Back to Journals » Nature and Science of Sleep » Volume 17

A Prospective Observational Study Investigating the Relationship Between Vitamin D Deficiency and STOP-Bang Parameters in Elderly Populations
Authors Chen YA ![]() , Chang WJ, Liao TW
, Chang WJ, Liao TW ![]() , Hung WS, Tung PH, Lin SW
, Hung WS, Tung PH, Lin SW ![]() , Hu HC, Chen NH, Fang JT, Chuang LP
, Hu HC, Chen NH, Fang JT, Chuang LP ![]()
Received 15 December 2024
Accepted for publication 25 August 2025
Published 29 September 2025 Volume 2025:17 Pages 2399—2410
DOI https://doi.org/10.2147/NSS.S509108
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Video abstract of “Vitamin D Deficiency in Elderly Patients in the STOP-Bang Questionnaire” [509108]
Views: 44
Yi-An Chen,1,2 Wen-Jui Chang,1,3 Ting-Wei Liao,4 Wei-Syun Hung,1 Pi-Hung Tung,1,5 Shih-Wei Lin,1 Han-Chung Hu,1,6 Ning-Hung Chen,1,6 Ji-Tseng Fang,7 Li-Pang Chuang1,2,6 On behalf of the Integrated Systematic Geriatric Medicine Information and Solutions for Exploring Healthy Aging (ISDHA)
1Department of Pulmonary and Critical Care Medicine, Sleep Center, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan; 2School of Medicine, College of Medicine, Chang Gung University, Taoyuan, Taiwan; 3Department of Pulmonary and Critical Care Medicine, New Taipei City Municipal TuCheng Hospital, Chang Gung Medical Foundation, New Taipei City, Taiwan; 4Department of Neurology, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan; 5Department of Pulmonary and Critical Care Medicine, Saint Paul’s Hospital, Taoyuan, Taiwan; 6Department of Respiratory Therapy, Chang Gung University, Taoyuan, Taiwan; 7Kidney Research Center, Department of Nephrology, Chang Gung Memorial Hospital and Department of Medicine, Chang Gung University, Taoyuan, Taiwan
Correspondence: Li-Pang Chuang, Department of Pulmonary and Critical Care Medicine, Sleep Center, Linkou Chang Gung Memorial Hospital, Taoyuan, 33380, Taiwan, Tel +886 3281200 ext 8470, Email [email protected]
Purpose: Could a simple sleep questionnaire reveal more than just obstructive sleep apnea (OSA) risk? Our study suggests it might. OSA is the most prevalent yet frequently underdiagnosed sleep disorder. Vitamin D deficiency shares multiple risk factors with OSA, such as obesity, older age, and hypertension. The STOP-Bang questionnaire, a simple, self-report screening tool originally designed to identify individuals at risk for OSA, may also highlight those susceptible to vitamin D deficiency. Therefore, this study aimed to investigate the associations between STOP-Bang parameters and vitamin D deficiency risk among elderly individuals.
Materials and Methods: This prospective observational study included 451 elderly individuals from the Healthy Aging Project at Chang Gung Memorial Hospital. Participants completed the STOP-Bang questionnaire for OSA screening and underwent clinical evaluation and blood testing for serum 25(OH)D levels.
Results: There was a statistically significant inverse correlation between vitamin D levels and body mass index (BMI). Additionally, participants with larger neck circumferences and female sex were significantly more likely to have vitamin D deficiency. In addition, people with more daytime tiredness had significantly lower serum 25(OH)D levels than did those in the other group.
Conclusion: We suggest screening for vitamin D deficiency among OSA patients with several risk factors identified with the STOP-Bang parameters, such as a larger neck circumference, higher BMI levels, and increased daytime sleepiness, to enable timely interventions addressing vitamin D deficiency and its associated consequences. Further research should investigate the causal relationship between vitamin D deficiency and OSA risk in elderly populations.
Keywords: obstructive sleep apnea, neck circumference, body mass index, daytime tiredness, 25(OH)D deficiency, STOP-Bang score
Introduction
Vitamin D is a fat-soluble hormone that modulates multiple physiological mechanisms.1–4 Studies have reported that vitamin D receptors (VDRs) are expressed in several brain regions responsible for circadian clock and sleep regulation, including prefrontal cortex, hypothalamus, substantia nigra, raphe nuclei, and midbrain central gray.3–6 Due to their involvement in circadian rhythm and sleep, vitamin D deficiency may contribute to sleep disturbances. Vitamin D deficiency is defined as a serum vitamin D concentration less than 20 ng/mL.7 In fact, previous studies have revealed age-related vitamin D deficiency and decreases in VDR expression, which may be one of the reasons why vitamin D deficiency is commonly observed in older populations.5
Recently, emerging observational and epidemiologic studies have suggested relationships between serum 25(OH)D deficit and sleep disorders.3,5 Evidence indicates that chronic low concentrations of serum 25(OH)D could result in muscle atrophy and increase the risk of nasal airflow restriction.8,9 As a result, the reduced ability of skeletal muscle to maintain the upper airway during sleep might be responsible for the elevated risk of developing Obstructive sleep apnea (OSA) in patients with low serum 25(OH)D levels.10,11 Vitamin D deficiency cause an increased risk of various conditions, including autoimmune diseases, chronic rhinitis, cardiovascular disease, and diabetes. These conditions may involve elevated inflammatory cytokines such as TNF-α, IL-1, and prostaglandin D2, which are known to influence immune modulation and infection susceptibility. Furthermore, evidence suggests that Vitamin D deficiency may result in the pathogenesis of OSA through pathways involving myopathy, inflammatory rhinitis, and tonsillar hypertrophy. The associated systemic inflammatory response and immune disturbances could potentially affect sleep regulation, further strengthening the relationship between Vitamin D deficiency and OSA.12,13 Schiza et al have also emphasized similar pathophysiologic mechanisms by which low vitamin D may impact upper airway function and predispose to sleep-disordered breathing.6 25(OH)D deficiency shares several relevant risk factors with OSA, such as obesity, age, hypertension, and neck circumference.5 Indeed, a cross-sectional study revealed that both insufficient and excessive sleep durations were linked to vitamin D deficiency in elderly Chinese women.14 Additionally, another study indicated that the association between serum 25(OH)D levels and an increased likelihood of sleep apnea was explained by the presence of a higher BMI and larger neck circumference among individuals with lower 25(OH)D levels.11
OSA is the most prevalent sleep disorder and is characterized by repetitive, partial, or complete obstruction of the upper respiratory tract during sleep.11,15,16 Patients with OSA may experience symptoms such as inattention, daytime sleepiness, fatigue, or memory loss, which seriously affect their life expectancy and quality of life.2,6 OSA is correlated with multiple factors, including age, sex, ethnicity, obesity, neck circumference and others.5,8,12,13,17,18 However, OSA is often underdiagnosed. Failure to diagnose and address OSA can result in severe health consequences, such as cognitive deterioration and increased overall mortality risk.19 Polysomnography is the gold standard for diagnosing OSA; nevertheless, it is costly and time-consuming.20
The STOP-Bang questionnaire provides a straightforward and self-reportable screening tool to identify patients at high risk of developing OSA, and it includes eight parameters (snoring, tiredness, observed apnea, high blood pressure, body mass index (BMI), age, neck circumference, and sex).19 The STOP-Bang questionnaire typically completed within 1–2 minutes, with overall response rates ranging from 90% to 100%. Due to its user-friendliness, efficiency, and high sensitivity, it has been broadly validated and applicated among diverse populations and clinical settings.21 Although an increasing number of studies have reported the impact of vitamin D deficiency on sleep disorders, few have systematically examined whether specific components of the STOP-Bang questionnaire—which is routinely used for OSA risk stratification—may also serve as indicators of vitamin D deficiency, particularly in elderly Asian populations. Given that vitamin D deficiency and OSA share common risk factors—including obesity, hypertension, and increased neck circumference—understanding their relationship is clinically relevant. Accordingly, the aim of this study was to determine the risk factors for vitamin D deficiency in elderly individuals via an OSA screening tool, the STOP-Bang questionnaire.
