Back to Journals » Journal of Blood Medicine » Volume 12
A Prospective Observational Study of Antihemophilic Factor (Recombinant) Prophylaxis Related to Physical Activity Levels in Patients with Hemophilia A in the United States (SPACE)
Authors Konkle BA ![]() , Quon DV, Raffini L, Recht M
, Quon DV, Raffini L, Recht M ![]() , Radulescu VC, Carpenter SL, Dunn AL, Lu M, Watt M
, Radulescu VC, Carpenter SL, Dunn AL, Lu M, Watt M
Received 1 July 2021
Accepted for publication 15 September 2021
Published 14 October 2021 Volume 2021:12 Pages 883—896
DOI https://doi.org/10.2147/JBM.S327180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Barbara A Konkle,1 Doris V Quon,2 Leslie Raffini,3 Michael Recht,4 Vlad C Radulescu,5 Shannon L Carpenter,6 Amy L Dunn,7 Mei Lu,8 Maureen Watt9
1Department of Medicine, The University of Washington and Bloodworks Northwest, Seattle, WA, USA; 2Orthopaedic Hemophilia Treatment Center, Orthopaedic Institute for Children, Los Angeles, CA, USA; 3Division of Hematology, Children’s Hospital of Philadelphia, Philadelphia, PA, USA; 4The Hemophilia Center, Oregon Health & Science University, Portland, OR, USA; 5Department of Pediatric Hematology and Oncology, University of Kentucky Medical Center, Lexington, KY, USA; 6Department of Hematology/Oncology, Children’s Mercy Hospital, Kansas City, MO, USA; 7Hemophilia Treatment Center, Nationwide Children’s Hospital and The Ohio State University College of Medicine, Columbus, OH, USA; 8Takeda Development Center Americas, Inc, Lexington, MA, USA; 9Outcomes Research & Epidemiology, Takeda Pharmaceuticals International AG, Zurich, Switzerland
Correspondence: Maureen Watt
Takeda Pharmaceuticals International AG, Thurgauerstrasse 130, Glattpark-Opfikon, Zurich, 8152, Switzerland
Tel +41 44 555 10 00
Fax +41 44 555 10 01
Email [email protected]
Introduction: High collision-risk physical activity can increase bleeding risk in people with hemophilia A, as can increasing the time between factor VIII (FVIII) administration and physical activity. FVIII prophylaxis may be tailored to planned activities to prevent activity-related bleeding.
Aim: To explore the relationship between physical activity levels, FVIII infusion timing, and occurrence of bleeding in patients with severe/moderately severe hemophilia A without FVIII inhibitors receiving antihemophilic factor (recombinant) (rAHF; ADVATE®; Baxalta US Inc., a Takeda company, Lexington, MA, USA).
Methods: SPACE was a 6-month, prospective, multicenter, observational outcomes study (NCT02190149). Enrolled patients received an eDiary application and a wearable activity tracker, which recorded physical activity, rAHF infusion, and occurrence of bleeding. Physical activity risks were ranked using National Hemophilia Foundation criteria.
Results: Fifty-four patients aged 11– 58 years (n = 47 prophylaxis, n = 7 on-demand) were included in the analysis. Patients had a mean (SD) 8.14 (10.94) annualized bleeding rate, and recorded 4980 intervals between an rAHF infusion and physical activity; 1759 (35.3%) of these intervals were ≤ 24 hours. Analysis of recorded eDiary data showed that the risk of activity-related bleeding did not significantly increase with time between last infusion and activity, but did increase with higher-risk physical activities. Analysis of activity tracker recorded data showed that the risk of bleeding reported by patients as spontaneous increased with prolonging time (≤ 24 to > 24 hours) from last infusion to physical activity start (odds ratio 2.65, p < 0.05). Joint health data collected at baseline were not included in the regression analysis because of small sample size; therefore the study could not assess whether patients with more joint disease at baseline were at higher risk of injury-related and reported spontaneous occurrence of bleeding.
Conclusion: These results show that activities with a high risk of collision lead to an increased risk of bleeding. Further investigation is warranted to explore potential benefits of FVIII infusion timing to reduce the risks of activity-related occurrence of bleeding.
