Back to Journals » Risk Management and Healthcare Policy » Volume 16
A Prognostic Study for the Development of Risk Prediction Model for the Success of Vaginal Birth Following a Cesarean Surgery at Felege Hiwot Comprehensive Specialized Hospital, Northwest Ethiopia
Authors Mesay F ![]() , Melese ES
, Melese ES ![]() , Wudie G, Feleke SF
, Wudie G, Feleke SF ![]() , Dessie AM
, Dessie AM ![]()
Received 29 October 2022
Accepted for publication 11 January 2023
Published 20 January 2023 Volume 2023:16 Pages 55—68
DOI https://doi.org/10.2147/RMHP.S395388
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Filipos Mesay,1 Ergoye Melese,2 Gebiyaw Wudie,2 Sefineh Fenta Feleke,3 Anteneh Mengist Dessie4
1Department of Public Health, Gafat Health Center, Debre Tabor, Ethiopia; 2Department of Epidemiology and Biostatistics, School of Public Health, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia; 3Department of Public Health, College of Health Sciences, Woldia University, Woldia, Ethiopia; 4Department of Public Health, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia
Correspondence: Sefineh Fenta Feleke; Filipos Mesay, Tel +251928573882 ; Tel +251984929331, Email [email protected]; [email protected]
Background: An attempt at vaginal delivery by a woman who has previously had a cesarean section is known as a trial of labor after cesarean section. The most important issues are how to accurately anticipate successful vaginal birth after cesarean surgery and how to calculate the likelihood of success of vaginal birth after caesarean section that is suitable for women. Consequently, a tailored prediction of vaginal birth after caesarean section may result in a more effective counseling.
Objective: To create a clinical risk score and prediction model for the success of vaginal birth following a previous caesarean section in women.
Methods: A prognostic analysis was carried out at Felege Hiwot Comprehensive and Specialized Referral Hospital from 30 February 2017 to 30 March 2021. R statistical programming language version 4.0 was used for analysis once the data had been coded and entered into Epidata, version 3.02. Significant factors (P< 0.05) were kept in the backward multivariable logistic regression model, and variables with (P< 0.25) from the bi-variable logistic regression analysis were also added.
Results: After a cesarean section, 67% of women were successful in giving birth vaginally. Previous successful vaginal birth after cesarean surgery, rupture of the membranes, and initiation time of ANC, the beginning of labor, parity and time since the previous delivery were remained in the final multivariable prediction model. The AUC of the model was 0.748 (95% CI: 0.714– 0.781).
Conclusion: Overall, this study demonstrated the likelihood of predicting vaginal birth utilizing the ideal confluence of parity, membrane rupture, and onset of labor, prior history of VBAC, inter-delivery gap, and ANC beginning time. Sixty-seven percent of VBACs were successful. As a result, this model may aid in identifying pregnant women who are candidates for VBAC and who have a better likelihood of success.
Keywords: prediction model, vaginal birth after cesarean section, risk score, Ethiopia
Introduction
A woman who has previously undergone a caesarean section is said to be in a trial of labor after the procedure.1 In 1981, vaginal birth after a low transverse Caesarean delivery was acknowledged as a secure and respectable option.2 One of the most significant advancements in obstetric practice recently is the trial of labor following cesarean birth, which is seen as a vital strategy for lowering the rate of cesarean deliveries.3
If there are no contraindications, women with uterine scars should consider trying to give birth naturally instead of having a cesarean section. In most situations, a successful VBAC is safe for both the mother and the baby.4 In March 2010, the National Institutes of Health Consensus Development Conference Panel issued a statement on VBAC. In order to make an informed choice, it was underlined that expectant mothers who had had a previous cesarean should obtain the proper counseling regarding VBAC versus elective repeat cesarean. This counseling would probably involve a personal risk-benefit analysis of labor trial and the chance of a successful VBAC.5
Recent research indicates that VBAC is associated with less blood loss during delivery, a shorter hospital stays, a decrease in the need for blood transfusions, and a decrease in the frequency of intrapartum and postpartum infections and thromboembolic events. An increase in the rate of VBAC would reduce the financial burden on both nations and individuals.5
As if VBAC has many advantages for women with previous cesarean section, it has also its own complication if women’s who are candidate for VBAC were not selected appropriately. Different scholars stated those complications that were related with VBAC. Women who experience failure after VBAC have the highest morbidity. Due to this, women who do not have any contraindications should think about trying labor following CS.6 Successful VBAC, however, is linked to less blood loss, a significantly lower risk of neonatal respiratory morbidities and placenta previa, a shorter hospital stay, and a quicker recovery. Major complications linked to failed VBAC include scar dehiscence, hysterectomy and uterine rupture, death, neonatal respiratory morbidity, and mortality.7
The most important issues are how to accurately anticipate successful vaginal birth after cesarean surgery and how to calculate the likelihood of success of VBAC that is suitable for women. Consequently, a tailored prediction of VBAC may result in a more effective counseling. A more precise forecast of the results of a maternal VBAC may not only help clinician’s advice patients on the mode of delivery to use but also help them avoid complications. There are models that aid in predicting VABC.8–10 Although most of the prediction models were created using non-African populations, because of the disparities in obstetrical policies and the completely diverse mix of ethnicities, these models cannot be directly applied to African contexts without risking the models’ performance and validity.11 Women are advised based on medical professionals’ experiences and data from other nations without population-validated and evidence-based calculators for successful TOLAC, which may result in skewed judgments.
As a result, this research developed a prediction model and clinical risk score for vaginal delivery after a cesarean section for use in today’s doctor-patient joint decision-making regarding vaginal birth after a cesarean section. Physicians have an evidence-based tool to aid in patient counseling and risk classification through the use of trial of labor after cesarean delivery calculators, which predict the success of vaginal birth following cesarean delivery.