Materials and Methods
Patients and Study Protocol
This research is a part of the Healthy Aging Project, a prospective observational study conducted by Chang Gung Memorial Hospital (CGMH). The inclusion criteria were elderly individuals aged 60 years or above, who had CGMH admission records within one year and who had stayed in Taiwan for more than 180 days in the past year. The study protocol received approval from the Institutional Review Board of Chang Gung Memorial Hospital (IRB No. 2306300083), and all participants provided written informed consent before participation.
The exclusion criteria were severe organ abnormalities, such as congestive heart failure (New York Heart Association Functional Classification ≥ III), chronic obstructive pulmonary disease (hospitalization/emergency room visit or medication adjustment due to worsened condition in the past month), decompensated liver cirrhosis, or currently undergoing blood dialysis or cancer treatment; a history of severe autoimmune diseases; preliminary cognitive and mental assessment showing a Mini-Mental State Examination (MMSE) score of ≤ 26 and a Geriatric Depression Scale (GDS) score of ≥ 5; unable to undergo magnetic resonance imaging (MRI); having taken antibiotics in the past month; having impairments in hearing, vision, or cognition affecting communication; being unable to stand or walk unassisted (may use walking aids) or exhibiting unsteady gait while walking; having undergone relevant follow-up outpatient evaluations that may affect cognitive function assessment, including but not limited to stroke, Parkinson’s syndrome, Parkinson’s dementia, epilepsy, or brain tumors; having a history of psychiatric disorders such as schizophrenia, severe depression, bipolar disorder, alcohol or substance abuse; having a history of severe head injury leading to loss of consciousness; being currently diagnosed with depression and undergoing treatment; being previously diagnosed with dementia or depression; and being deemed unable to participate after physician evaluation.
Prior to this study, we referred to previous literature that reported correlation coefficient of approximately r= −0.2 and −0.132, respectively, between serum vitamin D level and BMI. Based on this previously reported correlation, a power analysis was conducted, indicating that a minimum sample size of approximately 200 and 448 participants was required to achieve sufficient statistical power (≥0.8) at an alpha level of 0.05.22,23 However, the study that determined a minimum sample size of 448 participants was conducted in adolescent population.23 To account for potential data variability, missing data, and unanticipated confounders, we aimed to recruit a larger sample. Ultimately, our study enrolled 451 participants, ensuring adequate statistical power and robustness of our findings.
Blood Sampling and Vitamin D (25-OH) Measurement
A total of 451 individuals meeting these criteria were enrolled in the study from September 2019 to May 2023. The data collected included previous medical history, current medications, tobacco use status, alcohol consumption status, age, sex and ethnicity. Physical measurements such as body height, body weight, heart rate, blood pressure, neck circumference, hip circumference, and waist circumference were taken via standardized techniques. BMI was calculated via the following formula: weight (kg)/height (m).2 Neck circumference was measured at the level of the cricothyroid membrane using a non-elastic tape with the subject sitting upright, head in a neutral position, and shoulders relaxed. All measurements were conducted by trained personnel following a uniform methodology to ensure consistency and reduce potential discrepancies. Measurements were taken to the nearest 0.1 cm at the end of a normal expiration. Fasting blood samples were obtained at 7 AM to assess vitamin D levels (evaluated as 25(OH)D) and other biochemical parameters. The 25(OH)D levels were measured using an electrochemiluminescence immunoassay (ECLIA), a highly sensitive method based on the interaction between vitamin D, labeled binding proteins, and chemiluminescent detection. This technique allows for accurate quantification of vitamin D by using ruthenium-labeled vitamin D binding protein and biotin-labeled vitamin D (25-OH), which form a complex that is detected through electrochemiluminescence signals.
Mini-Mental State Examination and Geriatric Depression Scale
To ensure that only cognitively intact individuals were included in the study and to screen for mental health conditions that might influence the study outcomes, we incorporated the Mini-Mental State Examination (MMSE) and the Geriatric Depression Scale (GDS) into our preliminary cognitive and psychological assessment. The MMSE is a widely used tool for assessing global cognitive function, with scores ranging from 0 to 30. A cutoff of ≤26 was used to exclude individuals with possible cognitive impairment, as lower scores indicate mild cognitive dysfunction.13 The GDS, a validated screening tool for late-life depression, consists of 15 items with a maximum score of 15. A cutoff of ≥5 was used to identify individuals likely to exhibit clinically significant depressive symptoms.24 These criteria were implemented to minimize potential confounding effects of cognitive decline and depression on participants’ responses and physiological parameters.
STOP-Bang Questionnaire
In this study, we used the STOP-Bang questionnaire (Taiwan version, 2015) to screen patients for OSA.25 It consists of eight self-reportable binary (yes or no) items (snoring, tiredness, observed apnea, high blood pressure, BMI, age, neck circumference, and sex) associated with the clinical features of sleep apnea, and the global scores range from 0 to 8. The scoring criteria for each item are as follows: snore loudly, often feel tired, fatigued or sleepy during the daytime, anyone observed you stop breathing during sleep, having (or being treated for) high blood pressure, BMI > 35 kg/m², age > 50 years old, neck circumference > 40 cm, and male sex.
The likelihood of moderate and severe OSA increases with increasing STOP-Bang scores, and likelihood of OSA can be predicted on the basis of the respective scores.21 A STOP-Bang score ≥ 3 demonstrates a sensitivity of 93% for identifying moderate to severe OSA (apnea-hypopnea index [AHI] > 15) and 100% for severe OSA (AHI > 30). The corresponding negative predictive values are 90% and 100%, respectively. Patients scoring 0 to 2 are considered low probability for moderate to severe OSA, whereas those scoring 5 to 8 can be categorized as high probability for moderate to severe OSA.26 For patients scoring in the intermediate range (3 or 4), further criteria are necessary for classification.21 Studies have demonstrated that STOP-Bang score of ≥5 is an effective threshold for identifying individuals at higher probability of significant OSA, with a score of 5 corresponding to an odds ratio of 4.8 for moderate-to-severe OSA and 10.4 for severe OSA.27 Accordingly, in this study, we used a STOP-Bang score ≥ 5, which represents a high probability for moderate to severe OSA, as a cutoff point to compare the mean vitamin D level.