Keywords: hemophilia A, recombinant factor VIII, physical activity, post-authorization study, prophylaxis, bleeding
Introduction
In people with hemophilia A (PwHA), prophylactic factor VIII (FVIII) replacement therapy has been the standard of care for bleeding prevention by maintaining plasma FVIII activity levels of ≥1%.1,2 The World Federation of Hemophilia (WFH) 2020 guidelines recommend FVIII activity levels of ≥3%.3 FVIII prophylaxis reduces frequency of bleeding with the goal of improving quality of life in PwHA.4–6 Individualized prophylactic regimens that aim to tailor FVIII levels to lifestyle and physical activity requirements are likely to offer further beneficial effects in minimizing bleeding risk while facilitating the physical and psychosocial benefits of exercise.7,8
Limited data exist on the relationship between FVIII levels and bleeding risk in PwHA and physically active lifestyles. Participation in vigorous, high-risk collision sports has been associated with a transient increase in bleeding risk, with most activity-related episodes manifesting within 1 hour of physical activity.9 While tailoring FVIII replacement therapy to a patient’s physical activity pattern is likely to be beneficial, it has only recently become part of routine practice.10 The evolution of hemophilia treatment in recent years, including the development of extended half-life FVIII products and non-factor replacement therapies,11 has meant that personalization of treatment is now becoming more widespread. Indeed, personalization of therapy based on each individual’s activities and lifestyle is recommended in the WFH 2020 guidelines.3
Patient questionnaires have typically been used to monitor physical activity in relation to occurrence of bleeding in PwHA. The use of commercial activity trackers in hemophilia research is limited, but continuous and long-term monitoring of activity with activity trackers was suitable in PwHA in an observational prospective study.12 Mobile applications for recording and monitoring occurrence of bleeding and dosing regimens offer an innovative method of data collection in clinical studies, with applications in telehealth for promoting appropriate use of clotting factors in patients with hemophilia.13
The prospective non-interventional Study of Prophylaxis, ACtivity and Effectiveness (SPACE) explored the effect of physical activity levels and timing of antihemophilic factor (recombinant) (rAHF; ADVATE®; Baxalta US Inc., a Takeda company, Lexington, MA, USA) infusion on occurrence of bleeding in patients with hemophilia A.
Materials and Methods
Study Design and Conduct
This prospective, multicenter, post-authorization, 6-month, observational outcomes study (NCT02190149) was conducted at 21 centers in the United States from June 2014 to June 2016. The study was approved by independent ethics committees for all participating sites and conducted in accordance with standards of good clinical practice in effect at the time of the study and the Declaration of Helsinki. All patients (or their legally authorized representatives) were provided with information about the purpose of the study and gave written consent before enrolment.
Patients
Inclusion criteria were: patients aged 13–65 years with severe or moderately severe hemophilia A (FVIII ≤2%), receiving rAHF and with a history of plasma-derived or recombinant FVIII replacement therapy for ≥150 exposure days. Patients with hemophilia B (factor IX [FIX] ≤2%) receiving recombinant factor IX, nonacog gamma (BAX 326, Rixubis®; Baxalta US Inc., a Takeda company, Lexington, MA, USA) were also eligible, but those results are not reported here. Patients with an inhibitor titer of ≥0.6 Bethesda units, or being treated for an inhibitor, or who had elective surgery planned within 6 months after enrolment that might interfere with daily activities, or those continuously requiring walking assistance devices were not eligible for enrolment.
Procedures
At baseline, investigators recorded treatment regimens (prophylaxis vs on-demand) and infusion timing schedules for patients receiving prophylactic rAHF (routine prophylaxis: 20–40 IU/kg every other/every third day; dosage targeted to maintain FVIII trough levels ≥1%).13 Patients remained on rAHF treatment as directed by their physician throughout this non-interventional study (12-month recruitment period, 6-month observation period). Patients received a customized eDiary smartphone application (Exco InTouch, an ERT company, Nottingham, United Kingdom) and a wearable activity tracker (Fitbit®; Fitbit, Inc., San Francisco, CA, USA), which recorded data during the observation period (ie, period between eDiary/activity tracker start and end dates) and at study completion (Figure 1A). The eDiary application was downloaded onto the patient’s smartphone and served as the primary data collection tool for patient physical activity, infusion timing, and occurrence of bleeds; if the patient did not have access to a suitable phone, one was provided for the study duration. During the observation period, upon occurrence of a bleeding episode, patients recorded in the eDiary the doses and reasons for infusions (routine prophylaxis or on-demand [ie, treatment for new occurrence of bleeding]). Lastly, the patients captured changes in treatment regimen at the time of study completion. Data collected via the activity tracker included steps taken and active minutes. Additionally, upon activity-related occurrence of bleeding, patients indicated what type of activity was associated with the occurrence of bleeding.
 |
Figure 1 (A) SPACE study design and timing of assessments. (B) Patient disposition. †For inactivity (n = 1), loss to follow-up (n = 1), non-compliance with required reporting (n = 1), or non-compliance with data entry (n = 1). ‡Technical problems, difficulty committing time (n = 6); non-compliance, withdrew consent (n = 5). §Non-compliance (n = 1) and technical difficulties (withdrawn per protocol; n = 2). ¶Other data includes number of concomitant medications, non-drug therapies and available pharmacokinetic data history. ††Completed 1 week before study end. Abbreviations: CRF, case report form; ED, exposure day; FVIII, factor VIII; HAL, Hemophilia Activities List; PedHAL, Paediatric Hemophilia Activities List; rFIX, recombinant factor IX; rAHF, antihemophilic factor (recombinant); SAE, serious adverse event. |
Objectives
The primary study objective was to explore the relationship between physical activity level, rAHF infusion timing, and occurrence of bleeding episodes in PwHA during a 6-month observation period. Secondary objectives included collecting physical activity data (type, frequency) using a patient self-reported eDiary and a consumer-based activity tracker.