Methods
Study Area and Period
The study’s participants were women who gave birth at the Felege Hiwot Comprehensive Specialized Hospital (FHCSH), which is situated in Bahir Dar, the capital of the Amhara National Regional State, 575 kilometers northwest of Addis Ababa.
Felege Hiwot Comprehensive specialized hospital, one of the nation’s oldest public hospitals, was established in April 1963 G.C. with the assistance of the German State government, under the reign of Emperor H/Selassie I. It is located in the northern part of the city, next to Lake Tana, and strives to create a prosperous, healthy society and a center of superior medical care by the year 2029. Plans for the initial construction provided space for 25,000 people. Currently, Bahir Dar city, the west and east Gojjam zones, the Awi zone, the north and south Wollo zones, the south and north Gondar zones, some portions of the Benishangul Gumuz, and more than 10 million people receive its services. There are now 1431 employees working for the hospital in a variety of occupations, including 5 obstetricians and gynecologists and 63 midwives. It has 500 formal beds in total, 11 wards (including emergency wards and inpatient wards for gynecological and obstetric, orthopedic, medical, pediatric, L&D, eye unit, NICU, psychiatrics, oncology, and 22 OPDS), 39 clinical and nonclinical departments/service units, and provides services for disease prevention and health promotion in addition to laboratory, diagnostic, curative, and rehabilitation needs.12
Study Design
A retrospective follow-up study design was carried out. The current study’s theoretical foundation was based on the likelihood of a successful vaginal delivery following a cesarean section as a function of several markers of current and previous obstetric history.
Reference Population
All pregnant mothers who have previously undergone cesarean sections and are candidates for VBAC made up the study’s domain.
Study Population
All expectant mothers who attempted a VBAC at the FHCSH between February 30, 2017, and March 30, 2021, and who were candidates for a VBAC.
Study Unit
Selected cards of those mothers who gave birth at FHCSH from February 30/2017 to March 30/2020.
The Inclusion and Exclusion Criteria
Inclusion Criteria
Mothers who have recorded data and tried VBAC at FHCRH from February 30/2019 to March 30/2021.
Exclusion Criteria
Mothers who had no recorded data in Felege Hiwot comprehensive and referral hospital.
Mothers who were referred to Felege Hiwot Comprehensive and Referral Hospital after having a cesarean section but did not try for a vaginal delivery as well as mothers who had had more than one prior cesarean section.
Research Variables
Outcome Variable
Success of vaginal birth after cesarean surgery (it categorized as successful VBAC and failed VBAC).
Independent Variables
Demographic and socioeconomic data: Age, marital status, and level of education of the patient.
Previous obstetric history: parity, previous vaginal deliveries, previous history of successful VBAC, previous cesarean indication, parity, and chronic diseases.
Current obstetrical information: gestation age by date, mode of labor induction, bishop score on admission, augmentation, onset of labor, rupture of membrane, place of ANC, initiation time of ANC, estimated fetal weight and inter-delivery time from previous delivery.
The independent variables will be used as the predictors for the outcomes of VBAC; they were analyzed by cross tabulations to determine which amongst these are significant.
Operational Definitions of the Variables
VBAC Success: was characterized in this study as the spontaneous or aided vaginal delivery of the fetus, regardless of neonatal and maternal problems.
Cesarean section: is a procedure used to deliver a baby by uterine incision.
Not successful VBAC: is described as the inability of women having a TOLAC to give birth vaginally following a caesarean section, with the delivery terminating in an emergency CS.
Sample Size Determination
Based on the assumption of the rule of thumb, the sample size was computed. First, for each putative VBAC predictor that was assessed in the multi-variable regression analysis, at least 10 occurrences were gathered.13 N is the sample size, n is the number of potential predictor variables, and I is the anticipated event rate in the population. According to the formula, N = (n 10)/I.14 However, I utilized 15 events for each predictor to increase statistical power. In the context of this study, an event is defined as the least frequent outcome status of a failed vaginal birth following a cesarean section. According to a study conducted in the teaching hospitals of Addis Ababa University, 32% of VBAC attempts fail.15 At least 225 events must occur in order to create a model with 15 possible predictors, hence the sample size changed to 15*15/.32%=700.
Sampling Method and Procedures
In Figure 1, a simple random sampling procedure was used to choose participants by using medical registration number of delivered mother from delivery registration book. First all mother with previous cesarean section delivered at FHCSH from February 30/2017 to March 30/20201 was identified from the delivery registration book. After those records of mothers who meet the inclusion criteria was included in the study. Subsequently, a sampling frame was prepared. Finally, study unit was selected by using computer generated random number.
 |
Figure 1 Schematic representation of sampling technique at FHCSH Northeast Ethiopia. |
The primary source of information was the outpatient department’s admittance record books, where the card numbers of patients admitted with prior cesarean scars could be located. Then, to determine which women had been offered VBAC, ward discharge reports and delivery log books were used. Participants were selected from the available charts during the study periods by the use of systematic random sampling up until the sample size was met.
Data Quality Control
Data collectors and supervisors received training on the goal of the study, how to gather data, how to store that data, and how to oversee the data collection process. After that, a pretest was conducted on 5% of the sample size to ensure that the data collectors and supervisors were qualified to oversee and collect data. English was used to develop the checklist.
Data Processing and Analysis
R software 4.0 was used to do statistical analysis after importing the data into Epidata 3.02. The relationship between each predictor and the success of VBAC was investigated using binary logistic regression. Variables from the binary logistic regression analysis that were significant (P< 0.05) were kept in the multiple logistic regression models, and variables with (P< 0.25) were also added. Coefficients, odds ratios (ORs), and 95% confidence intervals (CIs) were used to report the outcomes of important predictors (CI). By computing the area under the ROC curve (AUC), sensitivity, and specificity, the discrimination was evaluated. The Hosmer Lemeshow goodness-of-fit statistic and calibration graphs of the observed and projected success rates of VBAC were created. Internal validation of the model was calculated by bootstrapping 1000 samples with replacement.