Statistical Analysis
Information regarding the categorical variables of the participants is presented in terms of occurrence frequency and proportion. Variations were examined via chi-square analysis. The means and standard deviations (SDs) were used to summarize the quantitative data. The relationships between biochemical parameters and average serum 25(OH)D levels were assessed via Pearson correlation analysis. Independent-samples t tests were employed to compare mean serum 25(OH)D levels between distinct positive and negative parameters in the STOP-Bang questionnaire. Multiple linear regression (enter method) was used to quantify the association between the average serum 25(OH)D levels and STOP-Bang questionnaire variables, as well as control for potential confounders. All the statistical analyses were conducted via Statistical Product and Service Solutions (SPSS) statistical software (version 26.0. Armonk, NY: IBM Corp). The results are presented as the means ± SDs, and the reported P values are two-tailed, with a p value < 0.05 considered to indicate statistical significance.
Results
Overall, 451 participants with a mean age of 72.2 years were included. The average total serum vitamin D level was 29.7±10.7 ng/mL among all the participants. The demographic, comorbid disease, and lifestyle characteristics of the study individuals are provided in Table 1. Individuals were divided according to their total serum vitamin D level into a group with vitamin D deficiency (defined as a total serum vitamin D level ≤ 20 ng/mL) and a group without vitamin D deficiency (defined as a total serum vitamin D level > 20 ng/mL). There was a significantly greater proportion of female patients in the vitamin D deficiency group than in the non-deficiency group (P = 0.002). Additionally, there was a significantly higher proportion of patients with a smoking habit in the group without vitamin D deficiency (P = 0.034). Furthermore, the proportion of osteoarthritis patients was significantly higher in the group without vitamin D deficiency (P = 0.03). Although those with vitamin D deficiency had a higher mean BMI, the difference was not statistically significant. In addition, there were no statistically significant differences between the two groups in terms of age, body weight, waist circumference, other comorbid disease or lifestyle.
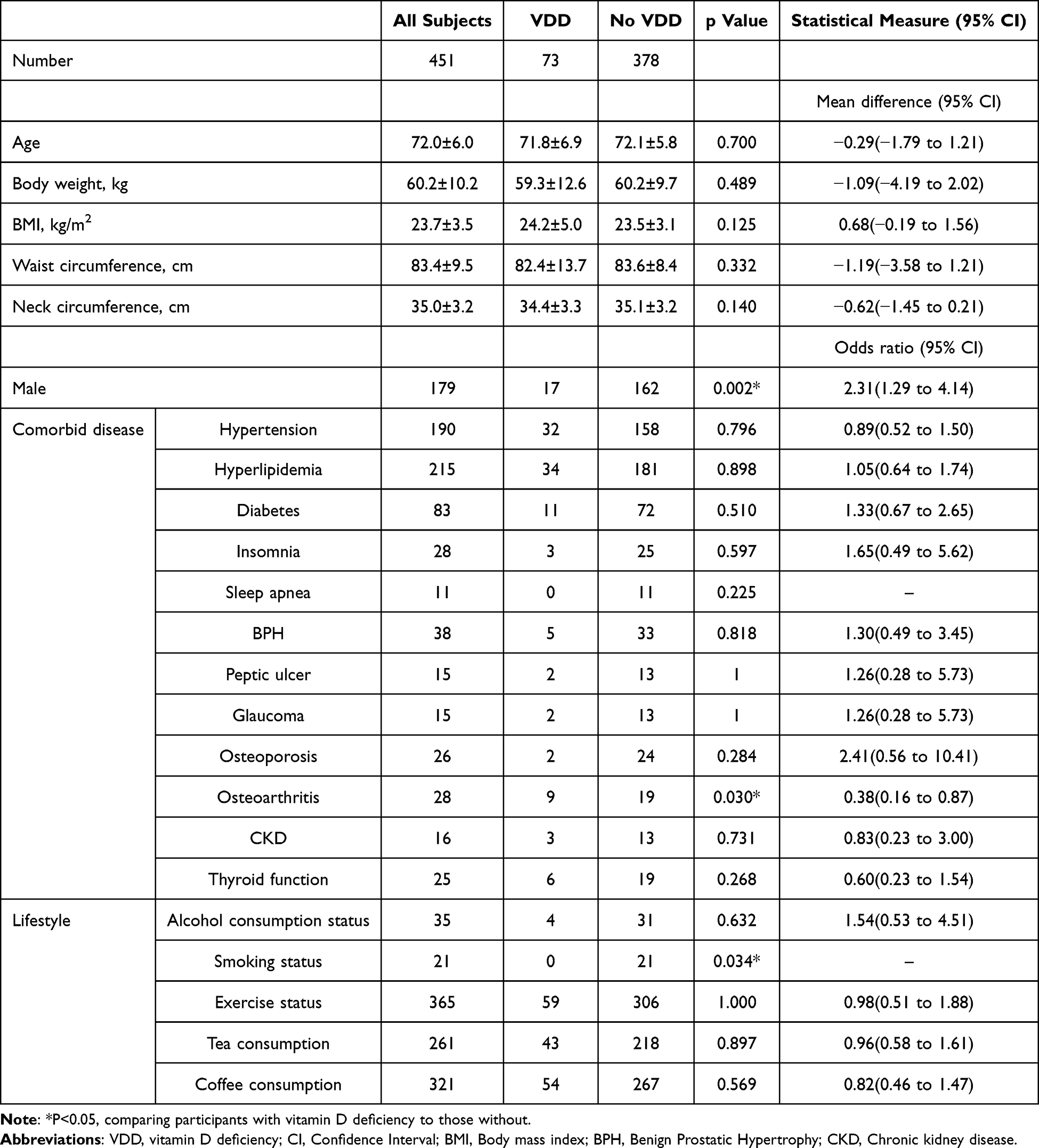 |
Table 1 Comparison of Anthropometric Characteristics Between Participants with Vitamin D Deficiency (Total Serum Vitamin D Level ≤ 20 ng/Ml) and Those Without Vitamin D Deficiency (Total Serum Vitamin D Level > 20 ng/Ml) |
A chi-square test was conducted to compare distributions of vitamin D deficiency and STOP-Bang parameters. Although those with observed apnea, tiredness, and older age composed a greater proportion of vitamin D deficiency patients, the difference was not statistically significant. In contrast, those with larger neck circumferences and female sex were significantly more predominant among patients with vitamin D deficiency than among patients without vitamin D deficiency (Table 2).
