Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 14
A Prospective, Observational Registry Study to Evaluate Effectiveness and Safety of Hyaluronic Acid-Based Dermal Fillers in Routine Practice: Interim Analysis Results with One Year of Subject Follow-Up
Authors Bhojani-Lynch T ![]() , Deckers A, Ohanes O, Poupard K, Maffert P
, Deckers A, Ohanes O, Poupard K, Maffert P
Received 14 July 2021
Accepted for publication 26 October 2021
Published 16 November 2021 Volume 2021:14 Pages 1685—1695
DOI https://doi.org/10.2147/CCID.S329415
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Tahera Bhojani-Lynch,1 Anne Deckers,2 Ohan Ohanes,3 Kevin Poupard,4 Pauline Maffert4
1The Laser and Light Clinic, Loughborough, UK; 2Centre Médical Esthétique Eureka, Dalhem, Belgium; 3Swiss Care Cosmetic & Laser Clinic, London, UK; 4Clinical Development Department, Teoxane S.A., Geneva, Switzerland
Correspondence: Pauline Maffert
Teoxane S.A., Rue de Lyon 105, Geneva, 1203, Switzerland
Tel +41 22 344 96 36
Email [email protected]
Background: Monitoring the effectiveness, safety and emerging uses of hyaluronic acid (HA) fillers in their wide range of indications requires a holistic approach.
Purpose: To propose an observational study design aiming to gather real-world evidence (RWE) and continuously evaluate the performance and safety of marketed devices in routine practice.
Materials and Methods: A prospective, observational registry was initiated at six European sites. Investigators enrolled any subject receiving at least one injection with a target study device (TEOSYAL Deep Lines [HADL] and/or Global Action [HAGA]). They followed their routine practice regarding injection technique, volume, and subject follow-up. Effectiveness was evaluated at 3 months using the global aesthetic improvement scale (GAIS). Safety was assessed based on common treatment reactions (CTR) and adverse events (AE).
Results: High quantity of RWE was collected following the initiation of this registry. In the first 158 subjects enrolled, 1220 injections were performed in more than 25 indications, including 679 with the target devices and 271 with devices of the same filler line. The primary objective was achieved, with 93.9% of treatments providing improvement at Month 3 according to the PI and subject. Post-injection CTR were mild to moderate and short-lived, and there was no clinically significant AE. More than 76% of treatments still provided some visible effect at month 12.
Conclusion: Based on RWE, HADL and HAGL are effective and safe in their respective indications mostly distributed in the midface, perioral region, and lower face. Observational registries are a valuable asset in the context of post-market clinical follow-up.
Keywords: aesthetic, facial rejuvenation, nonsurgical, real-world evidence, registry
Introduction
Dermal filler injections are now routinely performed in aesthetic and dermatological clinics worldwide.1,2 Soft-tissue fillers have been employed in an increasingly wider range of indications,3,4 with hyaluronic acid (HA) now superseding other permanent (poly-methyl methacrylate) and nonpermanent filler materials (autologous fat, Poly-L-Lactic Acid (PLLA), Calcium Hydroxyapatite, collagen) due to its potential reversibility and remarkable biocompatibility.3
HA is a naturally occurring glycosaminoglycan, particularly concentrated in the soft connective tissue extracellular matrix, skin dermis, vitreous of the eye, hyaline cartilage, synovial joint fluid, disc nucleus, and umbilical cord.3,5 It has been widely used in various dermatological applications, either as a space filler due to its intrinsic hydrating properties, or as a scaffold for tissue engineering. In vivo, endogenous HA is known to be implicated in several physiological processes including wound healing, inflammation, and angiogenesis regulation.5–7 High Molecular Weight HA (HMWHA) has a well-documented anti-inflammatory potential, and may also exhibit antioxidant effects.7,8
As HA alone is quickly degraded by endogenous hyaluronidase and other tissue factors such as oxidative and mechanical stress, most dermal filler formulations use chemically cross-linked HA to improve persistence of the implanted gel in vivo. Albeit chemically modified, HA fillers can be promptly degraded upon injection of high-dose hyaluronidase, which represents a key advantage of HA over other injectable materials from a safety perspective, especially to manage serious adverse events such as vascular compromise.9,10
Additionally, the degree of HA modification, and the crosslinking technology used, can both impact the rheological properties of the final product, allowing to fine tune its strength and malleability.11 As a result, multiple filler formulations, rheologically adapted to specific treatment areas and patient needs, have emerged over the past two decades.3,12
On the other hand, with the growing popularity of dermal filling procedures, HA products which have been on the market for more than a decade, may be routinely injected in a range of face and neck areas, extending beyond their original intended use. Specific indications come with tailored injection techniques, product volumes and depths, as these variations are related to both the treated area and desired outcome.13,14 Furthermore, some beautification procedures which are not exclusively related to aging – such as lip augmentation – concern a wider (eg, younger) patient population than the one targeted by rejuvenating procedures.15 Each filler use may therefore have its own safety and efficacy profile, with peculiarities regarding the nature, rate and duration of side effects, or the degree and durability of aesthetic improvement.
