Back to Journals » Patient Preference and Adherence » Volume 17
A Qualitative Study on the Perception of Medication Adherence by the Social Circles of Patients with Type 2 Diabetes
Authors Aloudah NM ![]()
Received 9 January 2023
Accepted for publication 1 April 2023
Published 6 April 2023 Volume 2023:17 Pages 973—982
DOI https://doi.org/10.2147/PPA.S404092
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Nouf M Aloudah
Clinical Pharmacy Department, King Saud University, Riyadh, Saudi Arabia
Correspondence: Nouf M Aloudah, Clinical Pharmacy Department, King Saud University, PO BOX 50351, Riyadh, 11523, Saudi Arabia, Tel +966504410662, Fax +966118052966, Email [email protected]
Introduction: Studies have indicated that half of all patients with diabetes do not take their medication as prescribed. Patient social circles, including professionals (health care providers) and nonprofessionals (family and friends) might contribute to low medication adherence. Therefore, this study explored the point of view of healthcare providers and family members of patients with diabetes on patient medication adherence.
Methods: Our study included health care providers and family members using in-depth, semi structured interviews. The theoretical domain framework (TDF) was used to explore their perspectives. TDF was used to build a topic guide and to frame the data analysis. The interviews were transcribed verbatim and thematically analyzed using the MAXQDA 2022 program.
Results: The participants identified a variety of factors potentially associated with diabetes medication adherence. Most factors were related to the environmental context and resources such as the burden of polypharmacy, medication shortages, and long wait times for care. In addition, factors related to patient beliefs concerning diabetes complications and insulin injections were reported. Several factors were identified that related to knowledge and social influences.
Discussion: Interventions that target the factors identified by the social circle of patients with diabetes might improve medication adherence and promote better disease management outcomes.
Keywords: social support, medication adherence, qualitative analysis, theory, family members, health care providers, type 2 diabetes
Introduction
Type 2 diabetes is a leading cause of morbidity in Saudi Arabia and affects a fourth of the population.1 Studies have shown that half of all patients with type 2 diabetes do not take their medications as prescribed.2 Thus, understanding the factors that affect diabetes medication adherence is vital for identifying barriers to disease management and enabling the design of effective interventions. In 2018, Jaam et al developed a conceptual framework model that used systematic reviews of more than 500 primary studies identified six major themes in patient behavior towards diabetes medication adherence. These themes included: patients, medications, the disease, providers, system, and societal-related factors.3 The model further showed that these themes were correlated. For instance, factors within the societal theme included stigma, social support, culture, and vicarious experience. The vicarious experience was further linked to patient fear. Hence, the same link could be used to reduce patient fear by having them observe others successfully injecting insulin.
In-depth explorations of the factors affecting medication adherence in patients with diabetes have indicated that social circles influence adherence.4,5 Social circles involve professionals, ie health care providers (HCPs) and non-professionals (family and friends).5,6 Positive social support has been shown to improve medication adherence to diabetes treatment,6 and qualitative and quantitative studies have further identified the physician-patient relationship and family support as main factors affecting medication adherence.7–9
In Saudi Arabia, medication adherence in patients with diabetes is low.2 Alodhaib et al interviewed 68 patients with diabetes and identified a number of barriers they organized into six categories: patient-related, medication-related, health-related, provider-related, disease-related, and social-related factors.10 In my previous research,2 I found that diabetes medication adherence was influenced by behavioral regulation, social influences, environmental context and resources, beliefs about consequences of adherence, memory attention, and gaps in knowledge about diabetes. In particular, social influences, including role models, the effect of family support - both positive and negative, and medication sharing were factors mentioned by participants in that study. In addition, family gatherings and having a poor patient-physician relationship affected adherence. However, the effect of physician-patient and family-patient relationships showed mixed results, with the relationships both supporting and sabotaging medication adherence behavior.2 Therefore, exploring the perspectives of diabetic patients’ social circles and analyzing their beliefs could help identify barriers that have not been previously identified. Given that socializing and maintaining good relationships help to shape an individual’s social image, interviewing family members and physicians using qualitatively designed methods could lead to a better understanding of medication adherence and how it can be influenced. Therefore, this study was carried out to understand what physicians and families think about patient medication adherence. To our knowledge, no previous studies have explored the point of view of HCPs and first-degree family members on the factors affecting medication adherence to diabetes treatment.
