Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
A Proposed Checklist for Optimizing COPD Patient Discharge Processes in Italian Internal Medicine Wards
Authors Benetti A, Fiorelli EM ![]() , Grassi D, Montano N
, Grassi D, Montano N
Received 30 September 2025
Accepted for publication 14 January 2026
Published 9 April 2026 Volume 2026:21 571480
DOI https://doi.org/10.2147/COPD.S571480
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jill Ohar
Alberto Benetti,1 Elisa Maria Fiorelli,2 Davide Grassi,3 Nicola Montano2,4
1Internal Medicine Unit, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy; 2Internal Medicine, Immunology and Allergology Unit, Fondazione IRCCS Ca’ Granda, Ospedale Maggiore Policlinico, Milan, Italy; 3Internal Medicine and Nephrology Unit, San Salvatore Hospital, Department of Life, Health and Environmental Sciences, University of L’Aquila, L’Aquila, Italy; 4Department of Clinical Sciences and Community Health, University of Milan, Milan, Italy
Correspondence: Elisa Maria Fiorelli, Internal Medicine, Immunology and Allergology Unit, Fondazione IRCCS Ca’ Granda, Ospedale Maggiore Policlinico, Milan, Italy, Email [email protected]
Abstract: Chronic obstructive pulmonary disease (COPD) is a major cause of hospital admissions and readmissions, particularly following acute exacerbations. The immediate post-discharge period is a vulnerable phase, often marked by clinical instability, poor adherence, and unaddressed needs related to inhaler use, comorbidities and rehabilitation. Despite guideline recommendations, key evidence-based interventions are often overlooked in hospital discharge processes, particularly in internal medicine wards where COPD may not be the primary focus. We conducted a targeted literature search using Medline/PubMed, screening approximately 240 relevant articles that support interventions across key domains of COPD discharge care. Building on this evidence, this narrative review and expert opinion aims to raise awareness and prompt systematic implementation of essential post-discharge care components and propose a structured COPD discharge checklist aimed at standardizing care and improving post-discharge outcomes. These include initiation of smoking cessation support, optimization of maintenance therapy, assessment and correction of inhaler technique, evaluation of vaccination status, referral to pulmonary rehabilitation, scheduling of early follow-up visits, and structured patient education on self-management strategies. The checklist is grounded in current evidence demonstrating that comprehensive discharge bundles reduce 30-day readmissions, enhance quality of life, and prevent further clinical deterioration. Early pulmonary rehabilitation, particularly within 3 weeks post-discharge, and timely initiation of appropriate pharmacotherapy, including triple inhaled therapy when indicated, further reduce exacerbation risk and healthcare utilization. By integrating these elements into a concise and actionable format, the checklist aims to support internists in delivering high-quality, standardized COPD care during hospital discharge. Broad adoption may improve care transitions, promote adherence to best practices, and ultimately enhance outcomes for patients with COPD.
Keywords: chronic obstructive pulmonary disease, hospital readmission, treatment optimization, patient discharge, discharge checklist
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the leading causes of morbidity and mortality worldwide, affecting approximately 300–400 million people.1–3 According to the 2025 Global Initiative for Chronic Obstructive Lung Disease (GOLD) report, COPD is defined as “a heterogeneous lung condition characterized by chronic respiratory symptoms (dyspnea, cough, sputum production and/or exacerbations) due to abnormalities of the airways (bronchitis, bronchiolitis) and/or alveoli (emphysema) that cause persistent, often progressive, airflow obstruction”.2
Hospitalizations for COPD represent a major clinical and economic burden. Among chronic diseases, COPD has the highest rate of hospital admissions,4,5 largely due to acute exacerbations of COPD (AECOPD), which affect 20–50% of patients.6,7 Moreover, 14–47% of patients experience two or more AECOPD episodes within a year, depending on the stage of the disease.8,9 Exacerbations frequently require urgent medical attention: up to 31% lead to emergency department visits and 19% result in hospital admission.10 Notably, influenza virus infection has been reported to significantly increase the risk of pneumonia, respiratory failure, AECOPD, and ischemic stroke, with detrimental effects on respiratory health in patients with COPD that extend beyond the acute phase of infection and may persist for up to 1 year.11 These risks are not only clinical but also economic, with higher rates of hospitalizations, prolonged inpatient stays, and increased health care costs; mechanisms include both direct viral injury and enhanced susceptibility to secondary bacterial pneumonia, underscoring the importance of preventive strategies, such as annual influenza vaccination.11,12
Rehospitalization following an AECOPD is common and associated with poor outcomes.13–22 Approximately 6–26% of patients are readmitted within 30 days of discharge,23–28 7–39% within 60 days28 and 10–41% are either readmitted or die within 90 days.27–30 Approximately 18–76% are readmitted within 1 year.13,14,28,31 Greater efforts should be directed towards preventing hospitalizations due to AECOPD. Recurrent exacerbations are not only markers of disease severity but also drivers of clinical deterioration,32 contributing to a faster decline in lung function33 and increased risk of future exacerbations, cardiovascular complications and mortality.13–22,34
AECOPD is widely recognized as the primary contributor to the economic burden of COPD, accounting for approximately 45–70% of the total costs associated with disease management.35,36 In particular, hospital admissions for AECOPD account for approximately 50% of total disease-related costs, contribute significantly to COPD-related healthcare utilization, and are associated with reduced quality of life and increased mortality.5,37–47 Despite this, exacerbations are often under-recognized, under-treated, and inadequately prevented in routine clinical practice.48–50
There is strong evidence supporting structured post-discharge care in reducing these adverse outcomes.22 Timely follow-up visits, patient education, inhaler technique training, optimization of maintenance therapy, smoking cessation support, vaccination, referral to pulmonary rehabilitation (PR), and case management have all been shown to reduce readmissions and improve recovery.51–54 These interventions are also associated with decreased healthcare costs, reduced patient economic burden, and improved adherence.24,51–63
Discharge bundles, concise, evidence-based protocols designed to be implemented before discharge, have emerged as a practical tool to ensure consistency and quality in transitional care in COPD. Their use is endorsed by the British Thoracic Society and supported by numerous studies that suggest that these structured interventions may help to reduce readmissions and improve post-hospital outcomes.24,51–55,57–62,64–70
Internal medicine wards face unique challenges in COPD discharge care, as they often treat elderly, multimorbid patients reliant on caregivers. Limited time and resources can hinder in-hospital therapy optimization and patient education, with treatment adjustments often postponed to outpatient settings. This highlights the value of structured discharge checklists to support clinical decision-making.
Recent international guidelines, including GOLD 2025,2 National Institute for Health Care and Excellence (NICE),71 American Thoracic Society (ATS)72 and the 2025 New Zealand recommendations,73 emphasize a comprehensive, multidisciplinary approach to COPD discharge care. Key priorities include assessment of smoking status at every visit,2,71,73 optimization of inhaled therapy (with clear criteria for escalation to triple therapy based on symptom burden, exacerbation history, and eosinophil count),2,73,74 cardiovascular risk evaluation,2,71,73 and routine vaccination against influenza, pneumococcus, COVID-19 and varicella zoster.2,71,73 Nutritional screening is increasingly recognized as essential, particularly at hospital discharge, given its strong association with mortality and recovery outcomes.2,71,73,75 PR is universally endorsed following AECOPD hospitalization to improve exercise capacity and reduce readmissions.2,71,73,74,76,77 Follow-up care is another area of focus: while NICE advises flexible, locally coordinated review schedules, GOLD 2025 provides more specific timelines (1–4 weeks and 12–16 weeks post-discharge).2,71 Despite this strong framework, evidence gaps remain regarding the impact of discharge bundles on long-term outcomes such as mortality and quality of life,26,66,67 and real-world implementation continues to be hampered by constrained staffing, time pressures, resource limitations, inconsistent application, and logistical challenges such as scheduling follow-up appointments, maintaining clear and consistent communication, and delineating responsibilities across multidisciplinary care team members.26,78,79
The limited and inconsistent implementation of discharge bundles further complicates the assessment of their true clinical impact, while also undermining potential patient benefits.80–82
As highlighted in the qualitative study by Shaw et al, the modest improvements observed in clinical outcomes may be attributable to these systemic barriers, particularly the inconsistent application of bundles, lack of electronic integration, and poor coordination between hospital and community care settings.83
The successful deployment of discharge bundles relies on local healthcare context, adequate resources, dedicated training, and strong leadership to ensure consistent and effective delivery.
In Italy, the healthcare system is a public, universalistic model with approximately 20% private sector involvement. Internal Medicine wards are present in all hospitals and currently number around 1200 nationwide. These wards manage approximately one million hospital admissions per year, representing about 16% of total hospitalizations.
This context underscores the relevance of developing a structured COPD discharge checklist tailored to the needs of internal medicine physicians, who often care for elderly, multimorbid patients and face specific logistical and organizational challenges in delivering post-exacerbation care.
Recognizing these implementation challenges, and in an effort to support more consistent application of evidence-based discharge practices, the authors drew from both the existing literature and their clinical experience to develop a structured discharge checklist. The checklist was conceived as a clinical tool derived from guideline-based recommendations (eg, GOLD 20252) and practical considerations observed in daily hospital practice, designed to assist internal medicine physicians in addressing key elements of COPD discharge, including therapeutic optimization, vaccination, patient education, and follow-up planning. Although not formally validated in a multicenter study, the checklist has been adopted in the authors’ clinical workflows. It is proposed as a standardized model for improving care transitions and reducing preventable readmissions in routine practice across Italy. Its goal is to ensure the implementation of evidence-based interventions that may reduce readmission rates and improve patient outcomes following COPD-related hospitalization.
This expert opinion review aims to highlight key evidence-based interventions at hospital discharge and to propose a structured COPD discharge checklist to support internal medicine physicians in optimizing transitional care and reducing preventable readmissions.
Methods
We conducted a comprehensive literature search on Medline/PubMed using the search string “COPD” AND “discharge”, retaining articles relevant to interventions assessed at the time of hospital discharge to optimize transitional care and reduce preventable readmissions. We also identified additional articles through targeted searches with the terms “COPD” AND “smoking cessation” OR “therapy optimization” OR “inhaled therapy” OR “oxygen therapy” OR “cardiovascular risk” OR “vaccination” OR “nutritional status” OR “corticosteroid tapering” OR “pulmonary rehabilitation” OR “follow-up”.
Searches were conducted up to December 2025. In addition, the reference lists of retrieved articles were screened to identify further relevant publications. There were no restrictions regarding study design or publication year, and only articles published in English were included.
We assessed the eligibility of retrieved articles by screening titles and abstracts, ultimately retaining approximately 240 articles for analysis. Data were then extracted and narratively synthesized, with evidence prioritized based on clinical relevance and methodological rigor.
The literature selection process is summarized in an algorithm (Figure 1).
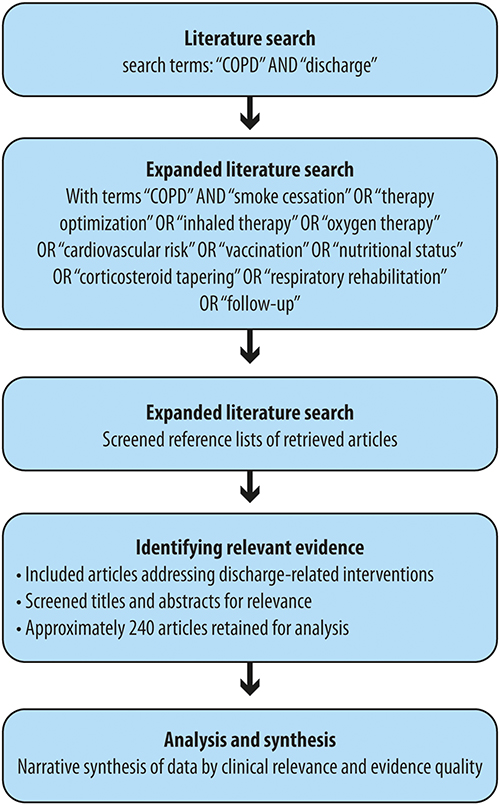 |
Figure 1 Literature search flowchart. |
The proposed checklist has not been previously published or presented in conference abstracts or institutional reports. At the time of manuscript submission, a preliminary feasibility assessment of the checklist is ongoing in several Italian internal medicine departments to explore its usability and current discharge practices. A prospective study is planned to formally evaluate its impact on post‑discharge outcomes, including hospital readmissions.
Integrated Transitional Care in COPD
Several studies support the implementation of structured discharge bundles and care pathways that encompass early post-discharge follow-up, verification of inhaler technique, patient education on self-management, scheduling of follow-up visits, smoking cessation support, spirometry reassessment, vaccination status review, and referral to PR.24,51–55,57–62,76 These components have been shown to reduce 30-day readmissions, prevent clinical deterioration, and improve quality of life in patients with COPD.24,51–55,57–62,67,69,76,84–88
A systematic review found that the implementation of COPD discharge care bundles was associated with a reduction in hospital readmissions, reporting a pooled risk ratio of 0.80 (95% CI, 0.65–0.99), without significant improvement in mortality or health-related quality of life.66 Several individual studies have failed to demonstrate reductions in readmission or mortality rates following bundle implementation.65,70,89,90 In one randomized clinical trial, the use of a transition bundle led to substantial reductions in both 7-day and 30-day readmissions (83% and 26% relative risk reduction, respectively).53 Despite this, patients in the intervention group experienced a 7.3% increase in hospital length of stay, and emergency department revisits rose by 76% within 30 days. The authors hypothesized that this increase may reflect greater symptom awareness resulting from enhanced education during hospitalization.53
In contrast, a pilot study by Hopkinson et al did not show a significant reduction in 30-day readmission rates but did report marked improvements in care delivery processes.65 After bundle implementation, the provision of smoking cessation support increased from 18% to 100%, referrals to PR rose from 14% to 68%, the distribution of self-management plans improved from 55% to 98%, and inhaler technique reviews increased from 59% to 91%.65 Notably, referrals to PR grew by 158%.65
In another study, Epstein et al integrated a clinical decision support tool into the electronic health record system to promote adherence to discharge recommendations for acute exacerbations of COPD.91 This intervention significantly improved discharge practices, with appropriate recommendations provided to 80.5% of patients, compared to 25.4% previously.91 Patients in the intervention group were also more likely to receive prescribed medications within 60 days (54% vs 20%), had higher vaccination rates (92% vs 13%), and were almost universally scheduled for follow-up visits (98%).91
Building on this foundation, comprehensive self-management programs, including smoking cessation interventions, personalized action plans for exacerbations, monthly follow-up calls by case managers or nurses, regular general practitioner visits, encouragement of PR, and influenza vaccination, have demonstrated efficacy in reducing the risk of future AECOPD events and hospital readmission.59–61,63,92
Notably, in patients with COPD who had a prior hospitalization, participation in a disease-specific self-management program, delivered alongside structured education and supported by healthcare professionals, led to a 39.8% reduction in hospital admissions and a 41.0% decrease in emergency department visits.61 These patients also experienced significantly greater improvements in quality of life compared to those receiving standard care.61
In parallel, telehealth interventions can also serve as valuable components of the post-discharge strategy. In particular, early video-based PR programs delivered via telemedicine have been associated with significant reductions in 30-day readmission rates for both all-cause and COPD-related hospitalizations.93
To translate these evidence-based strategies into routine clinical practice, a structured discharge checklist, based on a COPD discharge algorithm (Figure 2), can provide a practical and systematic approach to ensure consistent implementation of key elements of transitional care.
