Back to Journals » Patient Preference and Adherence » Volume 17
A Qualitative Exploration of Perceived Medication Adherence Determinants Conducted Among Older Adults with HIV and Type 2 Diabetes Mellitus
Authors Pack AP ![]() , Masters MC, O'Conor R, Alcantara K, Svoboda S, Smith R
, Masters MC, O'Conor R, Alcantara K, Svoboda S, Smith R ![]() , Yeh F, Wismer G
, Yeh F, Wismer G ![]() , Wallia A, Bailey SC
, Wallia A, Bailey SC
Received 22 July 2023
Accepted for publication 10 October 2023
Published 31 October 2023 Volume 2023:17 Pages 2667—2678
DOI https://doi.org/10.2147/PPA.S431869
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Allison P Pack,1 Mary Clare Masters,2 Rachel O’Conor,1 Kenya Alcantara,1 Sophia Svoboda,1 Reneaki Smith,1 Fangyu Yeh,1 Guisselle Wismer,1 Amisha Wallia,2,3 Stacy C Bailey1
1Division of General Internal Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA; 2Department of Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA; 3Institute for Public Health and Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA
Correspondence: Allison P Pack, Division of General Internal Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA, Email [email protected]
Background: People living with HIV (PLWH) are at higher risk of developing type 2 diabetes (T2DM). Both chronic conditions require individuals to adhere to medication regimens, yet few studies have sought to explore medication-taking behaviors among individuals with comorbid HIV and T2DM (HIV+T2DM).
Objective: This qualitative study sought to: 1) identify and compare perceived determinants of medication adherence for HIV and, separately, for T2DM, and 2) explore how participants prioritize conditions.
Methods: Between October 2022 and January 2023, we conducted in-depth interviews with individuals aged 50 or older, living with comorbid HIV+T2DM. Participants were prescribed oral medications to treat their conditions and had recent clinical measures indicating probable challenges with medication adherence. Interviews with consented participants from a large academic health center in the Midwest were conducted remotely. Questions largely drew from the Theoretical Domains Framework (TDF), a widely used implementation science framework. Additional questions explored the prioritization of conditions. Analysis employed the Framework Method and a side-by-side comparison of key determinants of medication adherence by condition.
Results: A total of 19 interviews were audio recorded, transcribed, and analyzed. Participants were an average age of 61, mostly male (89.5%), and Non-Hispanic White (47.4%). Although results revealed many commonalities between perceived determinants of medication adherence for HIV and for T2DM, differences relating to two TDF domains were noted: nature of the behavior (taking medications as prescribed), and motivations and goals. Many participants viewed their conditions as equally important, though they suggested T2DM was more difficult to manage, largely due to lifestyle modifications.
Conclusion: As individuals with HIV develop chronic conditions, such as T2DM, they may require additional medication adherence support. Attention should be paid to offering support early. Disease perceptions may differ by condition, and as such, one’s motivations to take medication as prescribed may also differ by condition.
Keywords: qualitative, HIV, type 2 diabetes, medication adherence
Introduction
Four decades into the HIV epidemic, treatment regimens have vastly improved and increased life expectancies for people living with HIV (PLWH).1 Due to the natural aging process and factors related to HIV and antiviral treatment itself, PLWH are now living longer and are more likely to develop comorbid conditions over their lifetime, including type 2 diabetes (T2DM). National data show that the incidence of T2DM among PLWH is four times higher than among the general population.2 Compared with the general population, adults with comorbid HIV and T2DM (HIV+T2DM) are also more likely to experience worse outcomes, including chronic kidney disease, cognitive impairment, and mortality.3–5
For those living with HIV and/or T2DM, medication adherence is a critical component of chronic disease management.6–13 A large body of literature has elucidated individual-level challenges to safe and consistent medication use, revealing inadequate adherence is associated with suboptimal treatment, adverse drug events, and poor quality of life.14,15 Nevertheless, research has overwhelmingly focused on single treatments and/or conditions instead of considering the often-complex treatment regimens that are prescribed for individuals with comorbid conditions, including HIV+T2DM.11 This siloed approach limits our understanding of medication adherence and how individuals manage and prioritize co-occurring chronic conditions. Understanding the unique factors that impact medication taking behaviors for HIV and T2DM, together and separately, is essential to informing future interventions that promote chronic disease self-management among the growing population of individuals with HIV+T2DM.
To address this research gap, we conducted a qualitative study among older adults living with HIV+T2DM whose recent clinical measures indicated probable poor medication adherence. Our study aimed to: 1) identify and compare perceived determinants (barriers and facilitators) of medication taking for HIV and T2DM, considering these conditions both separately and together, and 2) explore how adults with HIV+T2DM prioritize and manage each condition.
