Back to Journals » International Journal of Women's Health » Volume 18
A Psychosocial Intervention to Enhance Psychological Empowerment Among Women Survivors of Intimate Partner Violence: A Randomized Controlled Trial
Authors Khodadadi M, Hajihasani M ![]() , Kaveh M
, Kaveh M
Received 24 February 2026
Accepted for publication 10 June 2026
Published 16 June 2026 Volume 2026:18 601216
DOI https://doi.org/10.2147/IJWH.S601216
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marta Barba
Mahdieh Khodadadi, Mehrdad Hajihasani, Manijeh Kaveh
Department of Counseling and Psychology, Faculty of Literature and Humanities, Shahrekord University, Shahrekord, Iran
Correspondence: Mehrdad Hajihasani, Email [email protected]
Objective: Intimate partner violence (IPV) is a major public health concern with long-lasting psychological consequences for women survivors. The present randomized controlled trial examined the effectiveness of a structured psychosocial intervention in enhancing psychological empowerment as a mechanism of recovery among women who had experienced IPV in Iran.
Methods: A randomized controlled trial with a posttest-only design and a 50-day follow-up was conducted on 28 women survivors of IPV, who were randomly assigned to either an intervention group or a control group. The intervention consisted of eight 90-minute group sessions focused on cognitive restructuring and strengthening internal psychological resources. Psychological empowerment was assessed using a validated multidimensional instrument measuring competence, impact, meaning, self-determination, and trust. Data were analyzed using ANCOVA, MANCOVA, and paired-sample t-tests, with age included as a covariate.
Results: At post-test, the intervention group showed significantly higher psychological empowerment across all domains compared to the control group, including competence (F = 26.31, p < 0.001, η2 = 0.51), impact (F = 21.97, p < 0.001, η2 = 0.46), meaning (F = 33.25, p < 0.001, η2 = 0.57), trust (F = 20.16, p < 0.001, η2 = 0.44), and self-determination (F = 39.12, p < 0.001, η2 = 0.61). However, no statistically significant differences were observed between post-test and follow-up in the intervention group across all dimensions (all p > 0.05), indicating that gains were not significantly different at follow-up.
Conclusion: The findings suggest that structured psychosocial interventions may enhance psychological empowerment among women survivors of intimate partner violence. However, given the small sample size and posttest-only design, the results should be interpreted with caution. These interventions show promise as a supportive clinical approach, but further studies with larger samples and more rigorous designs are needed to confirm their effectiveness and generalizability.
Plain Language Summary: Intimate partner violence can negatively affect women’s mental health, confidence, and sense of control in daily life. This study investigated whether a structured psychosocial group program could help improve these outcomes among women survivors of intimate partner violence in Iran. In a small randomized controlled pilot study, participants were assigned either to receive an eight-session group intervention focused on strengthening coping skills and internal psychological resources or to a control group. We measured changes in psychological empowerment, which refers to a person’s sense of competence, meaning in life, ability to influence events, self-determination, and trust in oneself. The results suggest that women who participated in the program showed higher levels of psychological empowerment compared to those who did not receive the intervention. These findings provide preliminary evidence that such structured psychosocial support may be beneficial in helping survivors recover and rebuild confidence. However, because the study included a small sample size and did not include baseline outcome measurements, the results should be interpreted with caution. Further research with larger samples and more rigorous designs is needed to confirm and extend these findings.
Keywords: intimate partner violence, psychosocial intervention, psychological empowerment, resilience, women survivors
Introduction
Intimate partner violence (IPV) is a widespread global problem that transcends cultural boundaries and socioeconomic statuses, seriously undermining women’s health, autonomy, and social participation.1 IPV refers to a pattern of coercive and assaultive behaviors, including physical, psychological, sexual, and cyber abuse, as well as intimidation, threats, and social isolation.2–4 As a major public health concern, it is associated with a range of adverse psychological outcomes, such as depression, posttraumatic stress disorder, self-harm, and increased suicide risk, along with long-term physical health consequences.5–8
Beyond its psychological and health impacts, IPV also imposes substantial social and economic costs, including increased healthcare utilization, loss of productivity, legal system involvement, and welfare dependence.9,10 Despite extensive evidence on IPV prevalence across different regions—including high rates reported in the Middle East, Western countries, and Iran11–15—there remains a need for culturally responsive, evidence-based interventions that support recovery among women survivors. Accordingly, the present study aimed to evaluate the effectiveness of a culturally adapted psychosocial intervention designed to enhance psychological empowerment among women survivors of intimate partner violence in Iran.