Pre-market clinical trials are usually designed to show effects of a single filler for a given indication, based on standardized treatment protocols.16,17 Once on the market and routinely used by health-care practitioners, the product may end up being injected in diverse locations, with more variable indications and techniques than those evaluated through clinical investigations.18 Therefore, specific post-market study designs are needed to collect clinical evidence supporting routine practice.
This publication proposes a specific observational study design, well suited for post-market clinical follow-up programs, which was adopted to evaluate the effectiveness and safety of a whole range of fillers in routine practice. Preliminary results of one of these observational registries confirm the potential of such study to generate high quantity and diverse data, thereby gaining insight on the day-to-day use of HA fillers within variable treatment plans.
The investigational devices for this study, the TEOSYAL® products, are HA fillers intended to cover a wide range of clinical indications, from skin quality treatments to volumizing injections. The product line includes formulations with different HA concentrations, degrees of modification and rheological behaviors, with and without integrated lidocaine. Several published clinical trials have demonstrated the safety and tolerability of the range and have established the clinical effectiveness of specific formulations for various indications.16,17,19–22
Objective
To report preliminary results of the GRADUAL study, designed to assess the performance, safety, and routine use of two target products (TEOSYAL Deep Lines (HADL) and Global Action (HAGA)). Evaluation of routine practice, injection technique, and associated safety profile of other TEOSYAL fillers injected at study visits was also evaluated.
Materials and Methods
Study Design and Population
This was a prospective, multicenter, observational registry conducted as part of a post-market clinical follow-up program. The objective was to assess the effectiveness of HAGA and HADL, and to confirm the safety of all TEOSYAL devices injected in the study, for aesthetic treatments, as per routine practice.
The study was conducted in accordance with the International Conference on Harmonization (ICH), Good Clinical Practice guidelines, and the Declaration of Helsinki. Subjects were enrolled at six investigational sites located in the UK, Belgium and Romania. Ethics committee approval was obtained as required by local regulations. In the UK, the study was deemed a non-interventional registry falling outside the remit of GAfREC (Governance Arrangement for Research Ethics Committees) as confirmed by the Competent Authority (MHRA). In Belgium, the clinical study was approved by the Ethics Committee of CHU – Liège. For the three sites which were initiated in Romania in 2020, ethical approval was granted by the Comisia Națională de Bioetică a Medicamentului și a Dispozitivelor Medicale. Given their later initiation, data from these three sites was not included in this interim analysis.
The target population for inclusion was of patients over 18 years of age, having signed an informed consent and willing to undergo aesthetic procedure(s) using dermal fillers. Subjects having received prior dermal filler injections in the six months preceding the study, and/or presenting any contraindication as per the instructions for use of the devices, were excluded from participation.
Study Devices and Treatment Protocol
The study devices assessed for safety and routine practice included all HA fillers of the TEOSYAL product line, injected by the investigator at study visits.
All TEOSYAL products incorporate high molecular weight hyaluronic acid, either non-crosslinked or chemically crosslinked with 1,4 – butanediol diglycidyl ether (BDDE), in a physiological buffer (pH 7.3). The HA concentration in the final products varies from 15 mg/mL to 25 mg/mL throughout the range, with reticulation degrees ranging between 0% and 9%.
In this study, the two target products – used for at least one injection site per subject – were Global Action (HAGA) and Deep Lines (HADL). HAGA and HADL are formulated with 25 mg/mL high molecular weight (exceeding 1 MDa) crosslinked hyaluronic acid, available with or without 0.3% of lidocaine. HADL is slightly more crosslinked than HAGA, resulting in a HA Modification Degree of about 8% versus 7%. Both HADL and HAGA were purchased by the study investigators as 1 mL pre-filled syringes supplied with 27G ½” and 30G ½” needles, respectively. However, the use of other needles or cannulas was authorized by the study protocol.
All principal investigators (PI) treated the subjects according to their usual practice, selecting their usual product to treat any indication using an appropriate technique, volume and depth, at their own discretion. To be included in the study, subjects had to be treated at least once with either HAGA or HADL. The study protocol included an initial visit (D0) and follow-up visits at 3, 6, 9 and 12 months, which were optional as per the observational study design. Additional visits were allowed at any time throughout the follow-up period. Each visit included efficacy and satisfaction assessments for all indications initially treated with HAGA and/or HADL, safety assessments for all treatments performed during any study visit, and could include any type of additional injection: touch-up or retreatment of a previously treated indication, or initial injection in a new area (Figure 1). All new injections could be performed using HAGA, HADL, or any other TEOSYAL/non TEOSYAL device. An optional smartphone application was proposed to allow close monitoring of subject safety and enhance overall data collection, as well as to motivate subjects’ adherence to the study.