Methods
We conducted a cross-sectional, qualitative study guided by the Theoretical Domains Framework (TDF). The TDF is an implementation science framework used to facilitate the development and implementation of healthcare practices.16,17 The original TDF includes 12 multi-level constructs designed to capture determinants of current or future successful intervention implementation strategies.17 These include, among others, skills and beliefs about capabilities, social influences, and environmental context and resources. While initially designed to examine determinants of evidence-based practices at the clinician or health system level, the application of the TDF at the individual or patient level, including for medication adherence, is increasingly common.18,19
All research activities were approved by the Northwestern University Institutional Review Board and complied with the Declaration of Helsinki.
Study Participants
To be eligible for this study, participants had to be: 1) English-speaking, 2) aged 50 or older, 3) diagnosed with HIV and T2DM, 4) taking oral medications to treat their HIV and diabetes, 5) receiving care at any practice affiliated with the participating health center, and 6) elevated clinical values within the past 12 months: HIV RNA >50 copies/mL and/or hemoglobin A1c (HbA1c) ≥7.5%, an indication of probable poor medication adherence. Exclusion criteria included having any severe, uncorrectable vision or hearing challenges, as well as any cognitive impairment that would prohibit informed consent.
Recruitment
Potentially eligible participants were identified through a query of an electronic health record (EHR) data warehouse at a large academic medical center in the Midwest. Research coordinators (RCs), trained in qualitative research, contacted identified individuals by phone to confirm eligibility. Informed consent, via electronic signatures, was subsequently obtained prior to conducting the interview; this included consent for the publication of de-identified responses.
Data Collection
One-time, semi-structured, interviews were conducted between October 2022, and January 2023. Interviews were conducted remotely over secure web conferencing software by RCs and were audio-recorded; these lasted approximately 60 minutes. Interview guides were informed by the TDF with questions pertaining to domains in accordance with published guidelines.16 Questions sought to identify determinants of medication adherence separately for HIV and for T2DM and to explore how participants prioritized conditions. Participants also completed a brief demographic questionnaire as well as validated measures of health literacy and patient activation. Health literacy was measured using a three-item screener,20 while patient activation was measured using the 10-item Consumer Health Activation Index.21 Participants were compensated $75 for their time. All quantitative responses were captured in REDCap. RCs took detailed field notes; audio files were professionally transcribed.
Analysis
To analyze qualitative data, we employed a multi-step process for the Framework Method, a largely deductive approach to content analysis of qualitative data.22 We began by reading transcripts for familiarity; we also wrote content memos. We then created codebooks of a priori codes derived from the original TDF and emergent codes derived from the transcripts.17 Using NVivo qualitative software, we piloted the codebook on an initial set of four transcripts. These were coded by three separate coders using simultaneous coding, with all coding reconciled and the codebook modified. The remaining transcripts were independently coded, and analysts held regular meetings to review coding and to iteratively discuss emergent themes.23 Excel matrices were subsequently used for data reduction purposes with individual participants represented in rows and individual codes represented in columns; this approach allowed for the further examination of determinants, as well as the display of illustrative quotes.23 Summaries across participants revealed key themes.
In keeping with published guidance, only themes pertaining to relevant TDF domains are presented.16 Relevant domains were those identified by the study team as having the following criteria:
(1) relatively high frequency of specific beliefs and/or themes; (2) presence of conflicting beliefs; and (3) evidence of strong beliefs that may affect the target behavior.16
This process was implemented separately for TDF domains pertaining to medication adherence for HIV and for T2DM. Analysts then compared findings across conditions using a side-by-side table Simple, descriptive statistics were calculated using SAS software (version 9.4, Cary, NC) to describe sample demographic and psychosocial characteristics.
Results
Study Sample
We analyzed data from a total of 19 participants, a sample size sufficient to achieve saturation of qualitative themes.24,25 Sample demographics are presented in Table 1. In brief, participants had an average age of 61. They were mostly male (89.5%), and identified as lesbian or gay (83.3%), non-Hispanic (84.2%), and White (47.4%). The majority (84.2%) had at least one HbA1c greater than or equal to 7.5% in the past year, while about a third (31.6%) had at least one viral load (VL) of 50 copies/mL or greater in the same timeframe. Some participants had a bachelor’s degree (31.6%) and were employed (42.1%). Most had adequate health literacy (89.5%), and about half had low patient activation (47.4%).