Psychological empowerment has emerged as a key strategy in supporting women affected by domestic violence by enhancing their sense of control, competence, and autonomy.16 Empowerment-based interventions—such as goal-setting and individualized counseling—help reduce depression, anxiety, and trauma-related symptoms while fostering agency and self-efficacy.17 For example, the HOPE program (Helping to Overcome PTSD through Empowerment) combines CBT techniques with empowerment tools to improve safety, autonomy, and coping among women exposed to IPV. Although two randomized trials of Helping to Overcome PTSD through Empowerment showed mixed results—with one improving PTSD symptoms and the other reducing victimization—both demonstrated gains in empowerment.18,19 Similarly, Iverson et al found that the Recovering from Intimate Partner Violence through Strengths and Empowerment intervention significantly enhanced empowerment and self-efficacy, while also reducing depressive symptoms and IPV.20
Numerous studies indicate that empowerment-based interventions for the prevention of and recovery from intimate partner violence are most effective when they are tailored to the cultural, social, and economic contexts in which women live.21,22 Cultural factors such as collectivism and power distance may play an important role in shaping women’s experiences of IPV. Collectivism emphasizes interdependence and the importance of maintaining social harmony and “face”, which may reduce women’s willingness to disclose abuse or seek help.23,24 In addition, higher levels of power distance, often observed in traditional societies, may reinforce hierarchical gender roles and contribute to the normalization of male authority within intimate relationships.25 Consistent with this, evidence suggests that gendered and patriarchal beliefs are associated with increased risk of IPV and may shape how violence is interpreted and tolerated.25,26 This consideration is particularly critical in developing countries such as Iran, where distinctive cultural norms, family structures, and gender roles may shape both the origins and consequences of domestic violence.27
Although cultural beliefs have largely been examined as direct risk factors for IPV, emerging evidence suggests that they may also function as contextual moderators of psychological outcomes following abuse. Drawing on psychological empowerment theory and prior research conducted in Iran, the present study developed a culturally adapted psychosocial intervention that integrates cognitive restructuring with contextually relevant empowerment strategies for women survivors of IPV. Using a randomized controlled design, this study empirically evaluates the effectiveness of this intervention in strengthening key dimensions of psychological empowerment, thereby contributing context-specific evidence to the growing literature on culturally responsive interventions for survivors of intimate partner violence.
Hypothesis 1. Women who participate in the psychosocial empowerment intervention will report significantly higher overall psychological empowerment, conceptualized as a multidimensional construct comprising competence, impact, meaning, self-determination, and trust, compared to women in the control group at posttest. Hypothesis 2. Consistent with psychological empowerment theory, women in the intervention group will show significantly greater improvements in each core dimension of empowerment—competence, impact, meaning, self-determination, and trust—compared to the control group. Hypothesis 3. Improvements in psychological empowerment, including its core theoretical dimensions (competence, impact, meaning, self-determination, and trust), among women in the intervention group will be maintained at follow-up.
Method
This study employed a quantitative randomized controlled trial design with a posttest-only control group and a follow-up assessment. The study was conducted in accordance with CONSORT reporting guidelines, and a CONSORT flow diagram is provided in Figure 1. The study was designed as a pilot randomized controlled trial; therefore, no a priori power analysis was conducted prior to participant recruitment. The primary aim was to generate preliminary estimates of intervention effects and assess feasibility in a sensitive and high-risk population. In the context of intimate partner violence research, recruitment and retention of larger samples present ethical and practical challenges, including concerns related to participants’ safety, emotional vulnerability, and potential risks associated with group-based interventions. In addition, limiting the sample size was considered appropriate to ensure close monitoring of participants and maintain intervention quality. The posttest-only design was selected based on methodological and ethical considerations, where baseline assessment may lead to pretest sensitization, recall reactivation, and increased emotional or cognitive awareness, potentially influencing participants’ responses and coping processes prior to the intervention. Consistent with previous IPV-related randomized controlled trials,28 this approach was used to minimize measurement reactivity and reduce ethical burden. Accordingly, no pre-intervention outcome assessment was conducted. Random assignment was used as the primary strategy to ensure initial group comparability and control for potential confounders; however, due to the small sample size (N = 28), perfect baseline equivalence cannot be assumed, which is considered in the interpretation of findings. Future studies with larger samples and fully powered designs are required to confirm and extend these preliminary findings.
 |
Figure 1 CONSORT flow diagram of participant recruitment, allocation, follow-up, and analysis in a randomized controlled trial. |
Participants
The statistical population consisted of women who had experienced intimate partner violence within the past year and had referred to a social emergency center. A total of 28 participants were recruited through convenience sampling and randomly assigned to either the experimental (n = 14) or control group (n = 14). Randomization was performed using a simple random allocation procedure after recruitment, in which participants were assigned to groups based on an equal random distribution to ensure group comparability. Given the small sample size, baseline equivalence was additionally examined statistically. The experimental group received the psychological empowerment intervention, while the control group received no intervention during the study period. The control condition can therefore be considered a no-treatment control group, which does not control for attention effects and should be considered when interpreting the results. The mean age in the experimental group was 37.5 years (SD = 9.95), and in the control group was 43.3 years (SD = 5.04). Education levels were similarly distributed across groups, with six participants in each group having education below diploma level and eight participants having diploma-level education or higher. All participants completed the posttest and follow-up assessments, and no attrition was observed throughout the study period.
Intervention Procedures, Fidelity, and Study Blinding
The psychological empowerment intervention consisted of eight 90-minute group sessions focusing on cognitive restructuring and strengthening internal psychological resources. Intervention fidelity was ensured through a structured manual, standardized session content, and supervision by the principal researcher to maintain consistency across sessions. This study employed a single-blind design in which participants were not informed about their group allocation.