Data Collection and Analyses
Estimation of Time Since Last Infusion to Start of Activity
To estimate the time (ie, number of hours) since the last rAHF infusion to the start of physical activity, each day was divided into the following four 6-hour cycles: Morning, 06:00 to 12:00; afternoon, >12:00 to 18:00; evening, >18:00 to sleep; and night, 24:00 to <06:00.
Physical Activity
At baseline, patients documented in the eDiary the physical activity type, average number of days per week spent participating at each risk level, barriers to participation, and information on FVIII infusions before planned activities. Patients rated their activities in the eDiary according to the National Hemophilia Foundation “Playing it safe” activity listing, which identifies a risk collision score associated with various activities; if an activity was not listed, patients were asked to estimate the risk level.14 Activities were thus classified into one of the following three categories based on the associated risk: (1) significant collisions are not expected; (2) significant collisions might occur, and (3) significant collisions are inevitable. During the observation period, patients recorded type, duration, and timing of activities undertaken daily in the eDiary. Timing of physical activity was recorded as a time range (ie, not the exact time); for the purposes of the analysis, the “morning” time range was set to start at 06:00 (morning), the “afternoon” time range at 12:00 (noon) and the “night” range at 18:00 (night). The activity tracker recorded daily totals for steps taken and active minutes.
Occurrence of Bleeding
At baseline, patients recalled from memory the number and location of occurrences of bleeding (eg, total and joint bleeds) during the 6 months before the date of informed consent, as well as the number and location of target joints, which were recorded on the case report form. Information on bleed history was also compiled from patient medical records. During the study’s 6-month observation period, patients recorded location, cause (any, activity-related, spontaneous, or other), type (joint or non-joint), and duration of occurrence of bleeding in the eDiary (retrospective entry for previous 2 days of data was permitted). If no end date was recorded for a bleeding episode, the study site followed up with the individual for bleed status. If the patient did not record/report bleed or infusion timing data during the allowed window of time, the data were considered missing. Only observed data were used in the analysis.
The number of bleeding episodes that happened during the study period was summarized by treatment regimen (prophylaxis or on-demand) vs type of bleed and by age group vs bleed type. Bleed frequency, annualized bleeding rate (ABR), and annualized joint bleeding rate (AJBR) were calculated for patient-level data.
Safety
From the time of informed consent to study completion, patients reported serious adverse events (SAEs) directly to study sites (ie, not in the eDiary); additional safety information was collected during follow-up calls every other month. SAEs included medical occurrences where the outcome was fatal, life-threatening, required inpatient hospitalization, or was a medically important event. AEs were categorized according to the Medical Dictionary for Regulatory Activities (version 19.0). The potential causal relationship between rAHF treatment and an SAE was also evaluated.
Treatment Adherence
Measures of adherence to prophylactic treatment during the 6-month observation period included dose adherence (proportion of total prescribed dose actually administered) and infusion timing schedule adherence vs baseline regimen. Infusion schedule was calculated both as a proportion of planned infusions administered and a proportion of planned infusions administered on schedule (within a 1-day window). All parameters were reported as means (SDs) of proportions.
Compliance to Data Entry
Data entry compliance was calculated as proportion of days during the observation period with complete entries. Patients received a motivational phone call every other month to ensure data entry compliance. Individuals with no recorded data for 2 consecutive weeks or for a total of 3 weeks were withdrawn from the study. Compliance was categorized by quintiles.
Data Collection Procedures
Patients were trained to use an integrated web portal (Exco InTouch database), which linked to the eDiary and activity tracker data. Data from the eDiary were automatically exported to the clinical database. Patients had to sync their activity tracker data to the web portal daily if their smartphone did not have the required capabilities for automatic syncing. A reminder message was sent to patients after a few days if they forgot to connect their activity tracker.
Statistics
To obtain 50 evaluable patients, the enrolment target was 60 patients. Because study objectives were exploratory, no formal power calculations were performed to determine sample size. Results were summarized by treatment regimen using descriptive statistics (Table S1 includes variables and subgroup definitions used in the analysis). The safety population comprised all patients who were treated with ≥1 rAHF dose. The full analysis set (FAS) population comprised patients in the SAS with valid eDiary activity data recorded.