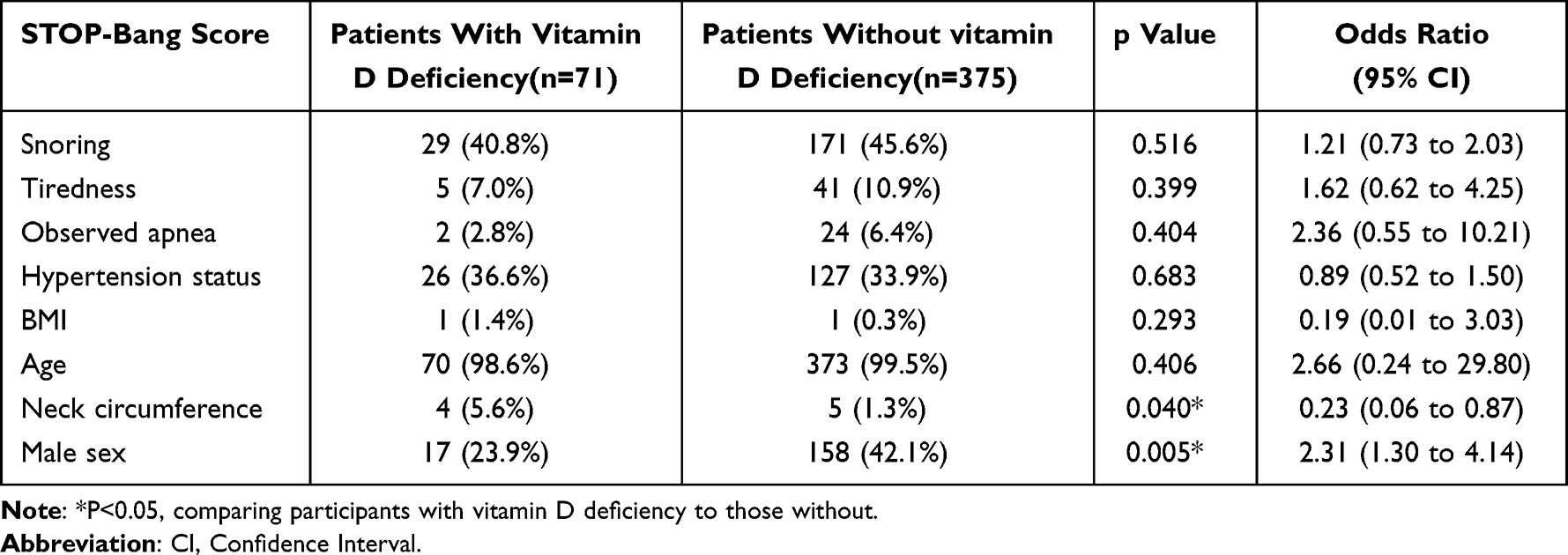 |
Table 2 Chi-Square Test for the Comparison of STOP-Bang Parameters Among Patients with and Without Vitamin D Deficiency |
Since the proportion of patients with vitamin D deficiency in our study is not very high, we further evaluated which OSA risk factors were related to vitamin D levels to better understand potential associations between sleep-related risk factors and vitamin D concentrations, even in individuals who may not meet the strict criteria for vitamin D deficiency. The vitamin D levels between those with or without positive STOP-Bang parameters are shown in Figure 1. People with more daytime tiredness had significantly lower serum 25(OH)D levels than did those in the other group (P=0.029). In addition, there was a significantly lower 25(OH)D level in participants with larger neck circumferences (P=0.023). The average vitamin D levels were slightly lower in patients with STOP-Bang scores ≥5, who are considered likely to have OSA, compared with those in the lower-score groups; however, this difference was not statistically significant (Table 3).
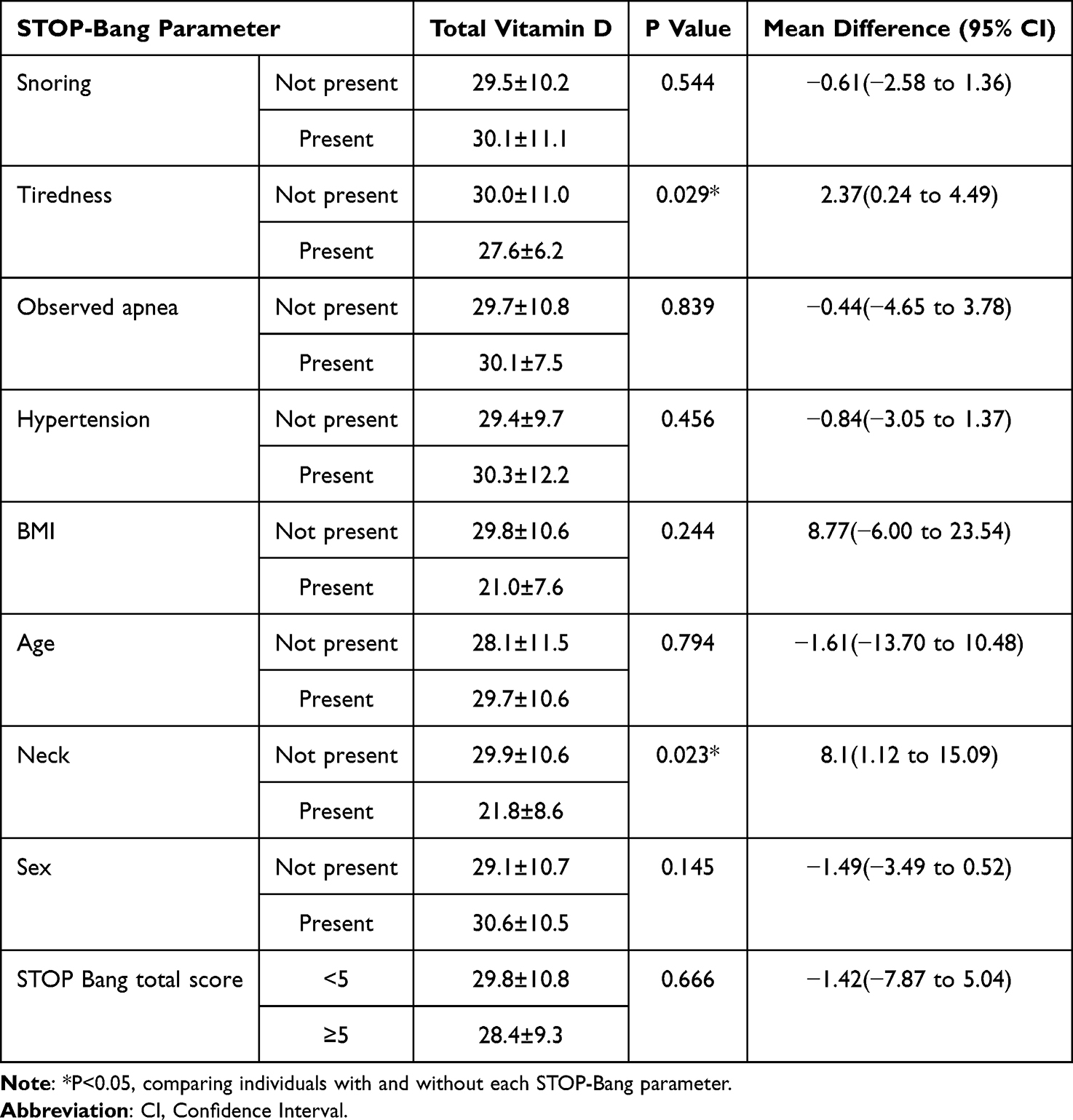 |
Table 3 Total Vitamin D Levels Among Individuals with or Without Each STOP-Bang Parameter |
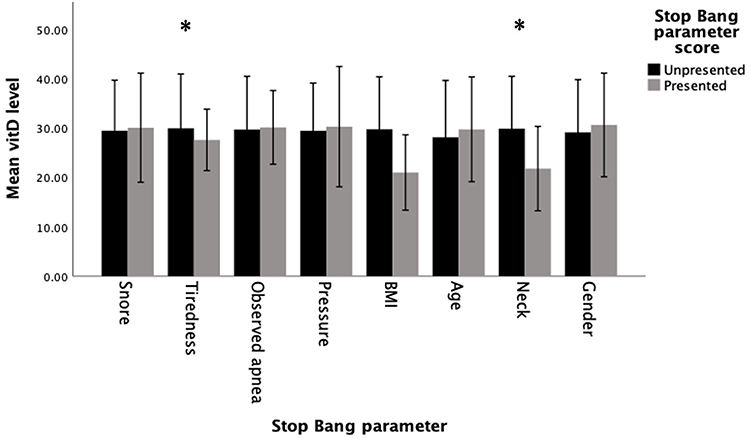 |
Figure 1 Average vitamin D levels among patients with and without each STOP-Bang parameter. Error bar: ± 1 SD; *: P < 0.05, unpresented compared with presented. |
We also performed Pearson correlation analysis to estimate the potential associations between vitamin D levels and the risk of developing OSA. Table 4 displays the correlations between vitamin D levels and scores on the different STOP-Bang parameters. There was a statistically significant inverse correlation between vitamin D levels and BMI (P= 0.005). However, there was no correlation between the serum vitamin D level and other linear STOP-Bang parameters, such as blood pressure, neck circumference, age, or total STOP-Bang score.
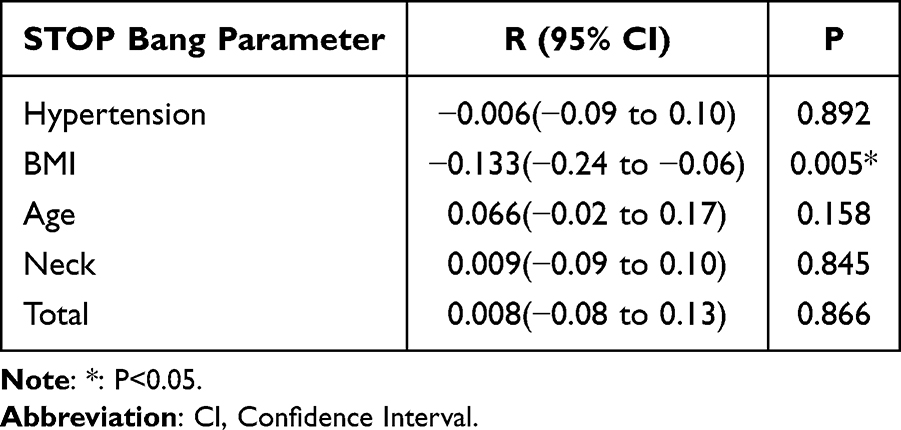 |
Table 4 Correlations Between Vitamin D Levels and STOP-Bang Parameters. The Pearson Correlation Coefficient and P value are Shown |