Inclusion and Exclusion Criteria
Inclusion criteria consisted of having experienced domestic violence within the past year, having visited a social emergency center, willingness to participate, and the ability to attend sessions. Individuals with severe psychiatric disorders or those receiving similar interventions were excluded. Exclusion criteria included withdrawal from the study, absence from more than two sessions, or requiring specialized treatment.
Data Collection Instrument
Data were collected using the Women’s Psychological Empowerment Questionnaire developed by Langroudi and Alibeigi,29 consisting of 39 items. This questionnaire measures five components: competence, impact, meaning, trust, and self-determination. It uses a 5-point Likert scale designed to assess the level of psychological empowerment and its components. Scoring involves summing the scores for each dimension; higher scores in any dimension indicate a greater impact of that component on psychological empowerment. The questionnaire’s Cronbach’s alpha coefficient was reported as 0.85, indicating good reliability and internal consistency. Its validity has been assessed through multiple versions of the questionnaire.29
Psychological Empowerment Program
The psychological empowerment program was specifically designed for this study based on scientific principles and empirical evidence. The design process began with an extensive review of previous studies on domestic violence, particularly research related to domestic violence in Iran. These studies provided a comprehensive understanding of the psychological needs and challenges faced by women affected by domestic violence in Iran. Additionally, similar empowerment programs implemented globally for women with experiences of domestic violence—such as the empowerment model by Cattaneo and Chapman30—were examined. This review included the assessment of intervention models and frameworks from various countries to extract best practices and techniques for developing an effective, culturally adapted local program. The adaptation process carefully considered the cultural and social context of Iran. Finally, the program content was presented to four experts for evaluation and feedback. These experts included a clinical psychologist, two family counselors, and a specialist in the field of domestic violence. The feedback collected in three stages from this panel played a crucial role in revising and enhancing the program’s structure and content. The description of each therapy session is provided in Table 1.
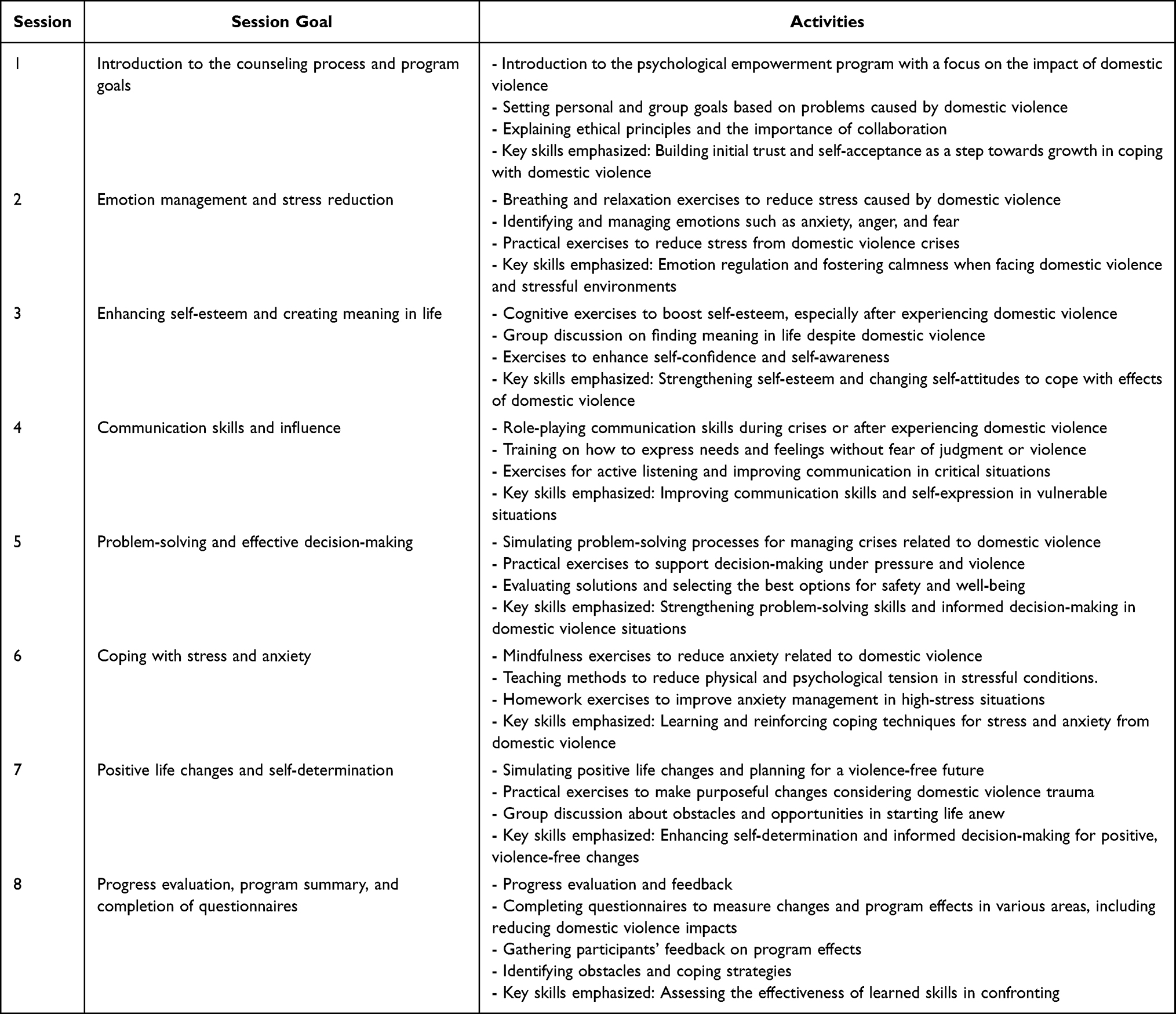 |
Table 1 Psychological Empowerment Program Session Protocol |
Implementation Procedure
After finalizing the program design, participants were randomly and equally assigned to the experimental and control groups. The experimental group participated in the psychological empowerment program, while the control group received no intervention. The intervention phase involved conducting the empowerment sessions according to the designed protocol in a safe, private, and supportive environment. These facilities were provided by the Social Emergency Services of Shahrekord and were deemed appropriate to ensure privacy and foster a trusting atmosphere. Sessions were held in groups focusing on skill training, practical exercises, and interactive discussions. Additionally, homework assignments were designed to reinforce learning and were reviewed and evaluated in subsequent sessions. After completing the intervention sessions, a post-test evaluation was conducted for both groups. To assess the sustainability of the intervention effects, a follow-up test was administered approximately 50 days after the program’s conclusion to evaluate the persistence of improvements and skill retention. The program was implemented in autumn 2024.