Materials and Methods
Setting, Sampling and Recruitment
Purposive sampling was used to recruit HCPs and family members of patients diagnosed with type 2 diabetes who were receiving treatment at Medical City of King Saud University. The sampling matrix is shown in Table 1.
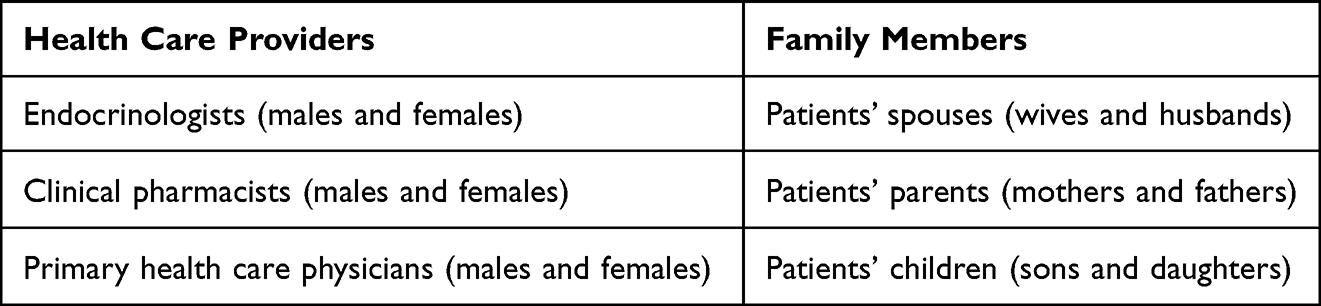 |
Table 1 The Sampling Matrix |
Study Design and Data Collection
In-depth, face-to-face and telephone interviews were carried out between May 2019 and December 2020.
Ethical Approval
The project (No. E-19-4000) was approved by the institutional review board of King Saud University on May 26, 2019 with ref. No. 19/0746/IRB. The study complies with the Declaration of Helsinki and all the participants provided informed consent for participation in the study and the recording and production of anonymized responses.
Interview Guide
The interview guide was created using the Theoretical Domain Framework (TDF) to explore the point of view of HCPs and family members towards diabetes medication adherence.9 Two versions of the interview guide were created: one for HCPs and another for family members. Questions from the TDF were modified to fit the topic and type of interviewee. The interview guide questions for physicians were developed in English and reviewed by two physicians working with patients with diabetes. The family members’ interview guide was developed in English, translated into Arabic by the first author (NA), and then reviewed by two family members of patients with diabetes. Reviews of the interview guides were conducted to help improve the clarity and structure of the questions. Using the TDF questions as a template for the interview guides helped to explore the domains that might contribute to participants’ point of view. However, the TDF questions were only used as a general guide and prompts and questions were used to nudge interviewees when necessary.
Data Analysis
Interview transcripts were transcribed verbatim into English and Arabic and thematically analyzed in their original language using MAXQDA 2022 (VERBI Software).11 The final themes and related quotations were discussed with Renad Alnaheet. The following steps were followed to ensure rigor and trustworthiness in the study: at the end of each interview a summary was prepared and validated by the participant to correct any ambiguity; after each interview, I reflected on the information that was provided and identified the main factors mentioned and compared them with the findings from my previous research with patients, and; memos and journaling were maintained throughout the data collection and analysis stages using the MAXQDA memos feature and online notation software (google keep©).
All interviews were analyzed using the original transcripts. These were in Arabic for family members’ interviews and in English for physician interviews. The results of family members’ interviews were translated by a certified translator into English.