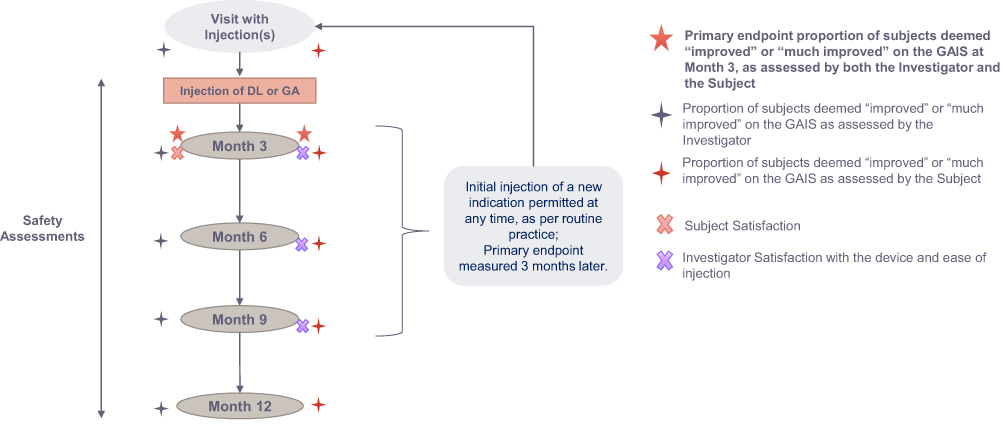 |
Figure 1 Study schematics. |
Study Endpoints and Variables
Study endpoints and variables are outlined in Figure 2.
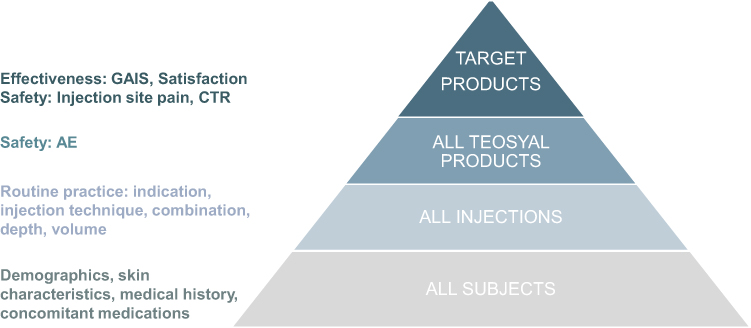 |
Figure 2 Clinical data collected per injection type. |
Global Aesthetic Improvement Scale (GAIS)
Treatment effectiveness was evaluated based on the GAIS, a 5-point scale to grade post-injection appearance from “much improved” to “much worse”. The degree of improvement with reference to the pre-injection level was assessed independently by both subject and PI, post-injection and at Month 3, 6, 9 and 12, for each indication initially injected with GA or DL.
Satisfaction
Patients were asked to rate their level of satisfaction on a 5-point balanced scoring system ranging from “very satisfied” to “very dissatisfied” at Month 3 after initial injection with GA or DL. They were also asked to select the word which best reflected their treatment outcome, from three suggestions (“natural-looking”, “improved”, “smoothed”).
The injector's satisfaction with the product and ease of injection was recorded after each treatment with GA or DL, using a 2-question survey.
Safety Endpoints
Injection site pain was measured based on subject’s self-assessment on a 100mm Visual Analog Scale (VAS), immediately after injection and at the end of the consultation.
Common Treatment Responses (CTR) were reported by the injector immediately after treatment and/or at follow-up visits, and by the subject using a 30-Day e-Diary. Adverse Events (AE) were monitored throughout the study.
Injection Characteristics
Routine practice was assessed by collecting data from injected products, any combination, injection volume, depth, technique, and type of needle or cannula used to treat every indication, at all study visits.
Study Objectives and Statistical Analysis
The primary objective of the study was to demonstrate efficacy of HAGA and HADL in aesthetic treatments, using the GAIS at Month 3 ± 4 weeks. Efficacy evaluation always considered the first injection in the treated indication as reference point for calculating the 3-month time frame of GAIS assessment, regardless of optional touch-ups and retreatments. Each “indication” referred to a specific aesthetic defect including skin quality issues, facial wrinkles and folds (such as NLFs, marionette lines, oral commissures, perioral rhytids), age-related volume loss or tissue sagging in the face and neck.
To show effectiveness, at least 70% of subjects had to be “improved” or “much improved”, according to both subject and PI. The analysis was performed globally, per product and per product*indication. To compensate for potential missing GAIS data within the required time window, two additional analyses using enlarged window imputations were performed: in case GAIS was missing at Month 3 ± 4 weeks, it was replaced by GAIS collected at [29–153] days. If still missing, the analysis relied on the independent, post-injection GAIS.
Secondary objectives were to assess effectiveness throughout the study using GAIS at Months 6, 9 and 12, to evaluate subject’s and injector’s satisfaction with the device and treatment outcomes, and to confirm desired safety based on the duration, nature, severity and rate of CTR and AE.
All statistical analyses were performed using SAS software version 9.4 (SAS Institute, Inc., Cary, NC).
Results
Subjects Demographics and Follow-Up
Preliminary results of the study were obtained based on clinical data extracted in July 2020, pertaining to 158 subjects enrolled from February to September 2019 at 3 (out of 6) participating sites, including 93 subjects (58.9%) having completed their last follow-up visit, 12 months after inclusion in the study. Most patients were female (96.2%) and Caucasian (89.9%) of lighter skin types (Fitzpatrick II or III, 82.9%). The average age at inclusion was 52.1 ± 10.5 years, and ranged from 21 to 76 (Table 1).
 |
Table 1 Subject Demographics |
Almost all included subjects (155, 98.1%) attended at least one follow-up visit, in average 2.4 ± 2.2 months following their baseline visit, and a significant part of the population (66, 40.7%) came back at least five times throughout the one-year study period. A few subjects (11, 7.0%) attended more than ten, and up to sixteen (1, 0.6%) follow-up visits.
