")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
A Prospective Trial of the Microneedle Fractional Radiofrequency System Application in the Treatment of Infraorbital Dark Circles
Authors Wu X, Liu Y, Zhu J, Yu W, Lin X
Received 3 May 2022
Accepted for publication 3 July 2022
Published 8 July 2022 Volume 2022:15 Pages 1293—1300
DOI https://doi.org/10.2147/CCID.S372409
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Xianglei Wu,1,* Ying Liu,1,* Jiafang Zhu,1,* Wenxin Yu,1 Xiaoxi Lin1,2
1Department of Laser and Aesthetic Medicine, Shanghai Ninth People’s Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, People’s Republic of China; 2Department of Plastic and Reconstructive Surgery, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenxin Yu; Xiaoxi Lin, Department of Laser and Aesthetic Medicine, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China, Email [email protected]; [email protected]
Background: Infraorbital dark circles (IDC) are commonly consulted in aesthetic practice. There is not yet a multifactorial approach to facilitating their treatment.
Objective: To investigate the safety and efficacy of the microneedle fractional radiofrequency (MRF) system for the treatment of IDC.
Methods: A prospective, split-face, evaluator-blind clinical trial was conducted to study the change in the overall appearance, color, and wrinkles in 21 female patients with mixed type IDC before and after MFR treatment.
Results: Both patients and independent evaluators found significant improvement on the global aesthetic scales after the MFR treatment, especially on periorbital wrinkles (p=0.031). Trends in decreased melanin density in the IDC area were found, but no statistical differences were established. No side effects were observed.
Conclusion: MFR is a safe and effective modality for improving mixed type IDC by correcting the structural factors.
Keywords: infraorbital dark circles, microneedle fractional radiofrequency, radiofrequency, periorbital hyperpigmentation
Introduction
Infraorbital dark circles (IDC) are generally defined as bilateral semicircular hyperpigmentation in the infraorbital region.1 As a common presentation of periorbital melanosis, this entity is frequently consulted in dermatology practice not only due to aesthetic blemish but also to a negative impact on the quality of life.2 To date, there is little evidence reported on its global prevalence. We have identified limited data on some reported cases, mostly researching literature. In the Indian population, for example, IDC are reported most commonly in females (81%) and are predominant in younger people (16–25 years old, 47.5%).3 Still, we have a poor understanding of the IDC etiology. Studies report that exogenous (atopic dermatitis, ultraviolet, trauma, etc.) and endogenous (genetics, superficial location of the vasculature, tear trough, the extension of pigmentary demarcation lines of the face) factors independently or collaboratively cause IDC.4 IDC is classified into a pigmented, vascular, structural, and mixed type according to the primary cause of pathogenesis.5 The treatment strategy is commonly determined based on the IDC clinical type. For instance, therapeutic options for pigmented IDC include topical depigmenting agents, chemical peels, surgical corrections, and laser therapy, focused on treating hyperpigmentation. However, as the mixed type represents the significant majority of IDC;5 therefore, multiple therapeutic modalities are usually needed. While such a strategy is time- and cost-consuming, it also presents potential risks.
The therapeutic effect of monopolar radiofrequency is reported to improve periorbital skin laxity and wrinkles,6 which are common contributing factors of the structural IDC. An MFR system, which delivers radiofrequency energy through a fractional microneedle electrode assembly with adjustable length, has been used in treating photoaging, acne vulgaris, and scarring.7 Recent studies reported its application in hyperpigmentation, erythema, vascular malformation, and lipolysis.8–12 Given the previously mentioned pathogenesis of IDC, MFR could theoretically target most of the primary causes using a single device.
Our study aimed to investigate the potential utility and safety of MFR in Chinese patients as a novel therapeutic modality of IDC.
Materials and Methods
Study Design
This study was conducted in the Department of Laser and Aesthetic Medicine of the Shanghai Ninth People’s Hospital. As a prospective split-face study, all participants left side of the face was treated with IDC, and their right sides were considered the control side. This study was approved by the Ethical Committee of Shanghai Ninth People’s Hospital (SH9H-2019-T127-2) and was performed according to the principles of the Declaration of Helsinki. The patients fully understood the clinical trial and signed the informed consent (Chinese Clinical Trial Registration Number: CHiCTR1900026090).