Theory
Using theory to explore behavior has been shown to increase research rigor.12,13 Therefore, TDF was used as a lens to approach the topic of medication adherence. TDF is a composition of 14 domains used to explain health-related behaviors. These domains are knowledge, skills, social identity, beliefs about capabilities, optimism, beliefs about consequences, reinforcement, intentions, goals, memory, resources, social influences, emotions, and behavioral regulation. These domains have been derived from other relevant theories found to be useful in understanding behavior. Furthermore, the TDF includes other theories that have been previously used to understand behavior such as the health belief model, social cognitive theory, and social determination theory, in addition to studies that have included constructs explaining health behaviors. One advantage of the TDF is that it has been simplified by using theories developed by researchers who are not experts in health psychology, which also enables theory implementation.12,13
Results
Seventeen participants completed semi structured interviews: 12 participants were HCPs and the remaining five were family members of patients with diabetes (Table 2). Participants identified a variety of factors potentially associated with diabetes medication adherence. Most were related to the environmental context and resources domain such as the burden of polypharmacy, medication shortages, and long wait times for care. Factors related to patient beliefs about consequences such as diabetes complications and insulin injections were also reported. Additionally, several factors were identified that were related to the knowledge and social influences domains. In the next sections, a presentation of each domain, factors related to the domains, and extracts of participant responses to interview questions are provided.
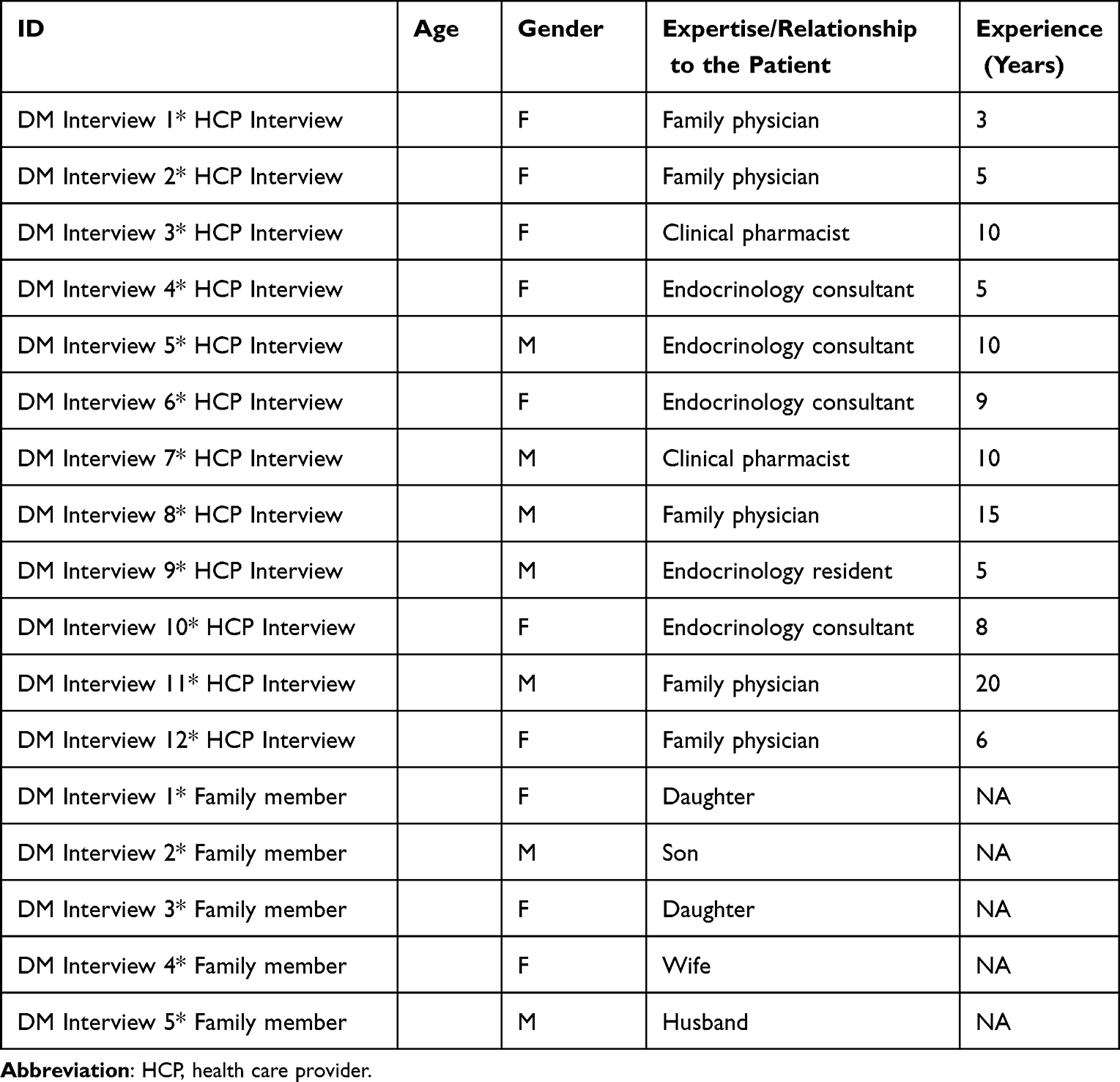 |
Table 2 Participant Characteristics |
Environmental Context and Resources
The Challenge of Multidrug Regimens
Participants shared their perception that patients’ low medication adherence was due to having to take other medications:
The patient does not only have diabetes, he has other problems and takes other medications. If we lessen his medications, he will be more adherent.