To ensure that the findings presented in Table 4 were not confounded by other variables, we employed a multiple linear regression analysis (Table 5). Multiple linear regression enables the assessment of the relationship between a dependent variable and multiple independent variables simultaneously, thereby controlling for potential confounders and isolating the effect of each predictor.28 The variables included in the model were BMI, neck circumference, age, blood pressure, snoring, tiredness, observed apnea, gender, osteoarthritis and smoking status. After accounting for other factors, BMI remained significantly correlated with 25(OH)D levels (p < 0.001), and there was no significant correlation between the serum vitamin D level and other STOP-Bang parameters.
 |
Table 5 Multiple Linear Regression Analysis for Variables Associated with 25(OH)D Serum Levels |
Since BMI was the only STOP-Bang parameter showing a significant correlation with serum vitamin D levels and due to the higher proportion of female participants in our study, we conducted a subgroup analysis by gender. Table 6 revealed that serum vitamin D levels were significantly negatively correlated with BMI among females (r = −0.163, p = 0.007), whereas no significant correlation was observed among males (r = −0.083, p = 0.272). This finding suggests the possibility of gender-specific relationship between vitamin D status and BMI.
 |
Table 6 Subgroup Analysis by Gender: Pearson Correlation Coefficients Between Serum Vitamin D Levels and BMI |
Discussion
In this research, we investigated the relationships of vitamin D levels with the STOP-Bang score, parameters, demographics, comorbid diseases, and lifestyle characteristics in an elderly Asian population. Our study revealed an association between lower vitamin D levels and greater neck circumference. Moreover, participants with more daytime tiredness and higher BMIs had lower vitamin D levels than did the matched group.
While prior studies have described overlapping risk factors between OSA and vitamin D deficiency, our study is among the first to systematically evaluate whether individual components of the STOP-Bang questionnaire—originally designed for OSA risk stratification—may also serve as potential screening markers for vitamin D deficiency in an elderly Asian population.5 Although the STOP-Bang questionnaire has been widely used to assess OSA risk, its role in identifying individuals with vitamin D deficiency has not been well explored. After further scrutinizing each STOP-Bang parameter, we found that among patients with vitamin D deficiency, those with larger neck circumferences represented a significantly greater proportion, this parameter may warrant further attention as a potential clinical clue for vitamin D deficiency.