Participants
Initially, 22 females aged 24 to 50 years old (mean age 31) with untreated mixed type IDC for > 1 year were enrolled in our study. The trial period started from April 2019 to July 2021. The study exclusion criteria were: no history of systemic disease (based on the approximately 3 months of physical examination), active inflammation/infection of the treated area, pregnancy, or new-onset diseases during treatment. Patients who received any medical treatment or surgery during the study were excluded. Also, patients were advised to avoid significant changes in diet and the use of skin-care products.
Treatment Protocol
The periorbital areas were cleaned, and then a topical anesthetic mixture of 2.5% prilocaine and 2.5% prilocaine cream (Ziguang Co. Ltd, Beijing, China) was applied 1 h before treatment. The IDC areas in all subjects were treated unilaterally with MFR (INTRAcelTM, Jeisys Medical, Seoul, Korea), the other side was not treated as the control group. The treatment protocol included three treatment sessions at 2 months intervals. In each session, patients were treated in two steps: the unipolar mode was applied during the first step and bipolar mode in the second. The MFR device was provided with disposable tips, which consisted of rows of 49 microneedle electrodes. The treatment parameters were set at: penetration depth 0.5 mm, fluency level 2, power 12.5 W, and duration 50 ms. No medication or specific care was indicated after treatment, except for the application of a cold compress to the treated area for 15 min every 2 h during the day of the procedure. The same physician performed all procedures. Postoperative instructions of the treated areas included: avoiding cleaning for 12 h, avoiding makeup application for 1 week, and strictly applying physical sun screening measures (hat, sunglasses, umbrella) for 1 week. Three follow-up visits were performed at 1, 3, and 6 months after the last treatment. The control side of face will be treated upon patients’ requests at the end of follow-ups.
Evaluations
The primary assessment focused on changes in the color of the IDC. Standardized digital photographs (60D camera, Canon, Melville, NY, USA) were taken at baseline and 1, 3, and 6 months after treatment for visual assessment. We applied the PAIS (patient’s aesthetic improvement scale) and GAIS (global aesthetic improvement scale) for global evaluation of the clinical outcome at the end of the treatment to all patients:13 1 = much worse, 2 = no change, 3 = improved, 4 = much improved, 5 = very much improved. Two independent physicians who were not involved in the medical treatments applied the GAIS. The average melanin density of the IDC area (melanin index, MI) was determined quantitatively by Skintel™ Melanin Reader™ (Palomar, USA) for an objective evaluation.14 The MI was calculated as the mean based on the detected value from three fixed points (medial canthus, medial point of lower eyelids, and lateral canthus).
The secondary assessment aimed to determine the improvement of the periorbital wrinkles and pain response in patients. Photo-documentation was gathered with the VISIA-CR (Canfield Scientific Inc., Fairfield, NJ, USA). This imaging system used analysis scripts to accurately detect and measure photographic evidence of periorbital wrinkles in a quantitative manner, which was recorded before each treatment and 6 months after the final treatment. Besides, patients recorded their pain response immediately during MFR treatment using the visual analog scale (VAS). Responses ranged from 0 (no pain) to 10 (unbearable pain).15 Other side effects, such as crusting, hematoma, infection, and scarring, were to be recorded as well.
Statistics
All data were analyzed using SPSS 26.0 (IBM, Armonk, NY, USA) and GraphPad Prism 7 (GraphPad Software, Inc., San Diego, CA, USA) to compare the therapeutic outcomes of MFR for treated unilateral IDC sides with untreated (control) sides for each patient. The differences in the measurement data were compared using the paired t-test, and ordinal data were analyzed using Spearman correlation coefficient. A P-value < 0.05 was considered statistically significant.
Results
Therapeutic Outcomes: Global Improvement of IDC After MFR Treatment
Twenty-one patients completed all three sessions of treatment and also at 6 months follow-up; one patient was excluded because of a nasal surgery performed during the study. PAIS was self-evaluated, and two independent physicians assessed GAIS based on digital photos. High correlations were found between these two scales (p<0.05). Both patients and physicians found significant improvement of IDC on the treated side compared with the control side after the MFR treatment (PAIS=3.44±0.88, GAIS=3.33±0.71, Spearman correlations, p=0.03). As shown in Figure 1, the appearance of IDC showed a narrowed area and lighter color.