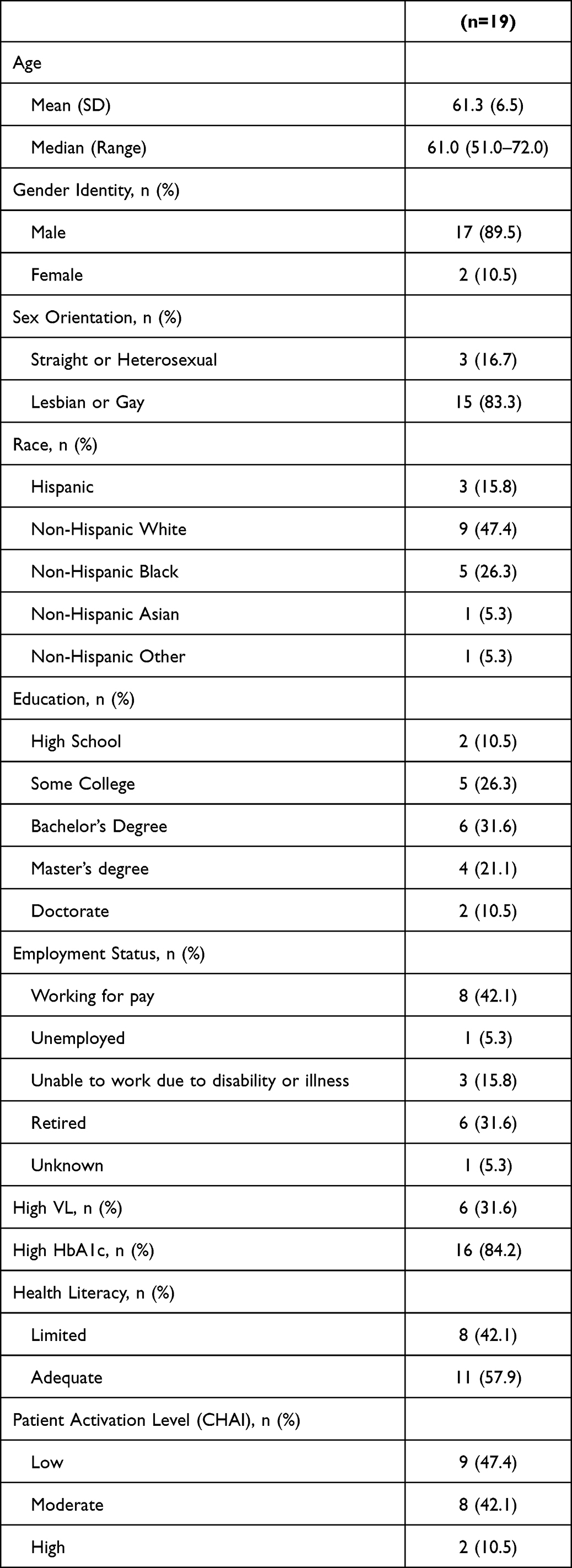 |
Table 1 Participants Demographics |
Thematic Findings
In Table 2, we list the TDF domains we examined alongside sample questions. Results from our analysis identified the following relevant TDF domains for medication adherence related to either chronic condition: 1) beliefs about capabilities, 2) beliefs about consequences, 3) memory, attention, and decision processes, 4) social influences, 5) emotion, 6) nature of the behavior and 7) motivation and goals. Table 3 presents a side-by-side listing of these domains and the determinants (barriers and facilitators) they revealed for each condition; illustrative quotes are also provided. Below, we describe similarities and differences for perceived determinants of HIV and T2DM medication adherence by relevant domain. We subsequently report perceived priorities between conditions.
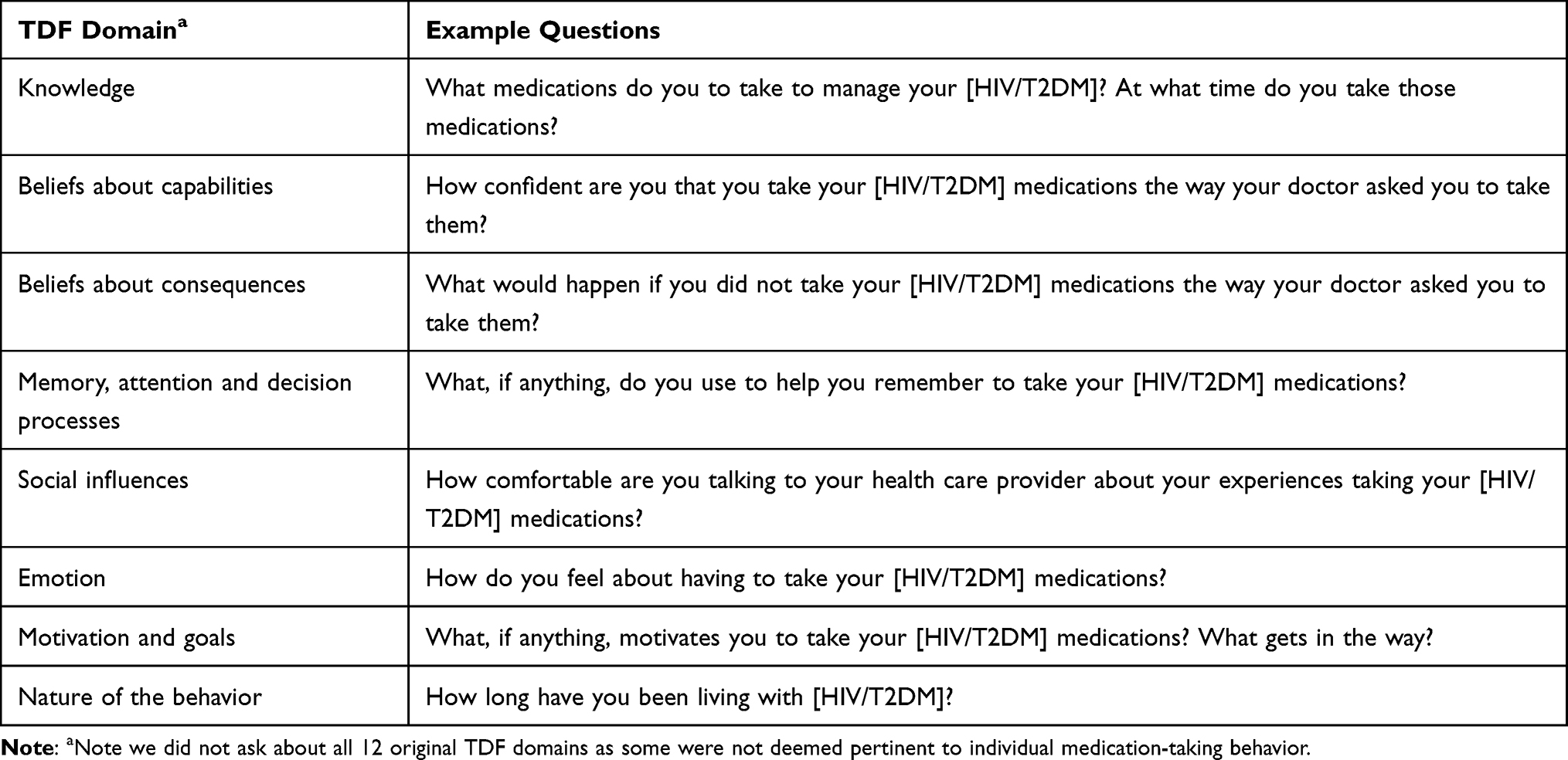 |
Table 2 Example Interview Questions by TDF Domain |
 |
Table 3 Illustrative Quotes by TDF Domains and Condition |
Most Perceived Determinants of Medication Adherence for HIV and T2DM are Similar
Beliefs About Capabilities for Medication Adherence
All participants reported feeling confident in their abilities to take their HIV medications as prescribed; most often, they attributed their confidence to established routines and supportive care teams. Similar findings were reported for T2DM, with nearly all participants revealing they also felt confident in their abilities to take their T2DM medications as prescribed. However, while some suggested their confidence hinged on established routines, many described their confidence in relation to lifestyle modifications, indicating that they felt more confident in their abilities to take T2DM medications than to follow diet and exercise regimens.
Beliefs About Consequences of Non-Adherence
For both conditions, nearly all participants viewed the consequence of non-adherence as poor health outcomes. Most participants reported that non-adherence to HIV medications could lead to increased viral loads, drug resistance and/or susceptibility to other health conditions. Several revealed their perspectives were rooted in their own past experiences with non-adherence. Participants similarly indicated that non-adherence to T2DM medications would negatively affect their glucose or HbA1c levels, leaving them feeling unwell or leading to an eventual insulin prescription. Many participants also acknowledged the potential for diabetes-related complications such as amputations, vision loss, poor kidney functioning, and neuropathy.