Evidence has indicated that low 25(OH)D concentrations may be a marker of greater BMI and neck circumference.11 Previous research indicated that increased adiposity can lead to the sequestration of vitamin D in adipose tissue, thereby reducing its bioavailability. This process may result in lower circulating levels of vitamin D in individuals with higher BMI.29 Although no studies have identified a direct mechanism linking vitamin D deficiency to a larger neck circumference, the strong correlation between neck circumference and BMI suggests that this association may be driven by adipose-related mechanisms.30 Several previous studies have revealed that neck circumference is a risk factor for severe OSA, as it is significantly greater in patients with severe OSA than in those with non-severe OSA.18 Elevated neck circumference in patients with OSA may be associated with physical inactivity, aerobic capacity, and the accumulation of excess body fluid.26
Although our study revealed no statistically significant correlation between neck circumference and 25(OH)D levels, this could be due to the presence of confounding variables such as dietary fat intake, obesity, cardiovascular diseases and metabolic diseases.31–36 These factors can influence both neck circumference and vitamin D levels independently, potentially masking any direct relationship between the two variables, which was not further investigated in this research. For example, studies have shown that consuming vitamin D with a high-fat meal increases its absorption, leading to higher serum 25(OH)D levels.37 However, this study did not further investigate these potential confounding factors.37 In summary, a potential relationship between vitamin D levels and neck circumference could be inferred. A multicenter cohort study also supported this inference.11 Among those with lower 25(OH)D levels, the association between lower serum 25(OH)D levels and greater odds of sleep apnea can be explained by a larger neck circumference.11,32
Our results also demonstrated that individuals with more daytime tiredness presented lower serum vitamin D levels than did the other group, which is consistent with previous reports linking vitamin D deficiency to symptoms such as fatigue and sleepiness.38 However, excessive daytime sleepiness is not universally present in patients with OSA, particularly among the elderly, and its presence alone may not reliably indicate OSA status.39 Furthermore, although serum vitamin D concentrations are known to decrease during winter months, there is no evidence that OSA incidence or severity follows a seasonal pattern. This is likely because OSA is a multifactorial condition influenced by a combination of anatomical, neuromuscular, metabolic, and lifestyle-related factors, with vitamin D deficiency being only one of many contributors.11,13,17,40 Therefore, while low vitamin D levels may be associated with fatigue—a symptom that overlaps with OSA—it is unlikely that seasonal variation in vitamin D contributes directly to OSA pathogenesis. Given the multifactorial nature of both conditions, and the observational design of our study, our findings should be interpreted as correlational rather than causal. Nevertheless, several plausible mechanisms have been proposed to explain how vitamin D deficiency might contribute to OSA development, including impaired pharyngeal muscle function, increased upper airway collapsibility, and systemic inflammation. Conversely, OSA may predispose individuals to vitamin D deficiency due to factors such as obesity, physical inactivity, and reduced sunlight exposure. This underscores the importance of considering the bidirectional nature of the relationship between vitamin D and OSA, and further studies are required to clarify the underlying mechanisms.6
In our study, we found a significant inverse correlation between BMI and vitamin D levels. In addition, those with a BMI over 35 kg/m2 seemed to have lower vitamin D levels on average, although the difference was not statistically significant. Earlier research suggested that obesity increases the risk of vitamin D deficiency due to the greater amount of subcutaneous fat in obese individuals, which inhibits the release of 25(OH)D from the skin into the circulation.11 On the other hand, individuals with obesity are prone to reduced outdoor or physical activity, which limits their sun exposure and leads to lower concentrations of 25(OH)D.2,41 Furthermore, both obese OSA patients and overweight OSA patients had low 25(OH)D levels, indicating that the interaction between BMI and OSA status influences vitamin D levels.2
The subgroup analysis revealed that BMI was significantly correlated with vitamin D levels in females but not in males. This discrepancy may be attributed to differences in body fat distribution and vitamin D metabolism between sexes. Females generally have a higher proportion of body fat and greater subcutaneous adipose tissue, which serves as a storage site for vitamin D, leading to increased sequestration and reduced bioavailability.42,43 Accordingly, while evaluating the relationship between BMI and vitamin D status in elderly populations, sex-specific factors should be considered. Besides, the larger female sample size may have provided greater statistical power to identify significant associations, so future studies with more balanced male-to-female ratios are needed to confirm whether these associations persist in a more evenly distributed.
Vitamin D deficiency is highly prevalent among the elderly and has been associated with multiple systemic health consequences, including osteoporosis, sarcopenia, immune dysregulation, cardiovascular diseases, and cognitive impairment.44 Given the observed associations between vitamin D deficiency and certain STOP-Bang parameters, including a larger neck circumference, higher BMI, and increased daytime sleepiness, screening for vitamin D deficiency in high-risk elderly individuals may be beneficial to enable timely interventions and preventive measures against vitamin D deficiency and its associated consequences. This aligns with recommendations by Schiza et al advocating for timely recognition and management of vitamin D deficiency in populations at risk for OSA.6 While some studies revealed a potential link between vitamin D supplementation and improvements in inflammatory status and metabolic parameters, the direct impact of vitamin D supplementation on OSA outcomes remains inconclusive.12,13,17 Accordingly, future randomized controlled trials are required to determine its potential therapeutic role in OSA management.
There are several limitations in our study. In the initial investigation, our focus was on exploring the relationship between OSA and vitamin D levels. Despite observing a discernible trend, the results did not reach statistical significance when the vitamin D levels were compared with the OSA diagnostic surrogate, the STOP-Bang questionnaire. Although we adjusted for major confounders, factors such as dietary vitamin D intake, sun exposure, and physical activity were not included in the analysis. However, the elderly participants in our study all led an urban lifestyle and lived in the same area, resulting in similar sunlight exposure times, with only subtle differences. In addition, our study population is focused on elderly individuals, so the majority of participants are older people. Besides, due to the initial exclusion of participants with severe organ abnormalities, the proportions of fatigue and witnessed apnea were low. Although the STOP-Bang score is a reliable instrument, its self-assessment character represents one of the most important limitations of this study. Furthermore, although the STOP-Bang Questionnaire is very sensitive for detecting OSA in obese patients, its specificity is low (7%–28%), resulting in high false-positive rates.21 Addition of the Modified Mallampati score to the STOP-BANG Questionnaire may improve specificity without sacrificing sensitivity, yielding better identification rates for OSA.45 Additionally, other sleep disorders, such as circadian rhythm disorders, periodic limb movement disorders, and insomnia, were not assessed in this study. In subsequent studies, the use of polysomnography, which is the gold standard technique in the diagnosis of OSA, is strongly recommended. Future research should include longitudinal or interventional studies to validate the relationship between OSA and vitamin D levels, explore potential causal links, examine a broader range of comorbid sleep disorders in greater detail, and adjustments for potential confounders such dietary habits and physical activity levels to provide a more comprehensive understanding of the relationship between vitamin D deficiency and STOP-Bang parameters.6,46
Conclusions
In conclusion, this is the first study to specifically examine the connection between STOP-Bang parameters and vitamin D deficiency in an elderly Asian population. A potential relationship between vitamin D levels and neck circumference could be inferred, and a significant inverse correlation between BMI and vitamin D levels was noted. We suggest being aware of the possibility for vitamin D deficiency among OSA patients with several risk factors identified with the STOP-Bang parameters, such as a larger neck circumference, higher BMI levels, and increased daytime sleepiness. Screening for vitamin D deficiency in elderly individuals with these parameters may help identify those at risk for sleep-related disorders, validating further clinical assessment. Further research should investigate the causal relationship between vitamin D deficiency and OSA risk in elderly populations.
Data Sharing Statement
All data included in this study are available from the corresponding author, Dr. Li-Pang Chuang, upon reasonable request.