Model Development and Validation
To gain understanding of the relationship between each potential predictor and the success of VBAC, bivariate logistic regression was conducted for model creation. In a backward stepwise multivariable logistic regression model, significant variables (P< 0.05) were kept, while variables with (P< 0.25) from the bivariate analysis were added. Significant predictors’ outcomes were presented as coefficients with 95% confidence intervals (CI).
We calculated the calibration plot and area under the ROC curve using the R “classifier plots” and “givitiR” packages, respectively, to evaluate the model’s accuracy and goodness-of-fit. The AUC had a range of 0.5 (no predictive power) to 1. Using the bootstrapping technique, the regression coefficients, their 95% confidence intervals, and the AUC will be corrected for overfitting or over optimism. Internal validation was performed by computing 1000 random bootstrap samples with replacement for all predictors in the data. The model’s predictive performance after bootstrapping is considered as the performance that can be expected when the model is applied to future similar populations.
We used standardized net benefit over a range of threshold probabilities to undertake a decision curve analysis (DCA) to assess the model’s effects on clinical and public health (0 to 1). The model was evaluated in the DCA against two extreme cases: “intervention for everyone” and “no intervention.”
In our case, the intervention took into account choosing moms who are candidates for full VBAC success in order to facilitate optimal selection of mothers and lower the risk of complications, morbidity, and death associated with repeated cesarean procedures.
Risk Score Development
We converted each model coefficient to a rounded number by dividing to the lowest coefficient in order to create a TOLAC prediction score that is simple to use. Following that, the number of points was rounded to the nearest integer. Each person’s overall score was calculated by allocating points for each variable that was present and then adding those scores together. For reasons of statistical stability and practical usability, the anticipated chance of a VBAC’s success was reported according to two risk score categories, allowing each pregnant woman to be categorized as having a high or low risk of succeeding.
Ethical Consideration
At Bahir Dar University’s College of Medicine and Health Sciences, the Institutional Review Board (IRB) with reference number 080/2021 granted ethical permission. The hospital management was requested to provide oral informed consent after receiving a formal letter of cooperation from us. Personal identities were not utilized on the data gathering checklist because it is retrospective research of medical records. Therefore, the IRB decided not to require each participant to provide informed consent. The study complies in any way with the Helsinki Declaration’s basic principles. All information was gathered from the register, which was held in a secure location, and was completely anonymized before we had access to it and any of research participants were above the age of 18 years. After data collection, all patient cards and records were put back in a safe location. For ethical considerations, data were not disclosed to anyone but the authors. A password-protected computer was used to enter all of the data.
Result
Societal and Demographic Characteristics
Out of a total of 700 research cards, 469 (89%) belonged to the 35 and under age group. Mothers in 579 (82.7%) had at least a high school diploma and 679 (97%) were married (Table 1).
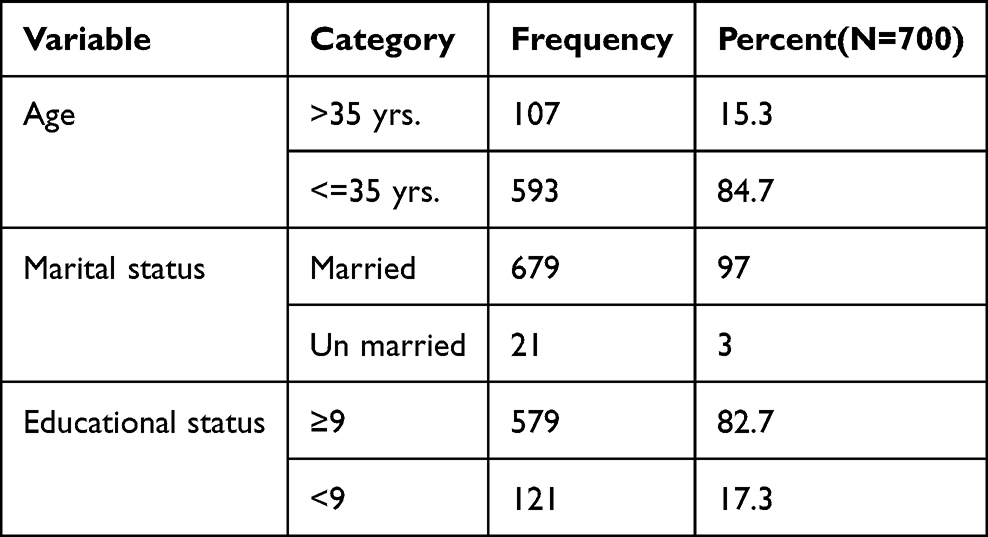 |
Table 1 Societal and Demographic Characteristics of Mothers, Who Was Candidate for VBAC, Gave Birth at FHCSH from January 30/2017 to January 30/2021 |
Maternal Obstetric Related Factors
In (Table 2) the total of mothers who delivered at FHCSH 700 more than two-third 667 (95.3%) were multipara. Concerning past obstetric history, 169 (24.1%) of them had not history of previous vaginal delivery, 27 (3.9%) of them had a history of chronic diseases, and 96 (18.9%) of them had the previous cesarean indication were recurrent, 258 (36.9%) had previous history of successful VBAC.