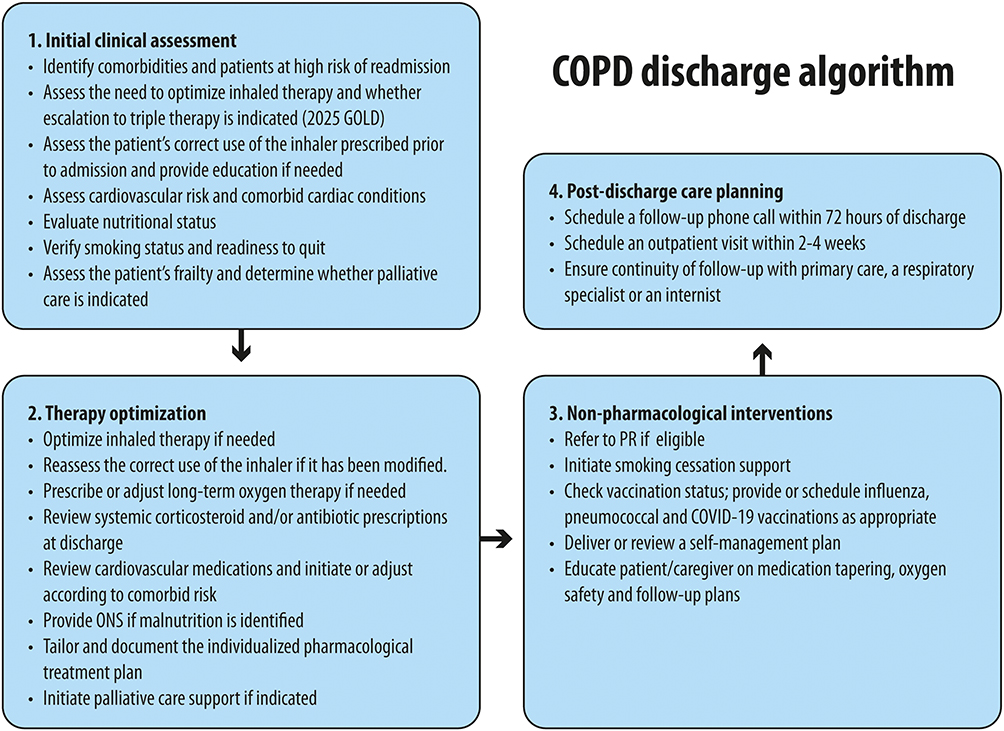 |
Figure 2 COPD discharge algorithm. Abbreviations: ONS, oral nutrition supplements; PR, pulmonary rehabilitation. |
Proposed COPD Discharge Checklist
A comprehensive discharge checklist should provide a structured framework to ensure that key domains, including smoking cessation, therapy optimization and comorbidity management, PR, education and care continuity, are adequately addressed.26
The authors developed and implemented a structured discharge checklist during their clinical practice, informed by both guideline recommendations2 and clinical experience, which may serve as a valuable tool to promote consistency and comprehensiveness in COPD discharge planning (Table 1).
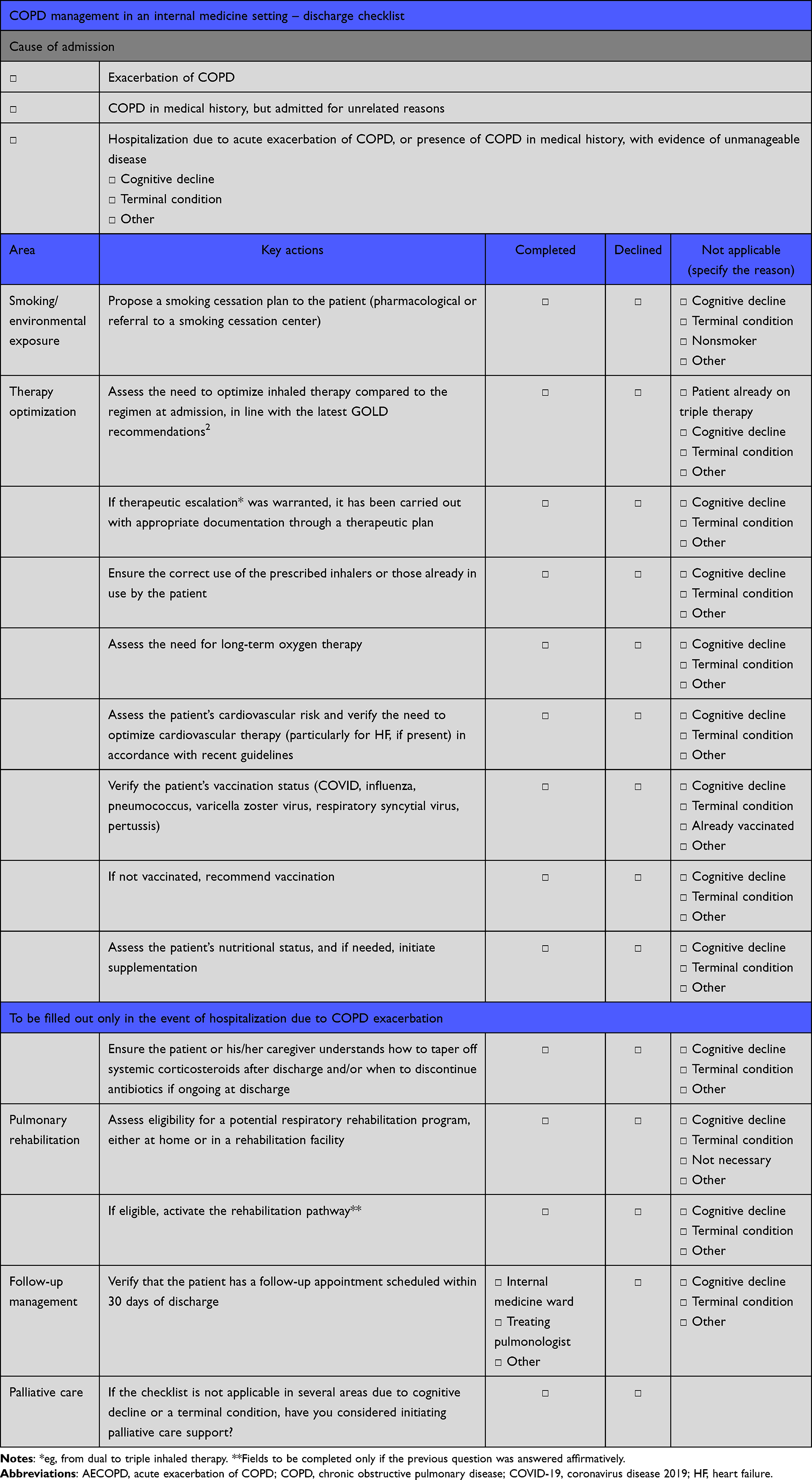 |
Table 1 Checklist for Key Interventions at COPD Hospital Discharge |
The use of the proposed COPD discharge checklist may support improved adherence to the GOLD 2025 recommendations,2 as well as enhance clinical outcomes and reduce resource utilization in internal medicine wards across Italy. In particular, the checklist is designed to prompt internists discharging COPD patients to consider a series of actions that have been shown to reduce the risk of subsequent hospitalizations, thereby improving prognosis and mitigating the economic burden associated with readmissions. Notably, in patients with cognitive impairment, the degree of cognitive decline needs to be considered when planning discharge interventions. Caregiver education should be emphasized, particularly in cases of mild-to-moderate impairment, where a meaningful benefit in treatment adherence and symptom management was expected.
In advanced cognitive decline or terminal conditions, educational and therapeutic interventions should be individualized in accordance with goals of care.
Of course, the proposed checklist should undergo external validation before it can be used as a clinical tool. We are currently conducting a preliminary test with several Italian internal medicine departments, in collaboration with the Italian Society of Internal Medicine (SIMI), to assess the checklist and to capture a snapshot of the current situation.
The Role of Smoke Cessation
Among the key domains included in the discharge checklist, smoking cessation holds a foundational role, as it directly influences disease progression, symptom burden, and long-term outcomes in patients with COPD. The GOLD 2025 guidelines recommend assessing current smoking status and exposure at every visit, followed by appropriate intervention as needed (Table 2).2 In addition, the NICE and the 2025 New Zealand guidelines recommend offering smoking cessation advice and treatment, along with referral to specialist stop-smoking services (Table 2).71,73 Addressing tobacco dependence and environmental exposures during hospitalization presents a critical opportunity to initiate behavior change. Smoke cessation is the only evidence-based intervention proven to slow the progression of COPD; it can decelerate the decline in lung function and disease progression, alleviate respiratory symptoms, improve nocturnal sleep disturbances, and reduce mortality compared to continued smoking.2,94,95 Former smokers were found to have a 22% lower risk of experiencing exacerbations compared to individuals who continued smoking.96 A combination of behavioural support and pharmacological therapy has been shown to be effective in helping COPD patients quit smoking.2,97 A 10-week smoking cessation program led to a lower mortality rate when assessed 14.5 years later, compared to those who received usual care in a randomized trial.98 Therefore, it is essential that healthcare professionals actively offer cessation counseling to strengthen patients’ confidence and ability to quit and emphasize this intervention prior to the discharge of patients with COPD.99
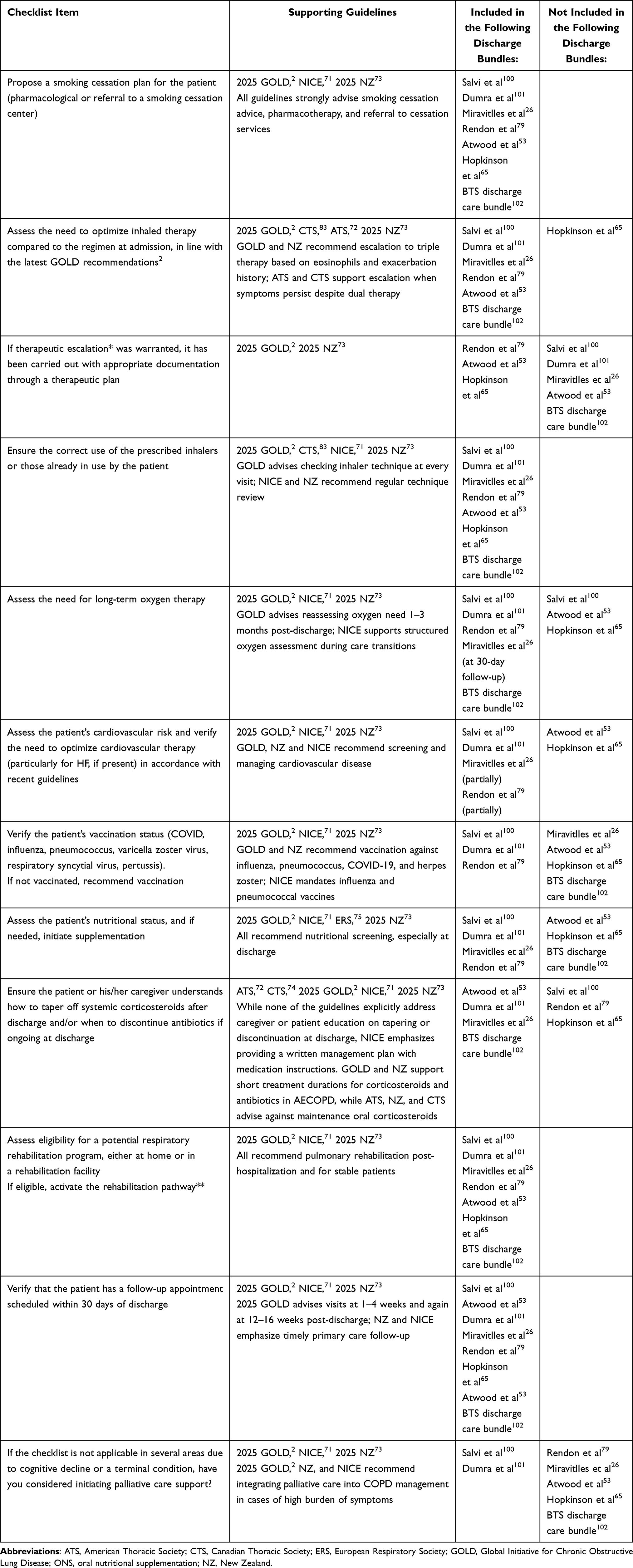 |
Table 2 Alignment of COPD Discharge Checklist Items with International Guidelines |
In addition to active smoking, exposure to secondhand smoke, indoor air pollutants, and occupational hazards, such as chemicals and fumes, are significant contributors to the development and progression of COPD2 and should be carefully considered at the time of discharge.