Ethics Approval and Informed Consent
The questionnaire and methodology for this study was approved by the Institutional Review Board of Chang Gung Memorial Hospital (IRB No. 2306300083). Informed consent was obtained from all individual participants included in the study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
All necessary permissions and licenses for the use of the STOP-Bang questionnaire, MMSE, and GDS were obtained as per institutional and publisher guidelines.
Consent for Publication
Patients signed informed consent regarding publishing their data.
Acknowledgment
We sincerely acknowledge role of Professor Shwu-Hua Lee as one of the project leaders. All administrative processes related to the study, were conducted under her name. Although Professor Lee is not listed as an author of this paper, her involvement in these procedures was essential for the completion of the study. The abstract of this paper was presented at the 22nd Annual Meeting of Taiwan Society of Sleep Medicine as an oral presentation with interim findings. The poster’s abstract was published in page 111 in manual of 22nd Annual Meeting of Taiwan Society of Sleep Medicine.
Author Contributions
W.J.C- Conceptualization, Writing – Original Draft, Supervision. T.W.L- Conceptualization, Writing – Review & Editing. J.T.F- Conceptualization, Methodology, Supervision, Writing – Review & Editing. W.S.H- Conceptualization, Methodology, Writing – Review & Editing. P.H.T- Data Curation, Investigation, Writing – Review & Editing. S.W.L- Data Curation, Investigation, Resources, Writing – Review & Editing. H.C.H- Data Curation, Investigation, Resources, Writing – Review & Editing. N.H.C- Data Curation, Investigation, Resources, Writing – Review & Editing. Y.A.C- Formal Analysis, Writing – Original Draft, Visualization. L.P.C- Formal Analysis, Writing – Original Draft, Supervision, Funding acquisition, Project administration. All authors agreed on the journal to which the article will be submitted, reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage, and agreed to take responsibility and be accountable for the contents of the article.
Funding
This study was supported by the Chang Gung Memorial Hospital [Grant CMRPG390391, CMRPD190341], grant XMRPG3L102, and sponsored by Wang Chang Gung Charity Trust. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the paper.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liguori C, Romigi A, Izzi F. et al. Continuous Positive Airway Pressure Treatment Increases Serum Vitamin D Levels in Male Patients with Obstructive Sleep Apnea. J Clin Sleep Med. 2015;11(06):603–607. doi:10.5664/jcsm.4766
2. Li X, He J, Yun J. The association between serum vitamin D and obstructive sleep apnea: an updated meta-analysis. Respir Res. 2020;21(1):294. doi:10.1186/s12931-020-01554-2
3. Beydoun MA, Ng AE, Fanelli-Kuczmarski MT, et al. Vitamin D status and its longitudinal association with changes in patterns of sleep among middle-aged urban adults. J Affect Disord. 2021;282:858–868. doi:10.1016/j.jad.2020.12.145
4. Gao Q, Kou T, Zhuang B, et al. The Association between Vitamin D Deficiency and Sleep Disorders: a Systematic Review and Meta-Analysis. Nutrients. 2018;10(10):1395. doi:10.3390/nu10101395
5. Piovezan RD, Hirotsu C, Feres MC, et al. Obstructive sleep apnea and objective short sleep duration are independently associated with the risk of serum vitamin D deficiency. PLoS One. 2017; 12:e0180901.
6. Schiza S, Bouloukaki I, Kaditis A, Lombardi C, Bonsignore MR. Vitamin D deficiency: a forgotten aspect in sleep disorders? A critical update. Sleep Med. 2024;121:77–84.
7. Salepci B, Caglayan B, Nahid P, et al. Vitamin D Deficiency in Patients Referred for Evaluation of Obstructive Sleep Apnea. J Clin Sleep Med. 2017;13(04):607–612. doi:10.5664/jcsm.6554
8. Neighbors CLP, Noller MW, Song SA, et al. Vitamin D and obstructive sleep apnea: a systematic review and meta-analysis. Sleep Med. 2018;43:100–108. doi:10.1016/j.sleep.2017.10.016
9. Dzik KP, Kaczor JJ. Mechanisms of vitamin D on skeletal muscle function: oxidative stress, energy metabolism and anabolic state. Eur J Appl Physiol. 2019;119:825–839. doi:10.1007/s00421-019-04104-x
10. Dempsey JA, Veasey SC, Morgan BJ, O’Donnell CP. Pathophysiology of sleep apnea. Physiol Rev. 2010;90(1):47–112. doi:10.1152/physrev.00043.2008
11. Goswami U, Ensrud KE, Paudel ML, et al. Vitamin D Concentrations and Obstructive Sleep Apnea in a Multicenter Cohort of Older Males. Ann Am Thorac Soc. 2016;13(5):712–718. doi:10.1513/AnnalsATS.201507-440OC
12. Ayyildiz F, Yildiran H, Afandiyeva N, Gulbahar Ö, Kokturk O. The effects of vitamin D supplemantation on prognosis in patients with mildobstructive sleep apnea syndrome. Turk J Med Sci. 2021;51(5):2524–2533. doi:10.3906/sag-2101-83
13. Kerley CP, Hutchinson K, Bolger K, et al. Serum Vitamin D Is Significantly Inversely Associated with Disease Severity in Caucasian Adults with Obstructive Sleep Apnea Syndrome. Sleep. 2016;39(2):293–300. doi:10.5665/sleep.5430
14. Liu X, Ke L, Ho J, et al. Sleep duration is associated with vitamin D deficiency in older women living in Macao, China: a pilot cross-sectional study. PLoS One. 2020;15(3):e0229642. doi:10.1371/journal.pone.0229642
15. Eckert DJ, White DP, Jordan AS, Malhotra A, Wellman A. Defining phenotypic causes of obstructive sleep apnea. Identification of novel therapeutic targets. Am J Respir Crit Care Med. 2013;188(8):996–1004. doi:10.1164/rccm.201303-0448OC
16. Hong SO, Chen YF, Jung J, Kwon YD, Liu SYC. Hypoglossal nerve stimulation for treatment of obstructive sleep apnea (OSA): a primer for oral and maxillofacial surgeons. Maxillofac Plast Reconstr Surg. 2017;39:27. doi:10.1016/j.clnu.2018.08.039
17. Kerley CP, Hutchinson K, Bramham J, et al. Vitamin D Improves Selected Metabolic Parameters but Not Neuropsychological or Quality of Life Indices in OSA: a Pilot Study. J Clin Sleep Med. 2017;13(01):19–26. doi:10.5664/jcsm.6378