For both conditions, many participants also reported a variety of ways in which non-adherence might impact relationships with their health care providers. Of these, the majority believed that if they did not take their medications as prescribed, their providers would likely express disappointment with them, though some commented that their providers would also be quick to help resolve challenges.
Social Influences on Medication Adherence
Nearly all participants reported feeling comfortable with their health care providers. They noted specifically that they feel comfortable talking to health care providers about medication adherence – for either HIV or T2DM. For many, an established rapport, developed slowly over time, was thought to contribute to this sense of comfort.
Emotions Provoked by Having to Take Medications
Whether discussing HIV or T2DM medication adherence, participants reported a variety of emotions. For many, medication taking was just something they did, and the behavior did not invoke any specific emotions. However, for a slight majority, there were positive feelings of gratitude and reassurance. In taking their medications, they felt they were “doing what they’re supposed to be doing” to take care of their health. Fewer participants revealed negative emotions such as shame, disappointment, or frustration with having to take their medications. Those who did, largely noted that these emotions were present at diagnosis but have dissipated in the time since; medication taking is no longer a negative reminder of their condition(s) and they no longer feel “overwhelmed” by their treatments. Only two participants insisted that, regardless of the reason or condition, they disliked having to take medications.
Memory, Attention, and Decision Processes Related to Medication Adherence
The use of resources such as pill boxes and alarms were mentioned by more than half of all participants as being useful reminders, helping them to take their medications for both conditions. These resources were described as particularly helpful for organizing medications and for facilitating medication taking consistently as prescribed.
Several participants separately described apps that facilitate both medication taking and lifestyle management for T2DM. A few others noted that the act of taking their HIV medication, subsequently reminds them to take their T2DM medications.