Therapy Optimization Upon Discharge
In addition to addressing tobacco dependence and environmental exposures, effective discharge planning for COPD must also focus on optimizing pharmacological treatment. While smoking cessation is the only intervention proven to slow disease progression, appropriate therapy plays a central role in controlling symptoms, reducing exacerbation frequency, and improving patients’ functional status in the short to medium term. Failure to promptly optimize bronchodilation may lead to persistent negative impacts on patient-reported outcomes.103 Despite hospitalization, a substantial proportion of patients continue to receive inadequate treatment for COPD. In a retrospective, population-based cohort study conducted in Sweden, 16.6% of individuals hospitalized for an exacerbation did not receive any form of maintenance therapy for COPD within the four months following their initial admission.104
Triple therapy with long-acting β-agonists, long-acting muscarinic antagonists and inhaled corticosteroids has been shown to significantly improve symptoms and lung function in real-world COPD populations, as reported in recent systematic reviews and meta-analyses.105–107 In patients with moderate to very severe COPD who experience frequent exacerbations, triple therapy has been shown to more effectively reduce exacerbation rates and potentially lower mortality, compared to dual bronchodilation alone.74,106–111 Moreover, initiating triple therapy promptly after hospital discharge has been associated with a reduced risk of subsequent exacerbations and a notable decrease in healthcare resource utilization, particularly when compared to delayed or late initiation strategies.112 Although inhaled corticosteroids are associated with an increased risk of pneumonia, the overall clinical benefit, particularly the observed reduction in mortality, has been considered to outweigh this risk.74 Accordingly, several published discharge protocols recommend initiating or maintaining triple-therapy, preferably as a single-inhaler regimen, in COPD patients with recurrent exacerbations,79,100 consistent with recent COPD management guidelines.2,26,71–74 The GOLD 2025 report2 recommends initiating triple therapy as a first-line option in patients at high risk of exacerbations with a blood eosinophil count ≥300 cells/μL. For those with a blood eosinophil count between 100 cells/μL and 300 cells/μL who continue to experience exacerbations despite dual bronchodilator (long-acting β-agonist + long-acting muscarinic antagonist), escalation to triple therapy is also advised.2 The 2025 New Zealand guidelines recommend escalation to triple therapy for patients with COPD who experience frequent exacerbations (more than one per year), have been hospitalized for an AECOPD, or continue to suffer from breathlessness and limited exercise capacity despite treatment with LABA+LAMA dual bronchodilation (Table 2).73 Escalation is also advised for individuals with blood eosinophil counts ≥300 cells/μL while on dual therapy.73 In comparison, the ATS guidelines provide a conditional recommendation for initiating triple therapy in patients with ongoing dyspnea and exercise limitation who have experienced at least one exacerbation in the previous year requiring antibiotics, corticosteroids, or hospitalization.72 Additionally, the 2023 Canadian Thoracic Society COPD Pharmacotherapy Guideline,74 which relies solely on a systematic review of randomized controlled trials, recommends initiating triple therapy for all symptomatic patients at high risk of exacerbations, irrespective of their eosinophil count. The NICE guidelines recommend weighing the risk of pneumonia against the expected clinical benefits of triple therapy.71 For patients with less severe symptoms, they advise a time-limited (3‑month) trial of triple therapy to assess treatment response, with the option to step back to LAMA+LABA if no clear benefit is achieved.71
Evidence from real-world studies indicates that single-inhaler triple therapy leads to better lung function, fewer exacerbations, improved treatment adherence, and lower mortality rates, without raising the risk of pneumonia when compared to multiple-inhaler triple therapy.113,114 Given these advantages, early use of single-inhaler triple therapy should be considered in symptomatic COPD patients who are at risk of exacerbations.103
The selection of inhalation devices for patients with COPD should be personalized and guided by multiple patient-specific factors, including cognitive status and manual skills.2,115 Lung deposition efficiency and the patient’s inspiratory flow capacity are critical parameters in determining the suitability of a given device.116 Optimizing device selection not only supports effective drug delivery but also plays a pivotal role in promoting medication adherence and improving overall clinical outcomes.115
Education on proper inhaler technique is another critical yet suboptimally addressed aspect of COPD management. In patients with COPD, improper inhaler technique and poor adherence to prescribed medications are frequently observed and have been linked to worse clinical outcomes.117 These include increased rates of hospital admissions, emergency department visits, suboptimal disease control, higher mortality, and elevated healthcare expenditures.118,119 Notably, patients treated by GPs may be less likely to receive both pharmacological and non-pharmacological therapies, and may perform inhalation techniques less accurately than those managed by pulmonologists.120 Correct inhaler use is essential for achieving therapeutic efficacy, particularly given the chronic nature of COPD and the dependence of outcomes on long-term adherence.121 Educational interventions, including demonstrations of inhaler technique and reinforcement over time, have been consistently associated with increased adherence, better disease control, and reduced hospital readmission rates.40,55,56,59–61
The indication for long-term oxygen therapy should be evaluated on an individualized basis.2 Its greatest clinical benefit is observed in COPD patients with severe resting hypoxemia, in whom it has also been shown to improve survival.122–127 By contrast, the benefits are more limited in cases of moderate hypoxemia, and the evidence remains inconsistent for patients with exertional or nocturnal hypoxemia.122,123
Oral corticosteroids are effective in the acute treatment of AECOPD, contributing to faster symptom resolution, reduced hospital length of stay, and improved recovery of lung function.128–131 Despite their short-term benefits, oral corticosteroids are not recommended for chronic use in COPD management due to their association with significant adverse effects, including an elevated risk of pneumonia.132
When appropriately prescribed, antibiotics can also facilitate a more rapid recovery from exacerbations, reduce the duration of hospital stay, and lower the likelihood of early relapse and therapeutic failure.2,131 Limiting the duration of antibiotic therapy may help mitigate the emergence of antimicrobial resistance and minimize related complications.2
Upon discharge, it is essential to verify that patients understand the intended discontinuation of acute-phase medications, such as oral corticosteroids and antibiotics. If gaps in understanding are identified, clear explanations should be provided to ensure patients are aware of the rationale behind medication withdrawal.
Cardiovascular Comorbidities
Comorbidities should be systematically addressed during discharge planning, as they influence treatment decisions, prognosis, and the risk of readmission.
Among comorbidities, cardiovascular events represent the predominant cause of hospitalization for patients with COPD,2,133 accounting for as many as half of admissions in smokers with mild-to-moderate disease.123–136 COPD itself represents a risk factor for cardiovascular disease,137 and mortality patterns confirm this strong association: up to one-third of patients with COPD die from cardiovascular disease, a proportion that increases to nearly 40% in those with pre-existing cardiac conditions.134,138 Additionally, an AECOPD is associated with a marked increase in the risk of cardiovascular events, including acute coronary syndrome and stroke, peaking in the first 10–30 days and remaining elevated for up to 1 year.2,19,139
The most prevalent comorbidity observed in COPD is elevated systolic blood pressure,2 which is more common in individuals who experience frequent exacerbations.140,141 Reported prevalence estimates vary widely, ranging from roughly 28–65%.142–145 Moreover, hypertension acts as a major vascular risk factor, contributing to the development of heart failure (HF) and ischemic heart disease (IHD), thereby worsening prognosis.146
The prevalence of HF among patients with COPD is consistently higher than in the general population, ranging from 5% to 40%,142,147–149 underscoring its role as a frequent and clinically significant comorbidity.22 The burden is particularly marked during acute events: HF is present in approximately 30% of patients hospitalized for COPD exacerbations and in up to 75% of those requiring mechanical ventilation.150–152 HF also represents the leading cause of hospital readmission in this population and significantly worsens both short- and long-term outcomes following COPD exacerbations.150
From the perspective of HF, the coexistence of COPD is also frequent: the prevalence of COPD in patients with HF lies between 13% and 39%.22,134,153,154 Notably, concomitant COPD negatively influences prognosis in HF patients as it is associated with poorer health status, an increased risk of hospitalization for both cardiovascular and non-cardiovascular causes,155 higher rates of acute exacerbations, and mortality.156–159 From a therapeutic standpoint, continuation of β-blocker therapy remains essential in HF patients, as these drugs are not contraindicated in individuals with COPD.100,160–162
Despite some variability among studies, it is estimated that between 20% and 60% of individuals with COPD are affected by coronary artery disease.142,143 Evidence from the 2017 Global Burden of Disease Study further underscores the impact of this association, identifying coronary artery disease as the leading cause of premature death in COPD, responsible for more than 1 million deaths globally.163
From a clinical standpoint, coronary artery disease manifests as IHD, which represents the spectrum of symptoms and complications arising from reduced coronary blood flow. Patients with COPD exhibit a significantly higher risk of developing IHD compared with the general population, and IHD is a major contributor to mortality, particularly in those with mild-to-moderate airflow limitation.164–167
Reported prevalence rates of IHD vary between 7% and 33%168–170 in stable COPD, and approximately 17–22% among patients hospitalized for exacerbations.171 When COPD and IHD coexist, the likelihood of hospital admission doubles,172 and short-term mortality is increased.150
Conversely, COPD is also frequently observed in individuals with IHD. A study reported a prevalence of 20% for moderate-to-severe airflow obstruction in a group of patients with IHD and undiagnosed airflow obstruction, a subgroup in which one-third also had concomitant HF.173 Accordingly, a recent systematic review and meta-analysis reported a COPD prevalence of about 12% in a population of over 18 million IHD patients; COPD leads to a greater comorbidity burden, worse acute outcomes, higher long-term mortality, and lower β-blocker prescription rates in these patients.174
Long-term data from a nationwide cohort further confirm the bidirectional link: over a median of 8 years, 2.5% of participants with COPD developed IHD, compared with only 0.8% of those without COPD.175 Notably, the study included 86 participants with incident COPD and 4128 participants without COPD.175
Within the IHD spectrum, acute myocardial infarction represents one of the most severe clinical outcomes. Among individuals with COPD, the likelihood of developing an acute myocardial infarction is markedly increased; estimates suggest a 1.4- to 4-fold elevation in risk, particularly in patients with severe disease.147,176,177 Between 10% and 17% of patients with a confirmed COPD diagnosis have a history of myocardial infarction, which is associated with adverse clinical outcomes and poorer survival.136,178
This same risk profile extends to cerebrovascular disease, with stroke representing another major outcome of systemic vascular involvement. COPD increases the likelihood of stroke, which affects approximately 10% of stable patients and up to 20% of those hospitalized for AECOPD.179
Beyond ischemic complications, COPD has also been identified as an independent risk factor for ventricular tachyarrhythmias and sudden cardiac death, irrespective of the presence of traditional cardiovascular risk factors.133,180
Patients with COPD have a heightened susceptibility to cardiac arrhythmias, particularly during AECOPD, which contributes to increased all-cause mortality.181–183 An analysis of 21.5 million COPD-related hospitalizations in the USA between 2010 and 2014 revealed that approximately 30% were complicated by arrhythmias.184 Available data indicate that 5–15% of patients with stable COPD experience arrhythmias, with the proportion rising to 20–30% among those with advanced disease.168 Two systematic reviews similarly reported a prevalence ranging from 5% to 29%, with higher rates associated with more severe impairment in lung function.142,143
Among the various rhythm disorders, atrial fibrillation (AF) is the most common supraventricular arrhythmia observed in COPD.185,186 Patients with COPD face nearly a fivefold higher risk of AF compared with individuals without COPD.185,186 The estimated prevalence of AF in stable COPD is between 4.7% and 15%, but this figure escalates to 15–30% in cases of very severe disease.187,188 In the setting of AECOPD, when AF is more likely to occur,188 AF has been documented in about 21% of hospitalized patients, and overall arrhythmias in 27%.171
The coexistence of AF in COPD carries significant clinical implications. Patients with both conditions report poorer health-related quality of life, and mortality among those hospitalized for exacerbations is higher when AF is present.189,190 Evidence also suggests a bidirectional relationship: AECOPD may precipitate AF episodes, while AF itself can act as a trigger for AECOPD.191 Moreover, COPD increases the likelihood of hospitalization for AF.192 For these reasons, systematic ECG monitoring and individualized risk stratification should be considered essential components of care to improve outcomes in this high-risk population.
COPD can also be complicated by systemic vascular diseases. Peripheral artery disease (PAD), such as coronary artery disease, is driven by atherosclerotic plaque formation that progressively obstructs arterial flow, particularly in the lower limbs. Reported prevalence rates of PAD in COPD vary widely, from 8.5% to over 80%, depending on population characteristics, such as ethnicity, disease severity, and whether analyses excluded nonsmokers or asymptomatic individuals.150,171,193–195 Conversely, COPD is also frequent in patients with PAD: one study reported a prevalence of 27.2%,196 while another found COPD in 37.5% of hospitalized smokers with PAD.197 From a clinical standpoint, the coexistence of COPD and PAD is unsurprising given their shared risk factors, particularly tobacco exposure.193 Chronic systemic inflammation, a hallmark of COPD, also plays a central role in the pathogenesis of atherosclerosis and likely contributes to the strong association between these conditions.198 Importantly, COPD is associated with elevated in-hospital mortality among patients treated for PAD.199
The current GOLD guidelines highlight the need to actively identify and manage cardiovascular comorbidities in patients with COPD, both in the stable phase and during AECOPD (Table 2).2
Given the heightened risk of cardiovascular events following an AECOPD, routine monitoring of cardiovascular markers is advised, despite limited supporting evidence, as any abnormalities observed during an exacerbation should prompt further evaluation and management in accordance with established cardiovascular disease guidelines.2
Similarly, the 2025 New Zealand and NICE guidelines recommend conducting cardiovascular assessments, including electrocardiography, echocardiography, and measurement of natriuretic peptides, particularly when cardiac disease or pulmonary hypertension is suspected (Table 2).71,73
In line with these recommendations, cardiovascular evaluation is also incorporated into discharge protocols published in the literature.22,26,101
Vaccination
In addition to optimizing pharmacologic therapy, preventive strategies aimed at reducing infection-related exacerbations are critical in the post-discharge period. Among these, vaccination represents a key preventive strategy to reduce the frequency of exacerbations, which are frequently triggered by respiratory infections.200 Importantly, no increase in exacerbation rates has been reported following influenza vaccination.201 COVID-19 vaccination is strongly recommended, as COPD patients are more susceptible to SARS-CoV-2 infection due to increased ACE2 receptor expression and face a higher risk of severe disease, hospitalization and mortality.200 The GOLD 2025 guidelines2 and the 2025 New Zealand guidelines73 recommend vaccination against COVID-19, influenza, pneumococcus, and varicella zoster virus in all COPD patients (Table 2). The NICE guidelines advise that all individuals with COPD should receive pneumococcal vaccination and an annual influenza vaccine71 (Table 2). Pertussis, tetanus and diphtheria vaccination status should also be reviewed, with immunization recommended for individuals who have not been previously vaccinated.2 Additionally, vaccination against the respiratory syncytial virus is advised in COPD patients aged over 60 years and/or in those with coexisting cardiovascular or pulmonary disease.2
Evaluation of Nutritional Status
Beyond infection prevention, nutritional status is another often-overlooked but clinically important determinant of outcomes in COPD, particularly at hospital discharge. Malnutrition is a common complication in COPD patients, with estimates ranging from 30% to 60% among patients hospitalized for an AECOPD, and results from chronic systemic inflammation, increased energy expenditure, and reduced dietary intake.202–204 These factors contribute to the loss of both fat and lean body mass, which may manifest as malnutrition, sarcopenia, cachexia or frailty, all of which have been associated with longer hospital stays and increased mortality risk.26,202,203 Malnutrition in particular negatively affects clinical symptoms, including greater lung hyperinflation, reduced pulmonary function, diminished exercise capacity, and weakened respiratory muscles, which can impair effective coughing and secretion clearance, and worsen the overall prognosis.100,202,203
Nutritional status should be assessed on an individual basis, as it varies depending on disease stage and severity.202
Weight loss in patients with respiratory disease was traditionally considered an unavoidable and irreversible condition, and even viewed as a protective adaptation aimed at reducing the body’s metabolic burden.100 However, recent evidence has overturned this perspective, demonstrating that malnutrition in COPD is both treatable and responsive to targeted nutritional interventions.205 Recent national and international guidelines underscore the importance of nutritional screening and intervention in COPD (Table 2).2 GOLD 2025 recommends that nutritional screening and counseling be part of routine COPD care, noting that unintentional weight loss is associated with increased mortality.2 The European Respiratory Society (ERS),75 NICE,71 and 2025 New Zealand73 guidelines all emphasize the use of standardized screening tools, such as BMI, weight history, or the Malnutrition Universal Screening Tool (MUST),206 especially during hospital admissions or exacerbations (Table 2). Notably, NICE71 and 2025 New Zealand73 guidelines specifically highlight the importance of assessing nutritional status at hospital discharge and integrating this into rehabilitation planning (Table 2).
