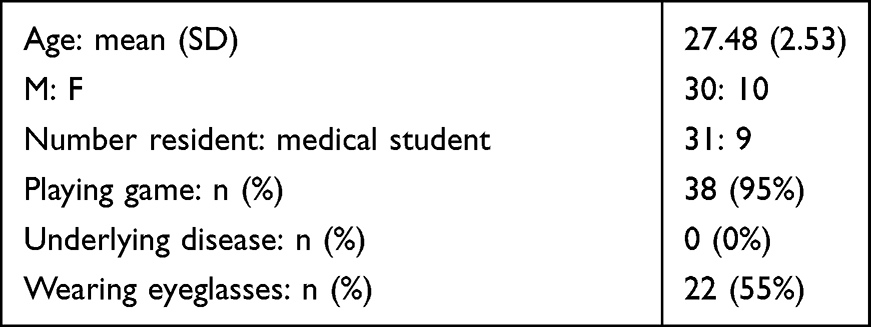 |
Table 1 Baseline Characteristic of Participant |
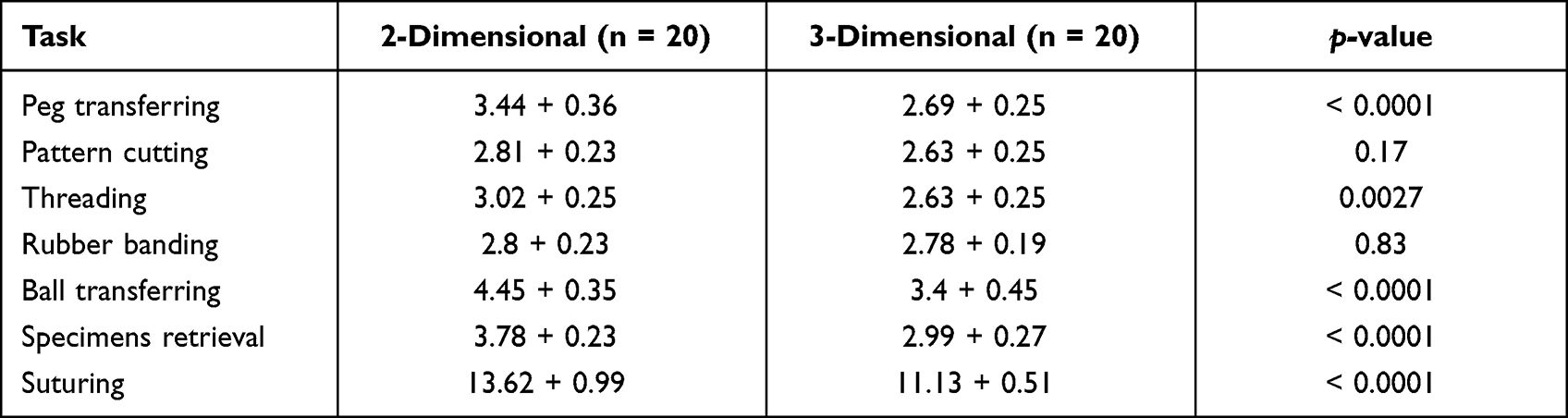 |
Table 2 Time (Minutes) to Perform Each Task of Essential Laparoscopic Box Training |
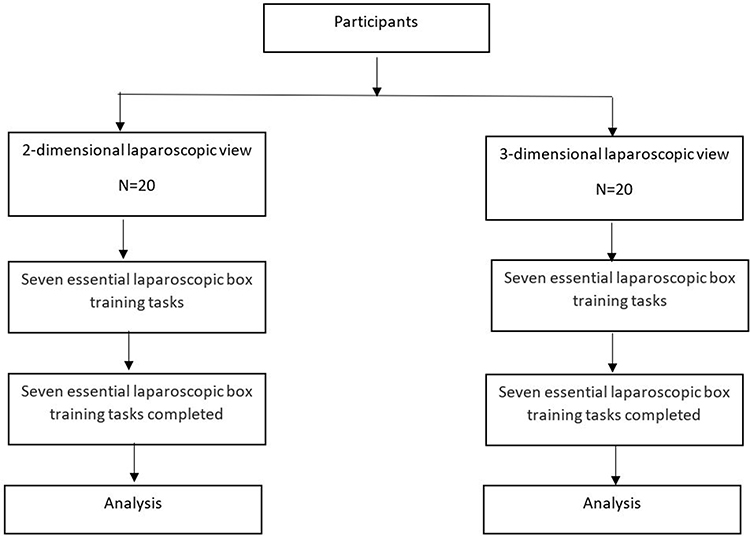 |
Figure 2 Flow diagram of study participants. |
Discussion
Laparoscopic surgery works by converting an image through a camera head and transferring the signal onto a TV screen, where the viewed images are usually two-dimensional. The disadvantages of traditional laparoscopy include its lack of in-depth perception and that it requires surgeons with advanced surgical skill and hand-eye coordination. Three-dimensional laparoscopic instruments were developed to overcome the conventional 2D laparoscopy’s lack of in-depth perception; with the 3-dimensional view, surgeons are able to perceive a true representation of the operative field.