Ethical Considerations
All ethical principles were observed, including obtaining informed consent, maintaining confidentiality, providing psychological support when needed, ensuring a safe environment, preventing harm, and respecting participants’ right to withdraw. This research was approved by the Ethics Committee.
Data Analysis
To evaluate the effectiveness of the program, univariate analysis of covariance (ANCOVA) was conducted on the total psychological empowerment score controlling for age, which was included as a covariate due to its potential association with psychological outcomes and differential responsiveness to psychosocial interventions, and multivariate analysis of covariance (MANCOVA) was used to assess the empowerment components. Assumptions of the tests, including homogeneity of covariance matrices, normality of distributions, and homogeneity of variances, were confirmed. Additionally, paired t-tests were applied to compare posttest and follow-up results to examine the sustainability of the program effects. All analyses met the necessary assumptions and yielded valid results.
Results
According to Table 2, at the post-test stage, the experimental group scored higher means than the control group across all examined components (competence, impact, meaning, trust, self-determination, and psychological empowerment). For example, the mean psychological empowerment score in the experimental group was 176.21 with a standard deviation of 7.82, while in the control group it was 142.29 with a standard deviation of 6.77. At the follow-up stage, the experimental group’s mean psychological empowerment score reached 174.79 with a standard deviation of 7.85, showing a slight decrease compared to the post-test, indicating relative stability of the intervention’s effect. This relative stability was also observed in other components; for instance, the mean competence score in the experimental group decreased from 42.57 at post-test to 42.28 at follow-up. These findings suggest that the intervention’s effect was not only effective in the short term but also remained relatively stable over time (Table 2), supporting Hypothesis 1 regarding the increase in overall psychological empowerment.
 |
Table 2 Descriptive Statistics of Psychological Empowerment Scores at Two Measurement Points by Experimental and Control Groups |
To evaluate the effectiveness of the training program on the total psychological empowerment score, a univariate analysis of covariance (ANCOVA) was conducted, controlling for the age variable to more accurately assess the intervention’s impact on the total score. Additionally, a multivariate analysis of covariance (MANCOVA) was used to examine the program’s effect on increasing the psychological empowerment components among women with experiences of domestic violence. The assumptions for the tests were first checked using Box’s test, which showed a significance level greater than 0.05, confirming the homogeneity of covariance matrices. The Kolmogorov–Smirnov test indicated normal distribution of scores for all variables in both post-test and follow-up stages (all significance levels above 0.05). Levene’s test confirmed the homogeneity of variances. To compare post-test results with the follow-up stage, a paired t-test was used to assess the stability of the training program’s effects. Accordingly, all necessary assumptions for conducting ANCOVA, MANCOVA, and paired t-tests were met, ensuring the validity of these analyses.
In Table 3, the results of the univariate ANCOVA examining the effect of group (experimental vs. control) on the total psychological empowerment score are presented, with age controlled as a covariate. The findings indicate that the effect of group on the total empowerment score is significant (F = 27.08, p < 0.001) with a relatively large effect size (η2 = 0.52), confirming Hypothesis 1. Additionally, the effect of age on the total score is not significant (F = 0.51, p = 0.48), suggesting that after controlling for age, there remains a significant difference between the groups.
 |
Table 3 Univariate ANCOVA Results for the Effect of Group on Total Psychological Empowerment Score Controlling for Age |
The results of the multivariate analysis of variance (MANOVA) indicate a significant difference in psychological empowerment between the experimental and control groups (Table 4), supporting Hypothesis 2 regarding the improvement of individual components of psychological empowerment. All test indices, including Pillai’s Trace, Wilks’ Lambda, Hotelling’s Trace, and Roy’s Largest Root, showed significance levels less than 0.001, indicating a strong statistical difference between the two groups. Additionally, the F values in all tests were high, and the large effect size (0.87) reflects the substantial impact of the intervention on the psychological empowerment variables. These results confirm that the psychological empowerment training program significantly improved the psychological empowerment of women who have experienced domestic violence in the experimental group compared to the control group.