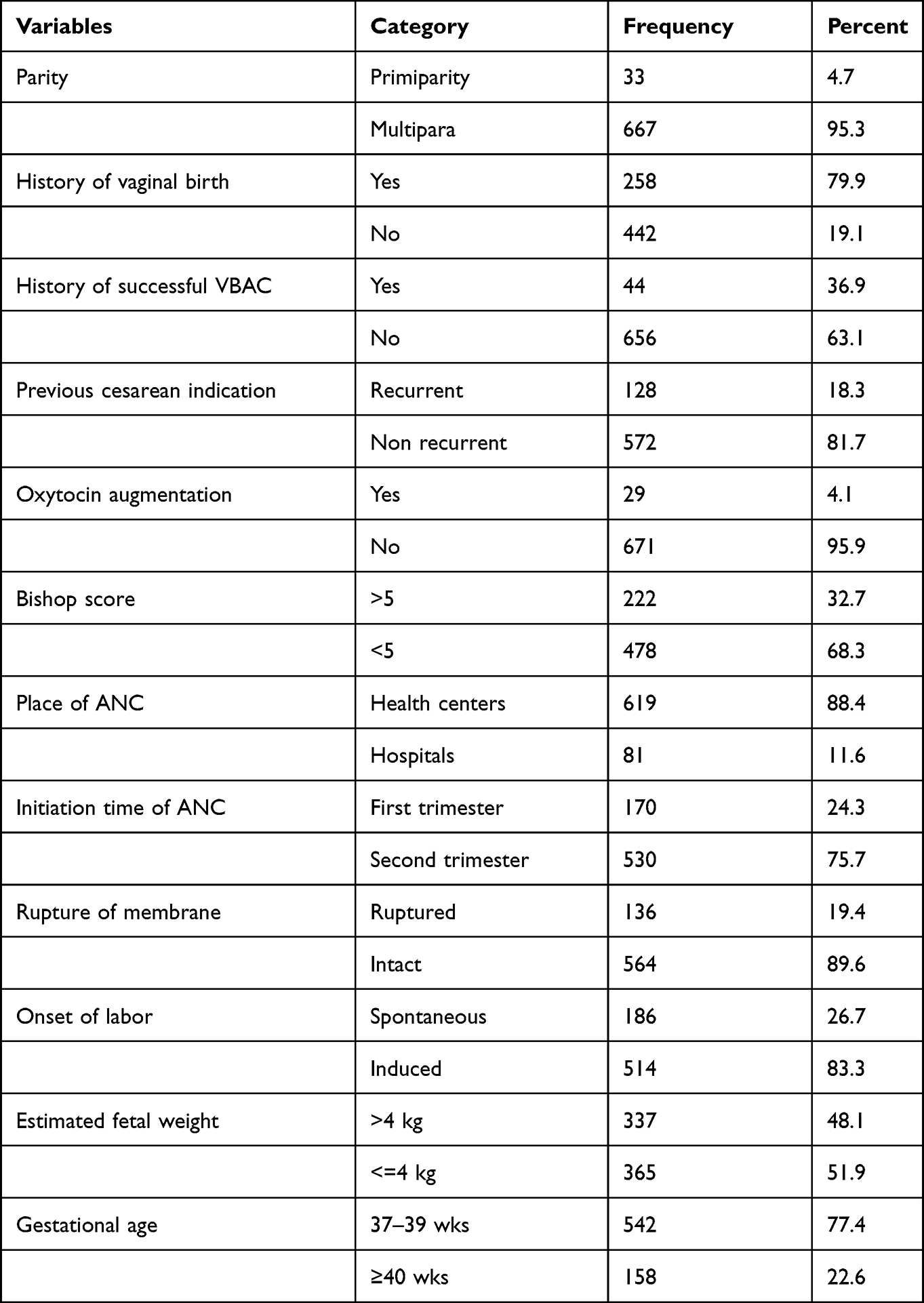 |
Table 2 Current and Past Obstetric-Related Factors of Mothers Who Gave Birth by VBAC at FHCSH from January 30/2019 to January 30/2021 |
Regarding current obstetric characteristics, 187 (26.7%) participants gave birth by spontaneous vaginal birth, the majority of the participants are bishop score of <=5478 (68.3%) and 136 (19.4%) of the participants had a history of rupture of membrane. 29 (4.1%) had oxytocin augmentation, 81 (11.6) % had ANC follow-up at hospitals during the current pregnancy.
Building of a Prediction Model for Vaginal Delivery Success Following Cesarean Section
Out of 700 trial of VBAC, 469 (67%) had successful VBAC. In the bivariate logistic regression analysis, variables with a P value less than 0.25 were, estimated fetal weight, educational status, previous history of vaginal delivery, previous history VBAC, place on ANC, initiation time of ANC, chronic disease, onset of labor, rupture of membrane, bishop Score, and parity (Table 3).