The Nature of the Behavior and Motivations Differed by Condition
Nature of the Behavior [Taking Medications as Prescribed]
Differences were noted in the length of time participants reported following their current HIV regimens compared to their T2DM regimens. For HIV, most reported they have followed the same regimen of one or two pills for six or more years. During that time, the behavior formed part of their daily routines. Just over half of the participants mentioned taking more than one medication for their HIV; only one mentioned needing to take HIV medication multiple times a day. Nevertheless, participants also acknowledged missed doses, though their reasons varied widely. Sudden changes to routines, including weekend trips or nights out, were most often mentioned. A few participants each also explained that missed doses can occur if they encounter problems with pharmacy refills, stressful life events, depression, fatigue, or unwelcome side effects. Of the few who reported having no conflicts, all had low VL levels.
In contrast to the length of time participants reported following their current HIV regimens, a majority reported following their T2DM regimens for five years or less. Nearly all participants reported taking more than one T2DM medication; just over half reported needing to take T2DM medications multiple times a day. Furthermore, while occasional missed doses were also noted for T2DM medications, most often participants attributed this to an initial adjustment period, with fewer participants suggesting persistent challenges. Challenges mentioned included adjustment to complex regimens, often requiring multiple dosages per day, and the onset of new side effects. Of note, among the several participants who reported no conflicts taking their T2DM medications, all had high HbA1c levels.
Motivation and Goals for Medication Adherence
Most participants revealed that a desire to maintain health motivates them to adhere to their medications, though differences were noted by condition. When asked about motivations for HIV medication adherence, some participants explained they were motivated by important people in their lives, including family, friends, partners, and health care providers. Some specified they would like to be present for significant life events of loved ones, while others noted a desire to prevent HIV transmission to partners.
In contrast, when asked what motivates adherence to T2DM medications, some participants described a desire to avoid diabetes-related complications, as well as a desire to reduce or avoid additional medications. A fear of potential amputations, loss of eyesight, and the need to self-administer insulin shots, were all specifically noted.
Managing Both Conditions is Possible and Important, Though T2DM is More Difficult
Most participants reported that managing HIV+T2DM together is something they have accepted and something they feel capable of doing. Some attributed these beliefs to the fact that they could see or feel the benefits of their regimens.
… Well, I can’t say I’m jumping for joy…but I am in full acceptance of both of them [HIV and T2DM]. My life is better when I manage my diseases better – without question – and that is always something that sticks with me. (PID 30, high HbA1c)
In other instances, participants noted how managing their comorbid conditions had become “second nature” to them, a “routine” part of their lives that keeps them feeling well:
By now, I’m used to [it]… It becomes a second nature. If I feel good, I go, ‘Well, it’s because I’m taking my medications correctly. (PID 14, high HbA1c)
When asked how they prioritize their conditions, half of all participants reported that they perceived HIV and T2DM as equally important; managing both conditions, they explained, helped with their goals of maintaining health and avoiding complications. Nevertheless, there were some participants who viewed one condition or the other as the most important to them, largely due to worry about potential complications or immediate health effects. Of those, an equal number of participants viewed either HIV or T2DM as the most important to them.
With HIV, I’m undetectable. I know it may be doing some damage to my body, but it’s not affecting my health as much as the diabetes is. (PID 29, high HbA1c)
When asked which condition was most difficult to manage, most participants revealed that T2DM was most difficult for them, either because of necessary lifestyle modifications or regimen complexity.
…I basically think there are more— I’m taking four [T2DM] medications. As I said, insulin is one of them, and it’s three times a day… HIV is one pill and I’m done. (PID 32, high HbA1c)
As described by this participant, management of T2DM often required more complex regimens than HIV.
Discussion
In this theory-informed qualitative study conducted among older adults living with HIV+ T2DM, we identified and compared perceived determinants of medication adherence. We also examined how participants prioritized their conditions. Despite the fact that our sample was largely comprised of White males, results from our study are similar to those presented in recent systematic reviews, including one comparing self-management strategies for HIV+T2DM among Black women,10 and another identifying strategies to enhance medication adherence, generally, among older adults.26
Participants in our study reported feeling confident in their abilities to adhere to their medications, explaining that medication taking has formed part of their daily routines. However, it is important to note that all participants also had some clinical indication of potential adherence challenges. Moreover, several participants reported having no conflicts taking their T2DM medications, and yet they had high HbA1c levels. There are a few potential reasons for this. One is potential cognitive difficulties. It may be that those who are having trouble remembering to take their medications are also having trouble remembering to report their adherence challenges. Another potential reason is challenges with lifestyle modifications. It may be that individuals are taking their medications as prescribed, though their diets comprise foods high in glycemic index, or they have challenges exercising and maintaining optimal lifestyles. Nevertheless, results from our study suggest self-reported confidence, alone, or perceptions of one’s own behavior may not be sufficient facilitators of medication adherence.