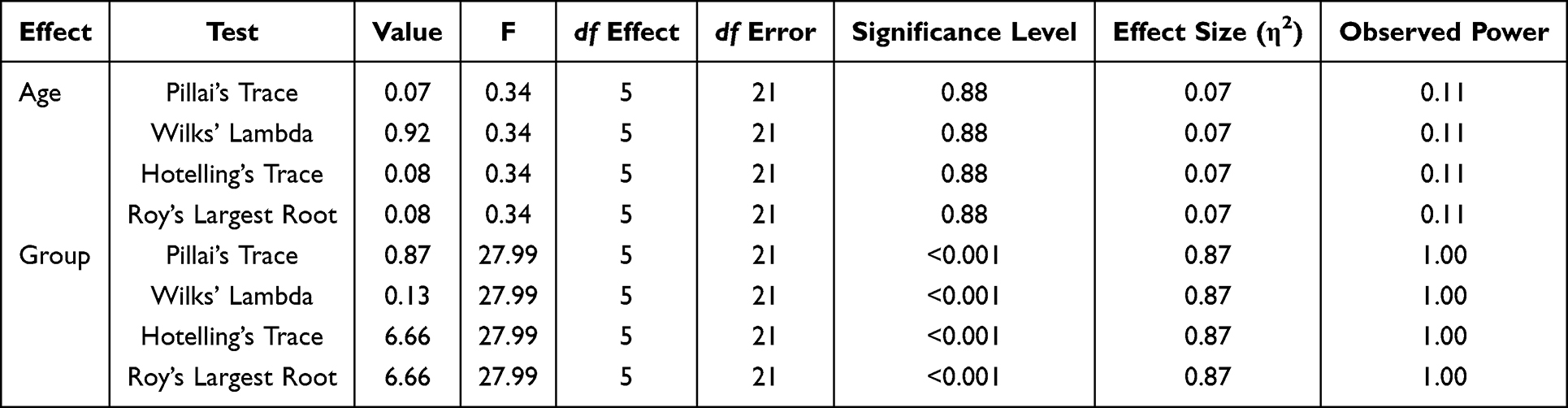 |
Table 4 Results of Multivariate Tests (MANCOVA) for the Effect of Group and Age on the Psychological Empowerment Components |
In Table 5, the effect of group (experimental vs. control) on the components of psychological empowerment was examined while controlling for age. The results of the ANCOVA indicated that there were statistically significant differences between the experimental and control groups across all components, after adjusting for age (all p < 0.001). The covariate (age) did not show a significant effect on any of the outcomes (all p > 0.05), indicating that age did not contribute meaningfully to the dependent variables.
 |
Table 5 Between-Group Effects for Comparing Psychological Empowerment Components in Experimental and Control Groups at Post-Test |
The effect sizes (partial η2) indicated large and substantial effects of the intervention on all components. The strongest effect was observed for self-determination (η2 = 0.61, 95% CI [0.40, 0.74]), followed by meaning (η2 = 0.57, 95% CI [0.36, 0.71]), competence (η2 = 0.51, 95% CI [0.31, 0.66]), impact (η2 = 0.46, 95% CI [0.26, 0.62]), and trust (η2 = 0.44, 95% CI [0.24, 0.60]). These findings support Hypothesis 2, demonstrating a strong positive effect of the educational intervention on all dimensions of psychological empowerment after controlling for age.
The results of the paired t-tests comparing psychological empowerment components at post-test and follow-up revealed different patterns across groups. In the experimental group (Table 6), none of the individual components showed statistically significant changes over time (p >0.05), indicating that the intervention effects on competence, impact, meaningfulness, trust, and self-determination were largely maintained at follow-up. In contrast, the control group (Table 7) demonstrated significant declines in several components, including impact, trust, and self-determination (p <0.05), along with non-significant downward trends in other dimensions. This pattern indicates a natural deterioration in psychological empowerment over time in the absence of intervention. Overall, these findings support Hypothesis 3, suggesting that the intervention contributed to the stability of psychological empowerment.