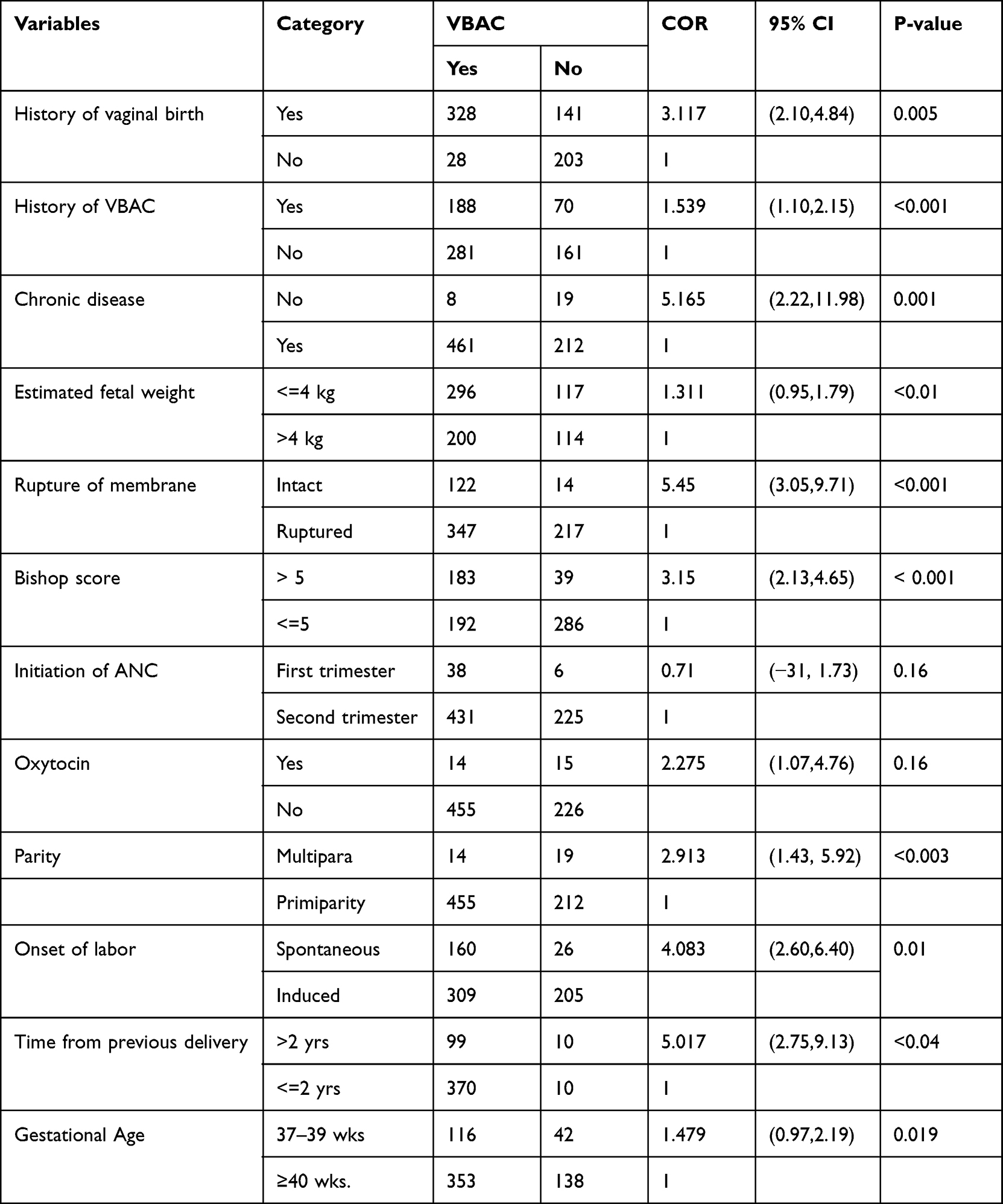 |
Table 3 Analysis of Bivariable logistic Regression to Construct a VBAC Prediction Model |
In Table 4, displays the findings of the multivariable analysis. In the final model, variables—prior success of VBAC, rupture of membranes, ANC initiation time, start of labor, parity, and time from previous delivery—were kept.
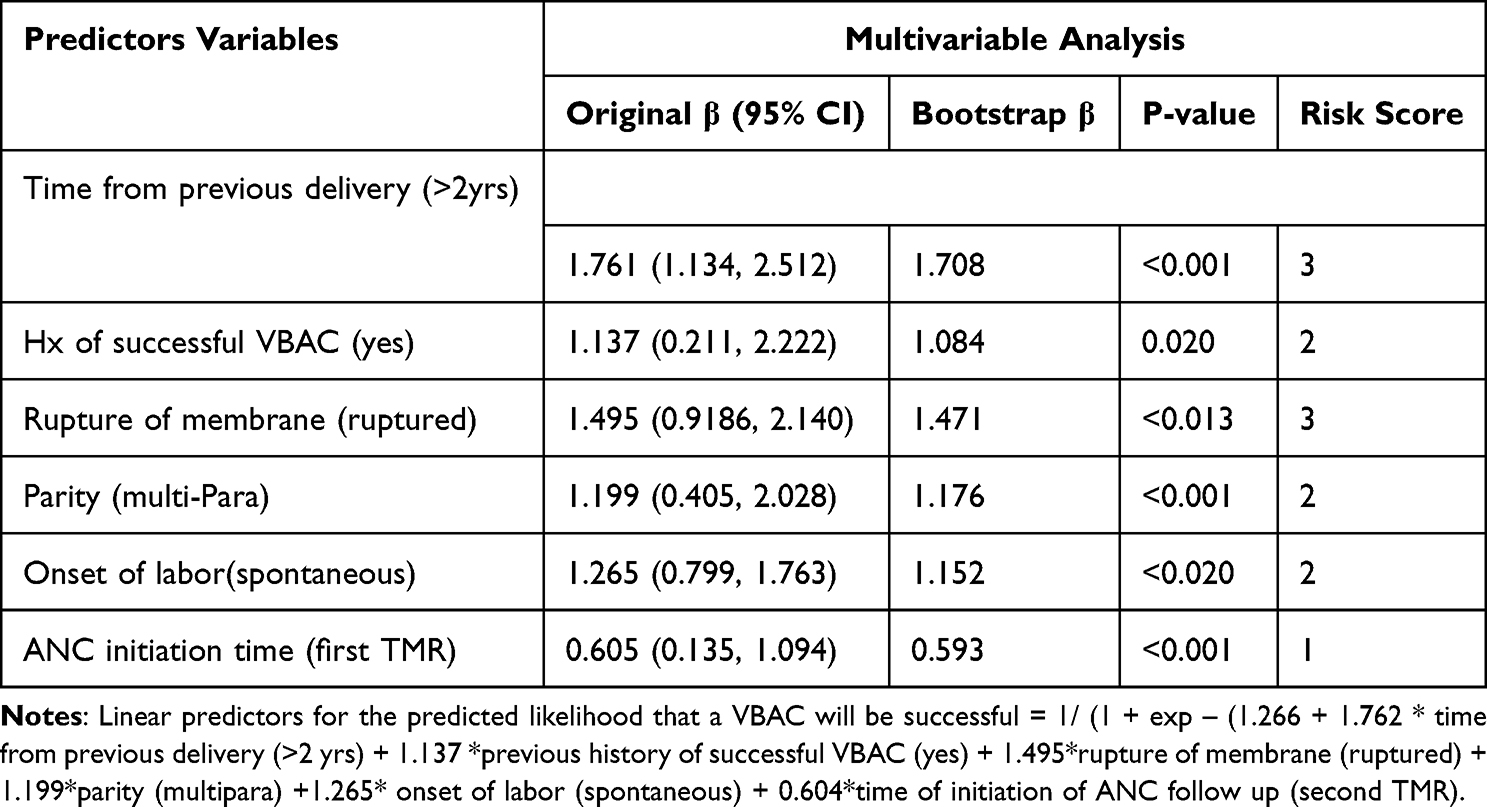 |
Table 4 Each Predictor’s Risk Scores and Coefficients Were Incorporated in the Model to Predict VBAC (n = 700) |
Receiver Operating Curve Analysis and Calibration Plot
(Figure 2) The discriminatory power of the model has AUC of 0.754 (95% CI: 0.720–0.787).