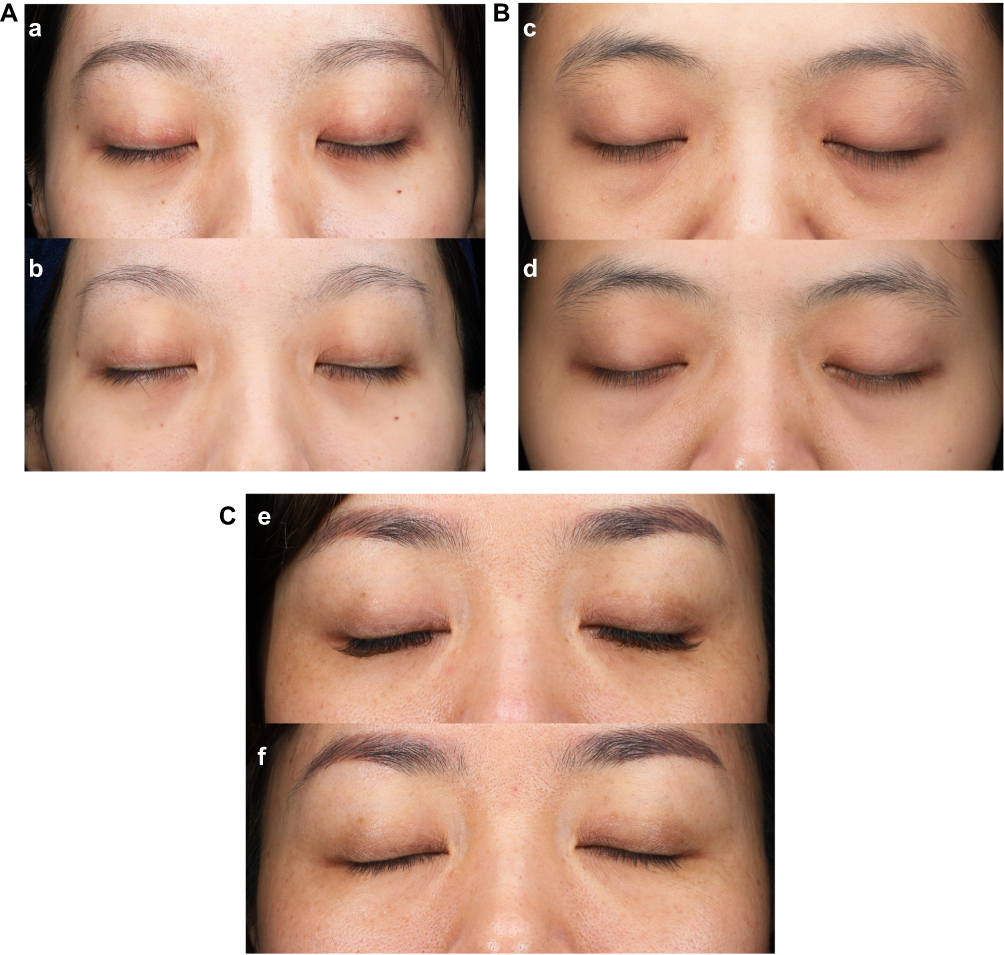 |
Figure 1 Typical cases. (A) Case No.1 Female, 26 years old, mixed type IDC (pigmented + vascular + structural). a. Baseline. b. Six months after the last treatment: left side (MFR treated) shows global improvement, disappearance of deep wrinkles, tightening of infraorbital skin, and whitening of IDC; right side (control) is unchanged. (B) Case No.2 Female, 25 years old, mixed-type IDC (pigmented + structural). c. Baseline. d. Six months after the last treatment. Left side (MFR treated): global improvement, of wrinkles, tightening of infraorbital skin. Right side (control): unchanged. (C) Case No.3 Female, 42 years old, mixed-type IDC (pigmented + structural). e. Baseline. f. Six months after the last treatment. Left side (MFR treated): disappearance of wrinkles, tightening of infraorbital skin, whitening of IDC. Right side (control): unchanged. |
Melanin Index (MI): Trends of Melanin Density Decreased in the IDC Area
The MI of the IDC area on the control side remained almost unchanged. On the treated side, in 6 patients, MI stayed at the same level, and in 2, it slightly increased, while the rest participants showed decreasing trends, but there was no statistical difference compared with the control side (p > 0.05) (Figure 2).