Nutritional assessment is advocated as part of a multidimensional COPD management strategy, and targeted interventions, including high-protein and energy-dense nutritional supplements, have been shown to improve body weight, muscle strength, and physical performance.
Enhanced nutrition has been associated with improved respiratory muscle strength, increased functional capacity, and better quality of life, particularly when combined with PR.2,73,75,204,207
An expanding body of research, along with the GOLD 2025 guidelines, advocates for the use of oral nutritional supplements (ONS) as a means to enhance energy intake, promote weight gain, increase muscle strength, and improve health-related quality of life.2,204,205 Notably, the use of oral nutritional supplements during AECOPD hospitalizations has been shown to significantly reduce 30-day readmission rates, likely by restoring energy balance.208,209 Meta-analyses indicate that in malnourished patients, gaining more than 2 kg, achievable with an intake of at least 45 kcal/kg/day and 1.2–1.5 g protein/kg/day, is linked to improved long-term survival.100,202,204 In addition, providing nutritional support to individuals undergoing PR, even those who are not clinically malnourished, may help prevent energy deficits and enhance the overall effectiveness of the intervention.210,211
In obese patients with COPD, combining dietary energy restriction with resistance training has been shown to significantly improve BMI, exercise tolerance, and overall health status, while preserving muscle mass.212
For these reasons, it is essential to increase internists’ awareness of the importance of assessing nutritional status at the time of discharge and prescribing appropriate ONS when indicated. Equally important are the knowledge and training of healthcare professionals, together with adequate time devoted to patient education, to ensure that the prescription and adherence to oral nutritional supplements are clinically meaningful and sustainable in COPD management. A collaborative approach with dietitians is crucial, as structured dietary training can help educate both patients and caregivers, fostering long-term adherence and empowering them to actively participate in nutritional care.
Pulmonary Rehabilitation
PR is one of the most effective non-pharmacologic interventions in COPD; it has been shown to significantly improve exercise capacity, alleviate clinical symptoms, and enhance quality of life in COPD patients.2,76,77 It is strongly recommended by 2025 GOLD, 2025 New Zealand, NICE and Canadian Thoracic Society guidelines both in stable disease and following hospitalization for AECOPD, as a means to interrupt the vicious cycle of disease progression and dyspnea-driven inactivity (Table 2).2,71,73,74,76,77 Discharge protocols in the literature have recommended incorporating PR as part of a broader multidisciplinary approach including physical training, education about the disease, and support addressing nutritional, psychological, and behavioural needs.26,53,79,86,100,101,213
A cohort study involving 291 consecutive hospitalizations for AECOPD found that delivery of a COPD discharge bundle by PR practitioners, compared to non-PR staff, significantly increased both referral to PR (60% vs 12%, p<0.001) and patient uptake (40% vs 32%, p=0.001).213 This study underscores the importance of stronger integration between hospital-based care and PR services.213 Notably, the study also reported that when a discharge bundle was not administered, no patients were referred to or enrolled in PR, emphasizing the critical role discharge bundles play in facilitating access to post-hospital rehabilitation.213
Importantly, recent evidence from a systematic review confirms that PR initiated within three weeks after hospital discharge for an AECOPD significantly reduces the risk of hospital readmissions and leads to clinically meaningful improvements in exercise capacity, dyspnea, and health-related quality of life, including fatigue and emotional well-being domains of the disease.214 Similarly, a large cohort retrospective study reported reduced all-cause readmission 1 year after discharge and a reduced mean number of readmissions when PR was initiated within 3 months after discharge for an AECOPD.215 Number of days spent in hospital per person-year was also lower in those who initiated PR within 90 days of discharge (11.5 vs 22.6), and those who initiated PR also spent fewer days in a nursing home after discharge.215 Initiation of PR was also associated with a lower risk of COPD-specific rehospitalizations.215 Despite its proven efficacy, PR remains markedly underutilized, with large cohort studies indicating that only 1.5% of COPD patients initiated PR within 90 days of discharge, a timeframe that is in contrast with current guideline recommendations.40,216,217 Other data have shown that this poor rate of uptake for PR continues longitudinally, with only 1.9% of patients receiving PR within 6 months of hospitalization and 2.7% of patients receiving PR at 12 months post-discharge.218 Additionally, even patients discharged directly from the emergency department, who face a significantly higher risk of readmission compared to those discharged from inpatient care, often fail to receive appropriate referrals to PR.219 This highlights the need to improve referral practices to PR services.
Beyond pulmonary improvements, PR also improves whole-body function, mental health, and quality of life in COPD.103 The future lies in individualized PR, greater accessibility, and integrated delivery models to reach all patients in need. Notably, internet-based telerehabilitation has emerged as a safe, effective, and comparable alternative to conventional PR in terms of improving functional capacity and maintaining quality of life, particularly in settings where access to standard rehabilitation programs is limited.220
Post-Discharge Follow-Up
A retrospective cohort study in the USA reported that 66.9% of COPD patients had a follow-up appointment scheduled with their pulmonologist or primary care provider within 30 days.51 In contrast, a retrospective cohort study conducted in an Israeli hospital reported that only 44.1% of COPD patients had a follow-up appointment with a pulmonologist within 30 days post-discharge.58 These gaps are clinically significant, as multiple studies have demonstrated that structured and timely follow-up care is associated with reduced hospital readmissions and improved long-term outcomes.51–55,58 The NICE guidelines recommend that people with COPD should be reviewed at least annually, or more frequently if clinically indicated.71 While they state that routine hospital follow-up is generally unnecessary for most people with stable, severe COPD, they emphasize the need for locally agreed mechanisms to ensure rapid access to hospital assessment when needed.71 For individuals with very severe COPD, the NICE guidelines advise at least two reviews per year in primary care, although they do not specify the appropriate timing for the first visit after hospital discharge (Table 2).71
In contrast, the GOLD 2025 guidelines provide clearer guidance, recommending a first follow-up assessment 1–4 weeks post-discharge, followed by a second visit at 12–16 weeks (Table 2).2 These visits should include evaluation of treatment understanding, inhaler technique, reassessment of the need for long-term oxygen therapy, assessment of physical activity capacity and eligibility for pulmonary rehabilitation, as well as a review of symptoms and comorbidities.2
Similarly, the 2025 New Zealand guidelines advise that patients receive a primary care follow-up within two weeks of hospital discharge for patients hospitalized due to an AECOPD (Table 2).73 Several studies recommending discharge protocols emphasize the importance of scheduling follow-up appointments within 2–4 weeks after discharge,26,83,101 Other studies highlight the value of early post-discharge contact, including evidence that a hospital-initiated phone call within 72 hours can significantly reduce readmission rates, further supporting the need for prompt and proactive follow-up care.53,79
Beyond care continuity, early follow-up also provides a critical window for diagnostic reassessment and treatment adjustment. According to the GOLD guidelines,2 spirometries should be performed when the patient is clinically stable and free of respiratory tract infection. Interestingly, studies have shown no significant differences between spirometry obtained at the time of hospital admission for AECOPD and those repeated 1 month later.221,222 Despite this, spirometry remains significantly underused during hospitalization. It is essential, in patients who have never undergone spirometric evaluation, to confirm a COPD diagnosis and initiate prompt treatment.221,222 Spirometry is a reliable tool for detecting obstructive patterns,221,222 although it may overestimate disease severity during AECOPD due to transient pathophysiological changes.221 Performing spirometry approximately 1 month after discharge is especially valuable to confirm that COPD was the underlying cause of hospitalization and to accurately assess disease severity.221 This is particularly important in patients with comorbidities, such as HF, which may decrease forced vital capacity (FVC) and potentially obscure the diagnosis.221 Identifying such cases early allows for timely re-evaluation and tailored management.
Palliative Care
Patients with advanced COPD often experience symptom burdens that are comparable to, or even exceed, those of individuals with terminal cancer.223 Despite evidence showing that palliative care can reduce 30-day hospital readmission rates by as much as 50% and lower the risk of heart failure events by 73%,224–226 its use in COPD remains limited and frequently delayed until the very late stages of disease.227,228 Major guidelines recommend the integration of palliative care into discharge protocols for patients with a high symptom burden or persistent, refractory symptoms (Table 2).2,71,73 Increasingly, clinical consensus supports the early integration of palliative care alongside standard COPD management (Table 2),100,101 particularly in response to markers such as progressive lung function decline, frequent exacerbations, or escalating symptom burden.228,229 Early palliative care can address unmet needs related to breathlessness, pain, fatigue, poor nutrition, anxiety, and depression, symptoms that may persist despite optimal medical therapy.228,229 Moreover, timely intervention has been shown to enhance quality of life, reduce unnecessary hospitalizations, and provide essential support to caregivers.228 Nevertheless, several barriers hinder its implementation, including clinician misconceptions, limited training, time constraints, and systemic inequities in access to palliative services. Innovative approaches, such as targeted provider education, supportive policies, and telemedicine, offer promising pathways to broader adoption.228,230
Importantly, for patients with advanced disease, cognitive impairment, or limited life expectancy, palliative care should be considered not only as a supportive component of post-discharge care but also as a framework for identifying interventions that may no longer align with the patient’s goals or clinical status, such as PR, vaccinations, or long-term inhaled therapy optimization. In such cases, individualized care planning may involve the de-escalation or omission of certain checklist items, prioritizing comfort, quality of life, and caregiver support.
Individualized planning should thus allow for selective deimplementation of checklist items when appropriate. The experts support the integration of palliative care into COPD discharge protocols as a strategy to mitigate symptom burden, enhance patient-centered outcomes, and guide treatment decisions in more complex cases.
Existing COPD Discharge Bundles: A Comparative Perspective
A comparison of our proposed checklist with existing COPD discharge bundles highlights both commonalities and important distinctions (Table 2). Our checklist shares substantial overlap with the protocols proposed by Salvi et al and Dumra et al, including key components such as therapeutic optimization, patient education, assessment of nutritional status, and palliative care considerations.100,101 Additionally, Salvi’s 7-point strategy does not directly address patient or caregiver education regarding corticosteroid tapering or antibiotic discontinuation,100 an aspect explicitly included in our checklist in line with GOLD 2025 recommendations.2
The discharge checklist proposed by Miravitlles et al26 shares similarities with ours, but it refers only generally to comorbidities without explicitly emphasizing the need to assess cardiovascular risk and optimize cardiovascular therapy, an important consideration given the well-documented overlap between COPD and cardiovascular disease discussed earlier. Despite stating that therapy should be individualized, it does not include the need to assess and update the vaccination status, nor does it include the role of palliative care in cases where multiple components of the discharge process may no longer be appropriate or feasible for the patient.
The discharge bundle developed by Rendon et al also aligns closely with our approach and emphasizes individualized care planning.79 Nevertheless, it omits critical elements such as guidance on corticosteroid tapering or antibiotic discontinuation at discharge, cardiovascular risk assessment and treatment, and the consideration of palliative care when clinical interventions may no longer be appropriate.79 These omissions may limit its applicability in complex or frail patients.
By contrast, the bundle proposed by Atwood et al53 is less comprehensive. It does not address key aspects such as nutritional screening, cardiovascular evaluation, vaccination counseling, or long-term oxygen therapy anddoes not incorporate palliative care.53 Compared to our checklist and others,79,101 it provides a more limited and less detailed framework.
The British Thoracic Society discharge care bundle, summarized by Shaw et al, likewise omits several essential components, including cardiovascular risk management, nutritional assessment, vaccination status, oxygen therapy needs, and palliative care planning, limiting its breadth in addressing the multidimensional needs of COPD patients.83,102
Compared with the discharge bundle described by Hopkinson et al,65 our checklist adopts a broader and more integrated approach. While both tools emphasize smoking cessation support, inhaler technique review, pulmonary rehabilitation referral, and scheduled follow-up,65 our checklist expands on these foundations by incorporating guideline-based pharmacological strategies (including escalation to triple therapy), assessment of patient’s of discharge medication instructions, cardiovascular risk assessment and optimization of related therapy, long-term oxygen therapy, vaccination review, nutritional support, comorbidity management, and the integration of palliative care planning when appropriate.