Treatment Exposure
Overall, 1220 injections were performed in less than 18 months, of which 950 (77.9%) were performed with 9 different TEOSYAL products. All were included in the safety analysis (Table 2).
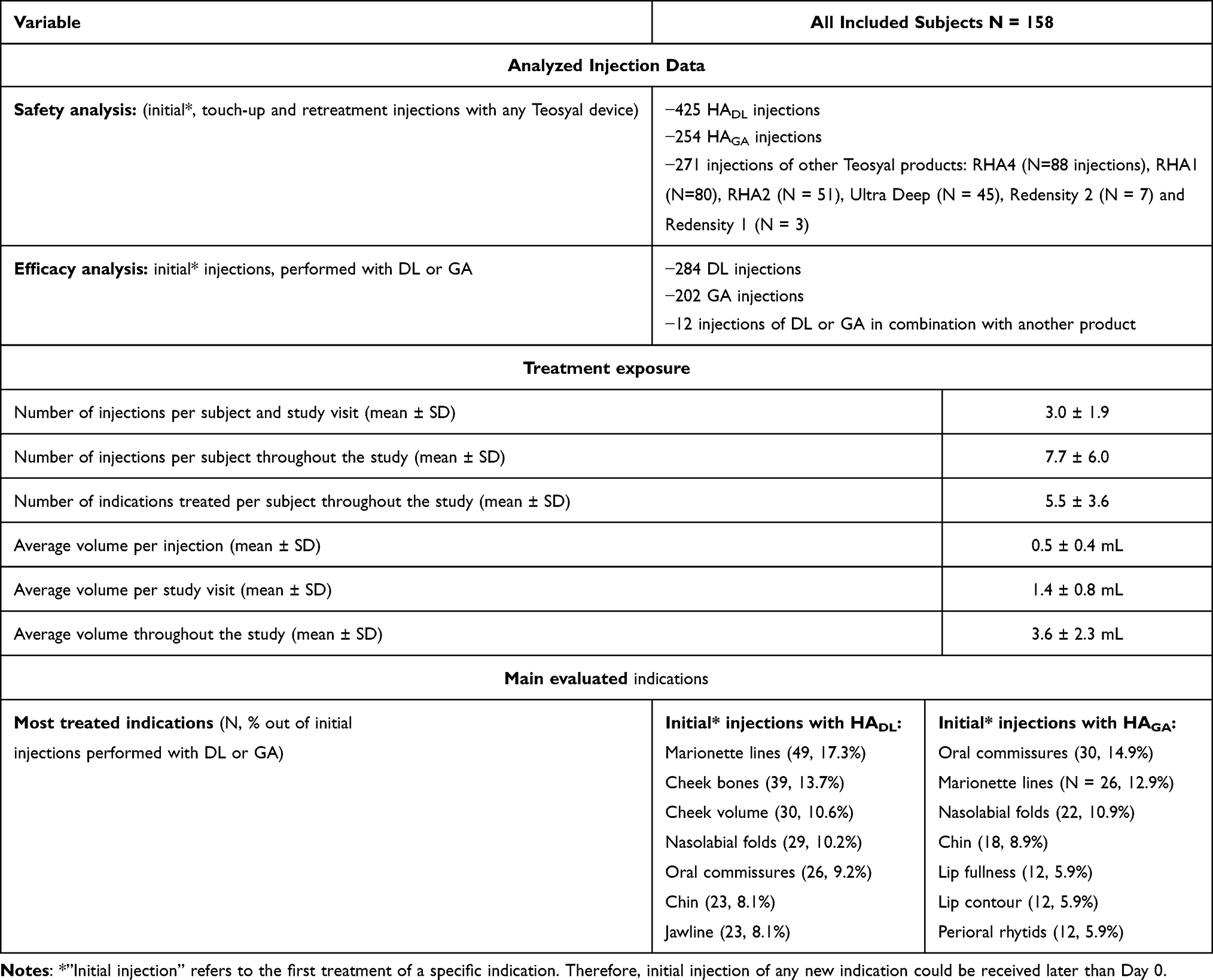 |
Table 2 Treatment Exposure and Injected Indications |
Following routine practice, the two target devices (HAGA and HADL) were respectively injected in 29 and 25 different aesthetic indications which were mostly distributed in the midface (cheeks and nasolabial folds (NLF)), perioral region (marionette lines, oral commissures, lips and vertical perioral rhytids) and lower face (chin and jawline) (Figure 3). Overall, 202 treatments performed with HAGA in 82 subjects and 284 treatments with HADL in 112 subjects, were included in the effectiveness analysis (Table 2). As the injection of new indications was permitted at any time throughout the study, respectively 58 (28.7%) and 98 (34.5%) of all HAGA and HADL injections evaluated for effectiveness had been performed during a follow visit.
 |
Figure 3 Distribution of main product indications based on the proportion of injections performed in each area (%), out of all initial treatments performed with the target study device (HAGA: left, HADL: right). |
On average, each subject received 1.4 ± 0.8 mL of filler per study visit and 3.6 ± 2.3 mL throughout the follow-up, to treat approximately 6 ± 4 indications (up to 15) (Table 2).