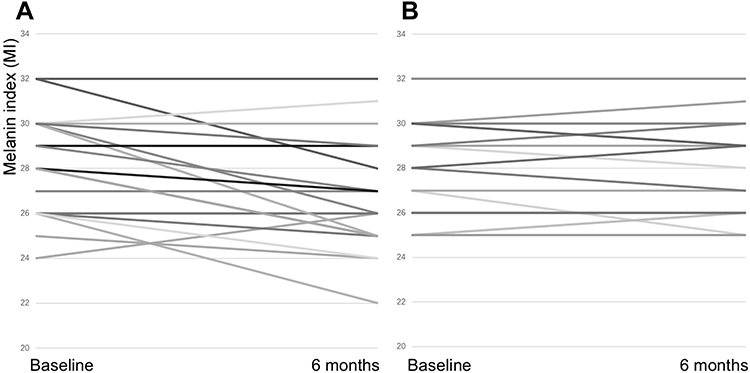 |
Figure 2 Improvement of Melanin index. (A) Treated side. (B) Control side. No statistical difference was found between the two sides (p > 0.05). |
Periorbital Wrinkles: Significant Improvement
The apparent disappearance of thick, deep wrinkles after treatment was found through a 3-dimensional analysis of VISIA-CR (Figure 3A). Compared with the initial image, the periorbital wrinkles decreased by 8.55%±9.03% on the treated side and by 1.07%±3.73%, on the control side. Significant differences were found between the two sides (Figure 3B, p=0.031, 95% CI 0.90–14.05).
 |
Figure 3 Improvement of periorbital wrinkles. (A) VISIA-CR images showing the improvement of periorbital wrinkles through 3-dimensional visual analysis. a1-a6: MFR-treated side, a7-a12: control side. (1–3, 7–9, baseline; 4–6, 10–12, after treatment). (B) Quantificational comparison based on VISIA results showed significant improvement on the rate of wrinkles of MFR-treated side (*p < 0.05). |
Side Effects: Tolerable Pain During the Treatment Procedure
The average VAS scores were 4.93±0.91. The participants did not report any side effects.
Discussion
This study represents the first effort to evaluate the role of MFR in IDC treatment. Overall, the MFR treatment showed clinical improvements in the mixed type IDC, especially in reducing the wrinkles.
Periorbital wrinkles were significantly reduced after the treatment, which might be the primary reason for the mixed type IDC global improvement. The results of our study were consistent with those of previous research on the rejuvenation of the periorbital area.12 As a type of radiofrequency system, MFR system facilitates the tightening the skin by promoting cell necrosis, collagen denaturation, and remodeling, eventually leading to skin contraction.10 Generally, the infraorbital area is challenging to treat using the classic radiofrequency system because of its narrow and irregular shape. MFR system showed an advantage in treating the infraorbital area while using a minute tip and dermal stamping mode.
Only trends but no significant decreases were established regarding the evolution of the melanin density in the treated IDC area. Q-switched or picosecond lasers are commonly used for treating periorbital hyperpigmentation. Laser therapy that targets melanin or water (ablative fractional carbon dioxide laser or non-ablative fractional Erbium laser) is generally safe and effective for patients with Fitzpatrick I–III skin types.16,17 However, the Asian population presents a higher risk of side effects, such as post-inflammatory hyperpigmentation (PIH) after aesthetic therapy due to higher melanin density.18,19 Furthermore, the etiology of IDC is complicated by ethical factors. Watanabe et al20 studied periorbital biopsies of 12 Japanese patients with IDC, and histology results showed that all of them had dermal melanocytosis. Boruah et al21 however, did not find any significant increase in melanocytes or pigmentation in the dermis, but only an increase in the melanocytes/pigmentation in the epidermis itself. The increase in dermal melanocytes or pigmentation is probably not a significant causative factor in the Indian population. Several studies reported the improvement of pigmentation following radiofrequency treatment. It might be explained by epidermal and dermal regeneration, hyaluronan increase, and the role of inflammation in the healing process.22–24 Therefore, the application of MFR system, which is not a chromophore-dependent device, might be a safer and more effective modality for improving hyperpigmentation if large scale studies could verify its use. Since the relapse of IDC is not rare in clinical practices, especially caused by skin laxity and dyspigmentation, a relative long follow-up should be considered for giving the treatment greater value. Previous studies conducted the follow-ups between 4 to 12 months25,26 and no recurrence was reported. Our study also did not find any relapse at the end of the study, which might be explained by durable regenerated collagen fiber and improved pigmentation.