Regarding the timeframe for scheduling follow-up visits, Salvi et al100 and Atwood et al53 do not recommend a specific interval, whereas Dumra et al,101 Miravitlles et al,26 Rendon et al79 and Hopkinson et al65 highlight the need for a follow-up visit scheduled within 4 weeks or 30 days of discharge. In addition, Atwood et al,53 the BTS discharge care bundle and Hopkinson et al65 recommend a follow-up telephone call within 72 hours of discharge.102
Designed specifically for the internal medicine setting, where time constraints, multimorbidity, and caregiver involvement pose significant challenges, our checklist aims to enhance the consistency and quality of post-discharge care. By facilitating structured decision-making and supporting adherence to international guidelines, it may help address the persistently low implementation rates of GOLD-recommended interventions,80,81,231 an issue associated with increased hospitalizations and emergency department visits.82
Barriers to Implementing COPD Discharge Care
Although discharge bundles have shown promise in improving outcomes and reducing readmissions for patients with COPD, the authors highlight several important limitations to their real-world application. A major challenge is the lack of standardization; discharge bundles vary significantly in their structure, content, and delivery across different studies and healthcare settings, making consistent implementation and identification of which specific components drive improved outcomes difficult.26,79 Even where such bundles are available, they are often applied incompletely or inconsistently, with only a fraction of patients receiving all recommended components, due to resource limitations, time constraints, challenges with integration in electronic medical records, payer variability, staff availability, and generalizability outside of the local context.26,78,79,83,84,232 In many cases, successful implementation depends on the presence of particularly motivated individuals or teams, which limits scalability.26 The logistical and organizational elements, such as scheduling follow-up appointments, ensuring consistent communication, and delineating responsibilities among care team members, have been identified as the most significant obstacles to successfully applying COPD discharge bundles.78 Communication and engagement challenges, such as poor coordination between hospital and community-based providers and limited patient engagement in post-discharge self-management due to patients’ perceived confusion about follow-up care, insufficient education, and difficulty accessing services, such as PR, have been reported.78 Patient-related barriers, such as low health literacy, poor engagement, and socioeconomic challenges, also affect adherence to discharge recommendations.26,79,84 Moreover, poor communication and coordination between hospital and primary care services can create additional gaps during the transition of care.26 Miravitlles et al also point out that while discharge bundles may offer short-term benefits, evidence on their long-term effectiveness remains limited.26 Importantly, they caution against a one-size-fits-all approach and emphasize the need for discharge planning to be individualized, taking into account patient-specific risk factors, comorbidities, and care preferences.26
Overall, the authors of this study stress the need for more standardized, evidence-based, and context-sensitive discharge protocols that are feasible to implement across diverse healthcare environments. Discharge bundles should be adapted to local contexts and available resources, and implementation must be supported by health system strengthening, local leadership, and policy commitment.
Conclusion
In summary, this narrative review highlights significant opportunities to improve and standardize discharge practices in COPD care in Italian internal medicine settings. The frequent coexistence of multiple comorbidities and the need for long-term oxygen therapy and palliative care activation highlight the complexity and clinical frailty of patients hospitalized for AECOPD, reflecting the typical case mix managed in internal medicine settings.
The discharge checklist proposed in this study integrates key domains critical to post-discharge outcomes, including smoking cessation, pharmacologic optimization, comorbidity management, vaccination, nutritional assessment, pulmonary rehabilitation, and early follow-up or palliative care activation when needed. By consolidating these evidence-supported interventions into a unified tool, the checklist may offer a practical, evidence-informed tool to guide internists in delivering comprehensive transitional care. Its integration into routine practice could help reduce variability, support guideline adherence, and ultimately improve outcomes for COPD patients transitioning from hospital to home.
Looking ahead, after this preliminary phase test, we plan to conduct a prospective study to assess the effect of this discharge checklist in reducing hospitalizations. Broader adoption may facilitate nationwide standardization, enhance interdisciplinary collaboration, and ultimately improve the quality of transitional care for patients hospitalized with COPD.
Acknowledgments
Editorial assistance was provided by Valeria Benedusi, Simonetta Papa and Aashni Shah (Polistudium srl, Milan, Italy). This assistance was supported by AstraZeneca S.r.l.
Funding
Editorial assistance was unconditionally supported by AstraZeneca S.r.l.
Disclosure
The authors declare no conflicts of interest related to the present paper. The sponsor had no role in the conception, design, analysis, interpretation, or writing of the manuscript. All content reflects the independent opinions of the authors.
AB, EF, DG: Consultancy and advisory roles from AstraZeneca.
NM: Advisory Boards for AstraZeneca, Bayer, Novo Nordisk, Gilead, Philips, Sanofi, Merck.
References
1. Ntritsos G, Franek J, Belbasis L, et al. Gender-specific estimates of COPD prevalence: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2018;13:1507–26. doi:10.2147/COPD.S146390
2. Initiative Global. 2025 GOLD Report. Available from: https://goldcopd.org/2025-gold-report/. (
3. Varmaghani M, Dehghani M, Heidari E, Sharifi F, Moghaddam SS, Farzadfar F. Global prevalence of chronic obstructive pulmonary disease: systematic review and meta-analysis. East Mediterr Health J. 2019;25:47–57. doi:10.26719/emhj.18.014
4. Alshabanat A, Otterstatter MC, Sin DD, et al. Impact of a COPD comprehensive case management program on hospital length of stay and readmission rates. Int J Chron Obstruct Pulmon Dis. 2017;12:961–971. doi:10.2147/COPD.S124385
5. Mulpuru S, McKay J, Ronksley PE, Thavorn K, Kobewka DM, Forster AJ. Factors contributing to high-cost hospital care for patients with COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:989–995. doi:10.2147/COPD.S126607
6. Athanazio RA, Villada LB, Avdeev SN, et al. Rate of severe exacerbations, healthcare resource utilisation and clinical outcomes in patients with COPD in low-income and middle-income countries: results from the EXACOS international study. BMJ Open Respir Res. 2024;11. doi:10.1136/bmjresp-2023-002101
7. Melles M, In T Veen J, Slebos DJJ, Franssen F, van Dijk M, Hekking PPP. Prevalence of COPD with frequent exacerbations and biomarkers of type 2 airway inflammation in a real-world setting. Am J Respir Crit Care Med. 2025;211:A3257–A3257. doi:10.1164/ajrccm.2025.211.Abstracts.A3257
8. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363:1128–1138. doi:10.1056/NEJMoa0909883
9. Han MK, Quibrera PM, Carretta EE, et al. Frequency of exacerbations in patients with chronic obstructive pulmonary disease: an analysis of the SPIROMICS cohort. Lancet Respir Med. 2017;5:619–626. doi:10.1016/S2213-2600(17)30207-2
10. Mittmann N, Kuramoto L, Seung SJ, Haddon JM, Bradley-Kennedy C, Fitzgerald JM. The cost of moderate and severe COPD exacerbations to the Canadian healthcare system. Respir Med. 2008;102(3):413–421. doi:10.1016/j.rmed.2007.10.010
11. Liao K-M, Chen Y-J, Shen C-W, Ou S-K, Chen C-Y. The influence of influenza virus infections in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2022;17:2253–2261. doi:10.2147/COPD.S378034
12. Wallick C, To TM, Korom S, Masters H, Hanania NA, Moawad D. Impact of influenza infection on the short- and long-term health of patients with chronic obstructive pulmonary disease. J Med Econ. 2022;25:930–939. doi:10.1080/13696998.2022.2098630
13. Garcia-Aymerich J, Farrero E, Félez MA, Izquierdo J, Marrades RM, Antó JM. Risk factors of readmission to hospital for a COPD exacerbation: a prospective study. Thorax. 2003;58:100–105. doi:10.1136/thorax.58.2.100
14. Almagro P, Barreiro B, Ochoa A, et al. Risk factors for hospital readmission in patients with chronic obstructive pulmonary disease. Respiration. 2006;73:311–317. doi:10.1159/000088092
15. Donaldson GC, Seemungal TAR, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57:847–852. doi:10.1136/thorax.57.10.847
16. McGhan R, Radcliff T, Fish R, Sutherland ER, Welsh C, Make B. Predictors of rehospitalization and death after a severe exacerbation of COPD. Chest. 2007;132:1748–1755. doi:10.1378/chest.06-3018
17. Lau A, L YAM, Poon E. Hospital readmission in patients with acute exacerbation of chronic obstructive pulmonary disease. Respir Med. 2001;95. doi:10.1053/rmed.2001.1180.
18. Suissa S, Dell’Aniello S, Ernst P. Long-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortality. Thorax. 2012;67:957–963. doi:10.1136/thoraxjnl-2011-201518
19. Donaldson GC, Hurst JR, Smith CJ, Hubbard RB, Wedzicha JA. Increased risk of myocardial infarction and stroke following exacerbation of COPD. Chest. 2010;137:1091–1097. doi:10.1378/chest.09-2029
20. Watz H, Tetzlaff K, Magnussen H, et al. Spirometric changes during exacerbations of COPD: a post hoc analysis of the WISDOM trial. Respir Res. 2018;19:251. doi:10.1186/s12931-018-0944-3
21. Hogea S-P, Tudorache E, Fildan AP, Fira-Mladinescu O, Marc M, Oancea C. Risk factors of chronic obstructive pulmonary disease exacerbations. Clin Respir J. 2020;14:183–197. doi:10.1111/crj.13129
22. Bianco A, Canepa M, Catapano GA, et al. Implementation of the care bundle for the management of chronic obstructive pulmonary disease with/without heart failure. J Clin Med. 2024;13:1621. doi:10.3390/jcm13061621
23. Matkovic Z, Huerta A, Soler N, et al. Predictors of adverse outcome in patients hospitalised for exacerbation of chronic obstructive pulmonary disease. Respiration. 2012;84:17–26. doi:10.1159/000335467
24. Shah T, Churpek MM, Coca Perraillon M, Konetzka RT. Understanding why patients with COPD get readmitted: a large national study to delineate the medicare population for the readmissions penalty expansion. Chest. 2015;147:1219–1226. doi:10.1378/chest.14-2181
25. Li J, Liang L, Cao S, et al. Secular trend and risk factors of 30-day COPD-related readmission in Beijing, China. Sci Rep. 2022;12:16589. doi:10.1038/s41598-022-20884-3
26. Miravitlles M, Bhutani M, Hurst JR, et al. Implementing an evidence-based COPD hospital discharge protocol: a narrative review and expert recommendations. Adv Ther. 2023;40:4236–4263. doi:10.1007/s12325-023-02609-8
27. Alqahtani JS, Njoku CM, Bereznicki B, et al. Risk factors for all-cause hospital readmission following exacerbation of COPD: a systematic review and meta-analysis. Eur Respir Rev. 2020;29:190166. doi:10.1183/16000617.0166-2019
28. Ruan H, Zhang H, Wang J, et al. Readmission rate for acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Respir Med. 2023;206. doi:10.1016/j.rmed.2022.107090
29. Echevarria C, Steer J, Heslop-Marshall K, et al. The PEARL score predicts 90-day readmission or death after hospitalisation for acute exacerbation of COPD. Thorax. 2017;72:686–693. doi:10.1136/thoraxjnl-2016-209298
30. Crinion S, Cotter O, Kennedy B, et al. COPD exacerbations — a comparison of Irish data with European data from the ERS COPD Audit. Ir Med J. 2013;106(268):270–272.
31. Gudmundsson G, Gislason T, Janson C, et al. Risk factors for rehospitalisation in COPD: role of health status, anxiety and depression. Eur Respir J. 2005;26:414–419. doi:10.1183/09031936.05.00078504
32. Guo J, Chen Y, Zhang W, Tong S, Dong J. Moderate and severe exacerbations have a significant impact on health-related quality of life, utility, and lung function in patients with chronic obstructive pulmonary disease: a meta-analysis. Int J Surg. 2020;78:28–35. doi:10.1016/j.ijsu.2020.04.010
33. Mercer P, Shute J, Bhowmik A, Donaldson G, Wedzicha J, Warner J. MMP-9, TIMP-1 and inflammatory cells in sputum from COPD patients during exacerbation. Respir Res. 2005;6:151. doi:10.1186/1465-9921-6-151
34. Fortis S, Wan ES, Kunisaki K, et al. Increased mortality associated with frequent exacerbations in COPD patients with mild-to-moderate lung function impairment, and smokers with normal spirometry. Respir Med X. 2021;3:100025. doi:10.1016/j.yrmex.2020.100025
35. Stafyla E, Geitona M, Kerenidi T, Economou A, Daniil Z, Gourgoulianis KI. The annual direct costs of stable COPD in Greece. Int J Chron Obstruct Pulmon Dis. 2018;13:309–315. doi:10.2147/COPD.S148051
36. Agarwal D. COPD generates substantial cost for health systems. Lancet Glob Health. 2023;11:e1138–e1139. doi:10.1016/S2214-109X(23)00304-2
37. Miravitlles M, Murio C, Guerrero T, Gisbert R. Pharmacoeconomic evaluation of acute exacerbations of chronic bronchitis and COPD. Chest. 2002;121:1449–1455. doi:10.1378/chest.121.5.1449
38. Press VG, Konetzka RT, White SR. Insights about the economic impact of chronic obstructive pulmonary disease readmissions post implementation of the hospital readmission reduction program. Curr Opin Pulm Med. 2018;24:138–146. doi:10.1097/MCP.0000000000000454
39. McIlvennan CK, Eapen ZJ, Allen LA. Hospital readmissions reduction program. Circulation. 2015;131:1796–1803. doi:10.1161/CIRCULATIONAHA.114.010270
40. Criner GJ, Bourbeau J, Diekemper RL, et al. Prevention of acute exacerbations of COPD: American College of Chest Physicians and Canadian Thoracic Society Guideline. Chest. 2015;147:894–942. doi:10.1378/chest.14-1676
41. Iheanacho I, Zhang S, King D, Rizzo M, Ismaila AS. Economic burden of chronic obstructive pulmonary disease (COPD): a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:439–460. doi:10.2147/COPD.S234942
42. Green SA, Bell D, Mays N. Identification of factors that support successful implementation of care bundles in the acute medical setting: a qualitative study. BMC Health Serv Res. 2017;17:120. doi:10.1186/s12913-017-2070-1
43. Dhalla IA, O’Brien T, Ko F, Laupacis A. Toward safer transitions: how can we reduce post-discharge adverse events? Healthc Q. 2012;15 Spec No:63–67. doi:10.12927/hcq.2012.22839
44. Hussey PS, Schneider EC, Rudin RS, Fox DS, Lai J, Pollack CE. Continuity and the costs of care for chronic disease. JAMA Intern Med. 2014;174:742–748. doi:10.1001/jamainternmed.2014.245
45. Blanchette CM, Gross NJ, Altman P. Rising costs of COPD and the potential for maintenance therapy to slow the trend. Am Health Drug Benefits. 2014;7:98–106.