[DM Interview 1* HCP Interview]
… a lot of medication … they said ‘I cannot take all the medication at the same time. How many tablets do I have to take per day …’. So it’s very difficult to manage with all this medication. This is the primary thing.
[DM Interview 2* HCP Interview]
Medication Shortage
Participants discussed the effect of unavailable medications and the inability of patients to pay out-of-pocket expenses on medication adherence:
… patients cannot buy [medication], it’s expensive. I mean, they must wait for it to be available. This is another factor…the availability of medications…
[DM Interview 5* HCP Interview]
Long Wait Times for Care
Participants reported that long wait times between appointments contributed to low adherence:
… for example, we have appointments every 8 months for patients, which is wrong. You can’t know anything after 8 months, and this long wait for the patient to make a follow-up appointment, ideally it’s supposed to be 3 months at least, but we can’t do it.
[DM Interview 5* HCP Interview]
Additionally, the interviewees reported that lack of a follow-up system affected adherence:
As I told you, loss of follow up is always responsible for adherence problems.
[DM Interview 4* HCP Interview]
High Workload
Interviewees mentioned that the lack of time affected their ability to discuss adherence issues with patients:
Sometimes we do not have time in the clinic to explain the drug’s mechanism of action. We do not have time in the clinic to give detailed explanations to patients about side effects and their fear of injections. We have educators, but they are also busy.
[DM Interview 1* HCP Interview]
Communication Between HCPs
Participants noted that the gaps in communication between HCPs contributed to lowered adherence:
There is also miscommunication… for example, we are endocrinologists and this patient is also followed up by a nephrologist, then the nephrologist decides to stop one type of diabetic medication and we do not have any communication about it and we must ask the patient why they do not take the medication.
[DM Interview 2* HCP Interview]
Beliefs Concerning Consequences
Avoiding Diabetic Complications
There was an agreement that adherence occurs because it helps avoid diabetes complications:
… and there are people who maintain their health because of fear of complications such as loss of vision … they do not want to be blind and depend on others…
[DM Interview 1* HCP Interview]
Furthermore, interviewees mentioned patients’ fear of insulin injections improving adherence:
… once you introduce the sentence ‘I am going to have insulin injections.’ automatically in the next visit their blood sugar level and readings are better and hemoglobin 1AC drops suddenly! And why? Because they are afraid of the stigma instead of the disease itself!
[DM Interview 4* HCP Interview]
Medication Side Effects
Participants further identified experiencing side effects as a contributing factor that decreased adherence:
… I think because of the pain of Glucophage, she discontinued it, then we told the doctor…
[DM Interview 3* Family member]
Side effects… if they experience it once, that’s it! They try to avoid taking the medications.
[DM Interview 5* HCP Interview]
Knowledge
Education Level
Participants discussed how a patients’ level of education positively affected medication adherence:
Mostly highly educated [patients]… are more compliant about their medication for sure
[DM Interview 3* HCP Interview]
Patients’ Education
There was an agreement concerning the lack of knowledge about the medications that negatively affected adherence:
I think one of the major reasons for non-adherence is that patients are not aware of why they are taking the medications and how to take the medications … the majority of the patients know this drug is for diabetes, but do they know what, exactly, what the drug does?