Longitudinal logistic regression models were used to evaluate the dynamic association between physical activity levels, time since last infusion to start of physical activity cycle, and activity-related bleeding risk of patients in the FAS, regardless of treatment discontinuation. eDiary and activity tracker data were analyzed separately. Covariates are described in Table S1. Occurrence of bleeding episodes in each cycle was modelled as a binary dependent variable, and outcomes were expressed as the odds of bleeding in a given situation (odds ratio [OR] [95% confidence interval (CI)]) vs in absence of the situation (activity vs no activity). For safety data, p-values were calculated using chi-square or Fisher’s exact tests for categorical variables.
Results
Patients
Of 64 patients enrolled, 60 with hemophilia A receiving rAHF were eligible and 54 had both activity and rAHF infusion data recorded in the eDiary (FAS). Forty-two patients completed the study; 3 failed screening and 19 discontinued prematurely (Figure 1B). Information on data entry compliance for both eDiary and activity tracker entries was available for 53/54 patients, of whom 16 (30.2%) had entries for ≥60% of observation days (Table S2).
Mean (SD) age at screening was 23.7 (12.1) (range 11.0–58.0) years (Table 1). One patient in the FAS was younger than the lower age limit for study eligibility (13 years) and received a waiver to permit enrolment. Patients had a mean (SD) 5.0 (9.0) bleeding episodes (all bleeds) in the 6 months before providing informed consent. The majority of patients (47/54) received prophylaxis. The most common prophylactic dosing schedule at baseline and during the observation period was three infusions per week (n = 26, 55.3%), then infusions every second day (n = 8, 17.0%), then twice per week (n = 7, 14.9%). One patient in each regimen group at baseline switched regimens during the study.
 |
Table 1 Patient Baseline Characteristics |
Physical Activity
Physical activity intensity data recorded via the eDiary were available for 54 patients at baseline and 34 at study completion. In the 6-month pre-observation period, mean (SD) number of days per week spent on mild, moderate, and strenuous activity was 2.74 (2.29), 2.30 (1.70), and 1.65 (1.75), respectively. At study completion, mean (SD) number of days spent on each activity per week was 2.50 (2.29), 2.50 (1.80), and 2.35 (1.95) days, respectively (Table 2). Of 34 evaluable patients with available physical activity data at study completion, 29 (85.3%) patients reported that they infused prior to activity (27/31 patients on prophylaxis; 2/3 on-demand regimen).
 |
Table 2 Physical Activity Duration and Intensity at Baseline and Study End (eDiary Data) |
Among all 54 patients (prophylaxis or on-demand treatment) during the 6-month observation period, there were 4980 total intervals recorded between an rAHF infusion and the next recorded physical activity (morning, noon, or night). Overall, patients administered most infusions >24 hours before initiating activity (64.7%, 3221/4980 intervals); 479 (9.6%) intervals were ≥5 days. Overall, 27.8% of patients infused 1–2 days before starting an activity; the proportion was consistent across the activity risk level categories. Of 4980 total intervals, 3761 (75.5%) were associated with low-risk activities and 196 (3.9%) with high-risk activities (Table 3).
 |
Table 3 rAHF Infusions by Time from Most Recent Infusion Before Start of Physical Activity Based on NHF Activity Risk Level (eDiary Data) |
Occurrence of Bleeding
During the 6-month observation period, 17/54 (31.5%) patients reported no bleeding episodes (Table S3). The remaining 37 patients reported 185 bleeding episodes in total. Overall (n = 54), mean (SD) number of bleeds per person was 3.43 (5.06) for all bleeds, of which 1.52 (2.94) were reported by patients as spontaneous and 1.39 (2.11) as related to physical activity. For 31 patients receiving prophylaxis, there were 3.02 (4.72) bleeds per person (1.21 [2.41] reported by patients as spontaneous, and 1.26 [2.03] reported as activity-related); for six patients receiving on-demand treatment, there were 6.14 (6.77) bleeds per person (3.57 [5.13] reported as spontaneous and 2.29 [2.63] reported as activity-related).
At study end, mean (SD) ABR for all bleeds was 8.14 (10.94) among patients with ≥5 months of data during the observation period. ABR for all bleeds was higher for patients receiving on-demand therapy vs prophylaxis (Figure 2A). AJBR was 4.09 (8.05) overall, with a higher AJBR observed for patients receiving on-demand treatment vs prophylaxis (Figure 2B).
 |
Figure 2 Annualized bleeding rates (ABR) at study end by treatment regimen. (A) All bleeds. (B) Joint bleeds. †Patients with ≥5 months of follow-up data. Abbreviation: AJBR, annualized joint bleeding rate. |
Safety
Overall, 10 AEs, of which 7 were SAEs, were reported in 7 patients (all on prophylaxis); none of these AEs or SAEs were considered related to rAHF. The proportion of patients experiencing AEs did not differ significantly between age groups (Table S4).