This study evaluated inexperienced doctors’ learning experience on essential laparoscopic box training. Our results show that the 3D group required less time to complete all the tasks; a reduction in time that was statistically significant for four of the seven tasks. This time reduction could be the effect of the 3D instruments, which permit better perception and more depth of view, like open surgeries. This study confirms the results of previous studies, which demonstrated that 3D laparoscopic instruments can improve surgical performance compared to that of 2D instruments.5–8
However, the early study showed no difference between 2D and 3D laparoscopy, and the 3D instruments had the disadvantage of high price and surgeon eye strain and fatigue.9,10 Therefore, while the 3D instruments can improve surgeon’s performance, practice is required to improve hand-eye coordination, become familiar with the instruments, and improve general surgical skills.
Limitations of this study included its small number of participants and potential lack of generalizability. As this study was established in a training box, it may not show the correct impact on real surgery. Future research comparing 2D and 3D laparoscopic surgery in patients undergoing laparoscopy by experienced surgeons or comparing 2D and 3D laparoscopy to modern technology, such as 4K enhancing instruments or robotic surgeries, should be performed.
Conclusion
Three-dimensional laparoscopy are the one factor that may help an inexperienced surgeon improve their learning experience.
Abbreviations
2D, 2-dimensional; 3D, 3-dimensional; 4K, ultra-high-definition display technique.
Data Sharing Statement
Data and materials used in this study are available and can be presented by the corresponding author upon reasonable requests.
Ethics Approval and Consent to Participate
Ethical approval to conduct the research was obtained from Research Facilitation Division, Faculty of Medicine Vajira Hospital, Navamindradhiraj University (IRB/IEC Certification: COA 159/2561). Informed consent was taken from each study population after brief explanation. The research process was carried out under the guidelines outlined in the Declaration of Helsinki.
Acknowledgment
The authors gratefully acknowledge Miss Thanita Akethanin on data entry, Mr. Thawin Techapongsatorn, Mr. Shussana Jungsuwadee on English proofreading, Mr. Nathakorn Techapongsatorn, and Mr. Pohpdham Kasetsermwiriya on picture editing.
Author Contributions
All authors contributed significantly to the work reported, whether in the conception, study design, execution, data acquisition, analysis, and interpretation, or all of these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article was submitted; and agreed to be accountable for all aspects of the work.
Funding
This study was funded from the Faculty of Medicine Vajira Hospital, Navamindradhiraj University.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Vecchio R, MacFayden BV, Palazzo F. History of laparoscopic surgery. Panminerva Med. 2000;42:87–90.
2. McIntyre RC
3. Smith JF, Boysen D, Tschirhart J, Williams T, Vasilenko P. Comparison of laparoscopic cholecystectomy versus elective open cholecystectomy. J Laparoendosc Surg. 1992;2:311–317. doi:10.1089/lps.1992.2.311
4. Kargar S, Mirshamsi MH, Zare M, Arefanian S, Shadman Yazdi E, Aref A. Laparoscopic versus open appendectomy; which method to choose? A prospective randomized comparison. Acta Med Iran. 2011;49:352–356.
5. Zwimpfer TA, Lacher D, Fellmann-Fischer B, Mueller M. A laparoscopic study investigating 3D vs 2D imaging systems using a pelvitrainer model with experts, non-experts, and students. BMC Surg. 2020;20:276. doi:10.1186/s12893-020-00892-8
6. Bracale U, Merola G, Rizzuto A, et al. Does a 3D laparoscopic approach improve surgical outcome of mininvasive right colectomy? A retrospective case-control study. Updates Surg. 2020;72:445–451. doi:10.1007/s13304-020-00755-0
7. Rojano-Rodríguez M, Torres-Ruíz M, Cuendis-Velazquez A, et al. Three-dimensional vs two-dimensional laparoscopic gastric bypass for manual gastrojejunal anastomosis: a prospective and randomized trial. Cir Cir. 2020;88:170–174. doi:10.24875/CIRU.19001064
8. Alaraimi B, El Bakbak W, Sarker S, et al. A randomized prospective study comparing acquisition of laparoscopic skills in three-dimensional (3D) vs. two-dimensional (2D) laparoscopy. World J Surg. 2014;38:2746–2752. doi:10.1007/s00268-014-2674-0
9. McDougall EM, Soble JJ, Wolf JS
10. Hanna GB, Shimi SM, Cuschieri A. Randomised study of influence of two-dimensional versus three-dimensional imaging on performance of laparoscopic cholecystectomy. Lancet. 1998;351:248–251. doi:10.1016/S0140-6736(97)08005-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.