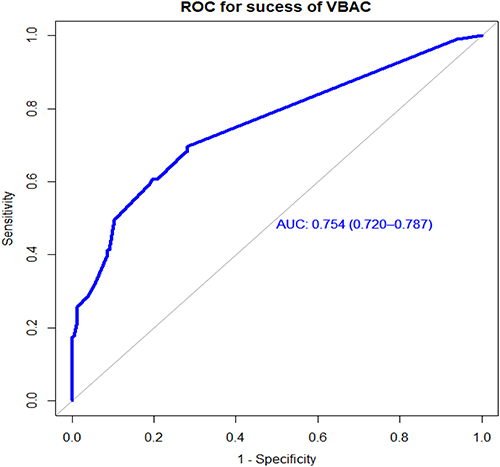 |
Figure 2 Area under the ROC curve for the prediction model success of VBAC. |
A better performance is shown by classifiers that provide curves that are closer to the top-left corner. A random classifier is anticipated to provide points that are diagonal by default (FPR = TPR). The ideal outcome would be the point (0, 1), which would represent 100% true positives and 0% false positives. The projected risk cutoff threshold using the coefficients () was a probability of (you den=0.4998); the model’s sensitivity, specificity, positive predictive value, and negative predictive value are all 69.7%, 71.8%, 83.4%, and 53.9%, respectively.
With an AUC of 0.744 (corrected 95% CI: 0.710–0.778), validation of the model using the bootstrap method revealed that there was rarely any evidence of excessive effect by specific observations (Figure 3).
 |
Figure 3 ROC (AUC) of risk prediction model after bootstrapping for success of VBAC among mothers who gave birth at FHCSH. |
Since observed and projected probabilities were similar, the calibration test resulted in a p-value of 0.255, indicating that the model did not visually misrepresent the data or that it was visually accurate (Figure 4).
 |
Figure 4 Predicted versus observed preterm birth probability in the sample. Calibration plot created using “givitiCalibrationBelt” in R programming. |
Decision Curve Analysis
It is abundantly evident that the model has the most clinical and public health value since it has the highest net benefit throughout the whole range of threshold probabilities. Thus, regardless of their risk thresholds, referral decisions made using the model have a better net benefit than not referring at all or referring everything (Figure 5).
 |
Figure 5 A decision curve plotting the net benefit of the model against threshold probability. |
Use of a Simplified Risk Score for Risk Classification
The simplified model’s prediction score was made simpler to use in real-world scenarios by rounding all regression coefficients. With an AUC of 0.748 (95% CI: 0.714–0.781), the simplified score showed extremely comparable prediction accuracy to the original coefficients. A mother’s score might range from 0 to 13, with 13 being the best possible result.
With a sensitivity of 68.23% and a specificity of 71.86%, the “Youden index” suggests a threshold score of 3 to predict the success of VBAC using risk scores. When the risk score was dichotomized into low risk (<3) and high risk (>3), 332 (47.4%) were classified as high risk and 368 (52.57%) as low risk for a successful VBAC (Table 5).
 |
Table 5 Utilizing a Streamlined Prediction Score, Classify the Risk of Successful VBAC (n = 700) |
Discussion
Utilizing maternal characteristics of mothers who gave delivery at FHCSH, the current study was created to establish and validate a risk score to predict the success of VBAC.
Predicting the likelihood of a successful VBAC in pregnant women is therefore crucial in order to take the proper action. A crucial responsibility for clinical care providers is identifying women who have a high chance of a successful VBAC. The approaches for accurately forecasting the success of VBAC in women are scarce in low and middle income countries, nonetheless. The explanation of maternal VBAC success factors was the main goal of prior research. In recent years, the emphasis has switched to predicting VBAC success as accurately as possible utilizing a combination of factors.
This retrospective analysis discovered maternal traits that could be used to create a reliable VBAC prediction risk score. Residence, parity, prior successful VBAC experience, membrane rupture, inter delivery gap, start of labor, and ANC initiation time are the best combinations of maternal characteristics to predict preterm birth.16
AUC for the model is 0.748 (95% CI: 0.714–0.781). Furthermore, we found that the sensitivity and specificity of this prediction model reached 68.23% and 71.86%, respectively, at the score threshold of 3, using (you den) as an ideal cut point.