 |
Table 6 Results of the Paired t-Test Comparing Psychological Empowerment Components in the Experimental Group at Post-Test and Follow-Up |
 |
Table 7 Results of the Paired t-Test Comparing Psychological Empowerment Components in the Control Group at Post-Test and Follow-Up |
Discussion
The results of the present study indicated that the psychological empowerment program was associated with improvements in several psychological components among women who had experienced intimate partner violence (IPV), providing support for Hypothesis 1 regarding an increase in overall psychological empowerment. However, given the methodological limitations of the study, including the small sample size and the absence of baseline measurements, these findings should be considered preliminary, and causal attribution of effectiveness to the intervention should be made with caution. Within this context, the results are broadly consistent with previous empirical evidence suggesting that psychological empowerment programs may contribute to reductions in psychological distress and improvements in mental well-being. For example, studies by Shamsaie et al31 Rezaeian et al32 Garcia et al33 and Taccini et al34 have reported that empowerment-based interventions are associated with reductions in depression and stress symptoms, as well as improvements in self-esteem, quality of life, and perceived agency among women exposed to IPV. The intervention in this study was developed based on prior research and well-established theoretical frameworks addressing the empowerment of abused women.17,35,36
A major strength of this intervention was its focus on facilitating attitudinal and psychological changes in participants, supporting Hypothesis 2 regarding improvements in individual components of psychological empowerment. Attitudinal shifts are crucial precursors to behavioral change, especially for women who have experienced chronic violence. As Varkey et al37 notes, empowerment helps women reconstruct their value systems, enabling them to participate more actively in broader social contexts. This transformation in worldview often leads to the development of new behavioral strategies and recognition of alternatives to violent relationships. By fostering such internal changes, the program helped participants reframe their experiences, identify personal sources of strength, and understand that IPV is a social, rather than merely a private, problem.
The program’s emphasis on components such as self-efficacy, collective consciousness, competence, meaning in life, and self-determination further strengthened its effectiveness, providing strong evidence for Hypothesis 2. For instance, self-efficacy—defined as one’s belief in their ability to influence life events38—is fundamental to building resilience and autonomy in abused women. Collective consciousness enabled participants to realize that their experiences were not isolated and that shared social awareness could facilitate collective solutions.39 Other critical elements, including the reduction of guilt and the enhancement of competence, empowered women to view themselves as deserving of safe and fulfilling lives.40 Finally, self-determination—the capacity to make autonomous life choices—was central to restoring participants’ sense of control and dignity.41 Collectively, these components are widely recognized in the literature as foundational to psychological empowerment.
With respect to Hypothesis 3, the findings should be interpreted with caution. Although the intervention group demonstrated relative stability in most psychological components over time, the absence of baseline measurement and limited methodological controls restrict the strength of causal inference regarding long-term effectiveness. Nonetheless, the pattern of results suggests that the intervention may have contributed to maintaining gains over the follow-up period compared to typical fluctuations observed in similar populations. Educational empowerment programs such as the one implemented in this study may serve as structured catalysts for change by enhancing self-awareness, coping strategies, and interpersonal skills. These processes may also influence interpersonal trust, which is a dynamic and context-sensitive construct. Trust has been conceptualized as a malleable psychological state that can be reconstructed within safe and supportive environments,35 and its observed variation in this study may reflect such contextual and temporal influences rather than a stable dispositional change.
Limitations
This study has several limitations that should be acknowledged. First, the relatively small sample size and recruitment from a single cultural context (Iran) may limit the generalizability of the findings. Second, the absence of baseline (pretest) measurements and lack of an attention control group restricts the ability to draw strong causal conclusions regarding the effectiveness of the intervention. Third, reliance on self-report measures may introduce social desirability and response biases, which could influence the observed outcomes. Finally, the relatively short follow-up period limits conclusions regarding long-term sustainability. Therefore, the findings should be considered preliminary and interpreted with caution. Future research should replicate this intervention using larger and more diverse samples, stronger experimental designs, and extended follow-up periods. In addition, further studies may benefit from examining potential moderating variables such as socioeconomic status, educational level, and prior exposure to violence.
Future Research Directions
Future research should directly address the methodological limitations identified in the present study. First, replication of the intervention with larger and more diverse samples is essential to improve generalizability across different cultural and socioeconomic contexts, particularly beyond the Iranian setting. Second, future studies should employ more rigorous experimental designs, including pretest–posttest assessments and the use of attention control groups, in order to strengthen internal validity and allow for more robust causal inferences regarding intervention effectiveness. Third, incorporating multiple data sources beyond self-report measures—such as clinician ratings, behavioral observations, or qualitative interviews—may help reduce response biases and provide a more comprehensive understanding of psychological empowerment processes. In addition, longer follow-up periods are recommended to better evaluate the sustainability of intervention effects over time, as short-term follow-up limits conclusions about long-term maintenance of psychological empowerment. Finally, future research should examine potential moderating variables such as socioeconomic status, educational level, and prior exposure to violence, in order to identify for whom and under what conditions empowerment-based interventions are most effective.
Clinical and Policy Implications
Empowerment-based educational programs, such as the intervention used in this study, may serve as potential catalysts for psychological and social change by providing structured learning opportunities, constructive feedback, and opportunities for developing interpersonal and coping skills. By targeting self-awareness, emotional regulation, and communication skills, such interventions may contribute to improvements in self-confidence and may also support the development of trust—both in oneself and in others—which is considered an important component of psychological empowerment. Trust is particularly relevant in the recovery process following intimate partner violence, as it may influence emotional regulation and social reintegration. However, given the methodological limitations of the present study, including the small sample size and absence of baseline measurement, these findings should be interpreted as preliminary. Overall, the results provide tentative evidence that culturally adapted psychosocial interventions may be useful in clinical and community contexts for supporting resilience, self-efficacy, and well-being among women survivors of IPV. Policymakers and practitioners may consider integrating empowerment-based approaches into broader IPV support services; however, such recommendations should be viewed as suggestive rather than definitive, and further evidence from larger and more rigorous studies is required before strong policy conclusions can be drawn.