46. Shah T, Press VG, Huisingh-Scheetz M, White SR. COPD readmissions: addressing COPD in the era of value-based health care. Chest. 2016;150:916–926. doi:10.1016/j.chest.2016.05.002
47. Miravitlles M, García-Polo C, Domenech A, Villegas G, Conget F, de la Roza C. Clinical outcomes and cost analysis of exacerbations in chronic obstructive pulmonary disease. Lung. 2013;191:523–530. doi:10.1007/s00408-013-9487-z
48. Langsetmo L, Platt RW, Ernst P, Bourbeau J. Underreporting exacerbation of chronic obstructive pulmonary disease in a longitudinal cohort. Am J Respir Crit Care Med. 2008;177:396–401. doi:10.1164/rccm.200708-1290OC
49. Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157:1418–1422. doi:10.1164/ajrccm.157.5.9709032
50. Xu W, Collet J-P, Shapiro S, et al. Negative impacts of unreported COPD exacerbations on health-related quality of life at 1 year. Eur Respir J. 2010;35:1022–1030. doi:10.1183/09031936.00079409
51. Sharma G, Kuo Y-F, Freeman JL, Zhang DD, Goodwin JS. Outpatient follow-up visit and 30-day emergency department visit and readmission in patients hospitalized for chronic obstructive pulmonary disease. Arch Intern Med. 2010;170:1664–1670. doi:10.1001/archinternmed.2010.345
52. Sin DD, Bell NR, Svenson LW, Man SFP. The impact of follow-up physician visits on emergency readmissions for patients with asthma and chronic obstructive pulmonary disease: a population-based study. Am J Med. 2002;112:120–125. doi:10.1016/s0002-9343(01)01079-8
53. Atwood CE, Bhutani M, Ospina MB, et al. Optimizing COPD acute care patient outcomes using a standardized transition bundle and care coordinator: a randomized clinical trial. Chest. 2022;162:321–330. doi:10.1016/j.chest.2022.03.047
54. Bourbeau J, Echevarria C. Models of care across the continuum of exacerbations for patients with chronic obstructive pulmonary disease. Chron Respir Dis. 2020;17:1479973119895457. doi:10.1177/1479973119895457
55. Lenferink A, Brusse-Keizer M, van der Valk PD, et al. Self-management interventions including action plans for exacerbations versus usual care in patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017;8:CD011682. doi:10.1002/14651858.CD011682.pub2
56. Benzo R, Vickers K, Novotny PJ, et al. Health coaching and chronic obstructive pulmonary disease rehospitalization. a randomized study. Am J Respir Crit Care Med. 2016;194:672–680. doi:10.1164/rccm.201512-2503OC
57. Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the medicare fee-for-service program. N Engl J Med. 2009;360:1418–1428. doi:10.1056/NEJMsa0803563
58. Gavish R, Levy A, Dekel OK, Karp E, Maimon N. The association between hospital readmission and pulmonologist follow-up visits in patients with COPD. Chest. 2015;148:375–381. doi:10.1378/chest.14-1453
59. Rice KL, Dewan N, Bloomfield HE, et al. Disease management program for chronic obstructive pulmonary disease: a randomized controlled trial. Am J Respir Crit Care Med. 2010;182:890–896. doi:10.1164/rccm.200910-1579OC
60. Rea H, McAuley S, Stewart A, Lamont C, Roseman P, Didsbury P. A chronic disease management programme can reduce days in hospital for patients with chronic obstructive pulmonary disease. Intern Med J. 2004;34:608–614. doi:10.1111/j.1445-5994.2004.00672.x
61. Bourbeau J, Julien M, Maltais F, et al. Reduction of hospital utilization in patients with chronic obstructive pulmonary disease: a disease-specific self-management intervention. Arch Intern Med. 2003;163:585–591. doi:10.1001/archinte.163.5.585
62. Zwerink M, Brusse-Keizer M, van der Valk PDLP, et al. Self management for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014:CD002990. doi:10.1002/14651858.CD002990.pub3.
63. Kessler R, Casan-Clara P, Koehler D, et al. COMET: a multicomponent home-based disease-management programme versus routine care in severe COPD. Eur Respir J. 2018;51:1701612. doi:10.1183/13993003.01612-2017
64. Kong CW, Wilkinson TMA. Predicting and preventing hospital readmission for exacerbations of COPD. ERJ Open Res. 2020;6. doi:10.1183/23120541.00325-2019.
65. Hopkinson NS, Englebretsen C, Cooley N, et al. Designing and implementing a COPD discharge care bundle. Thorax. 2012;67:90–92. doi:10.1136/thoraxjnl-2011-200233
66. Ospina MB, Mrklas K, Deuchar L, et al. A systematic review of the effectiveness of discharge care bundles for patients with COPD. Thorax. 2017;72:31–39. doi:10.1136/thoraxjnl-2016-208820
67. Westbroek LF, Klijnsma M, Salomé P, et al. Reducing the number of hospitalization days for COPD: setting up a transmural-care pathway. Int J Chron Obstruct Pulmon Dis. 2020;15:2367–2377. doi:10.2147/COPD.S242914
68. British Thoracic Society (BTS). COPD discharge care bundle. Available from: https://www.brit-thoracic.org.uk/quality-improvement/clinical-resources/copd-spirometry/.
69. Gentene AJ, Guido MR, Woolf B, et al. Multidisciplinary team utilizing pharmacists in multimodal, bundled care reduce chronic obstructive pulmonary disease hospital readmission rates. J Pharm Pract. 2021;34:110–116. doi:10.1177/0897190019889440
70. Casas A, Troosters T, Garcia-Aymerich J, et al. Integrated care prevents hospitalisations for exacerbations in COPD patients. Eur Respir J. 2006;28:123–130. doi:10.1183/09031936.06.00063205
71. Chronic Obstructive Pulmonary Disease in Over 16s: Diagnosis and Management. London: National Institute for Health and Care Excellence (NICE); 2019.
72. Nici L, Mammen MJ, Charbek E, et al. Pharmacologic management of chronic obstructive pulmonary disease. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020;201:e56–e69. doi:10.1164/rccm.202003-0625ST
73. Hancox R, Jones S, Baggott C, et al. New Zealand chronic obstructive pulmonary disease guidelines: 2025 update. N Z Med J. 2025;138:59–63. doi:10.26635/6965.7149
74. Bourbeau J, Bhutani M, Hernandez P, et al. Canadian thoracic society guideline on pharmacotherapy in patients with stable COPD. Chest. 2023;164:1159–1183. doi:10.1016/j.chest.2023.08.014
75. Schols AM, Ferreira IM, Franssen FM, et al. Nutritional assessment and therapy in COPD: a European Respiratory Society statement. Eur Respir J. 2014;44:1504–1520. doi:10.1183/09031936.00070914
76. Rochester CL, Alison JA, Carlin B, et al. Pulmonary rehabilitation for adults with chronic respiratory disease: an Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2023;208:e7–e26. doi:10.1164/rccm.202306-1066ST
77. Troosters T, Janssens W, Demeyer H, Rabinovich RA. Pulmonary rehabilitation and physical interventions. Eur Respir Rev. 2023;32. doi:10.1183/16000617.0222-2022.
78. Michas M, Deuchar L, Leigh R, et al. Factors influencing the implementation and uptake of a discharge care bundle for patients with acute exacerbation of chronic obstructive pulmonary disease: a qualitative focus group study. Implement Sci Commun. 2020;1:3. doi:10.1186/s43058-020-00017-5
79. Rendon A, Luhning S, Bardin P, et al. Recommendations for improving discharge-related care following a COPD exacerbation: An expert panel consensus with emphasis on low- and middle-income countries. Int J Chron Obstruct Pulmon Dis. 2025;20:1111–1129. doi:10.2147/COPD.S502971
80. Kim TO, Shin HJ, Kim YI, et al. Adherence to the GOLD guideline in COPD management of South Korea: findings from KOCOSS study 2011-2018. Chonnam Med J. 2019;55:47–53. doi:10.4068/cmj.2019.55.1.47
81. Marmy JL, Diedrich JP, Cadus C, et al. Adherence to GOLD recommendations among Swiss pulmonologists and general practitioners. COPD. 2021;18:9–15. doi:10.1080/15412555.2020.1859469
82. Mannino DM, Yu TC, Zhou H, et al. Effects of GOLD-adherent prescribing on COPD symptom burden, exacerbations, and health care utilization in a real-world setting. Chronic Obstr Pulm Dis. 2015;2:223–235. doi:10.15326/jcopdf.2.3.2014.0151
83. Shaw A, Morton K, King A, et al. Using and implementing care bundles for patients with acute admission for COPD: qualitative study of healthcare professionals’ experience in four hospitals in England. BMJ Open Respir Res. 2020;7:e000515. doi:10.1136/bmjresp-2019-000515
84. Saifan AR, Elshatarat RA, Sawalha MA, et al. Assessing the impact of a respiratory care bundle on health status and quality of life of chronic obstructive pulmonary disease patients in Jordan: a quasi-experimental study. J Educ Health Promot. 2024;13:191. doi:10.4103/jehp.jehp_1110_23
85. Lainscak M, Kadivec S, Kosnik M, et al. Discharge coordinator intervention prevents hospitalizations in patients with COPD: a randomized controlled trial. J Am Med Dir Assoc. 2013;14:450.e1–6. doi:10.1016/j.jamda.2013.03.003
86. Laverty AA, Elkin SL, watt HC, et al. Impact of a COPD discharge care bundle on readmissions following admission with acute exacerbation: interrupted time series analysis. PLoS One. 2015;10:e0116187. doi:10.1371/journal.pone.0116187
87. Zafar MA, Loftus TM, Palmer JP, et al. COPD care bundle in emergency department observation unit reduces emergency department revisits. Respir Care. 2020;65:1–10. doi:10.4187/respcare.07088
88. Abad-Corpa E, Royo-Morales T, Iniesta-Sánchez J, et al. Evaluation of the effectiveness of hospital discharge planning and follow-up in the primary care of patients with chronic obstructive pulmonary disease. J Clin Nurs. 2013;22:669–680. doi:10.1111/j.1365-2702.2012.04155.x
89. Cousse S, Gillibert A, Salaün M, et al. Efficacy of a home discharge care bundle after acute exacerbation of COPD. Int J Chron Obstruct Pulmon Dis. 2019;14:289–296. doi:10.2147/COPD.S178147
90. Jennings JH, Thavarajah K, Mendez MP, et al. Predischarge bundle for patients with acute exacerbations of COPD to reduce readmissions and ED visits: a randomized controlled trial. Chest. 2015;147:1227–1234. doi:10.1378/chest.14-1123
91. Epstein D, Barak-Corren Y, Isenberg Y, et al. Clinical decision support system: a pragmatic tool to improve acute exacerbation of COPD discharge recommendations. COPD. 2019;16:18–24. doi:10.1080/15412555.2019.1593342
92. Schrijver J, Lenferink A, Brusse-Keizer M, et al. Self-management interventions for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2022;1:CD002990. doi:10.1002/14651858.CD002990.pub4
93. Bhatt SP, Patel SB, Anderson EM, et al. Video telehealth pulmonary rehabilitation intervention in chronic obstructive pulmonary disease reduces 30-day readmissions. Am J Respir Crit Care Med. 2019;200:511–513. doi:10.1164/rccm.201902-0314LE
94. Pezzuto A, Carico E. Effectiveness of smoking cessation in smokers with COPD and nocturnal oxygen desaturation: functional analysis. Clin Respir J. 2020;14:29–34. doi:10.1111/crj.13096
95. Tashkin DP. Smoking cessation in chronic obstructive pulmonary disease. Semin Respir Crit Care Med. 2015;36:491–507. doi:10.1055/s-0035-1555610
96. Au DH, Bryson CL, Chien JW, et al. The effects of smoking cessation on the risk of chronic obstructive pulmonary disease exacerbations. J Gen Intern Med. 2009;24:457–463. doi:10.1007/s11606-009-0907-y
97. van Eerd EA, van der Meer RM, van Schayck OC, Kotz D. Smoking cessation for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2016;2016:CD010744. doi:10.1002/14651858.CD010744.pub2
98. Anthonisen NR, Skeans MA, Wise RA, et al. The effects of a smoking cessation intervention on 14.5-year mortality: a randomized clinical trial. Ann Intern Med. 2005;142:233–239. doi:10.7326/0003-4819-142-4-200502150-00005
99. Lu W, Aarsand R, Schotte K, et al. Tobacco and COPD: presenting the World Health Organization (WHO) tobacco knowledge summary. Respir Res. 2024;25:338. doi:10.1186/s12931-024-02961-5
100. Salvi S, Ghorpade D, Nair S, et al. A 7-point evidence-based care discharge protocol for patients hospitalized for exacerbation of COPD: consensus strategy and expert recommendation. NPJ Prim Care Respir Med. 2024;34:44. doi:10.1038/s41533-024-00378-7
101. Dumra H, Mittal S, Christopher DJ, et al. Hospital discharge protocol for patients with chronic obstructive pulmonary disease: expert consensus from India. Expert Rev Respir Med. 2025;19:1137–1147. doi:10.1080/17476348.2025.2527963
102. British Thoracic Society Reports. British Thoracic Society Pilot Care Bundle Project: a care bundles-based approach to improving standards of care in chronic obstructive pulmonary disease and community acquired pneumonia, 2014. BTS Rep 6, 4. https://www.brit-thoracic.org.uk/quality-improvement/clinical-resources/copd-spirometry.