Treatment Adherence and rAHF Consumption
For dose adherence assessment, the mean (SD) proportion of total rAHF dose received vs dose prescribed was 0.65 (0.31). For schedule adherence, the mean (SD) proportion of infusions received on schedule vs infusions planned was 0.48 (0.32) based on gap between infusions and 0.64 (0.28) based on number of infusions (Table 4); 19.1% (9/47) of patients received 80–100% of the prescribed prophylactic rAHF dose and 19.1% (9/47) received 80–100% of planned infusions (based on gap between infusions). Individuals aged ≥18 years were more adherent to prophylactic rAHF than those aged <18 years, with statistically significant differences for schedule adherence but not dose adherence (Table 4).
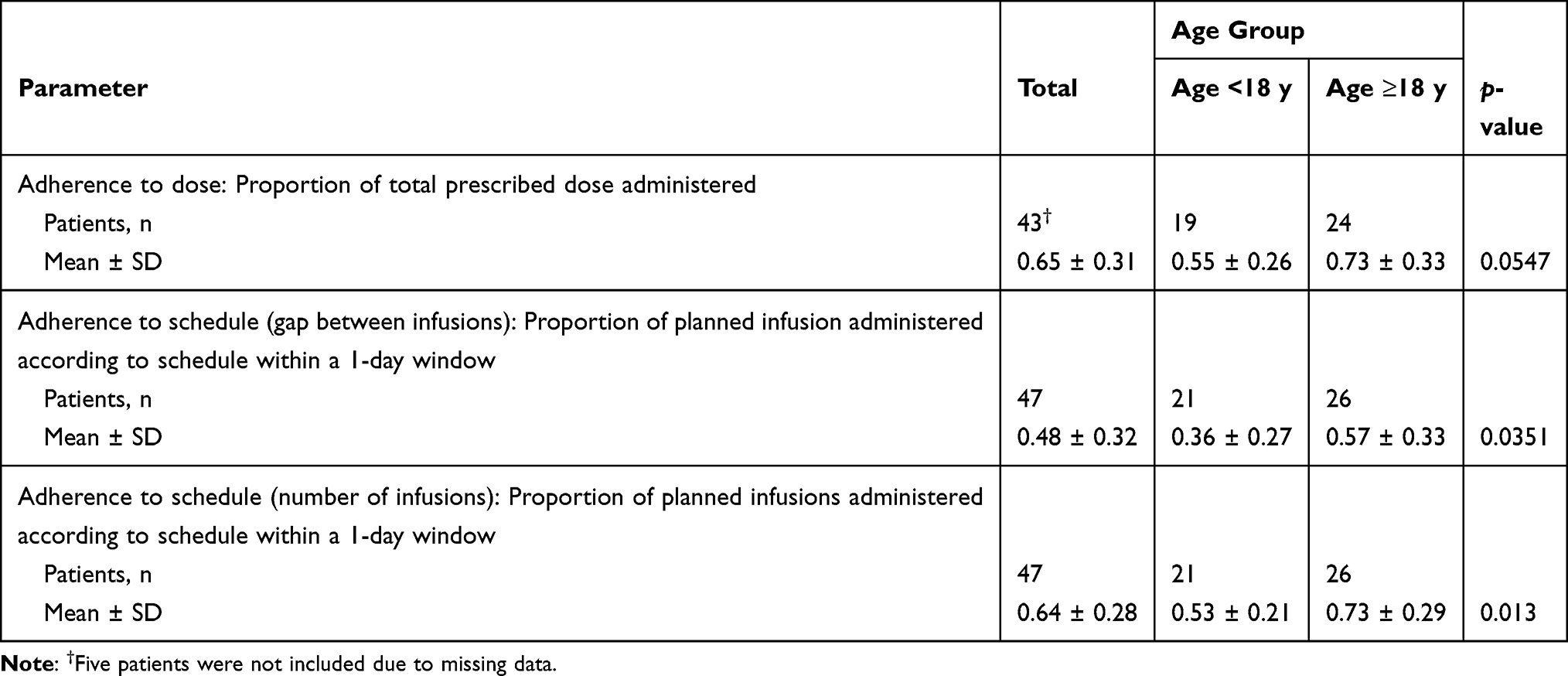 |
Table 4 Treatment Adherence to Prophylaxis |
Risk of Physical Activity-Related and Spontaneous Bleeds
According to data recorded in the eDiary, activity-related bleeding risk tended to increase commensurately with physical activities classified as higher risk (odds of activity-related bleeding for level 3 risk activity were 5 times that for no activity in those receiving prophylaxis; OR [95% CI] 5.06 [1.33–19.27], p = 0.0173; Table 5A). There was no significant correlation between bleeds recorded in the eDiary as activity-related and the time since last rAHF infusion.