Effectiveness
The primary efficacy objective was achieved globally and for each study device taken individually. Indeed, the proportion of improvement was consistently above 93.9% with applying the main analysis timeframe, and above 94% when using an enlarged window imputation. Results of the main and sensitivity analyses were found to overlap as shown by 95% confidence intervals (Figure 4). Furthermore, the proportion of initial treatments that provided an aesthetic improvement according to both PI and subject was consistently high in the sub-analyses per indication, as shown in Table 3 for main injected areas.
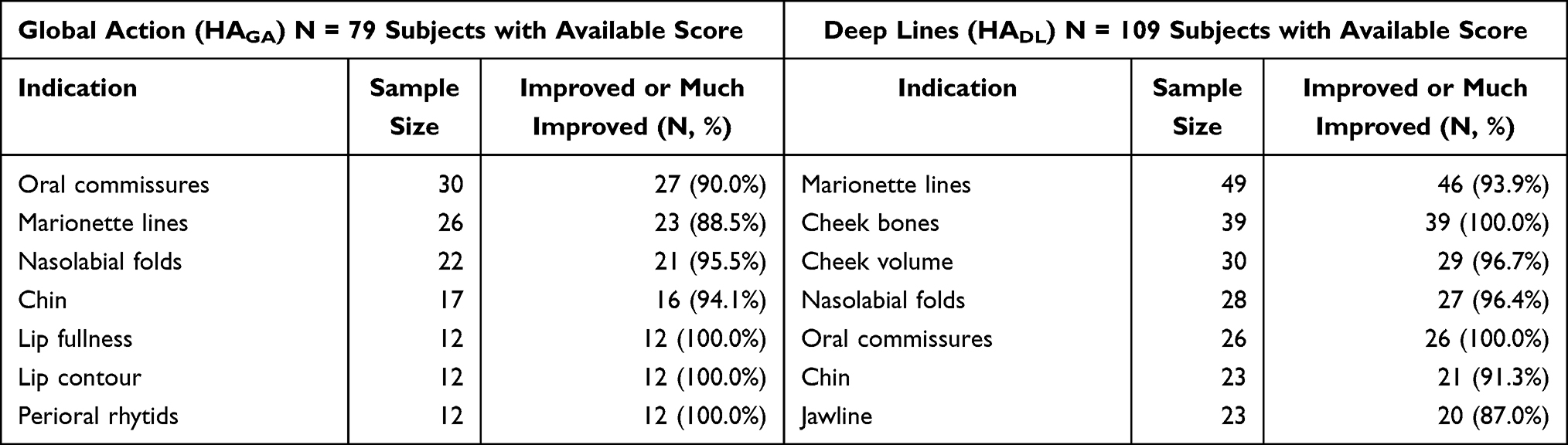 |
Table 3 Primary Efficacy Endpoint by Product and Indication (Sensitivity Analysis). Proportion of “Improved” or “Much Improved” GAIS at Day [29–153] or Post-Injection (PI and Subject Assessment) |
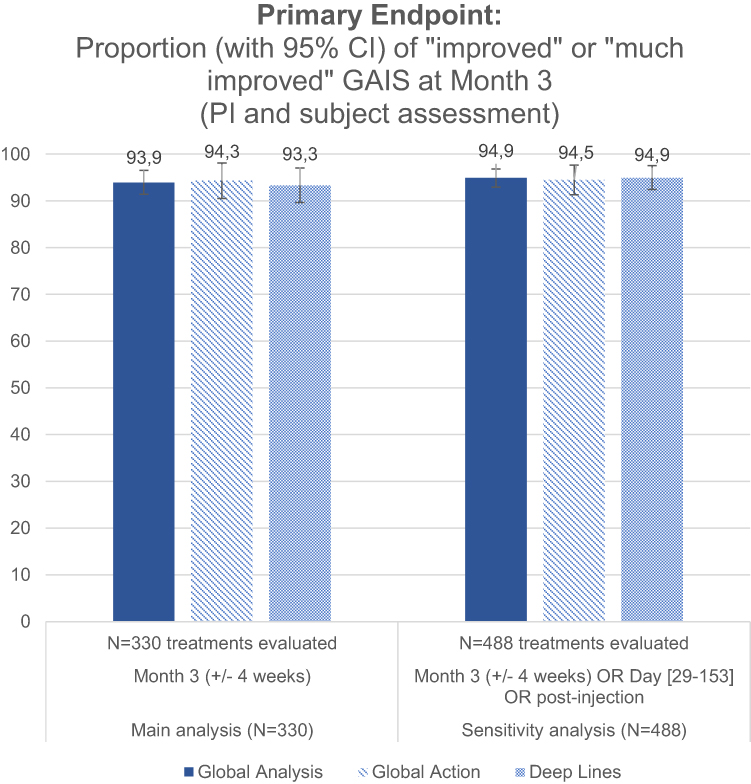 |
Figure 4 Primary efficacy endpoint (main and sensitivity analyses). |
Overall, the proportion of outcomes deemed at least “improved” remained above 93% and 76% up to Month 12, as respectively assessed by the PI and the subject. Secondary effectiveness analyses showed a progressive GAIS decrease over time, with a lesser proportion of treatments recorded as “much improved” with regard to baseline, particularly after Month 6 (Figure 5).
 |
Figure 5 GAIS scores provided by either the PI (A) or the subject (B) throughout the study period, evaluating the aesthetic improvement in the indication, as compared to baseline level. |
Subject satisfaction at Month 3, evaluated on 360 answers pertaining to initial treatments with GA or DL, revealed that 95% of subjects were satisfied to very satisfied with their treatment. In decreasing order, they chose the words “natural-looking” (76.4%), “rejuvenated” (13.1%) and “smoothed” (2.2%) to define the aesthetic outcome.