Ethical Consideration
This study was approved by the Ethics Committee of Shahrekord University, Shahrekord, Iran (Approval code: IR.SKU.REC.1403.012). All procedures performed in this study involving human participants were conducted in accordance with the ethical standards of the institutional research committee and the Declaration of Helsinki. Written informed consent was obtained from all participants prior to their enrollment in the study. Participants were assured of the confidentiality of their information and their right to withdraw from the study at any time without any consequences.
Acknowledgments
This article was derived from the Master’s thesis of the first author (Mahdieh Khodadadi). The authors would like to express their sincere gratitude to all the participants who generously shared their time and experiences, making this research possible.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any financial support.
Disclosure
The authors declare that there is no financial or personal conflict of interest related to this research.
References
1. Klein LB, Chesworth BR, Howland-Myers JR, Rizo CF, Macy RJ. Housing interventions for intimate partner violence survivors: a systematic review. Trauma Violence Abuse. 2021;22(2):249–12. doi:10.1177/1524838019836284
2. Dicola D, Spaar E. Intimate partner violence. Am Family Phys. 2016;94(8):646–651.
3. De Souza Santos D, Bittencourt EA, de Moraes Malinverni AC, Kisberi JB, de França Vilaça S, Iwamura ESM. Domestic violence against women during the Covid-19 pandemic: a scoping review. Forens Sci Int Rep. 2022;5:100276. doi:10.1016/j.fsir.2022.100276
4. Witkowska-Paleń A. Cyber-violence in intimate relationships: modern technologies as tools of domestic violence. Probation. 2024;1:139–168. doi:10.5604/01.3001.0054.4163
5. Beydoun HA, Beydoun MA, Kaufman JS, Lo B, Zonderman AB. Intimate partner violence against adult women and its association with major depressive disorder, depressive symptoms and postpartum depression: a systematic review and meta-analysis. Soc Sci Med. 2012;75(6):959–975. doi:10.1016/j.socscimed.2012.04.025
6. Cénat JM, Jacob G, Guillaume D, et al. Intimate partner violence and posttraumatic stress disorder among adolescents and young adults in Haiti. Psychiatry Res. 2024;338:115981. doi:10.1016/j.psychres.2024.115981
7. Kafka JM, Moracco KE (Beth), Taheri C, et al. Intimate partner violence victimization and perpetration as precursors to suicide. SSM Population Health. 2022;18:101079. doi:10.1016/j.ssmph.2022.101079
8. Lutwak N. The psychology of health and illness: the mental health and physiological effects of intimate partner violence on women. J Psychol. 2018;152(6):373–387. doi:10.1080/00223980.2018.1447435
9. Duvvury N, Callan A, Carney P, Raghavendra S. Intimate Partner Violence: Economic Costs and Implications for Growth and Development. World Bank; 2013. http://hdl.handle.net/10986/16697.
10. Peterson C, Liu Y, Kresnow M-J, et al. Short-term lost productivity per victim: intimate partner violence, sexual violence, or stalking. Am J Preventive Med. 2018;55(1):106–110. doi:10.1016/j.amepre.2018.03.007
11. Chen S, Ma N, Kong Y, et al. Prevalence, disparities, and trends in intimate partner violence against women living in urban slums in 34 low-income and middle-income countries: a multi-country cross-sectional study. EClinicalMedicine. 2025;81:103140. doi:10.1016/j.eclinm.2025.103140
12. Abujilban S, Mrayan L, Damra JK. Intimate partner violence among Jordanian pregnant women and its predictors. Nursing Open. 2022;9(1):267–276. doi:10.1002/nop2.1060
13. Ameli A, Salehi A, Molavi Vardanjani H, Vojoud M, Rahmati F. Prevalence of intimate partner violence among Iranian women: a systematic review and meta-analysis from 2010–2020. J Health Sci Surveillance Syst. 2024;12(2):106–116. doi:10.30476/jhsss.2023.96679.1665
14. Breiding MJ, Smith SG, Basile KC, Walters ML, Chen J, Merrick MT. Prevalence and characteristics of sexual violence, stalking, and intimate partner violence victimization—national intimate partner and sexual violence survey, United States, 2011. MMWR Surveill Summ. 2014;63(8):1–18.
15. Office for National Statistics. Domestic abuse in England and Wales overview: 2022. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/crimeandjustice/articles/domesticabuseinenglandandwalesoverview2021/2021-03-18.