 |
Table 5 Effect of Physical Activity and Time Since Last rAHF Infusion to Start of Activity on Risk of Bleeding Events Reported as Activity-Related by Patients with Hemophilia A Receiving Prophylactic rAHF: Logistic Regression Model Based on Data from the (A) eDiary and (B) Activity Tracker |
Regression analysis of activity tracker data showed no significant relationship between odds of physical activity-related occurrence of bleeding with either physical activity type or time between last rAHF infusion and start of physical activity (Table 5B), although prolonging time from last rAHF infusion to start of physical activity from ≤24 to >24 hours was significantly associated with higher risk of bleeding reported by patients as spontaneous (OR range, 2.61–2.65; all p < 0.05; Table 6).
 |
Table 6 Effect of Physical Activity and Time Since Last rAHF Infusion to Start of Activity on the Risk of Bleeding Events Reported as Spontaneous by Patients with Hemophilia A Receiving Prophylactic rAHF: Logistic Regression Model (Activity Tracker Data; N = 46)†,‡ |
Discussion
This study was designed to elucidate the temporal relationship between physical activity levels, FVIII infusion timing, and occurrence of bleeding episodes in adolescents and adults with hemophilia A who were prescribed rAHF in the United States. As expected, a higher-risk physical activity correlated with greater probability of bleeding reported as physical activity-related. However, eDiary and activity tracker data did not show that a longer time between last rAHF infusion and start of physical activity (≤24 vs > 24 hours) was associated with significantly greater risk of occurrence of bleeding reported by patients as physical activity-related. Although most patients infused before physical activity, nearly 65% of infusions occurred >24 hours (35.3% ≤24 hours) before initiating physical activity. rAHF infusion was timed more closely to physical activity and occurred more frequently among patients engaging in higher-risk activities, although 60% of infusion intervals for level 2.5–3 activities exceeded 24 hours. Together, these findings suggest that less than half of patients adjusted rAHF infusion timing for higher-risk physical activities.
The study cohort presented in this analysis represented a generally healthy population with hemophilia A, with a number of pre-study bleeding episodes comparable with that of prophylactically treated patients with severe hemophilia A in the United States.15 Time since last infusion was not significantly associated with an increased risk of activity-related bleeds, and this may be partially explained by patient-reported categorization of bleeding types as “any”, “spontaneous”, “activity-related”, or “other”. Some patients may have had difficulty identifying an occurrence of bleeding as physical activity-related vs spontaneous. Therefore, “activity-related” occurrence of bleeding may have been under-reported.
The study design did not mandate for exact timing of physical activities to be recorded; activity time was reported in the eDiary as morning, afternoon, and night (the statistical approach to these data was using 6-hour cycles), and assumed all activities occurred before bleeding onset. While this methodology may accurately reflect the sequence of physical activity and physical activity-related occurrence of joint bleeding episodes, it may not for other bleeding types (ie, spontaneous, any, and other). The 6-hour cycles may therefore have been too imprecise to robustly explore the relationship between timing of rAHF infusion and physical activity and bleed risk. Further, patient entries were retrospective and based on memory, thus subject to recall bias.16 In addition, activity tracker data may have been skewed towards including physically active patients and those interested in tracking physical activity. The results may therefore not be indicative of causal relationships and the findings should be interpreted with caution. Further, it may suggest that the National Hemophilia Foundation “Playing it safe” activity listing could predict high-risk activities inaccurately.
Analysis by physical activity level as a group meant that data were not skewed by individual patient physical activity levels. Nevertheless, further research on patient physical activity in relation to FVIII treatment patterns is warranted, preferably with inclusion of pharmacokinetic data so that correlations between FVIII levels and physical activity can be investigated. The small sample size of regression models for the physical activity level group would likely reduce their ability to control for confounding risk factors such as bleeding history.
Although joint health data were collected at baseline, they were not included in the regression analysis because of small sample size; therefore the study could not assess whether patients with more joint disease at baseline were at higher risk of injury-related and reported spontaneous bleeding. Lastly, only one-third of patients were ≥60% compliant with both eDiary and activity tracker data entry.
ABRs for all bleeds in this study were similar to bleeding rates from other real-world settings,17,18 although somewhat higher than rates reported at year 3 of rAHF treatment in the observational AHEAD study,19 and after ≥5 years of rAHF treatment in the AHEAD study.20 This may be explained by suboptimal prophylaxis adherence compared with other studies.18 Hemophilia A treatment adherence rates vary across studies due in part to lack of standardized estimation methods21 and barriers to prophylaxis adherence in a real-world setting.22 In the current study, adolescents exhibited worse adherence than adults, which is consistent with findings from elsewhere.23 We observed a small number of reported AEs or SAEs, none of which were considered related to rAHF.