Participants also identified general and disease specific consequences of non-adherence. And while some revealed that medication taking invoked no real emotion for them, a slight majority reported that taking their medications as prescribed invoked positive emotions about self-management. These determinants could be used to inform gain and loss-framed educational messages, both of which have been found to successfully modify health behaviors among individuals living with chronic conditions.27
Most participants in our study also acknowledged using a variety of resources such as pill boxes and alarms to facilitate medication adherence, regardless of the condition; some also noted that the act of taking their HIV medications subsequently reminded them to take their T2DM medications. These facilitators are important, as results from numerous studies have supported the effectiveness of pill boxes,28 and intervention studies have demonstrated that text messaging reminders can improve medication adherence, including among older adults living with HIV.29,30 Qualitative studies among older adults with HIV and other chronic conditions have additionally identified that taking medication for an index condition (such as HIV) can serve as a reminder to take medications for other, additional, chronic conditions.31
However, our study also demonstrated important differences in determinants of medication adherence for HIV and T2DM. These largely hinged on two TDF domains: 1) nature of the behavior and 2) motivation and goals. Most participants reported a longer duration of time following their HIV medication regimens compared to their T2DM medication regimens; this likely impacts their abilities to establish effective medication taking routines for their T2DM medications. Furthermore, many participants suggested either that their T2DM regimens are more complex than their HIV regimens, or that the side effects are more difficult to manage. Clinicians may need to provide additional early support to aging individuals who are not only increasing the number of medications they take, but also the complexity of their regimens. This is particularly the case for T2DM, as the progressive nature of the condition means treatment regimens are likely to change with time.
While participants generally recognized health maintenance as a motivator for medication adherence, they also revealed disease-specific motivators. For HIV medication adherence, some participants explained they were motivated by important people in their lives to take their medication and maintain health. For T2DM, however, participants largely reported being motivated to avoid having to take additional medications or endure potential complications. Motivational interviewing within the context of clinical care could tease out these differences and facilitate enhanced medication adherence among older adults with multiple chronic conditions, including during early adjustment periods following a new diagnosis.32,33
Our study also explored how participants prioritized their conditions. Results revealed HIV and T2DM were perceived by many to be of equal importance. However, most participants perceived T2DM to be more difficult to manage, explaining that lifestyle modifications and complex medication regimens are challenging. This was likely reflective of the higher prevalence of HbA1c levels >7.5% in our study sample. Nevertheless, limited studies have examined these perceptions and results could inform intervention studies to support self-management and medication adherence among individuals with multiple conditions.
This study is not without limitations. We conducted a qualitative, cross-sectional study; as such, our results are not generalizable. Furthermore, despite our recruitment efforts, our study sample lacked the racial and ethnic diversity reflected in the HIV epidemic in the United States. That said, the study sample is reflective of the patient population at the large, participating academic health center. Finally, we should note that while all participants in our study had some clinical indication of medication adherence challenges in the past year, most were high HbA1c measures as opposed to high VL levels. This, too, is reflective of the patient population at the participating health center.
Conclusions
As individuals living with HIV age, they are likely to develop other chronic health conditions; we can no longer consider HIV in a silo.34 Some health conditions, such as T2DM, may be more complex or difficult to manage in comparison to HIV. Additional support for self-management may be required; this includes the need to provide early adherence support for new medications. Furthermore, while many determinants of medication adherence for T2DM may be similar to those for HIV, health care providers should explore the possibility that motivations to take medications may differ by condition. Understanding these differences can lead to more effective support strategies.
Funding
This work was supported by funding from the Chicago Center for Diabetes Translation Research, (NIDDK P30 DK092949), Deans’ offices of the Biological Sciences Division of the University of Chicago and Feinberg School of Medicine at Northwestern University. The work was also funded in part, by the National Institutes of Health’s National Institute on Aging, Grant Number P30AG059988. REDCap software is supported by the National Institutes of Health’s National Center for Advancing Translational Sciences, Grant Number UL1TR001422. The opinions expressed in this paper are those of the authors and do not necessarily represent National Institutes of Health.
Disclosure
APP reports grants from Merck, Pfizer, Gordon and Betty Moore Foundation, RRF Foundation for Aging, Lundbeck, Gilead, and Eli Lilly through her institution; and personal fees from Gilead. SCB reports grants from the NIH, Merck, Pfizer, Gordon and Betty Moore Foundation, RRF Foundation for Aging, Lundbeck, Gilead and Eli Lilly through her institution; and personal fees from Gilead, Sanofi, Pfizer, University of Westminster, Lundbeck, and Luto outside the submitted work. MCM reports grants from the NIH and Merck through her institution. AW reports grants from NovoNordisk through her institution, and research salary support from UnitedHealth Group. FY reports grants from NIH, Merck, Pfizer, Gordon and Betty Moore Foundation, RRF Foundation for Aging, Lundbeck, Gilead, and Eli Lilly, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. The Centers for Disease Control and Prevention (CDC). HIV and Older Americans; 2021. Available from: https://www.cdc.gov/hiv/group/age/olderamericans/index.html.