Analyses of PI satisfaction surveys filled after each injection provided a 99.3% satisfaction rate (684 out of 689 answers). Products were deemed easy to inject in 99.6% of cases (688 out of 691 answers).
Safety
When pooling all TEOSYAL products and indications, injection site pain reported on a 100 mm VAS averaged 21.2 ± 14.6 mm during the injection and decreased to 0.9 ± 4.3 mm at the end of the consultation (ie, 15 to 30 minutes later). Similar scores were obtained when evaluating injection site pain with HADL (21.0 ± 15.1 mm) and HAGA (21.7 ± 13.9 mm) separately.
Immediate CTR reported by the PI after the injection occurred following 29.9% of injections (combining initial, touch-up and repeat treatments), and all were mild or moderate. Of reported rates of CTR within the safety assessment, redness (23.4%), bruising (20.9%) and swelling (17.1%) were the most frequent, whilst tenderness (6.3%), lumps and bumps (6.3%), pain (1.9%), firmness (1.9%), discoloration (1.3%) and itching (0.6%) were less common. Based on 30-day e-Diary entries, subject-reported CTR were similar in nature and severity to PI-reported reactions. No subject reported a persistent CTR after Day 8.
Seven AEs which occurred during the study were deemed definitely (N = 4) or possibly (N = 3) related to the procedure and/or the device and consisted in Tyndall effect (1, 0.6%), product migration and asymmetry in a single subject (each 1, 0.6%), burning (2, 1.3%), slight bump (1, 0.6%) and cold sore (1, 0.6%). None was clinically significant or was deemed as a SAE or UADE.
Discussion
This publication presented preliminary results of the GRADUAL study, belonging to a broader clinical registries program. The observational design of the study allowed systematic collection of RWE on a line of HA fillers approved in the EU for more than fifteen years, for a wide range of aesthetic indications. Moreover, the treatment of new indications at any time throughout the study, combined with a flexible and adaptative clinical database, allowed to collect extensive primary endpoint data (from 488 injections) compared to the population size (158 subjects).
Interim study results confirmed the versatility of the two target devices, which were effective to treat various indications across the midface, perioral area and lower face. Furthermore, collected data confirmed that investigators adopted a global rejuvenation approach, treating an average of 5 indications per subject throughout the follow-up. This suggested that routine practice with HA fillers commonly involves combined treatments of several areas of the face, aiming to provide a harmonious and aesthetically pleasing result. This was also consistent with previous studies showing that patients usually have interest in improving a variety of facial features.23
The heterogeneity in the number of follow-up visits (0 to 16 per subject), some of which included injections in new indications, revealed a highly variable treatment path, as approximately one-third of subjects came back at least once to improve new aesthetic features after having received their original treatment.
Interestingly, despite the simultaneous treatment of several indications, injection volumes were relatively low – averaging 1.4 mL per visit and 3.6 mL throughout the study – as compared to quantities used in “indication-specific” studies: in recent randomized controlled trials (RCT), average injection volumes of 2.7 mL to treat the lips and perioral area, and of 2.2 mL to correct chin retrusion, were reported. Hence, by defocusing the attention from a main defect and adopting a global rejuvenation approach, subject satisfaction was achieved with a limited amount of filler.24,25 The reality of routine practice, where the injector is limited by patient finances, may further explain these small injection volumes.
Treatment was well tolerated, causing mild injection site pain, which promptly improved or disappeared as confirmed by subjects at the end of injection sessions. Side effects were those typically expected following any type of filler injection.26,27 Other than common treatment reactions, few (7) device-related AEs emerged, none of which were clinically significant. The safety of TEOSYAL devices, specifically HADL and HAGA, was thereby confirmed in a large range of aesthetic indications treated, as per routine practice, based on this interim study analysis, providing up to 12-month subject follow-up.
This observational study design, which provides a holistic view of the use of dermal fillers in clinical practice, appears well adapted to continuously assess the performance and safety profile of approved products, and to identify alternative product use through post-market clinical follow-up. While this approach differs from previous observational trials on HA fillers which focused on specific areas or indications,28,29 the special interest of registries is widely exploited in other therapeutic fields. In addition to monitoring treatment efficacy and safety, registries are powerful tools to understand the course of a medical condition, understand variations in procedures and outcomes, and examine factors that influence prognosis and treatment.30,31
There are inherent limitations of this clinical strategy, including a lower evidence level induced by the high variability of evaluated treatments, and potential missing data especially at optional follow-up visits. To overcome these risks, it is essential to plan the interim and final analyses accordingly to guarantee statistical significance of the results. Properly designed registries which collect data in a comprehensive manner can have an important complementary role to RCT in evaluating patient outcomes, and do not systematically overestimate the magnitude of treatment effects.32,33
In this particular registry, the primary objective was first validated based on GAIS assessments performed in the required timeframe (Month 3 ± 4 weeks), allowing evaluation of 330 treatments (performed in 119 subjects). The rate of improvement (93.9%) being well above the requested 70%, the efficacy of treatments performed with HADL and HAGA in routine practice was confirmed.