The limitations of our study included small sample size and a relatively short follow-up period. Future research on this therapeutic modality should consider these factors for further evaluation.
Conclusion
In conclusion, our study is the first to report the safe and effective application of MFR system for treating IDC of mixed type through correcting structural factors in Chinese patients.
Abbreviations
IDC, infraorbital dark circles; MFR, microneedle fractional radiofrequency; PAIS, patient’s aesthetic improvement scale; GAIS, global aesthetic improvement scale; VAS, visual analog scale; PIH, hyperpigmentation; MI, melanin index.
IRB Status
This study was approved by the investigational review board of our hospital, the Shanghai Ninth People’s Hospital.
Ethics Statement
This study was approved by the Ethical Committee of Shanghai Ninth People’s Hospital (SH9H-2019-T127-2) and was performed according to the principles of the Declaration of Helsinki. The patients fully understood the clinical trial and signed the informed consent to participate as well as consent to publish the data (Chinese Clinical Trial Registration Number: CHiCTR1900026090).
Funding
The Project of Biobank from Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine. (No. YBKA201902).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sarkar R, Ranjan R, Garg S, Garg VK, Sonthalia S, Bansal S. Periorbital hyperpigmentation: a comprehensive review. J Clin Aesthet Dermatol. 2016;9:49–55.
2. Freitag FM, Cestari TF. What causes dark circles under the eyes? J Cosmet Dermatol. 2007;6:211–215. doi:10.1111/j.1473-2165.2007.00324.x
3. Sheth PB, Shah HA, Dave JN. Periorbital hyperpigmentation: a study of its prevalence, common causative factors and its association with personal habits and other disorders. Indian J Dermatol. 2014;59:151–157. doi:10.4103/0019-5154.127675
4. Roh MR, Chung KY. Infraorbital dark circles: definition, causes, and treatment options. Dermatol Surg. 2009;35:1163–1171. doi:10.1111/j.1524-4725.2009.01213.x
5. Huang YL, Chang SL, Ma L, Lee MC, Hu S. Clinical analysis and classification of dark eye circle. Int J Dermatol. 2014;53:164–170. doi:10.1111/j.1365-4632.2012.05701.x
6. Biesman BS, Baker SS, Carruthers J, Silva HL, Holloman EL. Monopolar radiofrequency treatment of human eyelids: a prospective, multicenter, efficacy trial. Lasers Surg Med. 2006;38:890–898. doi:10.1002/lsm.20452
7. Hantash BM, Renton B, Berkowitz RL, Stridde BC, Newman J. Pilot clinical study of a novel minimally invasive bipolar microneedle radiofrequency device. Lasers Surg Med. 2009;41:87–95. doi:10.1002/lsm.20687
8. Carruthers J, Carruthers A. Shrinking upper and lower eyelid skin with a novel radiofrequency tip. Dermatol Surg. 2007;33:802–809. doi:10.1111/j.1524-4725.2007.33173.x
9. Zhang M, Fang J, Wu Q, Lin T. A prospective study of the safety and efficacy of a microneedle fractional radiofrequency system for global facial photoaging in Chinese patients. Dermatol Surg. 2018;44:964–970. doi:10.1097/DSS.0000000000001469
10. Lu W, Wu P, Zhang Z, Chen J, Chen X, Ewelina B. Curative effects of microneedle fractional radiofrequency system on skin laxity in Asian patients: a prospective, double-blind, randomized, controlled face-split study. J Cosmet Laser Ther. 2017;19:83–88. doi:10.1080/14764172.2016.1256485
11. Hongcharu W, Gold M. Expanding the clinical application of fractional radiofrequency treatment: findings on rhytides, hyperpigmentation, rosacea, and acne redness. J Drugs Dermatol. 2015;14:1298–1304.