103. Bourbeau J, Bhutani M, Hernandez P, Penz E, Marciniuk DD. Optimizing pharmacotherapy management of chronic obstructive pulmonary disease: don’t miss the forest for the trees. Am J Respir Crit Care Med. 2024;210(5):545–547. doi:10.1164/rccm.202402-0338VP
104. Janson C, Nwaru BI, Wiklund F, et al. Management and risk of mortality in patients hospitalised due to a first severe COPD exacerbation. Int J Chron Obstruct Pulmon Dis. 2020;15:2673–2682. doi:10.2147/COPD.S276819
105. Rogliani P, Manzetti GM, Cazzola M, Calzetta L. Real-world effectiveness of triple extrafine fixed-dose combination with beclomethasone/formoterol/glycopyrronium on symptoms and lung function in COPD: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2025;20:1723–1736. doi:10.2147/COPD.S511334
106. Long H, Xu H, Janssens J-P, et al. Single-inhaler triple vs single-inhaler dual therapy in patients with chronic obstructive pulmonary disease: a meta-analysis of randomized control trials. Respir Res. 2021;22(1):209. doi:10.1186/s12931-021-01794-w
107. Koarai A, Yamada M, Ichikawa T, et al. Triple versus LAMA/LABA combination therapy for patients with COPD: a systematic review and meta-analysis. Respir Res. 2021;22(1):183. doi:10.1186/s12931-021-01777-x
108. Rabe KF, Martinez FJ, Ferguson GT, et al. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N Engl J Med. 2020;383(1):35–48. doi:10.1056/NEJMoa1916046
109. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
110. Lipson DA, Crim C, Criner GJ, et al. Reduction in all-cause mortality with fluticasone furoate/umeclidinium/vilanterol in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2020;201(12):1508–1516. doi:10.1164/rccm.201911-2207OC
111. Martinez FJ, Rabe KF, Ferguson GT, et al. Reduced all-cause mortality in the ETHOS trial of budesonide/glycopyrrolate/formoterol for chronic obstructive pulmonary disease. a randomized, double-blind, multicenter, parallel-group study. Am J Respir Crit Care Med. 2021;203(5):553–564. doi:10.1164/rccm.202006-2618OC
112. Tkacz J, Evans KA, Touchette DR, et al. PRIMUS – Prompt initiation of maintenance therapy in the US: a real-world analysis of clinical and economic outcomes among patients initiating triple therapy following a COPD exacerbation. Int J Chron Obstruct Pulmon Dis. 2022;17:329–342. doi:10.2147/COPD.S347735
113. Cabrera César E, López García J, Vega Lizarazo DE, et al. Inhaled triple therapy with extrafine single inhaler versus multiple devices in chronic obstructive pulmonary disease (Tripoli): a post-authorization retrospective study. Int J Chron Obstruct Pulmon Dis. 2025;20:1737–1747. doi:10.2147/COPD.S513351
114. Halpin DMG, Rothnie KJ, Banks V, et al. Comparative adherence and persistence of single- and multiple-inhaler triple therapies among patients with chronic obstructive pulmonary disease in an english real-world primary care setting. Int J Chron Obstruct Pulmon Dis. 2022;17:2417–2429. doi:10.2147/COPD.S370540
115. Usmani OS. Choosing the right inhaler for your asthma or COPD patient. Ther Clin Risk Manag. 2019;15:461–472. doi:10.2147/TCRM.S160365
116. Baloira A, Abad A, Fuster A, et al. Lung deposition and inspiratory flow rate in patients with chronic obstructive pulmonary disease using different inhalation devices: a systematic literature review and expert opinion. Int J Chron Obstruct Pulmon Dis. 2021;16:1021–1033. doi:10.2147/COPD.S297980
117. Lavorini F, Magnan A, Dubus JC, et al. Effect of incorrect use of dry powder inhalers on management of patients with asthma and COPD. Respir Med. 2008;102:593–604. doi:10.1016/j.rmed.2007.11.003
118. Melani AS, Bonavia M, Cilenti V, et al. Inhaler mishandling remains common in real life and is associated with reduced disease control. Respir Med. 2011;105:930–938. doi:10.1016/j.rmed.2011.01.005
119. van Boven JFM, Chavannes NH, van der Molen T, Ruttenvan Mölken MPMH, Postma MJ, Vegter S. Clinical and economic impact of nonadherence in COPD: a systematic review. Respir Med. 2014;108:103–113. doi:10.1016/j.rmed.2013.08.044
120. GarciaAymerich J, Escarrabill J, Marrades RM, Monsó E, Barreiro E, Antó JM. Differences in COPD care among doctors who control the disease: general practitioner vs. pneumologist. Respir Med. 2006;100:332–339. doi:10.1016/j.rmed.2005.04.021
121. Press VG. RealWorld use of inhaled COPD medications: the good, the bad, the ugly. Chronic Obstr Pulm Dis. 2024;11:331–340. doi:10.15326/jcopdf.2024.0546
122. Hess MW. Oxygen Therapy in COPD. Respir Care. 2023;68:998–1012. doi:10.4187/respcare.10876
123. Katsenos S, Constantopoulos SH. LongTerm oxygen therapy in COPD: factors affecting and ways of improving patient compliance. Pulmonary Med. 2011;2011:325362. doi:10.1155/2011/325362
124. Stoller JK, Panos RJ, Krachman S, Doherty DE, Make B. Oxygen therapy for patients with COPD: current evidence and the longterm oxygen treatment trial. Chest. 2010;138:179–187. doi:10.1378/chest.09-2555
125. Ringbaek TJ, Viskum K, Lange P. Does longterm oxygen therapy reduce hospitalisation in hypoxaemic chronic obstructive pulmonary disease? Eur Respir J. 2002;20:38–42. doi:10.1183/09031936.02.00284202
126. Cho KH, Kim YS, Nam CM, et al. Home oxygen therapy reduces risk of hospitalisation in patients with chronic obstructive pulmonary disease: a populationbased retrospective cohort study, 20052012. BMJ Open. 2015;5:e009065. doi:10.1136/bmjopen-2015-009065
127. Mannino DM, Kiriz VA. Changing the burden of COPD mortality. Int J Chron Obstruct Pulmon Dis. 2006;1:219–233. doi:10.2147/copd.2006.1.3.219
128. Davies L, Angus RM, Calverley PM. Oral corticosteroids in patients admitted to hospital with exacerbations of chronic obstructive pulmonary disease: a prospective randomised controlled trial. Lancet. 1999;354:456–460. doi:10.1016/s0140-6736(98)11326-0
129. Niewoehner DE, Erbland ML, Deupree RH, et al. Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med. 1999;340:1941–1947. doi:10.1056/NEJM199906243402502
130. Aaron SD, Vandemheen KL, Hebert P, et al. Outpatient oral prednisone after emergency treatment of chronic obstructive pulmonary disease. N Engl J Med. 2003;348:2618–2625. doi:10.1056/NEJMoa023161
131. Wedzicha JA, Miravitlles M, Hurst JR, et al. Management of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;49. doi:10.1183/13993003.00791-2016
132. Sivapalan P, Ingebrigtsen TS, Rasmussen DB, et al. COPD exacerbations: the impact of long versus short courses of oral corticosteroids on mortality and pneumonia: nationwide data on 67,000 patients with COPD followed for 12 months. BMJ Open Respir Res. 2019;6:e000407. doi:10.1136/bmjresp-2019-000407
133. Papaporfyriou A, Bartziokas K, Gompelmann D, et al. Cardiovascular diseases in COPD: from diagnosis and prevalence to therapy. Life. 2023;13:1299. doi:10.3390/life13061299
134. Morgan AD, Zakeri R, Quint JK. Defining the relationship between COPD and CVD: what are the implications for clinical practice? Ther Adv Respir Dis. 2018;12:1753465817750524. doi:10.1177/1753465817750524
135. Anthonisen NR, Connett JE, Kiley JP, et al. Effects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1: the Lung Health Study. JAMA. 1994;272:1497–1505. doi:10.1001/jama.1994.03520190043033
136. MacDonald MI, Shafuddin E, King PT, et al. Cardiac dysfunction during exacerbations of chronic obstructive pulmonary disease. Lancet Respir Med. 2016;4:138–148. doi:10.1016/S2213-2600(15)00509-3
137. Maclagan LC, Croxford R, Chu A, et al. Quantifying COPD as a risk factor for cardiac disease in a primary prevention cohort. Eur Respir J. 2023;62:2202364. doi:10.1183/13993003.02364-2022
138. Mannino DM, Thorn D, Swensen A, Holguin F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. 2008;32:962–969. doi:10.1183/09031936.00012408
139. Kunisaki KM, Dransfield MT, Anderson JA, et al. Exacerbations of chronic obstructive pulmonary disease and cardiac events. A post hoc cohort analysis from the summit randomized clinical trial. Am J Respir Crit Care Med. 2018;198:51–57. doi:10.1164/rccm.201711-2239OC
140. Rao S, Nazarzadeh M, Li Y, et al. Systolic blood pressure, chronic obstructive pulmonary disease and cardiovascular risk. Heart. 2023. doi:10.1136/heartjnl-2023-322431
141. Ben Halima M, Saidane A, Boudiche S, et al. Hypertension: a trigger or a consequence of exacerbations in COPD? Arch Cardiovasc Dis Suppl. 2019;11:102. doi:10.1016/j.acvdsp.2018.10.225
142. Chen W, Thomas J, Sadatsafavi M, FitzGerald JM. Risk of cardiovascular comorbidity in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Lancet Respir Med. 2015;3:631–639. doi:10.1016/S2213-2600(15)00241-6
143. Müllerova H, Agusti A, Erqou S, Mapel DW. Cardiovascular comorbidity in COPD: systematic literature review. Chest. 2013;144:1163–1178. doi:10.1378/chest.12-2847
144. Higashimoto Y, Yamagata T, Maeda K, et al. Influence of comorbidities on the efficacy of pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Geriatr Gerontol Int. 2016;16:934–941. doi:10.1111/ggi.12575
145. Battaglia S, Basile M, Scichilone N, Bellia V. Prevalence of comorbidities and severity of COPD. COPD. 2015;12:390–394. doi:10.3109/15412555.2014.974734
146. Wakabayashi K, Gonzalez MA, Delhaye C, et al. Impact of chronic obstructive pulmonary disease on acute-phase outcome of myocardial infarction. Am J Cardiol. 2010;106:305–309. doi:10.1016/j.amjcard.2010.03.026
147. Sidney S, Sorel M, Quesenberry CP, et al. COPD and incident cardiovascular disease hospitalizations and mortality: Kaiser Permanente Medical Care Program. Chest. 2005;128:2068–2075. doi:10.1378/chest.128.4.2068
148. Pirina P, Martinetti M, Spada C, et al. Prevalence and management of COPD and heart failure comorbidity in the general practitioner setting. Respir Med. 2017;131:1–5. doi:10.1016/j.rmed.2017.07.059
149. Hesse K, Bourke S, Steer J. Heart failure in patients with COPD exacerbations: looking below the tip of the iceberg. Respir Med. 2022;196. doi:10.1016/j.rmed.2022.106800
150. Almagro P, Cabrera FJ, Diez J, et al. Comorbidities and Shortterm Prognosis in Patients Hospitalized for Acute Exacerbation of COPD: the EPOC en Servicios de Medicina Interna (ESMI) Study. Chest. 2012;142:1126–1133. doi:10.1378/chest.11-2413
151. Mentz RJ, Fiuzat M, Wojdyla DM, et al. Clinical characteristics and outcomes of hospitalized heart failure patients with systolic dysfunction and chronic obstructive pulmonary disease: findings from OPTIMIZEHF. Eur J Heart Fail. 2012;14:395–403. doi:10.1093/eurjhf/hfs009
152. Matamis D, Tsagourias M, Papathanasiou A, et al. Targeting occult heart failure in intensive care unit patients with acute chronic obstructive pulmonary disease exacerbation: effect on outcome and quality of life. J Crit Care. 2014;29:315.e7–315.e14. doi:10.1016/j.jcrc.2013.11.011
153. Kitzman DW, Gardin JM, Gottdiener JS, et al. Importance of heart failure with preserved systolic function in patients ≥65 years of age. Am J Cardiol. 2001;87:413–419. doi:10.1016/S0002-9149(00)01393-X
154. Kwon BJ, Kim DB, Jang SW, et al. Prognosis of heart failure patients with reduced and preserved ejection fraction and coexistent chronic obstructive pulmonary disease. Eur J Heart Fail. 2010;12:1339–1344. doi:10.1093/eurjhf/hfq157
155. EhteshamiAfshar S, Mooney L, Dewan P, et al. Clinical characteristics and outcomes of patients with heart failure with reduced ejection fraction and chronic obstructive pulmonary disease: insights from PARADIGMHF. J Am Heart Assoc. 2021;10:e019238. doi:10.1161/JAHA.120.019238
156. Lee H, Jhun BW, Cho J, et al. Different impacts of respiratory symptoms and comorbidities on COPDspecific healthrelated quality of life by COPD severity. Int J Chron Obstruct Pulmon Dis. 2017;12:3301–3310. doi:10.2147/COPD.S145910
157. Almagro P, Calbo E, Ochoa de Echaguïen A, et al. Mortality after hospitalization for COPD. Chest. 2002;121:1441–1448. doi:10.1378/chest.121.5.1441
158. Axson EL, Ragutheeswaran K, Sundaram V, et al. Hospitalisation and mortality in patients with comorbid COPD and heart failure: a systematic review and meta-analysis. Respir Res. 2020;21:54. doi:10.1186/s12931-020-1312-7
159. Canepa M, StraburzynskaMigaj E, Drozdz J, et al. Characteristics, treatments and 1year prognosis of hospitalized and ambulatory heart failure patients with chronic obstructive pulmonary disease in the European Society of Cardiology Heart Failure LongTerm Registry. Eur J Heart Fail. 2018;20:100–110. doi:10.1002/ejhf.964
160. Du Q, Sun Y, Ding N, Lu L, Chen Y. Betablockers reduced the risk of mortality and exacerbation in patients with COPD: a metaanalysis of observational studies. PLoS One. 2014;9:e113048. doi:10.1371/journal.pone.0113048
161. Ponikowski P, Voors AA, Anker SD, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Eur Heart J. 2016;37:2129–2200. doi:10.1093/eurheartj/ehw128
162. Yang YL, Xiang ZJ, Yang JH, Wang WJ, Xu ZC, Xiang RL. Association of βblocker use with survival and pulmonary function in patients with chronic obstructive pulmonary and cardiovascular disease: a systematic review and meta-analysis. Eur Heart J. 2020;41:4415–4422. doi:10.1093/eurheartj/ehaa793
163. GBD 2017 Causes of Death Collaborators. Global, regional, and national agesexspecific mortality for 282 causes of death in 195 countries and territories, 19802017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392:1736–1788. doi:10.1016/S0140-6736(18)32203-7
164. Lee H, Shin SH, Gu S, et al. Racial differences in comorbidity profile among patients with chronic obstructive pulmonary disease. BMC Med. 2018;16:178. doi:10.1186/s12916-018-1159-7
165. Sin DD, Anthonisen NR, Soriano JB, A.g A. Mortality in COPD: role of comorbidities. Eur Respir J. 2006;28:1245–1257. doi:10.1183/09031936.00133805
166. Santos NCD, Miravitlles M, Camelier AA, Almeida VDC, Maciel RRBT, Camelier FWR. Prevalence and impact of comorbidities in individuals with chronic obstructive pulmonary disease: a systematic review. Tuberc Respir Dis. 2022;85:205–220. doi:10.4046/trd.2021.0179