[DM interview 3* HCP Interview]
Specifically, there was a lack of education about normal blood glucose levels:
… the problem is, they don’t know. They are used to having blood sugar levels of three hundred and, if they measure it once as one hundred, which is normal, they mention that it is hypo and stop the medication!
[DM Interview 2* HCP Interview]
Moreover, participants raised concerns about a of lack of knowledge about diabetes-related nutrition on medication adherence:.
Even my mother has the misconception. She thinks if she commits herself to eating well she won’t need to take the medications! …. Even though the amount of the meal is too much and insulin will rise!
[DM interview 2* Family member]
Furthermore, participants linked low adherence to lack of knowledge concerning when to refill their medication:
We find that if you prescribe medication for six months, the patient goes to the pharmacy, takes medication for three months and does not come again to refill! … they thought they had to wait until their appointment.
[DM Interview 2* HCP Interview]
Participants discussed obstacles facing patient education including a lack of both time and a multidisciplinary approach:
The other factor is the patient’s education. the ideal model in all diabetic clinics is to have a pharmacist next to you, to give the patients some information about each medication, the timing of the medications. so there is a lack of education from our side.
[DM Interview 5* HCP Interview]
Also, I think the problem here is that we do not have a diabetes nurse or team for diabetic patients to discuss what the problem is with them because there is no time for discussion.
[DM Interview 2* HCP Interview]
Another obstacle that participants mentioned related to patients’ knowledge and their poor understanding of the nature of diabetes and that the absence of symptoms does not mean the absence of disease:
[Patients say] ‘I feel okay, why do I have to take medication?’.
[DM Interview 2* HCP Interview]
Mass Media Effect
Participants mentioned the impact of rumors and false news that negatively affected medication adherence:
Of course, there is the media. Our patient received information via WhatsApp that another patient suffered renal failure because of Glucophage. Educated patients come to ask about the solution for this while other patients stop their medication without even coming back to us!
[DM Interview 9* HCP Interview]
Social Influences
Influence of Family Support
There was variability in the effect of family on patient medication adherence. Some support was observed such as between wives and mothers to their husbands and sons. In contrast, a lack of support was apparent in cases of elderly patients coming to clinics alone:
I think men are more likely to adhere to their medications because of their wives and mothers.
[DM Interview 2* HCP Interview]
Unfortunately, … I rarely saw diabetic patients come to the clinic with a family member, unlike with cardiology follow-ups or renal follow-ups, where a family member was always involved
[DM Interview 4* HCP Interview]
The influence of family gatherings on medication adherence was also mentioned, with participants voicing conflicting points of views regarding family gatherings and medication adherence. On the one hand, it was seen as positively affecting adherence as it improved the mood of the patient and helped them adhere to their diet and medication. On the other hand, others believed it sabotaged outcomes:
So. if my sisters come to visit and they bring dessert [diabetes friendly] for her and another dessert for them to eat together… she takes her medication, but if they go. she doesn’t eat her food or take her medications
[DM Interview 1* Family member]
…. I have a patient who is very old and her diabetes reaches 400! Why? She told me, ‘my daughters were with me and I snacked with them’ …I noticed this with my patients, that if there is no family support, the patients take a long time to achieve our goals.
[DM Interview 8* HCP Interview]
Physician- Patient Relationship
Having a supportive physician was also mentioned as facilitating medication adherence:
… When I tell her… ‘Excellent, you did it’, sometimes her blood sugar is high, but I tell her it’s ok, and after a little while they feel they are good and adhere to their meds. This really motivates the patient.
[DM Interview 5* HCP Interview]
In contrast, a weak patient-physician relationship can result in low medication adherence:
… The patient said ‘I will not go to my appointment. I do not like the attitude of the doctor with me’
[DM Interview 1* HCP Interview]
Herbal Use
Participants discussed how the use of herbal medicine caused patients to stop taking their medication:
Some patients come to the clinic and say ‘we use herbal [medicine]’… and they come three months later and we do the lab tests. They say ‘to be honest with you, I never take this medication.’ Why? Because they needed to compare whether the herbs had the same effect as the medication.