In both high-income and low-income nations, VBAC has long been advocated as a practical way to lower overall cesarean birth rates.17 According to a sub-Saharan African study, when combined with cautious client selection and effective labor management, VBAC is safe and has success rates between 60% and 80%.18
However, significant obstacles to providing high-quality intrapartum care, such as uneven access to full emergency obstetric care functions, exist in low-income countries like Ethiopia. These countries therefore present considerable VBAC trialing issues.19
Moreover, a recent study in Ethiopia also showed the TOLAC rate is 38.5%.20 In our study, 67% of patients experienced a successful VBAC. This data is consistent with a meta-analysis that revealed a 69% success rate for VBAC in sub-Saharan African nations.19 In addition, similar results were found in other research, which also mentioned similar levels of VBAC success rates in the United States. (71%),21 India (73%),19 Ghana (61%),22 Nigeria (73%).23
The current study’s VBAC success rate was lower than that of studies conducted in Japan (91.5%),24 Australia (83%),25 and China (80%).26 It might be because the maternity care systems in these nations and Ethiopia differ.
The variances in TOLAC criteria and predictors of VBAC, such as prior obstetric performance like prior VBAC, ethnic differences, prior vaginal deliveries, and indication for prior cesarean deliveries, may be the cause of the disparity in VBAC success rates between studies.
Given that the study was conducted in comprehensive and referral hospitals for undergraduate and graduate students, the relatively high percentage of successful VBAC revealed in the current study may partly be due to the careful selection of cases for the provision of TOLAC.
This high level of overall success rates for VBACs should be utilized to advise expectant mothers on the next delivery method in situations like these.
According to research by Krait et al (19), which is comparable to my study, women who spontaneously go into labor are more likely to have a successful VBAC.
In this study, gestational age was not found to be a reliable indicator of success. There have been studies that show a bad correlation between poor outcomes and gestational ages exceeding 40 weeks.27
A successful delivery is over six times more likely when the inter-delivery gap is beyond two years. According to other investigations, a shorter time span was linked to less success than two years.28 This could be partly due to recall bias.
Similar to past research, it was discovered that a mother who had previously undergone a successful VBAC was associated with success24 Many authors reported history of prior spontaneous vaginal delivery as important determinant for success in VBAC. But our study failed to show this.
According to a study done in China, a model created with the use of gestational age, a history of successful VBACs, the rupturing of the membranes, the Bishop score, the start of labor, and the predicted birth weight may predict the overall success of VBAC with an AUC of.7 (0.70). This slightly differs from my study. This might occur as a result of the final model’s different predictor variable.29
My research is in line with a study done in America that used predictor variables such as mother age, BMI, past vaginal delivery, prior vaginal delivery, and indication for prior cesarean section to determine whether a VBAC would be successful with an AUC of (73.4)10 and an analysis of studies in western Europe found that ethnicity, pre-pregnancy BMI, prior cesarean for non-progressive labor, estimated fetal weight, and prior vaginal birth with AUC were all predictors of the outcome (72.3).30
There were various restrictions on this study. Due to the study’s retrospective nature, missing data cannot be avoided. Our obstetric patients come from a comprehensive and referral hospital, which may not accurately reflect Ethiopia’s population and restricts the generalizability to other diverse groups. The study also attempted to include extremely significant predictor factors that might play a substantial role for the prediction model, which is strength of the study.
Conclusion
In women with a prior history of CS, TOLAC had a comparatively high success rate (69%); this suggests that TOLAC could be a key tactic for lowering CS rates in Ethiopia. Therefore, the best combination of maternal traits, including parity, membrane rupture, the start of labor, prior history of VBAC, the time between deliveries, and the initiation of ANC, suggests the possibility of predicting the success of VBAC using a straightforward prediction model built from maternal traits.
Additionally, the model-based method of the original coefficients was comparable in accuracy to the risk score calculation based on a mixture of predictors. The prediction score was used to risk stratify pregnant women who had previously undergone only one cesarean section and to determine which of these women had a higher chance of successfully undergoing a VBAC. After that, a lady with a strong possibility of having a VBAC would be seen as a good candidate. The study’s model for TOLAC success prediction could be used to provide women who had their first caesarean delivery with more targeted TOLAC counseling.
Recommendation
For Researchers
The TOLAC success prediction model developed in the study has the potential to be a tool for more targeted TOLAC counseling for women who have had a primary caesarean delivery. To establish effectiveness prior to widespread implementation among Ethiopian women, additional prospective validation studies with bigger sample numbers and in the general population should be conducted.
For Mothers
Women with one previous should be made aware that the outcomes of TOS and inform TOS has the advantage of reducing long-term complications of having multiple cesarean scars. This will increase community awareness and thus early initiative to seek medical counseling among women with previous scar.
For Physicians
Physicians should consider different predictors studied by different scholars, those may have significant role in determination of success of vaginal delivery after cesarean surgery. I recommend health workers to consider and use clinical risk score developed by this research.
Acknowledgments
The study’s active participants, data collectors, and supervisors are all gratefully acknowledged by the authors.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Senturk MB, Cakmak Y, Atac H, Budak MS. Factors associated with successful vaginal birth after cesarean section and outcomes in rural area of Anatolia. Int J Womens Health. 2015;7:693–697. doi:10.2147/IJWH.S83800
2. Trojano G, Damiani GR, Olivieri C, et al. VBAC: antenatal predictors of success. Acta Biomed. 2019;90(3):300–309. doi:10.23750/abm.v90i3.7623
3. Berghella V. Obstetric Evidence Based Guidelines/Edited by Vincenzo Berghella. London: Informa Healthcare; 2007.
4. Sentilhes L, Vayssière C, Beucher G, et al. Delivery for women with a previous cesarean: guidelines for clinical practice from the French College of Gynecologists and Obstetricians (CNGOF). Eur J Obstetrics Gynecol Reproductive Biol. 2013;170(1):25–32. doi:10.1016/j.ejogrb.2013.05.015
5. Shao M-J, Hu M-X, Hu M. Temporary bilateral uterine artery occlusion combined with vasopressin in control of hemorrhage during laparoscopic management of cesarean scar pregnancies. J Minim Invasive Gynecol. 2013;20(2):205–208. doi:10.1016/j.jmig.2012.10.018
6. Durnwald CP, Mercer BM. Vaginal birth after Cesarean delivery: predicting success, risks of failure. J Mater Fetal Neonatal Med. 2004;15(6):388–393.