Extending the analysis timeframe through sensitivity analyses did not significantly affect the responder rate, as 94.9% of the 488 treatments (performed in 158 subjects) evaluated either at [29–153] days post-treatment, or directly post-injection (at D0), were deemed improved by both PI and subject. The chosen approach was thus validated, confirming the relevance of enlarged window imputations to evaluate product efficacy in the context of observational studies.
Both target products were found to be quite versatile in routine practice, as shown by their effectiveness throughout various indications including marionette lines, NLF, oral commissures and chin. Being the stiffest, HADL was also effective in volumizing and contouring injections targeting the cheek and jawline, whereas HAGA appeared well suited for enhancing contour or adding volume to the lips and correcting perioral rhytids.
Interestingly, despite the non-binding follow-up schedule, participating investigators organized end-of-study visits at Month 12 for 86 subjects (54.4%), allowing confirmation of treatment durability based on PI- and/or subject-reported GAIS. According to subject assessments, for 76% of evaluated treatments, some degree of improvement was still visible at twelve months, though progressive product degradation was evidenced by the decreasing proportion of “much improved” results (14.8%) with regard to post-injection levels (55.1%). Subject assessments were generally less favorable than PI evaluations throughout the study, possibly reflecting higher expectations. Overall, a complete loss of effect (represented by the proportion of “no change” answers) was observed in 23.2% and 6.7% of cases at Month 12, as respectively assessed by subject and PI.
Conclusion
An observational design was adopted to monitor the performance and safety of marketed HA fillers in day-to-day clinical practice. Effectiveness, safety and durability of the devices were evidenced based on RWE gathered from 158 subjects injected in more than 25 different indications.
The evaluation of routine practice reveals some differences between “real world” treatment strategy and interventional clinical trials. In this study, most patients were treated in multiple indications, often over several treatment sessions, resulting in global aesthetic improvements with moderate injection volumes. Effectiveness and safety outcomes gathered though pre-market randomized controlled trials are closely related to product quantities, treatment areas and injection techniques dictated by the study protocol. To confirm the favorable benefit/risk profile of a product outside of its restricted intended use, it is reasonable to adopt a global, observational approach to corroborate these findings in a broader diversity of indications.
Data being collected through similar registries, taken individually or pooled in a meta-analysis, may be further sub-analysed, with original approaches to investigate specific areas or indications, product formulations, injection techniques, or patient groups.
Funding
Materials and funding for this study, as well as medical writing assistance, were provided by TEOXANE.
Disclosure
Drs. Bhojani-Lynch, Deckers and Ohanes were clinical investigators for this study and received research grants from TEOXANE for study participation. Mr Kevin Poupard and Ms Pauline Maffert are employees of TEOXANE. The authors report no other conflicts of interest in this work.
References
1. (ASPS) ASoPS. Plastic surgery statistics report 2019; 2020. Available from: https://www.plasticsurgery.org/documents/News/Statistics/2019/plastic-surgery-statistics-full-report-2019.pdf.
2. Monheit GD. Nonsurgical facial rejuvenation. Facial Plas Surg. 2014;30(4):462–467.
3. Fallacara A, Manfredini S, Durini E, Vertuani S. Hyaluronic acid fillers in soft tissue regeneration. Facial Plas Surg. 2017;33(1):87–96.
4. Rzany B, Cartier H, Kestemont P, et al. Full-face rejuvenation using a range of hyaluronic acid fillers: efficacy, safety, and patient satisfaction over 6 months. Dermatol Surg. 2012;38(7 Pt 2):1153–1161.
5. Valachova K, Svik K, Biro C, et al. Impact of ergothioneine, hercynine, and histidine on oxidative degradation of hyaluronan and wound healing. Polymers (Basel). 2020;13(1):95.
6. Zamboni F, Okoroafor C, Ryan MP, et al. On the bacteriostatic activity of hyaluronic acid composite films. Carbohydr Polym. 2021;260:117803.
7. Litwiniuk M, Krejner A, Speyrer MS, Gauto AR, Grzela T. Hyaluronic acid in inflammation and tissue regeneration. Wounds. 2016;28(3):78–88.
8. Gao Y, Sun Y, Yang H, et al. A low molecular weight hyaluronic acid derivative accelerates excisional wound healing by modulating pro-inflammation, promoting epithelialization and neovascularization, and remodeling collagen. Int J Mol Sci. 2019;20:15.
9. Jung H. Hyaluronidase: an overview of its properties, applications, and side effects. Arch Plast Surg. 2020;47(4):297–300.
10. Kwak SS, Yoon KH, Kwon JH, et al. Comparative analysis of hyaluronidase-mediated degradation among seven hyaluronic acid fillers in hairless mice. Clin Cosmet Investig Dermatol. 2021;14:241–248.
11. Edsman K, Nord LI, Ohrlund A, Lärkner H, Kenne AH. Gel properties of hyaluronic acid dermal fillers. Dermatol Surg. 2012;38(7 Pt 2):1170–1179.