2. Brown TT, Cole SR, Li X, et al. Antiretroviral therapy and the prevalence and incidence of diabetes mellitus in the multicenter AIDS cohort study. Arch Intern Med. 2005;165(10):1179–1184. doi:10.1001/archinte.165.10.1179
3. Medapalli RK, Parikh CR, Gordon K, et al. Comorbid diabetes and the risk of progressive chronic kidney disease in HIV-infected adults: data from the veterans aging cohort study. J Acquir Immune Defic Syndr. 2012;60(4):393–399. doi:10.1097/QAI.0b013e31825b70d9
4. Park J, Zuñiga JA, García AA. Diabetes negatively impacts the ten-year survival rates of people living with HIV. Int J STD AIDS. 2019;30(10):991–998. doi:10.1177/0956462419857005
5. Dufouil C, Richert L, Thiébaut R, et al. Diabetes and cognitive decline in a French cohort of patients infected with HIV-1. Neurology. 2015;85(12):1065–1073.
6. Rivera-Picón C, Benavente-Cuesta M, Quevedo-Aguado M, et al. Factors associated with adherence to treatment in patients with HIV and diabetes mellitus. J Pers Med. 2023;13(2):269. doi:10.3390/jpm13020269
7. Monroe AK, Rowe TL, Moore RD, et al. Medication adherence in HIV-positive patients with diabetes or hypertension: a focus group study. BMC Health Serv Res. 2013;13:488. doi:10.1186/1472-6963-13-488
8. Miller MJ, Eberhart LG, Jefferson CR, et al. Beyond antiretroviral treatment: patterns and factors associated with composite medication adherence before and during the COVID-19 pandemic in patients with HIV with multiple chronic conditions. J Acquir Immune Defic Syndr. 2023;92(5):405–413.
9. Ohueri CW, García AA, Zuñiga JA. Counting, coping, and navigating the flux: a focused ethnographic study of HIV and diabetes self-management. Qual Health Res. 2022;32(3):399–412. doi:10.1177/10497323211064231
10. Zuniga JA, Wright C, Fordyce J, et al. Self-management of HIV and diabetes in African American women: a systematic review of qualitative literature. Diabetes Educ. 2018;44(5):419–434. doi:10.1177/0145721718794879
11. Yang Z, Zhu Z, Lizarondo L, et al. Experience of chronic noncommunicable disease in people living with HIV: a systematic review and meta-aggregation of qualitative studies. BMC Public Health. 2021;21(1):1651. doi:10.1186/s12889-021-11698-5
12. Altice F, Evuarherhe O, Shina S, et al. Adherence to HIV treatment regimens: systematic literature review and meta-analysis. Patient Prefer Adherence. 2019;13:475–490. doi:10.2147/PPA.S192735
13. Hamilton JE, Blanco E, Selek S, et al. Patient and provider perspectives on medication non-adherence among patients with depression and/or diabetes in diverse community settings - a qualitative analysis. Patient Prefer Adherence. 2022;16:1581–1594. doi:10.2147/PPA.S328785
14. Sarkar U, López A, Maselli JH, et al. Adverse drug events in U.S. adult ambulatory medical care. Health Serv Res. 2011;46(5):1517–1533. doi:10.1111/j.1475-6773.2011.01269.x
15. Makovski TT, Schmitz S, Zeegers MP, et al. Multimorbidity and quality of life: systematic literature review and meta-analysis. Ageing Res Rev. 2019;53:100903. doi:10.1016/j.arr.2019.04.005
16. Atkins L, Francis J, Islam R, et al. A guide to using the theoretical domains framework of behaviour change to investigate implementation problems. Implement Sci. 2017;12(1):77. doi:10.1186/s13012-017-0605-9
17. Michie S, Johnston M, Abraham C, et al. Making psychological theory useful for implementing evidence based practice: a consensus approach. Qual Saf Health Care. 2005;14(1):26–33. doi:10.1136/qshc.2004.011155
18. Lynch T, Ryan C, Cadogan CA. ‘I just thought that it was such an impossible thing’: a qualitative study of barriers and facilitators to discontinuing long-term use of benzodiazepine receptor agonists using the Theoretical Domains Framework. Health Expect. 2022;25(1):355–365. doi:10.1111/hex.13392
19. Patton DE, Cadogan CA, Ryan C, et al. Improving adherence to multiple medications in older people in primary care: selecting intervention components to address patient-reported barriers and facilitators. Health Expect. 2018;21(1):138–148. doi:10.1111/hex.12595
20. Chew LD, Griffin JM, Partin MR, et al. Validation of screening questions for limited health literacy in a large VA outpatient population. J Gen Intern Med. 2008;23(5):561–566. doi:10.1007/s11606-008-0520-5
21. Wolf MS, Smith SG, Pandit AU, et al. Development and validation of the consumer health activation index. Med Decis Making. 2018;38(3):334–343. doi:10.1177/0272989X17753392
22. Gale NK, Heath G, Cameron E, et al. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13:117. doi:10.1186/1471-2288-13-117
23. Tolley EE, Ulin PR, Mack N, et al. Qualitative Methods in Public Health: A Field Guide for Applied Research. Wiley; 2016.