[DM Interview 2* HCP Interview]
Discussion
This study examined the point of view of HCPs and family members who are involved with patients with diabetes. Four main themes were identified that affected medication adherence. These were environmental contexts and resource-related factors, beliefs about consequences, knowledge-related factors, and factors related to social influence.
Environmental Context and Resource-Related Factors
The in-depth interviews identified five related factors related to the environmental context and resources. These were the challenges of multidrug regimens, medication shortages, long wait times for care, high HCP workloads, and a lack of communication between HCPs.
Participants raised concerns over polypharmacy and its influence on medication adherence. Although the literature has failed to come to a consensus regarding the predictors of medication adherence,14 polypharmacy was one of the few factors that consistently appeared as an agreed upon predictor across the studies.15 Promoting rational, conservative prescribing, avoiding the “prescribing cascade”, and taking into account the patient’s beliefs about medication use have been suggested as ways to counter the effect of polypharmacy on medication adherence.14,15
Medication shortages were also mentioned as a factor that negatively affected adherence. Unfortunately, this is a growing issue that is known to worsen clinical, economic, and humanistic patient outcomes.16 Although medication shortages are a global problem, there is limited research that has explored its disadvantageous outcomes, including medication adherence.16
In one quantitative study that identified and compared the point of view of more than 1400 HCPs on the factors affecting medication adherence to type 2 diabetes mellitus in Spain found that the complexity of the medication, adverse events, costs, and copayments had the most influence.9 Asking patients to adhere to medication without providing available resources is unreasonable.16 To improve medication adherence, the barriers that hinder patients’ ability to engage in adherence must occur.9 This means ensuring that regimens are simplified and available at the appropriate time and in the needed quantity.17
Beliefs About Consequence-Related Factors
Participants believed patients’ adhered to medication due to a fear of complications and/or taking insulin injections, and if a patient did not feel any symptoms, that meant they did not have the disease and did not need to take medication. Previous studies investigating beliefs that affect medication adherence18 have found negative associations between harm beliefs and medication adherence for chronic illness.19 Therefore, HCPs should explore patients’ beliefs and, if necessary, try to modify them. For example, empowering patients to self-manage their condition by asking them to describe the consequences of not taking their medications and restating the benefits of taking them could help to improve adherence.17 Providing rewards for adherence such as certificates, coupons and/or points programs have also been indicated by change behavior models and suggested by patients themselves and could correct beliefs and motivate patients to adhere to their medications.17
Side effects also appear to play a role in determining patients’ adherence to medication. Both the in-depth interviews in this study, as well as in previous studies18,20 have raised concerns about negative associations with side effects, which have been found to be significant in patients with hypertension20 and schizophrenia,18 but has not yet been studied in patients with diabetes. HCPs need to effectively communicate potential side effects of medications with patients. This communication should also include confirming patients’ complaints, exhibiting empathy, and involving them in the decision-making process.17 HCP communication can be improved by bettering interviewing skills, practicing active listening, and encouraging patient autonomy, all of which should be part of every day clinical practice.5
Knowledge
Participants referred to variable aspects in the knowledge domain and their influence on medication adherence in patients with diabetes. The factors were patient educational levels, gaps in information provided to patients, and the impact of media. Our in-depth interviews showed that patients’ level of education and the information knowledge gap may contribute to medication adherence in diabetes. While studies have encouraged patient autonomy, without proper patient education the results could be negative.21 Moreover, studies have shown that educated patients, who are able to make decisions for themselves, may refuse a physician’s recommendations based on personal views that may not match proper disease management.21 Thus, much more work needs to be done in regard to patient education concerning medication adherence in diabetes. Furthermore, when educating patients, a one-size-fits-all approach does not work; education must be tailored to individual needs and preferences.22 Using multiple modalities and exploring the right tools and information for patients in diabetes education program is lacking and requires further research.21
Social Influence