Conclusions
The findings of this study did not demonstrate that a longer time between last rAHF infusion and physical activity start was associated with risk of occurrence of bleeding reported by patients as physical activity-related. Further studies designed to address the limitations herein described are needed to confirm the association between physical activity level, timing of infusions, and the occurrence of bleeding in patients with hemophilia A.
Data Accessibility
The datasets, including the redacted study protocol, redacted statistical analysis plan, and individual participant data supporting the results reported in this paper, will be made available within 3 months from initial request to researchers who provide a methodologically sound proposal. The data will be provided after its de-identification, in compliance with applicable privacy laws, data protection, and requirements for consent and anonymization. Data requests should follow the process described in the Data Sharing section on https://clinicaltrials.takeda.com/ and https://vivli.org/ourmember/takeda/.
Additionally, Friedrich Maritsch ([email protected]) can be contacted regarding data-sharing information.
Acknowledgments
The authors acknowledge all participating patients and all study site staff, including clinical investigator Susan Lattimore. This study was funded by the sponsor, Baxalta US Inc., a Takeda company, Lexington, MA, USA. Medical writing support for this paper was provided by Rosalind Bonomally, MSc, of Excel Medical Affairs (Fairfield, CT, USA), and was funded by Baxalta US Inc., a Takeda company, Cambridge, MA, USA.
Author Contributions
All authors contributed to the study concept and design. BAK, DVQ, LR, MR, VCR, SLC, and ALD were clinical trial investigators, and were involved in the execution of the study and acquisition of data. All authors participated in interpreting the data and critically reviewing the paper. All authors read and approved all versions of the paper before submission, including the final manuscript before submission, and agreed on the journal to which the paper was submitted. All authors take responsibility and are accountable for the contents of the paper.
Disclosure
BAK has received research support from Baxalta, Pfizer, Sanofi, Sigilon, Takeda, and Uniqure; and consulting fees from BioMarin, CSL Behring, Pfizer, Sanofi, Takeda, Sigilon, Spark, and Uniqure. DVQ has received consulting fees/honoraria from Bayer, BioMarin, Genentech, Novo Nordisk, Sanofi, and Octapharma; and has been a speaker for BioMarin, Genentech, Novo Nordisk, Sanofi, and Takeda. LR has participated on advisory boards for Bayer, CSL Behring, Genentech, Roche, HemaBiologics, and XaTek. MR has received research support for Oregon Health & Science University from BioMarin, Bioverativ/Sanofi, Catalyst Biosciences, Genentech, Hema Biologics, Novo Nordisk, Shire/Takeda, Spark, and uniQure; has been a consultant for the American Thrombosis and Hemostasis Network, Bayer, Bioverativ/Sanofi, CSL Behring, Genentech, Grifols, Kedrion, LFB, Novo Nordisk, Octapharma, Pfizer, Shire/Takeda, and uniQure; has been on the board of directors of the Foundation for Women and Girls with Blood Disorders and Partners in Bleeding Disorders; and is an employee of Oregon Health & Science University. VCR has received research support from Grifols, Pfizer, and Takeda. SLC has received honoraria from CSL Behring, Genentech, Kedrion, and Novo Nordisk; has received research support from the American Thrombosis and Hemostasis Network; and has been on the board of directors for the American Thrombosis and Hemostasis Network and the Hemostasis and Thrombosis Research Society. ALD has received research support from BioMarin and Takeda; and personal fees from CSL Behring, Genentech, Medscape, and uniQure. ML is an employee of Shire US Inc., a Takeda company, and a Takeda stock owner. MW is an employee of Shire International GmbH, a Takeda company, and a Takeda stock owner. The authors report no other conflicts of interest in this work.