24. Guest G, Johnson L, Johnson L. How many interviews are enough?: an experiment with data saturation and variability. Field Methods. 2006;18(18):59–82. doi:10.1177/1525822X05279903
25. Guest G, McKenna K, McKenna K. How many focus groups are enough? Building an evidence base for nonprobability sample sizes. Field Methods. 2017;29(1):3–22. doi:10.1177/1525822X16639015
26. Pratiwi H, Kristina SA, Widayanti AW, et al. A systematic review of compensation and technology-mediated strategies to maintain older adults’ medication adherence. Int J Environ Res Public Health. 2023;20(1):803. doi:10.3390/ijerph20010803
27. Gao R, Guo H, Li F, et al. The effects of health behaviours and beliefs based on message framing among patients with chronic diseases: a systematic review. BMJ Open. 2022;12(1):e055329. doi:10.1136/bmjopen-2021-055329
28. Conn VS, Ruppar TM, Chan KC, et al. Packaging interventions to increase medication adherence: systematic review and meta-analysis. Curr Med Res Opin. 2015;31(1):145–160. doi:10.1185/03007995.2014.978939
29. Pagan-Ortiz ME, Goulet P, Kogelman L, et al. Feasibility of a texting intervention to improve medication adherence among older HIV+ African Americans: a mixed-method pilot study. Gerontol Geriatr Med. 2019;5:2333721419855662. doi:10.1177/2333721419855662
30. Whiteley LB, Olsen EM, Haubrick KK, et al. A review of interventions to enhance HIV medication adherence. Curr HIV/AIDS Rep. 2021;18(5):443–457. doi:10.1007/s11904-021-00568-9
31. Bevilacqua KG, Brinkley C, McGowan J, et al. “We are getting those old people things”. Polypharmacy management and medication adherence among adult HIV patients with multiple comorbidities: a qualitative study. Patient Prefer Adherence. 2022;16:2773–2780. doi:10.2147/PPA.S382005
32. Mohan A, Majd Z, Johnson ML, et al. A motivational interviewing intervention to improve adherence to ACEIs/ARBs among nonadherent older adults with comorbid hypertension and diabetes. Drugs Aging. 2023;40(4):377–390. doi:10.1007/s40266-023-01008-6
33. Dillard PK, Zuniga JA, Holstad MM. An integrative review of the efficacy of motivational interviewing in HIV management. Patient Educ Couns. 2017;100(4):636–646.
34. Warren-Jeanpiere L, Dillaway H, Hamilton P, et al. Taking it one day at a time: African American women aging with HIV and co-morbidities. AIDS Patient Care STDS. 2014;28(7):372–380. doi:10.1089/apc.2014.0024
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Interventions Incorporating Therapeutic Alliance to Improve Medication Adherence in Black Patients with Diabetes, Hypertension and Kidney Disease: A Systematic Review
Desta R, Blumrosen C, Laferriere HE, Saluja A, Bruce MA, Elasy TA, Griffith DM, Norris KC, Cavanaugh KL, Umeukeje EM
Patient Preference and Adherence 2022, 16:3095-3110
Published Date: 14 November 2022
Validating a Self-Reported Medication Nonadherence Measure in the Context of Multiple Chronic Diseases and Routes of Medication Administration Among Patients with Type 2 Diabetes
Voils CI, Gavin KL, Thorpe CT, Pabich SK, Reeve BB, Mian GJ, Faacks A, Kronish IM
Patient Preference and Adherence 2022, 16:3119-3130
Published Date: 17 November 2022
Optimizing Type 2 Diabetes Management in a Medically Complex Patient: A Case Report of a Patient with Type 2 Diabetes and HIV
Kabakambira JD, Kong JM
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2401-2406
Published Date: 11 August 2023
Medication Adherence and Its Associated Determinants in Older Adults with Type 2 Diabetes and Cardiovascular Comorbidities
Al-Azayzih A, Kanaan RJ, Altawalbeh SM, Al-Qerem W, Smadi S
Patient Preference and Adherence 2023, 17:3107-3118
Published Date: 29 November 2023
Correlation Between Anthropometric Measurements with Cardiometabolic Biomarkers and Ten-Year Cardiovascular Risk Score Among People with HIV in Uganda
Baluku JB, Mutinye Kwesiga J, Adzemovic T, Nabwana M, Olum R, Bongomin F, Rhein J
HIV/AIDS - Research and Palliative Care 2025, 17:287-296
Published Date: 6 September 2025