Participants in this study discussed a number of aspects related to the social influence domain. Research has indicated that positive social support improves medication adherence to diabetes treatment while negative support worsens it.23 Social support by HCPs may include identifying nonadherence, evaluating patients, and providing solutions to patient problems.4 Supportive HCPs can inspire patients to take their medication and, by helping to resolve problems, they can positively effect treatment outcomes.4 Specifically, HCPs can identify early behavioral signs that predict a lack of adherence, help patients understand why and how to take medications, simplify the medication regimen, and resolve financial constraints that hinder adherence.8 Similarly, support from family and friends can also enhance medication adherence. Family members who are knowledgeable about diabetes were associated with more supportive behavior that positively affected medication adherence.6 In contrast, non-supportive behaviors from close family members (such as being not motivated to make lifestyle changes) sabotaged adherence behavior.6 Moreover, a lack of social support (neither positive nor negative) also contributed to diabetes medication nonadherence.8
This study is qualitative and the results are not generalizable; however, the purpose was to identify and explore factors affecting patients with diabetes adherence toward their medications from the perspective of their social circles. Further surveys and studies should be conducted with these factors to generalize the results to a wider population. The interviews conducted in this study identified a number of barriers related to the resources available to patients, with medication shortages and refill issues leading to patients discontinuing their medications. Empowering patients with the support required to be adherent is a task that is overlooked, and patient blaming is common. Systems must be built that ensure patients can obtain their medications and obstacles are effectively resolved. Patient autonomy should also be undertaken in line with proper patient education that is tailored to the individual’s preferences. Furthermore, a strong physician-patient relationship is needed to counteract inaccurate media effects. Family involvement in education also appears to be lacking. Empowering families to help fight diabetes with the patients can further the benefits of educating the patient. In conclusion, improving medication adherence in patients with diabetes in Saudi Arabia requires multidimensional interventions that need validation and further research.
Acknowledgments
The author would like to thank Renad Alnaheet for reviewing the themes and quotations. The author is also grateful to Noura Aldosari and Hend Almalki for participation in reviewing the interview transcriptions.
Disclosure
The author reports no conflicts of interest in this work.
References
1. International Diabetes Federation. IDF Middle East and North Africa MENA; 2022; Available from: https://refworks.proquest.com/library/615be7b68f0832c826bd625f/?eml=activation.
2. Aloudah NM, Scott NW, Aljadhey HS, Araujo-Soares V, Alrubeaan KA, Watson MC. Medication adherence among patients with Type 2 diabetes: a mixed methods study. PLoS One. 2018;13(12):e0207583. doi:10.1371/journal.pone.0207583
3. Jaam M, Awaisu A, Mohamed Ibrahim MI, Kheir N. A holistic conceptual framework model to describe medication adherence in and guide interventions in diabetes mellitus. Res Social Adm Pharm. 2018;14(4):391–397. PMID: 28533079. doi:10.1016/j.sapharm.2017.05.003
4. Shahin W, Kennedy GA, Stupans I. The association between social support and medication adherence in patients with hypertension: a systematic review. Pharm Pract. 2021;19(2):2300.
5. Zolnierek KBH, Dimatteo MR. Physician communication and patient adherence to treatment: a meta-analysis. Med Care. 2009;47(8):826–834. doi:10.1097/MLR.0b013e31819a5acc
6. Mayberry LS, Osborn CY. Family support, medication adherence, and glycemic control among adults with type 2 diabetes. Diabetes Care. 2012;35(6):1239–1245. doi:10.2337/dc11-2103
7. Balkrishnan R. The importance of medication adherence in improving chronic-disease related outcomes: what we know and what we need to further know. Med Care. 2005;43(6):517–520. doi:10.1097/01.mlr.0000166617.68751.5f
8. Bussell JK, Cha E, Grant YE, Schwartz DD, Young LA. Ways Health care providers can promote better medication adherence. Clin Diabetes. 2017;35(3):171–177. doi:10.2337/cd016-0029
9. Labrador Barba E, Rodríguez de Miguel M, Hernández-Mijares A, et al. Medication adherence and persistence in type 2 diabetes mellitus: perspectives of patients, physicians and pharmacists on the Spanish health care system. Patient Prefer Adherence. 2017;11:707–718. doi:10.2147/PPA.S122556
10. Alodhaib G, Alhusaynan I, Mirza A, Almogbel Y. Qualitative exploration of barriers to medication adherence among patients with uncontrolled diabetes in Saudi Arabia. Pharmacy. 2021;9(1):16. PMID: 33440884; PMCID: PMC7838809. doi:10.3390/pharmacy9010016
11. MAXQDA. Software for qualitative and mixed methods research. Available from: https://www.maxqda.com/what-is-maxqda.
12. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
13. Lawton R, Heyhoe J, Louch G, et al. Using the Theoretical Domains Framework (TDF) to understand adherence to multiple evidence-based indicators in primary care: a qualitative study. Implement Sci. 2016;11:1.