12. Lee SJ, Kim JI, Yang YJ, Nam JH, Kim WS. Treatment of periorbital wrinkles with a novel fractional radiofrequency microneedle system in dark-skinned patients. Dermatol Surg. 2015;41:615–622. doi:10.1097/DSS.0000000000000216
13. Jain R, Huang P, Ferraz RM. A new tool to improve delivery of patient-engaged care and satisfaction in facial treatments: the Aesthetic Global Ranking Scale. J Cosmet Dermatol. 2017;16:132–143. doi:10.1111/jocd.12297
14. Dolotov LE, Sinichkin YP, Tuchin VV, Utz SR, Altshuler GB, Yaroslavsky IV. Design and evaluation of a novel portable erythema-melanin-meter. Lasers Surg Med. 2004;34:127–135. doi:10.1002/lsm.10233
15. Myles PS, Myles DB, Galagher W, et al. Measuring acute postoperative pain using the visual analog scale: the minimal clinically important difference and patient acceptable symptom state. Br J Anaesth. 2017;118:424–429. doi:10.1093/bja/aew466
16. Altalhab S, Aljamal M, Mubki T, et al. Q-switched 532nm Nd:YAG laser therapy for physiological lip hyperpigmentation: novel classification, efficacy, and safety. J Dermatolog Treat. 2020;33:1–5.
17. Kim YJ, Suh HY, Choi ME, Jung CJ, Chang SE. Clinical improvement of photoaging-associated facial hyperpigmentation in Korean skin with a picosecond 1064-nm neodymium-doped yttrium aluminum garnet laser. Lasers Med Sci. 2020;35:1599–1606. doi:10.1007/s10103-020-03008-z
18. Chung JH, Hanft VN, Kang S. Aging and photoaging. J Am Acad Dermatol. 2003;49:690–697. doi:10.1067/S0190-9622(03)02127-3
19. Chung JH, Lee SH, Youn CS, et al. Cutaneous photodamage in Koreans: influence of sex, sun exposure, smoking, and skin color. Arch Dermatol. 2001;137:1043–1051.
20. Watanabe S, Nakai K, Ohnishi T. Condition known as “dark rings under the eyes” in the Japanese population is a kind of dermal melanocytosis which can be successfully treated by Q-switched ruby laser. Dermatol Surg. 2006;32:785–789. doi:10.1111/j.1524-4725.2006.32161.x
21. Boruah D, Manu V, Malik A, Chatterjee M, Vasudevan B, Srinivas V. A morphometric and immunohistochemical study of melanocytes in periorbital hyperpigmentation. Indian J Dermatol Venereol Leprol. 2015;81:588–593. doi:10.4103/0378-6323.168327
22. Verner I, Kutscher TD. Clinical evaluation of the efficacy and safety of combined bipolar radiofrequency and optical energies vs. optical energy alone for the treatment of aging hands. Lasers Med Sci. 2017;32:1387–1392. doi:10.1007/s10103-017-2257-z
23. Kołodziejczak AM, Rotsztejn H. Mexametric and cutometric assessment of the signs of aging of the skin area around the eyes after the use of non-ablative fractional laser, non-ablative radiofrequency and intense pulsed light. Dermatol Ther. 2017;30:e12470. doi:10.1111/dth.12470
24. Gold MH, Biron J, Wilson A. Improvement of skin texture and wrinkles using radiofrequency ultra-thin electrode technology. J Cosmet Dermatol. 2020;19:388–392. doi:10.1111/jocd.13239
25. Kontochristopoulos G, Kouris A, Platsidaki E, Markantoni V, Gerodimou M, Antoniou C. Combination of microneedling and 10% trichloroacetic acid peels in the management of infraorbital dark circles. J Cosmet Laser Ther. 2016;18(5):289–292. doi:10.3109/14764172.2016.1157363
26. Ma G, Lin XX, Hu XJ, Jin YB, Chen H. Treatment of venous infraorbital dark circles using a long-pulsed 1064-nm neodymium-doped yttrium aluminum garnet laser. Dermatol Surg. 2012;38(8):1277–1282. doi:10.1111/j.1524-4725.2012.02457.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.