167. Jo YS. LongTerm outcome of chronic obstructive pulmonary disease: a review. Tuberc Respir Dis. 2022;85:289–301. doi:10.4046/trd.2022.0074
168. Putcha N, Drummond MB, Wise RA, Hansel NN. Comorbidities and chronic obstructive pulmonary disease: prevalence, influence on outcomes, and management. Semin Respir Crit Care Med. 2015;36:575–591. doi:10.1055/s-0035-1556063
169. Mapel D. Insights into COPD comorbidities from the OLIN study and other large databases. COPD. 2011;8:397–399. doi:10.3109/15412555.2011.636555
170. Mapel DW, Dedrick D, Davis K. Trends and cardiovascular comorbidities of COPD patients in the veterans administration medical system, 1991–1999. COPD. 2005;2:35–41. doi:10.1081/COPD-200050671
171. Almagro P, López García F, Cabrera FJ, et al. Comorbidity and genderrelated differences in patients hospitalized for COPD. The ECCO study. Respir Med. 2010;104:253–259. doi:10.1016/j.rmed.2009.09.019
172. Dalal AA, Shah M, Lunacsek O, et al. Clinical and economic burden of patients diagnosed with COPD with comorbid cardiovascular disease. Respir Med. 2011;105:1516–1522. doi:10.1016/j.rmed.2011.04.005
173. Franssen FME, Soriano JB, Roche N, et al. Lung function abnormalities in smokers with ischemic heart disease. Am J Respir Crit Care Med. 2016;194:568–576. doi:10.1164/rccm.201512-2480OC
174. Meng K, Zhang X, Liu W, et al. Prevalence and impact of chronic obstructive pulmonary disease in ischemic heart disease: a systematic review and metaanalysis of 18 million patients. COPD. 2024;19:2333–2345. doi:10.2147/COPD.S474223
175. Kim BG, Lee H, Kang MG, et al. Risk of ischemic heart disease in chronic obstructive pulmonary disease: a nationwide cohort study. J Korean Med Sci. 2023;38:e344. doi:10.3346/jkms.2023.38.e344
176. Feary JR, Rodrigues LC, Smith CJ, et al. Prevalence of major comorbidities in subjects with COPD and incidence of myocardial infarction and stroke: a comprehensive analysis using data from primary care. Thorax. 2010. doi:10.1136/thx.2009.128082
177. Schneider C, Bothner U, Jick SS, et al. Chronic obstructive pulmonary disease and the risk of cardiovascular diseases. Eur J Epidemiol. 2010;25:253–260. doi:10.1007/s10654-010-9435-7
178. Rothnie KJ, Smeeth L, Herrett E, et al. Closing the mortality gap after a myocardial infarction in people with and without chronic obstructive pulmonary disease. Heart. 2015. doi:10.1136/heartjnl-2014-307251
179. Yin L, Lensmar C, Ingelsson E, et al. Differential association of chronic obstructive pulmonary disease with myocardial infarction and ischemic stroke in a nationwide cohort. Int J Cardiol. 2014;173:601–603. doi:10.1016/j.ijcard.2014.03.140
180. Liu X, Chen Z, Li S, et al. Association of chronic obstructive pulmonary disease with arrhythmia risks: a systematic review and meta analysis. Front Cardiovasc Med. 2021;8:732349. doi:10.3389/fcvm.2021.732349
181. Ebihara A, Nagai A, Imamura N, et al. Evaluation of arrhythmia frequency in patients with COPD. Eur Respir J. 2015;46. doi:10.1183/13993003.congress-2015.PA3657
182. Coleman KM, Varrias D, Wolf E, et al. Unrecognized actionable cardiac arrhythmias in patients with moderate to severe chronic obstructive pulmonary disease: can continuous monitoring unmask the culprit. Respir Med. 2025;245:108190. doi:10.1016/j.rmed.2025.108190
183. Desai R, Patel U, Singh S, et al. The burden and impact of arrhythmia in chronic obstructive pulmonary disease: insights from the National Inpatient Sample. Int J Cardiol. 2019;281:49–55. doi:10.1016/j.ijcard.2019.01.074
184. Roversi S, Fabbri LM, Sin DD, et al. Chronic obstructive pulmonary disease and cardiac diseases. an urgent need for integrated care. Am J Respir Crit Care Med. 2016;194:1319–1336. doi:10.1164/rccm.201604-0690SO
185. RodríguezMañero M, LópezPardo E, Cordero A, et al. A prospective study of the clinical outcomes and prognosis associated with comorbid COPD in the atrial fibrillation population. Int J Chron Obstruct Pulmon Dis. 2019;14:371–380. doi:10.2147/COPD.S174443
186. Curkendall SM, deLuise C, Jones JK, et al. Cardiovascular disease in patients with chronic obstructive pulmonary disease, Saskatchewan Canada: Cardiovascular disease in COPD patients. Ann Epidemiol. 2006;16:63–70. doi:10.1016/j.annepidem.2005.04.008
187. Konecny T, Park JY, Somers KR, et al. Relation of chronic obstructive pulmonary disease to atrial and ventricular arrhythmias. Am J Cardiol. 2014;114:272–277. doi:10.1016/j.amjcard.2014.04.030
188. Ding N, Qiu W, Chen J, et al. Prevalence and risk factors of arrhythmias in patients with acute exacerbations of chronic obstructive pulmonary disease: a systematic review and meta analysis. COPD. 2025;20:3059–3072. doi:10.2147/COPD.S545658
189. Steer J, Gibson J, Bourke SC. The DECAF Score: predicting hospital mortality in exacerbations of chronic obstructive pulmonary disease. Thorax. 2012. doi:10.1136/thoraxjnl-2012-202103
190. Echevarria C, Steer J, HeslopMarshall K, et al. Validation of the DECAF score to predict hospital mortality in acute exacerbations of COPD. Thorax. 2016. doi:10.1136/thoraxjnl-2015-207775
191. Onishi K. Total management of chronic obstructive pulmonary disease (COPD) as an independent risk factor for cardiovascular disease. J Cardiol. 2017;70:128–134. doi:10.1016/j.jjcc.2017.03.001
192. Barrett TW, Self WH, Jenkins CA, et al. Predictors of regional variations in hospitalizations following emergency department visits for atrial fibrillation. Am J Cardiol. 2013;112:1410–1416. doi:10.1016/j.amjcard.2013.07.005
193. Kaszuba M, Śliwka A, Piliński R, et al. The comorbidity of chronic obstructive pulmonary disease and peripheral artery disease – a systematic review. COPD. 2019;16:292–302. doi:10.1080/15412555.2019.1653271
194. Terzikhan N, Lahousse L, Verhamme KMC, et al. COPD is associated with an increased risk of peripheral artery disease and mortality. ERJ Open Res. 2018;4:00086–02018. doi:10.1183/23120541.00086-2018
195. HoubenWilke S, Jörres RA, Bals R, et al. Peripheral artery disease and its clinical relevance in patients with chronic obstructive pulmonary disease in the COPD and systemic consequences–comorbidities network study. Am J Respir Crit Care Med. 2017;195:189–197. doi:10.1164/rccm.201602-0354OC
196. Tuleta I, Farrag T, Busse L, et al. High prevalence of COPD in atherosclerosis patients. Int J Chron Obstruct Pulmon Dis. 2017;12:3047–3053. doi:10.2147/COPD.S141988
197. Kaszuba M, Kościelniak J, Śliwka A, et al. The prevalence of chronic obstructive pulmonary disease in hospitalized tobacco smokers with peripheral artery disease. Vasa. 2025;54:91–98. doi:10.1024/0301-1526/a001168
198. Bethel M, Annex BH. Peripheral arterial disease: a small and large vessel problem. Am Heart J Plus. 2023;28:100291. doi:10.1016/j.ahjo.2023.100291
199. Keller K, Hobohm L, Münzel T, et al. Impact of chronic obstructive pulmonary disease on the outcomes of patients with peripheral artery disease. Respir Med. 2019;147:1–6. doi:10.1016/j.rmed.2018.12.010
200. Ji Z, JareñoEsteban JJ, de MiguelDíez J. Role of vaccines in COPD patients. Open Respir Arch. 2022;4:100191. doi:10.1016/j.opresp.2022.100191
201. BekkatBerkani R, Wilkinson T, Buchy P, et al. Seasonal influenza vaccination in patients with COPD: a systematic literature review. BMC Pulm Med. 2017;17:79. doi:10.1186/s12890-017-0420-8
202. Collins PF, Yang IA, Chang Y-C, Vaughan A. Nutritional support in chronic obstructive pulmonary disease (COPD): an evidence update. J Thorac Dis. 2019;11:S2230–S2237. doi:10.21037/jtd.2019.10.41
203. Deng M, Lu Y, Zhang Q, et al. Global prevalence of malnutrition in patients with chronic obstructive pulmonary disease: systemic review and meta-analysis. Clin Nutr. 2023;42:848–858. doi:10.1016/j.clnu.2023.04.005
204. Collins PF, Elia M, Stratton RJ. Nutritional support and functional capacity in chronic obstructive pulmonary disease: a systematic review and metaanalysis. Respirology. 2013;18:616–629. doi:10.1111/resp.12070
205. Collins PF, Stratton RJ, Elia M. Nutritional support in chronic obstructive pulmonary disease: a systematic review and metaanalysis. Am J Clin Nutr. 2012;95:1385–1395. doi:10.3945/ajcn.111.023499
206. Malnutrition Universal Screening Tool’ (‘MUST’). Available from: https://www.bapen.org.uk/must-and-self-screening/introducing-must/.
207. Fekete M, Csípő T, Fazekas-Pongor V, et al. The possible role of food and diet in the quality of life in patients with COPD-A state-of-the-art review. Nutrients. 2023;15:3902. doi:10.3390/nu15183902
208. Snider JT, Jena AB, Linthicum MT, et al. Effect of hospital use of oral nutritional supplementation on length of stay, hospital cost, and 30-day readmissions among Medicare patients with COPD. Chest. 2015;147:1477–1484. doi:10.1378/chest.14-1368
209. Riley K, Sulo S, Dabbous F, et al. Reducing hospitalizations and costs: a home health nutrition-focused quality improvement program. JPEN J Parenter Enteral Nutr. 2020;44:58–68. doi:10.1002/jpen.1606
210. Steiner MC, Barton RL, Singh SJ, et al. Nutritional enhancement of exercise performance in chronic obstructive pulmonary disease: a randomised controlled trial. Thorax. 2003;58:745–751. doi:10.1136/thorax.58.9.745
211. Schols AM, Soeters PB, Mostert R, et al. Physiologic effects of nutritional support and anabolic steroids in patients with chronic obstructive pulmonary disease. A placebo-controlled randomized trial. Am J Respir Crit Care Med. 1995;152:1268–1274. doi:10.1164/ajrccm.152.4.7551381
212. McDonald VM, Gibson PG, Scott HA, et al. Should we treat obesity in COPD? The effects of diet and resistance exercise training. Respirology. 2016;21:875–882. doi:10.1111/resp.12746
213. Barker RE, Kon SS, Clarke SF, et al. COPD discharge bundle and pulmonary rehabilitation referral and uptake following hospitalisation for acute exacerbation of COPD. Thorax. 2021;76(8):829–831. doi:10.1136/thoraxjnl-2020-215464
214. Jenkins AR, Burtin C, Camp PG, et al. Do pulmonary rehabilitation programmes improve outcomes in patients with COPD posthospital discharge for exacerbation: a systematic review and metaanalysis. Thorax. 2024;79:438–447. doi:10.1136/thorax-2023-220333
215. Stefan MS, Pekow PS, Priya A, et al. Association between Initiation of Pulmonary Rehabilitation and Rehospitalizations in Patients Hospitalized with Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2021;204:1015–1023. doi:10.1164/rccm.202012-4389OC
216. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188:e13–e64. doi:10.1164/rccm.201309-1634ST
217. Wedzicha JA, Calverley PMA, Albert RK, et al. Prevention of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;50. doi:10.1183/13993003.02265-2016
218. Spitzer KA, Stefan MS, Priya A, et al. Participation in pulmonary rehabilitation after hospitalization for chronic obstructive pulmonary disease among medicare beneficiaries. Ann Am Thorac Soc. 2019;16:99–106. doi:10.1513/AnnalsATS.201805-332OC
219. Bartels W, Adamson S, Leung L, et al. Emergency department management of acute exacerbations of chronic obstructive pulmonary disease: factors predicting readmission. Int J Chron Obstruct Pulmon Dis. 2018;13:1647–1654. doi:10.2147/COPD.S163250
220. Hartman M, Mináriková J, Batalik L, et al. Effects of home-based training with internet telehealth guidance in COPD patients entering pulmonary rehabilitation: a systematic review. COPD. 2023;18:2305–2319. doi:10.2147/COPD.S425218
221. Rea H, Kenealy T, Adair J, Robinson E, Sheridan N. Spirometry for patients in hospital and one month after admission with an acute exacerbation of COPD. Int J Chron Obstruct Pulmon Dis. 2011;6:527–532. doi:10.2147/COPD.S24133
222. Loh CH, Genese FA, Kannan KK, et al. Spirometry in hospitalized patients with acute exacerbation of COPD accurately predicts post discharge airflow obstruction. Chronic Obstr Pulm Dis. 2018;5:124–133. doi:10.15326/jcopdf.5.2.2017.0169
223. Solano JP, Gomes B, Higginson IJ. A comparison of symptom prevalence in far advanced cancer, AIDS, heart disease, chronic obstructive pulmonary disease and renal disease. J Pain Symptom Manage. 2006;31:58–69. doi:10.1016/j.jpainsymman.2005.06.007
224. Yazdanyar A, Vojtek A, Gupta S, et al. Association between inpatient palliative care encounter and 30-day all-cause readmissions after index hospitalization for chronic obstructive pulmonary disease. Heart Lung. 2023;58:69–73. doi:10.1016/j.hrtlng.2022.11.003
225. Yazdanyar A, Guthier D, Maitz T, et al. Inpatient palliative care encounter and 30-day readmission among hospitalizations for heart failure. Future Cardiol. 2022;18:809–816. doi:10.2217/fca-2022-0041
226. Brian Cassel J, Kerr KM, McClish DK, et al. Effect of a home-based palliative care program on healthcare use and costs. J Am Geriatr Soc. 2016;64:2288–2295. doi:10.1111/jgs.14354
227. Vermylen JH, Szmuilowicz E, Kalhan R. Palliative care in COPD: an unmet area for quality improvement. Int J Chron Obstruct Pulmon Dis. 2015;10:1543–1551. doi:10.2147/COPD.S74641
228. Iyer AS, Sullivan DR, Lindell KO, et al. The role of palliative care in COPD. Chest. 2022;161:1250–1262. doi:10.1016/j.chest.2021.10.032
229. Halpin DMG. Palliative care for people with COPD: effective but underused. Eur Respir J. 2018;51:1702645. doi:10.1183/13993003.02645-2017
230. Tavares N, Jarrett N, Hunt K, et al. Palliative and end-of-life care conversations in COPD: a systematic literature review. ERJ Open Res. 2017;3:00068–2016. doi:10.1183/23120541.00068-2016
231. Tsiligianni I, Papageorgakopoulou S, Bouloukaki I. Adherence to the Chronic Obstructive Pulmonary Disease guidelines in primary care: the Greek COPD COCARE study. Respir Med. 2025;248:108345. doi:10.1016/j.rmed.2025.108345
232. Lennox L, Green S, Howe C, et al. Identifying the challenges and facilitators of implementing a COPD care bundle. BMJ Open Respir Res. 2014;1:e000035. doi:10.1136/bmjresp-2014-000035
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.