References
1. Aledort L, Mannucci PM, Schramm W, Tarantino M. Factor VIII replacement is still the standard of care in haemophilia A. Blood Transfus. 2019;17(6):479–486. doi:10.2450/2019.0211-19
2. Srivastava A, Brewer AK, Mauser-Bunschoten EP, et al. Treatment Guidelines Working Group on Behalf of the World Federation of Hemophilia. Guidelines for the management of hemophilia. Haemophilia. 2013;19(1):e1–e47. doi:10.1111/j.1365-2516.2012.02909.x
3. Srivastava A, Santagostino E, Dougall A, et al. WFH guidelines for the management of hemophilia, 3rd edition. Haemophilia. 2020;26(Suppl 6):1–158. doi:10.1111/hae.14046
4. Manco-Johnson MJ, Abshire TC, Shapiro AD, et al. Prophylaxis versus episodic treatment to prevent joint disease in boys with severe hemophilia. N Engl J Med. 2007;357(6):535–544. doi:10.1056/NEJMoa067659
5. García-Dasí M, Aznar JA, Jiménez-Yuste V, et al. Adherence to prophylaxis and quality of life in children and adolescents with severe haemophilia A. Haemophilia. 2015;21(4):458–464. doi:10.1111/hae.12618
6. Krishnan S, Vietri J, Furlan R, Duncan N. Adherence to prophylaxis is associated with better outcomes in moderate and severe haemophilia: results of a patient survey. Haemophilia. 2015;21(1):64–70. doi:10.1111/hae.12533
7. Manco-Johnson MJ. Collision sports and risk of bleeding in children with hemophilia. JAMA. 2012;308(14):1480–1481. doi:10.1001/jama.2012.13303
8. Negrier C, Seuser A, Forsyth A, et al. The benefits of exercise for patients with haemophilia and recommendations for safe and effective physical activity. Haemophilia. 2013;19(4):487–498. doi:10.1111/hae.12118
9. Broderick CR, Herbert RD, Latimer J, et al. Association between physical activity and risk of bleeding in children with hemophilia. JAMA. 2012;308(14):1452–1459. doi:10.1001/jama.2012.12727
10. Wang M, Álvarez-román MT, Chowdary P, Quon DV, Schafer K. Physical activity in individuals with haemophilia and experience with recombinant factor VIII Fc fusion protein and recombinant factor IX Fc fusion protein for the treatment of active patients: a literature review and case reports. Blood Coagul Fibrinolysis. 2016;27(7):737–744. doi:10.1097/MBC.0000000000000565
11. Trinchero A, Sholzberg M, Matino D. The evolution of hemophilia care: clinical and laboratory advances, opportunities, and challenges. Hamostaseologie. 2020;40(3):311–321. doi:10.1055/a-1175-6530
12. Carrasco JJ, Pérez-Alenda S, Casaña J, Soria-Olivas E, Bonanad S, Querol F. Physical activity monitoring and acceptance of a commercial activity tracker in adult patients with haemophilia. Int J Environ Res Public Health. 2019;16(20):3851. doi:10.3390/ijerph16203851
13. Qian W, Lam TT, Lam HHW, Li CK, Cheung YT. Telehealth interventions for improving self-management in patients with hemophilia: scoping review of clinical studies. J Med Internet Res. 2019;21(7):e12340. doi:10.2196/12340
14. Anderson A, Forsyth A. Playing it safe: bleeding disorders, sports and exercise; 2005. Available from: http://www.hemophilia.ca/files/PlayingItSafe.pdf.
15. Manco-Johnson MJ, Soucie JM, Gill JC. Joint Outcomes Committee of the Universal Data Collection, US Hemophilia Treatment Center Network. Prophylaxis usage, bleeding rates, and joint outcomes of hemophilia, 1999 to 2010: a surveillance project. Blood. 2017;129(17):2368–2374. doi:10.1182/blood-2016-02-683169
16. Rudrapatna VA, Butte AJ. Opportunities and challenges in using real-world data for health care. J Clin Invest. 2020;130(2):565–574. doi:10.1172/JCI129197
17. Lou M, Ullman M, Baker J, et al. Comparison of clinical characteristics and health care utilization among individuals with hemophilia A and B in the hemophilia utilization group studies (HUGS) cohorts.
18. Kruse-Jarres R, Oldenburg J, Santagostino E, et al. Bleeding and safety outcomes in persons with haemophilia A without inhibitors: results from a prospective non-interventional study in a real-world setting. Haemophilia. 2019;25(2):213–220. doi:10.1111/hae.13655
19. Khair K, Mazzucconi MG, Parra R, et al. Pattern of bleeding in a large prospective cohort of haemophilia A patients: a three-year follow-up of the AHEAD (Advate in haemophilia A outcome database) study. Haemophilia. 2018;24(1):85–96. doi:10.1111/hae.13361
20. Tsakiris DA, Oldenburg J, Klamroth R, et al. Effectiveness and safety outcomes in patients with hemophilia a receiving antihemophilic factor (recombinant) for at least 5 years in a real-world setting: 6-year interim analysis of the AHEAD international and German studies.Presented at: 62nd American Society of Hematology Annual Meeting; December 5-8, 2020.
21. Young G. New challenges in hemophilia: long-term outcomes and complications. Hematology Am Soc Hematol Educ Program. 2012;2012:362–368. doi:10.1182/asheducation.V2012.1.362.3798344
22. Pipe SW. New therapies for hemophilia. Hematology Am Soc Hematol Educ Program. 2016;2016(1):650–656. doi:10.1182/asheducation-2016.1.650
23. Thornburg CD, Duncan NA. Treatment adherence in hemophilia. Patient Prefer Adherence. 2017;11:1677–1686. doi:10.2147/PPA.S139851
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.