12. Bacos JT, Dayan SH. Superficial dermal fillers with hyaluronic acid. Facial Plas Surg. 2019;35(3):219–223.
13. Fitzgerald R, Carqueville J, Yang PT. An approach to structural facial rejuvenation with fillers in women. Int J Womens Dermatol. 2019;5(1):52–67.
14. Uliana SGG. Illustrated Guide to Injectable Fillers: Basics, Indications, Uses. Quintescence Publishing Group; 2016.
15. Stojanovic L, Majdic N. Effectiveness and safety of hyaluronic acid fillers used to enhance overall lip fullness: a systematic review of clinical studies. J Cosmet Dermatol. 2019;18(2):436–443.
16. Kaufman-Janette J, Taylor SC, Cox SE, Weinkle SH, Smith S, Kinney BM. Efficacy and safety of a new resilient hyaluronic acid dermal filler, in the correction of moderate-to-severe nasolabial folds: a 64-week, prospective, multicenter, controlled, randomized, double-blind and within-subject study. J Cosmet Dermatol. 2019;18(5):1244–1253.
17. Monheit G, Kaufman-Janette J, Joseph JH, Shamban A, Dover JS, Smith S. Efficacy and safety of two resilient hyaluronic acid fillers in the treatment of moderate-to-severe nasolabial folds: a 64-week, prospective, multicenter, controlled, randomized, double-blinded, and within-subject study. Dermatol Surg. 2020;46(12):1521–1529.
18. McKee D, Remington K, Swift A, Lambros V, Comstock J, Lalonde D. Effective rejuvenation with hyaluronic acid fillers: current advanced concepts. Plast Reconstr Surg. 2019;143(6):1277e–1289e.
19. Berguiga M, Galatoire O. Tear trough rejuvenation: a safety evaluation of the treatment by a semi-cross-linked hyaluronic acid filler. Orbit (Amsterdam, Netherlands). 2017;36(1):22–26.
20. Galadari H, Mariwalla K, Delobel P, Sanchez-Vizcaino Mengual E. Pain and bruising levels after lip augmentation: a comparison of anterograde and retrograde techniques using an automated motorized injection device. A blinded, prospective, randomized, parallel within-subject trial. Dermatol Surg. 2020;46(3):395–401.
21. Nast A, Reytan N, Hartmann V, et al. Efficacy and durability of two hyaluronic acid-based fillers in the correction of nasolabial folds: results of a prospective, randomized, double-blind, actively controlled clinical pilot study. Dermatol Surg. 2011;37(6):768–775.
22. Rzany B, Converset-Viethel S, Hartmann M, et al. Efficacy and safety of 3 new resilient hyaluronic acid fillers, crosslinked with decreased BDDE, for the treatment of dynamic wrinkles: results of an 18-month, randomized controlled trial versus already available comparators. Dermatol Surg. 2019;45(10):1304–1314.
23. Sobanko JF, Taglienti AJ, Wilson AJ, et al. Motivations for seeking minimally invasive cosmetic procedures in an academic outpatient setting. Aesthet Surg J. 2015;35(8):1014–1020.
24. Beer K, Kaufman-Janette J, Bank D, et al. Safe and effective chin augmentation with the hyaluronic acid injectable filler, VYC-20L. Dermatol Surg. 2021;47(1):80–85.
25. Weiss R, Beer K, Cox SE, et al. A randomized, controlled, evaluator-blinded, multi-center study of hyaluronic acid filler effectiveness and safety in lip fullness augmentation. Dermatol Surg. 2021;47(4):527.
26. Goodman GJ, Liew S, Callan P, Hart S. Facial aesthetic injections in clinical practice: pretreatment and posttreatment consensus recommendations to minimise adverse outcomes. Australas J Dermatol. 2020;61(3):217–225.
27. Ortiz AE, Ahluwalia J, Song SS, Avram MM. Analysis of U.S. food and drug administration data on soft-tissue filler complications. Dermatol Surg. 2020;46(7):958–961.
28. Philipp-Dormston WG, Eccleston D, De Boulle K, Hilton S, van den Elzen H, Nathan M. A prospective, observational study of the volumizing effect of open-label aesthetic use of Juvederm(R) VOLUMA(R) with Lidocaine in mid-face area. J Cosmetic Laser Ther. 2014;16(4):171–179.
29. Philipp-Dormston WG, Hilton S, Nathan M. A prospective, open-label, multicenter, observational, postmarket study of the use of a 15 mg/mL hyaluronic acid dermal filler in the lips. J Cosmet Dermatol. 2014;13(2):125–134.
30. Kennedy L, Craig AM. Global registries for measuring pharmacoeconomic and quality-of-life outcomes: focus on design and data collection, analysis and interpretation. Pharmacoeconomics. 2004;22(9):551–568.
31. LaBresh KA, Gliklich R, Liljestrand J, Peto R, Ellrodt AG. Using “get with the guidelines” to improve cardiovascular secondary prevention. J Comm J Qual Saf. 2003;29(10):539–550.
32. AHRQ. Registries for Evaluation Patient Outcomes: A User’s Guide.
33. Concato J, Shah N, Horwitz RI. Randomized, controlled trials, observational studies, and the hierarchy of research designs. N Engl J Med. 2000;342(25):1887–1892.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.