7. Patel RM, Jain L: Delivery after previous cesarean: short-term perinatal outcomes. In:
8. Minh T, Phuoc H. The success rate and associate factors of vaginal birth after cesarean section at Tu Du Hospital in Vietnam. Int J Pregnancy Child Birth. 2018;4(3):129–133.
9. Metz TD, Stoddard GJ, Henry E, Jackson M, Holmgren C, Esplin S. Simple, validated vaginal birth after cesarean delivery prediction model for use at the time of admission. Obstet Gynecol. 2013;122(3):571. doi:10.1097/AOG.0b013e31829f8ced
10. Tessmer-Tuck JA, El-Nashar SA, Racek AR, Lohse CM, Famuyide AO, Wick MJ. Predicting vaginal birth after cesarean section: a cohort study. Gynecol Obstet Invest. 2014;77(2):121–126. doi:10.1159/000357757
11. Schoorel E, Melman S, Van Kuijk S, et al. Predicting successful intended vaginal delivery after previous caesarean section: external validation of two predictive models in a Dutch nationwide registration‐based cohort with a high intended vaginal delivery rate. BJOG. 2014;121(7):840–847. doi:10.1111/1471-0528.12605
12. Berghella M. Recurrent pregnancy loss. In: Berghella V, editor. Obstetric Evidence-Based Guidelines. London: Taylor & Farancis; 2007:109–115
13. Metz TD, Allshouse AA, Faucett AM, Grobman WA. Validation of vaginal birth after cesarean delivery prediction model in women with two prior cesareans. Obstet Gynecol. 2015;125(4):948. doi:10.1097/AOG.0000000000000744
14. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/s0895-4356(96)00236-3
15. Misgan E, Gedefaw A, Negash S, Asefa A. Validation of a vaginal birth after cesarean delivery prediction model in teaching hospitals of Addis Ababa University: a cross-sectional study. Biomed Res Int. 2020;2020:1–9. doi:10.1155/2020/1540460
16. Filipose Mesay. Available from: http://ir.bdu.edu.et.
17. Horey D, Kealy M, Davey MA, Small R, Crowther CA. Interventions for supporting pregnant women’s decision‐making about mode of birth after a caesarean. Cochrane Database Sys Rev. 2013;7:548.
18. Boulvain M, Fraser WD, Brisson‐Carroll G, Faron G, Wallast E. Trial of labour after caesarean section in sub‐Saharan Africa: a meta‐analysis. BJOG. 1997;104(12):1385–1390. doi:10.1111/j.1471-0528.1997.tb11008.x
19. Tripathi JB, Doshi HU, Kotdawala PJ. Vaginal birth after one caesarean section: analysis of indicators of success. J Indian Med Assoc. 2006;104(3):113–115.
20. Siraneh Y, Assefa F, Tesfaye M. Feto-maternal outcome of vaginal birth after cesarean and associated factors among mothers with previous cesarean scar at Attat Lord Merry Primary Hospital, Gurage Zone, South Ethiopia. J Pregnancy Child Health. 2018;5(5):390. doi:10.4172/2376-127X.1000390
21. Maykin MM, Mularz AJ, Lee LK, Valderramos SG. Validation of a prediction model for vaginal birth after cesarean delivery reveals unexpected success in a diverse American population. Am J Perinatology Rep. 2017;7(1):e31–e38. doi:10.1055/s-0037-1599129
22. Seffah J, Adu-Bonsaffoh K. Vaginal birth after a previous caesarean section: current trends and outlook in Ghana. J West Af College Surgeons. 2014;4(2):1.
23. Hassan A. Trial of scar and vaginal birth after caesarean section. J Ayub Med College Abbottabad. 2005;17(1):57–61.
24. Wu Y, Kataria Y, Wang Z, Ming W-K, Ellervik C. Factors associated with successful vaginal birth after a cesarean section: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2019;19(1):1–12. doi:10.1186/s12884-019-2517-y
25. Mooney SS, Hiscock R, Clarke IDA, Craig S. Estimating success of vaginal birth after caesarean section in a regional Australian population: validation of a prediction model. Australian N Z J Obstetrics Gynaecol. 2019;59(1):66–70. doi:10.1111/ajo.12809
26. Fhkcog FO. Developing a pilot model to predict successful vaginal birth after caesarean section for Hong Kong Chinese women. Hong Kong J Gynaecol Obstetrics Midwifery. 2017;17(1):24–29.
27. Shorten A, Shorten B, Kennedy HP. Complexities of choice after prior cesarean: a narrative analysis. Birth. 2014;41(2):178–184. doi:10.1111/birt.12082
28. Berghella M. Recurrent Pregnancy Loss. Berghella V Obstetric evidence based guidelines London Informa UK Ltd; 2007:109–115.
29. Li Y-X, Bai Z, Long D-J, et al. Predicting the success of vaginal birth after caesarean delivery: a retrospective cohort study in China. BMJ open. 2019;9(5):e027807. doi:10.1136/bmjopen-2018-027807
30. Schoorel E, Van Kuijk S, Melman S, et al. Vaginal birth after a caesarean section: the development of a W estern E uropean population‐based prediction model for deliveries at term. BJOG. 2014;121(2):194–201. doi:10.1111/1471-0528.12539
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.