18. Yenigün M, et al. Neck circumference. metabolic syndrome and obstructive sleep apnea syndrome; Evaluation of possible linkage. Med Sci Monit. 2013;19:111–117. doi:10.12659/MSM.883776
19. Chen L, Pivetta B, Nagappa M, et al. Validation of the STOP-Bang questionnaire for screening of obstructive sleep apnea in the general population and commercial drivers: a systematic review and meta-analysis. Sleep Breath. 2021;25:1741–1751. doi:10.1007/s11325-021-02299-y
20. Hung C-J, Kang B-H, Lin Y-S, Su -H-H. Comparison of a home sleep test with in-laboratory polysomnography in the diagnosis of obstructive sleep apnea syndrome. J Chin Med Assoc. 2022;85(7):788–792. doi:10.1097/JCMA.0000000000000741
21. Chung F, Abdullah HR, Liao P. STOP-Bang Questionnaire: a Practical Approach to Screen for Obstructive Sleep Apnea. Chest. 2016;149(3):631–638. doi:10.1378/chest.15-0903
22. Saarnio E, Pekkinen M, Itkonen ST, et al. Low free 25-hydroxyvitamin D and high vitamin D binding protein and parathyroid hormone in obese Caucasians. A complex association with bone? PLoS One. 2018;13(2):e0192596. doi:10.1371/journal.pone.0192596
23. Kumaratne M, Early G, Cisneros J. Vitamin D Deficiency and Association With Body Mass Index and Lipid Levels in Hispanic American Adolescents. Global Pediatric Health. 2017;4:2333794x17744141. doi:10.1177/2333794X17744141
24. Bijl D, Van Marwijk H, Ader H, Beekman A, Haan M. Test-Characteristics of the GDS-15 in Screening for Major Depression in Elderly Patients in General Practice. Clinical Gerontologist. 2005;29:1–9. doi:10.1300/J018v29n01_01
25. Duarte RLM, Fonseca LBM, Magalhães-da-silveira FJ, Silveira EAD, Rabahi MF. Validation of the STOP-Bang questionnaire as a means of screening for obstructive sleep apnea in adults in Brazil. J Bras Pneumol. 2017;43:456–463. doi:10.1590/s1806-37562017000000139
26. Pangerc A, Petek Ster M, Dolenc Groselj L. Validation of the Slovene Version of the Stop-Bang Questionnaire in a Primary Practice Setting. Zdr Varst. 2024;63:14–20. doi:10.2478/sjph-2024-0003
27. Chung F, Subramanyam R, Liao P, et al. High STOP-Bang score indicates a high probability of obstructive sleep apnoea. Br J Anaesth. 2012;108(5):768–775. doi:10.1093/bja/aes022
28. Slinker BK, Glantz SA. Multiple linear regression: accounting for multiple simultaneous determinants of a continuous dependent variable. Circulation. 2008;117(13):1732–1737. doi:10.1161/CIRCULATIONAHA.106.654376
29. Iftikhar M, Shah N, Khan I, Shah MM, Saleem MN. Association Between Body Mass Index (BMI), Vitamin D, and Testosterone Levels. Cureus. 2024;16(10):e71509. doi:10.7759/cureus.71509
30. Alfadhli EM, Sandokji AA, Zahid BN, et al. Neck circumference as a marker of obesity and a predictor of cardiometabolic risk among Saudi subjects. Saudi Med J. 2017;38(12):1219–1223. doi:10.15537/smj.2017.12.20926
31. McLarnon A. Dietary fat might influence serum vitamin D level. Nat Rev Endocrinol. 2011;7(10):562. doi:10.1038/nrendo.2011.150
32. Fu J, Han L, Zhao Y, et al. Vitamin D levels are associated with metabolic syndrome in adolescents and young adults: the BCAMS study. Clin Nutr. 2019;38:2161–2167.
33. Zhang Y, Wu H, Xu Y, et al. The correlation between neck circumference and risk factors in patients with hypertension: what matters. Medicine (Baltimore). 2020;99(47):e22998. doi:10.1097/MD.0000000000022998
34. Al-Oanzi ZH, Alenazy FO, Alhassan HH, et al. The Role of Vitamin D in Reducing the Risk of Metabolic Disturbances That Cause Cardiovascular Diseases. J Cardiovasc Dev Dis. 2023;10. doi:10.3390/jcdd10050209
35. He Y, Chen J, Cao J, et al. Neck Circumference is Associated with Metabolic Syndrome Components in Chinese Subjects with Type 2 Diabetes. Diabetes Metab Syndr Obes. 2022;15:2781–2787. doi:10.2147/DMSO.S379221
36. Mozafarinia M, Heidari-Beni M, Abbasi B, Kelishadi R. Association between dietary fat quality indices with anthropometric measurements in children and adolescents. BMC Pediatr. 2022;22(1):244. doi:10.1186/s12887-022-03307-0
37. Dawson-Hughes B, Harris SS, Lichtenstein AH, et al. Dietary fat increases vitamin D-3 absorption. J Acad Nutr Diet. 2015;115(2):225–230. doi:10.1016/j.jand.2014.09.014
38. Siarnik P, Jurik M, Hardonova M, et al. Excessive daytime sleepiness in sleep apnea: any role of testosterone or vitamin D? Physiol Res. 2020;63:907–917. doi:10.33549/physiolres.934507
39. Sunwoo BY, Kaufmann CN, Murez A, et al. The language of sleepiness in obstructive sleep apnea beyond the Epworth. Sleep and Breathing. 2023;27(3):1057–1065. doi:10.1007/s11325-022-02703-1
40. Itoh H, Mori I, Matsumoto Y, Maki S, Ogawa Y. Vitamin D deficiency and seasonal and inter-day variation in circulating 25-hydroxyvitamin D and parathyroid hormone levels in indoor daytime workers: a longitudinal study. Ind Health. 2011;49(4):475–481. doi:10.2486/indhealth.MS1255
41. Parikh SJ, Edelman M, Uwaifo GI, et al. The relationship between obesity and serum 1,25-dihydroxy vitamin D concentrations in healthy adults. J Clin Endocrinol Metab. 2004;89:1196–1199. doi:10.1210/jc.2003-031398
42. Muscogiuri G, Barrea L, Somma CD, et al. Sex Differences of Vitamin D Status across BMI Classes: an Observational Prospective Cohort Study. Nutrients. 2019;11(12):3034. doi:10.3390/nu11123034
43. Huang H, Guo J, Chen Q, et al. The synergistic effects of vitamin D and estradiol deficiency on metabolic syndrome in Chinese postmenopausal women. Menopause. 2019;26(10):1171–1177. doi:10.1097/GME.0000000000001370
44. Holick MF. The vitamin D deficiency pandemic: approaches for diagnosis, treatment and prevention. Rev Endocr Metab Disord. 2017;18(2):153–165. doi:10.1007/s11154-017-9424-1
45. Avincsal MO, Dinc ME, Ulusoy S, et al. Modified Mallampati Score Improves Specificity of STOP-BANG Questionnaire for Obstructive Sleep Apnea. J Craniofac Surg. 2017;28(4):904–908. doi:10.1097/SCS.0000000000003513
46. Laratta CR, Ayas NT, Povitz M, Pendharkar SR. Diagnosis and treatment of obstructive sleep apnea in adults. Cmaj. 2017;189(48):E1481–e1488. doi:10.1503/cmaj.170296
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.