16. Conger JA, Kanungo RN. The empowerment process: integrating theory and practice. Acad Manage Rev. 1988;13(3):471–482. doi:10.2307/258093
17. Kasturirangan A. Empowerment and programs designed to address domestic violence. Violence Against Women. 2008;14(12):1465–1475. doi:10.1177/1077801208325188
18. Johnson DM, Zlotnick C, Perez S. Cognitive behavioral treatment of PTSD in residents of battered women’s shelters: results of a randomized clinical trial. J Consulting Clin Psychol. 2011;79(4):542–551. doi:10.1037/a0023822
19. Johnson DM, Zlotnick C, Gonzalez A. Treatment of post-traumatic stress disorder in survivors of intimate partner violence. In: Geffner R, White JW, Hamberger LK, Rosenbaum A, Vaughan-Eden V, Vieth VI editors. Handbook of Interpersonal Violence and Abuse Across the Lifespan: A Project of the National Partnership to End Interpersonal Violence Across the Lifespan (NPEIV). Springer Nature Switzerland AG; 2022:3223–3246. doi:10.1007/978-3-319-89999-2_149
20. Iverson KM, Danitz SB, Shayani DR, et al. Recovering from intimate partner violence through strengths and empowerment: findings from a randomized clinical trial. J Clini Psych. 2021;83(1):21m14041. doi:10.4088/JCP.21m14041
21. Dalal K. Does economic empowerment protect women from intimate partner violence? J Injury Violence Res. 2011;3(1):35–44. doi:10.5249/jivr.v3i1.76
22. Rajkumar RP. Cultural collectivism, intimate partner violence, and women’s mental health: an analysis of data from 151 countries. Front Sociol. 2023;8:1125771. doi:10.3389/fsoc.2023.1125771
23. Hofstede G, Hofstede GJ, Minkov M. Cultures and Organizations: Software of the Mind.
24. Hwang KK. Foundations of Chinese Psychology: Confucian Social Relations. Springer; 2012.
25. Prospero M, Dwumah P, Ofori-Dua K. Violent attitudes and mental health symptoms among mutually violent Ghanaian couples. J Aggress Conflict Peace Res. 2009;1(2):16–23. doi:10.1108/17596599200900009
26. Thuc D, Hendra J. Results From the National Study on Domestic Violence Against Women in Viet Nam. United Nations; 2010.
27. Hajihasani M. Identification of Domestic Violence Patterns in Iran (Research Project). Shahrekord University. Commissioned by Chaharmahal and Bakhtiari Governorate; 2024.
28. Maruyama N, Kataoka Y, Horiuchi S. Effects of e-learning on the support of midwives and nurses to perinatal women suffering from intimate partner violence: a randomized controlled trial. Japan J Nurs Sci. 2022;19(2):e12464. doi:10.1111/jjns.12464
29. Charmchian Langerodi M, Alibaygi AH. An investigation of effective factors on rural women’s psychological empowerment in Sari. Quart J Woman and Soci. 2013;4(13):165–192.
30. Cattaneo LB, Chapman AR. The process of empowerment: a model for use in research and practice. Am Psychologist. 2010;65(7):646–659. doi:10.1037/a0018854
31. Shamsaie Z, Karimi Q, Akbari M. The effectiveness of an educational package based on domestic violence on reducing frustration and marital instability: a quasi-experimental study. J Rafsanjan Univ Med Sci. 2023;22(9):963–978. doi:10.61186/jrums.22.9.963
32. Rezaeian H, Rasooli R, Askarbiuky S, Asldehghan F. The effectiveness of psychological empowerment on the improvement of well-being and quality of life in householder women. Social Work Magazine. 2019;7(4):5–14.
33. Garcia ER, Stoever JK, Wang P, Yim IS. Empowerment, stress, and depressive symptoms among female survivors of intimate partner violence attending personal empowerment programs. J Interpersonal Violence. 2021;36(19–20):9557–9579. doi:10.1177/0886260519869693
34. Taccini F, Rossi AA, Mannarini S. Women’s EmotionS, Trauma and EmpowErMent (W-ES.T.EEM) study protocol: a psychoeducational support intervention for victims of domestic violence – a randomised controlled trial. BMJ Open. 2022;12(8):e060672. doi:10.1136/bmjopen-2021-060672
35. Anczewska M, Roszczynska-Michta J, Waszkiewicz J, Charzynska K, Czabala C. Empowering Women with Domestic Violence Experience. Bulgarian Comparative Education Society; 2012.
36. Wood L. Hoping, empowering, strengthening: theories used in intimate partner violence advocacy. Aff J Women Soc Work. 2015;30(3):286–301. doi:10.1177/0886109914563157
37. Varkey P, Kureshi S, Lesnick T. Empowerment of women and its association with the health of the community. J Women’s Health. 2010;19(1):71–76. doi:10.1089/jwh.2009.1444
38. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037/0033-295X.84.2.191
39. Lum D. Social Work Practice and People of Color: A Process-Stage Approach.
40. Gutierrez LM. Understanding empowerment: a conceptual framework. J Social Work. 1995;41(3):267–277. doi:10.1177/104973159500410030
41. GlenMaye LF. Empowerment-based practice with women who have experienced abuse. J Family Social Work. 1998;3(4):55–69. doi:10.1300/J039v03n04_05
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Association Between Intimate Partner Violence and Work Thriving/Work Alienation Among Chinese Female Nurses: The Mediating Impact of Resilience
Lei J, Lai H, Zhong S, Zhu X, Lu D
Journal of Multidisciplinary Healthcare 2024, 17:2741-2754
Published Date: 4 June 2024
The Association Between Intimate Partner Violence and Work Thriving/Work Alienation Among Chinese Female Nurses: The Mediating Impact of Resilience [Letter]
Mamuly WF, Sainafat A, Jotlely H
Journal of Multidisciplinary Healthcare 2024, 17:3617-3618
Published Date: 25 July 2024