14. Marcum ZA, Gellad WF. Medication adherence to multidrug regimens. Clin Geriatr Med. 2012;28(2):287–300. doi:10.1016/j.cger.2012.01.008
15. Omran D, Guirguis LM, Simpson SH. Systematic review of pharmacist interventions to improve adherence to oral antidiabetic medications in people with type 2 diabetes. Can J Diabetes. 2012;36(5):292–299. doi:10.1016/j.jcjd.2012.07.002
16. Phuong JM, Penm J, Chaar B, Oldfield LD, Moles R. The impacts of medication shortages on patient outcomes: a scoping review. PLoS One. 2019;14(5):e0215837. doi:10.1371/journal.pone.0215837
17. American College of Preventive Medicine. Medication adherence – improving health outcomes; 2011. Available from: https://cdn.ymaws.com/acpm.site-ym.com/resource/resmgr/timetools-files/adherenceclinicalreference.pdf.
18. Dibonaventura M, Gabriel S, Dupclay L, Gupta S, Kim E. A patient perspective of the impact of medication side effects on adherence: results of a cross-sectional nationwide survey of patients with schizophrenia. BMC Psychiatry. 2012;12:20. doi:10.1186/1471-244X-12-20
19. Shahin W, Kennedy GA, Stupans I. The consequences of general medication beliefs measured by the beliefs about medicine questionnaire on medication adherence: a systematic review. Pharmacy. 2020;8(3):147. doi:10.3390/pharmacy8030147
20. Tedla YG, Bautista LE. Drug side effect symptoms and adherence to antihypertensive medication. Am J Hypertens. 2016;29(6):772–779. doi:10.1093/ajh/hpv185
21. Jotterand F, Amodio A, Elger BS. Patient education as empowerment and self-rebiasing. Med Health Care Philos. 2016;19(4):553–561. doi:10.1007/s11019-016-9702-9
22. Lin GA. Patient education: one size does not fit all. JAMA Intern Med. 2013;173(14):1376. doi:10.1001/jamainternmed.2013.7402
23. Grant RW, Schmittdiel JA. Adults with diabetes who perceive family members’ behaviour as unsupportive are less adherent to their medication regimen. Evid Based Nurs. 2013;16(1):15–16. doi:10.1136/eb-2012-100947
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Association Between Medication Adherence, Internalized Stigma and Social Support Among Outpatients with Major Depressive Disorder in a Malaysian Hospital: A Cross-Sectional Study
Halim R, Kaur M, Syed Mokhtar SS, Chemi N, Sajatovic M, Tan YK, Siau CS, Ng CG
Psychology Research and Behavior Management 2025, 18:209-223
Published Date: 4 February 2025
Psychosocial and Clinical Factors That Differentiate and Predict Patients’ Adaptation to Chronic Diseases
Laza R, Al Ghazi L, Lustrea A, Lazureanu VE, Oancea CI, Luput-Andrica IM, Poplicean EI, Ilina R, Cireap N, Bob F, Olariu N, Ionita I, Lazar S, Dehelean L, Romosan RS, Romosan AM
Patient Preference and Adherence 2025, 19:1539-1556
Published Date: 24 May 2025
Exploring the Factors Related to Medication Adherence in Patients with Rheumatoid Arthritis Based on Social Cognitive Theory: A Path Analysis
Liang L, Zhang X, Pan Y, Huang L, Jia L, Xu P, Li K
Patient Preference and Adherence 2025, 19:2565-2575
Published Date: 20 August 2025
Social Support and Hospital Discharge Readiness in CHD Patients: Mediating Roles of Self-Efficacy and Adherence
Wang D, Yang N, Wei C, Wang J, Yuan L, Sun R
Patient Preference and Adherence 2026, 20:601646
Published Date: 4 June 2026